
Abstract
Background
Plantar warts, or verrucae plantaris, are common lesions causing considerable pain during weightbearing activity. Although current treatment modalities have low success rates, microwave therapy has been introduced as a promising intervention. This study aimed to determine the effectiveness of microwave therapy for the treatment of plantar warts and to determine the clinical factors associated with plantar wart resolution.
Methods
A retrospective analysis of 150 plantar warts from 45 patients treated with microwave therapy was undertaken. Binomial regression was conducted to explore clinical characteristics (age, gender, immunosuppression, impaired healing, multiple vs single wart, location of lesion, lesion diameter) associated with lesion resolution.
Results
Of the total 150 plantar warts treated with microwave therapy, 125 (83.3%) warts resolved and 25 (17%) warts did not resolve. The mean (SD) total treatment sessions for resolved lesions was 2.8 (1.0). Decreasing age (P = 0.046) was the only clinical characteristic associated with resolution.
Conclusions
This retrospective study has shown that plantar warts may be resolved with two to three sessions of microwave therapy, which may be more successful in younger populations.
Similar content being viewed by others


Background
Plantar warts, or verrucae plantaris, result from infection of epithelial keratinocytes by the human papilloma virus (HPV). Approximately 40% of the population is infected with HPV with a 14% annual incidence of plantar warts [1]. The highest occurrence is seen in children and adolescents [2]. Although spontaneous resolution is common in the majority of patients with intact cellular immunity [3], plantar warts can be associated with considerable pain during weightbearing, and cosmetic-related stress and embarrassment.
In some cases, plantar warts persist despite multiple treatments [4, 5] and in rare cases, these recalcitrant warts may be associated with the development of squamous cell carcinomas [6]. Few controlled studies have investigated treatment options for recalcitrant plantar warts, with many associated with adverse effects [7,8,9,10]. Over the past decades, the treatment of plantar warts has largely remained unchanged, with practitioners primarily using salicylic acid, liquid nitrogen (cryotherapy), and high-energy laser therapy [3]. More recently, microwave therapy has been introduced as a promising intervention [11]. Microwaves are a form of electromagnetic non-ionising radiation between 300 MHz-300 GHz. The application of microwaves to skin increases tissue temperature to a hyperthermic range (41°-44°), which renders tissue less capable of dissipating heat and leads to damage and apoptosis of keratinocytes [12]. Unlike cold treatment such as liquid nitrogen, heating of HPV-infected tissue has also been shown to promote induction of adaptive immunity [13,14,15,16,17].
Several clinical advantages of microwave therapy have been reported. Microwaves travel in straight lines which allows targeted treatment of HPV-infected tissue [18]. The therapy induces minimal, short-lived pain with no scarring. As it does not break skin at the site of application patients do not require dressings and can resume normal activity post treatment [18]. Finally, unlike ablative laser therapies, no vapour or smoke is produced, which eliminates the risk of spreading air-borne viral particles [19].
A pilot cohort study undertaken in the UK involving 32 adults with 54 refractory plantar warts demonstrated high resolution rates (75.9%) using microwave therapy [18]. However, the factors contributing to treatment success are unknown. The objective of this study was to determine the effectiveness of microwave therapy for the treatment of plantar warts and clinical factors associated with treatment success.
Methods
Design
Single-centre non-randomised experimental retrospective study.
Participants
A retrospective cohort study was undertaken using medical records from patients who received microwave therapy between July 2018 and March 2022 at a single podiatry clinic in Milford, Auckland (New Zealand). At present, only a handful of microwave therapy units are being used throughout New Zealand, with the Milford clinic being the first to offer it to patients in July 2018. All patients who received microwave therapy from this date were invited to share their clinical treatment records for the purposes of this study. An a-priori sample size calculation was not undertaken, and sample size was informed by the number of patients who had been offered microwave therapy in this timeframe and consented to the study. Patients were included if they had one or more plantar wart(s) diagnosed by an experienced podiatrist and underwent microwave therapy treatment. Ethical approval was obtained from the Auckland University of Technology Ethics Committee on 27th July 2021 (AUTEC 21/250). Data were only included from patients who provided written informed consent/assent for their clinical treatment records to be used for this study.
Microwave therapy
Patients were excluded from receiving microwave therapy at the podiatry clinic if they were pregnant or breast-feeding, had metal implants in their feet or ankles, or were < 5 years of age. During the initial appointment a podiatrist recorded information about the location(s) and duration(s) of the plantar wart(s), and details about previous treatment(s).
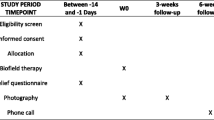
Microwave therapy was delivered using the Swift® (Emblation Ltd., UK) device, which is a hand-held tool that produces microwave heat energy within the 8 GHz range. Podiatrists at the clinic completed the manufactures standard training in using microwave therapy. The microwave energy was delivered directly to the infected tissue through a single use applicator tip to reduce the risk of cross-infection (Fig. 1). A standardised treatment procedure was followed for all patients. The first microwave therapy application at the first treatment session delivered 10 J using one application of 5W for 2 s. The wattage, frequency, and number of subsequent applications is determined by the level of pain tolerated by each patient. A 10-point scale was used at each appointment to collect patient-reported pain on arrival, during treatment, and on departure. Patients received a standard of three treatment sessions four weeks apart unless the lesion(s) resolved prior. A final review was undertaken at 12 weeks after the final treatment session where response to treatment was assessed by a podiatrist and recorded as either “resolved” or “unresolved”. Resolved lesions were defined as those no longer visible and where natural dermatoglyphics were restored. Before and after photographic evidence was used to support assessment. If unresolved at the 12-week review, patients were given the option continue further treatment sessions at 4 weeks apart until resolved, or to discontinue treatment.

Application of the microwave therapy applicator during a treatment session
Data collection
Data from clinical treatment records of all included patients were extracted into a standardised extraction form, including patient demographics, relevant medical history, and microwave therapy and treatment parameters.
Data analysis
The distribution of all continuous outcomes (lesion duration, total treatment sessions, average applications per session, average watts per application, average frequency setting per application, average pain, and average joules per treatment session) for both resolved and unresolved lesions were reviewed for normality using both visual inspection of histograms and formal tests of normality for skewness and kurtosis. Following confirmation of approximate normal distributions, clinical and treatment characteristics for participants were described as mean (SD) for continuous data and n (%) for categorical data. To determine clinical characteristics (age, gender, immunosuppression, impaired healing, multiple vs single wart, location of lesion, lesion diameter) that were associated with plantar wart resolution, a generalised linear model with binomial distribution and a logit link function was used. This approach was chosen as it also allowed for the inclusion of a participant-specific random effect which accounted for repeated measures taken from participants who had multiple lesions [20]. Person-specific factors (including age, sex, immune status, etc.,) result in a high-level of within-person dependence between lesions, meaning that data from different lesions within the same person will be highly correlated. The Nakagawa conditional R2 was computed which incorporates both fixed and random effects [21]. Adjusted estimates and p-values were reported. No multicollinearity was present between the clinical characteristics. All statistical analyses were performed in R (v4.1) using the lme4 package.
Results
Participants
A total of 135 eligible patients who received microwave therapy between July 2018 and March 2022 were invited to share their clinical treatment records for this research. A total of 47 (35%) patients responded to the invitation, including 2 who declined to participate and 45 who consented to participate. The characteristics for the 45 included patients are shown in Table 1. The majority of participants were female (n = 25, 56%) with a mean age of 46.6 years (range 6 to 74 years). Most participants had multiple plantar warts and had tried previous treatments which were unsuccessful including salicylic acid, cryotherapy, and cryotherapy.
Plantar warts
A total of 150 plantar warts were treated with microwave therapy across the 45 included patients (mean (SD) 3.3 (2.6) plantar warts per patient). Lesion-level characteristics and microwave therapy treatment details are summarised in Table 2. The majority of lesions were located on the plantar heel (n = 38, 25%) followed by the first metatarsal head, fifth metatarsal head, and hallux. The average lesion duration prior to treatment with microwave therapy was 35.2 months. Unresolved lesions received more treatment sessions (P = 0.043), a greater average number of microwave therapy applications per treatment session (P = 0.023), and higher average joules per treatment session (P = 0.034) compared to those with resolved lesions. However, average pain during treatment was significantly higher (P = 0.009).
Effectiveness of microwave therapy
In 32 patients full lesion resolution was achieved and in 10 patients lesion resolution was not achieved. Three patients with multiple plantar warts had both resolved and unresolved lesions. Of the total 150 total plantar warts treated with microwave therapy, 125 (83.3%) warts resolved and 25 (17%) warts did not resolve. Figure 2 presents examples of plantar lesions pre- and post-treatment. In the generalised linear model only decreasing age was a significant predictor of plantar wart resolution (odds ratio (95% confidence interval), 0.84 (0.71, 1.00), P = 0.046). The model explained 99.7% of the variance in plantar wart resolution (conditional R2).

Before and after microwave therapy. A right plantar heel; (B) left plantar heel; (C) left plantar hallux
Discussion
This retrospective study has shown that three to four sessions of controlled heating of keratinised skin with microwave therapy resolves the majority of longstanding plantar warts. The complete resolution rate of 83.3% is consistent with the resolution rate of 75.9% reported in a previous pilot study involving 32 patients with 54 recalcitrant plantar warts who were treated with microwave therapy [18]. These rates are substantially higher than the resolution rates for commonly used cryotherapy (45.6%) and salicylic acid (13.6%) and intralesional immunotherapy (68.1%) [22]. The analysis has also shown that lesion resolution is associated with a younger age which is consistent with existing research where both natural resolution and therapeutic cure rates for plantar warts across a number of different therapies are higher in younger populations [23, 24].
Compared with other commonly used therapies, which can result in pain, bleeding, secondary infection and ulceration [25], participants receiving microwave therapy in this study required no post-treatment recovery period. Although participants reported considerable pain during the application of microwave therapy, on departure from the appointment their pain levels had reduced to baseline, highlighting the short-lived nature of pain associated with this treatment. Participant-reported pain during treatment was significantly higher for unresolved lesions compared to those that resolved, which was likely due to the greater average joules used per treatment session for these more recalcitrant lesions.
The results of this study should be considered in light of some limitations. Firstly, the retrospective nature of the study design and the exclusion of data from patients not responding to the recruitment invitation may have introduced selection bias (i.e., patients who felt more strongly about the success of the treatment they received may have been more willing to participate) [26]. There was also missing data related to lesion duration and pain scales for some participants and there was no documentation of other factors which may have affected lesion resolution, including type of wart and HPV genotype. The patient sample size was also small, however most patients had multiple lesions which contributed to reducing type II errors and increasing power in the analysis. To confirm the efficacy of microwave therapy for the treatment of plantar warts a larger randomised trial is warranted.
In conclusion, this retrospective study of 45 participants has shown that plantar warts may be resolved with two to three sessions of microwave therapy, which may be more successful in younger populations.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Witchey DJ, Witchey NB, Roth-Kauffman MM, Kauffman MK. Plantar Warts: Epidemiology, pathophysiology, and clinical management. J Am Osteopath Assoc. 2018;118(2):92–105.
Kilkenny M, Marks R. The descriptive epidemiology of warts in the community. Australas J Dermatol. 1996;37(2):80–6.
Sterling JC, Gibbs S, Haque Hussain SS, Mohd Mustapa MF, Handfield-Jones SE. British Association of Dermatologists’ guidelines for the management of cutaneous warts 2014. Br J Dermatol. 2014;171:696–712.
Bzhalava D, Eklund C, Dillner J. International standardization and classification of human papillomavirus types. Virology. 2015;476:341–4.
Rivera A, Tyring SK. Therapy of cutaneous human Papillomavirus infections. Dermatol Ther. 2004;17(6):441–8.
Riddel C, Rashid R, Thomas V. Ungual and periungual human papillomavirus-associated squamous cell carcinoma. A review. J Am Acad Dermatol. 2011;64:1147–53.
Albalat W, Attwa E, Ebrahim HM. Intralesional cryotherapy versus cryotherapy spray for the treatment of recalcitrant plantar warts: a prospective, randomized study. J Dermatol Treatment. 2022;33(2):857–63.
Fathy G, Sharara MA, Khafagy AH. Intralesional vitamin D3 versus Candida antigen immunotherapy in the treatment of multiple recalcitrant plantar warts: a comparative case–control study. Dermatol Therap. 2019;32(5): e12997.
Nofal A, Adel L, Fawzy M, Elkholy BM. Intralesional immunotherapy for multiple recalcitrant plantar warts: Candida antigen is superior to intralesional purified protein derivative. Dermatol Therap. 2022;35(6): e15440.
Gamil HD, Nasr MM, Khattab FM, Ibrahim AM. Combined therapy of plantar warts with topical bleomycin and microneedling: a comparative controlled study. J Dermatol Treatment. 2020;31(3):235–40.
Bristow IR, Webb C, Ardern-Jones MR. The successful use of a novel microwave device in the treatment of a plantar wart. Case Reports Dermatol. 2017;9:102–7.
Hegyi G, Szigeti GP, Szász A. Hyperthermia versus Oncothermia. Cellular Effects in Complementary Cancer Therapy. Evid Based Complement Alternat Med 2013;2013:672873. https://doi.org/10.1155/2013/672873.
Wang X, Gao XH, Li X, Hong Y, Qi R, Chen HD, Zhang L, Wei H. Local hyperthermia induces apoptosis of keratinocytes in both normal skin and condyloma acuminata via different pathways. Apoptosis. 2009;14:721–8.
Zhu LL, Gao XH, Qi R, Hong Y, Li X, Wang X, McHepange UO, Zhang L, Wei H, Chen HD. Local hyperthermia could induce antiviral activity by endogenous interferon-dependent pathway in condyloma acuminata. Antiviral Res. 2010;88:187–92.
Ma Y, Huo W, Hong YX, Chen HD, Gao XH. Successful clearance of facial common warts by local hyperthermia. Report of two cases. Dermatol Ther. 2012;25:386–8.
Huo W, Di ZH, Xiao BH, Qi RQ, Weiland M, Gao XH. Clearance of genital warts in pregnant women by mild local hyperthermia. A pilot report. Dermatol Ther. 2014;27(2):109–12.
Gao X, Chen H. Hyperthermia on skin immune system and its application in the treatment of human papillomavirus-infected skin diseases. Front Med. 2014;8:1–5.
Bristow I, Lim WC, Lee A, Holbrook D, Savelyeva N, Thomson P, Webb C, Polak M, Ardern-Jones MR. Microwave therapy for cutaneous human papilloma virus infection. Eur J Dermatol. 2017;27:511–8.
Karsai S, Däschlein G. “Smoking guns”. Hazards generated by laser and electrocautery smoke. J Dtsch Dermatol Ges. 2012;10:633–6.
Stewart S, Pearson J, Rome K, Dalbeth N, Vandal AC. Analysis of data collected from right and left limbs: accounting for dependence and improving statistical efficiency in musculoskeletal research. Gait Posture. 2018;59:182–7.
Nakagawa S, Johnson P, Schielzeth H. The coefficient of determination R2 and intra-class correlation coefficient from generalized linear mixed-effects models revisited and expanded. J Royal Society Interface. 2017;14:20170213.
García-Oreja S, Álvaro-Afonso FJ, García-Álvarez Y, García-Morales E, Sanz-Corbalán I, Lázaro Martínez JL. Topical treatment for plantar warts. A systematic review. Dermatol Ther. 2021;34: e14621.
Bruggink SC, Eekhof JAH, Egberts PF, van Blijswijk SCE, Assendelft WJJ, Gussekloo J. Natural course of cutaneous warts among primary schoolchildren. A prospective cohort study. Ann Fam Med. 2013;11:437–41.
Khozeimeh F, Jabbari Azad F, Mahboubi Oskouei Y, Jafari M, Tehranian S, Alizadehsani R, Layegh P. Intralesional immunotherapy compared to cryotherapy in the treatment of warts. Int J Dermatol. 2017;56:474–8.
Bacelieri R, Johnson SM. Cutaneous warts: an evidence-based approach to therapy. Am Fam Phys. 2005;72(4):647–52.
Tripepi G, Jager KJ, Dekker FW, Zoccali C. Selection bias and information bias in clinical research. Nephron Clin Pract. 2010;115(2):c94–9.
Acknowledgements
We would like to thank the participants who consented for the use of their treatment records to be used for this study. This study was not supported by any funding.
Funding
None.
Author information
Authors and Affiliations
Contributions
WH, JH, and GN contributed to the design of the work, acquisition of data and interpretation of the results. ABR and SS contributed to the design of the work, analysis of the data and interpretation of the results. IB contributed to the design of the work and interpretation of the results. All authors contributed to drafting and revising of the manuscript and approved the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Auckland University of Technology Ethics Committee (AUTEC 22/91). All participants provided written informed consent to include their data in this analysis.
Consent for publication
Not applicable.
Competing interests
IB declares he is a consultant for Emblation Limited. The other authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hagon, W., Hagon, J., Noble, G. et al. Microwave therapy for the treatment of plantar warts. J Foot Ankle Res 16, 37 (2023). https://doi.org/10.1186/s13047-023-00638-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13047-023-00638-8