
Abstract
Background
Extragonadal germ cell tumor (EGCT) is a relatively rare condition, reportedly representing 3–7% of all germ cell tumors. We report a patient who had metachronous testicular tumor with uncommon metastases 20 years after primary retroperitoneal EGCT treatment, along with a corresponding literature review.
Case presentation
A 49-year-old Japanese man visited our department in November 2017 with chief complaints of indolent right scrotum enlargement and a right inguinal mass. History showed that the patient visited our department of gastroenterology with chief complaints of blackish feces and ill complexion in February 1997. Computed tomography (CT) showed a right retroperitoneal tumor, which was removed in the same month. Histopathological examination showed a teratoma and yolk sac tumor. He was diagnosed with primary retroperitoneal EGCT and received three courses of chemotherapy (bleomycin/etoposide/cisplatin; BEP). Periodic imaging and the determination of tumor markers (alpha-fetoprotein [AFP], human chorionic gonadotropin [HCG], and lactate dehydrogenase [LDH]) showed no recurrence or metastasis during the 5 years postoperatively. Subsequently, he did not visit the outpatient ward. In August 1999, he underwent surgery of right hydrocele. Contrast-enhanced CT showed a 35-mm contrast effect with uneven content in the right testicle and enlarged nodes that raised suspicion for metastases in the right inguinal and right external iliac lymph nodes. All tumor markers were within normal ranges. He underwent right high orchiectomy and resection of the right inguinal lymph nodes in the same month. Histopathological findings revealed seminoma (pT1, pN2, M0, S0, and TNM stage IIB). He received postoperative chemotherapy, one course of BEP therapy, and three courses of etoposide and cisplatin therapy. Post-chemotherapy CT confirmed a complete clinical response at the right external iliac lymph nodes, and this response continued 12 months later. No recurrence or metastasis has been found so far.
Conclusions
We report a patient in whom a testicular tumor with uncommon metastases occurred 20 years after primary retroperitoneal EGCT treatment. After EGCT treatment, testicular relapses tend to occur after relatively long-term follow-up. After EGCT treatment, such patients must be closely monitored for testicular recurrences and onset of testicular tumor.
Similar content being viewed by others
Background
The primary site of male germ cell tumors is most commonly the testicle. Extratesticular (extragonadal) onset of these tumors is reported in 3–7% of cases. It has been reported that metachronous testicular tumors may occur after the treatment of extragonadal germ cell tumor (EGCT) in 5% of EGCT patients [1]. This case report describes a patient who experienced a testicular tumor with uncommon metastases 20 years after primary retroperitoneal EGCT treatment, along with a corresponding literature review.
Case presentation
A 49-year-old Japanese man visited our department in November 2017 with chief complaints of indolent right scrotum enlargement and a right inguinal mass. History showed that the patient visited our department of gastroenterology with chief complaints of blackish feces and ill complexion in February 1997. Gastrointestinal fiberscopy was used to treat duodenal ulcer bleeding. Computed tomography (CT) showed a right retroperitoneal tumor, which was removed in the same month.
Histopathological examination showed a teratoma and yolk sac tumor (Fig. 1). He was diagnosed with primary retroperitoneal EGCT and underwent three courses of chemotherapy (bleomycin/etoposide/cisplatin; BEP) starting in May 1997. He was closely followed using procedures including periodic imaging, tumor markers determination, and self-palpation.

Histopathological findings of the primary retroperitoneal extragonadal germ cell tumor show the characteristics of teratoma for hematoxylin and eosin (HE) staining (a ×100) and yolk sac tumor for HE staining (b ×200); the site of the yolk sac tumor was positive for alpha-fetoprotein (AFP) immunostaining (c ×200).
He was followed up on an outpatient basis 5 years after treatment and was subsequently lost to follow-up. In August 1999, he underwent surgery of the right hydrocele. At that time, perioperative findings were unremarkable, indicating no clear tumor in either testicle.
At the first visit, his height was found to be 163 cm, and weight was 58.5 kg.
Blood pressure was 128/78 mmHg, heart rate was regular at 62 beats per minute, and body temperature was 36.4 °C.
He had no history of smoking or drinking, and there was nothing remarkable in the family history.
On physical examination, the right testicle was found to be elastic, hard, and enlarged to the size of 40 × 40 mm. A 45 × 40 mm sized induration was palpable in the right inguinal area and was adequately mobile. Neurological examination showed no abnormal findings. Blood biochemistry examination, urinalysis, and tumor markers (alpha-fetoprotein [AFP], human chorionic gonadotropin [HCG], and lactate dehydrogenase [LDH]) showed no abnormal findings.
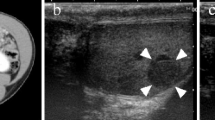
Ultrasound findings showed a mosaic shadow inside the right testicle, with no abnormal findings in the left testicle.
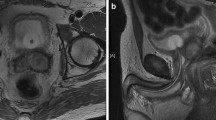
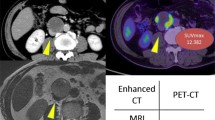
During other diagnostic imaging procedures, enlargements of the right external iliac lymph node (24 × 14 mm) and right inguinal lymph node (43 × 29 mm) and a 31 × 22 mm mass with uneven contents were found in the right testicle (Fig. 2). There was no evidence of any distant metastasis.

Contrast-enhanced pelvic CT. a Enlarged right external iliac lymph node (white arrow). b Enlarged right inguinal lymph node (white arrow). c Enhanced right testicular tumor (white arrow). The diagnosis was testicular tumor (cT1, N2, M0, S0, and TNM stage IIB)
For the right testicular tumor, the patient underwent high orchiectomy and resection of the right inguinal lymph nodes in November 2017. The testicular tumor was 40 × 40 × 30 mm in size and weighed 34 g. The lymph node was 40 × 40 × 30 mm in size and weighed 21 g. The cut surfaces of both specimens were yellowish and solid, and the testicular tumor was localized in the testicle (Fig. 3).

a Resected testicular tumor was 40 × 40 × 30 mm in size and weighed 34 g. b Resected inguinal lymph node was 40 × 40 × 30 mm in size and weighed 21 g. The cut surfaces of both specimens were yellowish and solid, and the testicular tumor was localized in the testicle.
Histopathological findings showed irregular cobblestone proliferations of germ cell-like atypical cells with clear nucleoli and massive necrotic changes that partially resulted from self-destruction. The tumor did not extend into the tunica albuginea, and no vascular infiltration was found. Spermatic cord stumps were negative. Tumor diagnosis was a classical seminoma with no other elements. Lymph node metastases were also diagnosed as a result of the seminoma (Fig. 4).

Both the testicular tumor and inguinal lymph node presented with irregular cobblestone proliferations of germ cell-like atypical cells with clear nucleoli and no vascular proliferation. Spermatic cord stump was negative, showing that this tumor was a classical seminoma for hematoxylin and eosin staining (left ×100, right ×200).
Based on the above findings, this seminoma was diagnosed as pT1, pN2, M0, S0, and TNM stage IIB [2].
The patient received postoperative chemotherapy with one course of BEP therapy and three courses of etoposide and cisplatin (EP) therapy at the Japan Community Health care Organization Kani Tono Hospital starting in January 2018.
Post-chemotherapy CT confirmed a complete clinical response (cCR) at the right external iliac lymph node, and this response continued 12 months later (Fig. 5).

Contrast enhanced pelvic CT images before chemotherapy. a Enlarged right external iliac lymph node (white arrow). b Clinical complete response was confirmed after chemotherapy (white arrow). c Clinical complete response continued 12 months after chemotherapy (white arrow)
Discussion
Metastases of the testicular tumor to the retroperitoneal lymph node are the most common. We reported a patient who had metachronous testicular tumor with metastases to the groin and external iliac lymph nodes 20 years after primary retroperitoneal EGCT treatment.
EGCT accounts for 3–7% of all germ cell tumors [1]. Several onset mechanisms have been reported; primordial germ cells remain at extragonadal sites, including the mediastinum and retroperitoneum, due to the abnormal migration of such cells during mobilization to the urogenital swelling at embryogenesis, and EGCT originates from germ cells that are physiologically distributed in the liver, bone marrow, and brain for the transport of hematological and immunological information [3, 4]. Among patients who experienced cCR, metachronous testicular tumor (MTT) was reported in approximately 5% of patients [1]. Among patients who experienced cCR after EGCT treatment, MTT onset was reported in 16 of 635 patients as reported by Bokemeyer et al. [5], and 5 of 51 patients as reported by Hashimoto et al. [6].
The mechanism of MTT after EGCT is unknown. Daugaard et al. performed bilateral testicular biopsy in 46 patients who were diagnosed with EGCT after excluding testicular tumors by palpation and ultrasound examinations [7]. Germ cell neoplasia in situ (GCNIS) was confirmed in 42% of the patients, and the origins of EGCT and GCNIS were reported to be the same. The patient in this report, however, received three courses of BEP therapy after EGCT diagnosis. It was impossible to establish why chemotherapy was administered. Our patient experienced cCR after BEP and EP therapies, similar to his treatment 20 years previously. If the origin was the same between EGCT and GCNIS, the latter tumor must have disappeared after the previous chemotherapy. We therefore did not consider that the origins of EGCT and GCNIS were the same.
Tanio et al. summarized 37 cases of MTT after EGCT treatment in Japan and overseas countries [8]. After exclusion of four patients whose primary sites were unknown and the mediastinum, the most frequent site was the retroperitoneum, as reported in 29 patients. According to our search of patients with primary retroperitoneal EGCT, including the patient in this article, MTT was found in 31 patients. Table 1 summarizes these patients [1, 6, 9,10,11,12,13,14,15,16,17,18]. The age of the patients ranged from 18 to 49 years, with a median age of 30 years. In most patients, the histological type was non-seminoma for EGCT and seminoma for MTT. The histological type in our patient also differed from previous reports. The time to MTT onset was relatively long, ranging from 14 to 248 months, with a median of 64 months, and the time to the second onset 20 years after treatment in our patient was the longest among the 31 patients. At the time of MTT diagnosis, 18 patients had no metastasis, and seven patients, including our patient, experienced metastases. All patients underwent a high orchiectomy. Patients with metastases received postoperative chemotherapy. Prognosis was satisfactory; among patients whose postoperative courses were available, 28 patients were alive, with no recurrence in all but one patient.
Conventionally, lymph ducts from the testicles flow into the para-aortic and para-vena cava lymph nodes via the spermatic cord. Metastases to the retroperitoneal lymph node were the most frequent, as reported in 88% of EGCT patients [19]. Our patient, however, experienced metastases to the groin and external iliac lymph nodes. Jerome et al. reported the following possible reasons for the occurrence of testicular tumor non-regional metastases to groin lymph nodes: (1) tumor infiltration to the epididymis, spermatic cord, and scrotal skin; (2) history of surgical procedures in the groin or scrotum; (3) retrograde metastases from metastases to the retroperitoneal lymph nodes; and (4) direct infiltration of residual lesions in the spermatic cord [20]. In the Japanese General Rules for the Surgical and Pathological Studies on Testicular Tumors, it is noted that in patients undergoing scrotal and groin surgical procedures, lymph nodes in the pelvis and groin are also regarded as regional lymph nodes [21]. Our patient also had a history of radical right hydrocele treatment 18 years previously. This treatment changed his lymph flow, probably causing metastases to the groin and external iliac lymph nodes. In the treatment of patients with testicular tumors who have undergone surgical treatment in the groin or scrotum, it is necessary to consider possible metastases to lymph nodes in the groin and pelvis.
As described previously, MTT prognosis tends to be satisfactory in patients with primary retroperitoneal EGCT. This is because seminoma is the most frequent type of MTT. Moreover, MTT tends to occur after relatively long periods of time and may be a biologically less malignant germ cell tumor. For MTT treatment, it is nevertheless important to consider the fact that MTT may occur 20 years after EGCT treatment, and that the tumor has already metastasized at its diagnosis, as in our patient.
Conclusion
We encountered a patient in whom a testicular tumor with uncommon metastases occurred 20 years after primary retroperitoneal EGCT treatment. After EGCT treatment, testicular relapses tend to occur after relatively long-term follow-up. After EGCT treatment, such patients must be closely monitored for testicular recurrences and onset of testicular tumor.
Availability of data and materials
Not applicable.
Abbreviations
- EGCT:
-
Extragonadal germ cell tumor
- MTT:
-
Metachronous testicular tumor
- CT:
-
Computed tomography
- AFP:
-
Alpha-fetoprotein
- HCG:
-
Human chorionic gonadotropin
- LDH:
-
Lactate dehydrogenase
- EP:
-
Etoposide and cisplatin
- cCR:
-
Complete clinical response
- GCNIS:
-
Germ cell neoplasia in situ
References
Hartman JT, Fossa SD, Nichols CR, et al. Incidence of metachronous testicular cancer in patients with extragonadal germ cell tumors. J Natl Cancer Inst. 2001;93:1733–8.
Moch H, Humphrey PA, Ulbright TM, Reuter VE. WHO classification of tumours of the urinary system and male genital organs. Geneva: WHO Press; 2016.
Friedman NB. The function of the primordial germ cell in extragonadal tissues. Int J Androl. 1987;10:43–9.
Chaganti RSK, Houldsworth J. Genetics and biology of adult human male germ cell tumors. Cancer Res. 2000;60:1475–82.
Bokemeyer C, Nichols CR, Droz JP, Schmoll HJ, et al. Extragonadal germ cell tumors of the mediastinum and retroperitoneum: results from an international analysis. J Clin Oncol. 2002;20:1864–73.
Hashimoto K, Fujimoto H, Kouno T, Koseki M, et al. The incidence and management of metachronous testicular germ cell tumors in patients with extragonadal germ cell tumors. Urol Oncol. 2012;30:319–24.
Daugaard G, Rørth M, von der Maase H, Skakkebaek NE. Management of extragonadal germ cell tumors and the significance of bilateral testicular biopsies. Ann Oncol. 1992;3:283–9.
Tanio M, Aoki Y, Kobayashi H, Yokoi S, et al. A case of metachronal testicular tumor eight years after medical treatment of extragonadal germ cell tumor. Hinyokika Kiyo. 2015;61:173–6.
González Quintela A, López Bonet E, Román J, Aramburo P. Testicular germ cell tumor seven years after a retroperitoneal germ cell tumor. Eur Urol. 1991;19:336–8.
Lokich J. Metachronous gonadal and extragonadal primary germ cell tumors: two case reports. Cancer Invest. 1994;12:406–8.
Hayashi T, Mine M, Kojima S, Sekine H. Extragonadal germ cell tumor followed by metachronous testicular tumor. A case report. Urol Int. 1996;57:194–6.
Gerl A, Clemm C, Lamerz R, Wilmanns W. Cisplatin-based chemotherapy of primary extragonadal germ cell tumors. A single institution experience. Cancer. 1996;77:526–32.
Allaway M, Nseyo UO. Primary testicular seminoma in a patient with a history of extragonadal non-seminomatous germ cell carcinoma. Urology. 2000;55:949–50.
Daniel C, Fizazi K, Culine S, Zelek L, Wibault P, Theodore C. Metachronous gonadal and extragonadal primaries, or late relapse of germ cell tumor? Urol Oncol. 2001;6:49–52.
Mindrup SR, Konety BR. Testicular recurrence from “primary” retroperitoneal germ cell tumor. Urology. 2004;64:1031.
Kuroda I, Ueno M, Mitsuhashi T, Nakagawa K, Yanaihara H, et al. Testicular seminoma after the complete remission of extragonadal yolk sac tumor: a case report. BMC Urol. 2004;4:13.
Yamada Y, Tomita K, Fujimura T, Nishimatsu H, et al. Metachronous testicular tumor developing eight years after retroperitoneal extragonadal germ cell tumor. Int J Urol. 2008;15:267–9.
Kawamura N, Yamamoto K, Yoshioka I, Kiuchi H, et al. A case of metachronous testicular tumor developing seven years after complete remission of retroperitoneal extragonadal germ cell tumor. Hinyokika Kiyo. 2009;55:635–8.
von der Maase H, Specht L, Jacobsen GK, Jakobsen A, et al. Surveillance following orchidectomy for stage I seminoma of the testis. Eur J Cancer. 1993;29:1931–4.
Jerome PR, Graeme SS, et al. Neoplasms of the testis. In: Walsh PC, Retrik AB, et al., editors. Campbell’s urology, vol. 4. 8th ed. Philadelphia: W.B. Saunders Co; 2002. p. 2882–3.
Japanese Urological Association, The Japanese Society of Pathology. General rule for clinical and pathological studies on testicular tumors. 4th ed. Tokyo: KANEHARA & CO., LTD.; 2018. p. 28.
Acknowledgements
The authors wish to thank the patient and his family for allowing them to publish this work.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
The surgery was performed at the Japan Organization of Occupational Health and Safety Asahi Rosai Hospital, and chemotherapy was performed at the Japan Community Health care Organization Kani Tono Hospital. MT drafted the manuscript. KO performed the pathological diagnosis. KH, SM, HM, and GN treated the patient. NA, KO, CN, AH, MN, and IT cared for the patient. SA and YY supervised the writing of the report. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
In our institution, institutional review board approval is not required for a case report.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tobiume, M., Aoki, S., Nishikawa, G. et al. Late testicular relapse two decades after primary extragonadal germ cell tumor with uncommon metastases: a case report. J Med Case Reports 15, 59 (2021). https://doi.org/10.1186/s13256-021-02667-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-021-02667-y