
Abstract
Background
Exercise tolerance plays a vital role in the process of cardiac rehabilitation in patients undergoing percutaneous coronary intervention (PCI). The study sought to determine the characteristics, risks and correlates of post-PCI exercise tolerance in patients with coronary artery disease (CAD).
Methods
We analyzed clinical data of 299 CAD patients undergoing elective PCI and completing cardiopulmonary exercise testing (CPET). According to the Weber classification, post-PCI exercise tolerance was evaluated by peak oxygen uptake (VO2 peak). We assessed the impact of 34 predefined clinical features, cardiac functional parameters, and blood biochemistry data on exercise tolerance by univariate analysis and logistics regression analysis.
Results
Of 299 patients, 74.92% were men and average age was 60.90 ± 10.68 years. VO2 peak in the entire population was 17.54 ± 3.38 ml/kg/min, and 24.41% (n = 73) were less than 16 ml/kg/min, who were considered to have exercise intolerance. Multivariate logistics regression results showed that sex, diabetes mellitus, number of stents, left atrial diameter (LAD), end-diastolic volume (EDV), and hemoglobin influenced the peak oxygen uptake of CAD patients undergoing elective PCI. (All p < 0.05).
Conclusions
Nearly one quarter of CAD patients have exercise intolerance in the early post-PCI period. Female, diabetes mellitus, number of stents, LAD, EDV might negatively impacted post-PCI exercise tolerance, which need further warrant by large scale cohort study.
Similar content being viewed by others

Introduction
Coronary artery disease (CAD) is the leading cause of mortality and loss of disability worldwide [1]. Patients with CAD suffers significant symptoms of ischemia and hypoxia, due to the insufficient coronary flow and pressure that rise to meet the demands of physical activity. Percutaneous coronary intervention (PCI) is the priority treatment for CAD patients because it can rapidly unblock the infarct-related artery, restore myocardial perfusion, and reduce the infarct size [2, 3]. Even though, CAD patients undergoing PCI might experience symptomatic complications overtime, such as dyspnea, palpitations, dizziness on exertion. Evidence from epidemiological survey demonstrated that over half of post-PCI patients with the confession of exercise intolerance or muscular fatigue often get overlooked in clinical setting [4, 5].
Exercise tolerance [6, 7] referred to the maximum aerobic exercise capacity that can be tolerated without morbid symptoms and/or medical signs, and represents the body’s ability to absorb oxygen. Peak oxygen uptake (VO2 peak), measured during the cardiopulmonary exercise test (CPET), is the body’s maximum capacity to deliver and utilize oxygen, and is also the gold standard for assessment of exercise tolerance [8]. It can predict reinfarction and all-cause death in CAD patients and was used for prognosis assessment [9,10,11]. Previous studies [12,13,14] have reported that factors contributing to exercise tolerance include age, sex, body mass index (BMI), fasting blood glucose, ejection fraction, as well as nephropathy and peripheral arterial disease, etc. However, few existing researches have focused on the exercise tolerance status among PCI patients.
We hypothesized that, in addition to demographic and disease factors, measures of cardiac function and blood biochemistry would predict exercise tolerance. The identification of predictors of exercise tolerance may help improve future study designs by revealing confounding variables, as well as providing a theoretical basis for future cardiac rehabilitation schemes for patients. Therefore, this study aimed to describe the current status of exercise tolerance as well as to identify its predictors in CAD patients undergoing PCI.
Methods
Participants
The study population consisted of CAD patients undergoing elective PCI for stable angina from January 2019 to December 2020. All subjects complete a maximal symptom limited, incremental CPET 1 month after PCI. Patients without contraindications were routinely treated with secondary prevention drugs such as dual antiplatelet agents, statins, angiotensin-converting enzyme inhibitors (ACEI)/angiotensin receptor blocker (ARB) and β-blockers postoperatively. Patients were excluded from this study if they met any of the following: (1) combination of other major systemic diseases, such as mid- to late-stage tumors, liver disease, renal disease and pulmonary impairment; (2) incomplete medical records; (3) presence of contraindications to CPET, including unstable angina, acute myocardial infarction 3–5 days, arrhythmias associated with unstable hemodynamic disturbances, active myocarditis or pericarditis, aortic stenosis, heart failure or pulmonary embolism, unstable lower extremity venous thrombosis, moderate to severe asthma, in the acute phase of infection, suffering from abnormal psychiatric symptoms or physical disability.
Interventional procedure
All patients provided explicit written informed consent prior to undergoing cardiac catheterization. Antiplatelet therapy was given to all patients before PCI with a specific regimen of Aspirin 100 mg once daily and Clopidogrel 75 mg once daily (or Tegretol 90 mg twice daily). Glycoprotein IIb/IIIa inhibitors were administered during the procedure and immediately after PCI, at the surgeon's discretion. The choice of coronary stent type and other adjuvant therapy is at the discretion of the primary surgeon, with a complete shift to drug-eluting stents in recent years. All stents were implanted at moderate to high deployment pressures (12–16 atm). Routine anticoagulation with low molecular heparin was continued postoperatively.
Measurements
Sociodemographic characteristics, medical and medication history, CPET parameters, echocardiographic parameters, and laboratory data were collected from participants’ medical records and interviews. The investigation conforms to the principles outlined in the Declaration of Helsinki [15]. The study was reviewed and approved by the Human Study Committee of Shanghai Seventh People’s Hospital (Registration No. 2021-7th-HIRB-012), and informed consent was formally obtained from each participant.
Cardiopulmonary exercise testing
Maximal symptom limited, incremental CPET was performed using cycle ergometers (Quark PFT Ergo, COSMED, Rome, Germany) with a ramp protocol [16, 17]. Before the test begins, the clinician will conduct a comprehensive evaluation and formulate an appropriate exercise increment plan for the patient. The exercise protocol started with a 3-min resting phase on the cycle ergometer, followed by a 3-min warm-up phase at 20-Watt initial workloads. Then, workload was set at 35 Watt followed by an increase of 10–30 Watt increments per min at pedaling speed > 60 rpm until the patient has exhaustion or restrictive symptoms or signs [18], e.g., reaching the submaximal heart rate; respiratory exchange rate (RER) ≥ 1.0; electrocardiogram ST segment changes, etc. The following recovery phase consisted of 2-min active recovery at 20 Watt at pedalling speed between 50 and 60 rpm, followed by 3-min passive recovery.
During the whole test process, clinicians pay attention to monitoring the patient’s real-time ECG, blood pressure, gas exchange parameters, etc. The test was terminated when the subject showed one of the following conditions: (1) chest pain, dyspnea, pallor, weakness, dizziness, lower extremity pain, or unsteadiness in standing and requested to terminate; (2) ECG suggestive of myocardial ischemia; (3) II- or III-degree atrioventricular block; (4) systolic blood pressure decreased > 20 mmHg; (5) hypertension: systolic blood pressure > 250 mmHg; diastolic blood pressure > 120 mmHg; (6) rating of perceived exertion (RPE) up to Borg 19–20.
CPET core indicators such as VO2 peak, oxygen uptake efficiency slope (OUES), ventilatory efficiency (VE/VCO2) slope, etc. were measured. According to the Weber classification [19], VO2 peak < 16 ml/kg/min was considered to have objective exercise intolerance.
Echocardiographic examination
A Vivid E9 Color Doppler Ultrasound System with a 3.4 MHz transducer (GE Ultrasound, Horten, Norway) was used to conduct standard transthoracic 2D echocardiography. Exploring the parasternal long-axis view of the left ventricle can measure the thickness of the interventricular septum (IVST), the end-diastolic diameter of the left ventricle (LVDd), the end-systolic diameter of the left ventricle (LVDs), and the left atrial diameter (LAD). In the apical four-chamber view and the two-chamber view, the left ventricular ejection fraction (LVEF) was calculated using the Simpson formula. Pulse-Doppler can detect the blood flow spectrum of the mitral valve in the apical four chambers, and measure the double peaks of the mitral valve during diastole. The images generated by the echocardiography are all gathered and kept in the instrument's hard disk by two qualified cardiology fellows.
Laboratory testing
All measurements were performed in a central laboratory. Blood hemoglobin and platelet were automatically assessed using high-volume hematology analyzer Siemens Advia 2120 (Siemens Healthcare Diagnostics, Deerfield, IL, USA). Homocysteine, serum creatinine (Scr), uric acid (UA), and lipid profile [blood total cholesterol (TC), triglyceride concentrations (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C)] were automatically assessed on Roche Cobas 8000 (Roche Diagnostics International Ltd, Rotkreuz, Switzerland).
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences ver. 24.0 (SPSS Inc., Chicago, IL, USA). One-sample K–S normality tests were performed on the measurement data. Normally distributed data were expressed as Mean ± SD and compared using the independent samples t-test; skewed data were expressed as median (interquartile range) and compared using the Mann–Whitney U test. The categorical variables were described as number of cases, and comparisons were performed by Chi-squared or Fisher analysis. The level of statistical significance was set at a p-value less than 0.05.
One-dimensional linear regression was used to assess the correlation between VO2 peak/Kg and selected variables. Logistic regression was performed to investigate significant predictors to identify exercise intolerance. The independent variables relevant to the logistic regression model were selected from the univariate analysis of demographic and procedural characteristics and clinical indicators, based on a threshold p-value of 0.05.
Results
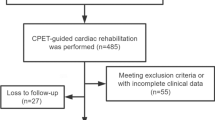
We finally recruited 299 consecutive post-PCI patients. Figure 1 presents the flow diagram for the recruitment and analysis. Demographic and procedural characteristics were summarized in Table 1. Of the 299 patients, 74.92% were male and the average age was 60.90 ± 10.69 years. The most frequent comorbidity was hypertension (88.63%), followed by dyslipidemia (73.24%) and diabetes mellitus (24.75%). The comparison between the two groups indicated that sex, BMI, number of stents, prevalence of dyslipidemia, and diabetes mellitus were statistically significant. No significant difference in drug categories and lesion vessel were observed between groups.

CONSORT diagram of study recruitment. PCI percutaneous coronary intervention, LVEF Left ventricular ejection fraction, CPET Cardiopulmonary exercise testing
Six patients were limited by musculoskeletal pain and failed to complete the CPET protocol and achieve a maximal effort. All remaining 299 subjects who completed CPET had no major cardiac events, ischemic ECG changes or sustained ventricular arrhythmias during the testing period. VO2 peak in the entire population was 17.54 ± 3.38 ml/kg/min, and 24.41% (n = 73) were less than 16 ml/kg/min, considered to have objective exercise intolerance. The distribution of VO2 peak is shown in Fig. 2, and the remaining core indicators of CPET were listed in Additional file 1: Table S1. In contrast, patients in exercise intolerance group were more likely to have decreased peak heart rate, VO2 peak, METs, and OUES, whereas VE/VCO2 slope and HRR Max showed increasing trend.

Distribution of peak oxygen consumption (VO2 peak/Kg) among entire cohort
Table 2 shows the differences in clinical features. In terms of transthoracic echocardiographic variables, LAD and EDV were higher in exercise intolerance group. As for blood biochemistry data, hemoglobin was 138.10 ± 14.13 g/l in the overall population and higher in normal exercise tolerance group. (All p < 0.001).
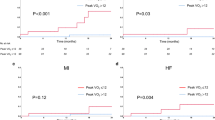
The linear regression plots between BMI, LAD, EDV, hemoglobin and VO2 peak/Kg were shown in Fig. 3. VO2 peak/Kg was inversely related to BMI (r = − 0.174, p = 0.003), LAD (r = − 0.206, p < 0.001) and EDV (r = − 0.135, p = 0.019), whereas it was positively correlated with hemoglobin (r = 0.268, p < 0.001). Furthermore, logistic regression models were performed to identify exercise intolerance, as presented in Table 3. Although dyslipidemia showed a trend towards an adverse effect on exercise capacity, it did not reach statistical significance (p = 0.054). Increased BMI (OR = 1.128, p = 0.003) was significantly associated with exercise intolerance in the univariate regression analysis; however, this association did not persist in the multivariate regression. Stepwise multivariate logistic analyses revealed that the number of stents (OR = 4.078, p < 0.001), diabetes mellitus (OR = 2.138, p = 0.027), LAD (OR = 1.173, p < 0.001), and EDV (OR = 1.199, p = 0.003) were linked to a higher risk of exercise intolerance, while being male (OR = 0.328, p = 0.003) and having a higher hemoglobin content (OR = 0.705, p = 0.006) were protective factors against exercise intolerance.

Regression plots between VO2 peak/Kg, BMI, LAD, EDV and hemoglobin. BMI Body mass index, LAD Left atrial diameter, EDV End-diastolic volume
Discussion
The VO2 peak is the most objective and reliable indicator to measure exercise tolerance in CAD patients [20, 21]. In our study, the average VO2 peak was found to be 17.54 ± 3.38 ml/kg/min, with nearly a quarter of the patients (73 cases, 24.41%) experiencing post-PCI cardiopulmonary dysfunction. These results suggest that even if coronary revascularization is successfully completed, exercise tolerance in the early postoperative period does not return swiftly to the normal level, which is in line with the findings of Li et al. [5]. Although PCI can improve symptoms of myocardial ischemia, myocardial contractile function and cardiac compliance remain abnormal in the early stages, resulting in reduced cardiac output and delayed recovery of exercise tolerance. Additionally, patients may opt not to exercise or exercise less due to concerns about wounds or myocardial infarction, or because they lack professional and scientific exercise planning guidance, all of which contributes to a lack of improvement in exercise tolerance in the early stages.
Our study found that men and patients with higher hemoglobin levels had better post-PCI exercise tolerance. As noted by Kodama et al. [22], men have higher cardiorespiratory fitness values, about 2 METs higher, compared to women of the same age. This disparity can be attributed to differences in anatomy and physiology, such as: (1) Women having smaller left ventricles and lower ejection volumes[23]; (2) Lower left ventricular diastolic compliance in women [24]; (3) A higher proportion of obesity in women [23]; (4) Women being more prone to iron deficiency and having lower hemoglobin levels compared to men [25, 26]. Hemoglobin is a main marker of anemia and a primary performer of red blood cell function, responsible for transporting and carrying oxygen and carbon dioxide within the red blood cells. Decreased hemoglobin levels can result in a further deterioration of the hemodynamic state. In addition, aging in elderly patients leads to an increase in underlying diseases, weakens the body's immune function, and makes them more prone to recurrent infections, all of which exacerbates the decline in post-PCI exercise tolerance.
Diabetes mellitus is a separate risk factor. According to Gürdal et al. [27], the VO2 peak and anaerobic threshold of diabetic patients were significantly lower than those in healthy adults. Plausibility of this mechanism is strengthened by several pathological pathways, such as microvascular disease, energy metabolism disorders, and autonomic dysfunction, which are independent of hypertension and coronary artery disease. These pathological changes result in ventricular diastolic dysfunction and impaired heart rate recovery, thereby impacting exercise tolerance [28,29,30,31].
With more stents implanted, CAD patients are at a higher risk of postoperative exercise intolerance, which is consistent with the findings of the SYNTAX trial [32]. The number of stents and the total length of the stents implanted are important indicators of the complexity of the coronary lesions and play a crucial role in predicting the clinical outcomes of patients undergoing PCI [33]. Studies have shown that an excessive number of stents can increase the damage to the endothelium during the procedure, exacerbating the local inflammatory response of the endothelium undergoing PCI [34, 35], which can trigger symptoms of exercise limitation.
LAD and EDV have been proposed as a morphophysiological marker of ventricular dysfunction. This study found that increased LAD and EDV are also risk factors for postoperative exercise intolerance in CAD patients. Previous research has shown that when ventricular dysfunction occurs, diastolic filling pressure increases, ventricular compliance decreases, left atrial pressure increases, pulmonary vein and capillary wedge pressure increases, and pulmonary ventilation perfusion is impaired. These changes result in elevated VE/VCO2, insufficient left ventricular filling, reduced cardiac output, shortness of breath during exertion, and decreased exercise tolerance [4, 36,37,38].
Interestingly, LVEF, a commonly used indicator, does not seem to predict exercise tolerance. One reason is that post-PCI patients with LVEF less than 50% are usually considered temporarily unfit for CPET and therefore do not have data for analysis in this study. On the other hand, the relationship between exercise capacity and LVEF may be impacted by diverse comorbidities, and various compensatory mechanisms can help preserve exercise ability [39]. Smart et al. [40] found that rest LVEF was weakly correlated with peak oxygen uptake, which was more closely related to a composite model filling pressure, systolic and diastolic function.
Patients with CAD tend to be sedentary undergoing PCI [41], which may lead to cardiorespiratory deconditioning as well as muscle atrophy and weakness that in turn leads to deterioration in metabolic, cardiorespiratory, and functional health. However, increasing physical activity through comprehensive cardiac rehabilitation can improve exercise tolerance and quality of life in these patients [42,43,44]. Meta-analyses reported that endurance and resistance training together increased peak oxygen uptake and 6-min walk test distance by 2.2 ml/kg/min and 33 m, respectively [45, 46]. It has been noted that an increase in cardiorespiratory fitness is associated with a reduction in the risk of all-cause mortality and cardiovascular mortality [22]. Thus, it is imperative that medical staff provide early exercise guidance and health education to CAD patients undergoing PCI, and offer personalized exercise rehabilitation programs to enhance their post-PCI exercise tolerance.
Limitations
As an observational study, it has a limited number of included cases and may have problems such as selection bias. It is necessary to further expand the sample size for prospective study design. Enrollment was limited by the prescription of CPET, patients who could not tolerate CPET were not included in the study, and patients with more severe disease were excluded. None of the included patients discontinued β-blockers during CPET, which had a certain impact on the study results. Compared with the treadmill exercise program, the peak oxygen uptake for cycle ergometer exercise program was reduced by about 10–20%, so the result of the CPET index was low.
Conclusions
Our main finding revealed that nearly a quarter (73 cases, 24.41%) of CAD patients have exercise intolerance in the early post-PCI period. Sex, the number of stents, diabetes mellitus, LAD, EDV and hemoglobin were identified as independent factors contributing to exercise intolerance. It is recommended to further explore a comprehensive cardiac rehabilitation model including exercise rehabilitation, symptom management and weight management, in order to improve the post-PCI exercise tolerance and relieve postoperative discomfort of CAD patients.
Availability of data and materials
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- ACEI:
-
Angiotensin-converting enzyme inhibitors
- ARB:
-
Angiotensin receptor blocker
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- CI:
-
Confidence interval
- CPET:
-
Cardiopulmonary exercise test
- HDL-C:
-
High-density lipoprotein cholesterol
- IVST:
-
Interventricular septum
- LAD:
-
Left atrial diameter
- LDL-C:
-
Low-density lipoprotein cholesterol
- LVDd:
-
End-diastolic diameter of the left ventricle
- LVDs:
-
End-systolic diameter of the left ventricle
- LVEF:
-
Left ventricular ejection fraction
- OR:
-
Odds ratio
- OUES:
-
Oxygen uptake efficiency slope
- PCI:
-
Percutaneous coronary intervention
- RER:
-
Respiratory exchange rate
- RPE:
-
Rating of perceived exertion
- Scr:
-
Serum creatinine
- TC:
-
Total cholesterol
- TG:
-
Triglyceride concentrations
- UA:
-
Uric acid
- VE/VCO2 slope:
-
Ventilatory efficiency slope
- VO2 peak:
-
Peak oxygen uptake
References
GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–71.
Neumann F-J, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165.
Cook CM, Ahmad Y, Howard JP, Shun-Shin MJ, Sethi A, Clesham GJ, et al. Impact of percutaneous revascularization on exercise hemodynamics in patients with stable coronary disease. J Am Coll Cardiol. 2018;72:970–83.
Tashiro H, Tanaka A, Ishii H, Motomura N, Arai K, Adachi T, et al. Reduced exercise capacity and clinical outcomes following acute myocardial infarction. Heart Vessels. 2020;35:1044–50.
Li Y, Feng X, Chen B, Liu H. Retrospective analysis of exercise capacity in patients with coronary artery disease after percutaneous coronary intervention or coronary artery bypass graft. Int J Nurs Sci. 2021;8:257–63.
Ross R, Blair SN, Arena R, Church TS, Després J-P, Franklin BA, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart association. Circulation. 2016;134:e653–99.
Valeur N. The prognostic value of pre-discharge exercise testing after myocardial infarction treated with either primary PCI or fibrinolysis: a DANAMI-2 sub-study. Eur Heart J. 2004;26:119–27.
Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;2019:140.
Forman DE, Arena R, Boxer R, Dolansky MA, Eng JJ, Fleg JL, et al. Prioritizing functional capacity as a principal end point for therapies oriented to older adults with cardiovascular disease: a scientific statement for healthcare professionals from the American heart association. Circulation. 2017;135:e894–918.
Hung RK, Al-Mallah MH, McEvoy JW, Whelton SP, Blumenthal RS, Nasir K, et al. Prognostic value of exercise capacity in patients with coronary artery disease: the FIT (Henry ford exercise testing) project. Mayo Clin Proc. 2014;89:1644–54.
Cai H, Zheng Y, Liu Z, Zhang X, Li R, Shao W, et al. Effect of pre-discharge cardiopulmonary fitness on outcomes in patients with ST-elevation myocardial infarction after percutaneous coronary intervention. BMC Cardiovasc Disord. 2019;19:210.
Fuller A, Okwose N, Scragg J, Eggett C, Luke P, Bandali A, et al. The effect of age on mechanisms of exercise tolerance: Reduced arteriovenous oxygen difference causes lower oxygen consumption in older people. Exp Gerontol. 2021;149:111340.
Marchionni N, Fattirolli F, Fumagalli S, Oldridge NB, Del Lungo F, Bonechi F, et al. Determinants of exercise tolerance after acute myocardial infarction in older persons. J Am Geriatr Soc. 2000;48:146–53.
Haykowsky MJ, Tomczak CR, Scott JM, Paterson DI, Kitzman DW. Determinants of exercise intolerance in patients with heart failure and reduced or preserved ejection fraction. J Appl Physiol. 2015;119:739–44.
World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA. 2013;310:2191.
Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al. Exercise standards for testing and training: a scientific statement from the American heart association. Circulation. 2013;128:873–934.
Guiraud T, Juneau M, Nigam A, Gayda M, Meyer P, Mekary S, et al. Optimization of high intensity interval exercise in coronary heart disease. Eur J Appl Physiol. 2010;108:733–40.
American Thoracic Society. ATS/ACCP statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;2003(167):211–77.
19. Writing Committee, EACPR, Guazzi M, Adams V, Conraads V, Halle M, et al. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Eur Heart J. 2012;33:2917–27.
Al-Mallah MH, Sakr S, Al-Qunaibet A. Cardiorespiratory fitness and cardiovascular disease prevention: an update. Curr Atheroscler Rep. 2018;20:1.
Kubozono T, Itoh H, Oikawa K, Tajima A, Maeda T, Aizawa T, et al. Peak VO2 is more potent Than B-type natriuretic peptide as a prognostic parameter in cardiac patients. Circ J. 2007;72:575–81.
Kodama S. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301:2024.
Beale AL, Meyer P, Marwick TH, Lam CSP, Kaye DM. Sex differences in cardiovascular pathophysiology: why women are overrepresented in heart failure with preserved ejection fraction. Circulation. 2018;138:198–205.
Redfield MM, Jacobsen SJ, Borlaug BA, Rodeheffer RJ, Kass DA. Age- and gender-related ventricular-vascular stiffening: a community-based study. Circulation. 2005;112:2254–62.
van der Wal HH, Grote Beverborg N, Dickstein K, Anker SD, Lang CC, Ng LL, et al. Iron deficiency in worsening heart failure is associated with reduced estimated protein intake, fluid retention, inflammation, and antiplatelet use. Eur Heart J. 2019;40:3616–25.
Martens P, Nijst P, Verbrugge FH, Smeets K, Dupont M, Mullens W. Impact of iron deficiency on exercise capacity and outcome in heart failure with reduced, mid-range and preserved ejection fraction. Acta Cardiol. 2018;73:115–23.
Gürdal A, Kasikcioglu E, Yakal S, Bugra Z. Impact of diabetes and diastolic dysfunction on exercise capacity in normotensive patients without coronary artery disease. Diab Vasc Dis Res. 2015;12:181–8.
Leenders M, Verdijk LB, van der Hoeven L, Adam JJ, van Kranenburg J, Nilwik R, et al. Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. J Am Med Dir Assoc. 2013;14:585–92.
Fang ZY, Sharman J, Prins JB, Marwick TH. Determinants of exercise capacity in patients with type 2 diabetes. Diabetes Care. 2005;28:1643–8.
Poirier P, Bogaty P, Garneau C, Marois L, Dumesnil J-G. Diastolic dysfunction in normotensive men with well-controlled Type 2 diabetes. Diabetes Care. 2001;24:5–10.
Carnethon MR, Jacobs DR, Sidney S, Liu K. Influence of autonomic nervous system dysfunction on the development of type 2 diabetes. Diabetes Care. 2003;26:3035–41.
Serruys PW, Morice M-C, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–72.
Généreux P, Giustino G, Redfors B, Palmerini T, Witzenbichler B, Weisz G, et al. Impact of percutaneous coronary intervention extent, complexity and platelet reactivity on outcomes after drug-eluting stent implantation. Int J Cardiol. 2018;268:61–7.
Koskinas KC, Chatzizisis YS, Antoniadis AP, Giannoglou GD. Role of endothelial shear stress in stent restenosis and thrombosis. J Am Coll Cardiol. 2012;59:1337–49.
Ellis SG. Refining the art and science of coronary stenting. N Engl J Med. 2009;360:292–4.
Left GJ, Function V, Capacity E. Left ventricular function and exercise capacity. JAMA. 2009;301:286.
Edelmann F, Gelbrich G, Düngen H-D, Fröhling S, Wachter R, Stahrenberg R, et al. Exercise training improves exercise capacity and diastolic function in patients with heart failure with preserved ejection fraction. J Am Coll Cardiol. 2011;58:1780–91.
Hsiao C-S, Hsiao S-H. Relationship of left atrial expansion index to exercise tolerance, pretest probability of restenosis, and positive predictive value of treadmill test in coronary artery disease. Echocardiography. 2020;37:388–98.
Tsougos E, Angelidis G, Gialafos E, Tzavara C, Tzifos V, Tsougos I, et al. Myocardial strain may predict exercise tolerance in patients with reduced and mid-range ejection fraction. Hellenic J Cardiol. 2018;59:331–5.
Smart N, Haluska B, Leano R, Case C, Mottram PM, Marwick TH. Determinants of functional capacity in patients with chronic heart failure: role of filling pressure and systolic and diastolic function. Am Heart J. 2005;149:152–8.
Charman SJ, van Hees VT, Quinn L, Dunford JR, Bawamia B, Veerasamy M, et al. The effect of percutaneous coronary intervention on habitual physical activity in older patients. BMC Cardiovasc Disord. 2016;16:248.
Swift DL, Lavie CJ, Johannsen NM, Arena R, Earnest CP, O’Keefe JH, et al. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ J. 2013;77:281–92.
Franklin BA, Lavie CJ, Squires RW, Milani RV. Exercise-based cardiac rehabilitation and improvements in cardiorespiratory fitness: implications regarding patient benefit. Mayo Clin Proc. 2013;88:431–7.
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee I-M, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–59.
Fukuta H, Goto T, Wakami K, Kamiya T, Ohte N. Effects of exercise training on cardiac function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials. Heart Fail Rev. 2019;24:535–47.
Ismail H, McFarlane JR, Nojoumian AH, Dieberg G, Smart NA. Clinical outcomes and cardiovascular responses to different exercise training intensities in patients with heart failure. JACC: Heart Fail. 2013;1:514–22.
Acknowledgements
This study was supported by Shanghai Seventh People’s Hospital affiliated to Shanghai University of Traditional Chinese Medicine. We appreciate the data support and research assistance provided by the hospital's information center and medical examination center.
Funding
The study was funded by the Discipline Leaders Training Program of Pudong New District Health Bureau (Program No. PWRd2020-07) to Prof. Xubo Wu and the Scientific Research Project of Shanghai Municipal Health Commission (Project No. 202150051) to Prof. Jing Wu, respectively.
Author information
Authors and Affiliations
Contributions
Conceptualization, LHS and WJ; Data curation, WMQ, ZLL, WYY and WJQ; Formal analysis, LHS; Funding acquisition, WXB; Investigation, LHS, WMQ and ZLL; Methodology, LHS, HL and WJ; Project administration, WMQ, ZSW and WJ; Resources, ZSW and WXB; Software, LHS; Supervision, WXB; Validation, HL and WJ; Visualization, LHS; Writing—original draft, LHS; Writing—review and editing, WXB and WJ. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The investigation conforms to the principles outlined in the Declaration of Helsinki. The study was reviewed and approved by the Human Study Committee of Shanghai Seventh People’s Hospital (Registration No. 2021-7th-HIRB-012), and informed consent was formally obtained from each participant.
Consent for publication
Not applicable.
Competing interests
The authors declare that they do not have a conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Table S1: Comparison of CPET core indicators.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, H., Wei, M., Zhang, L. et al. Factors contributing to exercise tolerance in patients with coronary artery disease undergoing percutaneous coronary intervention. BMC Sports Sci Med Rehabil 15, 35 (2023). https://doi.org/10.1186/s13102-023-00640-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-023-00640-4