
Abstract
Objectives
To investigate the optimal parameters of spectral CT for preferably visualizing the periprosthetic vasculature and metal artifact reduction (MAR) in total hip arthroplasty (THA).
Methods
A total of 34 THA of 30 patients were retrospectively included. Image reconstructions included conventional image (CI), CI combined with MAR (CIMAR), and virtual monoenergetic images (VMI) combined with MAR (VMIMAR) at 50–120 keV. The attenuation and standard deviation of the vessel and artifact, and the width of artifact were measured. Qualitative scoring was evaluated including the vascular contour, the extent of artifact, and overall diagnostic evaluation.
Results
The attenuation, noise of the vessel and artifact, and the width of artifact decreased as the energy level increased (p < 0.001). The downtrend was relatively flat at 80–120 keV, and the vascular attenuation dropped to 200 HU at 90 keV. The qualitative rating of vascular contour was significantly higher at CIMAR (3.47) and VMIMAR 60–80 keV (2.82–3.65) compared with CI (2.03) (p ≤ 0.029), and the highest score occurred at 70 and 80 keV (3.65 and 3.56). The score of the extent of artifact was higher at VMIMAR 80 keV than CIMAR (3.53 VS 3.12, p = 0.003). The score of the overall diagnostic evaluation was higher at VMIMAR 70 and 80 keV (3.32 and 3.53, respectively) than CIMAR (3.12) (p ≤ 0.035).
Conclusion
Eighty kiloelectron volts on VMIMAR, providing satisfactorily reduced metal artifacts and improved vascular visualization, can be an optimal recommended parameter of spectrum CT for the assessment of periprosthetic vasculature in THA patients.
Critical relevance statement
The metal artifact is gradually reducing with increasing energy level; however, the vascular visualization is worsening. The vascular visualization is terrible above 100 keV, while the vessel is disturbed by artifacts below 70 keV. The best performance is found at 80 keV.
Key points
• VMIMAR can provide both reduced metal artifacts and improved vascular visualization.
• Eighty kiloelectron volts on VMIMAR performs best in vascular visualization of total hip arthroplasty patients.
• Energy spectrum CT is recommended for routine use in patients with total hip arthroplasty.
Graphical Abstract

Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Total hip arthroplasty (THA) has become one of the most cost-effective and successful orthopedics procedures in patients with severely symptomatic hip disease [1]. With a significant increase in annual rates of primary and revision THA, accompanied by increasing concern about intraoperative and postoperative complications [2, 3]. Vascular injuries are uncommon but potentially devastating during replacement. The external iliac and common femoral vessels at the periprosthetic area are the most injured [4]. Early diagnosis and intervention are critical to avoid these dreaded complications. In addition, THA has been reported as an increased risk of peripheral arterial disease (PAD), and patients with THA exhibited a 1.24-fold higher risk of developing PAD than patients without THA [5,6,7,8,9]. Therefore, accurate assessment of relevant anatomy and pathology of periprosthetic vessels is essential to THA patients in both preoperative planning and postoperative follow-up for avoiding vascular-related complications.
Computed tomographic angiography (CTA) has gained wide acceptance as a valid modality for the noninvasive assessment of peripheral vasculatures. However, the metal artifacts resulting from beam hardening, photon starvation, and scattering are a great challenge for visualizing the periprosthetic vessels in THA patients [10,11,12]. Energy spectral CT has emerged as a promising tool in diagnostic imaging with multiple potential clinical applications. Virtual monoenergetic images (VMI) and orthopedic metal artifact reduction (O-MAR) software based on DE-CTA can provide high image quality of vessels and remarkably reduce metal artifacts compared to conventional CT and CTA, respectively [13,14,15,16,17,18,19,20]. Nevertheless, it is still unknown whether these advanced techniques are suitable for the evaluation of periprosthetic vessels in THA patients. According to previous studies, the recommended parameters seem somewhat contradictory, high keV level images prefer to display MAR while low keV levels are better for vessels, between optimal visualization of the vessel and MAR of the prosthetic joint [14, 21,22,23]. And the impact of O-MAR techniques on the surrounding vasculature is also unclear.
Thus, this study aimed to assess the quantitative image quality of VMI of DE-CTA and to define the optimal parameters for better visualizing the periprosthetic vasculature combined with metal artifact reduction in THA patients.
Materials and methods
Patients
This study was approved by our local institutional review board. Informed consent was waived because of its retrospective character. We included DE-CTA examinations of 34 THA joints with 30 patients (19 men, 11 women, mean age 66.13 ± 12.77 years, range 32–87 years, BMI 16.9–29.4) in our institution. The inclusion criteria were (1) patients were performed a preoperative evaluation of revision THA and (2) patients were conducted within the routine clinical practice for the evaluation of peripheral artery after THA. The exclusion criteria were examinations with severe motion artifacts, images with poor quality, or incomplete raw data influencing spectral reconstruction.
Image acquisition
All scans were performed on a dual-layer detector CT scanner (IQon spectral CT, Philips Healthcare). The scanning parameters were as follows: tube voltage, 120 kVp; collimation, 64 × 0.625; pitch, 0.391; rotation time: 0.5 s; matrix, 512 × 512. A bodyweight adapted bolus of contrast agent (370 mg I/mL, Iopromide, Ultravist, Bayer Healthcare, Germany) was injected through a peripheral vein with a flow rate of 2.5–4.0 mL/s. Bolus-tracking technique with a delay of 35–40 s was used for contrast-enhanced imaging.
Image reconstruction
Conventional image, conventional image combined with O-MAR, and VMI combined with O-MAR were reconstructed, which would be referred to as CI, CIMAR, and VMIMAR. CI, CIMAR, and VMIMAR were reconstructed in the axial plane with a slice thickness of 0.8 mm and section increments of 0.6 mm for meeting the clinical pre-operative requirement of 3D printing customized prostheses. CI, CIMAR, and VMIMAR were computed using a dedicated reconstruction algorithm (Spectral B, level 3, Philips Healthcare). To ensure sufficient opacification of the vessel (> 200 HU), the VMIMAR was reconstructed in the range of 50 to 120 keV at 10-keV intervals as vascular opacification is insufficient over 120 keV levels [13, 24].
Image analysis
Quantitative and qualitative analysis was carried out using the proprietary image viewer (Philips IntelliSpace Portal).
For quantitative assessment, the axial slices where the vessel was most disturbed by the metal artifact were selected. The regions of interest (ROI) were placed in the external iliac or common femoral arteries and the most pronounced hyperdense artifact close to the vessel by one musculoskeletal radiologist (Zhao, with 2 years of clinical experience). ROIs were placed on CI with soft tissue window (width 360 HU, center 60 HU) [17, 25]. The location and size of the ROIs (contour of artery and 20 mm2 for metal artifacts) were then used as a template for the other image reconstructions and thus kept constant on CI, CIMAR, and VMIMAR [17, 25, 26]. Attenuation values and standard deviation within the ROI were automatically recorded from the same ROI on CI, CIMAR, and VMIMAR at 50 keV, 60 keV, 70 keV, 80 keV, 90 keV, 100 keV, 110 keV, and 120 keV. In addition, the width of the most pronounced hyperdense artifact was manually measured (Fig. 1).

Illustration of the quantitative assessment of image quality. The axial slices where the vessel was most disturbed by the metal artifact were selected. Regions of interest (ROI) were placed in the external iliac or common femoral vessels (red circle) and the most pronounced hyperdense artifact (blue circle). Attenuation values and standard deviations within the ROI were automatically recorded. Additionally, the width of the most pronounced hyperdense artifact was measured close to the metal implant in its largest diameter (black line). ROIs were kept constant and measurements of width were conducted in the same location on CI, CIMAR, and VMIMAR (CI indicates conventional images; CIMAR indicates conventional images combined with orthopedic metal artifact reduction; VMIMAR indicates virtual monoenergetic images combined with orthopedic metal artifact reduction)
For qualitative assessment, the vascular contour, the extent of artifact, and overall diagnostic evaluation were separately assessed by two musculoskeletal radiologists (Zhao and Yang, with 2 and 18 years of clinical experience, respectively) using a five-point Likert scale in the same axial slice. The radiologists had accepted a series of training about the subjective scoring system and performed several group meetings for the consensus evaluation referring to previous studies [20, 27, 28]. The vascular contour was graded as follows: blurred vascular contour = 1, less clear vascular contour = 2, basically sharp vascular contour = 3, relatively sharp vascular contour = 4, and very sharp vascular contour = 5 [27]. The extent of artifact was rated as follows: massive artifacts = 1, pronounced artifacts = 2, moderate artifacts = 3, little artifacts = 4, no artifacts = 5. The overall diagnostic evaluation was rated as follows: nondiagnostic = 1, poor quality = 2, moderate quality = 3, good quality = 4, and excellent quality = 5 [28].
Statistical analysis
Statistical analysis was performed using SPSS software version 26 (IBM Corp., Armonk, NY, USA). All data were expressed as mean ± SD. Quantitative measurements (attenuation, noise of the vessel and artifact, and the width of artifact) were tested for normal distribution using the Shapiro–Wilk test, and repeated measures analysis of variance was applied if the data had a normal distribution; otherwise, the Friedman test and Wilcoxon test were used to compare the variables among the reconstructions. And the Friedman test and Wilcoxon test were also used for qualitative measurements. A p-value of less than 0.05 was considered statistically significant and adjustment for multiple comparisons was implemented with Bonferroni correction. Inter-rater agreement was assessed using Cohen’s kappa analysis.
Results
Reduction of hyperdense artifacts
Compared to the positive Hounsfield Unit (HU) of hyperdense artifacts measured on CI (696.04 ± 218.17 HU), the attenuation of artifacts on CIMAR significantly decreased (490.82 ± 181.42 HU, p < 0.001); the attenuation of artifacts on the VMIMAR at 60 – 120 keV were lower than CI, and the differences were significant on the VMIMAR at 80–120 keV (p < 0.001) (Table 1). And the significant difference was detected among the different keV levels of the VMIMAR (p < 0.05). In the VMIMAR series, the attenuation of hyperdense artifacts gradually decreased with increased keV levels; the attenuation of artifacts on VMIMAR 80 keV was significantly lower than CIMAR (469.36 ± 162.21 HU VS 490.82 ± 181.42 HU, p = 0.005). The downtrend showed sharp at 50–70 keV and, relatively flat at 80–120 keV (Fig. 2A).

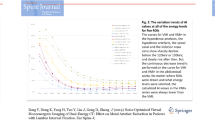
The trend chart of the attenuation (a), the noise (c) of the vessel and artifact, and the width of artifact (b) in CI, CIMAR, and VMIMAR of various keV levels (50 – 120 keV). The attenuations, widths, and noises of hyperdense artifacts and periprosthetic vessels all gradually decrease with increased keV levels. The similar downtrends all show sharp at 50–70 keV and, relatively flat at 80–120 keV. At 80 keV level, the vascular attenuation is higher than 200 HU which is sufficient vascular opacification, simultaneously, the attenuation of artifacts is also below 500 HU (a). The vascular attenuation gradually drops to 200 HU at 90 keV. And the change of the width of artifacts, the noises of vessels and artifacts tend to be stable and small among the keV levels over 80 compared to the 50–70 keV levels (b–c). The vascular noise on VMIMAR at 50–70 keV was even higher than that on CI (c)
The average width of the hyperdense artifacts on CI was 48.51 ± 16.33 mm, and significantly reduced on CIMAR (28.74 ± 9.9 mm, p < 0.001); the average width of the hyperdense artifacts on VMIMAR was lower than CI, and the differences were significant on the VMIMAR at 70–120 keV (p < 0.001, Table 1). The average width of the hyperdense artifacts gradually decreased with increased keV levels and was significantly lower than CIMAR on VMIMAR 80 keV (26.76 ± 10.37 mm VS 28.74 ± 9.9 mm, p < 0.001), with the lowest occurring on VMIMAR 120 keV (22.41 ± 10.69 mm, p < 0.001). A similar downtrend was observed at the different keV levels. The difference between 50 and 80 keV was about 9 mm, while it was only about 3 mm between 90 and 120 keV (Fig. 2B).
Vascular attenuation
Vascular attenuation was found highest on VMIMAR 50 keV (555.19 ± 141.19 HU) compared to all other reconstructions. Compared to the vascular attenuation measured on the CI (387.26 ± 73.65 HU), the attenuation decreased on CIMAR and VMIMAR at 70–120 keV, and the differences were significant on CIMAR and VMIMAR at 80–120 keV (p < 0.001). In the VMIMAR series, vascular attenuation gradually dropped to 200 HU at 90 keV with increased keV levels (Fig. 2A).
Image noise in vessels and artifacts
Image noise in artifacts was found highest on CI and VMIMAR 50 keV (122.92 ± 53.34, 125.37 ± 64.79, respectively). In the VMIMAR series, image noise in artifacts gradually decreased with increased keV levels. The downtrend was also steep at 50 – 80 keV and, relatively smooth at 90–120 keV. And no significant difference was detected at 100–120 keV (p > 0.655). Image noise in artifacts on VMIMAR 80 keV was lower than CIMAR without significant difference (80.68 ± 32.42 VS 82.08 ± 33.07, p = 0.274) (Table 1, Fig. 2C).
The image noise of the vessel was highest on VMIMAR 50 keV (64.61 ± 50.01), then gradually decreased with the increased keV levels. The vascular noise on CIMAR and VMIMAR at 50–70 keV was even higher than that on CI (37.42 ± 18.57). Compared to vascular noise on CIMAR (45.34 ± 27.78), vascular noise was lower on VMIMAR at 70–120 keV, and the differences were significant on VMIMAR at 80–120 keV (p = 0.004). In the VMIMAR series, the downtrend was not obvious at 90–120 keV and without significant difference (p > 0.815) (Table 1, Fig. 2C).
Reliability and subjective scoring
The two reading radiologists had similar scores in 916 out of 1020 ratings (89.8%), with a kappa value of 0.865 (SE = 0.013, 95% CI: 0.840–0.890). The score of vascular contours was measured as 2.03 on CI and 3.47 on CIMAR. The score of vascular contours was higher on CIMAR and VMIMAR at 50–90 keV than on CI, and the differences were significant on CIMAR and VMIMAR at 60–80 keV (p ≤ 0.029). In the VMIMAR series, the score of vascular contours gradually improved with the increased keV levels, higher than CIMAR at 70 keV and 80 keV (3.65 and 3.56 respectively, p > 0.083), and then gradually decreased to the lowest at 120 keV (1.09). The score of the extent of artifact was measured as 1.06 on CI and 3.12 on CIMAR. The score of the extent of artifact was significantly higher on CIMAR and VMIMAR than on CI (p < 0.018). In the VMIMAR series, score of the extent of artifact gradually improved with the increased keV levels, and was significantly higher on VMIMAR 80 keV than on CIMAR (3.53 vs. 3.12, p = 0.003), reaching the highest at 120 keV (4.03). However, no significant difference was detected at 80–120 keV (p > 0.291). The score of the overall diagnostic evaluation was measured as 1.06 on CI and 3.12 on CIMAR. The score of the overall diagnostic evaluation was significantly higher on CIMAR and VMIMAR than on CI (p < 0.043). In the VMIMAR series, the score of overall diagnostic evaluation gradually progressed with the increased keV levels, higher than CIMAR at 70 and 80 keV (3.32 and 3.53 respectively, p ≤ 0.035), and then gradually decreased to the lowest at 120 keV (1.91) (Table 2, Fig. 3).

Comparisons of qualitative rating of vascular contour (a), the extent of artifact (b), and overall diagnostic evaluation (c) in CI, CIMAR, and VMIMAR of various keV levels (50 – 120 keV). a In all reconstructions, the scores of vascular contours gradually increase to the highest level of 3.63 at 70 keV and 3.56 at 80 keV and then decrease to 1.09 at 120 keV. b The score of the extent of the artifact is 1.06 in CI, 3.12 in CIMAR and increases to a maximum of 4.03 at 120 keV. And the score of the extent of the artifact at 80 keV is higher than CIMAR. c The scores of overall diagnostic evaluations gradually increase from the minimum (CI, 1.06) to 3.53 at 80 keV and then decrease to 1.91 in all reconstructions
Discussion
In this study, we enrolled a small sample of THA patients to explore better visualizing the periprosthetic vasculature and to investigate the optimal parameter for balancing metal artifact reduction and vascular visualization in dual-energy CT. We verified VMI combined with O-MAR using appropriate parameters can successfully both reduce metal artifacts and improve vascular visualization. Try our best, we have not retrieved the previously published study focused on the relationship between metal artifact reduction and periprosthetic vascular visualization in total joint replacement and CTA of the lower extremities patients.
Many investigations have demonstrated using O-MAR and VMI can significantly reduce metal artifacts, and the combination could be more effective [17, 18, 26, 28,29,30,31,32]. This was substantiated by the results of our study, which showed significant differences between VMIMAR and CI regarding the attenuation, the width of the hyperdense artifacts as well as the score of artifacts in the subjective analysis. These metrics displayed that the artifacts gradually decreased with increasing VMI settings, which was consistent with previous studies [28, 32]. Hyperdense artifacts were improved significantly as high keV levels primarily reduce beam hardening because of the physical characteristics of the virtual monoenergetic x-rays [26, 31, 33]. Our study further found the downtrend of attenuation of hyperdense artifacts was comparatively sharp at 50–70 keV and relatively flat at 80–120 keV. However, to better visualize the vasculature, low keV VMI was recommended as the preferred parameter for obtaining superior image quality by previous studies [13,14,15,16]. A reduction in mean photon energy results in a significant increase in the incidence of photoelectric interactions, particularly as these are increased at and near the k-edge of iodine (33 keV) contained in contrast media. In turn, these increased photoelectric interactions result in increased CT attenuation of vascular-iodinated contrast material [34]. So there seems to be some contradiction in the choice of parameters for the pursuit of minimum artifact and optimal vascular visualization according to current study results. In our study, we chose the highest keV level 120 keV instead of 200 keV, which was recommended as the optimal keV reported previously and not appropriate for this study. With increasing VMI settings, vascular attenuation measured from VMI gradually decreased due to away from the k-edge of iodine (33 keV) [13, 21, 34]. This observation was consistent with data from previous studies [13, 35]. Sufficient attenuation was known to be greater than 180 HU for the pulmonary artery and greater than 200 HU for the aorta [24, 36]. In this study, we defined to be greater than 200 HU as sufficient opacification for the periprosthetic external iliac and common femoral artery which was achieved on VMIMAR at 50–90 keV. Bae et al. reported that sufficient opacification (> 180 HU) was achieved at 40–70 keV for the pulmonary artery [35]. While our study needed to consider the influence of both vasculature and artifacts on image quality. The HU values decreased on the VMI of 80–120 keV in comparison to the conventional image. And the HU values of all structures are lower in high keV images when compared to low keV images and conventional images due to the high keV. However, as the CT value of low keV levels and conventional images increased, the image noise and width of artifacts also amplified which inevitably affected the evaluation of adjacent vessels around the prosthesis, and resulted in a worsening of total imaging quality. Although the artery showed higher attenuation on low keV, it would also result in vascular noise growth. The vascular noise on VMIMAR at 50–70 keV was even higher than that on CI in this study.
We found that following the attenuation and width of metal artifacts gradually decreased with increasing VMI settings, while the periprosthetic vascular attenuation worsened to below 200 HU. Similarly, the score of artifacts gradually improved as the increased keV level, while the score of overall vascular contour and diagnostic evaluation gradually increased at 50 – 80 keV and then decreased at 90–120 keV. This may be due to the impact of the artifact on the vessel being more obvious at low energy levels. Thus, we considered that 80 keV might be an acceptable energy level and equilibrium point to better visualize the periprosthetic artery and reduce metal artifacts (Fig. 4). In this level, the score of overall vascular contour and diagnostic evaluation increased to the top, and the score of artifacts showed most artifacts were removed (Fig. 5). Besides, the vascular attenuation was still over 200 HU and got a satisfied diagnostic confidence. In a study about stent evaluation in lower extremity DE-CTA, Mangold et al. reported 80 keV-VMI + improved image quality, stent visualization, and diagnostic confidence for stent evaluation [37]. In another study about peripheral artery stents, Zhang et al. demonstrated the optimal keV level for peripheral artery stents was concluded at 90 keV [38].

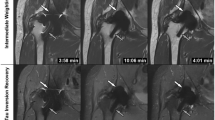
A series of axial enhanced CT images of a patient with THA. Images were reconstructed as CI, CIMAR, and VMIMAR at 50–120 keV with 10 intervals (window center 60 HU; window width 360 HU). Images show the metal artifact is gradually reducing with increasing energy level; however, the vascular visualization is worsening. The vascular visualization is terrible above 100 keV, while the vessel is disturbed by artifacts below 70 keV. The best performance is found at 80 keV

A series of post-processing CTA images of the same patient. 3D volume rendering (VR) (a), 3D VR without bone (b), maximum intensity projection (MIP) without bone (c), curved plannar reconstruction (CPR) (d, e), and slab MIP (f) images of the same patient on VMIMAR at 80 keV. Images show most artifacts are removed and the vessel is slightly affected with acceptable vascular attenuation and sharp vascular contour
The benefits of O-MAR technique in metal artifact reduction have been reported [17, 18, 39, 40]. In our study, CIMAR also provides relatively satisfactory both reduced metal artifacts and improved vascular visualization. Previous studies have found there were similar absolute attenuation and quality between the degree of enhancement and metal artifact reduction comparing 70-keV VMI to conventional 120-kVp CT [41, 42]. Compared with conventional polychromatic images, VMI has lower noise, higher contrast-to-noise ratio, and can reduce beam hardening artifacts and improve the accuracy of CT numbers [43, 44]. In this study, VMIMAR 80 keV was superior to CIMAR in terms of metal artifact reduction and vascular visualization, which was consistent with previous studies [43, 44].
This study has several limitations. First, the study population and number of THA are relatively small and our results should be confirmed in larger patient populations. Second, quantitative measurements and subjective assessment were all operated manually on the preselected axial images, and the vessels were probably disturbed by the metal artifact. This may confer a certain degree of measurement error. Third, the results only apply to the same CT scanner’s hardware and software configuration. It still needs to further verify if the recommended parameter in our study is also suitable for other devices.
In summary, our results demonstrate that VMI combined with O-MAR using appropriate parameters can provide both reduced metal artifacts and improved vascular visualization. 80 keV on VMIMAR can be an optimal energy level and equilibrium point to give both considerations and is recommended for routine use in the assessment of periprosthetic vasculature of THA patients and CTA of lower extremities in patients with THA.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CI:
-
Conventional image
- CIMAR :
-
Conventional image combined with orthopedic metal artifact reduction
- CTA:
-
Computed tomographic angiography
- DECT:
-
Dual-energy computed tomography
- HU:
-
Hounsfield Unit
- keV:
-
Kiloelectron volt
- O-MAR:
-
Orthopedic metal artifact reduction
- PAD:
-
Peripheral arterial disease
- ROI:
-
Region of interest
- THA:
-
Total hip arthroplasty
- VMI:
-
Virtual monoenergetic image
- VMIMAR :
-
Virtual monoenergetic image combined with orthopedic metal artifact reduction
References
Melvin JS, Karthikeyan T, Cope R, Fehring TK (2014) Early failures in total hip arthroplasty – a changing paradigm. J Arthroplasty 29:1285–1288
Singh JA (2011) Epidemiology of knee and hip arthroplasty: a systematic review. Open Orthop J 5:80–85
Tsantes AG, Papadopoulos DV, Lytras T et al (2019) Association of malnutrition with periprosthetic joint and surgical site infections after total joint arthroplasty: a systematic review and meta-analysis. J Hosp Infect 103:69–77
Street MWJ, Howard LC, Neufeld ME, Masri BA (2022) Vascular injuries during hip and knee replacement. Orthop Clin North Am 53:1–12
Regensteiner JG, Hiatt WR (2002) Current medical therapies for patients with peripheral arterial disease: a critical review. Am J Med 112:49–57
Lussana F, Squizzato A, Permunian ET, Cattaneo M (2014) A systematic review on the effect of aspirin in the prevention of post-operative arterial thrombosis in patients undergoing total hip and total knee arthroplasty. Thromb Res 134:599–603
Leung AG, Cabanela ME (1998) Aortic thrombosis after acetabular revision of a total hip arthroplasty. J Arthroplasty 13:961–965
Trousdale RT, Donnelly RS, Hallett JW (1999) Thrombosis of an aortobifemoral bypass graft after total hip arthroplasty. J Arthroplasty 14:386–390
Chou TY, Su TW, Jou HJ et al (2015) Increased risk of peripheral arterial disease after hip replacement: an 11-year retrospective population-based cohort study. Medicine (Baltimore) 94:e870
Mori I, Machida Y, Osanai M, Iinuma K (2013) Photon starvation artifacts of X-ray CT: their true cause and a solution. Radiol Phys Technol 6:130–141
Brooks RA, Di Chiro G (1976) Beam hardening in x-ray reconstructive tomography. Phys Med Biol 21:390–398
Wellenberg RHH, Hakvoort ET, Slump CH, Boomsma MF, Maas M, Streekstra GJ (2018) Metal artifact reduction techniques in musculoskeletal CT-imaging. Eur J Radiol 107:60–69
Leithner D, Mahmoudi S, Wichmann JL et al (2018) Evaluation of virtual monoenergetic imaging algorithms for dual-energy carotid and intracerebral CT angiography: effects on image quality, artefacts and diagnostic performance for the detection of stenosis. Eur J Radiol 99:111–117
Hamid S, Nasir MU, So A, Andrews G, Nicolaou S, Qamar SR (2021) Clinical applications of dual-energy CT. Korean J Radiol 22:970–982
Albrecht MH, Trommer J, Wichmann JL et al (2016) Comprehensive comparison of virtual monoenergetic and linearly blended reconstruction techniques in third-generation dual-source dual-energy computed tomography angiography of the thorax and abdomen. Invest Radiol 51:582–590
Albrecht MH, Scholtz JE, Husers K et al (2016) Advanced image-based virtual monoenergetic dual-energy CT angiography of the abdomen: optimization of kiloelectron volt settings to improve image contrast. Eur Radiol 26:1863–1870
Neuhaus V, Grosse Hokamp N, Zopfs D et al (2019) Reducing artifacts from total hip replacements in dual layer detector CT: combination of virtual monoenergetic images and orthopedic metal artifact reduction. Eur J Radiol 111:14–20
Park J, Kim SH, Han JK (2019) Combined application of virtual monoenergetic high keV images and the orthopedic metal artifact reduction algorithm (O-MAR): effect on image quality. Abdom Radiol (NY) 44:756–765
Bongers MN, Schabel C, Thomas C et al (2015) Comparison and combination of dual-energy- and iterative-based metal artefact reduction on hip prosthesis and dental implants. PLoS One 10:e0143584
Han SC, Chung YE, Lee YH, Park KK, Kim MJ, Kim KW (2014) Metal artifact reduction software used with abdominopelvic dual-energy CT of patients with metal hip prostheses: assessment of image quality and clinical feasibility. AJR Am J Roentgenol 203:788–795
Sudarski S, Apfaltrer P, Nance JW Jr et al (2013) Optimization of keV-settings in abdominal and lower extremity dual-source dual-energy CT angiography determined with virtual monoenergetic imaging. Eur J Radiol 82:e574–581
Goo HW, Goo JM (2017) Dual-energy CT: new horizon in medical imaging. Korean J Radiol 18:555–569
Yu L, Leng S, McCollough CH (2012) Dual-energy CT-based monochromatic imaging. AJR Am J Roentgenol 199:S9–S15
Delesalle MA, Pontana F, Duhamel A et al (2013) Spectral optimization of chest CT angiography with reduced iodine load: experience in 80 patients evaluated with dual-source, dual-energy CT. Radiology 267:256–266
Laukamp KR, Lennartz S, Neuhaus VF et al (2018) CT metal artifacts in patients with total hip replacements: for artifact reduction monoenergetic reconstructions and post-processing algorithms are both efficient but not similar. Eur Radiol 28:4524–4533
Neuhaus V, Grosse Hokamp N, Abdullayev N et al (2017) Metal artifact reduction by dual-layer computed tomography using virtual monoenergetic images. Eur J Radiol 93:143–148
Yin XP, Gao BL, Li CY et al (2018) Optimal monochromatic imaging of spectral computed tomography potentially improves the quality of hepatic vascular imaging. Korean J Radiol 19:578–584
Kosmas C, Hojjati M, Young PC, Abedi A, Gholamrezanezhad A, Rajiah P (2019) Dual-layer spectral computerized tomography for metal artifact reduction: small versus large orthopedic devices. Skeletal Radiol 48:1981–1990
Grosse Hokamp N, Neuhaus V, Abdullayev N et al (2018) Reduction of artifacts caused by orthopedic hardware in the spine in spectral detector CT examinations using virtual monoenergetic image reconstructions and metal-artifact-reduction algorithms. Skeletal Radiol 47:195–201
Hilgers G, Nuver T, Minken A (2014) The CT number accuracy of a novel commercial metal artifact reduction algorithm for large orthopedic implants. J Appl Clin Med Phys 15:4597
Lewis M, Reid K, Toms AP (2013) Reducing the effects of metal artefact using high keV monoenergetic reconstruction of dual energy CT (DECT) in hip replacements. Skeletal Radiol 42:275–282
Dangelmaier J, Schwaiger BJ, Gersing AS et al (2018) Dual layer computed tomography: reduction of metal artefacts from posterior spinal fusion using virtual monoenergetic imaging. Eur J Radiol 105:195–203
Lee YH, Park KK, Song HT, Kim S, Suh JS (2012) Metal artefact reduction in gemstone spectral imaging dual-energy CT with and without metal artefact reduction software. Eur Radiol 22:1331–1340
Vlahos I, Godoy MC, Naidich DP (2010) Dual-energy computed tomography imaging of the aorta. J Thorac Imaging 25:289–300
Bae K, Jeon KN, Cho SB et al (2018) Improved opacification of a suboptimally enhanced pulmonary artery in chest CT: experience using a dual-layer detector spectral CT. AJR Am J Roentgenol 210:734–741
Ozawa Y, Hara M, Shibamoto Y (2011) The frequency of insufficient contrast enhancement of the pulmonary artery in routine contrast-enhanced chest CT and its improvement with an increased injection rate: a prospective study. J Thorac Imaging 26:42–47
Mangold S, De Cecco CN, Schoepf UJ et al (2016) A noise-optimized virtual monochromatic reconstruction algorithm improves stent visualization and diagnostic accuracy for detection of in-stent re-stenosis in lower extremity run-off CT angiography. Eur Radiol 26:4380–4389
Zhang D, Xie Y, Wang Y et al (2020) Initial clinical experience of virtual monoenergetic imaging improves stent visualization in lower extremity run-off CT angiography by dual-layer spectral detector CT. Acad Radiol 27:825–832
Selles M, Stuivenberg VH, Wellenberg RHH et al (2021) Quantitative analysis of metal artifact reduction in total hip arthroplasty using virtual monochromatic imaging and orthopedic metal artifact reduction, a phantom study. Insights Imaging 12:171
Wellenberg RH, Boomsma MF, van Osch JA et al (2017) Low-dose CT imaging of a total hip arthroplasty phantom using model-based iterative reconstruction and orthopedic metal artifact reduction. Skeletal Radiol 46:623–632
Krishna S, Sadoughi N, McInnes MDF, Chatelain R, MacDonald DB, Schieda N (2018) Attenuation and degree of enhancement with conventional 120-kVp polychromatic CT and 70-keV monochromatic rapid kilovoltage-switching dual-energy CT in cystic and solid renal masses. AJR Am J Roentgenol 211:789–796
Wellenberg RH, Boomsma MF, van Osch JA et al (2017) Quantifying metal artefact reduction using virtual monochromatic dual-layer detector spectral CT imaging in unilateral and bilateral total hip prostheses. Eur J Radiol 88:61–70
Yu L, Christner JA, Leng S, Wang J, Fletcher JG, McCollough CH (2011) Virtual monochromatic imaging in dual-source dual-energy CT: radiation dose and image quality. Med Phys 38:6371–6379
Pessis E, Campagna R, Sverzut JM et al (2013) Virtual monochromatic spectral imaging with fast kilovoltage switching: reduction of metal artifacts at CT. Radiographics 33:573–583
Acknowledgements
We recognize the contribution of Xiaomei Lu, an employee of Philips Healthcare, for her advice.
Funding
None.
Author information
Authors and Affiliations
Contributions
Conceptualization: Haitao Yang. Data curation: Jie Zhao, Qiqi Wang. Formal analysis: Jie Zhao. Investigation: Ziyi Tang, Yuxi Luo. Methodology: Yuchan Lv, Jie Zhao. Project administration: Haitao Yang. Resources: Qiang Cheng, Chuan Liu. Supervision: Haitao Yang. Validation: Jie Zhao, Haitao Yang. Visualization: Jie Zhao. Writing-original draft: Jie Zhao. Writing-review and editing: Haitao Yang.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University, and individual consent for this retrospective analysis was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhao, J., Cheng, Q., Liu, C. et al. Optimal combination periprosthetic vasculature visualization and metal artifact reduction by spectral computed tomography using virtual monoenergetic images in total hip arthroplasty. Insights Imaging 14, 181 (2023). https://doi.org/10.1186/s13244-023-01533-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-023-01533-3