
Abstract
Background
Cholesterol plays important roles in β-amyloid (Aβ) metabolism and atherosclerosis. However, the relationships of plasma cholesterol levels with Aβ and cerebral small vessel disease (CSVD) burdens are not fully understood in Asians. Herein, we investigated the relationships between plasma cholesterol profile components and Aβ and CSVD burdens in a large, non-demented Korean cohort.
Methods
We enrolled 1,175 non-demented participants (456 with unimpaired cognition [CU] and 719 with mild cognitive impairment [MCI]) aged ≥ 45 years who underwent Aβ PET at the Samsung Medical Center in Korea. We performed linear regression analyses with each cholesterol (low-density lipoprotein cholesterol [LDL-c], high-density lipoprotein cholesterol [HDL-c], and triglyceride) level as a predictor and each image marker (Aβ uptake on PET, white matter hyperintensity [WMH] volume, and hippocampal volume) as an outcome after controlling for potential confounders.
Results
Increased LDL-c levels (β = 0.014 to 0.115, p = 0.013) were associated with greater Aβ uptake, independent of the APOE e4 allele genotype and lipid-lowering medication. Decreased HDL-c levels (β = − 0.133 to − 0.006, p = 0.032) were predictive of higher WMH volumes. Increased LDL-c levels were also associated with decreased hippocampal volume (direct effect β = − 0.053, p = 0.040), which was partially mediated by Aβ uptake (indirect effect β = − 0.018, p = 0.006).
Conclusions
Our findings highlight that increased LDL-c and decreased HDL-c levels are important risk factors for Aβ and CSVD burdens, respectively. Furthermore, considering that plasma cholesterol profile components are potentially modified by diet, exercise, and pharmacological agents, our results provide evidence that regulating LDL-c and HDL-c levels is a potential strategy to prevent dementia.
Similar content being viewed by others

Background
Alzheimer’s disease (AD) and cerebral small vessel disease (CSVD) are common causes of dementia in the elderly. AD is characterized by the deposition of β-amyloid (Aβ), which starts to accumulate 10–20 years before the onset of clinical symptoms. CSVD burdens, such as severe white matter hyperintensities (WMH), are also gradually deposited in subcortical regions over several decades, eventually resulting in subcortical vascular dementia. Recent advances in neuroimaging have enabled the detection of these pathological burdens in living individuals without dementia.
Plasma cholesterol levels are major risk factors for coronary artery disease and stroke. Plasma cholesterol levels are also closely associated with other components of the cardiometabolic syndrome, which may affect the development of dementia [1, 2]. However, epidemiological evidence of the association between plasma cholesterol levels and dementia is complex [3]. Some studies have shown that increased total cholesterol levels are predictive of an increased risk of dementia. In contrast, other studies have not shown a relationship between total cholesterol levels and the risk of dementia. In fact, other studies have reported that increased total cholesterol levels are associated with a reduced risk of dementia. These inconsistencies in the findings may be explained by several factors. First, most previous studies have not investigated the relationship between plasma cholesterol levels and biomarkers of AD and CSVD. The clinical diagnostic criteria for AD and CSVD do not necessarily represent the presence of AD and CSVD imaging markers. Moreover, most studies were limited to total cholesterol rather than dysregulation of cholesterol homeostasis, such as increased low-density lipoprotein cholesterol (LDL-c) or decreased high-density lipoprotein cholesterol (HDL-c). Dysregulation of cholesterol homeostasis is a more important risk factor for cardiovascular disease than total cholesterol levels are.
Cholesterol in the brain plays fundamental roles in the synthesis and maintenance of neuronal cells and is linked to brain health [4]. Cholesterol has also important roles in the synthesis, deposition, and clearance of Aβ [5, 6]. Plasma cholesterol levels are well-known atherogenic risk scores. Several studies have investigated the relationships between plasma cholesterol profile components and biomarkers [7,8,9]. However, the results of these studies were inconclusive because the sample sizes were small. In addition, racial diversity was lacking among the participants. In fact, differences exist in the body composition, effects of cardiometabolic syndromes on brain age, and frequencies of imaging marker abnormalities among Asians and non-Hispanic whites (NHWs). Specifically, the Asian population has a higher risk of hypercholesterolemia [10] and cardiometabolic syndromes [11] than NHWs with a similar body mass index (BMI), which is explained by unfavorable body composition and fat distribution [12, 13]. In addition, the Asian population has higher CSVD burdens and a lower Aβ frequency than NHWs [14, 15].
Therefore, in the present study, we investigated the relationships between plasma cholesterol profile components and biomarkers of AD and CSVD in a large non-demented Korean cohort. To avoid the potential reverse effects of dementia on blood cholesterol, participants were limited to non-demented participants, although participants with mild cognitive impairment (MCI) might be more likely to have poor cholesterol profile than those with unimpaired cognition (CU). We hypothesized that increased LDL-c and decreased HDL-c levels would be predictive of increased Aβ and CSVD burdens. Furthermore, these imaging markers may mediate the relationship between plasma cholesterol profile components and downstream imaging markers, including hippocampal atrophy.
Methods
Study participants
We enrolled 1,175 non-demented participants (456 with CU and 719 with MCI) aged ≥ 45 years who underwent Aβ PET in the memory clinic at the Samsung Medical Center (Seoul, Korea) between August 2015 and August 2020. All participants underwent a comprehensive dementia examination including a standardized neuropsychological test [16], APOE genotyping, and brain magnetic resonance imaging (MRI). All participants with CU met the following criteria: (1) no medical history that was likely to affect cognitive function based on Christensen’s health screening criteria [17]; (2) no objective cognitive impairment in any cognitive domain on a comprehensive neuropsychological test battery (above at least -1.0 SD of age-adjusted norms on any cognitive test); and (3) independence in activities of daily living. All participants with MCI met the criteria for MCI with the following modifications [18, 19]: (1) subjective cognitive complaints by the participants or caregivers; (2) objective memory impairment below -1·0 SD on verbal or visual memory tests; (3) no significant impairment in activities of daily living; and (4) non-demented status.
We excluded participants with severe WMH (cap or band > 10 mm and longest diameter of deep white matter lesion > 25 mm), structural lesions including cerebral infarction, intracranial hemorrhage, brain tumors, and hydrocephalus on MRI, and abnormal laboratory results on complete blood count, electrolyte, vitamin B12 and folate levels, syphilis serology, and liver/kidney/thyroid function tests.
The Institutional Review Board of the Samsung Medical Center approved this study. Written informed consent was obtained from all the participants.
Aβ PET acquisition
All participants underwent Aβ PET (18F-florbetaben) and 18F-flutemetamol PET scans using a Discovery STe PET/CT scanner (GE Medical Systems, Milwaukee, WI, USA). For 18F-florbetaben PET or 18F-flutemetamol PET, a 20-min emission PET scan in dynamic mode (comprising 4 × 5 min frames) was performed 90 min after an injection of a mean dose of 311.5 MBq 18F-florbetaben or 197.7 MBq 18F-flutemetamol, respectively. Three-dimensional PET images were reconstructed in a 128 × 128 × 48 matrix with 2 × 2 × 3·27 mm voxel size using the ordered-subsets expectation maximization algorithm (18F-florbetaben, iteration = 4 and subset = 20; 18F-flutemetamol, iteration = 4 and subset = 20).
Aβ PET quantification using dcCL scales
Aβ uptakes were quantified using BeauBrain Morph of BeauBrain Healthcare Co., Ltd., which performs fully-automated image analysis of Aβ uptakes on PET images. We used a direct comparison of the FBB-FMM CL (dcCL) method previously developed by our group [20] to standardize the quantification of Aβ PET images obtained using different ligands. The dcCL method for FBB and FMM PET enables the transformation of the standardized uptake value ratio (dcSUVR) of FBB and FMM PETs to dcCL scales directly, without conversion to the 11C-labeled Pittsburgh compound SUVR.
There are three steps to obtaining dcCL scales [20]: 1) pre-processing of PET images, 2) determination of the global cortical target volume of interest (CTX VOI), and 3) conversion of dcSUVR to dcCL scales. First, to preprocess the Aβ PET images, PET images were co-registered to each participant’s MR image and then normalized to a T1-weighted MNI-152 template using the SPM8 unified segmentation method. We used T1-weighted MRI correction with the N3 algorithm only for intensity nonuniformities without applying corrections to the PET images for brain atrophy or partial volume effects. Second, we used the FBB-FMM CTX VOI, defined as areas of AD-specific brain Aβ deposition in our previous study [20]. In our previous study [20], we developed CTX VOI using the similar methods with Klunk’s Centiloid methods [21]. In their original study [21], they included 19 patients with AD dementia and 25 older controls to determine areas of AD-specific brain Aβ deposition. Briefly, to exclude areas of age-related brain Aβ deposition, the FBB-FMM CTX VOI was generated by comparing SUVR parametric images (with the whole cerebellum as a reference area) between 20 typical patients with Alzheimer’s disease-related cognitive impairment (ADCI-CTX) and 16 healthy elderly participants (EH-CTX) who underwent both FBB and FMM PET scans. To generate the FBB-FMM CTX VOI, the average EH-CTX image is subtracted from the average ADCI-CTX image. We then defined the FBB-FMM CTX VOI as the area of ADCI-related brain Aβ accumulation common to both FBB and FMM PET. Finally, the dcSUVR values of the FBB-FMM CTX VOI were converted to dcCL scales by using the dcCL conversion equation. The dcCL equation was derived from the FBB-FMM CTX VOI separately for FBB and FMM PET, and applied to FBB and FMM dcSUVR.
To determine the participants’ dcCL cut-off-based Aβ positivity, we applied the optimal cut-off value derived using k-means cluster analysis in 527 independent samples of participants with normal cognition. The cut-off value was set at 27.08, representing the 95th percentile of the lower cluster, and the whole cerebellum was used as a reference region.
Cholesterol and other covariate measurements
All participants underwent blood tests. Blood samples were collected after an overnight fast. The mean ± SD of time interval between blood tests and Aβ PET was 3.9 ± 5.0 months. Cholesterol levels, including LDL-c, HDL-c, and triglycerides, were measured by an enzymatic colorimetric test using a Modular D2400 analyzer (Roche Diagnostics, Basel, Switzerland). Height and weight were measured for all participants. BMI was calculated as weight (kg) divided by the square of height (m). Cholesterol levels and BMI data were obtained by backtracking in the clinical data warehouse (CDW) of the Samsung Medical Center, which were measured within 12 months before or after Aβ PET scans. Prescriptions of lipid-lowering and dementia medications (donepezil, rivastigmine, galantamine, or memantine) were extracted from the CDW. Hypertension and diabetes were defined as a diagnostic history of hypertension and diabetes or current use of any antihypertensive medication and antidiabetic medication, respectively.
MRI acquisition
We acquired standardized three-dimensional T1 Turbo Field Echo and three-dimensional fluid-attenuated inversion recovery (FLAIR) images using a 3.0 T MRI scanner (Philips 3.0T Achieva; Philips Healthcare, Andover, MA, USA), as previously described [22].
Hippocampal and WMH volume
The images were processed using the CIVET anatomical pipeline (version 2.1.0). The native MRIs were registered to the MNI-152 template by linear transformation and corrected for intensity nonuniformities using the N3 algorithm. The registered and corrected images were divided into white matter, grey matter, cerebrospinal fluid, and background. In addition, the inner and outer surfaces of the cortex were automatically extracted using the marching-cubes algorithm to obtain the cortical thickness, which was defined as the Euclidean distance between the linked vertices of the inner and outer surfaces.
As we extracted cortical surface models from MRI volumes transformed into stereotaxic space, the cortical thickness was measured in the native space by applying an inverse transformation matrix to the cortical surface and reconstructing them in the native space.
To measure hippocampal volume, we used an automated hippocampus segmentation method using a graph cut algorithm combined with atlas-based segmentation and morphological opening, as described in a previous study [23]. WMH segmentation was replicated using the Lesion Segmentation Tool (LST) in Statistical Parametric Mapping 12 [24]. LST is an automated segmentation approach for quantifying whole-brain WMH volume and shows high agreement with manual tracing of WMH in FLAIR.
Statistical analyses
To investigate the association between cholesterol levels and Aβ uptake, we performed linear regression analyses with each cholesterol type (LDL-c, HDL-c, and triglyceride) as a predictor and quantified dcCL scales as an outcome after controlling for age, sex, BMI, APOE e4 allele (APOE4) genotype, hypertension, diabetes, lipid-lowering medication, and dementia medication.
To investigate the association between cholesterol levels and neurodegeneration, we performed linear regression analyses with each cholesterol type (LDL-c, HDL-c, and triglyceride) as a predictor and hippocampal volume as an outcome after controlling for age, sex, BMI, APOE4 genotype, hypertension, diabetes, lipid-lowering medication, dementia medication, and intracranial volume.
To investigate the association between cholesterol levels and WMH volume, we performed linear regression analyses with each cholesterol type (LDL-c, HDL-c, and triglyceride) as a predictor and hippocampal volume as an outcome after controlling for age, sex, BMI, APOE4 genotype, hypertension, diabetes, lipid-lowering medication, dementia medication, and intracranial volume.
To determine whether Aβ uptake mediates the effect of cholesterol levels on neurodegeneration, we used path analyses with each cholesterol type as a predictor, Aβ uptake as a mediator, and hippocampal volume as an outcome after controlling for age, sex, BMI, APOE4 genotype, hypertension, diabetes, lipid-lowering medication, dementia medication, and intracranial volume.
The standardized β was also calculated to compare the strength of the effect of each independent variable on each dependent variable in all analyses.
Sensitivity analyses using cut-off-based categorization rather than quantified dcCL values were performed to further validate the relationship between cholesterol levels and Aβ uptake. We used logistic regression analysis with each cholesterol type (LDL-c, HDL-c, and triglyceride) as a predictor and Aβ positivity as an outcome after controlling for age, sex, BMI, APOE4 genotype, hypertension, diabetes, lipid-lowering medication, and dementia medication. In addition, we performed a single model with all cholesterol type (LDL-c, HDL-c, and triglyceride) together as predictors after age, sex, BMI, APOE e4 allele (APOE4) genotype, hypertension, diabetes, lipid-lowering medication, and dementia medication.
All reported p-values were two-sided and the significance level was set at 0.05. All analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Clinical characteristics of the participants
The mean ± SD of age was 70.8 ± 8.2 years, and 641 out of 1125 (54.6%) participants were female (Table 1). Four hundred and forty-six out of 1125 (38.0%) patients had APOE4 genotype. The mean ± SD of Aβ uptake was 39.8 ± 46.7 dcCL. The mean ± SD of WMH and hippocampal volume were 5.27 ± 9.33 and 2.78 ± 5.07 mL, respectively. The mean ± SD of LDL-c, HDL-c, and triglyceride were 109.2 ± 35.1, 58.6 ± 16.7, and 118.5 ± 55.9 mg/dL. There were no differences in LDL-c (107.6 ± 33.9 vs 110.2 ± 35.8, p = 0.208), HDL-c (59.1 ± 16.4 vs 58.3 ± 16.9, p = 0.382), and triglyceride (120.0 ± 53.6 vs 117.6 ± 57.3, p = 0.477) level between CU and MCI groups.
Cholesterol levels and Aβ uptake
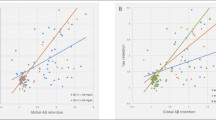
LDL-c levels (β = 0.064, p = 0.013) were independently associated with Aβ uptake. However, there were no relationships of HDL-c (β = 0.016, p = 0.552) and triglycerides levels (β = − 0.025, p = 0.308) with Aβ uptake (Table 2, Fig. 1).

Relationship on of cholesterol levels with Aβ uptake, WMH volume and HV. General linear regression analyses were performed using each cholesterol level (LDL-c, HDL-c, and triglycerides) as predictors, and dcCL scale, WMH volume, and HV as outcomes after controlling for age, sex, BMI, APOE4 genotype, hypertension, diabetes, lipid-lowering medication, and dementia medication. The standardized β was calculated to compare the strength of the effect of each independent variable on each dependent variable. Abbreviations: Aβ, amyloid-β; BMI, body mass index; HDL-c, high-density lipoprotein cholesterol; HV, hippocampal volume; LDL-c, low-density lipoprotein cholesterol; WMH, white matter hyperintensity
Cholesterol levels and WMH volume
HDL-c levels (β = − 0.069, p = 0.032) were negatively associated with WMH volume. However, LDL-c (β = 0.040, p = 0.204) and triglyceride (β = 0.022, p = 0.474) levels were not associated with WMH volume (Table 2, Fig. 1).
Cholesterol levels and hippocampal volume
LDL-c levels (β = − 0.065, p = 0.008) were negatively associated with hippocampal volume, whereas HDL-c (β = 0.015, p = 0.565) and triglyceride (β = − 0.004, p = 0.737) levels were not associated with hippocampal volume (Table 2, Fig. 1). Path analyses showed that Aβ uptake partially mediated the association between LDL-c and hippocampal volume. Specifically, increased LDL-c levels were associated with Aβ uptake (β = 0.078, p = 0.003), which was further associated with hippocampal volume (β = − 0.226, p < 0.001; indirect pathway β = − 0.018, p = 0.006). Increased LDL-c levels were also associated with hippocampal volume without mediation of Aβ uptake (direct pathway β = − 0.053, p = 0.040; Table 3, Fig. 2).

Schematic diagram of the path analyses among LDL-c, Aβ burden, and HV. Path analyses were performed using LDL-c as a predictor, Aβ uptake as a mediator, and hippocampal volume as an outcome, after controlling for age, sex, BMI, APOE4 genotype, hypertension, diabetes, lipid-lowering medication, dementia medication, and intracranial volume. Abbreviations: HV, hippocampal volume; LDL-c, low-density lipoprotein cholesterol
Sensitivity analysis
Regarding the categorical values of Aβ uptake, LDL-c levels (Odds ratio [OR] = 1.005, 95% confidence interval [CI] 1.001 to 1.009, p = 0.039) were independently associated with Aβ positivity. However, there were no relationships of HDL-c (OR = 1.002, 95% CI 0.993 to 1.012, p = 0.647) and triglycerides levels (OR = 0.997, 95% CI 0.995 to 1.000, p = 0.058) with Aβ positivity. In the analyses with all cholesterol type (LDL-c, HDL-c, and triglyceride) together as predictors, the results showed a similar trend. Specifically, LDL-c levels (β = 0.071, p = 0.001) were independently associated with Aβ uptake, while HDL-c (β = 0.004, p = 0.879) and triglycerides levels (β = − 0.036, p = 0.179) were not associated with Aβ uptake. HDL-c levels (β = − 0.071, p = 0.039) were negatively associated with WMH volume, while LDL-c (β = 0.040, p = 0.221) and triglyceride (β = − 0.009, p = 0.781) levels were not associated with WMH volume. LDL-c levels (β = − 0.067, p = 0.013) were negatively associated with hippocampal volume, whereas HDL-c (β = 0.018, p = 0.538) and triglyceride (β = 0.013, p = 0.640) levels were not associated with hippocampal volume.
Discussion
In the present study, we systematically investigated the relationships between plasma cholesterol profile components and biomarkers of AD and CSVD in a large non-demented Korean cohort. Our major findings are as follows: First, increased LDL-c levels were associated with greater Aβ uptake, independent of APOE4 genotype and lipid-lowering medication. Second, decreased HDL-c levels were predictive of higher WMH volumes. Finally, increased LDL-c levels were associated with a decreased hippocampal volume, which was partially mediated by Aβ uptake. Taken together, our findings suggest that increased LDL-c and decreased HDL-c levels are important risk factors for AD and CSVD, respectively. Furthermore, considering that plasma cholesterol profile components are potentially modified by diet, exercise, and pharmacological agents, our results provide evidence that regulating LDL-c and HDL-c levels may be a strategy to prevent dementia.
Our first major finding was that increased LDL-c levels were associated with increased Aβ uptake, independent of APOE4 genotype and lipid-lowering medication. Studies based on NHWs have shown inconsistent results regarding the association between hypercholesterolemia and Aβ uptake. Specifically, previous studies showed that increased LDL-c levels were associated with increased Aβ uptake [7, 25]. In contrast, another study did not show any relationship between the plasma cholesterol profile components and Aβ uptake [9]. However, the present study was based on the Korean population, and the sample size was the largest among studies investigating the effects of plasma cholesterol on Aβ uptake. Thus, our findings demonstrated that increased LDL-c levels were an important risk factor for increased Aβ uptake in non-demented participants, at least in the Korean population. However, unlike a previous study [7], we did not find any relationship between decreased HDL-c levels and Aβ uptake. One study suggested that decreased HDL-c levels are associated with increased Aβ uptake.
However, the potential pathophysiological role of LDL-c in Aβ uptake remains unclear. Although cholesterol in the brain plays important roles in Aβ synthesis and clearance, its bioactivity in the brain is independent of plasma cholesterol because of the blood–brain barrier (BBB). However, some studies have shown that plasma cholesterol levels are closely associated with BBB permeability [26,27,28]. Specifically, systemic hypercholesterolemia may damage the BBB via inflammation and other mechanisms, with consequent leakage of serum cholesterol, inflammatory cytokines, and amyloidogenic factors. Circulating cholesterol levels through BBB damage may lead to the destruction of cholesterol homeostasis in the brain, which may lead to AD pathology. In particular, LDL-c activates microvascular endothelial cells to increase the secretion of inflammatory mediators such as TNF-α and IL-6. LDL-c also mediates the decreased expression of tight junction protein ZO-1, indicating that LDL-c contributes to the increased permeability of the BBB in AD [29]. Conversely, there might be possibility that cholesterol metabolism is affected by Aβ uptake. Recent studies have found that Aβ have a deleterious effect on proteins involved in cholesterol metabolism including 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase and ATP-binding cassette transporter A1 [30].
Our second major finding was that decreased HDL-c levels were independently associated with increased WMH volume. This inverse association is consistent with the results of previous studies [31,32,33,34], which indicated that lower HDL-c levels were associated with higher WMH severity. HDL is well-known for its vasoprotective function via several mechanisms, such as reverse cholesterol transport, which removes cholesterol from lipid-laden macrophages in the vessel wall [35]. Additionally, HDL reduces neuroinflammation and increases bioavailability of endothelial nitric oxide synthase [36, 37]. Neuroinflammation and neurovascular decoupling caused by the impairment of endothelial nitric oxide synthase lead to CSVD burden [38].
In the present study, we found no relationship between triglyceride and imaging markers of AD and CSVD. Although triglyceride is another major cholesterol marker for hypercholesterolemia, results regarding the relationship between triglyceride and the development of dementia are inconclusive. A long-term follow-up longitudinal study revealed that increased triglyceride levels increase the risk of dementia [39]. However, another study showed no significant difference in triglyceride levels between patients with AD and cognitively unimpaired elderly individuals [40]. In fact, similar to our results, a pathological study found no association between triglyceride levels and AD pathological burden [25].
Our final major finding was that increased LDL-c levels were associated with decreased hippocampal volume, which was partially mediated by Aβ uptake. Previous results regarding the association between LDL-c and neurodegeneration have been somewhat inconsistent [41, 42]. However, considering that increased Aβ uptake was predictive of hippocampal atrophy [43], the mediating effects of Aβ uptake on the relationship between LDL-c levels and hippocampal atrophy observed in the present study could be explained. We also found that increased LDL-c levels were associated with decreased hippocampal atrophy, without the mediation of Aβ uptake. Given that LDL-c is a risk factor for arteriosclerosis and that the hippocampus is also vulnerable to cerebral ischemia, recurrent vascular insult associated with LDL-c may lead to hippocampal atrophy. Aβ-independent tauopathy may also be a possible mechanism underlying these findings. In fact, a recent study found that hypercholesterolemia directly affects tau deposition irrespective of Aβ uptake, which leads to hippocampal atrophy [42].
Limitations
The strength of the present study was that we systematically investigated the association of each cholesterol profile component with Aβ uptake and WMH volume in a large Korean cohort, after controlling for various potential confounding factors. However, our study had several limitations that need to be addressed. First, our major limitation is that our findings were cross-sectional and obtained later in life. Thus, the temporal relationship between LDL-c and Aβ uptake could not be determined because of the intrinsic limitations of a cross-sectional study. Second, the generalizability of the present study to community-based populations needs to be treated with caution because the cohort was recruited from a memory clinic setting, which results in the enrollment of a more “health-seeking” population. Third, the effect of LDL-c on Aβ uptake was relatively modest. However, given the paucity of modifiable risk factors for the development of Aβ, pharmacological agents targeting LDL-c might be clinically useful to prevent Aβ deposition. Nevertheless, our study is relevant as it provides a comprehensive understanding of the relationship between each cholesterol profile component and imaging biomarkers of AD and CSVD and their downstream markers.
Conclusions
In conclusion, increased LDL-c and decreased HDL-c levels were important risk factors for AD and CSVD, respectively. Furthermore, increased LDL-c levels are predictive of hippocampal atrophy related to Aβ uptake. Therefore, lowering LDL-c and increasing HDL-c levels may reduce Aβ uptake and CSVD burden, respectively, eventually resulting in a delay in cognitive decline.
Availability of data and materials
Anonymized data for our analyses presented in the present report are available upon request from the corresponding authors.
References
Johannesen CDL, Mortensen MB, Langsted A, Nordestgaard BG. ApoB and Non-HDL cholesterol Versus LDL cholesterol for ischemic stroke risk. Ann Neurol. 2022;92:379–89.
Colantonio LD, Bittner V, Reynolds K, Levitan EB, Rosenson RS, Banach M, et al. Association of serum lipids and coronary heart disease in contemporary observational studies. Circulation. 2016;133:256–64.
Anstey KJ, Ashby-Mitchell K, Peters R. Updating the evidence on the association between serum cholesterol and risk of late-life dementia: review and meta-analysis. J Alzheimers Dis. 2017;56:215–28.
Dietschy JM, Turley SD. Thematic review series: brain lipids. Cholesterol metabolism in the central nervous system during early development and in the mature animal. J Lipid Res. 2004;45:1375–97.
Di Paolo G, Kim TW. Linking lipids to Alzheimer’s disease: cholesterol and beyond. Nat Rev Neurosci. 2011;12:284–96.
Reitz C. Dyslipidemia and dementia: current epidemiology, genetic evidence, and mechanisms behind the associations. J Alzheimers Dis. 2012;30(Suppl 2):S127–45.
Reed B, Villeneuve S, Mack W, DeCarli C, Chui HC, Jagust W. Associations between serum cholesterol levels and cerebral amyloidosis. JAMA Neurol. 2014;71:195–200.
Nägga K, Gustavsson AM, Stomrud E, Lindqvist D, van Westen D, Blennow K, et al. Increased midlife triglycerides predict brain β-amyloid and tau pathology 20 years later. Neurology. 2018;90:e73–81.
Bennett EE, Gianattasio KZ, Hughes TM, Mosley TH, Wong DF, Gottesman RF, et al. The association between midlife lipid levels and late-life brain amyloid deposition. Neurobiol Aging. 2020;92:73–4.
Davis J, Juarez D, Hodges K. Relationship of ethnicity and body mass index with the development of hypertension and hyperlipidemia. Ethn Dis. 2013;23:65–70.
Yoon KH, Lee JH, Kim JW, Cho JH, Choi YH, Ko SH, et al. Epidemic obesity and type 2 diabetes in Asia. Lancet. 2006;368:1681–8.
Wulan SN, Westerterp KR, Plasqui G. Ethnic differences in body composition and the associated metabolic profile: a comparative study between Asians and Caucasians. Maturitas. 2010;65:315–9.
Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157–63. https://doi.org/10.1016/S0140-6736(03)15268-3.
Sperling RA, Donohue MC, Raman R, Sun CK, Yaari R, Holdridge K, et al. Association of factors with elevated amyloid burden in clinically normal older individuals. JAMA Neurol. 2020;77:735–45.
Kim J, Jung SH, Choe YS, Kim S, Kim B, Kim HR, et al. Ethnic differences in the frequency of β-amyloid deposition in cognitively normal individuals. Neurobiol Aging. 2022;114:27–37.
Kang SH, Park YH, Lee D, Kim JP, Chin J, Ahn Y, et al. The cortical neuroanatomy related to specific neuropsychological deficits in Alzheimer’s continuum. Dement Neurocogn Disord. 2019;18:77–95.
Christensen KJ, Multhaup KS, Nordstrom S, Voss K. A cognitive battery for dementia: development and measurement characteristics. Psychol Assess. 1991;3:168–74.
Petersen RC. Clinical practice. Mild cognitive impairment. N Engl J Med. 2011;364:2227–34.
Jeong HJ, Lee H, Lee S-Y, Seo S, Park KH, Lee Y-B, et al. [18F]THK5351 PET imaging in patients with mild cognitive impairment. J Clin Neurol. 2020;16:202–14.
Cho SH, Choe YS, Kim HJ, Jang H, Kim Y, Kim SE, et al. A new Centiloid method for (18)F-florbetaben and (18)F-flutemetamol PET without conversion to PiB. Eur J Nucl Med Mol Imaging. 2020;47:1938–48.
Klunk WE, Koeppe RA, Price JC, Benzinger TL, Devous MD Sr, Jagust WJ, et al. The Centiloid project: standardizing quantitative amyloid plaque estimation by PET. Alzheimers Dement. 2015;11:1–15.e1-4.
Kang SH, Kim ME, Jang H, Kwon H, Lee H, Kim HJ, et al. Amyloid positivity in the Alzheimer/subcortical-vascular spectrum. Neurology. 2021;96:e2201–11.
Kwak K, Yoon U, Lee DK, Kim GH, Seo SW, Na DL, et al. Fully-automated approach to hippocampus segmentation using a graph-cuts algorithm combined with atlas-based segmentation and morphological opening. Magn Reson Imaging. 2013;31:1190–6.
Jeon S, Yoon U, Park JS, Seo SW, Kim JH, Kim ST, et al. Fully automated pipeline for quantification and localization of white matter hyperintensity in brain magnetic resonance image. 2011;21:193–200. https://doi.org/10.1002/ima.20277.
Wingo AP, Vattathil SM, Liu J, Fan W, Cutler DJ, Levey AI, et al. LDL cholesterol is associated with higher AD neuropathology burden independent of APOE. J Neurol Neurosurg Psychiatry. 2022;93:930–8.
van de Haar HJ, Burgmans S, Jansen JF, van Osch MJ, van Buchem MA, Muller M, et al. Blood-brain barrier leakage in patients with early Alzheimer disease. Radiology. 2016;281:527–35.
Winocur G, Greenwood CE. Studies of the effects of high fat diets on cognitive function in a rat model. Neurobiol Aging. 2005;26(Suppl 1):46–9.
Thériault P, ElAli A, Rivest S. High fat diet exacerbates Alzheimer’s disease-related pathology in APPswe/PS1 mice. Oncotarget. 2016;7:67808–27.
Dias HK, Brown CL, Polidori MC, Lip GY, Griffiths HR. LDL-lipids from patients with hypercholesterolaemia and Alzheimer’s disease are inflammatory to microvascular endothelial cells: mitigation by statin intervention. Clin Sci (Lond). 2015;129:1195–206.
Azizidoost S, Babaahmadi-Rezaei H, Nazeri Z, Cheraghzadeh M, Kheirollah A. Amyloid beta increases ABCA1 and HMGCR protein expression, and cholesterol synthesis and accumulation in mice neurons and astrocytes. Biochim Biophys Acta Mol Cell Biol Lipids. 2022;1867:159069.
Carmelli D, Swan GE, Reed T, Wolf PA, Miller BL, DeCarli C. Midlife cardiovascular risk factors and brain morphology in identical older male twins. Neurology. 1999;52:1119–24.
Crisby M, Bronge L, Wahlund LO. Low levels of high density lipoprotein increase the severity of cerebral white matter changes: implications for prevention and treatment of cerebrovascular diseases. Curr Alzheimer Res. 2010;7:534–9.
Yin ZG, Wang QS, Yu K, Wang WW, Lin H, Yang ZH. Sex differences in associations between blood lipids and cerebral small vessel disease. Nutr Metab Cardiovasc Dis. 2018;28:28–34.
Willey JZ, Gardener H, Moon YP, Yoshita M, DeCarli C, Cheung YK, et al. Lipid profile components and subclinical cerebrovascular disease in the northern Manhattan study. Cerebrovasc Dis. 2014;37:423–30.
Mineo C, Shaul PW. Novel biological functions of high-density lipoprotein cholesterol. Circ Res. 2012;111:1079–90.
Nofer JR, van der Giet M, Tölle M, Wolinska I, von Wnuck LK, Baba HA, et al. HDL induces NO-dependent vasorelaxation via the lysophospholipid receptor S1P3. J Clin Invest. 2004;113:569–81.
Cockerill GW, Rye KA, Gamble JR, Vadas MA, Barter PJ. High-density lipoproteins inhibit cytokine-induced expression of endothelial cell adhesion molecules. Arterioscler Thromb Vasc Biol. 1995;15:1987–94.
Ungvari Z, Toth P, Tarantini S, Prodan CI, Sorond F, Merkely B, et al. Hypertension-induced cognitive impairment: from pathophysiology to public health. Nat Rev Nephrol. 2021;17:639–54.
Kalmijn S, Foley D, White L, Burchfiel CM, Curb JD, Petrovitch H, et al. Metabolic cardiovascular syndrome and risk of dementia in Japanese-American elderly men. The Honolulu-Asia aging study. Arterioscler Thromb Vasc Biol. 2000;20:2255–60.
Cagnin A, Zambon A, Zarantonello G, Vianello D, Marchiori M, Mercurio D, et al. Serum lipoprotein profile and APOE genotype in Alzheimer’s disease. J Neural Transm Suppl. 2007. https://doi.org/10.1007/978-3-211-73574-9_22.175-9.
Akinyemi RO, Mukaetova-Ladinska EB, Attems J, Ihara M, Kalaria RN. Vascular risk factors and neurodegeneration in ageing related dementias: Alzheimer’s disease and vascular dementia. Curr Alzheimer Res. 2013;10:642–53.
Vemuri P, Lesnick TG, Przybelski SA, Knopman DS, Lowe VJ, Graff-Radford J, et al. Age, vascular health, and Alzheimer disease biomarkers in an elderly sample. Ann Neurol. 2017;82:706–18.
Villemagne VL, Burnham S, Bourgeat P, Brown B, Ellis KA, Salvado O, et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. 2013;12:357–67.
Funding
This research was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI19C1132); a grant of the Korea Dementia Research Project through the Korea Dementia Research Center(KDRC), funded by the Ministry of Health & Welfare and Ministry of Science and ICT, Republic of Korea (grant number: HU20C0111); a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare and Ministry of science and ICT, Republic of Korea (grant number: HU22C0170); the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (NRF-2019R1A5A2027340, NRF-2022R1F1A1063966); Institute of Information & communications Technology Planning & Evaluation (IITP)grant funded by the Korea government(MSIT) (No.2021-0-02068, Artificial Intelligence Innovation Hub); Future Medicine 20*30 Project of the Samsung Medical Center [#SMX1230081]; the "Korea National Institute of Health" research project(2021-ER1006-02); Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education(grant number: 2022R1I1A1A01056956); and Korea University Guro Hospital (KOREA RESEARCH-DRIVEN HOSPITAL) grant (No. O2309441).
Author information
Authors and Affiliations
Contributions
Concept and design: S.H. Kang, J.P. Kim, S.W. Seo. Acquisition of data: S.H. Kang, B.K. Cheon, Y.H. Park, S-J. Kim, H. Ham, H. Jang, H.J. Kim, K. Oh, S-B. Koh, D.L. Na, J.P. Kim, S.W. Seo. Analysis, or interpretation of data: S.H. Kang, H. Yoo, J.P. Kim, S.W. Seo. Drafting of the manuscript: S.H. Kang. Intellectual content: S.H. Kang, J.P. Kim, S.W. Seo. Statistical analysis: S.H. Kang, H. Yoo. Obtained funding: S.H. Kang, S.W. Seo. Administrative, technical, or material support: J.P. Kim, S.W. Seo. Supervision: S.W. Seo.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Approval was obtained from the ethics committee of Samsung Medical Centre. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients and caregivers.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kang, S.H., Yoo, H., Cheon, B.K. et al. Distinct effects of cholesterol profile components on amyloid and vascular burdens. Alz Res Therapy 15, 197 (2023). https://doi.org/10.1186/s13195-023-01342-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-023-01342-2