
Abstract
Background
Immune system dysregulation plays a vital role in the pathogenesis of neurodegenerative diseases, even considered to be as important as classical pathological protein aggregation assumption. However, the associations of immune-mediated diseases with incident dementia are unclear and need to be clarified in prospective studies with a large population and long follow-up time.
Methods
We investigated the relationship between any or individual immune-mediated diseases and incident dementia based on a prospective cohort UK Biobank. The risk for dementia was assessed with multivariable hazard ratio (HR) and 95% confidence interval (CI) after adjusting for various potential confounders using time-varying Cox proportional hazards regression. We also performed the subgroup Cox analysis stratified by time since immune-mediated diseases and gender. Causal mediation analyses with 1000 bootstrapped iterations were conducted to explore the mediation effects of peripheral immune cells on the associations of immune-mediated diseases with dementia.
Results
A total of 375,894 participants were included in the study, among which 5291 developed dementia during a median follow-up of 9.08 years. Immune-mediated diseases were associated with an increased risk of dementia (HR, 1.10; 95% CI, 1.00–1.21), and the risk was highest between 1 and 2 years after immune-mediated diseases onset (HR, 2.74; 95% CI, 1.86–4.04). Females who suffered from immune-mediated diseases were more prone to AD, while males were more susceptible to VD. Four of the individual immune-mediated diseases including type I diabetes mellitus (HR, 2.49; 95% CI, 1.97–3.15), rheumatic fever or rheumatic heart diseases (HR, 1.36; 95% CI, 1.05–1.77), multiple sclerosis (HR, 2.87; 95% CI, 1.92–4.30), and necrotizing vasculopathies (HR, 1.71; 95%CI, 1.03–2.85) were significantly related to higher dementia incidence. The relationship between immune-mediated diseases and dementia was partially mediated by peripheral immune cells including neutrophils and lymphocytes.
Conclusions
In this large cohort study, immune-mediated diseases were proven to be significantly associated with an increased risk of incident dementia, especially for type I diabetes mellitus which was observed to be related to the higher incidence of all types of dementia. Our findings could provide new sights on dementia pathogenesis and intervention from the perspective of systemic immunology and immune-mediated diseases.
Similar content being viewed by others


Introduction
Aging accompanied neurodegeneration involving neuronal dysfunction and loss is critical in dementia pathogenesis. Since Alzheimer’s disease (AD) was first characterized by Alois Alzheimer in 1907, who found the hallmarks of extracellular plaques and intracellular neurofibrillary tangles, the mechanism studies of dementia in the past century mainly focused on protein aggregation such as amyloid β (Aβ), tau, α-synuclein, and transactive response DNA-binding protein 43 kDa (TDP-43) [1, 2]. In addition to protein aggregation, there has been growing recognition regarding the role of immune system dysfunction in neurodegenerative pathogenesis. Immune signaling molecules including the transforming growth factors, the interleukins, the complements, and the triggering receptor expressed on myeloid cells 2 (TREM2) directly cause neuron damage or indirectly interact with the protein aggregation process, which contributes to neurodegeneration [3,4,5]. Immune cells, including neutrophils and lymphocytes, were also proven to influence the neurodegenerative pathology [6, 7] and modify the risk of dementia [8, 9]. Corresponding immune-modulatory agents for dementia, especially AD, were set into preclinical or clinical investigation, although the efficiency is still controversial [10].
Immune-mediated diseases are systemic diseases of complex, multifactorial etiology in the context of immune system dysfunction as well, including but not limited to inflammatory bowel diseases, multiple sclerosis, type I diabetes, systemic lupus erythematosus, and rheumatoid arthritis [11, 12]. There have been studies revealing genetic links between immune-mediated diseases and dementia. One study found fifteen overlapped single-nucleotide polymorphisms (SNPs) within frontotemporal dementia (FTD) and immune-mediated diseases, and over half of the SNPs were mapped to the human leukocyte antigen (HLA) region, which is an area rich in genes related to microglial function [13]. Another study identified eight overlapped SNPs associated with the risk of both AD and immune-mediated diseases [14], and one of the loci was in the HLA region too. Further, the aforementioned immune molecules and cells in neurodegeneration like interleukins, neutrophils, and lymphocytes were also implicated as critical contributors in immune-mediated diseases [15]. These findings supported that immune-mediated diseases shared similar genetic, molecular, and cellular pathways with dementia, which may predict the onset of dementia.
To fully unravel the associations of immune-mediated diseases with incident dementia, we investigated the risk for dementia in immune-mediated diseases patients compared to healthy controls based on a prospective cohort UK Biobank (UKB) taking advantage of long follow-up time and large population. Considering the critical role of peripheral immune cells in both immune-mediated diseases and dementia, we further performed the causal mediation analyses to explore the effects of peripheral neutrophils and lymphocytes on the associations of immune-mediated diseases with dementia.
Methods
Study participants
The participants and data resources involved in this study were from a population-based prospective cohort UKB, under application number 19542. Between 2006 and 2010, over 500,000 participants aged 40–69 years were recruited in UKB with a comprehensive baseline assessment of health status at 22 centers throughout the UK [16]. Follow-up is conducted chiefly through linkages to routinely available national datasets, including death register data, cancer register data, hospital inpatient data, and primary care data (https://www.ukbiobank.ac.uk/). Environmental, genetic, disease status, and other clinical data were obtained from questionnaires, physical measures, sample assays, and linked electronic health data. Ethics approval for the UKB study was obtained from the North West Multicenter Research Ethical Committee. All participants provided written informed-consent paper at baseline. We restricted analyses to individuals with hospital inpatient data where the diagnosis information based on International Classification of Diseases (ICD)-10 codes were available to identify immune-mediated diseases patients. The control comparators were defined as the individuals with hospital inpatient data but none of the immune-mediated diseases was diagnosed. Prevalent dementia patients at baseline and those without traceable outcome data were excluded.
Ascertainment of the exposure variable immune-mediated disease
We identified immune-mediated diseases' status and diagnosis date by matching the corresponding ICD-10 codes [17] from hospital inpatient data (HESIN). If two or more different diagnosis dates were recorded for the same disease, the earliest one was used as the primary diagnosis date. Only the diseases with at least 500 affected individuals were kept for further analyses because the dementia incidence was low in some rare immune-mediated diseases. A total of 20 immune-mediated diseases were ascertained (Supplementary Table 1). We assessed the longitudinal associations of any immune-mediated diseases and the individual immune-mediated diseases with dementia. The immune-mediated diseases were required to be diagnosed at least one year before the dementia diagnosis.
Ascertainment of the outcome variable incident dementia
Incident all-cause dementia (ACD), AD, and vascular dementia (VD) were ascertained and classified according to the ICD codes and Read codes (Supplementary Table 2). ACD covered all the types of dementia including AD, VD, FTD, dementia with Lewy bodies (DLB), Parkinson’s disease dementia (PDD), dementia in corticobasal degeneration (CBD), dementia in other neurodegenerative, and specified diseases. The outcome records were extracted from algorithmically defined (Fields 42,018–42,025), first occurrences data reported (Fields 131,036–131,037, 130,836–130,843), death register data documented (Fields 40,001–40,002), HESIN summarized (Fields 41,270–41,271, 41,280–41,281), and primary care data recorded (Field 42,040) dementia. Follow-up visits began from the date of attending the assessment center (Field 53) to the earliest incident dementia diagnosis, date of death, the last data collection date by the general practitioner, or the last time of hospital inpatient admission, whichever occurred first.
Ascertainment of the mediator variable peripheral immune cell
Blood samples collected in ethylenediaminetetraacetic acid (EDTA) vacutainers of the UKB participants were analyzed at the UKB central laboratory within 24 h of blood draw. Differential leukocytes counts were acquired from the automated quantitative analyzer, the Beckman Coulter LH750 Hematology Analyzer. We extracted the blood count data of neutrophils and lymphocytes collected after immune-mediated diseases diagnosis and before dementia onset.
Statistical analyses
Baseline characteristics of participants were summarized for those with and without incident dementia status as mean and standard deviation (SD) for continuous variables, number, and percentage for categorical variables. Longitudinal associations of immune-mediated diseases with incident dementia were examined with multivariable time-varying Cox proportional hazard regression models and presented with hazard ratio (HR) and 95% confidence interval (CI). Participants who died, withdrew from the study before the end of follow-up, or had not developed dementia by the end of follow-up (April 7, 2021) were censored. In the primary analysis, we performed the model unadjusted, then adjusted for age, sex, ApoE-ε4, education, ethnicity, body mass index (BMI), socioeconomic status indicated by Townsend deprivation score, smoking, and alcohol consumption. The p values were further adjusted to control the false discovery rate (FDR) at 5% using the Benjamini–Hochberg procedure (labeled as Q values) when analyzing the associations of 20 individual immune-mediated diseases with dementia. In secondary analyses, we explored the effect of time since immune-mediated diseases on dementia. Time since immune-mediated diseases was split into overlapping periods (1 to 2 years, 1 to 3 years, 1 to 4 years, 1 to 5 years, 1 to 10 years, 1 to 15 years, 1 to 20 years, and 1 to over 20 years). We also estimated the effect differences of immune-mediated diseases on dementia across sex groups at recruitment. To evaluate the potential reverse causation biases, we also performed the sensitivity analyses by excluding the participants with follow-up time less than 5 or 10 years as suggested in work conducted by Sipila et al. [18]. Finally, the mediation analyses based on the methods proposed by Baron and Kenny [19] with the significance determined using 10,000 bootstrapped iterations were conducted to investigate whether the associations of immune-mediated diseases with dementia were mediated by peripheral immune cells which were proven to be related to dementia incidence in our previous study based on UKB. In addition, the interaction analyses were performed between sex and peripheral immune cells in contributing to the dementia incidence.
All the above analyses were carried out using R version 4.0.2. A p-value of less than 0.05 was considered to be statistically significant.
Results
Population characteristics
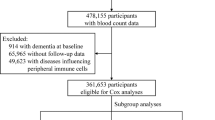
Among 502,493 participants at baseline in the UKB, 375,894 participants with HESIN ICD-10 data were eligible for Cox analysis after excluding 888 participants with prevalent dementia at baseline and 33,527 participants without follow-up data (Supplementary Fig. 1). Baseline characteristics of the included participants are presented by incident dementia status (Table 1) and immune-mediated diseases status (Supplementary Table 3). Overall, the mean age of participants was 57.32 (± 7.99) years, and 205,575 (54.69%) of them were females. Among these participants, 58,589 were diagnosed with at least one of the 20 immune-mediated diseases 1 year before dementia onset. During a median follow-up of 9.08 years, 5291 participants developed dementia, of which 2301 cases were AD and 1249 cases were VD.
Any immune-mediated diseases and dementia risk
Immune-mediated diseases in whole were associated with increased risk of ACD (HR, 1.10; 95% CI, 1.00–1.21) and VD (HR, 1.43; 95% CI, 1.19–1.73) while not associated with AD after multivariable adjustment for age, sex, education, ApoE-ε4, ethnicity, BMI, Townsend deprivation score, smoking, and alcohol consumption (Fig. 1 and Supplementary Table 4). When split the time since immune-mediated diseases into overlapping periods, the results were still statistically significant for ACD and VD in all periods. A similar risk efficacy was also observed for AD in three years before immune-mediated diseases diagnosis (Fig. 2). The risk of dementia was highest between 1 and 2 years after immune-mediated diseases onset for ACD (HR, 2.74; 95% CI, 1.86–4.04), AD (HR, 2.15; 95% CI, 1.12–4.16), and VD (HR, 5.39; 95% CI, 2.95–9.84). Subgroup analyses of sex stratification indicated that females with immune-mediated diseases were more prone to AD in the early years after immune-mediated disease (Fig. 2), while males were more susceptible to VD during a long follow-up time period (Fig. 2 and Supplementary Table 4). Sensitivity analyses showed that the risk associations with ACD and VD remained when immune-mediated diseases occurred more than 5 years before the diagnosis of dementia (Supplementary Table 5). While when dementia cases occurred from 10 years onward, the associations for ACD only persisted in models unadjusted or adjusted for age, sex, ApoE-ε4, and education, and the associations for VD were consistently robust in all models (Supplementary Table 5).

The cumulative dementia hazard according to the status of immune-mediated diseases. ACD, all-cause dementia; AD, Alzheimer’s disease; VD, vascular dementia

Risk for incident dementia according to the status of immune-mediated diseases stratified by time since immune-mediated diseases. Time periods are overlapping. Adjusted for age, sex, education, ApoE-ε4, ethnicity, BMI, Townsend deprivation score, smoking and alcohol consumption (*p < 0.05, **p < 0.01, ***p < 0.001). ACD, all-cause dementia; AD, Alzheimer’s disease; VD, vascular dementia; HR, hazard ratio; CI, confidence interval
Individual immune-mediated diseases and dementia risk
For individual immune-mediated diseases, participants were at higher risk of developing ACD when suffering from type I diabetes mellitus (HR, 2.49; 95% CI, 1.97–3.15), rheumatic fever or rheumatic heart diseases (HR, 1.36; 95% CI, 1.05–1.77), multiple sclerosis (HR, 2.87; 95% CI, 1.92–4.30), and necrotizing vasculopathies (HR, 1.71; 95%CI, 1.03–2.85) (Fig. 3 and Supplementary Table 6). However, the effect on subtypes of dementia varies in different immune-mediated diseases. Type I diabetes mellitus was the only disease consistently related to a higher risk of both AD (HR, 2.21; 95% CI, 1.49–3.28) and VD (HR, 4.25; 95% CI, 2.90–6.23). Necrotizing vasculopathies were related to a higher incidence of AD (HR, 2.13; 95% CI, 1.06–4.27), while ulcerative colitis was related to a lower incidence of AD (HR, 0.37; 95% CI, 0.17–0.83). Rheumatic fever or rheumatic heart diseases (HR, 1.36; 95% CI, 1.05–1.77) and psoriasis (HR, 1.36; 95% CI, 1.05–1.77) were proven to be risk factors for VD. In further FDR adjusting, the Q values remained statistically significant for associations of type I diabetes mellitus with ACD, AD and VD, for multiple sclerosis with ACD, for rheumatic fever or rheumatic heart diseases and psoriasis with VD (Supplementary Table 6). Sensitivity analyses showed that the results remained significant for associations of ACD with type I diabetes mellitus and multiple sclerosis, VD with type I diabetes mellitus and rheumatic fever or rheumatic heart diseases when immune-mediated diseases occurred more than 5 or 10 years before the diagnosis of dementia (Supplementary Table 7).

Risk for incident dementia according to the status of individual immune-mediated diseases. Model 1 unadjusted. Model 2 adjusted for age, sex, ApoE-ε4, and education. Model 3 adjusted for age, sex, education, ApoE-ε4, ethnicity, BMI, Townsend deprivation score, smoking, and alcohol consumption (*p < 0.05, **p < 0.01, ***p < 0.001). ACD, all-cause dementia; AD, Alzheimer’s disease; VD, vascular dementia; HR, hazard ratio
Peripheral immune cells mediated associations of immune-mediated diseases with dementia
Mediation analyses revealed that the associations between any immune-mediated diseases and dementia was partially mediated by peripheral immune cells, including neutrophils with the proportion of mediation 5.09% (p < 0.001) and lymphocytes with the proportion of mediation 1.55% (p = 0.024) respectively (Fig. 4). As for individual immune-mediated diseases, the risk effects on dementia of type I diabetes mellitus (Supplementary Fig. 2A), multiple sclerosis (Supplementary Fig. 2B), rheumatic fever or rheumatic heart diseases (Supplementary Fig. 2C), and necrotizing vasculopathies (Supplementary Fig. 2D) were partially mediated by neutrophils while not by lymphocytes. What is more, the interaction analyses results indicated that there was an interaction between sex and peripheral immune cells in contributing to the dementia incidence (Supplementary Table 8).

Peripheral immune cells mediation models of the associations between immune-mediated diseases and dementia. Controlling for age, sex, education, ApoE-ε4, ethnicity, BMI, Townsend deprivation score, smoking, and alcohol consumption (*p < 0.05, **p < 0.01, ***p < 0.001). ACD, all-cause dementia; IE, indirect effect; DE, direct effect
Discussion
This large population-based study found that immune-mediated diseases were associated with an increased risk of dementia after adjusting for potential confounders. Among these diseases, type I diabetes mellitus was the only one promoting the higher incidence of ACD and the main subtypes of dementia. The risk of dementia was significantly high between 1 and 3 years following immune-mediated diseases onset, which might be due to reverse causality that undiagnosed dementia may increase the risk of immune-mediated diseases. Nevertheless, such associations persisted for more than 20 years that the relationships were still robust for ACD and VD. Notably, apparent sex differences were observed that females with immune-mediated diseases were more prone to AD in the early years after immune-mediated disease, while males were more susceptible to VD during a long follow-up time period. Finally, the mediation analyses revealed that the associations were partially mediated by peripheral immune cells neutrophils and lymphocytes.
To our knowledge, the current study is the most comprehensive and largest cohort study to investigate the effect of various immune-mediated diseases on dementia risk compared with previous studies. Our findings of type I diabetes mellitus are highly consistent with prior retrospective [20] and prospective [21] cohort studies which verified its risk effect on dementia even stronger than type II diabetes. Further studies indicated that poor blood glucose control [22] or severe hypoglycemic and hyperglycemic events [23] would worsen the condition. The potential mechanisms may be attributed to type I diabetes associated dementia biomarkers alterations [24] and brain atrophy [25]. As for rheumatic diseases, several retrospective studies [26,27,28,29] explored the impact of rheumatoid arthritis, Sjögren’s syndrome, and systemic lupus erythematosus on dementia, but the results were too heterogeneous to come to reliable conclusions, while none studies about rheumatic fever or rheumatic heart diseases were retrieved. The associations of multiple sclerosis and necrotizing vasculopathies with dementia risk have never been discussed. Recently, some researchers examined the associations between inflammatory bowel diseases and dementia. One of the studies utilizing the data from UKB did not find significant associations between inflammatory bowel diseases and dementia [30], which is in line with our findings. However, the other two studies reported a higher risk of dementia among inflammatory bowel diseases patients [31, 32]. Two published observational studies systemically investigated the relationships between autoimmune diseases and dementia [33, 34] yielded more positive results than ours. These discrepancies should be interpreted with caution, probably due to the residue confounding and selection bias in different cohorts and study design.
In this study, the risk of dementia was most robust in the early years after hospitalization for the immune-mediated disease. Considering that dementia reflects a late clinical stage in the continuum of disease with long prodromal period when neuropathological changes occur [35], there is possibility that the participants with a dementia diagnosis in the early follow-up years already had neurodegenerative pathology, which could cause the potential reverse causality. Hereto, we performed the sensitivity analyses by excluding the participants with follow-up time less than 5 or 10 years, and the significant associations were only observed for ACD and VD, which could be explained by the much longer disease continuum for AD. Additionally, we reported the sex differences in the associations of immune-mediated diseases with dementia. Our mediation analysis results supported that the associations were partially mediated by peripheral immune cells neutrophils and lymphocytes, and the interaction analyses results indicated that there was an interaction between sex and peripheral immune cells in contributing to the dementia incidence. These findings provide some proof for the statement that sex-specific immune activity could contribute to downstream sex differences in neurodegenerative diseases [36]. In our previous study [8], we have proved the differential role of peripheral innate and adaptive immunity in dementia incidence. The increased neutrophils were associated with higher dementia risk while the elevated lymphocytes were associated with lower dementia risk [8]. The underlined mechanisms of peripheral immunity in dementia remain unclear yet. The assumptions are that these peripheral immune cells arrive at brain in particular disease stages through damaged blood–brain barrier and contribute to abnormal pathological proteins metabolism and inflammatory responses [37,38,39].
Limitations
Our study has several limitations. Firstly, the number of dementia cases was small due to the younger, healthier and better-educated background of participants in UKB. In addition, although the positive predictive value (PPV) of ascertaining ACD cases using the UK Biobank data is high, it is lower for AD and VD [40]. Missed dementia diagnoses were still possible and the misclassification of dementia subtype was probable. Secondly, the ascertainment of immune-mediated diseases was based on HESIN data only so we may have missed some diagnoses in other conditions. We also excluded the immune-mediated diseases with less than 500 affected individuals because the dementia incidence was low in some rare immune-mediated diseases. Thirdly, there is no available data of central immune cells such as microglia or data of fluid immune biomarkers such as interleukins in UKB; hence, the mediation analyses were only performed through peripheral immune cells. Fourth, the cohort participants are predominantly European ancestry and of White ethnicity; therefore, some of our findings may not apply to all general populations. Fifth, the control comparators in our study were not totally healthy. We divided the hospital inpatient data recorded participants into two groups according to whether they were diagnosed with immune-mediated disease or not. They could be suffered from some other diseases which may cause the selection bias. Sixth, the participants with immune-mediated diseases may have a more intensive medical follow-up, thus being more likely to be diagnosed with dementia and at earlier stages, which would bias results towards an adverse association between immune-mediated diseases and incident dementia. Finally, although the follow-up time is long and we adjusted for various potential confounders, the possibility of reverse causation remains.
Conclusions
Our study suggests that immune-mediated diseases were associated with an increased risk of dementia with the risk varying according to type, sex, and timing since immune-mediated diseases. Peripheral immune cells neutrophils and lymphocytes partially mediated such associations. These findings support the importance of immune system dysregulation in dementia pathogenesis. Future studies are needed to confirm our findings in a larger cohort with a longer follow-up period, to improve our understanding of the underlined mechanisms between immune-mediated diseases and dementia, and to explore whether prevention and interventions of immune-mediated diseases reduce the risk of dementia in high-risk populations.
Availability of data and materials
All data used in this study were accessed from the publicly available UK Biobank Resource under application number 19542. These data cannot be shared with other investigators.
Abbreviations
- Aβ:
-
Amyloid β
- ACD:
-
All-cause dementia
- AD:
-
Alzheimer’s disease
- BMI:
-
Body mass index
- CBD:
-
Dementia in corticobasal degeneration
- CI:
-
Confidence interval
- DLB:
-
Dementia with Lewy bodies
- EDTA:
-
Ethylenediaminetetraacetic acid
- FDR:
-
False discovery rate
- FTD:
-
Frontotemporal dementia
- HESIN:
-
Hospital inpatient data
- HLA:
-
Human leukocyte antigen
- HR:
-
Hazard ratio
- PDD:
-
Parkinson’s disease dementia
- ICD:
-
International Classification of Diseases
- PPV:
-
Positive predictive value
- SD:
-
Standard deviation
- SNP:
-
Single-nucleotide polymorphisms
- TDP-43:
-
Transactive response DNA-binding protein 43 kDa
- TGF:
-
Transforming growth factor
- TREM2:
-
Triggering receptor expressed on myeloid cells 2
- UKB:
-
UK Biobank
- VD:
-
Vascular dementia
References
Bourdenx M, Koulakiotis NS, Sanoudou D, Bezard E, Dehay B, Tsarbopoulos A. Protein aggregation and neurodegeneration in prototypical neurodegenerative diseases: examples of amyloidopathies, tauopathies and synucleinopathies. Prog Neurobiol. 2017;155:171–93.
Wolozin B. Regulated protein aggregation: stress granules and neurodegeneration. Mol Neurodegener. 2012;7(1):1–12.
Hammond TR, Marsh SE, Stevens B. Immune signaling in neurodegeneration. Immunity. 2019;50(4):955–74.
Brigas HC, Ribeiro M, Coelho JE, Gomes R, Gomez-Murcia V, Carvalho K, et al. IL-17 triggers the onset of cognitive and synaptic deficits in early stages of Alzheimer’s disease. Cell Rep. 2021;36(9). Available from: https://pubmed.ncbi.nlm.nih.gov/34469732/. cited 2022 Jun 2
Lopez-Rodriguez AB, Hennessy E, Murray CL, Nazmi A, Delaney HJ, Healy D, et al. Acute systemic inflammation exacerbates neuroinflammation in Alzheimer’s disease: IL-1β drives amplified responses in primed astrocytes and neuronal network dysfunction. Alzheimers Dement. 2021;17(10):1735–55. Available from: https://pubmed.ncbi.nlm.nih.gov/34080771/. cited 2022 Jun 2.
Hou JH, Ou YN, Xu W, Zhang PF, Tan L, Yu JT. Association of peripheral immunity with cognition, neuroimaging, and Alzheimer’s pathology. Alzheimer’s Res Ther. 2022;14(1):1–11. Available from: https://doi.org/10.1186/s13195-022-00968-y.
Gate D, Tapp E, Leventhal O, Shahid M, Nonninger TJ, Yang AC, et al. CD4 + T cells contribute to neurodegeneration in Lewy body dementia. Science. 2021;374(6569):868–74. Available from: https://pubmed.ncbi.nlm.nih.gov/34648304/. cited 2022 Jun 2.
ZZhang YR, Wang JJ, Chen SF, Wang HF, Li YZ, Ou YN, Huang SY, Chen SD, Cheng W, Feng JF, Dong Q, Yu JT. Peripheral immunity is associated with the risk of incident dementia. Mol Psychiatry. 2022;27(4):1956-62. https://doi.org/10.1038/s41380-022-01446-5. Epub 2022 Jan 25.
Ramos-Cejudo J, Johnson AD, Beiser A, Seshadri S, Salinas J, Berger JS, et al. The neutrophil to lymphocyte ratio is associated with the risk of subsequent dementia in the Framingham Heart Study. Front Aging Neurosci. 2021;13. Available from: https://pubmed.ncbi.nlm.nih.gov/34916927/. cited 2022 Jun 2
St-Amour I, Cicchetti F, Calon F. Immunotherapies in Alzheimer’s disease: too much, too little, too late or off-target? Acta Neuropathol. 2016;131(4):481–504.
El-Gabalawy H, Guenther LC, Bernstein CN. Epidemiology of immune-mediated inflammatory diseases: Incidence, prevalence, natural history, and comorbidities. J Rheumatol. 2010;37(SUPPL. 85):2–10.
Agrawal M, Shah S, Patel A, Pinotti R, Colombel JF, Burisch J. Changing epidemiology of immune-mediated inflammatory diseases in immigrants: a systematic review of population-based studies. J Autoimmun. 2019;105(July):102303.
Broce I, Karch CM, Wen N, Fan CC, Wang Y, Hong Tan C, et al. Immune-related genetic enrichment in frontotemporal dementia: an analysis of genome-wide association studies. PLOS Med. 2018;15(1):e1002487 (Brayne C, editor).
Yokoyama JS, Wang Y, Schork AJ, Thompson WK, Karch CM, Cruchaga C, et al. Association between genetic traits for immune-mediated diseases and Alzheimer disease. JAMA Neurol. 2016;73(6):691–7.
Schett G, McInnes IB, Neurath MF. Reframing immune-mediated inflammatory diseases through signature cytokine hubs. N Engl J Med. 2021;385(7):628–39.
Sudlow C, Gallacher J, Allen N, Beral V, Burton P, Danesh J, et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015;12(3):1–10.
He MM, Lo CH, Wang K, Polychronidis G, Wang L, Zhong R, et al. Immune-mediated diseases associated with cancer risks. JAMA Oncol. 2022;8(2):209–19.
Sipilä PN, Lindbohm JV, Singh-Manoux A, Shipley MJ, Kiiskinen T, Havulinna AS, et al. Long-term risk of dementia following hospitalization due to physical diseases: a multicohort study. Alzheimers Dement. 2020;16(12):1686–95.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
Smolina K, Wotton CJ, Goldacre MJ. Risk of dementia in patients hospitalised with type 1 and type 2 diabetes in England, 1998–2011: a retrospective national record linkage cohort study. Diabetologia. 2015;58(5):942–50.
Kuo CL, Lu CL, Chang YH, Li CY. Population-based cohort study on dementia risk in patients with type 1 diabetes mellitus. Neuroepidemiology. 2018;50(1–2):57–62.
Lacy ME, Gilsanz P, Karter AJ, Quesenberry CP, Pletcher MJ, Whitmer RA. Long-term glycemic control and dementia risk in type 1 diabetes. Diabetes Care. 2018;41(11):2339–45.
Whitmer RA, Gilsanz P, Quesenberry CP, Karter AJ, Lacy ME. Association of type 1 diabetes and hypoglycemic and hyperglycemic events and risk of dementia. Neurology. 2021;97(3):e275–83.
Ouwens DM, van Duinkerken E, Schoonenboom SNM, Herzfeld de Wiza D, Klein M, van Golen L, et al. Cerebrospinal fluid levels of Alzheimer’s disease biomarkers in middle-aged patients with type 1 diabetes. Diabetologia. 2014;57(10):2208–14.
Moulton CD, Costafreda SG, Horton P, Ismail K, Fu CHY. Meta-analyses of structural regional cerebral effects in type 1 and type 2 diabetes. Brain Imaging Behav. 2015;9(4):651–62.
Lin TM, Chen WS, Sheu JJ, Chen YH, Chen JH, Chang CC. Autoimmune rheumatic diseases increase dementia risk in middle-aged patients: a nationwide cohort study. PLoS ONE. 2018;13(1):1–12.
Chen KT, Chen YC, Fan YH, Lin WX, Lin WC, Wang YH, et al. Rheumatic diseases are associated with a higher risk of dementia: a nation-wide, population-based, case-control study. Int J Rheum Dis. 2018;21(2):373–80.
Park H, Yim DH, Ochirpurev B, Eom SY, Choi IA, Ju G, et al. Association between dementia and systemic rheumatic disease: a nationwide population-based study. PLoS One. 2021;16(3 March):1–11.
Lu K, Wang HK, Yeh CC, Huang CY, Sung PS, Wang LC, et al. Association between autoimmune rheumatic diseases and the risk of dementia. Biomed Res Int. 2014;2014:861812.
Sun Y, Geng J, Chen X, Chen H, Wang X, Chen J, et al. Association between inflammatory bowel disease and dementia: a longitudinal cohort study. Inflamm Bowel Dis. 2021;80(4):1471–8.
Zingel R, Bohlken J, Kostev K. Association between inflammatory bowel disease and dementia: a retrospective cohort study. J Alzheimers Dis. 2021;80(4):1471–8.
Zhang B, Wang HE, Bai YM, Tsai SJ, Su TP, Chen TJ, et al. Inflammatory bowel disease is associated with higher dementia risk: a nationwide longitudinal study. Gut. 2021;70(1):85–91.
Goldacre MJ, Wotton CJ. Associations between specific autoimmune diseases and subsequent dementia: retrospective record-linkage cohort study, UK. J Epidemiol Community Health. 2017;71(6):576–83.
Li X, Sundquist J, Zöller B, Sundquist K. Dementia and Alzheimer’s disease risks in patients with autoimmune disorders. Geriatr Gerontol Int. 2018;18(9):1350–5.
Jack CR, Bennett DA, Blennow K, Carrillo MC, Dunn B, Haeberlein SB, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018;14(4):535–62. Available from: https://pubmed.ncbi.nlm.nih.gov/29653606/. cited 2022 Jun 6.
Lopez-Lee C, Kodama L, Gan L. Sex differences in neurodegeneration: the role of the immune system in humans. Biol Psychiatry. 2022;91(1):72–80.
Sweeney MD, Sagare AP, Zlokovic BV. Blood-brain barrier breakdown in Alzheimer disease and other neurodegenerative disorders. Nat Rev Neurol. 2018;14(3):133–50. Available from: https://pubmed.ncbi.nlm.nih.gov/29377008/. cited 2022 Jun 6.
Wu KM, Zhang YR, Huang YY, Dong Q, Tan L, Yu JT. The role of the immune system in Alzheimer’s disease. Ageing Res Rev. 2021;70. Available from: https://pubmed.ncbi.nlm.nih.gov/34273589/. cited 2022 Jun 6
Fani L, Ahmad S, Ikram MK, Ghanbari M, Ikram MA. Immunity and amyloid beta, total tau and neurofilament light chain: Findings from a community-based cohort study. Alzheimers Dement. 2021;17(3):446–56. Available from: https://pubmed.ncbi.nlm.nih.gov/33215849/. cited 2022 Jun 6.
Wilkinson T, Schnier C, Bush K, Rannikmäe K, Henshall DE, Lerpiniere C, et al. Identifying dementia outcomes in UK Biobank: a validation study of primary care, hospital admissions and mortality data. Eur J Epidemiol. 2019;34(6):557–65.
Acknowledgements
This study utilized the UK Biobank Resource under application number 19542. We would like to thank all the participants and researchers from the UK Biobank.
Funding
This study was supported by grants from the Science and Technology Innovation 2030 Major Projects (2022ZD0211600), National Natural Science Foundation of China (82071201, 82071997), Shanghai Municipal Science and Technology Major Project (2018SHZDZX01), Research Start-up Fund of Huashan Hospital (2022QD002), Excellence 2025 Talent Cultivation Program at Fudan University (3030277001), Shanghai Talent Development Funding for The Project (2019074), Shanghai Rising-Star Program (21QA1408700), 111 Project (B18015), and ZHANGJIANG LAB, Tianqiao and Chrissy Chen Institute, the State Key Laboratory of Neurobiology and Frontiers Center for Brain Science of Ministry of Education, and Shanghai Center for Brain Science and Brain-Inspired Technology, Fudan University.
Author information
Authors and Affiliations
Contributions
All authors had full access to all the data in the study and accept responsibility to submit for publication. JT Yu and YR Zhang designed the study and drafted the manuscript. L Yang, BS Wu, and HF Wang were responsible for data analyses and interpretation. YR Zhang and SY Huang accessed and verified the underlying data reported in the manuscript. JT Yu, W Cheng, and JF Feng critically revised the manuscript, and all authors approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval for the UKB study was obtained from the North West Multicenter Research Ethical Committee. All participants provided written informed-consent paper at baseline.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
The list of immune-mediated diseases and their ICD-10 codes used in the study. Supplementary Table 2. The list of dementias and their codes used in the study. Supplementary Table 3. Baseline characteristics of UKB participants by immune-mediated diseases status. Supplementary Table 4. Risk for incident dementia according to the status of any immune-mediated diseases stratified by gender. Supplementary Table 5. Sensitivity analysis of the risk for incident dementia according to the status of any immune-mediated diseases. Supplementary Table 6. FDR adjusted risk for incident dementia according to the status of individual immune-mediated diseases. Supplementary Table 7. Sensitivity analysis of the risk for incident dementia according to the status of individual immune-mediated diseases. Supplementary Table 8. The interaction analyses between sex and peripheral immune cells in contributing to the dementia incidence. Supplementary Figure 1. Flowchart of the participants selection. Supplementary Figure 2. Peripheral immune cells mediation models of the relationship between individual immune-mediated diseases and dementia.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, YR., Yang, L., Wang, HF. et al. Immune-mediated diseases are associated with a higher incidence of dementia: a prospective cohort study of 375,894 individuals. Alz Res Therapy 14, 130 (2022). https://doi.org/10.1186/s13195-022-01072-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-022-01072-x