
Abstract
Background
Improving access to facility-based delivery care has the potential to reduce maternal and newborn deaths across settings. Yet, the access to a health facility for childbirth remains low especially in low-income settings. To inform evidence-based interventions, more evidence is needed especially accounting for demand- and supply-side factors influencing access to facility-based delivery care. We aimed to fill this knowledge gap using data from Tanzania.
Methods
We used data from a cross-sectional survey (conducted in January 2012) of 150 health facilities, 1494 patients and 2846 households with women who had given births in the last 12 months before the survey across 11 districts in three regions in Tanzania. The main outcome was the place of delivery (giving birth in a health facility or otherwise), while explanatory variables were measured at the individual woman and facility level. Given the hierarchical structure of the data and variance in demand across facilities, we used a multilevel mixed-effect logistic regression to explore the determinants of facility-based delivery care.
Results
Eighty-six percent of 2846 women gave birth in a health facility. Demand for facility-based delivery care was influenced more by demand-side factors (76%) than supply-side factors (24%). On demand-side factors, facility births were more common among women who were educated, Muslim, wealthier, with their first childbirth, and those who had at least four antenatal care visits. On supply-side factors, facility births were more common in facilities offering outreach services, longer consultation times and higher interpersonal quality. In contrast, facilities with longer average waiting times, longer travel times and higher chances of charging delivery fees had few facility births.
Conclusions
Policy responses should aim for strategies to improve demand like health education to raise awareness towards care seeking among less educated groups and those with higher parity, reduce financial barriers to access (including time costs to reach and access care), and policy interventions to enhance interpersonal quality in service provision.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Maternal mortality remains a global health challenge [1, 2]. Overall, the global maternal mortality rate (MMR) in 2020 was estimated at 223 maternal deaths per 100 000 live births [1, 2], substantially higher than the Sustainable Development Goal (SDG) three target of 70 maternal deaths per 100,000 live births by 2030 [3]. Although the MMR has dropped by about 34% between 2000 and 2020, it has stagnated or worsened in most regions of the world from 2016 to 2020 [2]. Almost 95% of all maternal deaths occurred in low and lower middle-income countries (LMICs) in 2020 [2]. Maternal deaths are often due to obstetric haemorrhage, hypertensive disorders and sepsis, which occur mainly during childbirth [4,5,6]. To reduce maternal and newborn deaths, there is consensus that women should access good-quality and timely facility-based delivery care by skilled personnel [7, 8]. However, there is wide variation in access to facility-based or skilled births within and across countries [9]. For instance, the proportion of skilled birth attendance deliveries was above 90% in 25 of the 80 LMICs, and below 40% in 11 LMICs [9], and across 25 sub-Saharan African countries, the rate of skilled birth attendance ranged from 24% in Chad to 97% in South Africa [10].
Demand for health care (e.g., facility-based delivery care) is influenced by demand-side and supply-side factors. Demand-side determinants are factors influencing the ability to use health services at individual, household or community levels (e.g., awareness, education, and economic status). Supply-side determinants are aspects inherent to the health system particularly at the point of service delivery (e.g., availability of services, medicines, diagnostics, and medical personnel) which may influence service delivery and uptake by individuals, households or the community [11,12,13]. Policy makers and practitioners need to understand a holistic picture of the determinants of demand on the demand and supply side, and the relative influence of each, in order to prioritize actions to increase uptake of delivery care services and improve maternal and newborn health outcomes. To date, many studies have examined the demand-side determinants of facility-based delivery care [14,15,16,17,18], with relatively few studies examining supply-side or facility-level determinants [14, 19, 20]. To our knowledge, the demand- and supply-side determinants of facility-based deliveries have not been studied simultaneously, and the relative contributions of each group of factors to demand have not been measured. This represents a significant research gap that warrants investigation. In this case, there is a need to shed light on the comprehensive interplay between the multifaceted demand and supply-side factors, allowing us to construct a more comprehensive and nuanced understanding of the factors associated with utilisation of facility-based delivery care.
This study aimed to broaden the understanding of the factors associated with facility-based delivery care and relative influence of these factors on how they associate with the demand for facility-based delivery care in the Tanzanian context. We used multiple sources of primary data (a survey of patients, households, and facilities) which offers a wider range of demand- and supply-side factors than available through routine surveys (e.g., demographic and health survey (DHS), service provision assessment (SPA)) [21, 22].
Materials and methods
Study setting
This study was conducted in three regions of Tanzania: Pwani, Morogoro and Lindi, with the population size of 2 million, 3.2 million, and 1.2 million in 2022, respectively [23]. The study surveyed all seven districts in Pwani, three districts in Morogoro (Morogoro urban, Morogoro rural and Mvomero), and one district in Lindi region (Kilwa). While Tanzania has made substantial progress on child survival, there has been little improvement in maternal health, which stands at 556 deaths per 100,000 live births in 2016 [24, 25]. Although almost all Tanzanian pregnant women accessed at least one antenatal care visit, a smaller share delivered at a facility (63%) and received postnatal care (33%) [24]. Public health facilities are the largest health service provider (70%) in Tanzania, and are organised in a hierarchical administrative structure: dispensaries serve villages, health centres serve wards with multiple villages, and hospitals serve a district or region. Most public health facilities in Tanzania are inadequately funded and experience shortages of staff, drugs and supplies [25,26,27]. The public health system in Tanzania is financed through general taxation (34%), donor support (36%), out-of-pocket payments (22%), and health insurance contributions (8%) [28]. Tanzania has an exemption and waiver policies to protect poor and vulnerable groups including pregnant women and children [29, 30], but the enforcement of these policies has been weak and exempted patients still incur out-of-pocket payments [31, 32].
Conceptual framework
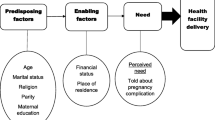
We developed a conceptual framework based on the demand and supply-side access barriers presented by Jacobs et al., [11]. They identified four dimensions of access (geographical accessibility, availability, affordability, and acceptability) from previous literature [12, 13, 33,34,35]. Our framework (Fig. 1) adapted the Jacobs et al. [11] framework by expanding access barriers on the demand and supply side within each dimension as follows: geographical accessibility (location of the health facility, means and cost of transport); availability (drugs, equipment, healthcare workers, information on health services); affordability (medical costs, informal payments, clients’ ability and willingness to pay); and acceptability (provider interpersonal care, individuals expectations, patients assertiveness and level of awareness about health services). Most of the demand-side barriers presented in Jacobs et al., [11] were also consistent with the Grossman model reflecting on the human capital model of the demand for health [35, 36] and the Andersen’s behavioural model of health care utilisation [34, 37]. The Andersen model includes three groups of individual level factors: (i) predisposing factors like age, household size, education, and parity; (ii) enabling factors like income, and health insurance coverage; and (iii) perceived need factors for healthcare such as health status or illness.

Conceptual framework adapted from Jacobs et al., [11]
Data
We used baseline cross-sectional data that were collected as part of an evaluation of the impact of a pay-for-performance programme in Pwani region, including data collected from two neighbouring comparison regions (Morogoro and Lindi) [38, 39]. A cross-sectional survey of 150 facilities, 1494 patients, and 2846 households was carried out in 11 district councils across the three regions. The 150 facilities included 12 hospitals, 32 health centres and 106 dispensaries as the primary sampling unit; and the majority were public facilities (82%) than non-public facilities. At each facility, we conducted exit interviews with a sample of at most 10 patients after receiving maternal and child health care (antenatal care, postnatal care and selected childhood immunizations) and other outpatient services (malaria, respiratory infection and diarrhoea). From each health facility’s catchment population, 20 eligible households (with women aged 15–49 years who gave birth in the last 12 months) were randomly sampled. All surveys were carried out by trained enumerators from January to February 2012. A facility survey and patient exit interviews captured supply-side factors at facility-level, while a household survey captured demand-side factors at the household and women level. All interviews were conducted in Swahili, and all survey tools were pre-tested for consistency, relevance, and clarity.
Outcome
Our primary outcome of interest was place of delivery among women who have given birth 12 months before the survey. This was measured through a household survey as an indicator variable which equals 1 if a woman gave birth in a health facility (institutional delivery) and equals 0 otherwise. We were interested with facility births irrespective of where that facility was located.
Explanatory variables
The explanatory variables as potential determinants of a facility-based delivery were selected based on the conceptual framework described above (Fig. 1). The unit of analysis was a woman because the outcome of interest was measured at the woman level. Thus, each supply-side factor measured at the facility level through a facility survey and exit interviews was shared among women residing in a particular facility catchment area. For instance, facility staffing level at facility A and average value of all patients from exit interviews (e.g., waiting time) were taken as facility-level factors and linked to all women in the catchment area of facility A. All demand-side factors were estimated from the survey of women, with an individual observation for each woman. Only one facility-level factor (facility likelihood of charging delivery fee) was estimated from the survey of women in a facility’s catchment area. This was estimated based on the share of women who paid for delivery care out of the sample women in a facility catchment area.
The household/ woman-level characteristics (demand-side factors) included: the woman’s age in years, her education level (4 categories), occupation status (4 categories), religion (Muslim vs. not Muslim), number of births (parity 1 vs. 2+), household wealth status (measured as wealth terciles (poorest, middle, least poor) derived from an index of assets and housing particulars), household ownership of health insurance (binary ‘yes’ / ‘no’), and women experience of care based on antenatal care visits (4 + visits vs. less visits).
The facility-level characteristics (supply-side factors) included factors measured through the facility survey across targeted 150 facilities, where targeted households/ women were sampled: facility level of care (hospital and health centre, vs. dispensary), facility ownership (public vs. non-public (private for profit, faith-based)), number of medical staff (doctors, clinicians, nurses, paramedics), number of maternity beds, availability of outreach services in the last 90 days, availability of utilities (water and electricity), availability of drugs for delivery care (an index based on three items: oxytocin, misoprostol, and ergometrine), and facility location (rural/ urban district). Other facility-level characteristics included facility likelihood of charging fees for delivery care measured from the women survey (percentage of women who paid out-of-pocket in the catchment area). Additional facility-level characteristics were estimated from exit interview data such as average patients’ waiting and consultation time in minutes, average patients’ travel time to access care (in minutes), and interpersonal quality based on patient-providers’ interaction score (unweighted mean score of seven items: spend enough time with client, given enough information about illness, staff had good explanation, treated with respect, cared more about patients, attended privately without being seen and without being heard).
Statistical analysis
We performed a descriptive analysis of the main outcome of interest as well as individual women, household and facility-level characteristics. To identify the demand and supply-side factors associated with the demand for facility-based delivery care, we used a multilevel modelling technique (mixed-effect logistic regression) to account for the hierarchical structure of the data (because women/households are nested within the catchment area of facilities) [40,41,42]. The use of multilevel mixed-effect logistic regression, also termed a random effects model [43], assumes that there is greater variation in outcomes between women in the catchment area of different facilities than between women in the catchment area of the same facility, since the experience of care at a given facility is likely to be more uniform than the experience of care at different facilities. To confirm this assumption, two prior analyses were performed. First, we estimated an empty/ random intercept model to determine the random variance and assessed the presence of random intercept variations through the likelihood ratio test. We found variation in variance estimates and the likelihood ratio test for the intercept only model was significant (Chi-square = 105.95, p-value < 0.01) (Additional file 1: Appendix Table 1), indicating a significant improvement in fit with random intercepts compared to a standard logistic model (Additional file 1: Appendix Table 1) [40]. Second, we estimated the intraclass correlation (ICC) to capture the degree of facility random effects or between facility variation in the outcome. The ICC results suggest that only 19.6% (ICC = 0.196) of the outcome variation was explained by between facility variation, with the majority being driven by within facility variation (Additional file 1: Appendix Table 1). We therefore used a multilevel mixed-effects model (random effects model) due to the presence of random intercept variations and a significant likelihood ratio test, together with the low intraclass correlation capturing the degree of facility random effects or within facility variation in the outcome (Additional file 1: Appendix Table 1). The following multilevel mixed-effect logistic regression was used to estimate simultaneously both levels of determinants (household/woman and facility).
where i and j are individual women and health facilities, respectively. \({Y}_{ij}\) is a binary indicator for the outcome of interest (i.e., place of delivery); \({X}_{ij}\) represents individual and household covariates, \({Z}_{j}\) represents health facility level covariates, \({\mu }_{j}\) represents random intercepts for facilities \({\mu }_{j}\). \({\beta }_{1}\) and \({\beta }_{2}\) are regression coefficients, α is a constant term and the error term is \({\epsilon }_{ij}\). As a robustness check, we also estimated a reduced model by using logistic backward stepwise regression (Additional file 1: Appendix Table 2). All analyses were performed using STATA software version 16.
Results
Descriptive statistics
The rate of facility-based deliveries among our sample of 2846 women giving birth in the 12 months preceding the survey was 85.8% (Table 1). Women were aged 26 years old on average, and most were educated to the primary level and above. The majority of women were farmers (50.4%), Muslim (76.1%), without health insurance (91.5%), had attended at least four ANC visits (67.4%), and had given birth more than once (67.9%).
Most facilities had both water and electricity (54%), conducted outreach services (76%), were located in rural districts (82%), were dispensaries (70%), and publicly owned (84%) (Table 1). On average, facilities had three maternity beds and sixteen medical staffs, with median values of two maternity beds, and five medical staffs. The surveyed facilities had low availability of delivery drugs (oxytocic) at 44% on average. According to patients who accessed care in these facilities, they spent on average 30 min travelling from home to the facility, 44 min waiting for care, and 13 min in consultation with a provider. Patients rated providers with an average interpersonal quality score of 79%, and the average share of women who paid for delivery care across facilities was low (21%).
Factors influencing facility-based delivery
Women who were educated, Muslim, given birth only once, wealthier, and had at least four ANC visits, were more likely to deliver in a health facility than their counterpart women (Table 2). Specifically, women’s level of education associated positively and significant with increased demand for facility-based delivery. For instance, women with secondary education/ above were almost 4 times more likely to have facility births [OR = 4.13 (CI: 1.65 to 10.3)] compare to women with no education. Muslim women were 1.4 more likely to have facility-based delivery [OR = 1.36 (CI: 1.01 to 1.84)] compared to non-Muslim women. Women who delivered for the first time were 1.7 more likely to deliver in a facility [OR = 1.72 (CI: 1.23 to 2.41)] compared to those with at least two births/ higher parity. The least poor (wealthier) women were almost twice as likely as poorest women to have facility-based delivery [OR = 1.93 (CI: 1.32 to 2.81)]. Women with at least four ANC visits during pregnancy were 1.3 more likely to have facility births [OR = 1.33 (CI: 1.05 to 1.70)] compared to women with less than four ANC visits.
Facility-based deliveries were more likely for women living near facilities offering outreach services, longer consultation times and offering higher interpersonal quality. Women living near facilities offering outreach services were almost twice as likely as women living near facilities without outreach services to deliver in a facility [OR = 1.55 (CI: 1.05 to 2.28)]. The odds of a facility-based delivery increased by 4% [OR = 1.04 (CI: 1.01 to 1.07)] for every additional minute of consultation time for facility outpatients; and, for each unit increase in facility-level interpersonal quality score, the odds of facility-based delivery increased five times on average [OR = 5.11 (CI: 1.12 to 23.4)].
On the other hand, longer waiting times, longer travel time to reach the facility, and a higher chance of charging delivery fee significantly associated with the reduced demand for facility-based delivery. The odds of facility-based delivery were reduced by 1% for each additional minute of travel time to health facility [OR = 0.99 (CI: 0.98 to 0.99)] and for each additional minute of waiting time for outpatient care [OR = 0.99 (CI: 0.98 to 1.00)]. For each percent increase in charging delivery fee at the facility associated with the reduced odds of facility-based delivery by 76% on average [OR = 0.24 (CI: 0.09 to 0.63)].
Overall, demand-side factors had stronger association with the demand for facility-based delivery care than supply-side factors (Table 3). The demand side factors explaining 79% of demand for facility-based delivery care, while the remaining share was explained by supply-side factors.
The reduced model revealed almost similar significant factors associated with the demand for facility-based delivery (Additional file 1: Appendix Table 2). The only discrepancy was the addition of staffing level which became statistically significant in a reduced model, while wealth status and religion were dropped.
Discussion
We estimated the proportion of women delivering in a health facility and identified the demand and supply-side factors associated with women’s decision regarding place of delivery across three regions in Tanzania. We found 86% of women delivered in a health facility with demand for facility-based delivery being higher for women who were educated, Muslim, wealthier, with first birth, and those who had at least four antenatal care visits. In terms of supply-side factors, facility births were more likely for women living near facilities offering outreach services, longer outpatient consultation times and higher interpersonal quality, while few facility births happened in communities that were far from facilities, or where the nearest facility had longer waiting time, and charged delivery fees. The type of facility by ownership and level of care, as well as the staffing level and availability of drugs did not associate with women’s decision on place of delivery. Overall, demand-side factors had relatively stronger association with the demand for facility births by 79% compared to supply-side factors.
The coverage of facility-based delivery was higher than average national coverage of 63% reported in the 2015/16 Tanzania DHS [24]. Our findings regarding the demand-side determinants of facility-based delivery are consistent with demand-side determinants of maternal health care utilisation (including delivery care) in the wider literature from LMICs [14,15,16,17,18,19], which found increased facility-based delivery among women who were educated [15,16,17, 19], Muslim [15], wealthier [15,16,17, 19], with low parity [15], and had higher utilisation of antenatal care [16, 17, 44]. Higher education level and economic status associated with higher demand for facility births partly because they both serve as enabling factors in healthcare seeking by increasing awareness and reducing cost barriers [11, 36, 45, 46]. Low parity associated with higher demand for facility births partly because of the absence of prior experience of delivery which pushes women to seek facility-based care as a way to avoid unforeseen health risks or complications. Many antenatal care visits associated with high demand for facility birth because healthcare workers use the antenatal care platform to encourage women for facility-based delivery care [47, 48]. The religion factor may remain context-specific; however, other studies have also found Muslim women utilised facility-based delivery care more than Christians in Malawi [49] and Tanzania [50].
The identified supply-side factors influencing facility-based delivery concur with findings from other studies. For instance, some studies reported that higher coverage of facility births was associated with facilities offering outreach services [51], facilities with longer consultation time and higher interpersonal quality [52]. Also, fewer facility births were associated with longer waiting time [53,54,55], longer travel time [56,57,58], and higher incidences of paying for delivery care [56, 57, 59, 60]. However, these studies did not examine both demand- and supply side factors simultaneously nor established the relative contribution of each group of factors, contrary to our analysis. The demand for facility births associated positively with increased outreach services, high interpersonal quality, and consultation time possibly because these factors reflect increased providers’ responsiveness to clients and patients’ satisfaction [61]. Direct healthcare payments (e.g., out-of-pocket payments) and indirect costs (e.g., travel and waiting time) were associated with low demand for facility births; this is possibly because they are access barriers which deters health care access and demand [12, 62].
This study expands the understanding of factors affecting healthcare demand in the following aspects. First, our study is the first study to examine simultaneously the demand and the supply-side factors associated with the demand for health care particularly facility delivery care. Second, this study is the first to quantify the relative contributions of demand- and supply-side factors in associating with demand for health care and more specifically on facility delivery care. Third, this study used primary data offering a wider range of supply-side factors from linking multiple data sources (patients, household, facility) (e.g., patient level information such interpersonal quality, waiting and consultation times). It is therefore important for routine facility surveys such as SPA to collect patient level information at the point of service delivery.
Our study had some limitations. First, we relied on only 20 women from each facility’s catchment area to estimate the rate of facility-based delivery and ascertain associated demand-side determinants. This may not reflect the actual status of all reproductive women in the catchment area. Second, we used women’s nearest facility to characterise the supply-side determinants, but due to bypassing tendency especially for primary healthcare facility in Tanzania [63], not all sampled women delivered in their nearest or local facility [64]. Nevertheless, this study is interested in how the characteristics of a woman’s local facility shapes the demand for delivery care. In other words, it is still reasonable to assume the local facility characteristics may influence the decision on where to deliver even if they do not delivery at their local facility. It is also important to know that some bypassing events are being referred from their local facilities. Third, facility level characteristics measured at the time of the survey, may not necessarily reflect the exact status of the facility prior to or at the time a woman delivered at health facility. Fourth, we were unable to include all potential determinants of demand such as actual distance from home to health facility, previous experience of delivery care, influence of women social network, facility capacity limit and traditional birth attendants. We used proxy measures such as travel time in minutes for distance, however, this relied on patient recall which may not have been accurate. Fifth, we used data from only three regions, which may limit the generalisability to other parts of the country, however, there was substantial variation within those three regions. Sixth, we used data from surveys of 2012, since such surveys captured comprehensive data for demand- and supply-side factors from multiple sources (patients, households, facilities) which are lacking in more recent surveys (e.g., DHS and SPA). It is possible some access barriers have been addressed that existed previously (e.g., construction of more facilities should reduce travel time, more resources at facilities might reduce charging delivery fees and drug stock-outs). Lastly, some facility characteristics were measured from a sample of patients interviews during the survey (e.g., waiting and consultation time, interpersonal quality), which may not necessarily represent the true characteristics of the facility in the presence of all patients.
We highlight important implications for improving demand for facility-based delivery care services in Tanzania. The predominance of demand-side influences indicates the need for targeted health education programmes in the community to improve awareness on care seeking among those with lower levels of education and higher parity. Lower demand among poorer households together with the large effect of delivery care costs on decision making, highlight the importance of interventions to increase the affordability of care especially for poorer groups (e.g., strengthening health insurance coverage and exemptions). The lack of effect of health insurance on demand, suggests that the benefit package may not be sufficient to offset financial barriers beyond user charges [65]. It is something to be considered by policy makers when designing the mandatory universal health insurance in Tanzania. Also, additional financial resources may be needed to improve facility level activities including offering outreach services [66, 67].
Moreover, we underscore the importance of antenatal care as a channel through which to encourage facility-based deliveries, suggesting that policy initiatives that enhance access to regular antenatal care are likely to increase the rate of institutional deliveries. Equally, our study highlights that local facility reputation characterised in our study by the length of outpatient consultations and the quality of patient-provider interactions has a substantial influence over decision-making for where a women would go for delivery. For instance, poor quality of services at local or nearest facility influences clients to bypass towards other or even a higher-level facility [63, 64]. In this case, policy makers need to incentivise health workers to improve productivity, motivation and provision of quality health care, for instance, by providing timely benefits (e.g., houses, extra-duty allowances), remuneration and training [68, 69]. Strengthening service provision is important because quality of care provided –including interpersonal quality such as respectful care –is critical to increase the demand for facility-based maternity care [52, 70,71,72,73]. To increase healthcare demand, policy makers should also ensure adequate supply of health workers to increase consultation times, reduce waiting time [74], and adequate development of primary health facilities to reduce both travel and waiting time [75]. Policy makers should think about additional ways to reduce the travel time such as improving road and public transport infrastructure [76]. However, the success of this approach depends on other sectors beyond the health sector (e.g., transportation and infrastructure sector), which indicates the need for multisectoral approaches to reduce access/ geographical barriers [65]. For effective results, there is a need for multifaceted interventions to enhance demand [69].
Conclusion
This study shows the importance of assessing both demand- and supply-side factors associated with the demand for facility-based delivery care in order to inform evidence-based interventions. Interestingly, we found the demand for facility-based delivery care was influenced more by demand-side factors than supply-side factors. This finding reinforces the need for policy makers to design interventions or strategies to improve healthcare demand like health education to raise awareness towards care seeking among less educated groups and those with higher parity, reduce financial barriers to access (including time costs to reach and access care), and policy interventions to enhance interpersonal quality in service provision.
Availability of data and materials
The data have been uploaded into a data repository. The DOI URL for the dataset is: https://doi.org/10.5281/zenodo.21709.
Abbreviations
- ANC:
-
Antenatal Care
- CI:
-
Confidence Interval
- DHS:
-
Demographic Health Survey
- ICC:
-
Intraclass Correlation
- LMICs:
-
Low- and middle-income countries
- MMR:
-
Maternal Mortality Rate
- OR:
-
Odds Ratio
- SD:
-
Standard Deviation
- SDG:
-
Sustainable Development Goal
- SPA:
-
Service Provision Assessment
References
Moyer CA, Lawrence ER, Beyuo TK, Tuuli MG, Oppong SA. Stalled progress in reducing maternal mortality globally: what next? Lancet. 2023;401(10382):1060–2.
WHO. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2023.
United Nations. The sustainable development goals report 2016. New York: United Nations; 2016.
Ronsmans C, Graham WJ. Maternal mortality: who, when, where, and why. Lancet. 2006;368(9542):1189–200.
Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J, Gülmezoglu AM, Temmerman M, Alkema L. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–333.
Khan KS, Wojdyla D, Say L, Gülmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066–74.
Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, Fat DM, Boerma T, Temmerman M, Mathers C, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-agency Group. Lancet. 2016;387(10017):462–74.
Madaj B, Smith H, Mathai M, Roos N, van den Broek N. Developing global indicators for quality of maternal and newborn care: a feasibility assessment. Bull World Health Organ. 2017;95(6):445–452i.
Joseph G, da Silva IC, Wehrmeister FC, Barros AJ, Victora CG. Inequalities in the coverage of place of delivery and skilled birth attendance: analyses of cross-sectional surveys in 80 low and middle-income countries. Reprod Health. 2016;13(1):77.
Bobo FT, Asante A, Woldie M, Dawson A, Hayen A. Spatial patterns and inequalities in skilled birth attendance and caesarean delivery in sub-Saharan Africa. BMJ Glob Health. 2021;6(10):e007074.
Jacobs B, Ir P, Bigdeli M, Annear PL, Van Damme W. Addressing access barriers to health services: an analytical framework for selecting appropriate interventions in low-income Asian countries. Health Policy Plan. 2012;27(4):288–300.
Ensor T, Cooper S. Overcoming barriers to health service access: influencing the demand side. Health Policy Plan. 2004;19(2):69–79.
O’Donnell O. Access to health care in developing countries: breaking down demand side barriers. Cad Saude Publica. 2007;23(12):2820–34.
Kyei-Nimakoh M, Carolan-Olah M, McCann TV. Access barriers to obstetric care at health facilities in sub-Saharan Africa-a systematic review. Syst Rev. 2017;6(1):110.
Mekonnen T, Dune T, Perz J. Maternal health service utilisation of adolescent women in sub-Saharan Africa: a systematic scoping review. BMC Pregnancy Childbirth. 2019;19(1):1–16.
Gabrysch S, Campbell OM. Still too far to walk: literature review of the determinants of delivery service use. BMC Pregnancy Childbirth. 2009;9:34.
Banke-Thomas OE, Banke-Thomas AO, Ameh CA. Factors influencing utilisation of maternal health services by adolescent mothers in low-and middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2017;17(1):65.
Say L, Raine R. A systematic review of inequalities in the use of maternal health care in developing countries: examining the scale of the problem and the importance of context. Bull World Health Organ. 2007;85(10):812–9.
Geleto A, Chojenta C, Musa A, Loxton D. Barriers to access and utilization of emergency obstetric care at health facilities in sub-Saharan Africa: a systematic review of literature. Syst Rev. 2018;7(1):183.
Parkhurst JO, Penn-Kekana L, Blaauw D, Balabanova D, Danishevski K, Rahman SA, Onama V, Ssengooba F. Health systems factors influencing maternal health services: a four-country comparison. Health Policy. 2005;73(2):127–38.
Demographic and Health Surveys (DHS) Program. https://dhsprogram.com/#CP_JUMP_16156. Accessed 11 Apr 2023.
Service Provision Assessment (SPA). Available at https://dhsprogram.com/methodology/Survey-Types/SPA.cfm. Accessed 11 Apr 2023.
NBS. Tanzania population and housing census: population distribution by administrative areas 2022. Dar es Salaam: National Bureau of Statistics (NBS); 2022.
TDHS. Tanzania demographic and health survey and malaria indicator survey 2015–16. National Bureau of Statistics (NBS): Dar es Salaam; 2016.
Afnan-Holmes H, Magoma M, John T, Levira F, Msemo G, Armstrong CE, Martinez-Alvarez M, Kerber K, Kihinga C, Makuwani A, et al. Tanzania’s countdown to 2015: an analysis of two decades of progress and gaps for reproductive, maternal, newborn, and child health, to inform priorities for post-2015. Lancet Glob Health. 2015;3(7):e396–409.
SIKIKA. Medicines and medical supplies availability report. Using absorbent gauze availability survey as an entry point. A case of 71 districts and 30 health facilities across Mainland Tanzania. Dar es Salaam: SIKIKA; 2011.
MoHSW. Tanzania Service Svailability and Seadiness Sssessment (SARA) 2012. Ministry of Health and Social Welfare and Ifakara Health Institute: Dar es Salaam; 2013.
MOHCDGEC. National Health Accounts (NHA) for financial years 2013/14, 2014/15 and 2015/16. Tanzania: Ministry of Health Community Development, Gender, Elderly and Children (MoHCDGEC); 2019.
Maluka SO. Why are pro-poor exemption policies in Tanzania better implemented in some districts than in others? Int J Equity Health. 2013;12:80.
Mtei G, Makawia S, Masanja H. Monitoring and evaluating progress towards Universal Health Coverage in Tanzania. PLoS Med. 2014;11(9):e1001698.
Kruk ME, Mbaruku G, Rockers PC, Galea S. User fee exemptions are not enough: out-of-pocket payments for ‘free’ delivery services in rural Tanzania. Trop Med Int Health. 2008;13(12):1442–51.
Manzi F, Schellenberg JA, Adam T, Mshinda H, Victora CG, Bryce J. Out-of-pocket payments for under-five health care in rural southern Tanzania. Health Policy Plan. 2005;20(Suppl 1):i85–93.
McIntyre D, Thiede M, Birch S. Access as a policy-relevant concept in low- and middle-income countries. Health Econ Policy Law. 2009;4(Pt 2):179–93.
Andersen R. A behavioral model of families' use of health services. Research Series No. 25. Chicago: Center for Health Administration Studies, University of Chicago; 1968.
Grossman M. On the concept of health capital and the demand for health. J Polit Econ. 1972;80(2):223–55.
Grossman M. Chap. 7 - The human capital model. In: Culyer AJ, Newhouse JP, editors. Handbook of health economics, vol 1. Amsterdam, New York: Elsevier; 2000. p. 347–408.
Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Mem Fund Q Health Soc. 1973;51(1):95–124.
Binyaruka P, Patouillard E, Powell-Jackson T, Greco G, Maestad O, Borghi J. Effect of paying for performance on utilisation, quality, and user costs of health services in Tanzania: a controlled before and after study. PLoS One. 2015;10(8):e0135013.
Borghi J, Mayumana I, Mashasi I, Binyaruka P, Patouillard E, Njau I, Maestad O, Abdulla S, Mamdani M. Protocol for the evaluation of a pay for performance programme in Pwani region in Tanzania: a controlled before and after study. Implement Sci. 2013;8:80.
Hox JJ, Moerbeek M, Van de Schoot R. Multilevel analysis: techniques and applications. Abingdon: Routledge; 2005. https://doi.org/10.4324/9781410604118. Accessed 3 May 2021.
Rabe-Hesketh S, Skrondal A. Multilevel and longitudinal modeling using Stata. College Station: STATA press; 2008.
Sommet N, Morselli D. Keep calm and learn multilevel logistic modeling: a simplified three-step procedure using Stata, R, Mplus, and SPSS. Int Rev Social Psychol. 2017;30:203–18.
Heck RH, Thomas S, Tabata L. Multilevel modeling of categorical outcomes using IBM SPSS. Abingdon: Routledge Academic; 2013.
Akazili J, Doctor HV, Abokyi L, Hodgson A, Phillips JF. Is there any relationship between antenatal care and place of delivery? Findings from rural northern Ghana. Afr J Health Sci. 2011;18(1–2):62–73.
Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36:1–10.
Marmot M, Friel S, Bell R, Houweling TA, Taylor S. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372(9650):1661–9.
Ensor T, Quigley P, Green C, Razak Badru A, Kaluba D, Siziya S. Knowledgeable antenatal care as a pathway to skilled delivery: modelling the interactions between use of services and knowledge in Zambia. Health Policy Plan. 2014;29(5):580–8.
Walker T, Woldegiorgis M, Bhowmik J. Utilisation of skilled birth attendant in low- and middle-income countries: trajectories and key sociodemographic factors. Int J Environ Res Public Health. 2021;18(20):10722.
Rai RK, Singh PK, Kumar C, Singh L. Factors associated with the utilization of maternal health care services among adolescent women in Malawi. Home Health Care Serv Q. 2013;32(2):106–25.
Exavery A, Kanté AM, Njozi M, Tani K, Doctor HV, Hingora A, Phillips JF. Access to institutional delivery care and reasons for home delivery in three districts of Tanzania. Int J Equity Health. 2014;13(1):48.
Mackenzie M, Turner F, Platt S, Reid M, Wang Y, Clark J, Sridharan S, O’Donnell CA. What is the ‘problem’ that outreach work seeks to address and how might it be tackled? Seeking theory in a primary health prevention programme. BMC Health Serv Res. 2011;11(1):350.
Hulsbergen M, van der Kwaak A. The influence of quality and respectful care on the uptake of skilled birth attendance in Tanzania. BMC Pregnancy Childbirth. 2020;20(1):681.
Mselle LT, Kohi TW, Mvungi A, Evjen-Olsen B, Moland KM. Waiting for attention and care: birthing accounts of women in rural Tanzania who developed obstetric fistula as an outcome of labour. BMC Pregnancy Childbirth. 2011;11(1):75.
Sialubanje C, Massar K, van der Pijl MS, Kirch EM, Hamer DH, Ruiter RA. Improving access to skilled facility-based delivery services: women’s beliefs on facilitators and barriers to the utilisation of maternity waiting homes in rural Zambia. Reprod Health. 2015;12:61.
Ganle JK, Parker M, Fitzpatrick R, Otupiri E. A qualitative study of health system barriers to accessibility and utilization of maternal and newborn healthcare services in Ghana after user-fee abolition. BMC Pregnancy Childbirth. 2014;14(1):425.
Shiferaw S, Spigt M, Godefrooij M, Melkamu Y, Tekie M. Why do women prefer home births in Ethiopia? BMC Pregnancy Childbirth. 2013;13:5.
Stekelenburg J, Kyanamina S, Mukelabai M, Wolffers I, van Roosmalen J. Waiting too long: low use of maternal health services in Kalabo, Zambia. Trop Med Int Health. 2004;9(3):390–8.
Niyitegeka J, Nshimirimana G, Silverstein A, Odhiambo J, Lin Y, Nkurunziza T, Riviello R, Rulisa S, Banguti P, Magge H, et al. Longer travel time to district hospital worsens neonatal outcomes: a retrospective cross-sectional study of the effect of delays in receiving emergency cesarean section in Rwanda. BMC Pregnancy Childbirth. 2017;17(1):242.
Worku AG, Yalew AW, Afework MF. Factors affecting utilization of skilled maternal care in Northwest Ethiopia: a multilevel analysis. BMC Int Health Hum Rights. 2013;13:20.
De Allegri M, Ridde V, Louis VR, Sarker M, Tiendrebéogo J, Yé M, Müller O, Jahn A. Determinants of utilisation of maternal care services after the reduction of user fees: a case study from rural Burkina Faso. Health Policy. 2011;99(3):210–8.
Donabedian A. The quality of care: how can it be assessed? JAMA. 1988;260(12):1743–8.
McIntyre D, Thiede M, Dahlgren G, Whitehead M. What are the economic consequences for households of Illness and of paying for health care in low- and middle-income country contexts? Soc Sci Med. 2006;62(4):858–65.
Kruk ME, Hermosilla S, Larson E, Mbaruku GM. Bypassing primary care clinics for childbirth: a cross-sectional study in the Pwani region, United Republic of Tanzania. Bull World Health Organ. 2014;92(4):246–53.
Bezu S, Binyaruka P, Mæstad O, Somville V. Pay-for-performance reduces bypassing of health facilities: evidence from Tanzania. Soc Sci Med. 2021;268:113551.
Binyaruka P, Borghi J. An equity analysis on the household costs of accessing and utilising maternal and child health care services in Tanzania. Health Econ Rev. 2022;12(1):36.
John TW, Mkoka DA, Frumence G, Goicolea I. An account for barriers and strategies in fulfilling women’s right to quality maternal health care: a qualitative study from rural Tanzania. BMC Pregnancy Childbirth. 2018;18(1):352.
Borghi J, Ensor T, Somanathan A, Lissner C, Mills A. Mobilising financial resources for maternal health. Lancet. 2006;368(9545):1457–65.
Mangham LJ, Hanson K. Employment preferences of public sector nurses in Malawi: results from a discrete choice experiment. Trop Med Int Health. 2008;13(12):1433–41.
Althabe F, Bergel E, Cafferata ML, Gibbons L, Ciapponi A, Alemán A, Colantonio L, Palacios AR. Strategies for improving the quality of health care in maternal and child health in low- and middle-income countries: an overview of systematic reviews. Paediatr Perinat Epidemiol. 2008;22(Suppl 1):42–60.
Rosen HE, Lynam PF, Carr C, Reis V, Ricca J, Bazant ES, Bartlett LA, On behalf of the quality of M, Newborn Care Study Group of the M, Child Health Integrated P. Direct observation of respectful maternity care in five countries: a cross-sectional study of health facilities in East and Southern Africa. BMC Pregnancy Childbirth. 2015;15(1):306.
Kruk ME, Paczkowski M, Mbaruku G, de Pinho H, Galea S. Women’s preferences for place of delivery in rural Tanzania: a population-based discrete choice experiment. Am J Public Health. 2009;99(9):1666–72.
Lavender T, Bedwell C, Kasengele CT, Kimaro D, Kuzenza F, Lyangenda K, Mills TA, Nsemwa L, Shayo H, Tuwele K, et al. Respectful care an added extra: a grounded theory study exploring intrapartum experiences in Zambia and Tanzania. BMJ Glob Health. 2021;6(4):e004725.
Mannava P, Durrant K, Fisher J, Chersich M, Luchters S. Attitudes and behaviours of maternal health care providers in interactions with clients: a systematic review. Global Health. 2015;11:36.
Dogba M, Fournier P. Human resources and the quality of emergency obstetric care in developing countries: a systematic review of the literature. Hum Resour Health. 2009;7:7.
Hanson K, Brikci N, Erlangga D, Alebachew A, De Allegri M, Balabanova D, Blecher M, Cashin C, Esperato A, Hipgrave D. The lancet global health commission on financing primary health care: putting people at the centre. Lancet Glob Health. 2022;10(5):e715–772.
Karra M, Fink G, Canning D. Facility distance and child mortality: a multi-country study of health facility access, service utilization, and child health outcomes. Int J Epidemiol. 2016;46(3):817–26.
Acknowledgements
We would like to thank all healthcare providers, health managers and all health stakeholders who participated or facilitated to ensure a successfully fieldwork for data collection. We also thank the whole P4P evaluation research team, COSMIC project team, as well as data collectors and field coordinators. We also acknowledge the support from all field respondents, and various officials such as Regional Medical Officers, District Medical officers, Health facility in-charges, and P4P implementing agency.
Funding
The Government of Norway funded the data collection for the program evaluation that was used in this paper (grant numbers: TAN-3108 and TAN 13/0005. http://www.norad.no/en/). The authors as part of the COSMIC project (https://www.lshtm.ac.uk/research/centres-projects-groups/cosmic) were funded for data analysis and manuscript write-up through the Medical Research Council under the Health Systems Research Initiative grant (MR/R013454/1). The funding bodies had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
PB conceptualized this sub-study and oversaw data collection together with JB. PB analyzed the data and wrote the first draft of the manuscript. JB, AF, AA, NM and RC involved in data interpretation, presentation, and revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was given for the evaluation of P4P by the Institutional Review Board of the Ifakara Health Institute (approval number: 1BI1IRB/38) and the Ethics Review Board of the London School of Hygiene & Tropical Medicine. Study participants provided written consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix Table 1.
Random effects parameters for random intercept only model (empty model). Appendix Table 2. Reduced model by using logistic backward stepwise regression.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Binyaruka, P., Foss, A., Alibrahim, A. et al. Supply-side factors influencing demand for facility-based delivery in Tanzania: a multilevel analysis. Health Econ Rev 13, 52 (2023). https://doi.org/10.1186/s13561-023-00468-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13561-023-00468-1