
Abstract
Introduction
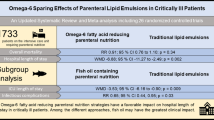
Early data suggest use of a mixed lipid emulsion (LE) with a soybean oil reduction strategy in parenteral nutrition (PN) may improve clinical outcomes. Duke University Hospital made a full switch to a Soybean oil/MCT/Olive/Fish Oil lipid (4-OLE) from pure soybean oil-based LE (Intralipid, Baxter Inc) in May 2017. Since 4-OLE has limited evidence related to its effects on clinical outcome parameters in US hospitals, evidence for clinical benefits of switching to 4-OLE is needed. Therefore, we examined the clinical utility of a hospital-wide switch to 4-OLE and its effect on patient outcomes.
Methods
We conducted a single-center retrospective cohort study among adult patients (> 18 years) requiring PN from 2016 to 2019. Our primary exposure was treatment period (1-year pre-4-OLE switch versus 2-year post). We used multivariable regression models to examine our primary outcomes, the association of treatment period with hospital length of stay (LOS), and secondary outcomes liver function, infections, and ICU LOS. Analyses were stratified into critically ill and entire adult cohort.
Results
We identified 1200 adults hospitalized patients. 28% of PN patients (n = 341) were treated pre-4-OLE switch and 72% post-4-OLE (n = 859). In the adult cohort, 4-OLE was associated with shorter hospital LOS (IRR 0.97, 95% CI 0.95–0.99, p = 0.039). The ICU cohort included 447 subjects, of which 25% (n = 110) were treated pre-4-OLE switch and 75% (n = 337) were post-switch. ICU patients receiving 4-OLE were associated with shorter hospital LOS (IRR 0.91, 95% CI 0.87–0.93, p < 0.0001), as well as a shorter ICU LOS (IRR 0.90, 95% CI 0.82–0.99, p = 0.036). 4-OLE ICU patients also had a significantly lower delta total bilirubin (− 1.6, 95% CI − 2.8 to − 0.2, p = 0.021) and reduced urinary tract infection (UTI) rates (OR 0.50, 95% CI 0.26–0.96, p = 0.038). There were no associations in AST, ALT, or total bilirubin in ICU and all adult patients.
Conclusion
4-OLE was successfully implemented and reduced soybean oil LE exposure in a large academic hospital setting. The introduction of 4-OLE was associated with reduced LOS, UTI rates, and mitigated hepatic dysfunction in critically ill patients. Overall, these findings prove a switch to a soybean oil-LE sparing strategy using 4-OLE is feasible and safe and is associated with improved clinical outcomes in adult PN patients.
Similar content being viewed by others


Introduction
Moderate-to-severe malnutrition is associated with an increased risk of mortality, infections, hospital length of stay, and higher healthcare-associated costs, especially in critically ill patients [1,2,3,4,5]. Historically, the use of various modalities to combat malnutrition in critical illness has primarily consisted of enteral and parenteral based nutritional support regimens. Parenteral nutrition (PN) is advocated for when enteral nutrition (EN) cannot be administered, such as those with recent abdominal surgery and/or GI intolerance, and is therefore recommended by current American Society for Parenteral and Enteral Nutrition (ASPEN) guidelines [6]. However, the use of PN, specifically the composition of traditional lipid emulsions (LE), is suggested to have detrimental effects on critically ill patients.
Pure soybean oil-based LEs have been predominantly used in the USA and have been implicated in the adverse outcomes related to PN. The use of soybean oil-based LE has been shown to propagate a pro-inflammatory cascade and increase reactive oxidative stress [7,8,9]. In severe critical illness, soybean oil-based LE has been shown to impair cellular-mediated immunity with amplification of IL-6 levels [9, 10]. Additionally, soybean oil-based emulsions are known to impair chemotaxis and phagocytotic ability, increasing bacteremia and infection risks [9, 11,12,13,14]. Traditionally, soybean oil-based LE also worsens hepatic dysfunction and cholestasis risks [15].
The negative effects seen with soybean oil-based emulsions are thought to be largely due to the high content of long-chain triglycerides and omega-6 fatty acids, inherent with pro-inflammatory properties. Given the issues surrounding traditional soybean oil-based LE, the use of “soybean oil-sparing” or “omega-6 sparing” strategies has come to the forefront of nutritional support in critical care [16, 17]. These strategies include mixed formulations with various compositions of medium-chain triglycerides, fish oil, and/or olive oil-based emulsions [16, 17]. The rationale behind this strategy is to increase the percentage of the key beneficial omega-3 fatty acids of EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) that have beneficial immunomodulating effects, including reduced inflammatory cytokine production [7, 18]. The benefit of EPA and DHA supplementation is due to active metabolites called resolvins, limiting inflammation and additional end-organ injury [19]. A systematic review found that soybean oil-reducing strategies, including use of lipid preparations with increased amounts of EPA and DHA containing lipids, may decrease intensive care unit (ICU) length of stay (LOS), hospital LOS, and time on the ventilator [20]. This same analysis failed to demonstrate any benefit in mortality with this strategy [20]. Related literature coincides with a lack of conclusive evidence to support soybean oil reduction strategies or their benefit on mortality [21,22,23].
Despite the controversy and paucity of the literature to support its use, “soybean oil-sparing” strategies are recommended for patients requiring PN [24, 25]. Of these varieties, one specific mixed-oil-based LE that has demonstrated increased interest and use outside of the USA is SMOFLipid (4-OLE), which is a mixture of 3 g soybean oil, 3 g medium-chain triglycerides, 2.5 g olive oil, 1.5 g fish oil, 200 mg alpha-tocopherol and 47.6 mg phytosterols per 100 ml of emulsion [26]. This type of LE contains 15% of the lipid as fish oil which contains 30% of the fish oil as EPA and DHA. Thus, this 4-OLE lipid has a 5% EPA + DHA acid composition which may convey potential anti-inflammatory properties discussed previously [19, 26]. A recent meta-analysis found significant benefits to LEs which reduce soybean oil content (and contain added EPA + DHA) showing reduced rates of sepsis, infection, and length of stay [27]. However, this study failed to show mortality benefits using soybean oil-reducing with added EPA/DHA-based LE supplementation [27]. Duke University Health System recently implemented 4-OLE as part of its PN regimen. Given the lack of evidence related to 4-OLE use and its relative infancy as an option for LE supplementation, the objective of this study was to investigate the clinical effect of 4-OLE supplementation after widespread implementation in an adult hospital population.
Methods
Study design and population
We conducted a retrospective cohort study using electronic health record data from 2016 to 2018. This study was reviewed by the Duke Institutional and Ethics Review Board and was granted approval (Approval Number: Pro00102602). In the pure soybean oil-based group (IL), all adult patients receiving PN with any lipid delivery from May 16, 2016–May 16, 2017, were included in analysis. This constituted one year prior to the full switch over from IL to 4-OLE at Duke University Hospital in all PN patients without contraindications (i.e., allergy) on May 16, 2017. The 4-OLE group consisted of all adult patients receiving PN with SMOFLipid from May 17, 2017–September, 1, 2019. Patients after May 17, 2016, who received IL due to an allergy to a 4-OLE component were excluded from analysis. Only 1 year prior to switch to 4-OLE was chosen to minimize effects of any potential changes in clinical practice on outcomes. Inclusion criteria were adults, defined as age ≥ 18 years of age, who required PN initiation for adequate goal nutrition. A subgroup analysis was performed those who required an ICU level of care.
The following data were collected for each patient: age, sex, race, ethnicity, body mass index (BMI), insurance status, ICU location, emergency department (ED) admission, ICU admission, malnutrition at admission, comorbidities using the binary Elixhauser’s comorbidity indicators [28], PN utilization profile (type of lipid emulsion and dose of lipids, protein, dextrose in g/kg/d, duration), hospital outcomes (ICU length of stay, hospital length of stay, in-hospital mortality, 30-day readmission, and 90-day readmission), infections (pneumonia, urinary tract infection, and all infections), mechanical ventilation, statin use, insulin use, antibiotic use, laboratory values (aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), total bilirubin, blood glucose, C-reactive protein, and triglycerides). Comorbidities and infections were identified using the International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes.
Exposure
Patients from 2016 to May 2017 prior to the change (Intralipid (IL) (Baxter Inc, Deerfield, IL, USA) group) were compared with patients from May 2017 to 2019 after the clinical change (4-OLE group).
Outcomes
The primary outcome was hospital LOS. Secondary outcomes included hospital mortality, 30-day readmission, ICU LOS, all-cause infections, calorie delivery, liver function tests (AST, ALT, ALP, and total bilirubin). We calculated delta values by subtracting initial values from max values.
Covariates
The following covariates were used in the analysis: age, sex, race, ethnicity, insurance status, cancer, malnutrition, ED admission, ICU admission, and BMI.
Statistical analysis
Descriptive statistics were calculated and presented as number (percentage) for categorical variables and median (interquartile range) or mean ± standard deviation (SD) for continuous variables. Continuous variables were compared using an unpaired t test or a Wilcoxon test. Pearson’s chi-squared test or Fisher’s exact test was used for categorical data.
We used multivariable Poisson regression models to analyze the association between 4-OLE and LOS. Coefficients in the Poisson model were exponentiated to obtain incidence rate ratios (IRRs). We used multivariable linear regression models for nutrition delivery variables and liver functions tests. We used multivariable logistic regression models for hospital mortality and 30-day readmission. All covariates above were included in the models. We stratified the cohort to patients admitted to ICU in the sensitivity analysis and performed the same analysis mentioned above except for covariates. (ICU admission was not included in the covariates.) We performed the complete case analysis—the type I error rate was set at 0.05 as the threshold for statistical significance. Statistical analyses were performed using SAS version 9.4 (SAS Institute; Cary, NC).
Results
Demographic and clinical characteristics in adults
We identified 1200 adults. 28% of PN patients (n = 341) received Intralipid (Baxter Inc, Deerfield, IL, USA (IL)) pre-switch and 72% received 4-OLE (n = 859). Median age of the overall cohort (58.5 years old, range 44–68 years, p = 0.049) was statistically different with the IL group having a slightly younger population (56 years old, range 42–67, p = 0.049) in Table 1. There was no significant difference in BMI (25.5 kg/m2, 21.6–29.6, p = 0.81) or in sex distribution between both cohorts. Baseline liver function tests were similar between the two groups. However, the 4-OLE group had significantly smaller number of patients with renal failure (10.4% vs 16.7%, p = 0.002), congestive heart failure (CHF) (8.7%vs 13.5%, p = 0.014), and underlying malignancy (18.4% vs 26.1%, p = 0.003).
Nutrition profiles and liver function tests are summarized in Table 2. 4-OLE was associated with higher ALP (29.0, 95% CI 6.2–51.8, p = 0.013). 4-OLE use was also associated with higher daily lipid dosage (0.06, 95% CI 0.01–0.11, p = 0.018).
Association of switch to 4-OLE with clinical outcomes
In adult patients, crude outcomes are summarized in Table 3. In multivariable regression models, 4-OLE was associated with a reduced LOS [incident rate ratio (IRR) 0.97, 95% CI 0.95–0.99, p = 0.039] (Table 3). However, overall infectious complications of any kind nor hospital mortality were different between groups. There was also no significant difference in 30 and 90 day readmission rates.
Demographic and clinical characteristics in critically ill patients
The ICU cohort included 447 total subjects, of which 25% (n = 110) received Intralipid (Baxter Inc, Deerfield, IL, USA) (IL) and 75% (n = 337) received 4-OLE (Table 4). The median age (61 years old, 47–70) and BMI (26.8 kg/m2, 22.1–30.9) for the total cohort were similar between both groups. 4-OLE patients were less likely to have liver disease (9.2% vs 16.4%, p = 0.03) and renal failure (13.1% vs 29.1%, p < 0.001). Statin use was significantly greater in the 4-OLE cohort, and insulin use was higher in the IL cohort. Baseline liver function tests were found to be similar in both groups.
Table 5 provides details regarding nutrition profiles and liver function tests in the ICU cohort. 4-OLE was not associated with total bilirubin, AST, ALT, ALP, or TG. 4-OLE use was also associated with higher daily lipid dosage (0.06, 95% CI 0.01 to 0.11, p = 0.018) (Table 5).
Association of switch to 4-OLE with clinical outcomes in critically ill patients
The crude outcomes are shown in Table 6. In multivariable regression models, we observed significant findings in comparing IL to 4-OLE patients in the ICU adult cohort with a significantly shorter hospital LOS (IRR 0.91, 95% CI 0.87–0.94, p < 0.0001) as well as a shorter ICU LOS (IRR 0.90, 95% CI 0.82–0.99, p = 0.036) (Table 6). 4-OLE was associated with reduced urinary tract infections (UTI) (odds ratio 0.50, 95% CI 0.26–0.96, p = 0.038). 4-OLE use was not associated with overall infections, hospital mortality, nor 30- or 90-day readmission rates.
Discussion
This study is among the first to examine a switch to a soybean oil-sparing LE strategy in PN patients to demonstrate significant clinical benefits after the successful widespread implementation of 4-OLE in a hospital-wide fashion. Our data show the use of 4-OLE was associated with a shorter hospital LOS in both critically ill and all hospitalized patients and a shorter ICU LOS. The switch to 4-OLE from Intralipid (Baxter Inc, Deerfield, IL, USA) also demonstrated a significant reduction in total bilirubin from baseline levels in ICU patients and reduced TG levels in all adult patients. The switch to 4-OLE was also found to lead to a reduced risk of UTIs in the critically ill cohort.
These data are also among the first to describe a successful switch to a soybean oil-lipid sparing strategy using 4-OLE in a US hospital system. The use of a soybean oil-sparing strategy for PN regimens has long been advocated to limit the adverse effects associated with traditional lipid emulsions [6, 16, 17]. However, evidence describing outcomes and benefits of a full-scale switch in all hospitalized adult PN patients (not just ICU patients or higher-risk PN patients) use have not previously been described in a US healthcare setting. This study is the first to demonstrate significant benefits of a full-scale switch to a soybean oil-LE sparing strategy in a hospital setting. These data would support a soybean oil-LE sparing strategy in all hospitalized adult PN patients using 4-OLE.
Specifically, a switch to 4-OLE use was associated with reductions in hospital LOS and ICU LOS. Previous studies have reported a trend toward a decrease in LOS when soybean oil-sparing LE strategies have been employed, with some evidence suggesting that a reduced omega-6 LE content reduces ICU LOS [20]. Our data are consistent with this very recent meta-analysis of omega-6 sparing parenteral lipid emulsions showing substantial hospital LOS reductions [6 studies; weighted mean difference (WMD) − 6.88; 95% CI − 11.27, − 2.49; p = 0.002] in patients receiving an omega-6 sparing strategy [20]. Specific to fish oil (FO) containing lipid emulsions which increase EPA + DHA delivery, such as 4-OLE examined in our study, this same meta-analysis found FO-containing PN reduced the length of intensive care (8 studies; WMD − 3.53; 95% CI − 6.16, − 0.90; p = 0.009) as seen in our real-world hospital data. In these data, the use of 4-OLE was provided for both a significantly earlier hospital discharge and ICU discharge with no significant differences in readmission rates at 30 and 90 days. Although hospital costs could not be evaluated in this study, it can be expected that the reduced hospital and ICU LOS associated with a switch to 4-OLE use may also be associated with a reduction in costs related to reduced LOS [29].
We also observed some benefits of a soybean oil-LE sparing strategy with 4-OLE on infectious complications in our analysis. The literature has long reported the associated complication risks related to traditional LE. These are largely due to the pro-inflammatory and immune system hampering effects of its high omega-6 fatty acid composition [7,8,9]. Thus, traditional LE has been associated with infectious complications ranging from bacteremia to profound sepsis [11,12,13]. The results of 4-OLE use in this study demonstrated a reduced incidence of UTIs, specifically in the ICU population. Previous literature has reported a reduction in septic complications by up to 56% when soybean oil-sparing LE enriched with EPH + DHA has been used [27]. Our data are also consistent with the aforementioned very recent meta-analysis of omega-6 sparing parenteral lipid emulsions in ICU patients where the risk of infectious complications was reduced in ICU patients receiving soybean oil-sparing LE with added EPA + DHA (4 studies; RR 0.65; 95% CI 0.44, 0.95; p = 0.03).
4-OLE patients in this study also showed no difference in LE associated hepatic dysfunction. We observed no significant elevations in liver function parameters in both critically ill and all adult patients, except for minor elevations of ALP in this all adult cohort. Given that observed ALP elevation was isolated with no concomitant rise in AST, ALT, or total bilirubin levels, this elevation could be explained by bile stasis commonly seen in PN patients without associated hepatosteatosis [30]. In contrast, patients post-switch to 4-OLE were found to have improved TG and reductions in elevation of total bilirubin levels in a cohort with more extensive liver and renal disease.
PN-associated hepatic dysfunction in the adult population can vary from benign elevations to causes such as sepsis-related cholestasis [31]. However, the hepatic dysfunction with traditional soybean oil LE can manifest as hypertriglyceridemia which can increase pancreatitis risk as well as potential increased risk of mortality, particularly in prolonged use [31, 32]. Typical strategies to combat this dysfunction involve reducing lipid infusion rates which often create a more significant calorie debt in already malnourished patients or a need for increased glucose delivery, which can be associated with worsened hyperglycemia and adverse outcomes [32]. Thus, the observed effects of 4-OLE on mitigating hepatic dysfunction in this study may help avoid these potential complications and can again be explained by the mixed composition of the LE, which has been proven to lower the risk of liver dysfunction [33]. Recent lipid dosing guidelines have called for a recommendation of 1–2 g/kg/d delivery for 4-OLE formulations [34]. In the period when our data were collected, we had agreed to continue a similar lipid dosing strategy that had been utilized when we previously used the traditional soybean LE to assess safety and outcomes of this new lipid formulation in our hospital. Given the data presented here for safety and signals of improved clinical outcomes, we have begun to increase our clinical 4-OLE delivery closer to 1 g/kg/d in most patients. It is possible that increasing this dose and thereby delivering additional fish oil (and importantly EPA/DHA) may further improve clinical outcomes and potentially show additional benefit in reducing elevations in liver function measures. Further studies will be needed to explore this.
Overall, the observed results in this study provide further evidence supporting a switch to soybean oil-LE sparing strategy using 4-OLE in all hospitalized adult PN patients, and not just selected groups (i.e., ICU or high risk patients). Our data demonstrating the successful implementation of 4-OLE hospital-wide are the first of its kind, and this analysis demonstrates that this switch to a soybean oil-LE sparing strategy is associated with safety and clinical benefit. The hospital-wide switch to 4-OLE reduced overall and ICU LOS compared to traditional IL use. Its use also significantly reduced the risk of UTIs and hepatic dysfunction, with decreased TG and total bilirubin levels in a hospital-wide patient population. Overall, the findings in this study prove a switch to a soybean oil-LE sparing strategy using a 4-OLE with additional EPA + DHA is feasible and safe and is associated with improved clinical outcomes in adult PN patients.
Limitations
This study has a number of limitations inherent to a retrospective before-/after-observational study. First, we do not have data regarding the specific characteristics leading to PN indications and contraindications to enteral feeding. Second, we do not know from our data if patients were fed simultaneously via oral or EN while receiving PN. In relation, we do not have information regarding interruptions or duration of PN in both cohorts, which could alter the interpretation of our findings. Lastly, given that this study was conducted in one isolated hospital system, the generalizability to a national population is limited. However, the results demonstrate significant value as it is the first to demonstrate clinical benefit with widespread 4-OLE implementation.
Conclusion
The use of soybean oil-sparing strategies for LE support in those receiving PN has long been advocated for with limited available evidence. 4-OLE use, though relatively new, was successfully implemented in a large institution. Switch to 4-OLE was associated with reduced LOS, complications, and mitigated hepatic dysfunction in critically ill adult patients. The findings in this study suggest that 4-OLE use is efficacious and safe and may improve clinical outcomes among patients requiring PN.
Availability of data and material
All raw data are available upon request.
References
White JV, Guenter P, Jensen G, Malone A, Schofield M, Group AMW, Force AMT, of Directors AB. Consensus statement of the academy of nutrition and dietetics/American Society for parenteral and enteral nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad Nutr Diet. 2012;112(5):730–8.
Osooli F, Abbas S, Farsaei S, Adibi P. Identifying critically ill patients at risk of malnutrition and underfeeding: a prospective study at an academic hospital. Adv Pharm Bull. 2019;9(2):314.
Saunders J, Smith T. Malnutrition: causes and consequences. Clin Med. 2010;10(6):624.
Jensen GL, Bistrian B, Roubenoff R, Heimburger DC. Malnutrition syndromes: a conundrum vs continuum. J Parenter Enter Nutr. 2009;33(6):710–6.
Mogensen KM, Robinson MK, Casey JD, Gunasekera NS, Moromizato T, Rawn JD, Christopher KB. Nutritional status and mortality in the critically ill. Crit Care Med. 2015;43(12):2605–15.
McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, McCarthy MS, Davanos E, Rice TW, Cresci GA. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (ASPEN). JPEN J Parenter Enteral Nutr. 2016;40(2):159–211.
Calder PC. Rationale and use of n-3 fatty acids in artificial nutrition. Proc Nutr Soc. 2010;69(4):565–73.
Wanten GJ, Calder PC. Immune modulation by parenteral lipid emulsions. Am J Clin Nutr. 2007;85(5):1171–84.
Hayes BD, Gosselin S, Calello DP, Nacca N, Rollins CJ, Abourbih D, Morris M, Nesbitt-Miller A, Morais JA, Lavergne V. Systematic review of clinical adverse events reported after acute intravenous lipid emulsion administration. Clin Toxicol. 2016;54(5):365–404.
Furukawa K, Yamamori H, Takagi K, Hayashi N, Suzuki R, Nakajima N, Tashiro T. Influences of soybean oil emulsion on stress response and cell-mediated immune function in moderately or severely stressed patients. Nutrition. 2002;18(3):235–40.
Fraser I, Neoptolemos J, Darby H, Bell P. The effects of intralipid and heparin on human monocyte and lymphocyte function. J Parenter Enter Nutr. 1984;8(4):381–4.
Chu RC, Barkowski SM. The effects of rate and dose of intralipid infusion on bacterial clearance and granulocytic activity of the rat. Nutr Res. 1989;9(5):513–22.
Fischer G, Wilson S, Hunter K, Mease A. Diminished bacterial defences with intralipid. The Lancet. 1980;316(8199):819–20.
Waitzberg DL, Bellinati-Pires R, Salgado MM, Hypolito IP, Colleto GM, Yagi O, Yamamuro EM, Gama-Rodrigues J, Pinotti HW. Effect of total parenteral nutrition with different lipid emulsions on human monocyte and neutrophil functions. Nutrition. 1997;13(2):128–32.
Hojsak I, Colomb V, Braegger C, Bronsky J, Campoy C, Domellöf M, Embleton N, Fidler Mis N, Hulst JM, Indrio F, et al. ESPGHAN committee on nutrition position paper. Intravenous lipid emulsions and risk of hepatotoxicity in infants and children: a systematic review and meta-analysis. J Pediatr Gastroenterol Nutr. 2016;62(5):776–92.
Vanek VW, Seidner DL, Allen P, Bistrian B, Collier S, Gura K, Miles JM, Valentine CJ, Kochevar M. Novel nutrient task force IFEW: ASPEN position paper: clinical role for alternative intravenous fat emulsions. Nutr Clin Pract. 2012;27(2):150–92.
Heyland D, Benstöm C: Nutrition support in mechanically ventilated, critically ill adult patients–study protocol for systematic reviews and meta-analyses. From website: www.criticalcarenutrition.com, URL: https://www.criticalcarenutrition.com/docs/systematic_reviews_2018/Systematic%20Review%20Protocol%20CCN_Dec%202018.pdf. Accessed 15 Oct 2022.
Köller M, Senkal M, Kemen M, König W, Zumtobel V, Muhr G. Impact of omega-3 fatty acid enriched TPN on leukotriene synthesis by leukocytes after major surgery. Clin Nutr. 2003;22(1):59–64.
Moro K, Nagahashi M, Ramanathan R, Takabe K, Wakai T. Resolvins and omega three polyunsaturated fatty acids: clinical implications in inflammatory diseases and cancer. World J Clin Cases. 2016;4(7):155.
Notz Q, Lee ZY, Menger J, Elke G, Hill A, Kranke P, Roeder D, Lotz C, Meybohm P, Heyland DK, et al. Omega-6 sparing effects of parenteral lipid emulsions-an updated systematic review and meta-analysis on clinical outcomes in critically ill patients. Crit Care. 2022;26(1):23.
Manzanares W, Dhaliwal R, Jurewitsch B, Stapleton RD, Jeejeebhoy KN, Heyland DK. Parenteral fish oil lipid emulsions in the critically ill: a systematic review and meta-analysis. J Parenter Enter Nutr. 2014;38(1):20–8.
Mertes N, Grimm H, Fürst P, Stehle P. Safety and efficacy of a new parenteral lipid emulsion (SMOFlipid) in surgical patients: a randomized, double-blind, multicenter study. Ann Nutr Metab. 2006;50(3):253–9.
Tian H, Yao X, Zeng R, Sun R, Tian H, Shi C, Li L, Tian J, Yang K. Safety and efficacy of a new parenteral lipid emulsion (Smof) for surgical patients: a systematic review and meta-analysis of randomized controlled trials. Nutr Rev. 2013;71(12):815–21.
Mayer K, Klek S, García-de-Lorenzo A, Rosenthal MD, Li A, Evans DC, Muscaritoli M, Martindale RG. Lipid use in hospitalized adults requiring parenteral nutrition. J Parenter Enter Nutr. 2020;44:S28–38.
Martindale RG, Berlana D, Boullata JI, Cai W, Calder PC, Deshpande GH, Evans D, Garcia-de-Lorenzo A, Goulet OJ, Li A. Summary of proceedings and expert consensus statements from the international summit “Lipids in Parenteral Nutrition.” J Parenter Enter Nutr. 2020;44:S7–20.
Leguina-Ruzzi AA, Ortiz R. Current evidence for the use of smoflipid® emulsion in critical care patients for parenteral nutrition. Crit Care Res Pract. 2018;2018:6301293.
Pradelli L, Mayer K, Klek S, Omar Alsaleh AJ, Clark RA, Rosenthal MD, Heller AR, Muscaritoli M. ω-3 fatty-acid enriched parenteral nutrition in hospitalized patients: systematic review with meta-analysis and trial sequential analysis. J Parenter Enter Nutr. 2020;44(1):44–57.
van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med Care. 2009;47(6):626–33.
Carey K. Hospital length of stay and cost: a multilevel modeling analysis. Health Serv Outcomes Res Method. 2002;3(1):41–56.
Siddique A, Kowdley KV. Approach to a patient with elevated serum alkaline phosphatase. Clin Liver Dis. 2012;16(2):199–229.
Hartl WH, Jauch K-W, Parhofer K, Rittler P. Medicine WGfDtGfPNotGAfN: Complications and monitoring–guidelines on parenteral nutrition, Chapter 11. GMS Ger Med Sci 2009;7:Doc17.
Llop J, Sabin P, Garau M, Burgos R, Pérez M, Masso J, Cardona D, Segura JS, Garriga R, Redondo S. The importance of clinical factors in parenteral nutrition-associated hypertriglyceridemia. Clin Nutr. 2003;22(6):577–83.
Torgalkar R, Dave S, Shah J, Ostad N, Kotsopoulos K, Unger S, Shah PS. Multi-component lipid emulsion vs soy-based lipid emulsion for very low birth weight preterm neonates: a pre-post comparative study. J Perinatol. 2019;39(8):1118–24.
Mirtallo JM, Ayers P, Boullata J, Gura KM, Plogsted S, Anderson CR, Worthington P, Seres DS, Nicolai E, Alsharhan M, et al. ASPEN lipid injectable emulsion safety recommendations, part 1: background and adult considerations. Nutr Clin Pract. 2020;35(5):769–82.
Funding
This study was funded in part by an Investigator-Initiated Grant from Fresenius Inc to Paul E. Wischmeyer via Duke University. The sponsor (Fresenius) did not participate in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation or approval of the manuscript; and decision to submit the manuscript for publication. Only the authors and investigators at Duke University participated in design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation and approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
KH, VK, TO, KR, and PEW contributed to manuscript concept and design. KH, VK, TO, OO, KR, CT, and PEW were involved in acquisition, analysis, or interpretation of data. KH, VK, TO, OO, CT, and PEW contributed to drafting of the manuscript and tables. KH, VK, TO, and PEW were involved in critical revision of the manuscript for important intellectual content. TO contributed to statistical analysis. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was reviewed by the Duke Institutional and Ethics Review Board and was granted approval (Approval No.: Pro00102602).
Consent for publication
Not applicable; all authors have seen and approved the final version of the manuscript.
Competing interests
Dr. Wischmeyer reports receiving investigator-initiated grant funding related to this work from National Institutes of Health, Department of Defense, Canadian Institutes of Health Research, Abbott, Baxter, and Fresenius. Dr. Wischmeyer has served as a consultant to Abbott, Fresenius, Baxter, Cardinal Health, and Nutricia, for research related to this work. Dr. Wischmeyer has received unrestricted gift donation for nutrition research from Musclesound and DSM. Dr. Wischmeyer has received honoraria or travel expenses for CME lectures on improving nutrition care from Abbott, Baxter, Fresenius, Danone-Nutricia, DSM, and Nestle. Dr. Haines has received investigator-initiated grant funding from American Society for Parenteral and Enteral Nutrition, National Institutes of Health, and Abbott. Dr. Haines has received honoraria for CME lectures from Fresenius.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Haines, K.L., Ohnuma, T., Trujillo, C. et al. Hospital change to mixed lipid emulsion from soybean oil-based lipid emulsion for parenteral nutrition in hospitalized and critically ill adults improves outcomes: a pre–post-comparative study. Crit Care 26, 317 (2022). https://doi.org/10.1186/s13054-022-04194-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-022-04194-8