
Abstract
Background
Bloodstream infections (BSI) and delirium are frequent in critically ill patients. During systemic inflammatory response to BSI, cytokines may interact with neurotransmitters and neuronal receptors driving acute brain dysfunction. However, prospectively collected data on incidence, prediction and impact of delirium in association with BSI are lacking. This study aimed to determine the incidence and predictors of new-onset delirium and its impact on outcome in critically ill adult patients with BSI.
Methods
From 2011 to 2014, all consecutive adult patients with BSI treated in the intensive care units of an academic medical care center were identified. Pertinent clinical and microbiological data including the Intensive Care Delirium Screening Checklist (ICDSC) were assessed. Multivariable analysis was performed to identify variables independently associated with ICDSC ≥4.
Results
Among 240 patients, 145 (60%) had an ICDSC ≥4 (i.e., delirium). In-hospital mortality was 34%. Delirious patients had a higher mortality (40 vs. 23%; p = 0.005), a lower proportion with return to functional baseline (30 vs. 46%; p = 0.012), and a higher proportion with unfavorable outcome in survivors (74 vs. 54%; p = 0.010). Multivariable analyses revealed age (OR 1.04, 95% CI 1.02–1.06), male gender (OR 2.26, 95% CI 1.17–4.36), and the number of catheters and drainages before diagnosis of BSI (OR for every additional catheter = 1.14, 95% CI 1.04–1.25) as independent predictors for delirium (adjusted for SAPS [simplified acute physiology score] II, Riker Sedation-Agitation Scale [SAS], Sequential Organ Failure Assessment [SOFA] score, dementia and/or leukoencephalopathy, and albumin levels).
Conclusions
The incidence of delirium in patients with BSI is high and associated with adverse outcome. The number of catheters and drainages may constitute a useful and readily available predictor of delirium in patients with BSI allowing to identify patients at high risk. Ultimately, reliable identification of patients at increased risk for delirium is key for allocation of specific prevention strategies.
Similar content being viewed by others


Background
Sepsis and delirium are frequent and associated with high morbidity and mortality in critically ill patients treated in intensive care units (ICUs) [1, 2]. Sepsis affects more than 25% [3–5], and delirium is present in as many as 80% of mechanically ventilated patients [6–8] and in up to 50% of non-mechanically ventilated patients [9–11]. They often concur, and a number of recent studies provide evidence of complex underlying mechanisms explaining how systemic inflammatory response drives acute brain dysfunction, possibly explaining this association. Systemic inflammation may disturb the integrity of the central nervous system by an increased production and release of cytokines interacting with the somatic autonomic nerve fibers. Associated changes in brain perfusion, and increased diffusion of cytokines through the loosened blood–brain barrier mainly in the circumventricular areas, the choroid plexus [12], or through saturable transport mechanisms [13] may further fuel these interactions. In addition, anorexia, lethargy, and depression in temporal association with systemic inflammation and fever, collectively named sickness behavior, are observed as a response of neurons to cytokines in different animal models [14, 15] and humans [16]. Although it seems evident that activation of the immune system can induce acute brain dysfunction and that sepsis, therefore, is a major risk factor for delirium, most studies are hampered by the fact that sepsis encompasses a variety of different sources and states of infection and do not focus on the immediate and acute neurological impact of specific infections in critical care settings. Although bloodstream infections (BSI) belong to the most important, frequent, and clearly defined infections encountered in ICUs, prospective studies regarding the incidence, prediction, and impact of delirium in association with BSI are not yet published.
We therefore sought to determine incidence and predictors of new-onset delirium and its impact on outcome in critically ill adult patients with BSI.
Methods
This study was performed in the ICUs of the University Hospital Basel, Switzerland, an academic tertiary medical care center treating more than 47,000 emergencies and with more than 35,000 admissions per year. Patients were derived from an ongoing prospective cohort of patients with BSI [17].
The study was approved by the local ethics committee (Ethikkommission Nordwest-und Zentralschweiz, Nr. 2014/165) according to the declaration of Helsinki, and patients’ consent was waived.
Demographics and clinical characteristics
From 2011 to 2014, all consecutive adult patients with BSI treated in the medical or surgical ICUs of an academic medical care center were identified. Patients without consecutive ICDSC scoring or with delirium prior to the diagnosis of BSI were excluded. We assessed pertinent clinical, laboratory, and microbiological data including principal diagnoses, the SAPS II scores, comorbidities, transient episodes of coma on the day of BSI diagnosis, and serum levels of acute-phase proteins as described below. Treatment characteristics of all patients were assessed including ICU and hospital stay, duration of mechanical ventilation, the number of catheters and drainages, the use of anesthetics and sedatives during the three days prior to BSI, and the administration of anesthetics and neuroleptic drugs during the three days following BSI. The Intensive Care Delirium Screening Checklist (ICDSC) and outcomes were assessed as mentioned below.
Sedation protocol
In all patients treated with sedatives, sedation was managed and titrated by using the Riker Sedation-Agitation Scale (SAS). In all patients treated with sedatives, daily interruption of sedation was an integral component of the sedation protocol. To establish sedation, short active sedatives such as disoprivan were preferred providing absence of hemodynamic instability. In patients with hemodynamic instability, sedation was achieved by administration of benzodiazepines given at the lowest possible dose and titrated according to the sedation level as determined by SAS.
Definition and detection of infections and BSIs
A protocol for monitoring infections was established for all patients in the ICUs during the entire study period. It included drawing cultures of blood and urine, cultures from tracheal aspirates or sputum, and performance of a chest X-ray in any patient with new onset of fever or hypothermia. If other foci were suspected, these were sampled accordingly. Infections were diagnosed based on the patients’ clinical examination, radiological exams, laboratory findings, and microbiological results according to the Centers for Disease Control and Prevention (CDC) criteria [18]. The diagnosis of BSI was defined according to the current guidelines [19] and confirmed by two infectious diseases specialists in patients with at least one positive blood culture and concurrent presence of the systemic inflammatory response syndrome. Systemic inflammatory response was diagnosed if two or more of the following criteria were fulfilled: body temperature >38 or <36 °C; heart rate >90/min; respiratory rate >20/min; serum leukocyte count >12 or <4 G/L or the presence of >10% immature neutrophil granulocytes in the blood samples. Catheter-related BSI was defined according to the CDC criteria (www.cdc.gov/hai/bsi/bsi.html).
New definitions for sepsis and septic shock were published in 2016 [20], recommending to define sepsis as life-threatening organ dysfunction, captured by the Sequential [Sepsis-related] Organ Failure Assessment (SOFA) score, and defining septic shock as the need for vasopressors to maintain a mean arterial blood pressure of ≥65 mmHg and serum lactate level >2 mmol/L in the absence of hypovolemia. Therefore, we retrospectively collected the respective information to calculate the SOFA score and to identify septic shock accordingly.
Definition and detection of new-onset delirium
Among several screening methods to detect delirium in ICUs, the Confusion Assessment Method for the ICU (CAM-ICU) [6] and the Intensive Care Delirium Screening Checklist (ICDSC) [9] have been most frequently employed. Both have been recommended for the screening of delirium in ICUs by the Society of Critical Care Medicine based on high-quality evidence. [21] Direct comparisons of the diagnostic accuracy of the CAM-ICU and the ICDSC have been performed in recent studies with heterogenous ICU populations revealing a higher sensitivity and specificity of the ICDSC than the CAM-ICU [22–24].
Based on these data, in our institution, the ICDSC is daily assessed in all ICU patients. For the present study, the ICDSC scores on the day before, the day of, and the day following diagnosis of BSI were used. To reduce the interference of sedation in mechanically ventilated patients, ICDSC assessments were performed in mechanically ventilated patients after routine daily interruption of sedation at our institution.
According to the studies and guidelines mentioned above, an ICDSC ≥4 was defined as delirium [9, 21].
Measurements of acute-phase proteins
For the present study, serum levels of acute-phase proteins (including CRP [C-reactive protein] and albumin), measured daily in all consecutive patients during the study period, were included on the day before, the day of, and the day following the diagnosis of BSI. CRP concentrations were determined by an enzyme immunoassay with a detection limit of 0.5 mg/l (EMIT; Merck Diagnostica, Switzerland). Values <10 mg/l are considered as normal.
Outcomes
The primary outcome was the development of delirium ±24 h around the diagnosis of BSI. Secondary outcomes were death during the same hospital stay, and return to functional baseline and unfavorable outcome in survivors defined as a Glasgow Outcome Score (GOS) of 1–3 at discharge.
Statistics
The Chi-square and Fisher exact test (where appropriate) were used for comparisons of proportions. For continuous variables, the Shapiro–Wilk test was used to distinguish between normal and abnormal distributions. Normally distributed variables were analyzed using the Student’s t test and non-normally distributed variables using the Mann–Whitney U test. To address possible confounding, all variables found to be significant in univariable analyses and known risk factors (i.e., SAPS II, dementia/leukoencephalopathy) were included in the multivariable regression models after calculating odds ratios by logistic regression. In addition, SAS and SOFA were included into the multivariable logistic regression model to correct for the effects of sedation and organ failure on ICDSC scores [25]. Stepwise logistic regression using stepwise forward and backward selection, as well as Akaike information criterion (AIC), was applied to identify variables independently associated with ICDSC ≥4, and collinearity between covariates was assessed.
The Hosmer–Lemeshow goodness-of-fit test was applied to check the final models. Areas under the receiver operating characteristic (ROC) curve were calculated for the final models to evaluate discrimination.
Two-sided p values ≤0.05 were considered statistically significant. Statistical analyses were performed with STATA® version 13.0 (Stata Corp., College Station, TX).
Results
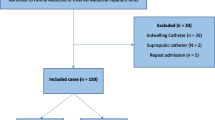
A total of 309 patients with BSI fulfilled the study criteria: 69 patients without consecutive ICDSC scores on all three defined days or with delirium prior to the diagnosis of BSI were excluded. There was no significant difference regarding all baseline characteristics, complications, and outcomes between the excluded and included patients. In the remaining 240 patients, median age was 68 years (interquartile range [IQR] 58–77), median ICU stay was 7 days (IQR 3–19), and median hospital stay 28 days (IQR 15–54). During intensive care, 141 patients (58.8%) were mechanically ventilated for a median of 8 days (IQR 3–19) and the median number of catheters and drainages per patient was 6 (IQR 4–9).
New-onset delirium, defined as an ICDSC ≥4 ± 24 h around BSI diagnosis, was identified in 145 (60%) patients with BSI. The median duration of new-onset delirium was 4 days (IQR 2–8). The median time from admission to BSI and delirium was 7 days (IQR 2–16) and 8 days (IQR 2–19), respectively. Delirium emerged in most patients immediately before or together with the diagnosis of BSI (in 75 patients [51.7%] on the day before BSI, in 50 patients [34.5%] on the day of BSI diagnosis, and in 20 patients [13.8%] one day following BSI diagnosis). The distribution of the highest ICDSC ±24 h around BSI diagnosis in patients with and without delirium is presented in Fig. 1. In delirious patients, 85.5% had an ICDSC of 4–6. The ICDSC of our patients with a ICDSC <4 was 1–3 in 72.6%, representing a significant proportion of patients with “sub-syndromal delirium.” The use of anesthetics and sedatives three days prior to BSI did not significantly differ between patients with and without an ICDSC ≥4 (40 vs. 35.8%; p = 0.512). The univariable comparisons of demographics, baseline characteristics, and details regarding BSIs between patients with BSI with and without new-onset delirium are presented in Tables 1 and 2. Among all patients with BSI, 92 (26.1%) developed septic shock. Serum levels of CRP and leukocytes on the day before, the day of, and the day after BSI diagnosis did not differ between delirious and non-delirious patients. Comparisons of treatment characteristics and outcomes are summarized in Table 3. In delirious patients, mortality was 33.8%. Delirious patients had an almost twofold increased mortality, a lower proportion with return to functional baseline, and a higher proportion with unfavorable outcome in survivors, as compared to non-delirious patients (Table 3). Multivariable analyses revealed that delirium was independently associated with death in our cohort (adjusting for well-established outcome predictors in ICU patients, such as age, SAPSII score, the Charlson Comorbidity Index, and albumin serum levels at admission, OR 1.90, 95% CI 1.01–3.63; p = 0.049). In univariable analysis, delirious patients were older, more often male, had lower median albumin serum levels at admission, prolonged ICU stay, and had more catheters and drainages before the diagnosis of BSI (Tables 1, 3). Every additional catheter or drainage increased the probability of delirium (ORfor every catheter/drainage = 1.14, 95% CI 1.05–1.24; p = 0.002; Fig. 2). The number and duration of mechanical ventilation did not differ between patients with and without delirium (Table 3). The sources of BSI, the distribution of gram-positive and gram-negative pathogens, and the number of infectious complications did not differ significantly between patients with and without delirium (Table 2). Most BSIs were catheter-related not differing between patients with and without delirium.

Distribution of the maximal ICDSC ±24 h around diagnosis of bloodstream infections in patients with and without delirium. ICDSC the Intensive Care Delirium Screening Checklist

Probability of an ICDSC ≥4 during bloodstream infections in relation to the number of catheters and drainages. ICDSC Intensive Care Delirium Screening Checklist, CI confidence interval
Uni- and multivariable logistic regression analyses including characteristics significantly differing between patients with and without delirium (Tables 1, 3), as well as established risk factors for delirium (i.e., SAPS II, dementia/leukoencephalopathy) and SAS and SOFA scores to correct for the effects of sedation and organ failure on ICDSC are shown in Table 4. All three stepwise selection approaches revealed older age, male gender, and the number of catheters and drainages as predictors for delirium, independent of possible confounders (i.e., age, gender, SAPS II, SAS, SOFA scores, dementia and/or leukoencephalopathy, and albumin serum levels). The mean variance inflation factor for all variables included in the multivariable models was 1.26, ranging from 1.03 to 1.68, ruling out high collinearity and indicating that the selected variables are independent from other predictors. The Hosmer–Lemeshow goodness-of-fit test for the model selection by AIC was χ 2 = 4.67 (p = 0.792) and for the stepwise forward and backward selection was χ 2 = 9.45 (p = 0.306), indicating adequate model fit. The area under the ROC curve for the stepwise regression model was 0.072 supporting its ability to discriminate between patients with and without ICDSC ≥4 during BSI.
Discussion
New-onset delirium in adult ICU patients with BSI is frequent and associated with increased morbidity and mortality. In our study, the incidence of new-onset delirium in close temporal association with BSI diagnosis (60%) is in the upper range of the incidence in the general ICU population (23–65%) [26], suggesting that BSI in critically ill patients may have a promotional effect on the development of delirium. In addition, the ICDSC of our patients with an ICDSC <4 was 1–3 in 72.6%, representing a significant proportion of patients with “sub-syndromal delirium” in close temporal relation to BSI. Similar to published studies, our multivariable analyses confirm that established risk factors for acute brain dysfunction in critically ill patients including older age [26], male gender, and low serum levels of albumin [27] are predictors of new-onset delirium in close temporal association with the diagnosis of BSI. Other well-known predictors for delirium in the general ICU population identified by a recent large systematic review [26] seem to have no significant influence on the development of delirium in the context of BSI, such as altered level of consciousness, or surgery. However, interpretations regarding the association between trauma and delirium in our study are hampered, as patients with trauma are underrepresented in our cohort. The underlying mechanisms of male gender being a predisposing factor for delirium are not fully understood. Our finding that males in our cohort were suffering more often from delirium than females is in line with other studies describing delirium more frequently in males in different clinical settings, such as in surgical ICUs [28] and in elderly patients of general medical and surgical wards [29, 30]. However, other studies of ICU populations did not confirm such an association.
A new finding compared to published studies was the number of catheters and drainages per patient prior to the diagnosis of BSI as another independent predictor of new-onset delirium. At first glance, the odds ratio of 1.14 for delirium by the number of catheters and drainages may seem small. However, it has to be taken into account that they are given for each additional catheter or drainage. Hence, the odds for delirium increases for example with two additional catheters by 28%. Given the inherent limitations of observational data, we attempted to overcome confounding by including all variables known or assumed to impact the emergence of delirium and characteristics differing significantly different between delirious and non-delirious patients in our cohort into the multivariable models. Therefore, the SAPS II score and transient episodes of coma [26] prior to BSI diagnosis were included in our multivariable models. Three different stepwise model selection techniques were applied, all yielding identical results, underlining the robustness of our results. We acknowledge that the association between the number of catheters and drainages and delirium identified in our cohort may still be confounded by unmeasured variables associated with both the use of catheters and drainages and delirium. Our result is, however, supported by other studies identifying use of physical restraints as an important risk factor for the development of delirium [31]. Catheters and drainages preclude mobilization and have been associated with delirium in cardiac surgery patients [32]. Use of restraint was identified as a risk factor for delirium in mechanically ventilated patients [33] and in a multicenter study of ICU patients, which, however, could not assess its independent predictive value [34]. In our cohort, the use of lines was related to delirium despite the fact that all patients were subjected to a systemic inflammatory response triggered by bacteremia—another important contributor to delirium—underscoring its independent contribution.
Strong systemic inflammatory responses can induce acute brain dysfunction. Pro-inflammatory cytokines, particularly interleukin (IL)-1beta and tumor necrosis factor alpha (TNF-alpha), are produced in the periphery, interact with the brain, and initiate cytokine synthesis in the central nervous system [35]. Another major hypotheses trying to explain inflammation-related acute brain dysfunction is the change in neurotransmitters in relation to inflammation. In a study of septic animals, the use of cholinergic agonists improved cognitive performance [36], indicating that cholinergic neurons may be particularly sensitive to systemic inflammation and acute stressors, such as infections, influence the GABA-A complex by altering binding sites and modulating the expression of selective GABA-A receptor subunits [37].
The results of our study and the examples of pathophysiologic aspects outlined above suggest a direct pathomechanistic link between BSI, systemic inflammatory response and acute brain dysfunction expressed as delirium, calling for heightened awareness for new-onset delirium in critically ill patients with BSI. The number of catheters and drainages in ICU patients may constitute a useful and readily available predictor of delirium in patients with BSI allowing to identify patients at high risk. Furthermore, the number of catheters and drainages represents a potential target in the prevention of delirium, as it seems the number of insertion sites is modifiable and likely to further drive delirium in ICU patients. While catheters and drainages are inserted for specific indications and therefore cannot be omitted in most cases, our findings suggest that emphasis should be placed on removing such accesses as soon as possible not only for prevention of catheter-related infections but also for prevention of delirium. In addition, the use of multi-lumen catheters with the aim of reducing the number of insertion sites may be an important consideration in patients at high risk for delirium.
Our cohort is representative of other adult ICU populations, reflected by median age [6, 10, 11, 24, 38], distribution of gender, the SAPS II [24, 38], the duration of delirium [39], the Charlson Comorbidity Index [10, 11, 38], the proportion of patients with mechanical ventilation [10, 24], ICU stay [10, 38] being similar to prior studies of delirium in ICU patients. However, mortality was higher in our cohort as compared to international epidemiological multicenter studies of delirium [10, 38], possibly indicating an intensifying effect on mortality by the concurrence of BSI and the genesis of delirium.
The limitations of this study include the observational single-center design and the restriction of our cohort to the ICUs. Hence, our results are limited to critically ill ICU patients. However, demographics, clinical characteristics, and outcomes in our cohort are similar to those in prior studies of delirium. Our results that traumatic brain injury and dementia were not predictive for the emergence of delirium in BSI patients need to be interpreted with great caution, as there was only a small number of dementia and traumatic brain injury in our cohort. Our analysis can only provide associations and inference regarding causality cannot be drawn. Despite our attempt to overcome confounding by using multivariable models including well-established confounders, unmeasured residual confounding may have occurred. The fact that delirium was diagnosed by using the ICDSC score limits the generalizability or our results to studies and cohorts examined and rated with the same checklist. However, among several screening methods to detect delirium in ICUs, the CAM-ICU scale [6] and the ICDSC [9] have been most frequently employed. Both have been equally recommended for the screening of delirium in ICUs by the Society of Critical Care Medicine Pain, Agitation, and Delirium guidelines based on high-quality evidence [21]. Direct comparisons of the diagnostic accuracy of the CAM-ICU and the ICDSC have been performed in recent studies with heterogenous ICU populations revealing a higher sensitivity and specificity of the ICDSC than the CAM-ICU [22–24]. The indications for the placement of catheters and drainages may be related to the development of delirium in our cohort. However, the exact indication for the use of catheters could not be identified reliably, especially, as in many patients several different indications concur. Due to the retrospective study design, consecutive data regarding cumulative sedative drug administration could not be assessed. However, such information would be critical, as the cumulative drug administration does not represent the actual individual serum concentrations of the drugs over time, as they largely depend on individual factors, such as renal or liver function, and body weight. In addition, individual drug sensitivity would not be addressed. We further acknowledge that despite daily stopping of sedation and the use of short acting anesthetics, a slight remaining sedative effect may have still influenced the ICDSC assessment—a shortcoming that can only be overcome by excluding mechanically ventilated and sedated patients resulting in a highly selected population not representative of general ICU populations.
Conclusions
The incidence of new-onset delirium in critically ill patients with BSI is high and associated with increased mortality and unfavorable outcome in survivors calling for heightened awareness and rigorous screening for delirium in patients with BSI during intensive care. Older age, male gender, and the number of catheters and drainages are independent predictors of delirium in close temporal association with BSI. The number of catheters and drainages may constitute a useful and readily available predictor of delirium in patients with BSI allowing to identify patients at high risk. Further studies are needed to externally validate our findings. Ultimately, reliable identification of patients at increased risk of delirium is key for allocation of specific prevention strategies.
Abbreviations
- AIC:
-
Akaike information criterion
- BSI:
-
bloodstream infections
- CAM-ICU:
-
Confusion Assessment Method for the ICU
- CDC:
-
Centers for Disease Control and Prevention
- CI:
-
confidence interval
- CRP:
-
C-reactive protein
- GOS:
-
Glasgow Outcome Score
- ICDSC:
-
Intensive Care Delirium Screening Checklist
- ICU:
-
intensive care unit
- IQR:
-
interquartile range
- OR:
-
odds ratio
- ROC:
-
receiver operating characteristic
- SAPS:
-
simplified acute physiology score
References
Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787–94.
Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291(14):1753–62.
Padkin A, Goldfrad C, Brady AR, et al. Epidemiology of severe sepsis occurring in the first 24 hrs in intensive care units in England, Wales, and Northern Ireland. Crit Care Med. 2003;31(9):2332–8.
Finfer S, Bellomo R, Lipman J, et al. Adult-population incidence of severe sepsis in Australian and New Zealand intensive care units. Intensive Care Med. 2004;30(4):589–96.
Alberti C, Brun-Buisson C, Burchardi H, et al. Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Med. 2002;28(2):108–21.
Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286(21):2703–10.
Girard TD, Kress JP, Fuchs BD, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008;371(9607):126–34.
Pandharipande PP, Pun BT, Herr DL, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA. 2007;298(22):2644–53.
Bergeron N, Dubois MJ, Dumont M, et al. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27(5):859–64.
Salluh JI, Soares M, Teles JM, et al. Delirium epidemiology in critical care (DECCA): an international study. Crit Care. 2010;14(6):R210.
Thomason JW, Shintani A, Peterson JF, et al. Intensive care unit delirium is an independent predictor of longer hospital stay: a prospective analysis of 261 non-ventilated patients. Crit Care. 2005;9(4):R375–81.
Vitkovic L, Konsman JP, Bockaert J, et al. Cytokine signals propagate through the brain. Mol Psychiatry. 2000;5(6):604–15.
Comim CM, Vilela MC, Constantino LS, et al. Traffic of leukocytes and cytokine up-regulation in the central nervous system in sepsis. Intensive Care Med. 2011;37(4):711–8.
Bluthe RM, Michaud B, Poli V, et al. Role of IL-6 in cytokine-induced sickness behavior: a study with IL-6 deficient mice. Physiol Behav. 2000;70(3–4):367–73.
Cartmell T, Poole S, Turnbull AV, et al. Circulating interleukin-6 mediates the febrile response to localised inflammation in rats. J Physiol. 2000;526(Pt 3):653–61.
Reichenberg A, Yirmiya R, Schuld A, et al. Cytokine-associated emotional and cognitive disturbances in humans. Arch Gen Psychiatry. 2001;58(5):445–52.
Elzi L, Babouee B, Vogeli N, et al. How to discriminate contamination from bloodstream infection due to coagulase-negative staphylococci: a prospective study with 654 patients. Clin Microbiol Infect. 2012;18(9):E355–61.
Garner JS, Jarvis WR, Emori TG, et al. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16(3):128–40.
Centers for Disease Control and Prevention. CDC/NHSN surveillance definitions for specific types of infections. Centers for Disease Control and Prevention; (updated 01.08.2014; cited 2016 10.01.2016). Available from http://www.cdc.gov/nhsn.
Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–10.
Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306.
van Eijk MM, van Marum RJ, Klijn IA, et al. Comparison of delirium assessment tools in a mixed intensive care unit. Crit Care Med. 2009;37(6):1881–5.
Gusmao-Flores D, Salluh JI, Dal-Pizzol F, et al. The validity and reliability of the Portuguese versions of three tools used to diagnose delirium in critically ill patients. Clinics (Sao Paulo). 2011;66(11):1917–22.
Nishimura K, Yokoyama K, Yamauchi N, et al. Sensitivity and specificity of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and the Intensive Care Delirium Screening Checklist (ICDSC) for detecting post-cardiac surgery delirium: a single-center study in Japan. Heart Lung. 2016;45(1):15–20.
Haenggi M, Blum S, Brechbuehl R, et al. Effect of sedation level on the prevalence of delirium when assessed with CAM-ICU and ICDSC. Intensive Care Med. 2013;39(12):2171–9.
Zaal IJ, Devlin JW, Peelen LM, et al. A systematic review of risk factors for delirium in the ICU. Crit Care Med. 2015;43(1):40–7.
Scholz AF, Oldroyd C, McCarthy K, et al. Systematic review and meta-analysis of risk factors for postoperative delirium among older patients undergoing gastrointestinal surgery. Br J Surg. 2016;103:e21–8.
Aldemir M, Ozen S, Kara IH, et al. Predisposing factors for delirium in the surgical intensive care unit. Crit Care. 2001;5(5):265–70.
Schor JD, Levkoff SE, Lipsitz LA, et al. Risk factors for delirium in hospitalized elderly. JAMA. 1992;267(6):827–31.
Millar HR. Psychiatric morbidity in elderly surgical patients. Br J Psychiatry. 1981;138:17–20.
Mehta S, Cook D, Devlin JW, et al. Prevalence, risk factors, and outcomes of delirium in mechanically ventilated adults. Crit Care Med. 2015;43(3):557–66.
McPherson JA, Wagner CE, Boehm LM, et al. Delirium in the cardiovascular ICU: exploring modifiable risk factors. Crit Care Med. 2013;41(2):405–13.
Micek ST, Anand NJ, Laible BR, et al. Delirium as detected by the CAM-ICU predicts restraint use among mechanically ventilated medical patients. Crit Care Med. 2005;33(6):1260–5.
Van Rompaey B, Elseviers MM, Schuurmans MJ, et al. Risk factors for delirium in intensive care patients: a prospective cohort study. Crit Care. 2009;13(3):R77.
van Gool WA, van de Beek D, Eikelenboom P. Systemic infection and delirium: when cytokines and acetylcholine collide. Lancet. 2010;375(9716):773–5.
Comim CM, Pereira JG, Steckert A, et al. Rivastigmine reverses habituation memory impairment observed in sepsis survivor rats. Shock. 2009;32(3):270–1.
Mora F, Segovia G, Del Arco A, et al. Stress, neurotransmitters, corticosterone and body-brain integration. Brain Res. 2012;1476:71–85.
van Eijk MM, Roes KC, Honing ML, et al. Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-blind, placebo-controlled randomised trial. Lancet. 2010;376(9755):1829–37.
Klein Klouwenberg PM, Zaal IJ, Spitoni C, et al. The attributable mortality of delirium in critically ill patients: prospective cohort study. BMJ. 2014;349:g6652.
Authors’ contributions
Dr. RS and TD planned the work, acquired and interpreted the data, and wrote the manuscript. Dr. ST-S performed the statistical analyses and helped in writing the manuscript. Drs. AFW, SM, and SR interpreted the data, revised the manuscript, and substantially contributed to the inaugural draft. All authors read and approved the final manuscript.
Competing interests
TD has no competing interests. Dr. ST-S is a member of the Fidaxomicin advisory board and is a recipient of a research grant by Astellas. Dr. AFW, member of advisory boards of MSD, Astella, and Roche, and recipient of grants of the Swiss government and an unrestricted grant from BODE, Hamburg. Dr. SR received unconditional research grants from UCB-pharma. He received honoraria from serving on the scientific advisory boards of Desitin, Eisai, GSK, and UCB-pharma, travel grants from GSK, Janssen-Cilag, UCB-pharma, speaker fees from UCB-pharma and from serving as a consultant for Eisai, GlaxoSmithKline, Janssen-Cilag, Pfizer, Novartis, and UCB-pharma. He does not hold any stocks of any pharmaceutical industries or manufacturers of medical devices. Dr. SM reports no competing interests. Dr. RS was supported by the Research Fund of the University Basel, the Scientific Society Basel, and the Gottfried Julia Bangerter-Rhyner Foundation. He received personal grants from UCB-pharma and holds stocks from Novartis and Roche.
The corresponding author had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. No funding was received for this study. This study was performed and designed without the input or support of any pharmaceutical company or other commercial interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Dittrich, T., Tschudin-Sutter, S., Widmer, A.F. et al. Risk factors for new-onset delirium in patients with bloodstream infections: independent and quantitative effect of catheters and drainages—a four-year cohort study. Ann. Intensive Care 6, 104 (2016). https://doi.org/10.1186/s13613-016-0205-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-016-0205-x