
Background
Recently, a flexible DROP-IN gamma-probe was introduced for robot-assisted radioguided surgery, using traditional low-energy SPECT-isotopes. In parallel, a novel approach to achieve sensitive radioguidance using beta-emitting PET isotopes has been proposed. Integration of these two concepts would allow to exploit the use of PET tracers during robot-assisted tumor-receptor-targeted. In this study, we have engineered and validated the performance of a novel DROP-IN beta particle (DROP-INβ) detector.
Methods
Seven prostate cancer patients with PSMA-PET positive tumors received an additional intraoperative injection of ~ 70 MBq 68Ga-PSMA-11, followed by robot-assisted prostatectomy and extended pelvic lymph node dissection. The surgical specimens from these procedures were used to validate the performance of our DROP-INβ probe prototype, which merged a scintillating detector with a housing optimized for a 12-mm trocar and prograsp instruments.
Results
After optimization of the detector and probe housing via Monte Carlo simulations, the resulting DROP-INβ probe prototype was tested in a robotic setting. In the ex vivo setting, the probe—positioned by the robot—was able to identify 68Ga-PSMA-11 containing hot-spots in the surgical specimens: signal-to-background (S/B) was > 5 when pathology confirmed that the tumor was located < 1 mm below the specimen surface. 68Ga-PSMA-11 containing (and PET positive) lymph nodes, as found in two patients, were also confirmed with the DROP-INβ probe (S/B > 3). The rotational freedom of the DROP-IN design and the ability to manipulate the probe with the prograsp tool allowed the surgeon to perform autonomous beta-tracing.
Conclusions
This study demonstrates the feasibility of beta-radioguided surgery in a robotic context by means of a DROP-INβ detector. When translated to an in vivo setting in the future, this technique could provide a valuable tool in detecting tumor remnants on the prostate surface and in confirmation of PSMA-PET positive lymph nodes.
Similar content being viewed by others


Background
Radioguided surgery (RGS) is an interventional nuclear medicine technique that enables surgeons to identify, during the surgical procedure, lesions that had been detected with non-invasive preoperative imaging. Such guidance is achieved using a combination of radioactive tracers (i.e., radiopharmaceuticals) and intraoperative detection modalities [1]. The direct correlation between preoperative tracer mapping using, e.g., PET/CT and intraoperative detection, reduces the probability of missing a lesion that had been preoperatively identified using the imaging [2]. Applications of this approach include the localization of metastases or primary tumor margins [3].
Nowadays, a noticeable amount of commercially available radiopharmaceuticals is used for radioguided surgery [4]. Radioguidance based on low-energy (< 150 keV) gamma ray emitting radiopharmaceuticals is most commonly applied for sentinel lymph node (SN) biopsy procedures using (indocyanine green-)99mTc-nanocolloid [5], radioguided occult lesion localization (ROLL) procedures using 99mTc-labeled macro-aggregates [6], radioguided 125I-seed localization (RSL) procedures [7], and 99mTc-PSMA-guided resection of lymph node metastases in prostate cancer patients [3]. Hence, the most frequently used detection modality for intraoperative localization is the gamma-detection probe, which provides numerical and acoustical feedback proportional to the amount of radiopharmaceutical localized. Unique for this modality is that it supports relatively “deep” signal detection (i.e., tissue only provides marginal attenuation of gamma ray emissions). Recently, the introduction of the DROP-IN gamma (DROP-INγ) probe concept helped to make radioguidance compatible with robotic surgery [8,9,10,11].
For many diagnostic evaluations (e.g., PSMA), PET radiopharmaceuticals are still preferred. These PET isotopes induce both gamma ray from annihilation (i.e., 511 keV photon) and β+ particle (i.e., positron) emissions, providing two possible detection routes that can be exploited for radioguidance purposes. Since the intraoperative detection of 511 keV gamma rays requires heavily collimated approaches, and thus cumbersome probes, direct detection of β+ particle emissions has been explored [4]. Recently, a sensitive β-probe detector-technology, appropriate for both β− (i.e. electron) and β+ radioguided surgery was introduced [12,13,14]. Due to intrinsic differences among the interaction with matter of beta and gamma particles, beta probes require a small active area and basically no collimation: as a result, such β-probes can be much smaller and lighter than γ-probes, especially when active materials are chosen that are insensitive to the 511 keV γ-ray background [15]. Therefore, such a detector allows to exploit the unique spatial resolution achievable with beta emission. In fact, tissue penetration of ~ 1 MeV β-particles is much smaller than that of γ-rays (~ millimeters vs ~ centimeters) making it a unique “surface scanning” technique, much less limited by the “shine-through” of deeper lying tracer uptake [12]. Direct beta detection might thus be a very effective methodology to detect tumors nearby healthy organs characterized by elevated physiological uptake of the radiopharmaceutical (e.g., tumor nearby healthy prostate).
In an effort to explore the use of the widely available PET radiopharmaceutical [68Ga]Ga-PSMA-11 (68Ga-labeled Glu-urea-Lys (Ahx)-HBED-CC) for robot-assisted radioguided surgery purposes, we have developed a DROP-IN beta (DROP-INβ) probe that exploits both the high beta detection efficiency and the compactness of such a detector [12] with the maneuverability of the DROP-IN concept [11] (see Fig.1). In this paper, we present its engineering together with its first characterization on ex vivo surgical specimens (i.e., prostate and lymph nodes) of PSMA-PET positive patients that received an additional dose of [68Ga]Ga-PSMA-11 during surgery.

DROP-INβ probe design. a Schematic representation of the probe components. b Example of one of the Monte Carlo simulations optimizing β-particle detection and γ-photon transparency. c Overview of the probe application setup, showing its high maneuverability
Methods
DROP-INβ probe development
The β-detection probe used in this study was based on a cylindrical scintillator (6 mm diameter and 3 mm height) made of mono-crystalline para-terphenyl (doped with 0,1% in mass of (E,E)-1,4-Diphenyl-1,3-butadiene) [15]. Being a non-hygroscopic organic scintillator with high light yield (~ 140% of anthracene) and low density (1.23 g/cm3), this material provides a high sensitivity to β particles and elevated transparency to photons (e.g., the 511 keV γ rays as induced by PET radiopharmaceuticals). To improve light collection from the scintillator, the detector was surrounded with a 2-mm-thick white diffusing Delrin ring and covered in front with two 4 μm layers of a reflective aluminized-Mylar film. The light tightness of this assembly was achieved by adding an external black poly-vinyl-chloride ring of 2 mm, covered on the front by a 15-μm layer of aluminum. Light collection efficiency was maximized using a 3 × 3 mm2 silicon photomultiplier (SiPM C-series 30035, SensL Ltd.). After a first Monte Carlo-based study of such a probe in a Ga-PSMA context [16], a dedicated laboratory characterization has been performed. A detection efficiency of ~ 90% for 68Ga β particles and ~ 2.5% for 511 keV γ rays has been found [17].
The β detector was placed at the tip of the DROP-IN probe housing. Similarly to the previously optimized DROP-INγ probe [11], a 45° angle grip was incorporated at the end of longitudinal axis of the probe, tailored to the ProGrasp Forceps (Intuitive Surgical Inc.), an instrument that is often used during a prostatectomy and lymph node dissection. Maintaining its compatibility with the da Vinci (Intuitive Surgical Inc.) apparatus, this ensured the maneuverability needed to fully exploit the specificity of beta-RGS. In fact, differently from gamma probes, beta detection requires the probe to have full access to the surface to be examined, due to the significant signal attenuation in tissue.
The housing was printed using acrylonitril-butadieen-styreen plastics and a Dimension Elite 3D printer (Stratasys Ltd.). Final dimensions of the whole probe were a length of 55 mm and a diameter of 12 mm, due to the available detector prototype. In the future, however, this diameter could be reduced (e.g., to 8 mm) if necessary.
Portable electronics based on an Arduino Due (Arduino AG) equipped with a custom analog shield providing signal conditioning and trigger logic were used for the readout [18]. Sampling time was 1 s. At the end of the chain, the output in terms of counts per second (CPS) was displayed on a tablet, via wireless connection.
Optimization of the DROP-INβ probe design
In order to optimize the design of the β-probe, a dedicated Monte Carlo simulation was performed in Geant4 [19]. In this simulation, the whole detector was reconstructed, and all physical processes of interest were taken into account to effectively reproduce particle scattering, absorption, energy deposition, and secondary particles generation. These simulations indicated that a cavity behind the β particle detector would result in a lower noise-background: additional layers of material could in fact promote β+ to γ conversion close to the detector, creating noise-background (Fig. 1b). This design concept yielded a light-weight probe construction (Fig. 1a), mostly transparent to 511 keV γ-induced noise.
First ex vivo probe evaluation
Patient selection
In total, 7 patients with primary diagnosed locally (advanced) high-risk prostate cancer were included (see Table 1). Inclusion criteria consisted of a primary tumor ≥ 2 cm (based on MRI) with a minimal average PSMA tracer uptake of 1.7 kBq/mL (based on PSMA PET/CT). These patients were mostly redirected to our clinical institute for prostate cancer treatment; initial diagnostics was performed at the referring hospital. Therefore, based on local availability and preferences, diagnostic PSMA-PET/CT was performed with 18F-DCFPyl. This should however provide comparable uptake as 6[68Ga]Ga-PSMA-11 [20]. SUVmean measurements were performed by manually defining a volume of interest in the prostate tumor, using OsiriX medical imaging software (Pixmeo SARL). All patients were scheduled for a robot-assisted radical prostatectomy and extended pelvic lymph node dissection. In order to minimize radioactive exposure to both patient and medical personnel, a limited dose of ~ 70 MBq (median 68, IQR 63.5–82) [68Ga]Ga-PSMA-11 for radioguidance was intravenously administered in the operating room (OR), after docking the da Vinci robot. The study was approved by the local ethics committee (NL66218.031.18, trial NL8256 at trialregister.nl) and all patients provided a written informed consent.
Probe countings
At the end of the surgical procedure, roughly 2.5 h after injection (median 150 min; IQR 120–172.5), the surgical specimens (prostate and lymph node packages if present) were rinsed with saline and scanned using the DROP-INβ probe mounted on a da Vinci robot using the ProGrasp forceps instrument. Rinsing of the ex vivo specimens was performed to remove possible urine contamination, since [68Ga]Ga-PSMA-11is known to undergo renal clearance [20]. For prostate samples, “signal” was defined as the highest counting area, as confirmed with preoperative imaging information. The “background” was defined as the area nearby the “signal” where the counting rate dropped to the plateau value that was found in the rest of the sample (thus representing tracer uptake in the healthy prostate tissue). For lymph node samples, the “signal” was acquired on the lymph node itself, and “background” on the surrounding tissue (i.e., fat tissue and negative lymph nodes).
Pathology
Following analysis, all specimens were sent to pathology for assessment using standard histopathological procedures [21]. Additionally, distances between the tumor and the inked specimen borders were measured at marked locations.
Monitoring of radioactive exposure in the operating room
To investigate the feasibility of radioguided surgery using [68Ga]Ga-PSMA-11, radiation safety was considered an important topic. Therefore, radiation dose, as received by the operating room staff, was carefully monitored [22]. The surgeon (located behind the robotic console), the scrub nurse (located next to the patient in the sterile field), the assisting nurse (moving around the operating room, outside the sterile field), the anesthetist (located at the head of the patient, outside the sterile field), and the researcher (located > 1 m away from the patient, outside the sterile field) all had their own electronic radiation dosimeter (MGPInstruments DMC 2000; Mirion Technologies, Ltd.).
Results
Probe usage
The developed DROP-INβ probe easily fitted through standard 12 mm trocars and pick-up of the probe was facile using the standard da Vinci instruments of the surgical robot. Being a tethered design, probe maneuverability allowed for positioning with 6 degrees of freedom, as inherited from the ProGrasp forceps, with an effective scanning range of 0–140o around the tip of the instrument. Scanning with the probe could be performed autonomously from the surgical robotic console, not requiring the help of an assistant.
Ex vivo probe evaluation
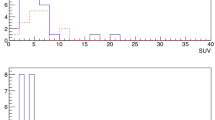
The seven included patients displayed clear PSMA-PET positive primary tumors (see Table 1), with a SUVmean in the tumor > 3. Additionally, two patients had PSMA-PET positive lesions, suspected for lymph node metastases (see Fig. 2 and Table 1).

Preoperative tumor mapping using PSMA-PET. a Example of total body PET maximum intensity projection with tumor focus in prostate (blue, upwards arrow) and lymph node metastasis (green, downwards arrow). b PET/CT slice of the same patient illustrating a clear tumor focus within the prostate (blue arrow; SUVmean = 17.8). c PET/CT slice of the same patient displaying a lymph node metastasis (green arrow; SUVmean = 5.6)
Figure 3 illustrates usage of the DROP-IN beta probe on surgical specimens using the da Vinci robot. Table 2 shows a summary of the collected data. In general, probe background measurements without any tissue (i.e., “dark counts”) were in the order of 0–2 CPS, while uncovered tumor areas, cleaved if necessary, provided count rates between 130 and 250 CPS. Due to its normal (i.e., default) PSMA expression levels, healthy prostate tissue yielded ~ 5–45 CPS. The primary tumor in patients 1, 3, 5, 6, and 7 provided a maximum S/B (signal to background ratio) > 5, displaying a maximum count rate of ~ 247 CPS on the surface of the excised prostate specimen. At pathology, only patients 1 and 7 harbored true positive resections margins (i.e., tumor cells were found in the inked borders of the prostate at pathology). However, in patients 3, 5, and 6, tumor was found within 1 mm of the resection margin, confirming a superficial tumor location. The maximum S/B measured for the prostate specimens in patients 2 and 4 was much lower, < 2.5. In these cases, pathology indicated that the tumor was located > 1.5 mm below the specimen margin, indicating a negative surgical margin. This occurrence, together with their smaller SUVmean with respect to other cases, ended up limiting as expected the possibility of beta-tracing.

DROP-INβ probe evaluation in relation to pathology. a Overview of the robot-assisted OR setup. b Example of robot-assisted beta-tracing with the DROP-INβ probe on the surface of a resected prostate sample. c Histopathology slide displaying tumor spread within the prostate with respect to the specimen surface. d Example of robot-assisted beta-tracing on the surface of a resected lymph node package. e Histopathology slide showing tumor spread within a PSMA-PET positive lymph node
Interestingly, patients 3 and 7 both harbored 2 lymph nodes each that were positive on preoperative PSMA-PET. Using the DROP-INβ probe, these lymph nodes also showed elevated tracer uptake with respect to the other lymph nodes and surrounding fat tissue: S/B > 3. At pathology, metastasis was only found in three of these lymph nodes, suggesting a false-positive PSMA uptake in one lymph node. In this limited group of PET positive lymph nodes, the smallest metastasis the probe was capable to detect had a 7-mm diameter (SUVmean of 5.6 on preoperative PSMA-PET, time between injection and measurement 3 h). All PET negative lymph nodes that were excised and analyzed yielded the same counting rates as nearby background tissue.
Monitoring of radioactive exposure in the operating room
The average radiation dose per surgery performed, as measured for the operating room staff, was 0.005 mSv for the surgeon, 0.016 mSv for the scrub nurse, 0.002 mSv for the assisting nurse, 0.001 mSv for the anesthetist, and 0.001 mSv for the researcher. Taking in to account the guidelines from the International Commission on Radiological Protection [23], this would mean that the surgeon would be allowed to perform 200 of such [68Ga]Ga-PSMA-11 guided procedures a year, while the scrub nurse would be limited to 62 procedures a year.
Discussion
In this study, the first steps are made towards integration of beta radioguided surgery within the robot-assisted setting. Using the DROP-IN concept, the surgeon has full control of probe placement, yielding autonomy and great maneuverability during radioguidance [8,9,10,11]. Direct beta detection provides, thanks to its specificity and sensitivity, a useful way to probe prostate margins and suspect lymph nodes.
This initial ex vivo validation of the DROP-INβ probe concept showed a high signal to background (> 5) for tumors located < 1 mm from the resected surface, suggesting that the technique has the potential to support robotic surface scanning of primary tumor margins in prostate cancer. Even more precise characterization of the possible lesion depth with respect to the surgical margin might be possible with future developments in the underlying detection software algorithms [24]. In addition, confirming PSMA-positive lymph nodes (S/B > 3), the DROP-INβ probe concept might also support the intraoperative identification of metastatic lymph nodes.
Compared to the previously reported use of a DROP-INγ probe in combination with the tracer [99Tc]Tc-PSMA-I&S (i.e., salvage procedures for lymphatic metastases) [10], the use of a DROP-INβ probe in combination with [68Ga]Ga-PSMA-11 possesses some unique advantages. First of all, this approach supports the use of more widely available PET tracers. Secondly, the limited tissue penetration of β particles (only a few millimeters) allows for an accurate surface scanning of the primary tumor margins [12], thus highlighting possible tumor localizations on the prostate surface. Indeed, in the current study, beta radiation was severely attenuated when > 1.5 mm of healthy tissue was located between the surface of the prostate specimen and the pathological tumor margins. In this sense, β-tracing benefits from similar positive features as fluorescence imaging [25], i.e., no ‘shine-through’ of neighboring or deeper lying tracer uptake and a superior spatial resolution [12, 26]. These features are essential when the extra-capsular spread of PSMA-overexpressing tumor lesions is pursued in a prostate with (significant) default PSMA expression [27]. Consequently, β-tracing could provide a superior means for margin assessment during, e.g., nerve sparing surgery [28, 29]. Alternative to investigated beta-radiation detection for tumor margin assessment on the prostate surface, fully matured ex vivo technologies are available (e.g., NeuroSAFE [30]) and alternative β-emission-based imaging technologies are being explored (e.g., Cerenkov [22]). Future research, and in particular randomized trials, will have to show which technology is superior, or if different technologies can work in synergy.
Potential limitations of the proposed [68Ga]Ga-PSMA-11-guided surgery concept are the radiation dose for the surgical staff (currently limited to about 62 procedures a year) and the contamination of the prostate margins by tracer containing urine. The DROP-INβ probes ability to detect lesions using < 70 MBq doses helps limit the exposure of the surgical staff. It is worth highlighting in particular that injecting the radiotracer directly in the operating room allowed ex vivo examination after ~ 2.5 × t1/2 (3 h, t1/2 = 68 m). Hence future in vivo application, e.g., 1 h p.i., would allow an even lower activity to be used to achieve a similar detection sensitivity, namely of the order of 40 MBq. Regarding the urine contamination of the samples, as stated previously, the accumulation of PSMA tracers in healthy organs and in particular urine may yield background signals that complicate intraoperative margin detection [20]. However, the direct detection of beta particles performed with a detector substantially transparent to gamma rays, as suggested in this paper, should drastically reduce the impact of such a background; only the signal originating from a few millimeters around the detector should be detected (i.e., thus only a small urine layer must be considered [24, 31]). Nonetheless, acknowledgement of this effect by radiochemists [32, 33] and the reduced renal clearance of for example [18F]F-PSMA tracers [34, 35] may in the future help to overcome these issues. In addition, the influence of renal clearance might also be overcome by using β-emitting isotopes that have a longer half-life, allowing the tumor resection to take place after all renal clearance of non-bound tracer is realized, e.g. using alternative PET isotopes such as 64Cu (t1/2 = 12.7 hours), or even theranostic isotopes such as 67Cu (t1/2 = 2.5 days), 90Y (t1/2 = 2.66 days), or 177Lu (t1/2 = 6.6 days) [36, 37].
Conclusion
In this study, we presented the integration of two recent developments in RGS: a high efficiency beta detector and a flexible DROP-IN probe housing compatible with robot-assisted surgery. The first prototype of DROP-INβ probe has been successfully validated on ex vivo samples of prostate tumors with [68Ga]Ga-PSMA-11, being able to detect all PET positive resected specimens, with a smallest detected dimension in this data sample of 7 mm. Probe maneuverability was found to be the same of the DROP-INγ concept, which has already demonstrated its efficacy in in vivo tests. This DROP-INβ probe could thus help exploit the growing amount of disease specific PET tracers and may help provide a new powerful tool to perform tumor margin evaluation and confirm metastatic spread.
Availability of data and materials
The Monte Carlo simulation datasets used during the current study are available from the corresponding author on reasonable request.
All data gained on patient samples during this study are included in this published article.
Abbreviations
- RGS:
-
Radioguided surgery
- PSMA:
-
Prostatic Specific Membrane Antigen
- S/B:
-
Signal to background ratio
- OR:
-
Operating room
References
Herrmann K, Nieweg OE, Povoski SP. Radioguided surgery: current applications and innovative directions in clinical practice; 2016. 503 p.
Meershoek P, Buckle T, van Oosterom MN, KleinJan GH, van der Poel HG, van Leeuwen F. Can fluorescence-guided surgery help identify all lesions in unknown locations or is the integrated use of a roadmap created by preoperative imaging mandatory? A blinded study in prostate cancer patients. J Nucl Med [Internet]. 2019 [cited 2020 Jan 27];jnumed.119.235234. Available from: http://jnm.snmjournals.org/lookup/doi/10.2967/jnumed.119.235234.
Horn T, Krönke M, Rauscher I, Haller B, Robu S, Wester HJ, et al. Single lesion on prostate-specific membrane antigen-ligand positron emission tomography and low prostate-specific antigen are prognostic factors for a favorable biochemical response to prostate-specific membrane antigen-targeted radioguided surgery in recurrent prostate cancer. Eur Urol. 2019;76(4):517–23.
Van Oosterom MN, Rietbergen DDD, Welling MM, Van Der Poel HG, Maurer T, Van Leeuwen FWB. Recent advances in nuclear and hybrid detection modalities for image-guided surgery. Vol. 16, Expert Review of Medical Devices. Taylor and Francis Ltd; 2019. p. 711–734.
KleinJan GH, van Werkhoven E, van den Berg NS, Karakullukcu MB, Zijlmans HJMAA, van der Hage JA, et al. The best of both worlds: a hybrid approach for optimal pre- and intraoperative identification of sentinel lymph nodes. Eur J Nucl Med Mol Imaging. 2018;45(11):1915–25.
Bowles H, Sánchez N, Tapias A, Paredes P, Campos F, Bluemel C, et al. Radioguided surgery and the GOSTT concept: from pre-operative image and intraoperative navigation to image-assisted excision. Rev Española Med Nucl e Imagen Mol (English Ed). 2017;36(3):175–84.
Pouw B, De Wit-Van Der Veen LJ, Stokkel MPM, Loo CE, Vrancken Peeters MJTFD, Valdés Olmos RA. Heading toward radioactive seed localization in non-palpable breast cancer surgery? A meta-analysis. J Surg Oncol. John Wiley and Sons Inc. 2015;111:185–91.
Fuerst B, Sprung J, Pinto F, Frisch B, Wendler T, Simon H, et al. First robotic SPECT for minimally invasive sentinel lymph node mapping. IEEE Trans Med Imaging. 2016;35(3):830–8.
Meershoek P, van Oosterom MN, Simon H, Mengus L, Maurer T, van Leeuwen PJ, et al. Robot-assisted laparoscopic surgery using DROP-IN radioguidance: first-in-human translation. Eur J Nucl Med Mol Imaging. 2019;46(1):49–53.
Van Leeuwen FWB, Van Oosterom MN, Meershoek P, Van Leeuwen PJ, Berliner C, Van Der Poel HG, et al. Minimal-invasive robot-assisted image-guided resection of prostate-specific membrane antigen-positive lymph nodes in recurrent prostate cancer. Clin Nucl Med. 2019;44(7):580–1.
van Oosterom MN, Simon H, Mengus L, Welling MM, van der Poel HG, van den Berg NS, et al. Revolutionizing (robot-assisted) laparoscopic gamma tracing using a drop-in gamma probe technology. Am J Nucl Med Mol Imaging [Internet]. 2016 [cited 2020 Jan 27];6(1):1–17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27069762.
Camillocci ES, Baroni G, Bellini F, Bocci V, Collamati F, Cremonesi M, et al. A novel radioguided surgery technique exploiting β− decays. Sci Rep [Internet]. 2015;4(1):4401 Available from: http://www.nature.com/articles/srep04401.
Solfaroli Camillocci E, Schiariti M, Bocci V, Carollo A, Chiodi G, Colandrea M, et al. First ex vivo validation of a radioguided surgery technique with β-radiation. Phys Med. 2016;32(9):1139–44.
Mancini-Terracciano C, Donnarumma R, Bencivenga G, Bocci V, Cartoni A, Collamati F, et al. Feasibility of beta-particle radioguided surgery for a variety of “nuclear medicine” radionuclides. Phys Med. 2017;43.
Angelone M, Battistoni G, Bellini F, Bocci V, Collamati F, De Lucia E, et al. Properties of para-terphenyl as a detector for α, β and γ radiation. IEEE Trans Nucl Sci. 2014;61(3):1483–7.
Collamati F, Bocci V, Castellucci P, De Simoni M, Fanti S, Faccini R, et al. Radioguided surgery with β radiation: a novel application with Ga68. Sci Rep. 2018;8(1):16171.
Collamati F, Moretti R, Alunni-Solestizi L, Bocci V, Cartoni A, Collarino A, et al. Characterisation of a β detector on positron emitters for medical applications. Phys Med. 2019;67:85–90.
Bocci V, Chiodi G, Iacoangeli F, Nuccetelli M, Recchia L. The ArduSiPM a compact trasportable software/hardware data acquisition system for SiPM detector. In: 2014 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC). 2014. p. 1–5.
Allison J, Amako K, Apostolakis J, Arce P, Asai M, Aso T, et al. Recent developments in GEANT4. Nucl Instruments Methods Phys Res Sect A Accel Spectrometers, Detect Assoc Equip. 2016;835:186–225.
Van Leeuwen FWB, Van Der Poel HG. Surgical guidance in prostate cancer: “from molecule to man” translations. Clin Cancer Res. 2016;22(6):1304–6.
Wang M, Tulman DB, Sholl AB, Kimbrell HZ, Mandava SH, Elfer KN, et al. Gigapixel surface imaging of radical prostatectomy specimens for comprehensive detection of cancer-positive surgical margins using structured illumination microscopy. Sci Rep. 2016;3:6.
olde, Heuvel J, de Wit-van der Veen BJ, van der Poel HG, Bekers EM, Grootendorst MR, Vyas KN, et al. 68Ga-PSMA Cerenkov luminescence imaging in primary prostate cancer: first-in-man series. Eur J Nucl Med Mol Imaging. 2020. https://link.springer.com/article/10.1007/s00259-020-04783-1#citeas.
The 2007 recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP. 2007;.
Morganti S, Bertani E, Bocci V, Colandrea M, Collamati F, Cremonesi M, et al. Tumor-non-tumor discrimination by a β- detector for Radio Guided Surgery on ex-vivo neuroendocrine tumors samples. Phys Med. 2020;72:96–102.
van Oosterom MN, van der Poel HG, van Leeuwen FWB, Meershoek P, Welling MM, Pinto F, et al. Extending the hybrid surgical guidance concept with freehand fluorescence tomography. IEEE Trans Med Imaging [Internet]. 2020 [cited 2020 Jan 27];39(1):226–235. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31247546.
Bluemel C, Rubello D, Colletti PM, de Bree R, Herrmann K. Sentinel lymph node biopsy in oral and oropharyngeal squamous cell carcinoma: current status and unresolved challenges. Eur J Nucl Med Mol Imaging. Springer Berlin. 2015;42:1469–80.
Fendler WP, Calais J, Allen-Auerbach M, Bluemel C, Eberhardt N, Emmett L, et al. 68Ga-PSMA-11 PET/CT interobserver agreement for prostate cancer assessments: an international multicenter prospective study. J Nucl Med. 2017;58(10):1617–23.
van Leeuwen FWB, Winter A, van Der Poel HG, Eiber M, Suardi N, Graefen M, et al. Technologies for image-guided surgery for managing lymphatic metastases in prostate cancer. Nat Rev Urol. Nature Publishing Group. 2019;16:159–71.
Yossepowitch O, Briganti A, Eastham JA, Epstein J, Graefen M, Montironi R, et al. Positive surgical margins after radical prostatectomy: a systematic review and contemporary update. Eur Urol. 2014;65:303–13.
Beyer B, Schlomm T, Tennstedt P, Boehm K, Adam M, Schiffmann J, et al. A feasible and time-efficient adaptation of NeuroSAFE for da Vinci robot-assisted radical prostatectomy. Eur Urol. 2014;66(1):138–44.
Collamati F, Maccora D, Alfieri S, Bocci V, Cartoni A, Collarino A, et al. Radioguided surgery with β − radiation in pancreatic neuroendocrine tumors: a feasibility study. Sci Rep. 2020;10(1):1–10.
Hensbergen AW, Buckle T, van Willigen DM, Schottelius M, Welling MM, van der Wijk FA, et al. Hybrid tracers based on cyanine backbones targeting prostate-specific membrane antigen – tuning pharmacokinetic properties and exploring dye–protein interaction. J Nucl Med. 2019. https://doi.org/10.2967/jnumed.119.233064.
Hensbergen AW, van Willigen DM, van Beurden F, van Leeuwen PJ, Buckle T, Schottelius M, et al. Image-guided surgery: are we getting the most out of small-molecule prostate-specific-membrane-antigen-targeted tracers? Bioconjug Chem [Internet]. 2020 [cited 2020 Jan 27];acs.bioconjchem.9b00758. Available from: https://pubs.acs.org/doi/abs/10.1021/acs.bioconjchem.9b00758.
Giesel FL, Hadaschik B, Cardinale J, Radtke J, Vinsensia M, Lehnert W, et al. F-18 labelled PSMA-1007: biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur J Nucl Med Mol Imaging. 2017;44(4):678–88.
Collamati F, Bellini F, Bocci V, De Lucia E, Ferri V, Fioroni F, et al. Time evolution of DOTATOC uptake in neuroendocrine tumors in view of a possible application of radioguided surgery with b2 decay. J Nucl Med. 2015;56(10):1501–6.
Zia NA, Cullinane C, Van Zuylekom JK, Waldeck K, McInnes LE, Buncic G, et al. A bivalent inhibitor of prostate specific membrane antigen radiolabeled with copper-64 with high tumor uptake and retention. Angew Chemie Int Ed [Internet]. 2019 [cited 2020 Jan 27];58(42):14991–4. Available from: http://doi.wiley.com/10.1002/anie.201908964.
Baur B, Solbach C, Andreolli E, Winter G, Machulla HJ, Reske SN. Synthesis, radiolabelling and in vitro characterization of the gallium-68-, yttrium-90- and lutetium-177-labelled PSMA Ligand, CHX-A-DTPA-DUPA-Pep. Pharmaceuticals. 2014;7(5):517–29.
Acknowledgements
The authors would like to thank Sven van Leeuwen (IMI-Lab, Department of Radiology, LUMC, the Netherlands) and Michael Boonekamp (Department of Technical Services subsection Development, LUMC, the Netherlands) for their assistance with the illustrations and prototyping of the probe housing. This study was supported in part by an NWO-TTW-VICI grant (no. TTW 16141).
Funding
This work was supported by Sapienza University of Rome [grant nos. RM116154C8EF4FBC, RM11715C7D2B14C5].
Author information
Authors and Affiliations
Contributions
F. C., M. F., C. M. T., and R. M. developed and tuned the Monte Carlo simulation and analyzed its output. M. D. S., R. F., R. M., E. S. C., and Silvio M. took care of the hardware development of the detector including its testing. M. N. van O., J. o. H., F. v. B., H. G. v. d. P., R. A. V. O., P. J. v. L., and F. W.B. v. L. organized and performed the medical part of the experimentation, from the nuclear medicine and surgical point of view. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the local ethics committee (NL66218.031.18) and all patients provided a written informed consent.
Consent for publication
Not applicable
Competing interests
F.C. and R.F are listed as inventors on an Italian patent application (RM2013A000053) entitled “Utilizzo di radiazione beta- per la identificazione intraoperatoria di residui tumorali e la corrispondente sonda di rivelazione” dealing with the implementation of an intraoperative beta- probe for radioguided surgery according to the results presented in this paper. The same authors are also inventors in the PCT patent application (PCT/IT2014/000025) entitled “Intraoperative detection of tumor residues using beta- radiation and corresponding probes” covering the method and the instruments described in this paper.
FWB van Leeuwen is a consultant for Hamamatsu Photonics and is Chief Innovation Officer at ORSI Academy.
No other potential conflicts of interest relevant to this article exist.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Francesco Collamati and Matthias N. van Oosterom are co-first authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Collamati, F., van Oosterom, M.N., De Simoni, M. et al. A DROP-IN beta probe for robot-assisted 68Ga-PSMA radioguided surgery: first ex vivo technology evaluation using prostate cancer specimens. EJNMMI Res 10, 92 (2020). https://doi.org/10.1186/s13550-020-00682-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13550-020-00682-6