
Abstract
Background
Cholesterol granuloma is not a common entity in the paranasal sinuses. It is a foreign body reaction to the cholesterol crystal deposition. Mostly associated with chronic middle ear diseases.
Case presentation
This article reports a case of cholesterol granuloma in the maxillary sinus. A 23-year-old Asian man presented with cough, nasal obstruction, and postnasal discharge. On endoscopy, there was a mass protruding from the right maxillary ostium. On computed tomograpy imaging, there was a polypoidal mass in the right maxillary sinus. Endoscopic sinus surgery was performed, the cholesterol granuloma was removed from the right maxillary sinus, and the tissue was submitted for histopathological examination, which showed foreign body giant cell reaction to cholesterol crystals.
Conclusion
Cholesterol granuloma of maxillary sinus is not common and often missed by clinicians. It is necessary to consider the cholesterol granuloma of maxillary sinus in the differential diagnosis sinonasal lesions. Histopathological analysis is required for confirmation and should be removed surgically. This case may help as a reference for clinician to approach these kinds of cases.
Similar content being viewed by others


Background
Cholesterol granuloma is a histopathologic term describing cholesterol crystals with surrounding foreign body giant cells, foam cells, and macrophages filled with hemosiderin embedded in fibrous granulation tissue [1]. Cholesterol granuloma (CG) is most commonly seen in middle ear; other sites include mastoid process, apex of the temporal bone pyramid, breast, sella turcica, cerebellopontine angle, testis, lungs, brain, and kidneys [2]. It is unlikely seen in the maxillary sinus and is difficult to diagnose because of nonspecific symptoms at the time of presentation, which includes facial pain, yellowish nasal discharge, and unilateral nasal obstruction. The endoscopy showed a polypoid mass emerging from the ostiomeatal complex, and imaging showed a cyst-like or massive opacification of the maxillary sinus and bony erosion. These lead to the other differentials, such as mucocele, nonsecreting cysts, chronic sinusitis, and malignant pathology of the maxillary sinus [3]. The aim of this paper is to emphasize the uncommonness of cholesterol granuloma in the maxillary sinus of an adult and to consider it in the differential diagnosis for all sinonasal lesions.
Case presentation
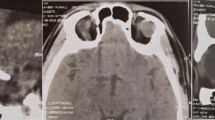
A 23-year-old Asian male presented with complaints of postnasal discharge, irritation to the throat, cough, right nasal obstruction, and headache, which was on and off in nature. Computed tomography (CT) imaging showed a polypoidal mass in the right maxillary sinus and extending into anterior nasal cavity with widened ostium (Fig. 1).

Showing soft tissue attenuation filling up right maxillary sinus and extending into the anteronasal cavity with widened ostium
Endoscopic sinus surgery was performed on the right maxillary sinus, and the specimen was sent for histopathological examination. Histopathological examination showed multiple gray–white soft tissues measuring 1 cm × 0.5 cm × 0.5 cm. In aggregate with the surface cut it was solid and gray–white to grey–yellow. On gross examination and on microscopy, the sections studied showed fibrocollagenous tissue lined by pseudostratified columnar respiratory epithelium.
Subepithelial tissue shows numerous cholesterol clefts surrounded by dense lymphoplasmacytic infiltrate with few multinucleated giant cells, hemosiderin laden macrophages, and congested blood vessels (Figs. 2 and 3). Cholesterol granuloma was confirmed postoperatively by the histopathological interpretation [4]. These pathologic findings were consistent with those of cholesterol granuloma. The postoperative course was favorable and uneventful.

Numerous cholesterol clefts surrounded by dense lymphoplasmacytic infiltrates

Numerous cholesterol clefts surrounded by dense lymphoplasmacytic infiltrates
Discussion
Cholesterol granuloma is not so common and unexpected finding in maxillary sinus, which is due to an uncommon tissue reaction to cholesterol crystals on the maxillary sinus and is often associated to chronic sinonasal diseases, trauma, and surgery in the area, which may cause focal bleed [5]. It has, been projected that one of the pathogenesis is hemorrhage and subsequent hemolysis along with accumulation of cholesterol granules [6]. Histopathological analysis is crucial for the final diagnosis of maxillary sinus cholesterol granuloma, as its clinical and radiographic characteristics are non-specific, and individually sinonasal diseases require specific approach [7,8,9,10]. Adequate therapy necessitates complete excision or wide drainage. Adequate therapy is succeeded by using an endoscopic approach.
Since its signs and symptoms are unspecific, it is necessary to consider the cholesterol granuloma in the differential diagnosis sinonasal lesions with definitive diagnosis and confirmed by the histopathological investigation.
Conclusion
The first faced case of cholesterol granuloma of maxillary sinus in this region with a current and updated literature review is presented here. Cholesterol granuloma of maxillary sinus is uncommon and often overlooked by clinicians. It is necessary to consider the cholesterol granuloma of maxillary sinus in the differential diagnosis sinonasal lesions. Confirmation is by the histopathological analysis and should be removed surgically. This case may act for a reference for clinician to approach these kinds of cases.
Availability of data and materials
Not applicable.
References
Kikuchi T, So E, Ishimaru K, Miyabe Y, Abe K, Kobayashi T. Endoscopic sinus surgery in cases of cholesterol granuloma of the maxillary sinus. Tohoku J Exp Med. 2002;197:233–7.
Almada CB, Fonseca DR, Vanzillotta RR, Pires FR. Cholesterol granuloma of the maxillary sinus. Braz Dent J. 2008;19(2):171–4.
Cassano M, Pennella A, Taranto FD, Limosani P, Simone M. Cholesterol granuloma of the maxillary sinus in a young patient with associated neurosurgical pathology. Int J Ped Otorhinolaryngol. 2009;4(3):129–33.
Paik SW, Lee YS, Park D-J, et al. Cholesterol granuloma of the maxillary sinus presenting as an antrochoanal polyp. Ear Nose Throat J. 2019. https://doi.org/10.1177/0145561319879231.
Am J Otolaryngol. 2006;27(5):370–2
Leon ME, Chavez C, Fyfe B, et al. Cholesterol granuloma of the maxillary sinus. Arch Pathol Lab Med. 2002;126(2):217–9.
Chao TK. Cholesterol granuloma of the maxillary sinus. Eur Arch Otorhinolaryngol. 2006;263:592–7.
Ramani P, Murugesan K, Chandrasekar T, Anuja N. Cholesterol granuloma of maxillary sinus. Int J Oral Maxillofac Surg. 2006;35:1063–5.
Bella Z, Torkos A, Tiszlavicz L, Iván L, Jóri J. Cholesterol granuloma of the maxillary sinus resembling an invasive, destructive tumor. Eur Arch Otorhinolaryngol. 2005;262:531–53.
Kim D-J, Kim S-D, Kim S-H, et al. Endoscopic removal of huge cholesterol granuloma in the maxillary sinus confused with odontogenic keratocyst. J Craniofac Surg. 2020;31(2):507–9.
Acknowledgements
Not applicable.
Funding
There was no source of funding for the study.
Author information
Authors and Affiliations
Contributions
I (Srilatha K) am the sole contributor of this article, there are no other contributors involved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was taken from the Ethics Committee of the Fathima Institute of Medical Sciences, Kadapa, Andhra Pradesh, India. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants involved in the study.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kavarthapu, S. Cholesterol granuloma of the maxillary sinus: a case report. J Med Case Reports 18, 426 (2024). https://doi.org/10.1186/s13256-024-04561-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-024-04561-9