
Abstract
Background
This study provides a quantitative meta-analysis of pancreatic CT perfusion studies, investigating choice of study parameters, ability for quantitative discrimination of pancreatic diseases, and influence of acquisition and reconstruction parameters on reported results.
Methods
Based on a PubMed search with key terms ‘pancreas’ or ‘pancreatic,’ ‘dynamic’ or ‘perfusion,’ and ‘computed tomography’ or ‘CT,’ 491 articles published between 1982 and 2020 were screened for inclusion in the study. Inclusion criteria were: reported original data, human subjects, five or more datasets, measurements of pancreas or pancreatic pathologies, and reported quantitative perfusion parameters. Study parameters and reported quantitative measurements were extracted, and heterogeneity of study parameters and trends over time are analyzed. Pooled data were tested with weighted ANOVA and ANCOVA models for differences in perfusion results between normal pancreas, pancreatitis, PDAC (pancreatic ductal adenocarcinoma), and non-PDAC (e.g., neuroendocrine tumors, insulinomas) and based on study parameters.
Results
Reported acquisition parameters were heterogeneous, except for contrast agent amount and injection rate. Tube potential and slice thickness decreased, whereas tube current time product and scan coverage increased over time. Blood flow and blood volume showed significant differences between pathologies (both p < 0.001), unlike permeability (p = 0.11). Study parameters showed a significant effect on reported quantitative measurements (p < 0.05).
Conclusions
Significant differences in perfusion measurements between pathologies could be shown for pooled data despite observed heterogeneity in study parameters. Statistical analysis indicates most influential parameters for future optimization and standardization of acquisition protocols.
Critical relevance statement
Quantitative CT perfusion enables differentiation of pancreatic pathologies despite the heterogeneity of study parameters in current clinical practice.
Graphical abstract

Key points
-
1.
Quantitative meta-analysis validates CT perfusion measurements for diagnosis of different pancreatic diseases.
-
2.
The contrast administration protocol shows a significant effect on reported blood flow.
-
3.
Study parameters are very heterogeneous between studies, showing a need for standardization
Similar content being viewed by others

Background
Dynamic CT perfusion is a functional imaging technique that enables measurement of physiological parameters of blood flow for the assessment of diseases that influence tissue perfusion. Early applications of CT perfusion focused on the brain [1], but some early studies also performed dynamic contrast-enhanced CT acquisitions of the pancreas without calculating quantitative parameters [2, 3]. Since then, new mathematical models of CT perfusion have been developed [4, 5] and applied to the pancreas [6, 7]. Studies have shown that quantitative measurements of physiological perfusion parameters by means of CT perfusion can aid in the detection of pancreatic ductal adenocarcinoma (PDAC) [8], even in difficult cases that appear isodense to the surrounding tissue on conventional CT images [9,10,11], and allow therapy response assessment for treatment of PDAC [12]. Furthermore, CT perfusion can be used to assess the severity of pancreatitis [13] as well as for the distinction of pancreatic diseases [14], i.e., to improve the difficult differentiation between mass-forming pancreatitis and PDAC [10, 15].
In view of the current role of imaging modalities in the workup of these pancreatic diseases, the German S3 guideline recommends preoperative liver magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI) in every patient with potentially resectable PDAC [16] for the reason of MRI being superior for the detection and characterization of liver lesions that are undetectable or indeterminate on CT [17, 18]. In 2017 in turn, a systematic review and meta-analysis rated transabdominal ultrasound (US) equivalent to CT and MRI for the diagnosis of PDAC [19]. Its diagnostic reliability, however, can be limited by overlying bowel gas and patient body habitus [19]. Furthermore, while the addition of positron emission tomography (PET)/CT is currently not routinely recommended in PDAC patients [18], it may be considered in patients who are at high risk for the presence of distant metastases [17]. PET/ CT with 68Ga-labeled somatostatin analogs has a high sensitivity and specificity for tumor manifestations of non-insulinoma pancreatic neuroendocrine tumors (NETs) and is therefore recommended by the European Neuroendocrine Tumor Society (ENETS) Consensus Guidelines to fully stage the extent of disease in these patients [20].
While CT perfusion is not explicitly mentioned in the most widely used pancreatic tumor guidelines, both the National Comprehensive Cancer Network (NCCN) and American Society of Clinical Oncology (ASCO) Clinical Practice Guidelines consider contrast-enhanced CT as the preferred imaging modality for assessment of extent of disease in PDAC [17, 21]. According to the European Society for Medical Oncology (ESMO) Clinical Practice Guidelines, CT also is the basic radiological method for imaging of pancreatic NETs [22]. This allows for a convenient extension of the pancreatic CT protocol with CT perfusion imaging in difficult cases, e.g., tumors that are obscure on standard CT imaging.
A number of studies have been performed to find optimum study parameters for CT perfusion measurements, but have also shown changes in the quantitative results of CT perfusion measurements based on CT examination parameters and evaluation procedures, e.g., depending on the temporal sampling rate [23, 24], the image noise [25], the motion correction [26, 27], the mathematical perfusion model [28] and even the employed version of the post-processing software [29]. That is, based on the acquisition parameters and evaluation settings, different quantitative results can be expected for the same measurement, which limits the comparability of measurements between studies and in clinical practice. Thus, a standardization of acquisition protocols and evaluation procedures is necessary to achieve reliable and clinically meaningful measurements. This need has also been recognized by the Experimental Cancer Medicine Centre Imaging Network Group which published their guidelines for the assessment of tumor vascular support with dynamic contrast-enhanced computed tomography in 2012 [30].
This study aims to provide a comprehensive overview of the study parameters and evaluation procedures used in clinical CT perfusion studies of the pancreas by means of a quantitative meta-analysis. Furthermore, statistical analysis is performed to confirm the individual study results on the potential applications of perfusion CT as well as to identify the acquisition parameters with the strongest influence on quantitative results for further investigation and standardization.
Methods
Search strategy
We explored the PubMed library, searching the database for published studies with the key terms ‘pancreas’ or ‘pancreatic,’ ‘dynamic’ or ‘perfusion,’ and ‘computed tomography’ or ‘CT’. All CT perfusion research studies published and indexed before July 3, 2020, were collected. A total of 491 research articles published from 1982 to 2020 were obtained from the search. In a first step, these research articles were scanned manually based on their titles and abstracts for inclusion/exclusion. In a second step, all suitable studies were then read and assessed by two authors independently (N.V. and S.S.). Disagreements regarding study inclusion/exclusion were resolved by consensus-based discussions in two cases.
Inclusion and exclusion criteria
We included studies that (1) reported original data, (2) included original human data, (3) included at least five or more datasets, (4) included measurements of the pancreas or pancreatic pathologies, and (5) reported quantitative perfusion parameters from perfusion CT. All study designs (prospective and retrospective) were included. Studies that had a cohort overlapping with previously published studies were not considered original data and excluded. Articles reporting different perfusion measurements for the same patient collective were counted as one study, since patient data were acquired only once [14, 31, 32]. Reviews, animal studies, or case reports (less than five patients) were excluded. To distinguish perfusion CT from conventional contrast-enhanced CT studies, only studies that reported quantitative perfusion parameters were included.
Data extraction
Data were extracted from all the included research studies by two authors independently (N.V. and S.S.). Disagreements regarding data extraction were resolved by consensus-based discussions in five cases. Data extracted included study parameters and reported mean values of quantitative perfusion parameters (blood flow (BF), blood volume (BV), and permeability). Here, study parameters include (1) sample size, (2) CT examination parameters: acquisition parameters (tube potential, tube current–time product, anatomical coverage, total acquisition time, lowest temporal sampling, highest temporal sampling, and use of variable temporal sampling), reconstruction parameters (slice thickness), contrast agent information (amount of contrast agent, iodine concentration, total amount of iodine, injection rate, and use of saline flush), dose information (effective dose), and (3) post-processing information (perfusion model and type of post-processing software). Many studies used variable temporal sampling rates, e.g., a sampling rate of one acquisition per second for the first 30 s followed by one acquisition every 5 s for the next 60 s. Therefore, the lowest temporal sampling rate and highest temporal sampling rate used in each study were considered separately for analysis. All reported quantitative measurements from the studies were then grouped into four categories based on the clinical entities reported by the study: (1) normal pancreas, (2) pancreatitis, (3) PDAC, and (4) non-PDAC. Here, the category “normal pancreas” includes both patients without pancreatic pathology and measurements in non-pathologic tissue. The non-PDAC group includes all pathologies other than pancreatitis and PDAC, i.e., insulinoma or endocrine tumors, etc., which were grouped despite their physiological differences because of the low number of studies.
Statistical analysis
Statistical analysis was performed using Microsoft Excel 2016 and SAS software (version 9.2, SAS Institute, Cary, N.C., USA). For all study parameters, histogram distribution plots were computed for qualitative analysis of parameter distributions, and medians and interquartile ranges were calculated. Year-wise means of number of studies, sample size and CT examination parameters were calculated and linear regression plots were computed using these mean values to analyze the trend of study parameters over the years. Mean values and standard deviations of reported perfusion values were calculated for each pathology. Weighted analysis of variances (W-ANOVA) followed by Student’s t test was performed for comparing reported perfusion values of different pancreatic pathologies to each other while weighting the measurements by the number of patients. Outliers have been removed from reported perfusion values based on a range of mean ± 1.96 * standard deviations of the parameter values, as some studies reported very high measurement values. W-ANCOVA was performed to test the effect of the individual CT examination parameters on reported perfusion values, simultaneously considering the effect of the clinical entities.
Qualitative box-plot analysis was performed for those CT acquisition parameters which showed a statistically significant effect on the quantitative measurements with respect to the pancreatic pathologies. To this end, quantitative measurements were separated into two groups based upon CT acquisition parameters (i.e., for each acquisition parameter a low-value and a high-value group), where the threshold value between the two groups was determined using K-means clustering algorithm, visualizing differences in quantitative measurements based on acquisition settings.
Total acquisition time and effective dose were compared between studies using single temporal sampling and studies using variable temporal sampling by Student’s t test.
Results
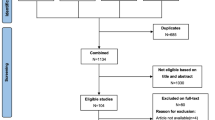
In total, 491 published research articles were collected for the current study. After manual screening of the title and abstracts, 117 articles were selected for full-text screening. Out of these, 39 articles reporting 37 studies were finally included in the current study based on the inclusion criteria [6, 7, 9, 10, 12,13,14, 28, 31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60]. A flowchart illustrating the selection of the studies is shown in Fig. 1. A summary of the information on the number of studies reporting each quantitative perfusion parameter (blood flow, blood volume, and permeability) for the respective clinical entity is shown in Table 1.

Flowchart illustrating the study design and the inclusion process
Figure 2a–l shows the histogram distribution of the study parameters in the included studies. For most of the parameters, a wide range of values have been reported over the years such as the number of patients with a median (interquartile range) of 36.0 (23.0–57.0), effective dose with a median of 8.8 (4.9–11.6) mSv, and CT acquisition parameters (anatomical coverage: 69.0 (29.4–105.0) mm, tube potential: 95.0 (80.0–100.0) kVp, tube current–time product: 100.0 (100.0–150.0) mAs and total acquisition time: 51.0 (40.0–79.5) s). By comparison, the contrast agent parameters show a considerable homogeneity and less variance around the median of 50.0 (40.0–50.0) mL of contrast agent, 17.5 (15.2–18.5) g of iodine, and 5.0 (5.0–5.0) mL/s of injection rate. The median of the lowest and highest temporal sampling rate was 1.5 (1.0–2.0) s and 2.0 (1.3–7.3) s, respectively, and median slice thickness was 5.0 (3.0–5.8) mm. Regarding the type of post-processing software, most of the research studies preferred to use vendor software as compared to third-party or in-house software. The most commonly used perfusion model for quantification of pancreatic perfusion parameters was the maximum slope model, followed by the deconvolution model.

Histogram distribution of: a sample size (number of patients), b–l CT examination parameters, and (m) the software and (n) perfusion model used for calculating the perfusion measurements, respectively. Please note that values higher than the highest histogram bin were put into the highest histogram bin. The total count of studies in histogram (n) is greater than the total number of studies as some of the reported studies have used more than one perfusion model for the analysis (i.e., maximum slope model and Patlak analysis)
Linear regression plots of the mean values of number of studies, sample size and CT examination parameters over the years are shown in Fig. 3, visualizing changes in parameters over time. The number of studies as well as the number of patients per study have been increasing after 2010. The amount of contrast agent used and hence the amount of iodine also shows an increasing trend. There was no notable trend for injection rate. Mean tube potential and tube current–time product have slightly decreasing and increasing trends, respectively. The total time taken for the acquisition and the effective dose do not show any notable trend over the years, while the anatomical coverage shows an increasing trend. The slice thickness also decreased over the years with mean minimum value reported as 2.5 mm. The lowest temporal sampling shows a notable decrease over the years, i.e., shorter intervals between individual acquisitions, whereas the highest temporal sampling rate only shows a slight decrease.

Linear regression plots of the means of (a) number of studies, (b) sample size (number of patients), and (c–l) all the CT examination parameters computed over the years. Please note that the plot for injection rate was omitted, as there was no observable trend of the mean injection rate
Mean ± SD (standard deviation) of the quantitative parameters (blood flow, blood volume, and permeability) have been calculated for the respective clinical entities, and the results are shown in Table 2. The lowest averaged values for all parameters were observed in the PDAC group as compared to pancreatitis, normal pancreas and non-PDAC. While mean blood flow was highest in non-PDAC, mean blood volume and permeability were highest in normal pancreas. Figure 4 also shows similar results with the box-plot representations of the reported quantitative parameters (blood flow, blood volume, and permeability) within different pancreatic pathologies. The W-ANOVA Tukey groupings for comparing the means of quantitative measurements (blood flow and blood volume) between different pancreatic pathologies are shown in Fig. 5. The W-ANOVA results show that blood flow (p < 0.001) and blood volume (p < 0.001) differ significantly between pancreatic pathologies and normal pancreas but permeability does not (p = 0.11). Student’s t test following W-ANOVA shows significant differences between normal pancreas/pancreatitis, normal pancreas/PDAC, and PDAC/non-PDAC based on the perfusion parameters blood flow and blood volume, and between pancreatitis/PDAC, and pancreatitis/non-PDAC for blood flow only (all p < 0.05, respectively).

Boxplots for comparing the reported results of quantitative measurements of blood flow, blood volume, and permeability within the different pancreatic pathologies. PDAC = pancreatic ductal adenocarcinoma

W-ANOVA Tukey grouping for comparing the weighted means of quantitative measurements (blood flow [mL/100 mL/min] and blood volume [mL/100 mL]) between the different pancreatic pathologies. Please note that no groupings are shown for permeability, as the W-ANOVA model was not significant for permeability (p = 0.11). PDAC = pancreatic ductal adenocarcinoma
Table 3 shows how many of the studies reported statistically significant differences for the comparison of different pancreatic pathologies based on quantitative perfusion measurements compared to the total number of studies reporting results of statistical analysis for each parameter and for each comparison. Similar to the total number of studies shown in Table 1, most of the studies focused on PDAC, followed by pancreatitis, with only a limited number of results available for non-PDAC. With two exceptions, all the studies reporting blood flow and blood volume showed significant differences in their results. For studies analyzing permeability, only 50% have reported significant differences between the investigated clinical entities.
The effects of the CT examination parameters and perfusion model on the quantitative measurements are summarized in Table 4. The amount of contrast agent, injection rate, and use of saline flush show a significant effect on reported blood flow. Tube current–time product, highest temporal sampling, and use of variable temporal sampling, have a significant effect on reported blood volume. None of the evaluated parameters show a significant effect on reported permeability.
Figure 6 shows examples of box plots comparing the effect of CT examination parameters (which were reported as significant, cf. Table 4) on the quantitative measurements (blood flow and blood volume) within different pancreatic pathologies. These plots illustrate how the acquisition parameters influence the results, e.g., that higher values of blood flow were found in normal pancreas when no saline flush was used (mean blood flow 127.69 ± 37.21 mL/100 mL/min vs. 90.35 ± 20.97 mL/100 mL/min). Similarly, higher values of blood volume were found when using variable temporal sampling rates (mean blood volume 22.81 ± 5.68 mL/100 mL vs. 17.40 ± 4.37 mL/100 mL).

Boxplots comparing the effect of acquisition parameters on the quantitative measurements (blood flow and blood volume) within different pancreatic pathologies: a, b show the binary effect of saline flush and temporal sampling on the blood flow and blood volume, respectively; c shows the effect of highest temporal sampling on blood volume. Please note the differences in sample sizes between the groups (cf. Tab. 1). PDAC = pancreatic ductal adenocarcinoma
The difference in total acquisition time between studies with single temporal sampling rates and studies with variable temporal sampling rates was statistically significant (p = 0.03). Longer acquisition times were found for studies with variable temporal sampling rates. However, the difference in effective dose between studies with single temporal sampling rates and studies with variable temporal sampling rates was not statistically significant (p = 0.19).
Discussion
The aim of this study was to perform a quantitative meta-analysis of pancreatic CT perfusion studies with regard to study parameters, the possibility to discriminate pancreatic diseases quantitatively based on perfusion measurements, and to investigate the connection between study parameters and quantitative measurements.
The results show significant differences of measured blood flow and blood volume between different pathologies as well as healthy tissue, validating the use of CT perfusion as a quantitative imaging biomarker despite the extremely heterogeneous nature of the dataset. This is in agreement with individual results of the evaluated studies, which reported significant differences in perfusion parameters when comparing different pathologies or pathologies to non-pathological tissue (cf. Table 3). However, further research is necessary regarding the value of measurements of permeability based on the results reported individually in the evaluated studies and this quantitative meta-analysis. Furthermore, significant differences between non-PDAC and normal pancreas reported in studies could not be reproduced by this quantitative meta-analysis [14, 39]. This can be explained by the heterogeneous definition of “non-PDAC” in this meta-analysis, which includes insulinomas and endocrine tumors, to compensate for the small number of available studies. Additionally, histopathological studies show an increased microvessel density (MVD) for PDAC over normal pancreas [61], while CT perfusion shows a decreased blood flow (cf. Fig. 4). One theory is that the increased fluid pressure in the tumor stroma leads to reduced blood flow through the compressed vessels despite high MVD [62], but further research is necessary.
Being a meta-analysis, the evaluation in the current study focused on differences between pathologies, which limits clinical applicability of the results. For example, the results show significant differences in blood flow between PDAC and pancreatitis. However, we did not perform sub-group analysis on mass-forming chronic pancreatitis, which can be difficult to distinguish from PDAC. This kind of specific clinical application falls outside of the scope of this meta-analysis, but individual studies show promising results for CT perfusion in this regard [50].
Study parameters in evaluated studies were very heterogeneous and changed over time, which highlights the need for standardization, if comparability between CT perfusion measurements performed at different institutions is to be achieved. This need for standardization is further highlighted by the statistical analysis showing a significant effect of multiple acquisition parameters on reported quantitative results. Furthermore, this analysis indicates which parameters might be most important for standardization, while the box-plot analysis provides a qualitative investigation of effect sizes. However, when interpreting these results, different sample sizes for parameters and pathologies have to be considered (cf. Table 1). Many studies did not fully comply with the reporting guidelines proposed by the Experimental Cancer Medicine Centre Imaging Network Group in 2012 [30], reporting only some acquisition parameters, further limiting sample sizes. In consequence, results regarding blood flow and normal pancreas should be considered most reliable when interpreting Table 3 and Fig. 6. While the current dataset does not allow to recommend specific acquisition settings, results are generally in line with previous studies, which agree on the importance of these acquisition parameters, e.g., temporal sampling rate [23], contrast agent injection protocols [36], and image noise [25]. The results also underline the value of variable temporal sampling, which can be used to reduce the sampling rate after the first-pass of the contrast agent, allowing for longer acquisition times without increasing radiation exposure. However, previous results on the influence of the perfusion model on quantitative measurements could not be reproduced [28]. This might be explained by the fact that many studies did not report the perfusion model and the wide range of models used (cf. Fig. 2).
The main limitation of this meta-analysis is the limited number of included studies, which is based on the number of available studies on the topic of pancreatic CT perfusion. Considering that not all of the evaluated parameters are reported in every study, the sample size is even more limited for some of the evaluations in the current study. The sample size was also even more limited for some of the investigated pathologies, which resulted in the pooling of all tumor entities that are not adenocarcinoma in a heterogeneous “non-PDAC” group. Similarly, some studies reported measurements for normal pancreatic tissue and pathological tissue from the same patients, but an effect of the investigated diseases on the normal tissue cannot be precluded, so a further distinction between patients with and without pancreatic disease might be necessary [61]. Based on the small sample size, multivariate statistical analysis was not possible, and only the detection and distinction of tumors/PDAC and pancreatitis was statistically validated in this study. Evaluating studies performed for a different organ, e.g., the brain, where a larger number of studies is available might yield further insights, but physiological differences between the organs and body regions have to be considered when interpreting and comparing results. In turn, results from this study cannot be directly transferred to perfusion studies of other organs and body regions. Furthermore, studies from a time frame of more than 25 years were included in this study. While CT technology advanced considerably during this time, reported perfusion values remain compatible with each other, and the statistical analysis reported no significant effect for many parameters indicative of technological progress, like anatomical coverage. Similarly, all study parameters from individual studies were included in the analysis as reported to avoid any bias toward certain sets of parameters. Finally, while this study highlights the study parameters with a significant influence on reported quantitative results, prospective studies are needed to determine optimum settings for those parameters.
In view of use in clinical practice, CT perfusion as well as MRI can be helpful for tumor detection when a suspected pancreatic tumor is not visible on routine pancreatic CT imaging [17]. Two small studies directly compared CT perfusion and diffusion-weighted (DW) MRI in PDAC patients and reported CT perfusion and (DW)-MRI parameters to be comparably applicable for differentiation of PDAC lesions and non-neoplastic pancreatic tissue [54, 63]. In addition, the performance of both PET/CT and CT perfusion was reported to exceed the performance of standard CT for insulinoma detection [64, 65]. However, studies which directly compare these imaging modalities are lacking.
Furthermore, a major limitation of standard pancreatic CT is its inability to reliably assess the response of PDAC lesions to (radio-)chemotherapy (RCT) since it cannot differentiate post-treatment fibroinflammatory changes from residual viable tumor tissue [66]. Here, DW-MRI and perfusion CT have both shown potential for prediction of histopathological response after RCT [60, 66], although no study compared these imaging modalities in this regard.
Conclusions
In conclusion, this study shows the value of pancreatic CT perfusion in the differentiation of pancreatic diseases, as results from individual studies could be reproduced in the pooled dataset despite the heterogeneity in CT protocols between studies. Furthermore, the need for standardization of CT perfusion protocols is highlighted, as a significant influence of study parameters on reported quantitative results was observed.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- ASCO:
-
American society of clinical oncology
- BF:
-
Blood flow
- BV:
-
Blood volume
- CT:
-
Computed tomography
- DWI:
-
Diffusion-weighted imaging
- ENETS:
-
European neuroendocrine tumor society
- ESMO:
-
European society for medical oncology
- MRI:
-
Magnetic resonance imaging
- MVD:
-
Microvessel density
- NCCN:
-
National comprehensive cancer network
- NET:
-
Neuroendocrine tumor
- PDAC:
-
Pancreatic ductal adenocarcinoma
- PET:
-
Positron emission tomography
- RCT:
-
(Radio-)chemotherapy
- SD:
-
Standard deviation
- US:
-
Ultrasound
- W-ANCOVA:
-
Weighted analysis of covariances
- W-ANOVA:
-
Weighted analysis of variances
References
Axel L (1980) Cerebral blood flow determination by rapid-sequence computed tomography: theoretical analysis. Radiology 137:679–686. https://doi.org/10.1148/radiology.137.3.7003648
Hosoki T (1983) Dynamic CT of pancreatic tumors. AJR Am J Roentgenol 140:959–965. https://doi.org/10.2214/ajr.140.5.959
Nuutinen P, Kivisaari L, Schröder T (1988) Contrast-enhanced computed tomography and microangiography of the pancreas in acute human hemorrhagic/necrotizing pancreatitis. Pancreas 3:53–60. https://doi.org/10.1097/00006676-198802000-00010
Mazzei FG, Volterrani L, Guerrini S et al (2014) Reduced time CT perfusion acquisitions are sufficient to measure the permeability surface area product with a deconvolution method. Biomed Res Int 2014:1–6. https://doi.org/10.1155/2014/573268
Miles KA (1991) Measurement of tissue perfusion by dynamic computed tomography. Br J Radiol 64:409–412. https://doi.org/10.1259/0007-1285-64-761-409
Miles K, Hayball M, Dixon A (1995) Measurement of human pancreatic perfusion using dynamic computed tomography with perfusion imaging. Br J Radiol 68:471–475. https://doi.org/10.1259/0007-1285-68-809-471
Tsuji Y, Yamamoto H, Yazumi S et al (2007) Perfusion computerized tomography can predict pancreatic necrosis in early stages of severe acute pancreatitis. Clin Gastroenterol H 5:1484–1492. https://doi.org/10.1016/j.cgh.2007.07.014
Xu J, Liang Z, Hao S et al (2009) Pancreatic adenocarcinoma: dynamic 64-slice helical CT with perfusion imaging. Abdom Imaging 34:759–766. https://doi.org/10.1007/s00261-009-9564-1
Klauß M, Stiller W, Fritz F et al (2012) Computed tomography perfusion analysis of pancreatic carcinoma. J Comput Assist Tomogr 36:237–242. https://doi.org/10.1097/rct.0b013e31824a099e
Aslan S, Nural MS, Camlidag I, Danaci M (2019) Efficacy of perfusion CT in differentiating of pancreatic ductal adenocarcinoma from mass-forming chronic pancreatitis and characterization of isoattenuating pancreatic lesions. Abdom Radiol (NY) 44:593–603. https://doi.org/10.1007/s00261-018-1776-9
Yoon SH, Lee JM, Cho JY et al (2011) Small (≤ 20 mm) pancreatic adenocarcinomas: analysis of enhancement patterns and secondary signs with multiphasic multidetector CT. Radiology 259:442–452. https://doi.org/10.1148/radiol.11101133
D’Assignies G, Couvelard A, Bahrami S et al (2009) Pancreatic endocrine tumors: tumor blood flow assessed with perfusion CT reflects angiogenesis and correlates with prognostic factors. Radiology 250:407–416. https://doi.org/10.1148/radiol.2501080291
Piekowska J, Gwodziewicz K, Skrobisz-Balandowska K et al (2016) Perfusion-CT-can we predict acute pancreatitis outcome within the first 24 hours from the onset of symptoms? PLoS One 11:e0146965. https://doi.org/10.1371/journal.pone.0146965
Delrue L, Blanckaert P, Mertens D et al (2012) Tissue perfusion in pathologies of the pancreas: assessment using 128-slice computed tomography. Abdom Imaging 37:595–601. https://doi.org/10.1007/s00261-011-9783-0
Schima W, Böhm G, Rösch CS et al (2020) Mass-forming pancreatitis versus pancreatic ductal adenocarcinoma: CT and MR imaging for differentiation. Cancer Imaging 20:52. https://doi.org/10.1186/s40644-020-00324-z
German Cancer Society (DKG), German Cancer Aid (DKH), Working Group of the Scientific Medical Societies (AWMF) (2021) [S3-Guideline Exocrine Pancreatic Cancer]. AWMF Register-No.: 032-010OL. https://www.leitlinienprogramm-onkologie.de/leitlinien/pankreaskarzinom. Accessed 13 May 2023.
National Comprehensive Cancer Network (NCCN) (2023) Pancreatic Adenocarcinoma, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf. Accessed 13 May 2023.
Ducreux M, Cuhna AS, Caramella C, et al (ESMO Guidelines Committee) (2015) Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 26:v56–v68. https://doi.org/10.1093/annonc/mdv295
Toft J, Hadden WJ, Laurence JM et al (2017) Imaging modalities in the diagnosis of pancreatic adenocarcinoma: a systematic review and meta-analysis of sensitivity, specificity and diagnostic accuracy. Eur J Radiol 92:17–23. https://doi.org/10.1016/j.ejrad.2017.04.009
Falconi M, Eriksson B, Kaltsas G, et al (Vienna Consensus Conference participants) (2016) ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology 103:153–171. https://doi.org/10.1159/000443171
Balaban EP, Mangu PB, Khorana AA et al (2016) Locally advanced, unresectable pancreatic cancer: american society of clinical oncology clinical practice guideline. J Clin Oncol 34:2654–2668. https://doi.org/10.1200/JCO.2016.67.5561
Pavel M, Öberg K, Falconi M, et al (ESMO Guidelines Committee) (2020) Gastroenteropancreatic neuroendocrine neoplasms: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 31:844–860. https://doi.org/10.1016/j.annonc.2020.03.304
Wintermark M, Smith WS, Ko NU et al (2004) Dynamic perfusion CT: optimizing the temporal resolution and contrast volume for calculation of perfusion CT parameters in stroke patients. AJNR Am J Neuroradiol 25:720–729
Klotz E, Haberland U, Glatting G et al (2015) Technical prerequisites and imaging protocols for CT perfusion imaging in oncology. Eur J Radiol 84:2359–2367. https://doi.org/10.1016/j.ejrad.2015.06.010
Skornitzke S, Hirsch J, Kauczor HU, Stiller W (2019) Evaluation of the effect of image noise on CT perfusion measurements using digital perfusion phantoms. Eur Radiol 29:2089–2097. https://doi.org/10.1007/s00330-018-5709-3
Skornitzke S, Fritz F, Klauss M et al (2015) Qualitative and quantitative evaluation of rigid and deformable motion correction algorithms using dual-energy CT images in view of application to CT perfusion measurements in abdominal organs affected by breathing motion. Br J Radiol 88:20140683. https://doi.org/10.1259/bjr.20140683
Chu LL, Knebel RJ, Shay AD et al (2018) CT perfusion imaging of lung cancer: benefit of motion correction for blood flow estimates. Eur Radiol 28:5069–5075. https://doi.org/10.1007/s00330-018-5492-1
Schneeweiß S, Horger M, Grözinger A et al (2016) CT-perfusion measurements in pancreatic carcinoma with different kinetic models: is there a chance for tumour grading based on functional parameters? Cancer Imaging 16:1–8. https://doi.org/10.1186/s40644-016-0100-6
Goh V, Shastry M, Engledow A et al (2011) Commercial software upgrades may significantly alter perfusion CT parameter values in colorectal cancer. Eur Radiol 21:744–749. https://doi.org/10.1007/s00330-010-1967-4
Miles KA, Lee TY, Goh V et al (2012) Current status and guidelines for the assessment of tumour vascular support with dynamic contrast-enhanced computed tomography. Eur Radiol 22:1430–1441. https://doi.org/10.1007/s00330-012-2379-4
Delrue L, Blanckaert P, Mertens D et al (2011) Assessment of tumor vascularization in pancreatic adenocarcinoma using 128-slice perfusion computed tomography imaging. J Comput Assist Tomogr 35:434–438. https://doi.org/10.1097/rct.0b013e318223f0c5
Delrue L, Blanckaert P, Mertens D et al (2011) Variability of CT contrast enhancement in the pancreas: a cause for concern? Pancreatology 11:588–594. https://doi.org/10.1159/000334547
Kanda T, Yoshikawa T, Ohno Y et al (2012) Perfusion measurement of the whole upper abdomen of patients with and without liver diseases: initial experience with 320-detector row CT. Eur J Radiol 81:2470–2475. https://doi.org/10.1016/j.ejrad.2011.10.009
Li H, Sun C, Xu Z et al (2014) Low-dose whole organ CT perfusion of the pancreas: preliminary study. Abdom Imaging 39:40–47. https://doi.org/10.1007/s00261-013-0045-1
Motosugi U, Ichikawa T, Sou H et al (2012) Multi-organ perfusion CT in the abdomen using a 320-detector row CT scanner: preliminary results of perfusion changes in the liver, spleen, and pancreas of cirrhotic patients. Eur J Radiol 81:2533–2537. https://doi.org/10.1016/j.ejrad.2011.11.054
Kandel S, Kloeters C, Meyer H et al (2009) Whole-organ perfusion of the pancreas using dynamic volume CT in patients with primary pancreas carcinoma: acquisition technique, post-processing and initial results. Eur Radiol 19:2641–2646. https://doi.org/10.1007/s00330-009-1453-z
Stiller W, Skornitzke S, Fritz F et al (2015) Correlation of quantitative dual-energy computed tomography iodine maps and abdominal computed tomography perfusion measurements: are single-acquisition dual-energy computed tomography iodine maps more than a reduced-dose surrogate of conventional computed tomography perfusion? Invest Radiol 50:703–708. https://doi.org/10.1097/rli.0000000000000176
Skornitzke S, Fritz F, Mayer P et al (2018) Dual-energy CT iodine maps as an alternative quantitative imaging biomarker to abdominal CT perfusion: determination of appropriate trigger delays for acquisition using bolus tracking. Br J Radiol 91:20170351. https://doi.org/10.1259/bjr.20170351
Zhu L, Xue H, Sun H et al (2016) Isoattenuating insulinomas at biphasic contrast-enhanced CT: frequency, clinicopathologic features and perfusion characteristics. Eur Radiol 26:3697–3705. https://doi.org/10.1007/s00330-016-4216-7
Bao J, Liu A, Zhao C et al (2019) Correlation between dual-energy computed tomography single scan and computed tomography perfusion for pancreatic cancer patients: initial experience. J Comput Assist Tomogr 43:599–604. https://doi.org/10.1097/rct.0000000000000878
Zhu L, Wu W, Xue H et al (2017) Sporadic insulinomas on volume perfusion CT: dynamic enhancement patterns and timing of optimal tumour–parenchyma contrast. Eur Radiol 27:3491–3498. https://doi.org/10.1007/s00330-016-4709-4
Li H, Guo J, Sun C et al (2015) Assessment of pancreatic adenocarcinoma: use of low-dose whole pancreatic CT perfusion and individualized dual-energy CT scanning. J Med Imaging Radiat Oncol 59:590–598. https://doi.org/10.1111/1754-9485.12342
Yin Y, Jiang J (2016) JOG technique versus nonspiral axial scan in pancreatic perfusion computed tomography imaging and their preliminary application. J Comput Assist Tomogr 40:880–885. https://doi.org/10.1097/rct.0000000000000445
Tian C, Xu X (2017) Multislice spiral perfusion computed tomography to assess pancreatic vascularity in mild acute pancreatitis. J Comput Assist Tomogr 41:284–288. https://doi.org/10.1097/rct.0000000000000500
D’Onofrio M, Gallotti A, Mantovani W et al (2013) Perfusion CT can predict tumoral grading of pancreatic adenocarcinoma. Eur J Radiol 82:227–233. https://doi.org/10.1016/j.ejrad.2012.09.023
Yadav AK, Sharma R, Kandasamy D et al (2016) Perfusion CT—can it resolve the pancreatic carcinoma versus mass forming chronic pancreatitis conundrum? Pancreatology 16:979–987. https://doi.org/10.1016/j.pan.2016.08.011
Sugimoto M, Takahashi S, Kobayashi T et al (2015) Pancreatic perfusion data and post-pancreaticoduodenectomy outcomes. J Surg Res 194:441–449. https://doi.org/10.1016/j.jss.2014.11.046
Fritz F, Skornitzke S, Hackert T et al (2016) Dual-energy perfusion-CT in recurrent pancreatic cancer–preliminary results. Rofo 188:559–565. https://doi.org/10.1055/s-0042-105765
Xie Q, Wu J, Tang Y et al (2013) Whole-organ CT perfusion of the pancreas: impact of iterative reconstruction on image quality, perfusion parameters and radiation dose in 256-slice CT-preliminary findings. PLoS One 8:e80468. https://doi.org/10.1371/journal.pone.0080468
Lu N, Feng XY, Hao SJ et al (2011) 64-slice CT perfusion imaging of pancreatic adenocarcinoma and mass-forming chronic pancreatitis. Acad Radiol 18:81–88. https://doi.org/10.1016/j.acra.2010.07.012
Kaufmann S, Schulze M, Horger T et al (2015) Reproducibility of VPCT parameters in the normal pancreas: comparison of two different kinetic calculation models. Acad Radiol 22:1099–1105. https://doi.org/10.1016/j.acra.2015.04.005
Kubota M, Murakami T, Nagano H et al (2012) Xenon-inhalation computed tomography for noninvasive quantitative measurement of tissue blood flow in pancreatic tumor. Dig Dis Sci 57:801–805. https://doi.org/10.1007/s10620-011-1915-4
Hirota M, Tsuda M, Tsuji Y et al (2011) Perfusion computed tomography findings of autoimmune pancreatitis. Pancreas 40:1295–1301. https://doi.org/10.1097/mpa.0b013e31821fcc4f
Kovač JD, Đurić-Stefanović A, Dugalić V et al (2019) CT perfusion and diffusion-weighted MR imaging of pancreatic adenocarcinoma: can we predict tumor grade using functional parameters? Acta Radiol 60:1065–1073. https://doi.org/10.1177/0284185118812202
Tsushima Y, Kusano S (1998) Age-dependent decline in parenchymal perfusion in the normal human pancreas: measurement by dynamic computed tomography. Pancreas 17:148–152. https://doi.org/10.1097/00006676-199808000-00006
Halperin DM, Lee JJ, Ng CS et al (2019) A phase II trial of ziv-aflibercept in patients with advanced pancreatic neuroendocrine tumors. Pancreas 48:381–386. https://doi.org/10.1097/mpa.0000000000001258
Nishikawa Y, Tsuji Y, Isoda H et al (2014) Perfusion in the tissue surrounding pancreatic cancer and the patient’s prognosis. Biomed Res Int. https://doi.org/10.1155/2014/648021
Bize PE, Platon A, Becker CD, Poletti PA (2006) Perfusion measurement in acute pancreatitis using dynamic perfusion MDCT. AJR Am J Roentgenol 186:114–118. https://doi.org/10.2214/ajr.04.1416
Yao JC, Phan AT, Hess K et al (2015) Perfusion computed tomography as functional biomarker in randomized run-in study of bevacizumab and everolimus in well-differentiated neuroendocrine tumors. Pancreas 44:190–197. https://doi.org/10.1097/mpa.0000000000000255
Hamdy A, Ichikawa Y, Toyomasu Y et al (2019) Perfusion CT to assess response to neoadjuvant chemotherapy and radiation therapy in pancreatic ductal adenocarcinoma: initial experience. Radiology 292:628–635. https://doi.org/10.1148/radiol.2019182561
Barău A, Ruiz-Sauri A, Valencia G et al (2013) High microvessel density in pancreatic ductal adenocarcinoma is associated with high grade. Virchows Arch 462:541–546. https://doi.org/10.1007/s00428-013-1409-1
Hessmann E, Buchholz SM, Demir IE et al (2020) Microenvironmental determinants of pancreatic cancer. Physiol Rev 100:1707–1751. https://doi.org/10.1152/physrev.00042.2019
Mayer P, Fritz F, Koell M et al (2021) Assessment of tissue perfusion of pancreatic cancer as potential imaging biomarker by means of intravoxel incoherent motion MRI and CT perfusion: correlation with histological microvessel density as ground truth. Cancer Imaging 21:13. https://doi.org/10.1186/s40644-021-00382-x
Yang Y, Shi J, Zhu J (2021) Diagnostic performance of noninvasive imaging modalities for localization of insulinoma: a meta-analysis. Eur J Radiol 145:110016. https://doi.org/10.1016/j.ejrad.2021.110016
Zhu L, Xue H, Sun Z et al (2017) Prospective comparison of biphasic contrast-enhanced CT, volume perfusion CT, and 3 Tesla MRI with diffusion-weighted imaging for insulinoma detection. J Magn Reson Imaging 46:1648–1655. https://doi.org/10.1002/jmri.25709
Soloff EV, Al-Hawary MM, Desser TS et al (2022) Imaging assessment of pancreatic cancer resectability after neoadjuvant therapy: AJR expert panel narrative review. AJR Am J Roentgenol 218:570–581. https://doi.org/10.2214/ajr.21.26931
Funding
Open Access funding enabled and organized by Projekt DEAL. For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding program “Open Access Publikationskosten” as well as by Heidelberg University. This project was supported by the German Federal Ministry of Education and Research (BMBF) under grant number 031L0163.
Author information
Authors and Affiliations
Contributions
SS involved in conceptualization, data collection and interpretation, methodology, funding acquisition, project supervision, writing—original draft, and writing—review and editing. NV involved in data collection and interpretation, methodology, formal analysis, statistical analysis, validation, writing—original draft, and writing—review and editing. PM involved in clinical input and writing—review and editing. HK involved in project supervision and writing—review and editing. WS involved in conceptualization, technical input, data interpretation, project supervision and writing—review and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
SS has ownership interests in investment funds containing stock of healthcare companies. The other authors declare that they have no competing interests related to the subject matter of the article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Skornitzke, S., Vats, N., Mayer, P. et al. Pancreatic CT perfusion: quantitative meta-analysis of disease discrimination, protocol development, and effect of CT parameters. Insights Imaging 14, 132 (2023). https://doi.org/10.1186/s13244-023-01471-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-023-01471-0