
Abstract
Background
Metabolites secreted by the gut microbiota may play an essential role in microbiota–gut–central nervous system crosstalk. In this study, we explored the changes occurring in the gut microbiota and their metabolites in patients with spinal cord injury (SCI) and analyzed the correlations among them.
Methods
The structure and composition of the gut microbiota derived from fecal samples collected from patients with SCI (n = 11) and matched control individuals (n = 10) were evaluated using 16S rRNA gene sequencing. Additionally, an untargeted metabolomics approach was used to compare the serum metabolite profiles of both groups. Meanwhile, the association among serum metabolites, the gut microbiota, and clinical parameters (including injury duration and neurological grade) was also analyzed. Finally, metabolites with the potential for use in the treatment of SCI were identified based on the differential metabolite abundance analysis.
Results
The composition of the gut microbiota was different between patients with SCI and healthy controls. At the genus level, compared with the control group, the abundance of UBA1819, Anaerostignum, Eggerthella, and Enterococcus was significantly increased in the SCI group, whereas that of Faecalibacterium, Blautia, Escherichia–Shigella, Agathobacter, Collinsella, Dorea, Ruminococcus, Fusicatenibacter, and Eubacterium was decreased. Forty-one named metabolites displayed significant differential abundance between SCI patients and healthy controls, including 18 that were upregulated and 23 that were downregulated. Correlation analysis further indicated that the variation in gut microbiota abundance was associated with changes in serum metabolite levels, suggesting that gut dysbiosis is an important cause of metabolic disorders in SCI. Finally, gut dysbiosis and serum metabolite dysregulation was found to be associated with injury duration and severity of motor dysfunction after SCI.
Conclusions
We present a comprehensive landscape of the gut microbiota and metabolite profiles in patients with SCI and provide evidence that their interaction plays a role in the pathogenesis of SCI. Furthermore, our findings suggested that uridine, hypoxanthine, PC(18:2/0:0), and kojic acid may be important therapeutic targets for the treatment of this condition.
Similar content being viewed by others

Introduction
Spinal cord injury (SCI), usually resulting from severe trauma such as falls and traffic accidents, is one of the most severe forms of injury to the central nervous system (CNS). SCI is associated with a high rate of disability and serious complications [1, 2]. Patients with SCI typically present with severe neurogenic intestinal dysfunction due to intestinal denervation [3]. In addition to changes in bowel habits, such as the occurrence of constipation and diarrhea, the gut microbiota of patients with SCI is also significantly disturbed, which has a marked impact on the quality of life of affected individuals [4]. The relationship between SCI and intestinal dysfunction has been extensively studied with the aim of developing novel and effective management methods for intestinal impairment. The CNS affects intestinal function via several mechanisms, including the regulation of intestinal motility, intestinal transport time, intestinal permeability, and hormone secretion [5]. Consequently, abnormal gastrointestinal function in patients with SCI can lead to changes in intestinal permeability and, consequently, the migration of intestinal bacteria to the bloodstream and dysbiosis [6]. Although the gut microbiome is thought to be confined to the intestinal lumen, it has been shown that it can also modulate the function of distant organs [7]. These observations highlight the importance of investigating the relationship between SCI and gut microbiota composition.
The gut microbiota is characterized as a collection of microorganisms that colonize the digestive tract. It is an indispensable “microbial organ” in the human body and plays a vital role in the health of the host, including in the CNS [8,9,10,11]. For decades, studies investigating the possible impact of microbes and viruses in SCI have been largely constrained by technical limitations; however, with the development of gut microbiota sequencing technology, the correlation between the complex gut microbiome and the CNS has been gradually revealed [12]. The gut microbiome and its metabolites regulate the normal development of the CNS, such as blood–brain barrier formation, myelination, neurogenesis, and microglia maturation [13, 14]. The gut microbiome produces neuroactive metabolites that can cross the intestinal barrier and enter the systemic circulation, where they can influence neural activity and promote neuroinflammation [15, 16]. A balanced microbiome is critical for its symbiotic relationship with the host. Dysbiosis occurs when the composition of the gut microbiome changes, particularly when there are fewer non-pathogenic bacteria or more pathogenic, proinflammatory bacteria. Evidence garnered over recent years has indicated that gut dysbiosis is related to secondary injury and the clinical symptoms of SCI [6, 17]. Studies in mice have shown that the gut microbiome becomes dysregulated after SCI, which exacerbates nerve injury and spinal cord pathology [18, 19]. Dysregulation of the gut microbiome activates the TLR4/Myd88 signaling pathway, which has been reported to aggravate SCI [19].
The exact mechanisms by which gut dysbiosis regulates SCI and the biological mediators of these effects remain largely unknown. Studies have shown that short-chain fatty acids (SCFAs), the primary metabolites produced by bacterial fermentation of dietary fiber, may regulate brain function through immune, endocrine, vagal, and other humoral pathways [20]. In addition, it has been reported that the metabolite 4-ethylphenyl sulfate influences the behavior of mice by affecting oligodendrocyte function and myelin patterning [21]. These findings suggest that gut microbiome-derived metabolites are important mediators of microbiota–gut–brain crosstalk. However, relatively few studies have investigated the changes in overall metabolite abundance in patients with SCI.
In this study, we conducted an omics analysis of gut microbiota structure in patients with SCI as well as a quantitative analysis of metabolites in serum samples. We further examined the relationship between the gut microbiota and changes in serum metabolites.
Materials and methods
Study design and sample collection
Eleven patients with SCI and 10 healthy individuals were recruited for this study. The inclusion criteria for the SCI group were (1) cervical or thoracic SCI confirmed via medical history and imaging examination; (2) aged 14 years or more; and (3) American Spinal Cord Injury Association (ASIA) neurological function scale ranging from A to D. The exclusion criteria were the presence of cauda equina injury, infectious disease, severe digestive disease, tumor, diabetes, immune metabolic disease, craniocerebral injury, and mental disorder; and patients receiving antibiotics or probiotics one month before the study. Healthy individuals (age > 14 years) were recruited based on the same exclusion criteria.
Data relating to gender, age, ASIA grade, injury duration, and site of enrolment were collected. Neurological function grade was based on the standardized ASIA Impairment Scale, as previously described [22].
Sample collection and preparation
Approximately 10 g of fresh stool samples were collected from SCI patients and healthy individuals using sterile plastic spoons and placed in test tubes. Fresh stool samples were frozen at − 80 °C for 16S rRNA gene sequencing within 2 h of collection. Venous blood samples (2 mL) were obtained from patients with SCI and healthy individuals and centrifuged at 3,000 × g for 10 min for serum extraction. The serum samples were stored at − 80 °C for UPLC–Q–TOF/MS analysis. The data were analyzed on the free online Majorbio cloud platform (www.majorbio.com).
16S rRNA amplicon sequencing
Total genomic DNA was extracted from each sample and purified using the cetyltrimethyl ammonium bromide (CTAB) method [23]. DNA purity and concentration were determined by agarose gel electrophoresis. The V3–V4 region of the 16S rRNA gene was PCR amplified using specific primers. PCR was performed in a 30-μL reaction volume, which included 15 μL of Phusion High-Fidelity PCR Master Mix (New England Biolabs, Ipswich, MA, USA), 0.2 μM of each of the forward and reverse primers, and 10 ng of template DNA. The PCR products were analyzed using 2% agarose gel electrophoresis, purified with an AxyPrepDNA Gel Extraction Kit (Axygen Bioscience, Union City, NJ, USA), and subjected to paired-end sequencing on an Illumina MiSeq/HiSeq 2500 platform.
Reads were clustered into operational taxonomic units (OTUs) at a 97% sequence similarity threshold based on Ribosomal Database Project (RDP) classification. Beta diversity analysis, including principal component analysis (PCA), principal coordinate analysis (PCoA), and partial least squares discriminant analysis (PLS-DA), was performed with the Quantitative Insights into Microbial Ecology (QIIME) software package. Differences between groups were analyzed using T-tests, linear discriminant analysis (LDA) effect size (LEfSe), and analysis of similarity (ANOSIM).
Serum metabolomics
Serum samples (100 µL) were centrifuged at 14,000×g for 20 min at 4 ℃ with an equal volume of pre-cooled acetonitrile/methanol (1:1, v/v) and the supernatant was collected. For LC–MS analysis, the samples were separated using ultra-high-performance liquid chromatography (UHPLC, 1290 Infinity LC, Agilent Technologies, Santa Clara, CA, USA). Electrospray ionization (ESI) was used for detection in both positive and negative ion modes. Mass spectrometric analysis and metabolite identification were performed using an Agilent 6550 iFunnel Q–TOF spectrometer (Agilent Technologies, Santa Clara, CA, USA) and a Triple TOF 6600 mass spectrometer (SCIEX, Framingham, MA, USA), respectively.
The raw data were converted to the mzXML format using ProteoWizard (http://proteowizard.sourceforge.net/) and imported into XCMS software for further analysis, including retention time correction, peak alignment, and picking. Following Pareto-scaling preprocessing, the data were subjected to multivariate (PCA, PLS-DA, and orthogonal PLS-DA [OPLS-DA]) and univariate (fold change [FC] and T-tests) analysis. Mean metabolite concentrations in each group were used to calculate FC values. Differentially expressed metabolites were identified using variable importance in projection (VIP) scores > 1 and p < 0.05 as criteria.
Correlation analysis
Correlations among the abundance of gut microbiota at the genus level, the levels of serum metabolites, injury duration, and neurological grading were visualized as a heatmap constructed using SCIPY (Python; Version 1.0.0).
Statistical analysis
Data were analyzed using SPSS, version 22 (IBM, Armonk, NY, USA). Continuous variables were expressed as means ± standard deviation and independent samples t-tests were employed for comparisons between groups. Categorical variables were expressed as rates and the chi-square test was used for comparisons between groups. p-values < 0.05 were considered significant.
Results
Baseline data for the two groups
The participants, all from Guangdong Province, had similar dietary habits and were given standard dietary guidance for three days before the study. There were no significant differences in age and gender between the SCI group and the control group, which minimized the influence of confounding factors on the study results. Detailed data for the SCI patients are shown in Table 1.
The gut microbiota profiles of the two groups
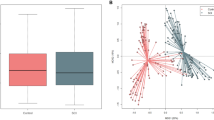
To investigate whether the gut microbiota profile was changed in patients with SCI, 16S rRNA gene sequencing was performed on fecal samples from both the SCI and Control groups. A total of 1,900,745 sequences were obtained. The OTU similarity level for index assessment was 97%. The richness and evenness of the gut microbiome of the two groups were analyzed using rank–abundance curves (Fig. 1a). The rarefaction curve had obvious asymptotes, the OUT coverage was 98.98% (Fig. 1b), and the core species curve had leveled off (Fig. 1c). These results indicated that the community was adequately sampled. Beta diversity analysis (PCoA and PLS-DA) results showed a significant separation of the gut microbiota between the SCI and Control groups (Fig. 1d, e). ANOSIM analysis demonstrated that the gut microbiota composition of the two groups was statistically different, suggesting that SCI induced gut dysbiosis (Fig. 1f).

Detection of fecal sample quality and differences in gut microbiota composition between groups. a Rank–abundance curves for fecal samples from the control and spinal cord injury (SCI) groups. The abscissa represents the rank of the number of operational taxonomic units (OTUs) and the ordinate represents the relative percentage of OTU number. b Sobs index of rarefaction curves at the OTU level between the two groups of samples detected using a 97% similarity threshold. c Core curves. The horizontal axis represents the number of observed samples and the vertical axis represents the number of all core species at the OTU level. d Principal coordinate analysis (PCoA) score plots. e Partial least squares discriminant analysis (PLS-DA) score plots. f Weighted UniFrac distances
Further analysis was performed at different taxonomic levels based on the annotated species results. Firmicutes, Actionbacteriota, Bacteroidetes, and Proteobacteria were the most abundant phyla among the gut microbiota of both groups (Fig. 2a). In addition, compared with the healthy controls, the abundance of Synergistota was significantly increased in patients with SCI, whereas that of Firmicutes was significantly decreased (Fig. 2b). At the genus level, the abundance of UBA1819 (LDA = 4.54) and Eggerthella (LDA = 3.88) was significantly increased in SCI patients relative to that in the healthy controls. The results also showed marked decreases in the abundances of Blautia (LDA = 4.51), Faecalibacterium (LDA = 4.57), Escherichia–Shigella (LDA = 4.41), Agathobacter (LDA = 4.13), Collinsella (LDA = 4.04), Dorea (LDA = 3.88), Roseburia (LDA = 3.97), Lachnospiraceae_ NK4A136 group (LDA = 3.82), Fusicatenibacter (LDA = 3.80), Holdemanella (LDA = 3.87), Ruminococcus (LDA = 3.81), UCG-002 (LDA = 3.74), and Clostridia_UCG-014 (LDA = 3.84) (Fig. 2c).

Alterations in the gut microbiota at the phylum and genus levels between the two groups. a The six most abundant species at the phylum level in the two groups. b, c Microbiota displaying significantly different abundances at the phylum and genus levels (*p < 0.05, **p < 0.01, ***p < 0.001). d A cladogram of linear discriminant analysis (LDA) effect size (LEfSe) results in the Control and spinal cord injury (SCI) groups. e Histogram of the LDA scores calculated for a differential abundance of functional profiles in the two groups. A LDA score cutoff of 3.0 was used to indicate a significant difference. Different colors represent different groups. f Correlation between fecal microbiota structure and samples
To further determine the specific gut microbiota components associated with SCI, LEfSe analysis was used to identify the gut microbiota components of both groups. The results revealed 68 components with different classification levels, 20 of which were enriched in SCI patients and 48 in the Control group (LDA > 3; p < 0.05, Fig. 2d, e). Classification results showed that the 20 species enriched in the SCI group belonged to the phyla Firmicutes (n = 16), Proteobacteria (n = 2), Actinobacteriota (n = 1), and Bacteroidota (n = 1), while the 48 species enriched in the Control group belonged to the phyla Firmicutes (n = 36), Proteobacteria (n = 6), Actinobacteriota (n = 4), and Bacteroidota (n = 2). The correlation between fecal microbiota structure and fecal samples is shown in Fig. 2f.
The serum metabolite profile of both groups
To determine the extent of metabolic disorder resulting from SCI, untargeted metabolomics analysis was used to evaluate the differences in metabolite abundance between serum samples of the SCI group (n = 10) and those of the Control group (n = 10). In the metabolic profiles of all the samples, 5,039 positive and 4,894 negative model features were identified. As shown in Fig. 3a, when the relative standard deviation (RSD) was < 0.3, the peak proportion was > 70%, indicating that the sample size was appropriate. A comprehensive multivariate statistical analysis of cations and anions was undertaken using PLS-DA and OPLS-DA. In the PLS-DA (Fig. 3b, c) and OPLS-DA (Fig. 3e, f) score plots, a significant separation was observed between the Control and SCI groups, indicating that SCI led to metabolic dysfunction. Furthermore, permutation tests showed that the PLS-DA (Fig. 3d) and OPLS-DA (Fig. 3g) patterns had good reliability.

Changes in serum metabolite abundance in the Control and spinal cord injury (SCI) groups. a Relative standard deviation (RSD) distribution plot. b, c Partial least squares discriminant analysis (PLS-DA) score plots in positive ion mode and negative ion mode, respectively. d Model verification map of PLS-DA (permutation test). e, f Orthogonal PLS-DA (OPLS-DA) score plots in positive ion mode and negative ion mode, respectively. g Model verification map of OPLS-DA (permutation test)
A total of 1511 differential metabolites (p < 0.05, VIP score > 1) were detected. Furthermore, 41 named differential metabolites were quantified. Forty-one metabolites exhibited significant differential abundance between the SCI patients and healthy controls, 18 of which were upregulated and 23 downregulated (Fig. 4a). The differentially abundant metabolites are listed in Table 2. The metabolites exhibiting significant differential abundance between the two groups are shown in the cluster heatmap in Fig. 4b.

Differential metabolite extraction and KEGG pathway enrichment analysis. a Volcano plot of the differentially abundant metabolites. The abscissa is the multiple change value of the expression difference of metabolites between the two groups, and the ordinate is the statistical test value of the expression difference of metabolites (p-value). Each point in the figure represents a specific metabolite. b Heatmap of the differentially abundant metabolites between the two groups (variable importance in projection [VIP] scores > 3, p < 0.05). The color represents the relative abundance of the metabolites in the samples. c Level 1 and 2 KEGG pathways related to the differentially expressed metabolites. The ordinate is the name of the level 2 pathway and the abscissa is the number of metabolites related to that pathway. Different colors represent different level 1 pathways. d KEGG pathway enrichment column chart. The abscissa is the name of the level 3 pathway. CP cellular processes, EIP environmental information processing, GIP genetic information processing, HD human diseases, M metabolism, OS organismal systems
Differential metabolites and KEGG pathway enrichment analysis
We next applied KEGG pathway enrichment analysis to the 41 named differential metabolites. The results suggested that the altered metabolites were mainly related to amino acid metabolism, digestive system, nucleotide metabolism, and membrane transport (Fig. 4c). The 41 metabolites were enriched in 20 KEGG pathways (p < 0.05). Histidine metabolism: M and FoxO signaling pathway: EIP were the two most significantly enriched pathways (p < 0.01, Fig. 4d).
Analysis of the correlations among gut dysbiosis, altered serum metabolites, and clinical parameters
Spearman’s correlation was used to investigate the relationship between gut microbiota and metabolites. The relationship between the 20 most differentially expressed metabolites and the 20 most differentially abundant gut microbiota at the genus level was analyzed in patients with SCI (Fig. 5a). Significant correlations were found between UBA1819 and uridine (C = 0.609, p = 0.004), Lachnospiraceae and hypoxanthine (C = 0.595, p = 0.006), Blautia and PC (18:2/0:0) (C = 0.659, p = 0.002), and Akkermansia and kojic acid (C = 0.628, p = 0.003). Meanwhile, the abundance of Akkermansia was significantly and negatively correlated with that of (5-{8-[1-(2,4-dihydroxyphenyl)-3-(3,4-dihydroxyphenyl)-2-hydroxypropyl]-3,5,7-trih-ydroxy-3,4-dihydro-2H-1-benzopyran-2-yl}-2-hydroxyphenyl) oxidanesulfonic acid in serum (C = 0.609, p = 0.004).

Analysis of the correlation among the gut microbiota, serum metabolites, and clinical parameters. a Heatmap of the correlations between differentially abundant species and metabolites (associations between 41 differentially abundant serum metabolites and the 20 most abundant genera). b Heatmap of the correlations between the gut microbiome and clinical parameters. c Heatmap of the correlations between metabolites and clinical parameters
To explore the clinical significance of gut microbiome and metabolite dysregulation in patients with SCI, the putative correlations among gut microbiota abundance, metabolite abundance, and clinical parameters (including injury duration and neurological grade) were analyzed using Spearman’s correlation (Fig. 5b, c). We found that neurological grade was significantly and positively correlated with the abundance of Dorea (C = 0.655, p = 0.001), Faecalibacterium (C = 0.587, p = 0.005), Agathobacter (C = 0.567, p = 0.007), and Collinsella (C = 0.575, p = 0.006) and significantly and negatively correlated with the abundance of UBA1819 (C = − 0.709, p = 0.000). Simultaneously, neurological grade was identified as being significantly and positively correlated with the level of 12-hydroxydodecanoic acid (C = 0.455, p = 0.001), gamma-D-glutamylglycine (C = 0.712, p = 0.000), asparaginyl-hydroxyproline (C = 0.613, p = 0.004), and allocholic acid (C = 0.581, p = 0.007) and significantly and negatively correlated with the level of kojic acid (C = − 0.617, p = 0.004). In addition, injury duration showed a significant positive correlation with the abundance of UBA1819 (C = 0.660, p = 0.001) and a significant negative correlation with the abundance of Dorea (C = − 0.691, p = 0.001), Blautia (C = 0.575, p = 0.006), Faecalibacterium (C = − 0.618, p = 0.003), Agathobacter (C = 0.652, p = 0.001), and Collinsella (C = 0.646, p = 0.002). Meanwhile, injury duration was significantly and negatively correlated with the level of 2-methylbutyroylcarnitine (C = − 0.730, p = 0.000) and deoxycholic acid (C = 0.642, p = 0.002). The overall correlation results suggested that gut microorganisms UBA1819, Dorea, Faecalibacterium, Agathobacter, and Collinsella and the metabolites kojic acid, 12-hydroxydodecanoic acid, gamma-D-glutamylglycine, asparaginyl-hydroxyproline, and allocholic acid were associated with neurological grade. The results further suggested that the gut microbes UBA1819, Dorea, Blautia, Faecalibacterium, Agathobacter, and Collinsella and the metabolites 2-methylbutyroylcarnitine and deoxycholic acid were related to injury duration.
Discussion
In this study, we compared the gut microbiota and serum metabolites of patients with SCI and healthy individuals using 16S rRNA sequencing and metabolomics. The patients and the controls recruited for our study were age- and gender-matched and were from the same geographical location. Despite these similarities, we found that gut microbiota and metabolite composition was significantly altered in SCI patients compared with that in the controls, and the changes were correlated. The main findings of our study were as follows: (1) The composition of the gut microbiota differed between SCI patients and healthy individuals, suggesting that SCI induced gut dysbiosis; (2) the serum metabolite profile of patients with SCI differed from that of healthy individuals, implying that SCI patients experience metabolic abnormalities; (3) the gut microbiota dysregulation that occurs following SCI is closely related to the changes in the serum metabolite profile as well as clinical parameters (including injury duration and neurological grade). The metabolomics analysis identified many metabolites that are closely associated with CNS diseases and may be important therapeutic targets for the treatment of SCI, a notion that merits further investigation.
Increasing evidence, both basic and clinical, has indicated that the gut microbiome is involved in regulating a variety of cellular and molecular processes under both physiological and pathological conditions. The gut microbiome and its metabolites can migrate from the gut to the intestinal wall and cross the intestinal barrier, thereby promoting inflammation and affecting other organs [24]. However, the precise mechanisms underlying these effects are unclear. Immune-, endocrine-, metabolism-, and neurotransmitter-related pathways are considered to be the main mechanisms via which the gut microbiota influence the occurrence and development of CNS diseases. In the last decade, an increasing number of studies have focused on the role of gut microbes in regulating CNS function, especially in animal models. One study showed that dysregulation of the gut microbiome is associated with impaired functional recovery and increased anxiety-like behavior after SCI [25]. Meanwhile, Jing et al. found that fecal microbiota transplantation can help restore the gut microbiota and the metabolite profile of mice with SCI, thereby improving intestinal and neurological function [26]. A different study reported that the feeding of commercial probiotics to mice promoted anti-inflammatory responses by increasing the number of regulatory T cells, thus alleviating neuropathology and promoting motor recovery in the animals [18]. The same study also demonstrated that lactic acid supplementation facilitates functional recovery after SCI. These results suggested that the gut microbiome is a key regulator of SCI pathogenesis. The modulation of the gut microbiome and derived metabolites in SCI patients is expected to reduce functional impairment and promote nerve regeneration.
At the phylum level, the gut microbiome primarily consists of Firmicutes, Bacteroidetes, Actinobacteria, Proteobacteria, and Verrucomicrobia [27]. Firmicutes and Bacteroidetes were reported to account for approximately 90% of all bacteria in the gut [28]. These bacteria ferment indigestible polysaccharides and produce metabolites that can be used as energy by the host. The relative abundance of some constituents of the gut microbiome was reported to be altered in patients with SCI [29]. In a Chinese cohort study involving patients with chronic traumatic complete SCI, Zhang et al. observed that the proportions of Proteobacteria and Verrucomicrobia were increased, while that of Bacteroidetes was decreased [6]. Another clinical study that enrolled 54 Turkish people (41 patients with SCI and 13 healthy individuals) reported that SCI patients had a significantly reduced abundance of Firmicutes compared with healthy individuals [17]. However, results from animal experiments have indicated that the abundance of Firmicutes is decreased and that of Bacteroidetes increased in mice with SCI and that Firmicutes is positively correlated with motor recovery [14, 30]. Similarly, the number of Bacteroidetes was reported to be increased in mice with acute or subacute SCI [18, 31]. Consistent with these studies, we also found significant changes in the composition of the gut microbiome in patients with SCI, namely, the abundance of Firmicutes was found to be decreased, whereas that of Synergistota was increased, in SCI patients. Our results related to the changes in gut microbiota composition after SCI are not entirely consistent with those of previous studies. Possible reasons for this include (1) differences in the severity of SCI, such as between complete and incomplete injury [32]; (2) differences in diet, environment, and gut microbe composition among individuals; (3) differences in antibiotic intake; and (4) experimental bias. To reduce the influence of confounding factors on our results, the two groups of participants enrolled in our study were matched for gender and age and all originated from the same region. Additionally, dietary management was standardized before sampling.
The gut microbiota regulates several key metabolic processes in the body; accordingly, gut microbiota imbalance is a major contributor to metabolic disorders in the host [27]. Clinical studies and studies involving animals have demonstrated that changes in the gut microbiome after SCI are closely linked to metabolic abnormalities. For instance, changes in the gut microbiome of patients with thoracic SCI were reported to be correlated with differences in serum biomarker levels, suggesting that gut dysbiosis was associated with multiple metabolic processes [32]. It has also been suggested that changes in the abundance of Bacteroidetes and Firmicutes after SCI may cause or lead to chronic metabolic disorder [32, 33]. Moreover, studies have shown that people with paraplegia or quadriplegia have significantly impaired metabolic function and higher body fat content than healthy people [33, 34]. Similar to the results of previous studies, our untargeted metabolomics analysis indicated that the serum metabolite profile was significantly altered in patients with SCI relative to that in the healthy controls and that this was correlated with changes in the gut microbiome.
In our study, 68 differentially abundant microbial strains and 41 differentially expressed metabolites were selected for association analysis and a combined analysis with clinical indicators. The abundance of UBA1819, Lachnospiraceae, Blautia, and Akkermansia was found to be significantly and positively correlated with that of serum uridine, kojic acid, hypoxanthine, and PC(18:2/0:0), respectively. Additionally, the increase in UBA1819 abundance observed in patients with SCI was positively correlated with injury duration, but negatively correlated with motor function. Importantly, the abundance of UAB1819 was positively correlated with serum uridine levels. UBA1819 belongs to the family Ruminococcaceae [35], the members of which produce SCFAs that help maintain the health of the digestive tract [36]. It has been shown that Ruminococcaceae is enriched in behavior-deficient mice and is closely associated with anxiety-like behavior [37]. In our study, we found that UBA1819 abundance was increased after SCI, which may be associated with chronic motor dysfunction and depression. Uridine is a precursor of the pyrimidine nucleotides necessary for RNA synthesis as well as an essential starting material for many metabolic processes. Uridine has many critical biological functions. For instance, it has been reported that uridine can reduce inflammation and oxidative stress levels [38], reduce cytotoxicity [39], and improve neurophysiological functions [40, 41]. Uridine can also influence regeneration in a variety of mammalian tissues and promote stem cell activity [42]. These observations imply that UBA1819 may play a role in SCI by influencing uridine metabolism and that countering oxidative stress and promoting nerve regeneration may serve to ameliorate the pathology of SCI.
In addition to uridine, hypoxanthine and kojic acid, identified as being differentially abundant in this study, are also closely related to neurological diseases. Hypoxanthine increases the expression of proinflammatory cytokines and that of NF-κB, decreases nitrite levels, and induces microglia and astrocyte activation [43]. Hypoxanthine and kojic acid have both been associated with the induction of oxidative stress. Moreover, kojic acid was reported to exert a significant inhibitory effect on glial cell activation and the release of inflammatory factors [44, 45]. These metabolites may serve as important therapeutic targets for SCI, a possibility that will be examined in subsequent studies.
Despite the importance of our findings, this study nevertheless had several limitations. The first was that it is not possible to eliminate the influence of confounding factors given that the factors that can affect the composition of the gut microbiota and metabolite abundance are extremely complex. The second limitation of this study was that, although the results indicated that the sampling of the microbial community was adequate, the sample size was still small. The third limitation was the lack of verification of the differential flora and metabolite abundance. However, this study was the first to use serum metabolomics combined with the gut microbiota to study the relationship between the intestinal environment and clinical parameters in patients with SCI. Importantly, we found that uridine, glutamate, hypoxanthine, and kojic acid are closely related to SCI and represent potentially important targets for the treatment of this condition. Our data provided a novel perspective for the study of the gut microbiota and associated metabolism after SCI.
Availability of data and materials
The data that support the findings in this study are available from the corresponding author upon reasonable request.
Abbreviations
- SCI:
-
Spinal cord injury
- CNS:
-
Central nervous system
- SCFAs:
-
Short-chain fatty acids
- ASIA:
-
American Spinal Cord Injury Association
- CTAB:
-
Cetyltrimethyl ammonium bromide
- OTUs:
-
Operational taxonomic units
- RDP:
-
Ribosomal Database Project
- PCA:
-
Principal component analysis
- PCoA:
-
Principal coordinate analysis
- PLS-DA:
-
Partial least squares discriminant analysis
- QIIME:
-
Quantitative insights into microbial ecology
- LDA:
-
Linear discriminant analysis
- ANOSIM:
-
Analysis of similarity
- ESI:
-
Electrospray ionization
- OPLS-DA:
-
Orthogonal PLS-DA
- FC:
-
Fold change
References
McDonald JW, Sadowsky C. Spinal-cord injury. Lancet. 2002;359:417–25.
Trgovcevic S, Milicevic M, Nedovic G, Jovanic G. Health condition and quality of life in persons with spinal cord injury. Iran J Public Health. 2014;43:1229–38.
Benevento BT, Sipski ML. Neurogenic bladder, neurogenic bowel, and sexual dysfunction in people with spinal cord injury. Phys Ther. 2002;82:601–12.
Krassioukov A, Eng JJ, Claxton G, Sakakibara BM, Shum S. Neurogenic bowel management after spinal cord injury: a systematic review of the evidence. Spinal Cord. 2010;48:718–33.
Martin CR, Osadchiy V, Kalani A, Mayer EA. The brain–gut–microbiome. Axis Cell Mol Gastroenterol Hepatol. 2018;6:133–48.
Zhang C, Zhang W, Zhang J, Jing Y, Yang M, Du L, et al. Gut microbiota dysbiosis in male patients with chronic traumatic complete spinal cord injury. J Transl Med. 2018;16:353.
Delgado JR, Benakis C. The gut ecosystem: a critical player in stroke. Neuromol Med. 2021;23:236–41.
Sender R, Fuchs S, Milo R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol. 2016;14: e1002533.
Zmora N, Suez J, Elinav E. You are what you eat: diet, health and the gut microbiota. Nat Rev Gastroenterol Hepatol. 2019;16:35–56.
Jarbrink-Sehgal E, Andreasson A. The gut microbiota and mental health in adults. Curr Opin Neurobiol. 2020;62:102–14.
Sanchez B, Delgado S, Blanco-Miguez A, Lourenco A, Gueimonde M, Margolles A. Probiotics, gut microbiota, and their influence on host health and disease. Mol Nutr Food Res. 2017;61:1600240.
Knight R, Vrbanac A, Taylor BC, Aksenov A, Callewaert C, Debelius J, et al. Best practices for analysing microbiomes. Nat Rev Microbiol. 2018;16:410–22.
Sharon G, Sampson TR, Geschwind DH, Mazmanian SK. The central nervous system and the gut microbiome. Cell. 2016;167:915–32.
Jing Y, Yu Y, Bai F, Wang L, Yang D, Zhang C, et al. Effect of fecal microbiota transplantation on neurological restoration in a spinal cord injury mouse model: involvement of brain-gut axis. Microbiome. 2021;9:59.
Yano JM, Yu K, Donaldson GP, Shastri GG, Ann P, Ma L, et al. Indigenous bacteria from the gut microbiota regulate host serotonin biosynthesis. Cell. 2015;161:264–76.
Haghikia A, Jorg S, Duscha A, Berg J, Manzel A, Waschbisch A, et al. Dietary fatty acids directly impact central nervous system autoimmunity via the small intestine. Immunity. 2016;44:951–3.
Gungor B, Adiguzel E, Gursel I, Yilmaz B, Gursel M. Intestinal microbiota in patients with spinal cord injury. PLoS ONE. 2016;11: e145878.
Kigerl KA, Hall JC, Wang L, Mo X, Yu Z, Popovich PG. Gut dysbiosis impairs recovery after spinal cord injury. J Exp Med. 2016;213:2603–20.
Rong Z, Huang Y, Cai H, Chen M, Wang H, Liu G, et al. Gut microbiota disorders promote inflammation and aggravate spinal cord injury through the TLR4/MyD88 signaling pathway. Front Nutr. 2021;8: 702659.
Dalile B, Van Oudenhove L, Vervliet B, Verbeke K. The role of short-chain fatty acids in microbiota-gut-brain communication. Nat Rev Gastroenterol Hepatol. 2019;16:461–78.
Needham BD, Funabashi M, Adame MD, Wang Z, Boktor JC, Haney J, et al. A gut-derived metabolite alters brain activity and anxiety behaviour in mice. Nature. 2022;602:647–53.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, Johansen M, et al. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med. 2011;34:535–46.
Gerstein AC, Fu MS, Mukaremera L, Li Z, Ormerod KL, Fraser JA, et al. Polyploid titan cells produce haploid and aneuploid progeny to promote stress adaptation. MBio. 2015;6:e1315–40.
Tilg H, Zmora N, Adolph TE, Elinav E. The intestinal microbiota fuelling metabolic inflammation. Nat Rev Immunol. 2020;20:40–54.
Schmidt E, Torres-Espin A, Raposo P, Madsen KL, Kigerl KA, Popovich PG, et al. Fecal transplant prevents gut dysbiosis and anxiety-like behaviour after spinal cord injury in rats. PLoS ONE. 2020;15: e226128.
Jing Y, Yang D, Bai F, Zhang C, Qin C, Li D, et al. Melatonin treatment alleviates spinal cord injury-induced gut dysbiosis in mice. J Neurotrauma. 2019;36:2646–64.
Arumugam M, Raes J, Pelletier E, Le Paslier D, Yamada T, Mende DR, et al. Enterotypes of the human gut microbiome. Nature. 2011;473:174–80.
Tyler PT, Grandhi R. Gut microbiota and neurologic diseases and injuries. Adv Exp Med Biol. 2020;1238:73–91.
Bazzocchi G, Turroni S, Bulzamini MC, D’Amico F, Bava A, Castiglioni M, et al. Changes in gut microbiota in the acute phase after spinal cord injury correlate with severity of the lesion. Sci Rep. 2021;11:12743.
Myers SA, Gobejishvili L, Saraswat OS, Garrett WC, Andres KR, Riegler AS, et al. Following spinal cord injury, PDE4B drives an acute, local inflammatory response and a chronic, systemic response exacerbated by gut dysbiosis and endotoxemia. Neurobiol Dis. 2019;124:353–63.
O’Connor G, Jeffrey E, Madorma D, Marcillo A, Abreu MT, Deo SK, et al. Investigation of microbiota alterations and intestinal inflammation post-spinal cord injury in rat model. J Neurotrauma. 2018;35:2159–66.
Yu B, Qiu H, Cheng S, Ye F, Li J, Chen S, et al. Profile of gut microbiota in patients with traumatic thoracic spinal cord injury and its clinical implications: a case–control study in a rehabilitation setting. Bioengineered. 2021;12:4489–99.
Baothman OA, Zamzami MA, Taher I, Abubaker J, Abu-Farha M. The role of gut microbiota in the development of obesity and diabetes. Lipids Health Dis. 2016;15:108.
Gorgey AS, Dolbow DR, Dolbow JD, Khalil RK, Castillo C, Gater DR. Effects of spinal cord injury on body composition and metabolic profile—part I. J Spinal Cord Med. 2014;37:693–702.
Hu Q, Niu Y, Yang Y, Mao Q, Lu Y, Ran H, et al. Polydextrose alleviates adipose tissue inflammation and modulates the gut microbiota in high-fat diet-fed mice. Front Pharmacol. 2021;12: 795483.
McNabney SM, Henagan TM. Short chain fatty acids in the colon and peripheral tissues: a focus on butyrate, colon cancer, obesity and insulin resistance. Nutrients. 2017;9:1348.
Gacias M, Gaspari S, Santos P M, Tamburini S, Andrade M, Zhang F, Shen N et al. Microbiota-driven transcriptional changes in prefrontal cortex override genetic differences in social behavior. elife. 2016; 5
Zhang X, Zhang H, Gong J, Yu H, Wu D, Hou J, et al. Aging affects the biological activity of fibroblast growth factor (FGF) in gastric epithelial cell, which is partially rescued by uridine. Bioengineered. 2022;13:3724–38.
McEvilly M, Popelas C, Tremmel B. Use of uridine triacetate for the management of fluorouracil overdose. Am J Health Syst Pharm. 2011;68:1806–9.
Gallai V, Mazzotta G, Montesi S, Sarchielli P, Del GF. Effects of uridine in the treatment of diabetic neuropathy: an electrophysiological study. Acta Neurol Scand. 1992;86:3–7.
Mironova GD, Khrenov MO, Talanov EY, Glushkova OV, Parfenyuk SB, Novoselova TV, et al. The role of mitochondrial KATP channel in anti-inflammatory effects of uridine in endotoxemic mice. Arch Biochem Biophys. 2018;654:70–6.
Liu Z, Li W, Geng L, Sun L, Wang Q, Yu Y, et al. Cross-species metabolomic analysis identifies uridine as a potent regeneration promoting factor. Cell Discov. 2022;8:6.
Biasibetti H, Pierozan P, Rodrigues AF, Manfredini V, Wyse A. Hypoxanthine intrastriatal administration alters neuroinflammatory profile and redox status in striatum of infant and young adult rats. Mol Neurobiol. 2017;54:2790–800.
Kim YJ, Ryu HM, Choi JY, Cho JH, Kim CD, Park SH, et al. Hypoxanthine causes endothelial dysfunction through oxidative stress-induced apoptosis. Biochem Biophys Res Commun. 2017;482:821–7.
Khan A, Park TJ, Ikram M, Ahmad S, Ahmad R, Jo MG, et al. Antioxidative and anti-inflammatory effects of kojic acid in abeta-induced mouse model of Alzheimer’s disease. Mol Neurobiol. 2021;58:5127–40.
Acknowledgements
Not applicable.
Funding
This work was supported by grant from the National Natural Science Foundation of China (82001307 and 82002398), Guangdong Basic and Applied Basic Research Foundation (2019A1515110460) and the Natural Science Foundation of Guangdong Province, China (2018A030313549).
Author information
Authors and Affiliations
Contributions
GK and BX designed the study; WZ, SZ and JC performed the experiments; WZ and KH wrote the manuscript. CZ and XY provided suggestions and participated in the revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University ([2021]808), and informed consent was obtained from each participant’s guardians. Patient consent for publication was obtained. All the ethical principles for medical research on human beings contained in the World Medical Association’s Declaration of Helsinki were followed in conducting this study.
Consent for publication
All authors have agreed to publish this manuscript.
Competing of interests
The authors declare no competing interest in this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kong, G., Zhang, W., Zhang, S. et al. The gut microbiota and metabolite profiles are altered in patients with spinal cord injury. Mol Brain 16, 26 (2023). https://doi.org/10.1186/s13041-023-01014-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13041-023-01014-0