
Abstract
Background
Despite the existence of evidence-based therapy options for the treatment of chronic pain and comorbid depressive symptoms (e.g., CBT), many individuals remain untreated. Treatment gaps result from a lack of specialists, patient fear of stigmatization, or patient immobility. Internet-based self-help interventions could serve as an anonymous and flexible alternative treatment option. In a pilot study, chronic pain patients with comorbid depressive symptoms who used a generic Internet-based depression program showed a significant reduction in depressive symptoms (but not pain symptoms) compared to a waitlist control group. Based on these findings, we developed the low-threshold, anonymous, and cost-free Internet-based self-help intervention Lenio that is tailored to the specific needs of chronic pain patients with comorbid depressive symptoms. Lenio is accompanied by the smartphone application (app) COGITO designed to increase therapeutic success. With Lenio and COGITO addressing both chronic pain and depressive symptoms, the trial aims to increase treatment effects of online interventions for chronic pain patients by reducing both depressive symptoms and pain.
Methods
The effectiveness of the Internet-based self-help intervention and accompanying smartphone app will be evaluated in a randomized controlled trial (RCT). A total of 300 participants will be randomized into an intervention group (Lenio/COGITO), an active control group (depression-focused smartphone app), or a waitlist control group. Assessments will be done at baseline, after an 8-week intervention period (post), and after 16 weeks (follow-up). The primary outcome is the post-assessment reduction in “pain impairment” (mean value of impairment in daily life, free time, and work) as assessed by the DSF (German pain questionnaire).
Secondary outcomes will include the reduction in depressive symptoms as well as in the severity of pain.
Discussion
Lenio is one of the first Internet-based interventions to reduce chronic pain and depression that will be empirically evaluated. Internet-based interventions could offer a promising alternative to conventional face-to-face psychotherapy in the treatment of chronic pain patients. The primary objective of the current study is to add essential insight into the feasibility, effectiveness, and acceptance of Internet-based interventions for people with chronic pain and depressive symptoms.
Trial registration
DRKS-ID DRKS00026722, Registered on October 6th, 2021.
Similar content being viewed by others


Introduction
Background and rationale {6a}
The interaction of pain and emotional well-being
Pain is a psychophysiological warning sign that protects us from potential danger [36]. However, pain, especially when it manifests as a chronic condition, may become a profound problem for the affected individual. Worldwide, chronic pain is among the most common causes for seeking medical care, with a global prevalence of 15% to 45% and estimated economic costs in the US at $600 billion annually [49, 54]. Research findings highlight the negative effects of chronic pain on quality of life [10] in both private and professional life [16]. Considering these findings, it is not surprising that up to 75% of chronic pain patients experience comorbid depressive symptoms [32].
The relationship between chronic pain and depressive symptoms is likely bidirectional. On the one hand, depression can contribute to the multifactorial genesis of chronic pain [47], while on the other hand depressive symptoms can emerge as a result of impairments in psychosocial functioning and low quality of life due to chronic pain [44].
Psychotherapeutic treatment of pain
The gate control theory was the first model to emphasize the role of psychological factors on the experience of chronic pain, and its development initiated the integration of psychological strategies in the treatment of chronic pain [37]. Multiple studies found significant improvements in chronic pain and depression scores after psychotherapeutic interventions [22, 48, 55]. A meta-analysis by Veehof and colleagues [52] reported significant improvements in chronic pain intensity, and chronic pain interference at medium effect sizes after acceptance- and mindfulness-based interventions compared to wait-list, medical treatment-as-usual, as well as educational and support control groups. Although effective psychotherapeutic treatments like this are available, many individuals remain untreated. Psychological and social influences on the genesis and maintenance of chronic pain are often not recognized or addressed in standard pain treatment [38]. Furthermore, a significant amount of affected individuals experience (self-)stigmatization, which often accompanies depressive symptoms and is detrimental to patients’ motivation to seek psychotherapeutic treatment [11]. Moreover, immobility among pain patients may make traveling to healthcare institutions difficult [13, 18]. As a result, there is a need for low-threshold, easily accessible, and anonymous support services to help overcome the treatment gap of individuals with both chronic pain and depressive symptoms.
Internet-based psychological interventions
Internet-based psychological interventions present an alternative to conventional face-to-face psychotherapy in the treatment of chronic pain patients [8, 30, 48]. In recent years, many studies have replicated the effectiveness of Internet-based interventions for numerous mental disorders [8, 30, 48]. Firstly, Internet-based interventions are resource efficient and safe [21]. Secondly, due to flexibility in timing, intensity, and focus as well as anonymity and privacy, compliance with Internet-based programs is high [26, 25].
Internet-based interventions can be implemented as unguided (self-help) or guided treatment (individual support by a therapist, such as by telephone). According to a meta-analysis, guided Internet-based interventions have a similar effectiveness to conventional face-to-face therapy [8]. Most studies show greater effect sizes for guided than for unguided Internet-based interventions [46]. However, unguided Internet-based interventions are superior in terms of cost and resource efficiency as well as anonymity [25]. Their main drawback, adherence, may be counteracted by e-mail reminders and by presenting information in textual rather than non-textual format [1].
Internet-based psychological interventions for chronic pain
A recent systematic review of online interventions targeted at chronic pain found a small to moderate effect on pain intensity reduction (Hedges' g = − 0.33) [6]. Programs that address both chronic pain and depressive symptoms are rare and randomized controlled trials (RCTs) examining their short- and long-term efficacy in large samples are scarce. To the best of our knowledge, there is no open-source Internet-based self-help program for the treatment of chronic pain and comorbid depressive symptoms.
Miegel and colleagues [39] evaluated an unguided Internet-based intervention named Novego for the treatment of depression in a sample of chronic pain patients. Significant reductions with small to moderate effect sizes in depressive symptoms in the Novego group were found compared to a wait-list control group (ηp2 = 0.043). However, reductions in pain intensity compared to the wait-list control group were only observed for a small subgroup (e.g., pain localization in the upper back or hands). Hence, an Internet-based program specifically tailored to the individual needs of chronic pain patients with comorbid depressive symptoms, rather than depressive symptoms only, could augment these effects.
To provide a low-threshold, anonymous, and open-source Internet-based self-help intervention for chronic pain patients with comorbid depressive symptoms, we developed Lenio as part of the current research project. Lenio is a novel Internet-based self-help intervention addressing both chronic pain and depression. It is to be used in combination with a smartphone application (app) called COGITO (uke.de/cogito). Research has shown that the combination of Internet-based programs and smartphone apps that transfer psychotherapeutic strategies into everyday life may increase therapeutic success as well as adherence [51]. Previous RCTs of a pilot version of the COGITO app found significant reductions in self-reported depressive symptoms and an increase in self-esteem among those who used the app regularly compared to wait-list controls [5, 33].
Objectives {7}
The aim of the current research project is to investigate the feasibility, effectiveness, and acceptance of the Internet-based self-help intervention Lenio in combination with the smartphone app COGITO in an RCT. As the primary objective, a significant reduction in pain impairment (mean value of impairment in daily life, leisure time, and work; primary outcome) as measured by the German Pain Questionnaire (German acronym: DSF) in the intervention group compared to a waitlist and an active control group is expected. Furthermore, we also assume that depressive symptoms, as well as pain-related cognitive biases (e.g., catastrophizing, fear-avoidance beliefs), will be significantly reduced in the intervention group compared to the two control groups. Hence, the treatment of a highly prevalent condition could be improved.
Trial design {8}
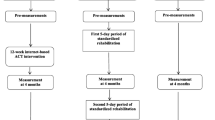
The self-guided Internet-based intervention Lenio will be evaluated in the framework of a randomized controlled trial (RCT). Participants will be randomly allocated (ratio 1:1:1) to one of three conditions: (1) intervention group (direct access to the Internet-based intervention Lenio and the smartphone app COGITO), (2) waitlist control group, or (3) active control group (access to a transdiagnostic smartphone app named MCT & More).
The waitlist control will show the effect of the intervention against no treatment, while the active control will show the effect of the intervention versus an Internet-based intervention addressing psychological problems but not chronic pain {6b}.
Methods: participants, interventions, and outcomes
Study setting {9}
Data will be collected online at baseline, post intervention (8 weeks after baseline), and follow-up (16 weeks after baseline). The online surveys will be generated using the software Qualtrics®, which meets standards of data safety regulations. Both the waitlist control group and the active control group will receive access to the Internet-based programs Lenio and COGITO after completion of the follow-up assessment 16 weeks after baseline.
Who will take informed consent? {26a}
At the online baseline survey, participants will be informed about the aims and the procedure of the study, inclusion and exclusion criteria, and their right to withdraw from study participation at any time. Subjects may request deletion of data already collected pending data evaluation.
Data management {19}
All participants will be instructed to create an e-mail address without personally identifiable information. No additional personal data (e.g., names, addresses) will be collected. All e-mail addresses will be treated confidentially, will not be passed on to third parties outside of the research team, and will be deleted after the study’s end.
Participant timeline {13}
After giving informed consent, sociodemographic and psychopathological data will be assessed. At the end of baseline, individuals will be randomized equally to one of the three conditions. Randomization will be conducted automatically in Qualtrics®, preventing influence by third parties {16a}. At post-intervention and follow-up, psychopathological data, subjective evaluation, and side effects will be examined. For participating in each of the three online surveys (baseline, post, follow-up), participants will receive €10 Amazon® vouchers (as much as €30 total) as an incentive.
Instructions after baseline will be delivered via e-mail. The intervention group will receive their login details for Lenio and COGITO. One week later, individuals in the intervention group who do not log into Lenio will receive a reminder, including an overview of the program. Adherence will be further enhanced by sending e-mails that include descriptions (including tips) of specific modules. The active control group will receive instructions and an MCT & More download link for Android and IOS. Both the active control and the waitlist control group will receive log-in details for Lenio after completion of the follow-up survey 16 weeks after baseline.
Links to the post and follow-up assessments will be sent by automatically triggered e-mails. If participants will have not participated in a particular survey, they will receive a maximum of two e-mail reminders at intervals of 1 week. (The first e-mail reminder will be automated. However, the second reminder will be a personal message from the principal study investigator) {18b} (Table 1).
Sample size {14}
The sample size calculation was conducted using G*Power®. Given that Miegel and colleagues [39] examining the effect of an unguided Internet-based interventions for depression on chronic pain patients found small to moderate effects, a moderate effect in the current study can be expected [39]. For analysis of covariance, the software yielded a required sample size of 246 with an expected effect size of ηp2 = 0.06 (moderate effect), an alpha of 0.05 (two-sided), and a power of 0.95. We expect a drop-out rate of 25%. Hence, we aim to recruit 300 participants in total, with 100 participants per condition.
Recruitment {15}
Participants will be recruited in inpatient and outpatient clinics and institutions that will inform potential participants about the study and distribute the study flyers. Flyers will include study information and a QR code that leads directly to the baseline survey. Furthermore, study information and links will be distributed in Facebook groups regarding relevant topics (e.g., self-help groups for chronic pain). In addition, a Facebook/Instagram and Google Ads campaign has already been set up. The campaign targeted different groups of pain patients (e.g., pain caused by accidental injury). Further sources of recruitment are through self-help groups, Internet forums, websites and newsletters of health insurance companies/associations, and various social media platforms (Instagram, Reddit, Twitter, YouTube, LinkedIn), which is especially helpful in reaching people from the community and not only patients that are already in treatment.
Eligibility criteria {10}
For inclusion in the RCT, participants must meet the following criteria:
-
(a)
Presence of depressive symptoms (Beck Depression Inventory-II (BDI-II) score ≥ 14; Patient Health Questionnaire-9 (PHQ-9) score ≥ 10),
-
(b)
Chronic pain symptoms (mean score pain intensity on the German Pain Questionnaire (DSF) ≥ 4),
-
(c)
Aged 18 to 75 years,
-
(d)
Informed consent,
-
(e)
Sufficient knowledge of the German language,
-
(f)
Willingness to participate in three anonymous online surveys,
-
(g)
Willingness to use the Internet-based treatment program over a period of 8 weeks minimum, and
-
(h)
Access to a computer/laptop and a smartphone.
The program has been developed for a heterogeneous target group of chronic pain patients with comorbid depressive symptoms. No formal diagnosis (of chronic pain and/or depressive symptoms) is needed as symptoms will be assessed by validated questionnaires at baseline. Effects of prior diagnoses as well as concurrent treatment programs will be analyzed in moderation analyses (see statistical analyses).
Exclusion criteria are a lifetime diagnosis of a schizophrenia spectrum disorder, bipolar disorder, substance abuse disorder, or acute suicidality (assessed by one item on suicidality on the Web Screening Questionnaire; WSQ).
Inclusion and exclusion criteria will be assessed at baseline. Excluded participants will be forwarded to an additional survey page providing the reason for exclusion and a contact e-mail address of the principal study investigator. In case of exclusion due to acute suicidality, participants will also be provided with phone numbers of crisis services.
Interventions
Intervention description {11a}
Lenio
The self-help Internet-intervention Lenio is based on principles of cognitive-behavior therapy (CBT) and its “third wave” properties (e.g., mindfulness-based and metacognitive techniques). Lenio includes a welcome module, an introduction module, and nine specific modules that all address chronic pain and emotional problems (see Table 2 for an overview of all modules). Some modules are more generic (e.g., social competence, self-worth), whereas other modules are more specific to chronic pain (e.g., modules on acceptance and commitment therapy [ACT], specific needs, and relapse prevention).
Modules are further divided into subunits. For example, the module Sleep is further divided into Introduction, Sleeping problems, Sleep hygiene, and Cognitive distortions. Participants are free to decide on the order in which they work on the modules. Once they decide on one module, they are advised to work through all its subunits in the given order. However, the division into subunits enables users to set priorities or to skip topics if they are already familiar with them. Moreover, participants do not have to work through one module in one session, as they can pause at any time and easily return to the last page visited, which will automatically be saved. Furthermore, we recommend they work through at least two modules per week. The time required to complete one module is 30 to 60 min on average.
When participants log into Lenio for the first time, an introductory video starts automatically that contains information on how to use Lenio. Subsequently, the welcome module starts, which was developed based on the theory of motivational interviewing. Participants start an interactive dialogue with an avatar. The aim is to motivate participants to work on the psychological aspects of their chronic pain. At the end of the welcome module, participants are introduced to five different avatars whose stories will be told in case vignettes throughout the program. All other modules include psychoeducational texts as well as interactive exercises and worksheets, graphics, videos, and audios. Participants are also provided with the possibility of communicating with a moderator via an internal messenger service. If participants have technical difficulties, the moderator will answer questions related to the program within three workdays. The moderator does not provide therapeutic guidance. Thus, Lenio is an unguided Internet-based intervention.
COGITO
The smartphone app COGITO can be accessed and downloaded via links to the Google Play Store (for Android users) and the App Store (for iOS users) that are provided in the desktop application Lenio. In the introduction module, participants are instructed on how to use the app. By sending daily push notifications with short exercises (reading time maximum 30 s) and providing elements of gamification (e.g., collecting medals for finished exercises), COGITO demonstrates high usability. Participants will be able to choose the time and frequency of push notifications. COGITO offers different packages of exercises (e.g. Mood and Self-Esteem, Psychosis, Gambling Problems, OCD, Chronic Pain). Participants will be instructed to activate the packages Chronic Pain and Mood & Self-Esteem. Most packages are deactivated by default but can be individually activated by the users. As with Lenio, COGITO exercises are based on CBT and third-wave techniques.
MCT & More
The active control group will receive access to the smartphone app MCT & More. As MCT & More is a pilot version of the COGITO app, its design and concept are similar to COGITO. MCT & More contains three packages (Mood, Metacognitive Training, and Gambling). However, the app does not contain pain-specific exercises. Participants in the active control group will be free to choose the packages they want to receive exercises from.
Outcomes {12}
The primary outcome will be pain impairment (mean value of impairment in daily life, free time, work) as assessed by the DSF (German pain questionnaire). The DSF is a commonly used, reliable, and validated instrument for the assessment of chronic pain [9]. We decided on pain impairment as the main outcome as Lenio especially targets the psychological aspects of chronic pain. Hence, we expect a significant improvement in different aspects of life, including daily life, leasure time, and work. The secondary outcomes will include depressive symptoms as well as the severity of pain symptoms. Furthermore, subjective evaluation and possible side effects will be assessed.
Primary outcomes
The German Pain Questionnaire (DSF)
The DSF is a reliable and valid self-report questionnaire used to assess pain symptoms [9, 41]. It captures pain in a multidimensional manner. It assesses pain location (e.g., head coded as “0” if no headache is reported and coded with “1” if it is reported), subjective description of pain, onset and course of pain, and the presence and characteristics of pain attacks. In addition, participants are asked to rate pain intensity (current intensity, mean intensity, highest intensity in the last 4 weeks, and tolerable intensity after successful treatment) on a 10-point scale (“no pain” to “strongest pain imaginable”). The number of days of illness and the pain-related impairment of everyday life (0 “no impairment” to 10 “total impairment”) are also assessed. The DSF assesses previous treatments, the number of stays in rehabilitation clinics, physician visits, surgeries, and comorbid illnesses.
Items of the DSF addressing well-being, anxiety, and depression will not be included in the survey as these dimensions are assessed by other questionnaires (e.g., BDI-II, PHQ-9). Moreover, some items will be excluded because they are irrelevant to this study. For all measurement time points, the pain intensity will be calculated according to von Korff [53].
Secondary outcomes
Beck Depression Inventory-II (BDI-II)
The BDI-II [3] is a 21-item self-report questionnaire that assesses depressive symptoms over the past two weeks. Scores range from 0 to 63, with higher scores indicating higher levels of depression (0–8 = no depression, 9–13 = minimal depression, 14–19 = mild depression, 20–28 = moderate depression, and 29–63 = severe depression). Internal consistency is good, with Cronbach’s α of 0.89 [17]. In a sample of pain patients, comparable results were found [7, 43]. For all measuring points the BDI will be assessed. For our analysis, the sum score will be calculated.
Patient Health Questionnaire-9 depression module (PHQ-9)
The PHQ-9 [2, 29] is a self-report questionnaire measuring depressive symptom severity over the previous week. The PHQ-9 has high internal consistency (Cronbach’s α = 0.86–0.89, [29]. Its scores range from 0 to 27, with scores from 0 to 4 indicating minimal depression, 5–9 mild depression, 10–14 moderate depression, and 15–27 severe depression. For all measuring points, the sum score will be calculated.
Web Screening Questionnaire (WSQ)
The WSQ is a brief online self-report instrument that screens for common mental disorders such as affective disorders, alcohol abuse/dependence, general anxiety disorder, posttraumatic stress disorder, social phobia, panic disorder, agoraphobia, specific phobia, obsessive–compulsive disorder, and suicide risk. Sensitivity ranges between 0.72 and 1.00, and specificity ranges between 0.44 and 0.77 [14]. The WSQ will be assessed at baseline and for the analysis, the sum score as well as the cumulative values for all subscales of the WSQ will be calculated.
Injustice Experience Questionnaire (IEQ).
The IEQ is a valid and reliable tool for the assessment of perceived injustice in people suffering chronic pain, with a Cronbach’s α of 0.92 [50]. The IEQ consists of 12 items that assess thoughts of unfairness related to symptoms on a 5-point scale ranging from “never” to “all the time.” Perceived injustice is examined by the following elements: severity of loss consequent to injury, blame, sense of unfairness, and irreparability of loss. A score of 30 is the cutoff for a clinically relevant level of perceived injustice. For all three measuring points, the IEQ subscale “blame/injustice” and “severity/irreparability” as well as the sum score will be calculated.
Pain Catastrophizing Scale (PCS)
The PCS is a valid and reliable measure of catastrophizing. It assesses the thoughts and feelings of chronic pain patients. The questionnaire contains 13 items. Participants are asked which thoughts and feelings they experience during pain on a 5-point scale from “not at all” to “all the time.” Besides the total score, three subscales (rumination, magnification, and helplessness) are assessed. The PCS has demonstrated good internal consistency in the past with a Cronbach’s α of 0.87 [45]. For all three measuring points, the PCS total score as well as the subscores “helplessness,” “reinforcement,” and “worrying” will be calculated.
Fear-Avoidance Beliefs Questionnaire (FABQ)
The emergence of the biopsychosocial model of low back pain (LBP) led Waddell et al. [56] to develop the Fear-Avoidance Beliefs Questionnaire (FABQ, [56]). The FABQ assesses the patient’s fear-avoidance beliefs about physical activity and its contribution to lower back pain. It consists of 16 items that can be rated on a 7-point Likert scale (0 = “completely disagree” to 6 = “completely agree”). Test–retest reliability of the FABQ is excellent (ICC = 0.97, [27]). For the current study, we have adapted the FABQ to assess general chronic pain (not specifically lower back pain). For all three measuring points, the sum scores for “bodily activity” and “work load” will be calculated.
Pain Self-Efficacy Questionnaire (FESS)
To assess self-efficacy in our sample, we will use the German version of the Pain Self-Efficacy Questionnaire (FESS). According to Mangels and colleagues [34], the questionnaire is a valid instrument to measure therapeutic success in pain research. Specifically, it measures one’s conviction in one’s own ability to tackle activities despite suffering from pain. Additionally, it has high internal consistency, with a Cronbach’s α of 0.93. For all three measuring points, the sum scores of the PSE subscales “active coping” and “catastrophizing” will be assessed.
World Health Organization: Quality of Life abbreviated version (WHOQOL-BREF
The WHOQOL is a cross-cultural questionnaire assessing generic quality of life (QoL). QoL is defined as an individual’s perceptions of their position in life. QoL considers the context of culture and value systems, including personal goals, standards, expectations, and concerns. The questionnaire was developed by the WHOQOL Group of the World Health Organization. For the present study, we will use the global QoL item (“How would you assess your quality of life?”), with responses ranging from “very poor” (1) to “very good” (5). Despite its brevity, the internal consistency of the questionnaire was high (α = 0.90) in a sample of students [23]. For all measuring points, the global item will be assessed.
University of Rhode Island Change Assessment Scale (URICA)
The URICA is a self-report questionnaire developed to assess various stages of change in complex problem behavior [35].The URICA has demonstrated high internal consistency, with a Cronbach’s α of 0.77 to 0.82 and good reliability [15]. It predicts both treatment success as well as drop-out rates [35]. The present study will use the German version of the URICA (Fragebogen zur Erfassung der Veränderungsbereitschaf, FEVER, [19]). The FEVER captures three different phases of change: (1) pre-contemplation, i.e., lack of readiness to engage in an intervention or no readiness to change, (2) contemplation, i.e., readiness to engage in an intervention or to change something, and (3) action, i.e., the decision to change something and the use of active strategies to change. For the current study, a shorter version with only three items per phase (total of nine items) will be used. The FEVER/URICA will be assessed at baseline only. The subscales “precontemplation,” “contemplation,” “preparation,” “action,” and maintenance” will be calculated.
Credibility/Expectancy Questionnaire (CEQ)
For reasons of test economy, only one item of the CEQ [4, 12] will be used. The CEQ measures treatment expectancy (“What do you think at the present time about how successful the self-help program Lenio offered here will be in alleviating your complaints?”), which can be rated on a scale from 1 (“not successful at all”) to 9 (“very successful”). The CEQ item will be assessed at baseline only.
PANEPS
The Positive and Negative Effects of Psychotherapy Scale (PANEPS) is a self-report questionnaire that assesses positive effects and adverse events during the most recent session of psychotherapy [42]. The PANEPS consists of 29 items on four subscales: Positive Effects, Unethical Conduct, Malpractice, and Side Effects. Internal consistency is high for all subscales, with a Cronbach’s α of 0.72 to 0.92 [40]. In the current study, an adapted version (PANEPS-I) will be used that has not been validated yet (e.g., the wording of some items has been adapted). All four sub scores will be calculated for post and follow-up assessment.
Subjective appraisal of the program
The subjective appraisal of Lenio will be assessed using the German version of the Client Satisfactory Questionnaire (CSQ-8; German acronym is ZUF-8). According to the literature, the psychometrics of the CSQ-8 are high, with internal consistency ranging from Cronbach’s α = 0.87 to 0.93 [24, 28]. Satisfaction can be assessed on a 4-point rating scale (“excellent,” “good,” “less good,” “bad”). A high score indicates high satisfaction. The wording has been adapted by replacing “psychotherapy” with “self-help intervention Lenio.” Additional subjective data will be assessed by 12 further questions on the quality, utility, and applicability of Lenio in both open and closed response format (see Table 3).
The answers to the seven closed questions will be assessed on a four-point Likert scale (“not applicable” to “completely true”). The open questions ask for positive and negative feedback on Lenio and will ask for improvement suggestions.
In addition, the participants will be asked to indicate how regularly Lenio was used during the intervention period. Subjective data will be assessed at post intervention and follow-up.
Statistical methods
Statistical methods for primary and secondary outcomes {20a}
All analyses will be conducted using IBM SPSS Statistics® 27. The data will be exported from Qualtrics® into SPSS® and initially stored on a secure server and later a password-protected computer. The security of data transmission via the Internet is also guaranteed by SSL encryption. Data will be analyzed using analysis of covariance (ANCOVAs), with between-group differences over time (pre-intervention to post-intervention) as the within-group factor and different conditions as the between-group factor. Baseline scores will serve as covariates, group allocation as the independent variable, and post- and follow-up scores of primary and secondary measures as dependent variables. Group differences at baseline will be assessed using independent t-tests for continuous variables. Partial eta square will be calculated as effect size.
Interim analyses {21b}
For the current trial, an interim report has been written on 03/31/2022.
Methods for additional analyses (e.g., subgroup analyses) {20b}
Explorative moderation analysis will be conducted using the SPSS® macro PROCESS [20] to identify potential moderators for treatment success (all types of baseline variables are being considered in this type of analysis). Furthermore, subjective evaluation of the intervention will be done descriptively by presenting the frequency of positive ratings as well as means and standard deviations.
Methods in analysis to handle protocol non-adherence and any statistical methods to handle missing data {20c}
Analyses will be conducted for both the intention-to-treat (ITT) and the per-protocol (PP) sample. The PP sample will include only those participants who completed the post-assessment and used Lenio and COGITO at least once. Missing values in the ITT analyses will be estimated using the multiple imputation procedure.
Plans to give access to the full protocol, participant-level data, and statistical code {31c}
Full protocol, dataset, and statistical codes will be provided upon request.
Data monitoring and auditing {21a; 23}
An interim report was prepared for the DGUV, who are funding the project, in March 2022. First data was analyzed for this purpose.
Ethical aspects and data safety
The study will be conducted in accordance with the Guidelines for Assuring Good Scientific Practice and the Principles and Responsibilities for the Conduct of Clinical Trials of the German Research Foundation (DFG). An ethics vote in support of the project has been obtained from the Local Psychological Ethics Committee of the Center of Psychosocial Medicine at the University Medical Center Hamburg-Eppendorf (LPEK-0078a). The study will be conducted in accordance with the Declaration of Helsinki. Any adverse events will be documented and reported {22}. Participants must sign informed consent prior to study participation, which informs them about the study procedure, data protection risks and compensation, and their right to withdraw from participation at any time without giving a reason. If they withdraw, all their data will be deleted.
The research project will be carried out in accordance with the EU General Data Protection Regulation. All other data will be stored on password-protected computers. Data collection will be conducted online using the survey software Qualtrics®, which guarantees high data protection standards such as end-to-end encryption. After completion of the study, the collected data will be archived for 10 years (e-mail addresses will be deleted after the end of the study). The clinical principal investigator (PI) will be responsible to carry out the study in accordance with the study protocol {5d}. The PI will ensure that everyone working in the research project is sufficiently qualified.
Current study status
Trial start date: November 8th 2021 (first participant was enrolled).
Recruitment is completed.
Discussion
Lenio is a novel Internet-based self-help intervention addressing symptoms of both chronic pain and depression. Whereas there is good evidence for the effectiveness of Internet-based interventions (guided and unguided) for depression and other mental disorders [8, 25, 30], programs targeting chronic pain and depressive symptoms are rare and often poorly validated, with a lack of data on long-term effects [6, 31]. RCTs with high methodological standards that examine both the short-term and long-term effects of Internet-based interventions for people with chronic pain and comorbid depression in large samples are scarce.
In the present study, we aim to evaluate the feasibility, effectiveness, and acceptance of Lenio in an RCT. To do so, we intend to reach out to individuals who either have not (yet) sought conventional face-to-face therapy or who are seeking complementary treatment, thus narrowing the existing treatment gap. The advantages of Internet-based interventions such as Lenio are their low cost, anonymity, flexibility, and low-threshold access. To the best of our knowledge, no Internet-based program exists that concurrently treats patients with both chronic pain and comorbid depressive symptoms. To offer complete anonymity for participants, we developed an unguided Internet-based intervention. Offering direct support might increase effectiveness but could also prevent patients from participating due to fear or self-stigmatization.
To increase adherence, we developed a smartphone app to be used in combination with Lenio. In addition, e-mail reminders will remind participants to access and use the program. Moreover, we integrated a welcome module containing motivational interviewing techniques to increase participants’ motivation to work on psychological aspects of their chronic pain. Within the welcome module, participants will receive an individualized recommendation of the modules most effective for them. Personal goals can be set and easily adjusted at any time.
One possibility for the future is that Lenio could be used as an after-care tool (e.g., after inpatient treatment) to prevent relapse. In addition, due to limited resources (e.g., too few specialists) patients currently have long wait times before they can start therapy. Internet-based interventions could be used to bridge this waiting time and provide patients with psychoeducational information and psychotherapeutic interventions. When they later start therapy, the time gained can be used to address other aspects (e.g., interpersonal problems, comorbidities) of treatment. Furthermore, participation in an Internet-based intervention could facilitate motivation to engage in face-to-face treatment and thus prepare patients for conventional face-to-face therapy. To shed light on the question of which baseline characteristics affect the outcome (e.g., if no add-on effects emerged when Lenio is used in addition to standard treatment), a moderation analysis will be calculated.
Currently, CBT interventions are most effective for patients with chronic pain and for depressed patients [22]. Lenio is based on CBT and its third-wave techniques. We expect to add to the understanding of the feasibility, effectiveness, and acceptance of Internet-based interventions for people with chronic pain and depressive symptoms. We expect that Lenio will significantly reduce chronic pain impairment as well as depressive symptoms when compared to the control groups (waitlist control group and active control group). In addition, we expect that the effects will be maintained long term as assessed by the follow-up measurement 4 months after the baseline assessment.
Trial status
Protocol version 03/22/2023. Second revision.
Any future changes to the study protocol will be recorded in separate amendment. See Table 4 for a detailed SPIRIT 2013 Checklist.
Availability of data and materials {29}
Data is available upon request.
Data will be communicated via publications on peer-reviewed journals and poster presentations or oral presentations at conferences.
Abbreviations
- BDI-II:
-
Beck Depression Inventory-II
- CEQ:
-
Credibility/Expectancy Questionnaire
- DSF:
-
German Pain Questoinnaire
- FABQ:
-
Fear-Avoidance Beliefs Questionnaire
- PSEQ:
-
Pain Self-Efficacy Questionnaire
- IEQ:
-
Injustice Experience Quesstionnaire
- PCS:
-
Pain Catastrophizing Scale
- CBT:
-
Cognitive-behavioral therapy
- RCT:
-
Randomized controlled trial
- PHQ-9:
-
Patient Health Questionnaire-9
- URICA:
-
University of Rhode Island Change Assessment
- WHQOL-BREF:
-
World Health Organization Quality of Life abbreviated version
- WSQ:
-
Web Screening Questionnaire
References
Barak A, Hen L, Boniel-Nissim M, Shapira N. A comprehensive review and a meta-analysis of the effectiveness of internet-based psychotherapeutic interventions. J Technol Hum Serv. 2008;26(2–4):109–60. https://doi.org/10.1080/15228830802094429.
Beard C, Hsu KJ, Rifkin LS, Busch AB, Björgvinsson T. Validation of the PHQ-9 in a psychiatric sample. J Affect Disord. 2016;193:267–73. https://doi.org/10.1016/j.jad.2015.12.075.
Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. 1996.
Borkovec TD, Nau SD. Credibility of analogue therapy rationales. J Behav Ther Exp Psychiatry. 1972;3(4):257–60. https://doi.org/10.1016/0005-7916(72)90045-6.
Bruhns A, LüdtkeT, Moritz S, Bücker L. A mobile-based intervention to increase self-esteem in students with depressive symptoms: Randomized controlled trial. JMIR MHealth and UHealth. 2021;9(7). https://doi.org/10.2196/26498
Buhrman M, Gordh T, Andersson G. Internet interventions for chronic pain including headache: A systematic review. Internet Interv. 2016;4:17–34. https://doi.org/10.1016/j.invent.2015.12.001.
Byrne BM, Stewart SM, Kennard BD, Lee PWH. The Beck Depression Inventory-II: Testing for measurement equivalence and factor mean differences across Hong Kong and American adolescents. Int J Test. 2007;7(3):293–309. https://doi.org/10.1080/15305050701438058.
Carlbring P, Andersson G, Cuijpers P, Riper H, Hedman-Lagerlöf E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: an updated systematic review and meta-analysis. Cognitive Behaviour Therapy. 2018;47(1):1–18. https://doi.org/10.1080/16506073.2017.1401115.
Casser HR, Hüppe M, Kohlmann T, Korb J, Lindena G, Maier C, Nagel B, Pfingsten M, Thoma R. Deutscher Schmerzfragebogen (DSF) und standardisierte Dokumentation mit KEDOQ-Schmerz. Auf dem Weg zur gemeinsamen Qualitätsentwicklung der Schmerztherapie. Schmerz. 2012;26(2):168–75. https://doi.org/10.1007/s00482-011-1142-0.
Clauw DJ, Essex MN, Pitman V, Jones KD. Reframing chronic pain as a disease, not a symptom: Rationale and implications for pain management. Postgrad Med. 2019;131(3):185–98. https://doi.org/10.1080/00325481.2019.1574403.
Clement S, Schauman O, Graham T, Maggioni F, Evans-Lacko S, Bezborodovs N, Morgan C, Rüsch N, Brown JSL, Thornicroft G. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol Med. 2015;45(1):11–27. https://doi.org/10.1017/S0033291714000129.
Devilly GJ, Borkovec TD. Psychometric properties of the credibility/ expectancy questionnaire. J Behav Ther Exp Psychiatry. 2000;31
Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, Watson PL, Weinhouse GL, Nunnally ME, Rochwerg B, Balas MC, van den Boogaard M, Bosma KJ, Brummel NE, Chanques G, Denehy L, Drouot X, Fraser GL, Harris JE, … Alhazzani W. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9). https://doi.org/10.1097/CCM.0000000000003299
Donker T, van Straten A, Marks I, Cuijpers P. A brief web-based screening questionnaire for common mental disorders: Development and validation. J Med Internet Res. 2009;11(3). https://doi.org/10.2196/jmir.1134
Dozois DJA, Westra HA, Collins KA, Fung TS, Garry JKF. Stages of change in anxiety: Psychometric properties of the University of Rhode Island Change Assessment (URICA) scale. Behav Res Ther. 2004;42(6):711–29. https://doi.org/10.1016/S0005-7967(03)00193-1.
Duenas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Re. 2016;9. https://doi.org/10.2147/JPR.S105892
García-Batista ZE, Guerra-Peña K, Cano-Vindel A, Herrera-Martínez SX, Medrano LA. Validity and reliability of the beck depression inventory (BDI-II) in general and hospital population of Dominican Republic. PLoS ONE. 2018;13(6). https://doi.org/10.1371/journal.pone.0199750
Goesling J, Lin LA, Clauw DJ. Psychiatry and pain management: At the intersection of chronic pain and mental health. Current Psychiatry Reports. 2018;20(2). https://doi.org/10.1007/s11920-018-0872-4
Hasler G, Klaghofer R, Buddeberg C. The University of Rhode Island Change Assessment Scale (URICA) Psychometric Testing of a German Version. PPmP Psychotherapie Psychosomatik Medizinische Psychologie. 2003;53(9–10):406–11. https://doi.org/10.1055/s-2003-42172.
Hayes AF. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling 1. http://www.afhayes.com/
Hedman-Lagerlöf M, Hedman-Lagerlöf E, Ljótsson B, Wicksell RK, Flink I, Andersson E. Cost-effectiveness and cost-utility of internet-delivered exposure therapy for fibromyalgia: Results from a randomized, controlled trial. J Pain. 2019;20(1):47–59. https://doi.org/10.1016/j.jpain.2018.07.012.
Hughes LS, Clark J, Colclough JA, Dale E, McMillan D. Acceptance and commitment therapy (ACT) for chronic pain. Clin J Pain. 2017;33(6):552–68. https://doi.org/10.1097/AJP.0000000000000425. (Lippincott Williams and Wilkins).
Ilić I, Šipetić S, Grujičić J, Mačužić IŽ, Kocić S, Ilić M. Psychometric properties of the world health organization’s quality of life (WHOQOL-BREF) questionnaire in medical students. Medicina (Lithuania). 2019;55(12). https://doi.org/10.3390/medicina55120772
Schmidt J, Lamprecht F, Wittmann WW. Zufrie- denheit mit der stationären Versorgung. Ent- wicklung eines Fragebogens und erste Va- liditätsuntersuchungen. Psychother Psycho- som.
Karyotaki E, EfthimiouO, Miguel C, Bermpohl FMG, Furukawa TA, Cuijpers P, Riper H, Patel V, Mira A, Gemmil AW, Yeung AS, Lange A, Williams AD, Mackinnon A, Geraedts A, van Straten A, Meyer B, Björkelund C, Knaevelsrud C, … Forsell Y. Internet-based cognitive behavioral therapy for depression: A systematic review and individual patient data network meta-analysis. JAMA Psychiatry. 2021;78(4), 361–371. https://doi.org/10.1001/jamapsychiatry.2020.4364
Karyotaki E, Riper H, Twisk J, Hoogendoorn A, Kleiboer A, Mira A, MacKinnon A, Meyer B, Botella C, Littlewood E, Andersson G, Christensen H, Klein JP, Schröder J, Bretón-López J, Scheider J, Griffiths K, Farrer L, Huibers MJH, … Cuijpers P. Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms a meta-analysis of individual participant data. JAMA Psychiatry. 2017;74(4), 351–359. https://doi.org/10.1001/jamapsychiatry.2017.0044
Kovacs FM, Muriel A, Medina JM, Abraira V, Sánchez MD, Jaúregui JO; the Spanish Back Pain Research Network. Psychometric characteristics of the Spanish version of the FAB questionnaire. Spine. 2006;31(1):104-10. https://doi.org/10.1097/01.brs.0000193912.36742.4f.
Kriz D, Nübling R, Steffanowski A, Wittmann WW, Schmidt J. Patientenzufriedenheit in der stationären Rehabilitation: Psychometrische Reanalyse des ZUF-8 auf der Basis multizentrischer Stichproben verschiedener Indikation. Zeitschrift Für Medizinische Psychologie. 2008;17(October 2015):67–79.
Kroenke K, Spitzer RL. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr Ann. 2002;32(9):509–15. https://doi.org/10.3928/0048-5713-20020901-06.
Lal S, Adair CE. E-mental health: A rapid review of the literature. Psychiatr Serv. 2014;65(1):24–32. https://doi.org/10.1176/appi.ps.201300009.
Lin J, Paganini S, Sander L, Lüking M, Daniel Ebert D, Buhrman M, Andersson G, Baumeister H. An Internet-based intervention for chronic pain - A three-arm randomized controlled study of the effectiveness of guided and unguided acceptance and commitment therapy. Deutsches Arzteblatt International. 2017;114(41):681–8. https://doi.org/10.3238/arztebl.2017.0681.
Linder J, Jansen G, Ekholm K, Ekholm J. Relationship between sleep disturbance, pain, depression and functioning in long-term sick-listed patients experiencing difficulty in resuming work. J Rehab Med. 2014;46(8). https://doi.org/10.2340/16501977-1833
Lüdtke T, Pult LK, Schröder J, Moritz S, Bücker L. A randomized controlled trial on a smartphone self-help application (Be Good to Yourself) to reduce depressive symptoms. Psychiatry Res. 2018;269:753–62. https://doi.org/10.1016/j.psychres.2018.08.113.
Mangels M, Schwarz S, Sohr G, Holme M, Rief W. Eine Adaptation des Pain Self-Efficacy Questionnaire für den deutschen Sprachraum. Diagnostica. 2009;55(2):84–93. https://doi.org/10.1026/0012-1924.55.2.84.
McConnaughy EA, Prochaska JO, Velicer WF. Stages of change in psychotherapy: Measurement and sample profiles. Psychotherapy: Theory, Research & Practice. 1983;20(3):368–75. https://doi.org/10.1037/h0090198.
Meldrum ML. Pain. Encyclopedia Britannica. 2021.
Melzack R, Wall PD. Gate-control-pain mechanisms - a new theory. Science. 1965;150(3699):971–979). https://www.canonsociaalwerk.eu/1846_anesthesie/Canon Palliatieve Zorg - Ontstaan van anesthesie - Science - melzackandwallgatecontroltheory.pdf
Michaelides A, Zis P. Depression, anxiety and acute pain: Links and management challenges. Postgraduate Med. 2019;131(7). https://doi.org/10.1080/00325481.2019.1663705
Miegel F, Gehlenborg J, Bücker L, Lion D, Moritz S. Kann eine Online-Intervention für Depressionen emotionale Probleme und Schmerzen lindern? Eine randomisiert-kontrollierte Studie. Verhaltenstherapie. 2019;166–181. https://doi.org/10.1159/000501736
Moritz S, Nestoriuc Y, Rief W, Klein JP, Jelinek L, Peth J. It can’t hurt, right? Adverse effects of psychotherapy in patients with depression. Eur Arch Psychiatry Clin Neurosci. 2019;269(5):577–86. https://doi.org/10.1007/s00406-018-0931-1.
Nagel B, Gerbershagen HU, Lindena G, Pfingsten M. Entwicklung und empirische überprüfung des Deutschen schmerzfragebogens der DGSS. Schmerz. 2002;16(4):263–70. https://doi.org/10.1007/s00482-002-0162-1.
Peth J, Jelinek L, Nestoriuc Y, Moritz S. Adverse effects of psychotherapy in depressed patients—First application of the Positive and Negative Effect of Psychotherapy Scale (PANEPS). PPmP Psychotherapie Psychosomatik Medizinische Psychologie. 2018;68(910):391–8.
Poole H, Bramwell R, Murphy P. Factor Structure of the Beck Depression Inventory-II in patients With chronic pain. Clin J Pain. 2006;22(9):790-8. https://doi.org/10.1097/01.ajp.0000210930.20322.93.
Poole H, White S, Blake C, Murphy P, Bramwell R. Depression in chronic pain patients: Prevalence and measurement. Pain Pract. 2009;9(3):173–80. https://doi.org/10.1111/j.1533-2500.2009.00274.x.
Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing a critical review. Expert Rev Neurotherapeutics. 2009;9(5):745–58. https://doi.org/10.1586/ern.09.34.
Richards D, Richardson T. Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev. 2012;32(4):329-42. https://doi.org/10.1016/j.cpr.2012.02.004.
Roditi D. The role of psychological interventions in the management of patients with chronic pain. Psychol Res Behav Manag. 2011. https://doi.org/10.2147/PRBM.S15375.
Simister HD, Tkachuk GA, Shay BL, Vincent N, Pear JJ, Skrabek RQ. Randomized controlled trial of online acceptance and commitment therapy for fibromyalgia. J Pain. 2018;19(7):741–53. https://doi.org/10.1016/j.jpain.2018.02.004.
Simon LS. Relieving pain in america. A blueprint for transforming preventions, care, education, and research. J Pain Paliat Care Pharmacother. 2021;
Sullivan MJL, Adams H, Horan S, Maher D, Boland D, Gross R. The role of perceived injustice in the experience of chronic pain and disability: Scale development and validation. J Occup Rehabil. 2008;18(3):249–61. https://doi.org/10.1007/s10926-008-9140-5.
Titov N, Dear BF, Johnston L, Lorian C, Zou J, Wootton B, Spence J, McEvoy PM, Rapee RM. Improving adherence and clinical outcomes in self-guided internet treatment for anxiety and depression: Randomised controlled trial. PLoS ONE. 2013;8(7). https://doi.org/10.1371/journal.pone.0062873
Veehof MM, Trompetter HR, Bohlmeijer ET, Schreurs KMG. Acceptance- and mindfulness-based interventions for the treatment of chronic pain: A meta-analytic review. Cognitive Behav Ther. 2016;45(1):5–31. https://doi.org/10.1080/16506073.2015.1098724. (Routledge).
von Korff M, Ormel J, Keefe FJ, Dworkin SF. Clinical Section Grading the severity of chronic pain. 1092.
Vos T, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, Abdulkader RS, Abdulle AM, Abebo TA, Abera SF, Aboyans V, Abu-Raddad LJ, Ackerman IN, Adamu AA, Adetokunboh O, Afarideh M, Afshin A, Agarwal SK, Aggarwal R, … Murray CJL. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. https://doi.org/10.1016/S0140-6736(17)32154-2
Vowles KE, Pielech M, Edwards KA, McEntee ML, Bailey RW. A comparative meta-analysis of unidisciplinary psychology and interdisciplinary treatment outcomes following acceptance and commitment therapy for adults with chronic pain. J Pain. 2020;21(5–6):529–45. https://doi.org/10.1016/j.jpain.2019.10.004. (Churchill Livingstone Inc).
Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157-68. https://doi.org/10.1016/0304-3959(93)90127-B.
Acknowledgements
We would like to thank Arne Sibilis for his contribution to the development and maintenance of the “Lenio” Online-Program.
Related articles
This manuscript or any publication regarding this study was neither submitted nor published in any other journal.
Revision chronology
... 2022-Mar-24: | Original |
... 2022-Aug-11: | Amendment 01.: Primary reason for amendment: Major adjustments to the SPIRIT guidelines |
... 2023-Mar-22: | Amendment 02: Primary reason for amendment: Further adjustments to the SPIRIT guidelines |
Funding
Open Access funding enabled and organized by Projekt DEAL. This study is funded by the DGUV (Deutsche Gesetzliche Unfallversicherung). The funding bodies played no role in the analysis and interpretation of data or in writing the manuscript. The funding bodies supported the data collection by establishing contact to cooperation partners.
Author information
Authors and Affiliations
Contributions
SB wrote a draft of the manuscript and will be responsible for the data collection. JG, SB, and SM designed the study and edited the manuscript. SM will supervise all stages of the research project. All authors contribute to the project, read the manuscript, and approved the final version. SB, JG, and SM will be involved in the data acquisition, data analysis, interpretation, and writing of the final report. A student assistant (AW) will also be involved in data acquisition, data analysis, interpretation, and writing of the final report. No professional writer will be hired.
Corresponding author
Ethics declarations
Ethics approval and consent to participate {24}
The study has been approved by the local psychological ethics committee (Lokale Psychologische Ethikkommission) at the center for psychosocial medicine (Universitätsklinikum Hamburg-Eppendorf, Martinistraße 52, 20246 Hamburg, www.uke.de) (ID: LPEK-0078a). Electronical informed consent to participate in the study is being obtained from every participant {27}.
Consent for publication {32}
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Borsutzky, S., Moritz, S., Hottenrott, B. et al. A self-guided Internet-based intervention for individuals with chronic pain and depressive symptoms: study protocol of a randomized controlled trial. Trials 24, 453 (2023). https://doi.org/10.1186/s13063-023-07440-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-023-07440-8