
Abstract
Objective
The research was aimed to evaluate the subclinical left ventricular (LV) myocardial systolic dysfunction in T2DM patients with or without hypertension (HT) by global and segmental myocardial work (MW).
Methods
A total of 120 T2DM patients (including 60 T2DM patients with HT) and 70 sex- and age- matched normal controls were included. The global and segmental variables of work index (WI), constrictive work (CW), waste work (WW), work efficiency (WE), and CW/WW were analysed by non-invasive pressure-strain loop. Receiver operating characteristic (ROC) analysis was performed for detection the subclinical LV systolic dysfunction in T2DM patients with and without HT.
Results
The global work index (GWI), global CW (GCW), global WE (GWE), and GCW/global WW (GWW) of T2DM and T2DM patients with HT were significantly lower than normal controls (p < 0.05). The WI, CW, WE, and CW/WW of the LV anterior wall in T2DM and T2DM patients with HT were significantly lower when compared with those of the normal controls (p < 0.05). ROC analysis showed that the value of area under the curve (AUC) in combined GWI, GCW, GWE, and GCW/GWW was significantly higher than the AUCs of the individual indices (p < 0.05).
Conclusions
MW can non-invasively and accurately evaluate subclinical global and segmental LV myocardial systolic dysfunction in T2DM patients with and without HT. Regulating total cholesterol levels and controlling blood pressure in T2DM patients with and without HT might reduce the impairment of LV myocardial systolic function.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
With the growth of the population and increased longevity, non-infectious chronic diseases (NCDs) are still the main causes of poor health worldwide. In a report released by the World Health Organization in 2022 [1], as one of the most common NCDs, type 2 diabetes mellitus (T2DM) has shown an increasing trend in both incidence and mortality over the last 20 years. Cardiovascular complications are viewed as dangerous complications of T2DM culminating in death [2]. Although ischaemic events dominate cardiovascular complications, in the absence of myocardial ischaemia and conditions of hypertension, diabetic cardiomyopathy also carries an increased risk of progression to heart failure [3]. In previous studies in which left ventricular (LV) global longitudinal strain (GLS) was measured using speckle-tracking echocardiography (STE), patients with T2DM who developed myocardial dysfunction could be identified even when LV ejection fraction (LVEF) was preserved [4, 5]. The acquisition of LV global radial, circumferential, and longitudinal strain by cardiovascular magnetic resonance (CMR) tissue tracking also enables the evaluation of myocardial systolic function in T2DM patients [6]. Due to the high cost and time-consuming nature of CMR, as well as LVGLS is excessively load dependent. Therefore, their ability to serve as accurate, widely used indicators of myocardial systolic function is limited [7, 8].
Myocardial work (MW) estimation has been validated as a novel, non-invasive method for constructing the LV pressure-strain loop (PSL) area, with good correlation with directly measured MW, and it is able to reflect the systolic and metabolic capacity of the myocardium [9, 10]. Previously, several studies have shown that the global myocardial work index (GWI) is significantly impaired in T2DM patients compared with normal controls [5, 11]. Nevertheless, subclinical LV myocardial systolic dysfunction has not been evaluated in T2DM patients with hypertension (HT), and whether there is LV segmental myocardial impairment in T2DM patients is unknown. Therefore, the aims of the present study were to (1) evaluate subclinical global and segmental LV myocardial systolic dysfunction by MW in T2DM patients with and without HT, (2) evaluate the influences of patients' clinical indices on myocardial systolic function, and (3) evaluate the sensitivity and specificity of MW in evaluating subclinical LV myocardial systolic dysfunction in T2DM patients with and without hypertension (HT).
Methods
Study population
The study population included 165 T2DM patients who had already been diagnosed or were diagnosed during hospitalization and 83 T2DM patients who were simultaneously diagnosed with HT or had a history of HT. The diagnostic criteria for T2DM conformed to the latest guidelines [12]: A1C ≥ 6.5%, fasting plasma glucose (FPG) ≥ 126 mg/dl (7.0 mmol/L), 2-h plasma glucose ≥ 200 mg/dl (11.1 mmol/L) during an oral glucose tolerance test (OGTT) or random plasma glucose ≥ 200 mg/dl (11.1 mmol/L) + typical hyperglycaemia symptoms. The diagnosis of hypertension followed the standards of the European Society of Cardiology [13]: systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg on two separate occasions or regular antihypertensive treatment. According to their clinical status, T2DM patients with (1) valvular disease, (2) arrhythmia, (3) cardiomyopathy, (4) previous or current ischemic events, (5) poor image quality, were excluded. Furthermore, 70 sex- and age-matched normal individuals were recruited as normal controls (Fig. 1). The study adhered to the guidelines of the Declaration of Helsinki. Approval was obtained from the human research and ethics committee of Changzhou Second People's Hospital Affiliated to Nanjing Medical University, and all patients provided complete informed consent.

Flow chart of participant screening for the study cohort
Conventional echocardiography
An ultrasound machine (Vivid E9; GE Vingmed Ultrasound, Horten, Norway) was used by senior sonographers to perform standard 2-dimensional transthoracic echocardiography. 40–60 frames of standard images in three cardiac cycles at the apical two-, three- and four- chamber views were collected, and the electrocardiogram was connected while images were collected. Proprietary software (EchoPAC 203; GE Vingmed Ultrasound) was used to store images and perform offline analysis.
Left atrium diameter (LAd), interventricular septum thickness diameters (IVSd), LV diameter (LVd) and LV posterior wall thickness diameters (LVPWd) were measured from the parasternal long-axis views in the end-diastole period [14].Maximal left atrial volume was measured from apical four- and two-chamber views, and correction of body surface area (BSA) differences between individuals was performed using the left atrial volume (LAV) index. Peak mitral valve medial flow velocity (E) and lateral annulus flow velocity (e′) in the early diastolic period were measured using the Doppler technique in the apical four-chamber view [15]. At the same time, the peak late diastolic annular velocity (A) was measured.
The displacement waveform of the mitral annulus during systole was measured from M-mode echocardiography in apical four-chamber views, with the distance between the peak point and the nadir as the magnitude of the mitral annular plane systolic excursion (MAPSE) [16]. LV end-systolic volume (LVESV), LV end-diastolic volume (LVEDV) and LVEF were measured by the biplane Simpson method [14]. Correction of BSA differences between individuals was executed using the LVESV and LVEDV indexes.
Myocardial work
The image analysis in this study was usually performed offline by two senior sonographers using EchoPAC 203. The regions of interest were automatically delineated in the acquired standard apical four-, two- and three-chamber views by STE, and if necessary, the endocardial borders were manually adjusted to better track myocardial motion. LV GLS was derived based on averaging the peak strain of 17 segments from three apical views. The ejection period was defined according to the open cut points of the mitral and aortic valves. LV PSL was constructed by non-invasive measurement of LV systolic pressure combined with LV GLS.
The area of LV PSL is equal to the LV GWI. During systole, the work done to promote the shortening of the myocardium is constructive work (CW), and myocardial work performed during elongation is waste work (WW). At isovolumetric diastole, the work contributing to myocardial lengthening is the CW, and the work of myocardial shortening is defined as the WW.
The basal, mid, and apical sections of the myocardium were confluent to generate six segments (septal, anteroseptal, inferior, lateral, posterior, and anterior) to evaluate segmental differences in MW.
Clinical parameters
All patients and normal controls underwent blood collection on the day of image collection, and blood biochemical parameters were analysed by the Department of Laboratory Medicine. The glycated haemoglobin A1c (HbA1c) of patients was obtained through HLC-723 G11 (Tosoh Bioscience) and its corresponding kit. The total cholesterol (TC), triglycerides (TG), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), fasting plasma glucose (FPG), blood urea nitrogen (BUN), and serum creatinine (SCR) concentrations of patients were obtained through Roche Cobas 8000 and these corresponding kits.
Statistical analysis
SPSS statistical software, version 23.0 (SPSS Inc., Chicago, USA), was used for the statistical analysis of all data. Statistical significance was indicated by a p value of < 0.05. The Shapiro‒Wilk test was used to test whether the data conformed to normal distribution. Continuous variable data are presented as the mean ± SD when normally distributed and the median (interquartile range) when not normally distributed. Absolute values and percentiles were used to represent categorical data. When comparing normal controls, T2DM patients, and T2DM patients with HT, one-way analysis of variance (ANOVA), the Kruskal‒Wallis test, or the x2 test were applied. Univariate regression analysis was first used to evaluate the relationship between traditional echocardiographic or clinical parametersand global and segmental myocardial work parameters. Each relevant parameter with a p value of < 0.20 was included in the multivariate regression analysis. The parameters of MW in the normal controls were defined as normal, and the corresponding indexes in T2DM patients with and without HT were defined as abnormal. The area under the receiver operating characteristic (ROC) curve (AUC) was used to evaluate the sensitivity and specificity of MW in evaluating subclinical LV myocardial systolic dysfunction in T2DM patients with and without HT. Reproducibility was tested by intra- and intergroup correlation coefficient analysis.
Results
Study population
The clinical parameters of the study cohort are shown in Table 1. 27 patients with poor image quality due to smoking or obesity that precluded speckle tracking and 18 patients with valvular disease, arrhythmia, cardiomyopathy, or ischaemic events were excluded. After recruitment and screening, a total of 190 individuals were included in the study: 60 T2DM patients (mean age, 48.58 ± 11.69 years); 60 T2DM patients with HT (mean age, 52.86 ± 13.13 years); and 70 sex- and age- matched normal individuals (mean age, 48.53 ± 9.68 years). There was no significant difference in age or sex among the three groups (p > 0.05). However, the body mass index (BMI) and body surface area (BSA) of T2DM patients with and without HT were remarkably higher than those of the normal controls (p < 0.05). The SBP and DBP in T2DM patients with HT were significantly higher than those in the other two groups (p < 0.05).
Conventional echocardiographic parameters
Traditional echocardiographic parameters of the study cohort are shown in Table 2. The LAd (p = 0.011), LVPWd (p < 0.001) and IVSd (p < 0.001) were significantly increased in T2DM patients with HT compared with patients with T2DM alone and normal controls. The MAPSE (p < 0.05), E/A (p < 0.001) and E/e′ (p < 0.05) of T2DM patients with HT were significantly lower than those of T2DM patients and normal controls. The LVEDV index (p < 0.001) and LVESV index (p = 0.025) of T2DM patients and T2DM patients with HT were significantly lower than those of normal controls. However, the LVEF of the three groups remained within the normal ranges.
Global myocardial work parameters
The global MW parameters of the study cohort are shown in Table 3 and Fig. 2. Significant reductions in GWI and GCW were observed in T2DM patients and T2DM patients with HT compared with normal controls (p < 0.001). In addition, from normal controls to T2DM patients with HT, GWI and GCW showed a decreasing trend first and then an increasing trend (ptrend < 0.05). GWE (p = 0.002) and GCW/GWW (p = 0.004) appeared significantly lower in T2DM patients with HT than in normal controls, and both showed a decreasing trend (ptrend < 0.05). Although the divergences in GWW among the three groups were not significant (p = 0.064), the overall value showed an increasing trend (ptrend = 0.003).

Differences in global MW parameters among normal controls, T2DM patients and T2DM patients with HT. **: significant differences were found between groups (p < 0.05). ***: p < 0. 001.ns: no significant differences were found between groups (p > 0.05)
Correlation and exposure factors
As shown in Table 4. GCW showed certain correlations with sex (p = 0.021), SBP (p < 0.001) and MAPSE (p < 0.001) in T2DM patients with and without HT.
Multivariate regression analysis was applied to appraise the independent effects of the above indicators on GCW. TC (p = 0.040), SBP (p < 0.001), and MAPSE (p < 0.001) were were independently associated with GCW in T2DM patients with and without HT.
Construction and analysis of an ROC curve
An ROC curve was constructed to analyse whether MW could accurately evaluate subclinical LV myocardial dysfunction in T2DM patients with and without HT (Table 5 and Fig. 3). The sensitivity and specificity of the GWI were 55.83% and 84.29%, respectively, with an area under the curve (AUC) of 0.691. The sensitivity and specificity of GCW were 40.83% and 92.86%, respectively, with an AUC of 0.672. The sensitivity and specificity of GWE were 44.17% and 75.71%, respectively, with an AUC of 0.637. The sensitivity and specificity of GCW/GWW were 55.83% and 65.71%, respectively, with an AUC of 0.630. The sensitivity and specificity of combined GWI, GCW, GWE, and GCW/GWW were 50.00% and 92.86%, respectively, with an AUC of 0.743, and the value of AUC in combined these variables was significantly higher than the AUCs of the individual indices (p < 0.05).

ROC analysis was used to determine the AUC, sensitivity and specificity of MW parameters to evaluate subclinical LV myocardial systolic function in T2DM patients
Intra- and interobserver variability analysis
The intraclass correlation coefficients (ICCs) for GWI, GCW, GWW, GWE and GCW/GWW were 0.96 (95% CI: 0.90–0.98, p < 0.001), 0.94 (95% CI: 0.85–0.98, p < 0.001), 0.94 (95% CI: 0.85–0.98, p < 0.001), 0.89 (95% CI: 0.75–0.96, p < 0.001) and 0.88 (95% CI: 0.73–0.95, p < 0.001), respectively. The interobserver ICCs were 0.94 (95% CI: 0.86–0.98, p < 0.001) for GWI, 0.91 (95% CI: 0.78–0.96, p < 0.001) for GCW, 0.88 (95% CI: 0.73–0.95, p < 0.001) for GWW, 0.86 (95% CI: 0.69–0.94, p < 0.001) for GWE and 0.86 (95% CI: 0.69–0.94, p < 0.001) for GCW/GWW.
Segmental MW parameters
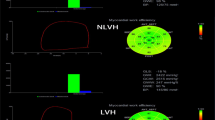
The segmental MW parameters of the study cohort are shown in Table 6 and Fig. 4. There were no significant differences in the myocardial work index (MWI) (p = 0.331), CW (p = 0.100), WW (p = 0.114) or CW/WW (p = 0.110) of the anteroseptal wall among normal controls, T2DM patients and T2DM patients with HT. Differences of WE in anteroseptal wall appeared milder (p = 0.048). In contrast, the MWI (p = 0.010), CW (p < 0.001), WW (p = 0.005), WE (p < 0.001) and CW/WW (p < 0.001) of the anterior wall showed significant differences among the three groups. In addition, the MWI and CW of the inferior, posterior, lateral, and septal segment showed significant differences among the three groups (p < 0.05).

Difference in segmental CW between normal controls, T2DM patients, and T2DM patients with HT. LAD left anterior descending coronary artery, LCA left circumflex artery, RCA right coronary artery
Discussion
The present study provides the followingfindings: (1) T2DM with and without HT patients have subclinical global and segmental LV myocardial systolic dysfunction, and the impairment of anterior wall is more significant. (2) TC, SBP, and MAPSE were independent influencing factors for GCW in T2DM patients. (3) The combination of GWI, GCW, GWE, and GCW/GWW was better than GWI, GCW, GWE, and GCW/GWW alone in evaluating subclinical LV myocardial systolic dysfunction in T2DM patients with and without HT (AUC = 0.743, p < 0.05).
Myocardial work
Micro- and macrovascular lesions that cause myocardial ischaemia [17] or diabetic cardiomyopathy in the absence of dyslipidaemia, hypertension, and coronary artery disease [18] have consequences for LV myocardial systolic function in T2DM patients. However, subclinical LV myocardial systolic dysfunction is not well reflected in conventional echocardiographic parameters (LVEF is maintained within normal values). Therefore, several earlier reports proposed diastolic dysfunction as the earliest functional change during the development of myocardial dysfunction in diabetes [19, 20]. Subsequently, Ernande et al.[21] noted that there were various degrees of abnormality in LV myocardial systolic function in T2DM patients with normal LV diastolic function at early stages, as reflected by impaired strain. However, the measurement of strain was overdependent on afterload, and Russell et al. [10] proposed to estimate MW by constructing PSL from non-invasive measurement of LV peak systolic pressure to accurately evaluate LV myocardial systolic function.
MW as a novel technique has been used in recent studies to evaluate the effects of cardiovascular disease on myocardial systolic function. Edwards et al. [22] found that GWI (AUC = 0.786) was more sensitive than GLS (AUC = 0.693) in coronary artery disease patients with normal LVEF and no segmental motion abnormalities. Hiemstra et al. [23] stated that GWI, GCW and GWE were significantly decreased in non-hypertrophic cardiomyopathy patients, but GWW was increased. The prognosis of patients with GCW > 1730 mmHg% was significantly better than that of patients with GCW < 1730 mmHg%. Ilardi et al. [24] retrospectively reviewed 170 patients with moderate to severe aortic stenosis with normal LVEF and found that GWI < 1951 mmHg% or GCW < 2475 mmHg% was predictive of all-cause mortality in this population. Tadic et al. [25] studied 110 HT patients and found that GWI and GCW were significantly increased in those patients compared with normal controls. In our previous study [11], we used MW to evaluate LV myocardial systolic function in T2DM patients with preserved LVEF, and we concluded that GWI, GCW and GWE were significantly lower in T2DM patients than in normal controls and proposed that MW estimation could be used as a novel technique to evaluate subclinical LV myocardial dysfunction in T2DM patients.
Therefore, in the present study, after applying MW estimation to evaluate LV myocardial systolic function in T2DM patients with and without HT, we found that GWI, GCW, GWE, and GCW/GWW were significantly impaired compared with those in normal controls. In addition, from the normal controls to T2DM patients with HT, GWE and GCW/GWW showed a decreasing trend, and GWW showed an increasing trend. Myocardial work efficiency is derived indirectly from the ratio of constructive and wasted myocardial work [26]. GCW/GWW is an intuitive expression of work efficiency, which can provide more reference values for the increase and decrease of GCW and GWW. This finding suggests that HT has additional influencing factors on the LV myocardial systolic function of T2DM patients and causes more impairment in LV myocardial systolic function. The myocardial systolic dysfunction is closely related to the compensatory hypertrophy of LV myocytes and the proliferation of fibroblasts caused by the long-term afterload increase in HT patients and eventually leads to myocardial fibrosis. However, the upwards trend of GWI and GCW in T2DM patients with HT compared with T2DM patients has been attributed to the need for the LV myocardium to use systolic reserve to overcome the increased afterload resulting from HT, thereby maintaining LVEF within normal values. Hyperinsulinemia and insulin resistance can cause alterations in vascular homeostasis, decreases in nitric oxide and increases in reactive oxygen species levels, leading to myocardial dysfunction, and together with aberrant activation or immune dysregulation of the renin–angiotensin–aldosterone system, they promote interstitial fibrosis in cardiac tissue [27], providing an explanation for subclinical LV myocardial systolic dysfunction in T2DM patients.
Additionally, in the present study, we evaluated the segmental differences in MW in T2DM patients and T2DM patients with HT compared with normal controls to identify the negative effects of myocardial segments in T2DM patients with and without HT. The impairment of anterior wall was more evident, and the lateral, inferior, posterior, and septum were also impaired to various degrees, but no significant impairment was observed in the anteroseptal wall. Segmental myocardial systolic dysfunction may be related to abnormal lipid metabolism in T2DM patients [28]. On the one hand, with increased delivery of fatty acids to cardiomyocytes, enhanced fatty acid β-oxidation leads to myocardial hypoxia. On the other hand, an increase in lipids and their metabolites increases the risk of coronary atherosclerosis, leading to a decrease in myocardial blood supply. However, existing studies do not better explain why the impairment of the anterior myocardium is more pronounced in T2DM patients. It seems to be related to myocyte fibrosis in the corresponding segment or ischemia of the diagonal branches in the left anterior descending coronary artery. The impairment of the anterior myocardium seems to serve as reference information to suggest the formation of corresponding coronary artery lesions or regional myocardial fibrosis. Further research is needed to demonstrate its reliability for clinical guidance. On the other hand, it is not possible to exclude the possible role exerted by the chest wall conformation in determining the impairment of myocardial strain and MW parameters, particularly at basal level, in T2DM patients with a narrow antero-posterior chest diameter [29, 30].
Clinical implications
Global and segmental analysis of MW in T2DM patients with and without HT can be more convenient and rapid for helping clinicians identify patients with global and segmental myocardial systolic dysfunction at subclinical stages with preserved LVEF. Therefore, treatment can be administered at an early stage, leading to fewer cardiovascular complications. We incorporated GCW/GWW, a new evaluation parameter, based on the original GWI, GCW, GWW and GWE. Thus, a more intuitive evaluation constructs a gain/loss relationship between work and waste. TC was independent influencing factor for the development of impaired GCW in T2DM patients with and without HT, suggesting that T2DM patients need control blood lipids to reduce the toxic effects of lipids on cardiomyocytes, also T2DM patients should control their blood pressure. These findings could be used to derive additional protocols and provide value when MW evaluation is applied to other cardiovascular diseases. In addition, it was concluded in ROC curve analysis that evaluation with a combination of the above four indices of subclinical LV myocardial systolic dysfunction was significantly better than that of single index evaluation.
Conclusion
MW can non-invasively evaluate subclinical global and segmental LV myocardial systolic dysfunction in T2DM patients with and without HT. TC and SBP were independent influencing factors for GCW in T2DM patients with and without HT. Regulating total cholesterol levels and controlling blood pressure in T2DM patients with and without HT might reduce the impairment of LV myocardial systolic function.
Limitations
There are still some limitations in the present study. First, patients with poor image quality due to obesity, smoking, etc., were excluded, so this exclusion criterion may be biased for different operators. Furthermore, the present study was a single-centre study, and multicentre large sample studies are needed to further provide reference value for this finding.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- BSA:
-
Body surface area
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- HbA1c:
-
Glycosylated hemoglobin A1c
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- FPG:
-
Fasting plasma glucose
- BUN:
-
Blood urea nitrogen
- SCR:
-
Serum creatinine
- LA:
-
Left atrial
- LAV:
-
Left atrial volume
- IVS:
-
Interventricular septum
- PW:
-
Posterior wall
- LV:
-
Left ventricular
- LVEDV:
-
LV end-diastolic volume
- LVESV:
-
LV end-systolic volume
- LVEF:
-
Left ventricular ejection fraction
- MAPSE:
-
Mitral annular plane systolic excursion
- LVGLS:
-
LV global longitudinal strain
- GWI:
-
Global myocardial work index
- GCW:
-
Global constructive work
- GWW:
-
Global waste work
- GWE:
-
Global work efficiency
References
Organization WH. World Health Statistics 2022. 2022.
Shah A, Isath A, Aronow WS. Cardiovascular complications of diabetes. Expert Rev Endocrinol Metab. 2022;17:383–8.
Bugger H, Abel ED. Molecular mechanisms of diabetic cardiomyopathy. Diabetologia. 2014;57:660–71.
Zoroufian A, Razmi T, Taghavi-Shavazi M, Lotfi-Tokaldany M, Jalali A. Evaluation of subclinical left ventricular dysfunction in diabetic patients: longitudinal strain velocities and left ventricular dyssynchrony by two-dimensional speckle tracking echocardiography study. Echocardiography. 2014;31:456–63.
Huang D, Cui C, Zheng Q, Li Y, Liu Y, Hu Y, et al. Quantitative analysis of myocardial work by non-invasive left ventricular pressure-strain loop in patients with type 2 diabetes mellitus. Front Cardiovasc Med. 2021;8: 733339.
Xie LJ, Dong ZH, Yang ZG, Deng MY, Gao Y, Jiang L, et al. Assessment of left ventricular deformation in patients with type 2 diabetes mellitus by cardiac magnetic resonance tissue tracking. Sci Rep. 2020;10:13126.
Roemer S, Jaglan A, Santos D, Umland M, Jain R, Tajik AJ, et al. The utility of myocardial work in clinical practice. J Am Soc Echocardiogr. 2021;34:807–18.
Lee SE, Nguyen C, Xie Y, Deng Z, Zhou Z, Li D, et al. Recent advances in cardiac magnetic resonance imaging. Kor Circul J. 2019;49:146–59.
Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, Gjesdal O, et al. Assessment of wasted myocardial work: a novel method to quantify energy loss due to uncoordinated left ventricular contractions. Am J Physiol Heart Circ Physiol. 2013;305:H996-1003.
Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, Remme EW, et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: a non-invasive index of myocardial work. Eur Heart J. 2012;33:724–33.
Wang T, Li L, Huang J, Fan L. Assessment of subclinical left ventricle myocardial dysfunction using global myocardial work in type 2 diabetes mellitus patients with preserved left ventricle ejection fraction. Diabetol Metab Syndr. 2022;14:17.
American DA. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36(Suppl 1):S67-74.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. 2018;2018(36):1953–2041.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1–39): e14.
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the american society of echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016;29:277–314.
Matos J, Kronzon I, Panagopoulos G, Perk G. Mitral annular plane systolic excursion as a surrogate for left ventricular ejection fraction. J Am Soc Echocardiogr. 2012;25:969–74.
Park JJ. Epidemiology, pathophysiology, diagnosis and treatment of heart failure in diabetes. Diabetes Metab J. 2021;45:146–57.
Dillmann WH. Diabetic cardiomyopathy. Circ Res. 2019;124:1160–2.
Poirier P, Bogaty P, Garneau C, Marois L, Dumesnil JG. Diastolic dysfunction in normotensive men with well-controlled type 2 diabetes: importance of maneuvers in echocardiographic screening for preclinical diabetic cardiomyopathy. Diabetes Care. 2001;24:5–10.
From AM, Scott CG, Chen HH. The development of heart failure in patients with diabetes mellitus and pre-clinical diastolic dysfunction a population-based study. J Am Coll Cardiol. 2010;55:300–5.
Ernande L, Bergerot C, Rietzschel ER, De Buyzere ML, Thibault H, Pignonblanc PG, et al. Diastolic dysfunction in patients with type 2 diabetes mellitus: is it really the first marker of diabetic cardiomyopathy? J Am Soc Echocardiogr. 2011;24:1268-75.e1.
Edwards NFA, Scalia GM, Shiino K, Sabapathy S, Anderson B, Chamberlain R, et al. Global myocardial work is superior to global longitudinal strain to predict significant coronary artery disease in patients with normal left ventricular function and wall motion. J Am Soc Echocardiogr. 2019;32:947–57.
Hiemstra YL, van der Bijl P, El Mahdiui M, Bax JJ, Delgado V, Marsan NA. Myocardial work in nonobstructive hypertrophic cardiomyopathy: implications for outcome. J Am Soc Echocardiogr. 2020;33:1201–8.
Ilardi F, Postolache A, Dulgheru R, Trung MN, de Marneffe N, Sugimoto T, et al. Prognostic value of non-invasive global myocardial work in asymptomatic aortic stenosis. J Clin Med. 2022;11:1.
Tadic M, Cuspidi C, Pencic B, Grassi G, Celic V. Myocardial work in hypertensive patients with and without diabetes: An echocardiographic study. J Clin Hypertens (Greenwich). 2020;22:2121–7.
Chan J, Edwards NFA, Khandheria BK, Shiino K, Sabapathy S, Anderson B, et al. A new approach to assess myocardial work by non-invasive left ventricular pressure-strain relations in hypertension and dilated cardiomyopathy. Eur Heart J Cardiovasc Imaging. 2019;20:31–9.
Jia G, Whaley-Connell A, Sowers JR. Diabetic cardiomyopathy: a hyperglycaemia- and insulin-resistance-induced heart disease. Diabetologia. 2018;61:21–8.
Lee TW, Bai KJ, Lee TI, Chao TF, Kao YH, Chen YJ. PPARs modulate cardiac metabolism and mitochondrial function in diabetes. J Biomed Sci. 2017;24:5.
Nomura K, Ajiro Y, Nakano S, Matsushima M, Yamaguchi Y, Hatakeyama N, et al. Characteristics of mitral valve leaflet length in patients with pectus excavatum: a single center cross-sectional study. PLoS ONE. 2019;14: e0212165.
Sonaglioni A, Nicolosi GL, Trevisan R, Lombardo M, Grasso E, Gensini GF, et al. The influence of pectus excavatum on cardiac kinetics and function in otherwise healthy individuals: A systematic review. Int J Cardiol. 2023;381:135–44.
Acknowledgements
We would like to thank the department of Echocardiography, Cardiology and Endocrinology, the Affiliated Changzhou Second People's Hospital with Nanjing Medical University.
Funding
Changzhou Science and Technique Program (Grant No.: CJ20190098).
Author information
Authors and Affiliations
Contributions
GAL and JH designed the study and carried out the study, data collection and analysis, wrote the manuscript and JH revised the manuscript. GAL and XS collected the T2DM patients and normal controls. LF and JH performed the statistical analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study complied with the Declaration of Helsinki and was reviewed and approved by the Human Subjects Committee of Changzhou Second People′s Hospital. Written informed consent was obtained from each couple enrolled in the study.
Consent for publication
This manuscript does not include any individual person′s data.
Competing interests
The authors declared no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, GA., Huang, J., Sheng, X. et al. Assessment of subclinical left ventricular myocardial systolic dysfunction in type 2 diabetes mellitus patients with or without hypertension by global and segmental myocardial work. Diabetol Metab Syndr 15, 200 (2023). https://doi.org/10.1186/s13098-023-01180-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-023-01180-0