
Abstract
Background
Fetal midgut volvulus is an uncommon yet potentially life-threatening condition. Prenatal diagnosis may pose a challenge, due to the paucity of specific signs and symptoms. Timely prenatal diagnosis of this condition is imperative to prevent fetal mortality and morbidity.
Case presentation
We present a rare case report of fetal midgut volvulus, malrotation, and intestinal obstruction at 32 weeks of gestation in a 31-year-old multigravida Indian patient who presented with decreased fetal movements. Fetal ultrasound revealed midgut volvulus with proximal bowel obstruction and polyhydramnios. The patient underwent emergency surgery, which revealed intestinal malrotation and confirmed the diagnosis of midgut volvulus. Untwisting of the volvulus was done followed by Ladd’s procedure. Follow-up postoperative ultrasound was unremarkable.
Conclusions
Delay in the diagnosis of fetal midgut volvulus leads to poor fetal and maternal outcomes. Hence, it is vital for radiologists, sonologists, and obstetricians to be aware of this condition while performing fetal sonography. Prompt diagnosis and surgical intervention are vital to reduce the morbidity and mortality associated with this condition.
Similar content being viewed by others


Background
Midgut volvulus refers to the twisting of bowel loops around the mesenteric artery [1]. This leads to vascular congestion, poor venous return and eventual bowel obstruction, bowel infarction, perforation, or peritonitis [1,2,3,4,5,6]. It is more commonly seen postnatally than in the prenatal period [2, 3, 6, 7]. When encountered prenatally, the diagnosis of midgut volvulus is often challenging in the absence of specific signs and symptoms [7]. Timely diagnosis of this life-threatening condition is imperative to prevent fetal morbidity and mortality [3, 8].
We present and discuss the prenatal diagnosis of a rare case of fetal midgut volvulus with malrotation and intestinal obstruction.
Case presentation
A healthy 31-year-old multigravida Indian female, gravida 4, abortions 2, para 1 was referred to our ultrasound clinic with complaints of reduced fetal movements. Her anomaly scan was previously conducted at our clinic and was unremarkable.
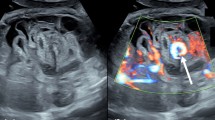
The fetus was 33 weeks 6 days of gestation according to her last menstrual period (LMP). Ultrasound was performed using a GE Voluson E10 ultrasound machine with a C2-9 curved array probe, and the fetus’s gestational age was found to be 32 weeks and 3 days. Head biometry and femur length of the fetus were below the tenth percentile. Polyhydramnios was noted. The fetal abdomen appeared distended with significantly dilated bowel loops. The maximum diameter of dilated bowel loops was approximately 23 mm (Fig. 1A). In fetal mid-abdomen, echogenic bowel loops with the classic “whirlpool sign” were demonstrated (Fig. 1B). The perianal muscular sphincter complex appeared normal. No signs of bowel perforation were detected on fetal ultrasound.

A,B Transverse transabdominal fetal sonography images demonstrating dilated bowel loops (white arrow) up to 2.3 mm (A) and classic “whirlpool sign” of twisted mesentery (yellow arrow) within the fetal abdomen (B)
The diagnosis of fetal volvulus with intestinal obstruction was made. The referring clinician was urgently informed about the findings, and the patient was referred to a tertiary care hospital. The patient was further counseled about the condition, regarding the need for emergency delivery and subsequent surgical intervention for the fetus.
Emergency lower-segment cesarean section (LSCS) was performed, and a female neonate weighing 1580 g was delivered. Apgar score was 9 and 10 at 1 and 5 minutes, respectively, and the vitals were within normal range.
On the basis of the fetal ultrasonography findings, emergency laparotomy was performed on the neonate at 4 hours after birth. Midgut volvulus was confirmed intraoperatively with the presence of malrotation (Fig. 2). No signs of bowel ischemia or necrosis were detected. Untwisting of the volvulus was performed followed by Ladd’s procedure. The postsurgical period was uneventful. Follow-up postoperative ultrasound done on day 1 postsurgery was unremarkable. On repeat visits, the infant’s growth was noted to be within the normal centiles for age. Follow-up ultrasound of the abdomen done at day 10 and at day 30 revealed nondilated bowel loops with normal peristalsis.

Intraoperative view of the intestine demonstrating midgut volvulus
Discussion
During the process of normal embryonic gut development, the fetal midgut undergoes a 270° counterclockwise rotation around the axis of the superior mesenteric artery between 4 and 8 weeks of gestation. Partial or complete failure of this rotation during embryogenesis leads to intestinal rotational abnormalities [9, 10]. Intestinal malrotation predisposes to midgut volvulus.
Fetal midgut volvulus is a rare entity diagnosed prenatally [3, 11]. It refers to the twisting of bowel loops around the mesenteric artery. This may lead to catastrophic complications, including intestinal obstruction, bowel ischemia, necrosis, perforation, and peritonitis [1].
Prompt diagnosis is vital to prevent undesirable maternal and fetal outcomes. Intrauterine diagnosis of fetal midgut volvulus is considered difficult and rare in literature [3, 9]. Ultrasound findings of fetal midgut volvulus include dilated intestinal loops and the classic “whirlpool sign” [12]. “Whirlpool sign” in midgut volvulus refers to the winding appearance of the mesentery and superior mesenteric vein wrapped around the superior mesenteric artery [12]. It has a high sensitivity, specificity, and accuracy for the detection of midgut volvulus [8]. Associated findings such as polyhydramnios, decreased fetal movements, and fetal ascites may be encountered [13, 14]. Fetal anemia may be seen in cases of intestinal volvulus. Increased peak systolic velocity (PSV) of the middle cerebral artery (MCA) on Doppler study can be indicative of fetal anemia, especially in the presence of fetal ascites, polyhydramnios, and dilated bowel loops [15]. Bartholmot et al. reported that decreased fetal movements in fetal volvulus was not an accidental finding. Moreover, the presence of a “fluid–fluid level” within the dilated bowel loops improves the diagnostic accuracy of findings on ultrasonography [16, 17]. The presence of a fluid–fluid level in dilated bowel loops indicates the absence of peristalsis and fetal intestinal distress [16].
“Coffee-bean sign” with or without whirlpool sign may be observed in fetuses with midgut volvulus [2, 16, 17]. It occurs in cases with closed-loop bowel obstruction and refers to the coffee-bean-like appearance of closely approximated dilated bowel loops [17, 18]
Detection of fetal midgut volvulus warrants an urgent neonatal surgical intervention. In the absence of associated anomalies, isolated midgut volvulus has a favorable prognosis postsurgery [14].
Conclusions
Intrauterine midgut volvulus is an uncommonly reported yet life-threatening condition. Delay in the diagnosis of fetal midgut volvulus leads to poor fetal and maternal outcomes. Hence, it is pertinent for radiologists, sonologists, and obstetricians to be aware of this condition while performing fetal sonography. Prompt diagnosis and surgical intervention are vital to reduce the morbidity and mortality associated with this condition.
Availability of data and materials
The data and materials supporting the findings of this study are available on request from the corresponding author.
Abbreviations
- LMP:
-
Last menstrual period
- LSCS:
-
Lower-segment cesarean section
- PSV:
-
Peak systolic velocity
- MCA:
-
Middle cerebral artery
References
Mustansir F, Farooq A, Baqir H, et al. A rare case of primary midgut volvulus necessitating extensive bowel resection in an adult. Cureus. 2019;11(6): e4833. https://doi.org/10.7759/cureus.4833.
Park JS, Cha SJ, Kim BG, Kim YS, Choi YS, Chang IT, Kim GJ, Lee WS, Kim GH. Intrauterine midgut volvulus without malrotation: diagnosis from the ‘coffee bean sign.’ World J Gastroenterol. 2008;14(9):1456–8. https://doi.org/10.3748/wjg.14.1456.
Gerçel G, Anadolulu Aİ. Intrauterine midgut volvulus as a rare cause of intestinal obstruction: a case report. J Med Case Rep. 2021;15:239. https://doi.org/10.1186/s13256-021-02778-6.
Steffensen TS, Gilbert-Barness E, DeStefano KA, Kontopoulos EV. Midgut volvulus causing fetal demise in utero. Fetal Pediatr Pathol. 2008;27(4–5):223–31. https://doi.org/10.1080/15513810802319608.
Best EJ, O’Brien CM, Carseldine W, Deshpande A, Glover R, Park F. Fetal midgut volvulus with meconium peritonitis detected on prenatal ultrasound. Case Rep Obstet Gynecol. 2018;2018:1–6. https://doi.org/10.1155/2018/5312179.
Molvarec A, Bábinszki Á, Kovács K, Tóth F, Szalay J. Intrauterine intestinal obstruction due to fetal midgut volvulus: a report of two cases. Fetal Diagn Ther. 2006;22(1):38–40. https://doi.org/10.1159/000095841.
Cañizo Vázquez D, Izquierdo Renau M, Inarejos Clemente EJ, Bejarano Serrano M, Suñol Capella M, Morillo Palomo A. Intrauterine intestinal volvulus. J Pediatr. 2019. https://doi.org/10.1016/j.jpeds.2019.11.017.
Zhang W, Sun H, Luo F. The efficiency of sonography in diagnosing volvulus in neonates with suspected intestinal malrotation. Medicine. 2017;96(42): e8287. https://doi.org/10.1097/MD.0000000000008287.
Langer JC. Intestinal rotation abnormalities and midgut volvulus. Surg Clin North Am. 2017;97(1):147–59. https://doi.org/10.1016/j.suc.2016.08.011.
Haqqani M, Seetharaman M, Teo R, Adkisson C, Nessen M, Dauer M, Kim PK. Midgut malrotation complicated by small bowel obstruction in an 80-year-old woman: a case report. Int J Surg Case Rep. 2019;63:89–93. https://doi.org/10.1016/j.ijscr.2019.09.008.
Pal K, Zayed LH, Khalid YM. Intrauterine intestinal volvulus prompting emergency delivery and surgery in a 32wk fetus. J Pediatr Surg Case Rep. 2020;61: 101618. https://doi.org/10.1016/j.epsc.2020.101618.
Rokade ML, Yamgar S, Tawri D. Ultrasound “whirlpool sign” for midgut volvulus. J Med Ultrasound. 2011;19(1):24–6. https://doi.org/10.1016/j.jmu.2011.01.001.
Chen J, Wu D. Prenatal diagnosis of fetal midgut volvulus: a case description. Quant Imaging Med Surg. 2022;12(8):4326–30. https://doi.org/10.21037/qims-22-37.
Monard B, Mottet N, Ramanah R, Riethmuller D. Prenatal diagnosis of a segmental small bowel volvulus with threatened premature labor. Case Rep Obstet Gynecol. 2017;2017:1–5. https://doi.org/10.1155/2017/7642784.
Kornacki J, Czarnecka M, Błaszczyński M, Skrzypczak J, Gadzinowski J, Jankowski A, Sardesai S. Congenital midgut volvulus associated with fetal anaemia. Fetal Diagn Ther. 2010;28(2):119–22. https://doi.org/10.1159/000315051.
Bartholmot C, Faure J, Grosjean F, Couture A, Forgues D, Fuchs F, Prodhomme O. Prenatal diagnosis of antenatal midgut volvulus: specific ultrasound features. Prenat Diagn. 2018. https://doi.org/10.1002/pd.5392.
Li X, Huang T, Zhou M, Zhang C. Prenatal diagnosis of midgut volvulus using two-dimensional and three-dimensional ultrasound. Am J Transl Res. 2022;14(3):1859–67.
Olutoye O, Ohuoba E, Fruhman G, Zacharias N. Perinatal survival of a fetus with intestinal volvulus and intussusception: a case report and review of the literature. Am J Perinatol Rep. 2013;03(02):107–12. https://doi.org/10.1055/s-0033-1349367.
Acknowledgements
The authors would like to express their deepest gratitude to Dr. Mithun KN, consultant pediatric surgeon and pediatric urologist and neonatal surgeon, Kiran Hospital, Surat, India for his guidance.
Funding
Not applicable as no funding or grants were available for this study.
Author information
Authors and Affiliations
Contributions
N.J.: conceived of the study, analyzed and interpreted the radiological studies, and participated in the manuscript design. S.S.A.: drafted the manuscript, reviewed the literature, and analyzed and interpreted the radiological studies. S.B.: analyzed and interpreted the radiological studies and participated in the manuscript design. T.G.: participated in the manuscript design. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved from ethical committee of the institution. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jain, N., Awal, S.S., Biswas, S. et al. Prenatal diagnosis of fetal midgut volvulus: a case report. J Med Case Reports 16, 482 (2022). https://doi.org/10.1186/s13256-022-03720-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-022-03720-0