
Abstract
Background
The hamstrings are an important muscle group that contribute to horizontal force during sprint acceleration and are also the most injured muscle group in running-based sports. Given the significant time loss associated with hamstrings injury and impaired sprinting performance following return to sport, identifying exercises that drive adaptations that are both protective of strain injury and beneficial to sprint performance is important for the strength and conditioning professional. This paper describes the study protocol investigating the effects of a 6-week training program using either the hip-dominant Romanian deadlift (RDL) or the knee-dominant Nordic hamstring exercise (NHE) on hamstring strain injury risk factors and sprint performance.
Methods
A permuted block randomized (1:1 allocation) intervention trial will be conducted involving young, physically-active men and women. A target sample size of 32 will be recruited and enrolled participants will undergo baseline testing involving extended-field-of-view ultrasound imaging and shear wave elastography of the biceps femoris long head muscle, maximal hamstrings strength testing in both the RDL and NHE, and on-field sprint performance and biomechanics. Participants will complete the 6-week training intervention using either the RDL or NHE, according to group allocation. Baseline testing will be repeated at the end of the 6-week intervention followed by 2 weeks of detraining and a final testing session. The primary outcome will be regional changes in fascicle length with secondary outcomes including pennation angle, muscle cross sectional area, hamstring strength, and maximal sprint performance and biomechanics. An exploratory aim will determine changes in shear wave velocity.
Discussion
Despite extensive research showing the benefits of the NHE on reducing hamstring strain injury risk, alternative exercises, such as the RDL, may offer similar or potentially even greater benefits. The findings of this study will aim to inform future researchers and practitioners investigating alternatives to the NHE, such as the RDL, in terms of their effectiveness in reducing rates of hamstring strain injury in larger scale prospective intervention studies.
Trial Registration
The trial is prospectively registered on ClinicalTrials.gov (NCT05455346; July 15, 2022).
Similar content being viewed by others

Background
The hamstrings muscles act to both extend the hip and flex the knee, which are particularly important movements during sprinting. The hamstrings are primary contributors to horizontal force production during both acceleration and maximal velocity phases of sprinting [1, 2] with their contribution to propulsion increasing substantially as an athlete nears maximum speed [3]. Due to the increased lengthening and high negative work done by the hamstrings during the swing phase of sprinting [4,5,6], the hamstrings are also highly susceptible to injury in running-based sports [7,8,9]. Considering the significant incidence and subsequent time loss of hamstring strain injuries (HSI) in sport [8,9,10,11,12,13,14], identifying exercises that emphasize adaptations that are both protective of strain injury and beneficial to sprint performance is important.
One exercise that has garnered a lot of attention as an effective component for HSI prevention is the Nordic hamstring exercise (NHE), which involves minimal equipment and has been integrated within injury prevention programs, such as the FIFA11+ [15, 16]. The high eccentric demand placed on the hamstrings during the exercise [17] is a potent stimulus for inducing beneficial adaptations thought to be protective of HSI. These adaptations include increased fascicle length with concurrent decreases in pennation angle, muscle hypertrophy, and increased eccentric knee flexor strength [18,19,20,21]. Additional ultrasound-derived shear wave speed (SWS)—a proxy for muscle material properties and stiffness—may also contribute to injury resiliency [22], though chronic adaptations following eccentric training have not been consistently established [23].
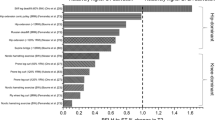
Studies using both surface electromyography (sEMG) and magnetic resonance imaging have shown the NHE preferentially recruits the semitendinosus compared to the biceps femoris—the latter of which is the more frequently injured hamstrings muscle [17, 24, 25]. One possible explanation for the preferential recruitment of the semitendinosus is that the NHE is a knee-dominant exercise, whereas studies have shown the biceps femoris muscle is more active (proportionally to the semitendinosus muscle) in hip dominant exercises, such as the 45-degree hip extension and Romanian deadlift (RDL) [17, 24, 26,27,28,29].
The NHE loads the hamstrings at relatively short muscle lengths [30,31,32,33] compared to the RDL, the latter of which can be progressively loaded throughout a greater range of motion [34, 35]. Higher neuromuscular activation was also observed in the proximal region compared to the distal region of the biceps femoris muscle during the stiff-leg deadlift – a similar exercise to the RDL [36]. Together, the higher lateral to medial hamstrings muscular activation ratio and force generation throughout longer muscle lengths induced by the RDL may increase the potential to elicit potentially beneficial adaptations in the injury-susceptible biceps femoris muscle [1,2,3,4,5,6].
Compared to its injury prevention effects, the impact of the NHE on sprint performance is less clear [37,38,39,40,41]. The implications of the RDL as it relates to improving sprint performance also have not been well-described. Sprint performance is often defined by time, but this measure provides limited information into different aspects (e.g., sprint mechanics) or phases (e.g., acceleration, transition, maximal velocity) of a sprint. Kinematics are often assessed during maximal velocity sprinting and relate to both performance and hamstrings injury susceptibility [42, 43], suggesting the importance of assessing sprint performance with other metrics than just total or split times. Simple biomechanical methods (i.e., force-velocity profiling) have been described to assess sprint kinetics during a 60 m sprint [44]. These methods may be useful in differentiating between horizontal force and maximal velocity contributions to sprint performance [2, 44,45,46,47].
Considering the hamstrings’ contribution toward horizontal force production during sprinting, the anatomical determinants that may predispose the biceps femoris muscle toward force production, and the significant stretch the biceps femoris undergoes during swing phase [1, 2, 4, 48, 49], selecting exercises that target this muscle, particularly in an eccentrically-biased manner, could prove vital for muscular adaptations for both injury risk mitigation and sprint performance. Yet, it is unclear how eccentric training, particularly with RDLs, influences sprint performance. Additionally, architectural adaptations to training interventions should be investigated along the length of the muscle to determine if changes are more pronounced in different regions [48, 50] and if these correspond to regions more susceptible to strain injury [51], such as the proximal muscle-tendon junction of the biceps femoris [52, 53].
Therefore, the purpose of the study is to investigate the effects of a 6-week training program matching volume and eccentric contraction time between the RDL and the NHE on hamstrings architecture, hamstrings strength, and sprint performance. As an exploratory aim, ultrasound shear wave speed (SWS) will also be measured along the length of the muscle to determine chronic adaptations in tissue material properties following eccentric training. Findings from this study will aim to provide evidence for targeted exercise selection in addressing HSI risk factors with potential to inform rehabilitation programming.
Methods/Design
Overall study design
This study is a randomized intervention trial where participants will be allocated to one of two experimental groups: RDL or NHE training. The primary outcome of the study is the change in regional biceps femoris fascicle length between the two intervention groups. Secondary outcomes will include ultrasound-derived changes in pennation angle, muscle thickness, anatomical cross-sectional area, in addition to hamstrings strength, and maximal sprint performance. As an exploratory aim, we will determine changes in regional SWS following training and between the two intervention groups.
The study is registered on ClinicalTrials.gov (Identifier: NCT05455346) with all procedures approved by the Health Sciences Institutional Review Board at the University of Wisconsin-Madison. Written informed consent will be obtained from all participants before inclusion by study personnel with Human Subjects Protection training. Any changes in the protocol will be reflected on the clinical registration website of ClinicalTrials.gov.
An overview of the experimental design is given in Fig. 1. Inclusion criteria for participants eligible for the intervention trial are 18–25 years of age (consistent with previous investigations [29, 47, 54]), self-report of being physically active—as defined by the Physical Activity Guidelines for Americans [55],, having > 6 months experience in resistance training, no history of HSI within the last 6 months, no history of lower extremity surgery, no current musculoskeletal injury to the lower extremity, and females not currently pregnant. Physical activity will be defined as participating in weekly totals of 150–300 min (5 h) of moderate-intensity, or 75–150 min (2 h and 30 min) of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous-intensity aerobic activity. Prior to the intervention, baseline assessments will be performed. These include regional ultrasound measures (see Ultrasound Measures); strength for the NHE and RDL (see Nordic Hamstring Exercise and Romanian Deadlift Strength Testing); and maximal 60 m sprints (see Maximum Sprint Testing). Each participant will also be asked to complete the Baecke questionnaire for determination of habitual physical activities and what current physical activities pertinent to the study in which they participate at baseline [56]. Participants will be able to continue usual levels and mode of physical activity but be asked to refrain from supplementary lower extremity resistance training and sprint-specific training.

Proposed experimental design and outcome measures at each testing time-point
An a priori power calculation using R statistical software and “WebPower” package (wp.kanova function) [57] was performed. Using an effect size based the median Cohen’s d extracted from several relevant studies investigating the effects of NHE on the primary aim of fascicle length changes [19, 21, 26, 54, 58] and converting to Cohen’s f (f = 0.8), 2 experimental groups (RDL vs. NHE), a total of 12 factors (levels of intervention x time x imaging location (proximal, mid-belly, distal) = 2 × 2 × 3), α = 0.05, and power = 0.80, a total sample size of 11 participants per group will be required. This sample size is consistent with previous investigations of fascicle length following NHE training [19, 21, 26, 54, 58]. Using a conservative effect size (Cohen’s d = 0.5) based on observed 2% differences detected in sprint times between two eccentric training interventions (Cohen’s d = 0.87) [47] and converting to Cohen’s f (f = 0.25), a total sample size of 28 (N = 14 per group) will be required for the secondary aims. Based on the larger sample size and accounting for a 10% attrition rate, a total of 16 participants per group (N = 32 in total) will be recruited from the University of Wisconsin to participate. Participants will be compensated on a pro-rated basis for completing study visits and provided their strength and sprint results.
Participants will be allocated to either the RDL or NHE training group using a random permuted block randomization (1:1 training group allocation) using a priori computer-generated group numbers. Each participant will undergo the 6-week intervention program based upon their group allocation (see Intervention). A 6-week period was chosen due to previous observations that additional changes in fascicle length (primary outcome) were minimal with NHE training lasting > 6 weeks [47, 59] and is consistent with previous investigations of architectural changes induced by NHE [54, 58]. Following the 6-week intervention, participants will return to the lab for post-intervention assessments of regional ultrasound of the hamstrings, RDL and NHE strength testing, and sprint testing, which will be carried out in the same manner as baseline assessments. Fascicle length changes are known to return to baseline values within 2 weeks after the cessation of NHE [54, 60]. To investigate the potential short-term washout effects of the training intervention on the primary and secondary outcomes, participants will be asked to return to the lab following a 2-week detraining period. During these 2 weeks, participants will be encouraged to resume all normal activities but limit any outside eccentric hamstring strength training.
Ultrasound
Participants will lay prone on an exam table with their hips and knees in a neutral position and feet off the end of the exam table. Participants will lie quietly at rest for 3 min prior to image acquisition to normalized fluid shift within the muscle [61, 62].
Ultrasound B-mode images will be collected unilaterally from the biceps femoris muscle of the dominant limb for each participant using a Logiq P9 ultrasound system (GE Healthcare, Waukesha, WI) and a linear array transducer (L3-12-RS, 47.1 mm aperture). The same researcher (SKC) will perform all image acquisitions and will be blinded to participant group allocation. The thigh length from the ischial tuberosity to the midpoint between the femoral condyles will be measured and recorded. Skin marks will be made at 33%, 50%, and 67% of the thigh length from the ischial tuberosity to standardize imaging locations between participants and correspond to approximately proximal, mid-belly, and distal regions of the hamstring muscle, respectively [63, 64].
Three longitudinal extended-field-of-view images of the entire biceps femoris muscle (i.e., from the most proximal to the most distal visualization of the muscle-tendon junctions) will be collected. According to extended-field-of-view image acquisition recommendations and previous studies [65,66,67,68,69,70,71], preliminary scans will be performed to determine the proximal and distal muscle-tendon junctions A longitudinal image will be captured along the path of the fascicle plane spanning the entire length of the biceps femoris muscle (Fig. 2).

Representative longitudinal extended-field-of-view image of the biceps femoris long head muscle with representative fascicles in the proximal, mid-belly, and distal regions (from left to right) outlined and highlighted in yellow
Three transverse extended-field-of-view images will be captured at the proximal, mid-belly, and distal locations to determine regional anatomical cross-sectional area of the biceps femoris long head muscle. The transducer will be placed perpendicular to the skin and the entire cross-sectional view of the hamstrings muscles imaged (Fig. 3) [70, 72]. A transverse image using traditional field-of-view B-mode imaging will also be captured at these locations.

Representative transverse extended-field-of-view image of the biceps femoris long head muscle (BFlh), semitendinosus (ST), and semimembranosus (SM) muscles. Anatomical cross-sectional area will be calculated from the transverse ultrasound images
To determine changes in tissue stiffness characterized by ultrasound SWS for the exploratory aim, the same transducer will be placed in the same proximal, mid-belly, and distal locations in a longitudinal view. A traditional field-of-view B-mode image will also be captured at these locations. This orientation (parallel to the muscle fascicles) has been shown to be more reliable for measuring SWS than transverse views [73, 74]. Minimal pressure will be applied to the muscle and the shear wave box (for wave speed detection) will be placed in the middle of the imaged muscle region (Fig. 4). Shear wave maps will be generated by the ultrasound system and SWS measures will be extracted from the middle of the SWS map using the measurement tools of the ultrasound system.

Representative ultrasound (A) B-mode image of the mid-belly biceps femoris long head muscle, (B) shear wave map at the same location, and (C) Q-box measures within the shear wave map with corresponding values in bottom lefthand subpanel
Nordic hamstring exercise and romanian deadlift strength testing
Hamstrings strength testing will be determined for 3 repetitions of the NHE and three-repetition maximum (3RM) in the RDL following ultrasound imaging. Prior to each test, participants will perform a standardized 5-minute general warm-up on a stationary bike followed by a task-specific warm-up including 3 sets of submaximal trials of the NHE and RDL (Additional File 1, Table A1). The RDL testing will precede the NHE for all participants with a full 15-minute rest between exercises to minimize fatigue.
The RDL will be performed in a multi-purpose, commercial power rack with a standard 20 kg Olympic barbell. Incremental load increases (5–20%) will be added for each subsequent trial until the participant cannot complete 3 repetitions through the full range of motion using proper technique. Participants will use wrist straps during the 3RM determination so maximal RDL loads will not be influenced by the participant’s grip strength. A 3 min rest will be administered between all warm-up and testing sets to allow for full recovery.
The NHE will be performed on the Nordbord (Vald Performance, Queensland, Australia), which is a reliable device to assess maximum eccentric knee flexor strength [75]. NHE testing will be performed consistent with previous investigations [2, 47, 54, 59, 60]. Participants will begin kneeled on the device in approximately 90° of flexion while their ankles are secured into fixed hooks placed superior to the lateral malleoli and oriented vertically. Participants will be asked to maintain a dorsiflexed ankle when performing the NHE [76]. Participants will cross their arms over their chest and be instructed to maintain a neutral (0° extension) hip posture while lowering their upper body to the ground as slowly as possible. They will be instructed to uncross their arms and gently catch themselves before hitting the ground if they feel their hips alignment “break” (i.e., they are unable to maintain 0° hip alignment).
Following submaximal NHE practice trials, participants will begin the maximal test, which will consist of 1 set of 3 maximal repetitions. Minimal rest (< 2 s) will be permitted between reps. If participants can control the eccentric portion of the movement towards full knee extension (i.e., not falling beyond ~ 20° knee flexion), then participants will repeat a subsequent set of 3 maximal repetitions while holding external load (5 kg increment) positioned on sternum. In the event participants need to sequentially add external load for maximum NHE testing, full recovery (3 min) will be administered between sets.
Maximum sprint testing data collection
A minimum of 15 min between strength testing and sprints will be administered. Sprints will be performed on artificial turf to minimize any effects of weather and variations in ground surface conditions on sprint performance outcomes. Prior to sprinting, participants will be weighed for subsequent sprint kinetics analysis (see Outcome Measures & Statistical Analysis) and to determine an accurate mass for proper calibration of the IMU system.
Participants will go through a standardized warm-up (Additional File, Table A2) [2, 77]. Following the warm-up, the participants will rest for 5 min to allow for placement of eight IMUs (Xsens MVN, Xsens Technologies B.V., The Netherlands) on the sternum, sacrum, and bilaterally on the thighs, legs, and foot. This system is reliable and validated to measure joint kinematics during dynamic trials and related to sprint mechanics [78,79,80]. Once the system is successfully calibrated, participants will then perform three maximal 60 m sprints.
Timing gates (SmartSpeed, Vald Performance, Queensland, Australia) will be placed at the start line (0 m), 5, 10, 20, 30, 40, 50, and 60 m. Each participant will perform a total of 3 maximal 60 m sprints from a standing position with 90 s rest in between each trial to minimize the effects of fatigue. Participants will begin with their front foot 0.5 m behind the first timing gate to prevent premature activation of the timing gates.
Intervention
All training sessions will be supervised by key study personnel with more than 4 years of exercise testing and prescription to monitor the training sessions and to keep the assessor for the primary outcome (i.e., fascicle length) blinded to the group allocation of individual participants. The key study personnel responsible for implementing the training intervention will contact each participant weekly for training sessions. A metronome (60 Hz) will be used to provide feedback for the execution of the eccentric contraction time throughout the range of motion.
Prior to each training session, participants will undergo a standardized warm-up that will include a 5 min general warm-up on a stationary bike followed by specific dynamic drills to prepare the athlete for the training session (Additional File, Table A1). The training intervention groups will undergo the same program with the only difference being the interventional hamstring exercise. The program will consist of a 2-week familiarization period followed by 4-weeks of progressive training [54]. A sample of the overall resistance training program is shown in Table 1 with each training session expected to last 45–60 min.
The hamstring-specific training will consist of the same number of repetitions performed between the RDL and the NHE. The NHE will be performed in the power rack with a pad placed under the knees and the ankles secured using the safety pins. Participants will be instructed to maintain their ankles in a dorsiflexed position, lower themselves as close to the ground as possible at a constant and controlled speed while maintaining a neutral position of the hips and trunk, and to cross their arms in front of their chest. Once an athlete reaches the ground, they will push themselves back up to the starting position while minimizing the amount of time between repetitions (< 2 s). During the familiarization period, the relative intensity will be lower compared to the 4-week progressive training to ensure each participant performs the exercise with proper technique and progressively works up to the demands of the intervention. We have observed in testing that most athletes complete the NHE in approximately 4 to 6 s [81]. This is consistent with a recent study in male field hockey players where mean (standard deviation) time to complete the NHE was 4.17 (1.14) seconds with a dorsiflexed ankle [76]. The relative intensity will be progressively increased by modifying the time to complete the NHE (from 4 to 6 s, Table 2) throughout the training period. The relative intensity during the intervention (8–9 RPE) will be maintained across the NHE by having athletes hold weight plates across their chest (as necessary). Training logs will be used to track athletes’ training loads.
The RDL will be performed in a similar manner as the 3RM testing with the barbell placed on the safety pins positioned slightly below the knee. The time to complete the eccentric portion of the RDL will be performed in a progressive manner and time-matched with the NHE (Table 2) with the athlete returning to the start position with a maximal concentric hip extension. Relative training intensity will be maintained by adding or removing resistance to the exercise. The prescribed 8–9 RPE equates to approximately 82–92% 3RM. Wrist straps will be worn during the RDL training sessions to ensure the training loads adhere to the intensity prescription and are not limited by the participant’s grip strength. The description of the interventional program is shown in Table 2. Both groups will train a total of 2 sessions per week.
Image analysis
Ultrasound images will be extracted from the ultrasound machine and analyzed offline. Using publicly available software (ImageJ, National Institutes of Health), the fascicle length, pennation angle, and muscle thickness from the extended-field-of-view and static B-mode longitudinal images will be analyzed according to previous methods [68, 69]. Anatomical cross-sectional area will be calculated from transverse images at the proximal, mid-belly, and distal locations.
Outcome measures & statistical analysis
All outcome results will be included in an anonymous database for statistical analysis. Using an intention-to-treat analysis, separate linear mixed effects models will be used to compare the effect of RDL and NHE on the primary outcome of biceps femoris long head fascicle length. Similar analyses will be performed for secondary analyses related to pennation angle, anatomical cross-sectional area, muscle thickness, and SWS. Full factorial models will be implemented with fixed effects of intervention group, muscle region, and time and a random effect to account for between-participant variation. Effect sizes will be calculated.
Sprint performance outcomes will be summarized using descriptive statistics. Given that the expected changes in sprint performance are numerically small but may still represent meaningful changes in overall sport performance and improvement, we will set a priori thresholds to describe the magnitude of change. Small, medium and large improvements in sprint times will be defined as < 2%, 2–4%, and > 4%, respectively, based off changes in 40 m sprint times observed previously [47, 82].
Discrete kinematic variables will be summarized using descriptive statistics and compared between time points for the maximal sprint using linear mixed effects models [83]. Due to the continuous time series data extracted from the IMUs, statistical parametric mapping (SPM) will also be used to determine any within-participant changes in kinematics throughout the entire sprint. SPM allows for the analysis of the entire time series and has been used in a variety of biomechanical studies [84,85,86]. Specifically, within-subject differences in trunk, hip, knee, and ankle kinematics will be calculated between test sessions
As an additional description of sprint performance, we will characterize the horizontal force production as detailed by Samozino et al. and adapted by others [1, 47, 87]. Descriptions of the theoretical maximal horizontal force (F0), velocity (v0), and maximal power output (Pmax) will be derived from participants’ split times and each participant’s body mass according to previous works [44, 88]. Intervention assessments for each variable across each time point will be compared using linear mixed effects models and R software [89, 90]
Discussion
Although much research has been dedicated to identifying the etiology and mechanisms of injury, potential risk factors, residual neuromuscular deficits, and evidence-based recommendations for rehabilitation protocols of HSI [4, 6, 10, 13, 18, 91,92,93,94,95,96,97,98,99,100,101,102], the incidence and injury burden of HSI have not improved [14, 103]. The NHE is a staple in injury prevention programs for HSI, but evidence suggests adherence is a major limitation in its effectiveness for reducing HSI [104,105,106,107]. Due to the high rate of injury within the proximal muscle-tendon junction of the biceps femoris and non-uniform muscular adaptation to resistance training, different exercises should be employed to target specific muscle regions and increase eccentric training adherence [52, 53, 108, 109]
Consistent eccentric hamstring strength training (specifically using the NHE) increases eccentric knee flexor strength and influences architectural adaptations thought to be protective of HSI—such as increased fascicle length with concurrent decreases in pennation angle [47, 50, 54, 59, 60, 97, 110]. Fascicle length, pennation angle, and muscle thickness are typically measured using ultrasonography at the mid-belly [2, 47, 54, 59, 60], but this does not account for the known variation in architecture along the length of the hamstrings muscles [48, 49, 111, 112] or the non-uniform lengthening, activation, and adaptations induced by resistance training [113,114,115,116]. Recent evidence indicated that changes in fascicle and sarcomere lengths only occur in the distal region of the biceps femoris muscle following NHE training [50]. This coincides with higher neuromuscular activation in the distal region compared to the proximal and middle regions of the biceps femoris muscle during the NHE [117]. Our proposed investigation aims to determine if hip-dominant (RDL) or knee-dominant (NHE) eccentric hamstring exercises influence regional differences in fascicle length adaptations
Although ultrasonography is typically used to characterize architectural adaptations following eccentric exercise training, some ultrasound systems have capabilities that can provide insight into characterizing tissue material properties. Shear wave imaging has been shown to be a reliable, non-invasive, quantitative technique to characterize tissue stiffness in both tendon [118,119,120] and muscle [74, 121, 122]. Ultrasound elastography-derived shear modulus (derived from the SWS) has also been related to both passive and active muscular force production [123] as well as isometric rate of torque development in the gastrocnemius muscle [124]. Therefore, SWS may relate to both sprint performance and injury resiliency, but chronic adaptations following eccentric training have not been consistently established [23]. As an exploratory aim, we will measure regional SWS in the biceps femoris muscle to determine any chronic adaptations in tissue material properties following eccentric strength training
Resistance training, specifically eccentric training, has shown positive effects for both injury prevention and athletic performance. Despite extensive research showing the benefits of the NHE on reducing HSI risk [125], there is ongoing debate whether alternative exercises, such as the RDL, may offer similar or potentially even greater benefits. This is particularly debated with respect to the biceps femoris muscle, which is most frequently injured and appears to be more proportionally targeted in hip extension versus knee flexion exercises [17, 25, 26, 29, 52, 53]. While it is acknowledged that interventions aimed at hamstring injury prevention and improving sprint performance should be multi-faceted, comparing two commonly prescribed exercises like the NHE and RDL allows practitioners to prescribe hamstring exercises in an evidence-based manner with descriptions of the underlying muscular adaptations and implications for sprint performance improvements. The methods and proposed sprint analyses will allow for a comprehensive view of the effects of both the NHE and RDL on sprint mechanics through force-velocity profiling and kinematic changes throughout key phases of the sprint
The findings from this proposed study have practical applications for strength and conditioning coaches, athletic trainers, and physical therapists to address HSI risk factors and sprint performance through targeted exercise selections. In addition to providing information for evidence-based hamstring exercise selection, it is hoped that the findings of this study also inform future research projects aimed at investigating alternatives to the NHE, such as the RDL, in terms of their effectiveness in reducing rates of HSI in larger scale prospective intervention studies
Data Availability
The anonymized dataset used for analysis will be made available from the corresponding author upon reasonable request.
References
Morin JB, Gimenez P, Edouard P, Arnal P, Jiménez-Reyes P, Samozino P et al. Sprint acceleration mechanics: The major role of hamstrings in horizontal force production. Front Physiol. 2015;6 DEC:404.
Prince C, Morin J-B, Mendiguchia J, Lahti J, Guex K, Edouard P, et al. Sprint specificity of isolated hamstring-strengthening exercises in terms of muscle activity and force production. Front Sport Act Living. 2021;2:609636.
Pandy MG, Lai AKM, Schache AG, Lin YC. How muscles maximize performance in accelerated sprinting. Scand J Med Sci Sport. 2021;31:1882–96.
Thelen DG, Chumanov ES, Hoerth DM, Best TM, Swanson SC, Li L, et al. Hamstring muscle kinematics during treadmill sprinting. Med Sci Sports Exerc. 2005;37:108–14.
Thelen DG, Chumanov ES, Best TM, Swanson SC, Heiderscheit BC. Simulation of biceps femoris musculotendon mechanics during the swing phase of sprinting. Med Sci Sport Exerc. 2005;37:1931–8.
Chumanov ES, Heiderscheit BC, Thelen DG. Hamstring musculotendon dynamics during stance and swing phases of high-speed running. Med Sci Sport Exerc. 2011;43:525–32.
van der Made AD, Almusa E, Whiteley R, Hamilton B, Eirale C, van Hellemondt F, et al. Intramuscular tendon involvement on MRI has limited value for predicting time to return to play following acute hamstring injury. Br J Sports Med. 2018;52:83–8.
Ekstrand J, Hägglund M, Waldén M. Epidemiology of muscle injuries in Professional Football (Soccer). Am J Sports Med. 2011;39:1226–32.
Dalton SL, Kerr ZY, Dompier TP. Epidemiology of hamstring strains in 25 NCAA Sports in the 2009–2010 to 2013–2014 academic years. Am J Sports Med. 2015;43:2671–9.
Mack CD, Kent RW, Coughlin MJ, Shiue KY, Weiss LJ, Jastifer JR, et al. Incidence of Lower Extremity Injury in the National Football League: 2015 to 2018. Am J Sports Med. 2020;48:2287–94.
Dompier TP, Powell JW, Barron MJ, Moore MT. Time-loss and non-time-loss injuries in youth football players. J Athl Train. 2007;42:395–402.
Feeley BT, Kennelly S, Barnes RP, Muller MS, Kelly BT, Rodeo SA, et al. Epidemiology of national football league training camp injuries from 1998 to 2007. Am J Sports Med. 2008;36:1597–603.
Okoroha KR, Conte S, Makhni EC, Lizzio VA, Camp CL, Li B et al. Hamstring Injury Trends in Major and Minor League Baseball: epidemiological findings from the Major League Baseball Health and Injury Tracking System. Orthop J Sport Med. 2019;7.
Ekstrand J, Bengtsson H, Waldén M, Davison M, Khan KM, Hägglund M. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA Elite Club Injury Study from 2001/02 to 2021/22. Br J Sports Med. 2022;Published.
Nouni-Garcia R, Carratala-Munuera C, Orozco-Beltran D, Lopez-Pineda A, Asensio-Garcia MR, Gil-Guillen VF. Clinical benefit of the FIFA 11 programme for the prevention of hamstring and lateral ankle ligament injuries among amateur soccer players. Inj Prev. 2018;24:149–54.
Thorborg K, Krommes KK, Esteve E, Clausen MB, Bartels EM, Rathleff MS. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11 + programmes. Br J Sports Med. 2017;51:562–71.
Bourne MN, Williams MD, Opar DA, Al Najjar A, Kerr GK, Shield AJ. Impact of exercise selection on hamstring muscle activation. Br J Sports Med. 2017;51:1021–8.
Medeiros DM, Marchiori C, Baroni BM. Effect of nordic Hamstring Exercise training on knee flexors eccentric strength and fascicle length: a systematic review and Meta-analysis. J Sport Rehabil. 2020;30:482–91.
Ribeiro-Alvares JB, Marques VB, Vaz MA, Baroni BM. Four weeks of nordic hamstring exercise reduce muscle injury risk factors in young adults. J Strength Cond Res. 2018;32:1254–62.
Behan FP, Vermeulen R, Whiteley R, Timmins RG, Ruddy JD, Opar DA. The dose-response of the nordic Hamstring Exercise on Biceps Femoris Architecture and eccentric knee flexor strength: a Randomized Interventional Trial. Int J Sports Physiol Perform. 2022;17:646–54.
Severo-Silveira L, Dornelles MP, Lima-E-Silva FX, Marchiori CL, Medeiros TM, Pappas E, et al. Progressive workload periodization maximizes Effects of Nordic Hamstring Exercise on muscle Injury Risk factors. J strength Cond Res. 2021;35:1006–13.
Miyamoto N, Hirata K, Miyamoto-Mikami E, Yasuda O, Kanehisa H. Associations of passive muscle stiffness, muscle stretch tolerance, and muscle slack angle with range of motion: individual and sex differences. Sci Rep. 2018;8:8274.
Dankel SJ, Razzano BM. The impact of acute and chronic resistance exercise on muscle stiffness: a systematic review and meta-analysis. J Ultrasound. 2020;23:473–80.
Suarez-Arrones L, Núñez FJ, Lara-Lopez P, Di Salvo V, Méndez-Villanueva A. Inertial flywheel knee- and hip-dominant hamstring strength exercises in professional soccer players: muscle use and velocity-based (mechanical) eccentric overload. PLoS ONE. 2020;15:e0239977.
Ekstrand J, Lee JC, Healy JC. MRI findings and return to play in football: a prospective analysis of 255 hamstring injuries in the UEFA Elite Club Injury Study. Br J Sports Med. 2016;50:738–43.
Bourne MN, Duhig SJ, Timmins RG, Williams MD, Opar DA, Al Najjar A, et al. Impact of the nordic hamstring and hip extension exercises on hamstring architecture and morphology: implications for injury prevention. Br J Sports Med. 2017;51:469–77.
Boyer A, Hug F, Avrillon S, Lacourpaille L. Individual differences in the distribution of activation among the hamstring muscle heads during stiff-leg deadlift and nordic hamstring exercises. J Sports Sci. 2021;39:1830–7.
Ono T, Higashihara A, Fukubayashi T. Hamstring functions during hip-extension exercise assessed with electromyography and magnetic resonance imaging. Res Sport Med. 2011;19:42–52.
Carmichael DS, Hickey JT, Tofari PJ, Bourne MN, Ward MR, Timmins RG. Effect of an isometric or eccentric hip extension Exercise intervention on Hamstring Strength, Architecture, and morphology. Med Sci Sport Exerc. 2022;54:2196–207.
Sconce E, Heller B, Maden-Wilkinson T, Hamilton N. Development of a Novel Nordic Hamstring Exercise device to measure and modify the knee flexors’ torque-length relationship. Front Sport Act Living. 2021;0:40.
Ditroilo M, De Vito G, Delahunt E. Kinematic and electromyographic analysis of the nordic Hamstring Exercise. J Electromyogr Kinesiol. 2013;23:1111–8.
Šarabon N, Marušič J, Marković G, Kozinc Ž. Kinematic and electromyographic analysis of variations in nordic hamstring exercise. PLoS ONE. 2019;14:e0223437.
Miralles-Iborra A, Elvira JLL, Urban T, Calado A, Del Coso J, Moreno-Pérez V. Agreement between isokinetic eccentric hamstring strength, nordic hamstring strength and nordic break-point angle in a sample of trained and healthy individuals. Eur J Sport Sci. 2021.
Rajic S, Legg HS, Maurus P, Nigg SR, Cleather DJ. The Effects of a 9-Week hip focused Weight Training Program on hip and knee kinematics and kinetics in experienced female dancers. J Hum Kinet. 2020;75:29.
Villanueva MG, Lane CJ, Schroeder ET. Short rest interval lengths between sets optimally enhance body composition and performance with 8 weeks of strength resistance training in older men. Eur J Appl Physiol. 2015;115:295–308.
Schoenfeld BJ, Contreras B, Tiryaki-Sonmez G, Wilson JM, Kolber MJ, Peterson MD. Regional differences in muscle activation during hamstrings exercise. J Strength Cond Res. 2015;29:159–64.
Bautista IJ, Vicente-Mampel J, Baraja-Vegas L, Segarra V, Martín F, Van Hooren B. The effects of the nordic hamstring exercise on sprint performance and eccentric knee flexor strength: a systematic review and meta-analysis of intervention studies among team sport players. J Sci Med Sport. 2021;24:931–8.
Ishøi L, Hölmich P, Aagaard P, Thorborg K, Bandholm T, Serner A. Effects of the nordic hamstring exercise on sprint capacity in male football players: a randomized controlled trial. J Sports Sci. 2018;36:1663–72.
Markovic G, Sarabon N, Boban F, Zoric I, Jelcic M, Sos K, et al. Nordic hamstring strength of highly trained Youth Football Players and its relation to Sprint Performance. J strength Cond Res. 2020;34:800–7.
Suarez-Arrones L, Lara-Lopez P, Rodriguez-Sanchez P, Lazaro-Ramirez JL, Salvo V, Di, Guitart M, et al. Dissociation between changes in sprinting performance and nordic hamstring strength in professional male football players. PLoS ONE. 2019;14:e0213375.
Raya-González J, Torres Martin L, Beato M, Rodríguez-Fernández A, Sanchez-Sanchez J. The effects of training based on nordic hamstring and sprint exercises on measures of physical fitness and hamstring injury prevention in U19 male soccer players. Res Sport Med. 2021.
Alt T, Komnik I, Severin J, Nodler YT, Benker R, Knicker AJ, et al. Swing phase mechanics of maximal velocity Sprints-Does isokinetic Lower-Limb muscle strength matter? Int J Sports Physiol Perform. 2021;16:974–84.
Kenneally-Dabrowski C, Brown NAT, Warmenhoven J, Serpell BG, Perriman D, Lai AKM, et al. Late swing running mechanics influence hamstring injury susceptibility in elite rugby athletes: a prospective exploratory analysis. J Biomech. 2019;92:112–9.
Samozino P, Rabita G, Dorel S, Slawinski J, Peyrot N, Saez de Villarreal E, et al. A simple method for measuring power, force, velocity properties, and mechanical effectiveness in sprint running. Scand J Med Sci Sports. 2016;26:648–58.
Mendiguchia J, Edouard P, Samozino P, Brughelli M, Cross M, Ross A, et al. Field monitoring of sprinting power–force–velocity profile before, during and after hamstring injury: two case reports. J Sports Sci. 2016;34:535–41.
Mendiguchia J, Samozino P, Martinez-Ruiz E, Brughelli M, Schmikli S, Morin JB, et al. Progression of mechanical properties during on-field sprint running after returning to sports from a hamstring muscle injury in soccer players. Int J Sports Med. 2014;35:690–5.
Timmins RG, Filopoulos D, Nguyen V, Giannakis J, Ruddy JD, Hickey JT, et al. Sprinting, strength, and architectural adaptations following hamstring training in australian footballers. Scand J Med Sci Sports. 2021;31:1276–89.
Kellis E, Galanis N, Natsis K, Kapetanos G. Muscle architecture variations along the human semitendinosus and biceps femoris (long head) length. J Electromyogr Kinesiol. 2010;20:1237–43.
Kellis E, Galanis N, Kapetanos G, Natsis K. Architectural differences between the hamstring muscles. J Electromyogr Kinesiol. 2012;22:520–6.
Pincheira PA, Boswell MA, Franchi MV, Delp SL, Lichtwark GA. Biceps femoris long head sarcomere and fascicle length adaptations after 3 weeks of eccentric exercise training. J Sport Heal Sci. 2021.
Malliaropoulos N, Papacostas E, Kiritsi O, Papalada A, Gougoulias N, Maffulli N. Posterior thigh muscle injuries in elite track and field athletes. Am J Sports Med. 2010;38:1813–9.
De Smet AA, Best TM. MR imaging of the distribution and location of acute hamstring injuries in athletes. Am J Roentgenol. 2000;174:393–9.
Koulouris G, Connell D. Evaluation of the hamstring muscle complex following acute injury. Skeletal Radiol. 2003;32:582–9.
Presland JD, Timmins RG, Bourne MN, Williams MD, Opar DA. The effect of nordic hamstring exercise training volume on biceps femoris long head architectural adaptation. Scand J Med Sci Sport. 2018;28:1775–83.
US Department of Health and Human Services. Physical Activity Guidelines for Americans. 2nd edition. Washington, D.C.; 2018.
Baecke JAH, Burema J, Frijters JER. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr. 1982;36:936–42.
Zhang Z, Yuan K-H. Practical statistical power analysis using WebPower and R. ISDSA Press; 2018.
Seymore KD, Domire ZJ, Devita P, Rider PM, Kulas AS. The effect of nordic hamstring strength training on muscle architecture, stiffness, and strength. Eur J Appl Physiol. 2017;117:943–53.
Pollard CW, Opar DA, Williams MD, Bourne MN, Timmins RG. Razor hamstring curl and nordic hamstring exercise architectural adaptations: impact of exercise selection and intensity. Scand J Med Sci Sport. 2019;29:706–15.
Timmins RG, Ruddy JD, Presland J, Maniar N, Shield AJ, Williams MD, et al. Architectural changes of the Biceps Femoris Long head after concentric or eccentric training. Med Sci Sports Exerc. 2016;48:499–508.
Palmer TB, Akehi K, Thiele RM, Smith DB, Thompson BJ. Reliability of panoramic Ultrasound Imaging in simultaneously examining muscle size and quality of the hamstring muscles in Young, healthy males and females. Ultrasound Med Biol. 2015;41:675–84.
Freitas SR, Marmeleira J, Valamatos MJ, Blazevich A, Mil-Homens P. Ultrasonographic Measurement of the Biceps Femoris Long-Head muscle Architecture. J Ultrasound Med. 2018;37:977–86.
Crawford SK, Lee KS, Bashford GR, Heiderscheit BC. Intra-session and inter-rater reliability of spatial frequency analysis methods in skeletal muscle. PLoS ONE. 2020;15:e0235924.
Crawford SK, Lee KS, Bashford GR, Heiderscheit BC. Spatial-frequency analysis of the anatomical differences in hamstring muscles. Ultrason Imaging. 2021;43:100–8.
Adkins AN, Murray WM. Obtaining quality extended field-of-view ultrasound images of skeletal muscle to measure muscle fascicle length. J Vis Exp. 2020;2020:1–16.
Adkins AN, Franks PW, Murray WM. Demonstration of extended field-of-view ultrasound’s potential to increase the pool of muscles for which in vivo fascicle length is measurable. J Biomech. 2017;63:179–85.
Elliott ST. A user guide to Extended Field of View in Ultrasonography. Ultrasound. 2006;14:55–8.
Ando R, Nosaka K, Inami T, Tomita A, Watanabe K, Blazevich AJ, et al. Difference in fascicle behaviors between superficial and deep quadriceps muscles during isometric contractions. Muscle Nerve. 2016;53:797–802.
Ando R, Nosaka K, Tomita A, Watanabe K, Blazevich AJ, Akima H. Vastus intermedius vs vastus lateralis fascicle behaviors during maximal concentric and eccentric contractions. Scand J Med Sci Sport. 2018;28:1018–26.
Franchi MV, Raiteri BJ, Longo S, Sinha S, Narici MV, Csapo R. Muscle Architecture Assessment: strengths, shortcomings and new frontiers of in vivo imaging techniques. Ultrasound Med Biol. 2018;44:2492–504.
Noorkoiv M, Stavnsbo A, Aagaard P, Blazevich AJ. In vivo assessment of muscle fascicle length by extended field-of-view ultrasonography. J Appl Physiol. 2010;109:1974–9.
Noorkoiv M, Nosaka K, Blazevich AJ. Assessment of quadriceps muscle cross-sectional area by ultrasound extended-field-of-view imaging. Eur J Appl Physiol. 2010;109:631–9.
Alfuraih AM, O’Connor P, Tan AL, Hensor E, Emery P, Wakefield RJ. An investigation into the variability between different shear wave elastography systems in muscle. Med Ultrason. 2017;19.
Dorado Cortez C, Hermitte L, Ramain A, Mesmann C, Lefort T, Pialat JB. Ultrasound shear wave velocity in skeletal muscle: a reproducibility study. Diagn Interv Imaging. 2016;97:71–9.
Opar DA, Piatkowski T, Williams MD, Shield AJ. A novel device using the nordic hamstring exercise to assess eccentric knee flexor strength: a reliability and retrospective injury study. J Orthop Sports Phys Ther. 2013;43:636–40.
Vicente-Mampel J, Bautista IJ, Martín F, Maroto-Izquierdo S, Van Hooren B, Baraja-Vegas L. Effects of ankle position during the nordic hamstring exercise on range of motion, heel contact force and hamstring muscle activation. Sport Biomech. 2022;:1–13.
Mendiguchia J, Conceição F, Edouard P, Fonseca M, Pereira R, Lopes H, et al. Sprint versus isolated eccentric training: comparative effects on hamstring architecture and performance in soccer players. PLoS ONE. 2020;15:e0228283.
Setuain I, Lecumberri P, Ahtiainen JP, Mero AA, Häkkinen K, Izquierdo M. Sprint mechanics evaluation using inertial sensor-based technology: a laboratory validation study. Scand J Med Sci Sport. 2018;28:463–72.
Horenstein RE, Lewis CL, Yan S, Halverstadt A, Shefelbine SJ. Validation of magneto-inertial measuring units for measuring hip joint angles. J Biomech. 2019;91:170–4.
Cottam DS, Campbell AC, Davey MPC, Kent P, Elliott BC, Alderson JA. Measurement of uni-planar and sport specific trunk motion using magneto-inertial measurement units: the concurrent validity of Noraxon and Xsens systems relative to a retro-reflective system. Gait Posture. 2022;92:129–34.
Wille CM, Stiffler-Joachim MR, Kliethermes SA, Sanfilippo JL, Tanaka CS, Heiderscheit BC. Preseason eccentric strength is not Associated with Hamstring strain Injury: a prospective study in Collegiate athletes. Med Sci Sports Exerc. 2022;54.
Freeman BW, Young WB, Talpey SW, Smyth AM, Pane CL, Carlon TA. The effects of sprint training and the nordic hamstring exercise on eccentric hamstring strength and sprint performance in adolescent athletes. J Sports Med Phys Fitness. 2019;59:1119–25.
Wilmes E, DE Ruiter CJ, Bastiaansen BJC, Goedhart EA, Brink MS, Helm VANDER. Associations between hamstring fatigue and Sprint Kinematics during a simulated football (Soccer) Match. Med Sci Sports Exerc. 2021;53:2586–95.
Dutaillis B, Opar DA, Pataky T, Timmins RG, Hickey JT, Maniar N. Trunk, pelvis and lower limb coordination between anticipated and unanticipated sidestep cutting in females. Gait Posture. 2021;85:131–7.
Honert EC, Pataky TC. Timing of gait events affects whole trajectory analyses: a statistical parametric mapping sensitivity analysis of lower limb biomechanics. J Biomech. 2021;119:110329.
Schuermans J, Van Tiggelen D, Palmans T, Danneels L, Witvrouw E. Deviating running kinematics and hamstring injury susceptibility in male soccer players: cause or consequence? Gait Posture. 2017;57:270–7.
Samozino P, Edouard P, Sangnier S, Brughelli M, Gimenez P, Morin J-B. Force-velocity profile: imbalance determination and effect on lower limb ballistic performance. Int J Sports Med. 2014;35:505–10.
Morin JB, Samozino P, Murata M, Cross MR, Nagahara R. A simple method for computing sprint acceleration kinetics from running velocity data: replication study with improved design. J Biomech. 2019;94:82–7.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing; 2021.
Wilkinson RD, Mazzo MR, Feeney DF. Rethinking the statistical analysis of Neuromechanical Data. Exerc Sport Sci Rev. 2023;51.
Diemer WM, Winters M, Tol JL, Pas HIMFL, Moen MH. Incidence of Acute Hamstring Injuries in Soccer: a systematic review of 13 studies involving more than 3800 athletes with 2 million Sport exposure hours. J Orthop Sports Phys Ther. 2021;51:27–36.
Silder A, Sherry MA, Sanfilippo J, Tuite MJ, Hetzel SJ, Heiderscheit BC. Clinical and morphological changes following 2 Rehabilitation Programs for Acute Hamstring strain injuries: a Randomized Clinical Trial. J Orthop Sport Phys Ther. 2013;43:284–99.
Sherry MA, Best TM. A comparison of 2 rehabilitation programs in the treatment of acute hamstring strains. J Orthop Sport Phys Ther. 2004;34:116–25.
Green B, Bourne MN, Van Dyk N, Pizzari T. Recalibrating the risk of hamstring strain injury (HSI): a 2020 systematic review and meta-analysis of risk factors for index and recurrent hamstring strain injury in sport. Br J Sports Med. 2020;54:1081–8.
Thelen DG, Chumanov ES, Sherry MA, Heiderscheit BC. Neuromusculoskeletal models provide insights into the Mechanisms and Rehabilitation of hamstring strains. Exerc Sport Sci Rev. 2006;34:135–41.
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sport Med. 2012;42:209–26.
Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016;50:1524–35.
Hickey JT, Timmins RG, Maniar N, Williams MD, Opar DA. Criteria for Progressing Rehabilitation and determining return-to-play clearance following hamstring strain Injury: a systematic review. Sport Med. 2017;47:1375–87.
Chumanov ES, Heiderscheit BC, Thelen DG. The effect of speed and influence of individual muscles on hamstring mechanics during the swing phase of sprinting. J Biomech. 2007;40:3555–62.
Liu H, Garrett WE, Moorman CT, Yu B. Injury rate, mechanism, and risk factors of hamstring strain injuries in sports: a review of the literature. J Sport Heal Sci. 2012;1:92–101.
Bahr R, Clarsen B, Ekstrand J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med. 2018;52:1018–21.
Heiderscheit BC, Sherry M, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J Orthop Sports Phys Ther. 2010;40:67–81.
Ekstrand J, Spreco A, Bengtsson H, Bahr R. Injury rates decreased in men’s professional football: an 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br J Sports Med. 2021;55:1084–92.
McCall A, Dupont G, Ekstrand J. Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA Elite Club Injury Study teams: a survey of teams’ head medical officers. Br J Sports Med. 2016;50:725–30.
Bahr R, Thorborg K, Ekstrand J. Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or norwegian Premier League football teams: the nordic hamstring survey. Br J Sports Med. 2015;49:1466–71.
Ekstrand J, Healy JC, Waldén M, Lee JC, English B, Hägglund M. Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br J Sports Med. 2012;46:112–7.
Ekstrand J, Bengtsson H, Walden M, Davison M, Hagglund M. Still poorly adopted in male professional football: but teams that used the nordic Hamstring Exercise in team training had fewer hamstring injuries - a retrospective survey of 17 teams of the UEFA Elite Club Injury Study during the 2020–2021 season. BMJ open Sport Exerc Med. 2022;8.
Schoenfeld BJ. The mechanisms of muscle hypertrophy and their application to resistance training. 2010.
Zabaleta-Korta A, Fernández-Peña E, Torres-Unda J, Garbisu-Hualde A, Santos-Concejero J. The role of exercise selection in regional muscle hypertrophy: a randomized controlled trial. J Sports Sci. 2021;39:2298–304.
Brooks JHM, Fuller CW, Kemp SPT, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34:1297–306.
Tosovic D, Muirhead JC, Brown JMM, Woodley SJ. Anatomy of the long head of biceps femoris: an ultrasound study. Clin Anat. 2016;29:738–45.
Woodley SJ, Mercer SR. Hamstring muscles: Architecture and innervation. Cells Tissues Organs. 2005;179:125–41.
Ema R, Wakahara T, Miyamoto N, Kanehisa H, Kawakami Y. Inhomogeneous architectural changes of the quadriceps femoris induced by resistance training. Eur J Appl Physiol. 2013;113:2691–703.
Wakahara T, Fukutani A, Kawakami Y, Yanai T. Nonuniform muscle hypertrophy: its relation to muscle activation in training session. Med Sci Sports Exerc. 2013;45:2158–65.
Narici MV, Hoppeler H, Kayser B, Landoni L, Claassen H, Gavardi C, et al. Human quadriceps cross-sectional area, torque and neural activation during 6 months strength training. Acta Physiol Scand. 1996;157:175–86.
Bennett HJ, Rider PM, Domire ZJ, DeVita P, Kulas AS. Heterogeneous fascicle behavior within the biceps femoris long head at different muscle activation levels. J Biomech. 2014;47:3050–5.
Hegyi A, Péter A, Finni T, Cronin NJ. Region-dependent hamstrings activity in nordic hamstring exercise and stiff-leg deadlift defined with high-density electromyography. Scand J Med Sci Sport. 2018;28:992–1000.
Peltz CD, Haladik JA, Divine G, Siegal D, Van Holsbeeck M, Bey MJ. ShearWave elastography: repeatability for measurement of tendon stiffness. Skeletal Radiol. 2013;42:1151–6.
Dirrichs T, Schrading S, Gatz M, Tingart M, Kuhl CK, Quack V. Shear Wave Elastography (SWE) of asymptomatic Achilles Tendons: a comparison between Semiprofessional athletes and the Nonathletic General Population. Acad Radiol. 2019;26:1345–51.
Payne C, Watt P, Cercignani M, Webborn N. Reproducibility of shear wave elastography measures of the Achilles tendon. Skeletal Radiol. 2018;47:779–84.
Šarabon N, Kozinc Ž, Podrekar N. Using shear-wave elastography in skeletal muscle: a repeatability and reproducibility study on biceps femoris muscle. PLoS ONE. 2019;14:e0222008.
Mendes B, Firmino T, Oliveira R, Neto T, Infante J, Vaz JR, et al. Hamstring stiffness pattern during contraction in healthy individuals: analysis by ultrasound-based shear wave elastography. Eur J Appl Physiol. 2018;118:2403–15.
Hug F, Tucker K, Gennisson JL, Tanter M, Nordez A. Elastography for muscle biomechanics: toward the estimation of individual muscle force. Exerc Sport Sci Rev. 2015;43:125–33.
Ando R, Suzuki Y. Positive relationship between passive muscle stiffness and rapid force production. Hum Mov Sci. 2019;66:285–91.
Van Dyk N, Behan FP, Whiteley R. Including the nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: a systematic review and meta-analysis of 8459 athletes. Br J Sports Med. 2019;53:1362–70.
Acknowledgements
Not applicable.
Funding
Support for this research was provided by the Office of the Vice Chancellor for Research and Graduate Education at the University of Wisconsin –Madison with funding from the Wisconsin Alumni Research Foundation (SKC). The authors would also like to thank the Marsh Center for Exercise and Movement Research for the generous support of this work. The funders had no role in the design and conduct of the study, nor the decision to prepare and submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
SKC and JH conceived the idea of the study. SKC, JH, and BH drafted the first version of the manuscript. JV, JSC, and SJM provided critical feedback to the manuscript and study design. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
List of abbreviations
HSI = hamstring strain injury, IMU = inertial measurement unit, NHE = Nordic hamstring exercise, RDL = Romanian deadlift, SPM = statistical parametric mapping, SWS = shear wave speed.
Ethics approval and consent to participate
The study will be conducted in accordance with the Declaration of Helsinki. This study is approved by the Institutional Review Board of the University of Wisconsin Madison (Protocol ID: 2022 − 0763) and the trial prospectively registered on ClinicalTrials.gov (NCT05455346; July 15, 2022). Written informed consent will be obtained from all participants before inclusion. Study participation is voluntary.
Consent for publication
Written informed consent was obtained from individuals who served as models in the images used in this publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.

Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Crawford, S.K., Hickey, J., Vlisides, J. et al. The effects of hip- vs. knee-dominant hamstring exercise on biceps femoris morphology, strength, and sprint performance: a randomized intervention trial protocol. BMC Sports Sci Med Rehabil 15, 72 (2023). https://doi.org/10.1186/s13102-023-00680-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-023-00680-w