
Abstract
The approval of anticancer therapeutic strategies is still slowed down by the lack of models able to faithfully reproduce in vivo cancer physiology. On one hand, the conventional in vitro models fail to recapitulate the organ and tissue structures, the fluid flows, and the mechanical stimuli characterizing the human body compartments. On the other hand, in vivo animal models cannot reproduce the typical human tumor microenvironment, essential to study cancer behavior and progression. This study reviews the cancer-on-chips as one of the most promising tools to model and investigate the tumor microenvironment and metastasis. We also described how cancer-on-chip devices have been developed and implemented to study the most common primary cancers and their metastatic sites. Pros and cons of this technology are then discussed highlighting the future challenges to close the gap between the pre-clinical and clinical studies and accelerate the approval of new anticancer therapies in humans.
Similar content being viewed by others


Background
Cancer is the main disease burden worldwide. An estimated 26.3% increase in incident cancer cases and a 20.9% one in cancer deaths have occurred since 2010. Significant growth is expected in the next two decades [1]. Prevention actions need to be defined and implemented, especially in low-to-middle-income countries [2]. However, much effort is constantly deployed to find successful therapeutic solutions to this widespread disease [3,4,5]. Notwithstanding, the lack of models reproducing the in vivo cancer physiology represents one of the main problems in the development of anti-cancer therapeutic strategies. Indeed, the limits of the currently used in vitro and in vivo models for tumor studies hampered the thorough understanding of its behavior and the underlying molecular mechanisms [6]. Cancer two-dimensional (2D) in vitro models are routinely used due to their easy application, low cost, and well-established procedures to perform cancer studies. However, their main limitation relies on the impossibility of correctly reproducing the three-dimensional (3D) structure of the human tumor niche, the complex interactions between tumor cells, and the associated stromal cells in the tumor microenvironment (TME) [7,8,9]. More sophisticated 3D in vitro models (e.g., spheroids, organoids) have been developed to address the need for a 3D physiological structure. However, these models still miss some important features, such as the presence of a flow and mechanical cues, like the shear stress [10,11,12]. Conversely, in vivo animal models offer a better resource to overcome the limits of the 2D models. They allow the assessment of tumor growth and the response to drug treatments [13, 14]. Nevertheless, it is recognized that these models fail to recapitulate the specific human TME [15]. Flourishing literature highlighted the important role of the TME in supporting and influencing tumor behavior, thus becoming an essential component in deciphering the pathways related to tumor development and progression [16]. In this scenario, organ-on-chip (OoC) platforms are emerging as innovative and advanced 3D approaches. Indeed, they usually host multiple cell types in a more in vivo-like microenvironment [17,18,19]. In the last years, cancer-on-chip (CoC) platforms have been developed with the purpose to emulate the relevant physiological characteristics of the TME in vitro while controlling the mechanical stimulus, the flow, and the rate of chemical release at the cellular scale [20].
This review summarizes the important characteristics of CoC technology and application, focusing on the main impacting primary cancers and their usual metastatic sites.
Insight into carcinogenesis, metastatic cascade, and the role of tumor microenvironment
Carcinogenesis and the metastatic cascade
Carcinogenesis is a complex process by which normal cells undergo genetic and epigenetic alterations leading to the development of cancer. These changes enable the cancer cells to evade regulatory mechanisms, invade surrounding tissues, and potentially spread to distant organs through metastasis [21]. The metastatic cascade is a complex and dynamic process involving a series of steps through which tumor cells disseminate from the primary tumor site to distant organs (Fig. 1) [22]. Intravasation is a critical step in the metastatic cascade, where cancer cells invade and cross endothelial barriers or lymphatic vessels to enter the circulatory system. This process involves changes in tumor cell adhesion molecules, cytoskeletal rearrangements, and the secretion of proteolytic enzymes that degrade the extracellular matrix. Subsequently, extravasation occurs, whereby tumor cells exit the bloodstream, adhere to the endothelial cells, migrate through the vessel walls, and establish secondary tumors in new tissue environments [23]. This highlights the importance of a deeper understanding of the molecular and cellular mechanisms underlying each stage of the metastatic cascade to develop effective therapeutic strategies.

The carcinogenesis and the metastatic cascade. The carcinogenesis and the metastatic cascade are complex processes that comprise the mechanisms associated with the primary tumor and its colonization of other organs (metastasis). The first phase is the primary tumor growth (1) followed by the generation of new capillary blood vessels (2), a crucial step for tumor progression and invasion. Once the cancer cells undergo the epithelial-to-mesenchymal transition (EMT), they acquire the metastatic phenotype (3), which allows the cells to move and enter the blood vessels through intravasation (4) and leave them (extravasation, 5) when they reach distant organs, the metastatic sites (6)
Tumor microenvironment
The TME is a complex and dynamic environment recognized to have a pivotal role in tumor initiation and progression [24]. Stromal cells (e.g., fibroblasts, endothelial cells, lymphatic vascular network, pericytes), immune cells from the adaptative and innate immunity (e.g., T and B lymphocytes, tumor-associated macrophages, natural killer cells), and extracellular matrix (ECM) components establish a bi-directional and complex cross-talk with tumor cells. This leads to the regulation of several cellular processes that promote tumor cell proliferation, invasion, and metastatization [16, 25].
Cancer-associated immune cells are recruited in the tumor niche in response to several chemokines and cytokines released from tumor cells, such as CCL2, IL-8, CXCL12, and CCL5. Consequently, an aberrant inflammatory response is triggered, and a strong immunosuppressive niche is induced [26, 27]. Indeed, the infiltration, density, or type of tumor-infiltrated immune cells is reported to have a prognostic value for several cancers [28,29,30,31].
Among the stromal components, cancer-associated fibroblasts (CAFs) represent one of the most predominant cell populations within the TME. They constitute a heterogeneous group of cells originating from different sources, such as tissue-resident fibroblasts, stellate cells, bone marrow mesenchymal stem cells, and pericytes [16, 32]. During tumorigenesis, fibroblasts are recruited to the tumor site due to the release of factors from neoplastic cells within the TME, such as fibroblast growth factors (FGF) and platelet-derived growth factors (PDGF) [33, 34]. Once CAFs are recruited and activated in the tumor site, an intensive mutual relationship is established between them and tumor cells. Extracellular components are secreted from CAFs modifying the surrounding TME and influencing the tumor cell behavior. CAFs release various metalloproteinases (e.g., MMP2, MMP9) influencing the remodeling of the ECM; growth factors, and cytokines are also let out such as CCL7, the transforming growth factor beta (TGFβ) and the stromal cell-derived factor 1 (SDF-1). These molecules promote tumor proliferation, spreading, and aggressiveness [35, 36]. CAFs are linked to high chemoresistance and a poor prognosis in many solid tumors [37,38,39,40].
Among the different cell types populating the TME, endothelial cells (ECs) also play a pivotal role in tumor progression and metastasis. Indeed, they respond to pro-angiogenic signals mainly released by tumor cells and in turn secrete several molecules that promote the sprouting of new blood vessels [41]. Through this process, namely angiogenesis, ECs provide oxygen and nutrients to the growing tumor, enabling its survival and expansion [42]. Furthermore, ECs actively regulate the recruitment and activation of the immune cells within the TME, while also contributing to tumor immunosuppression through the secretion of inflammatory cytokines, and angiogenic factors and exerting antigen-presenting functions [41, 43]. Notably, the tumor ECs have been shown to exhibit distinct molecular characteristics, including the upregulation of adhesion molecules and enhanced permeability, enhancing tumor cell adhesion on the ECs and dissemination to distant organs [44].
The ECM represents an essential component of the TME, which provides structural support to tumor cells, by creating a complex network of proteins (e.g., collagens, fibronectin) able to influence tumor growth and invasion [45]. Indeed, the different ECM components interact with the tumor cells, fostering pro-survival and pro-proliferation signals to cancer cells through the action of integrins, ECM transmembrane proteins, which act as mechanotransducers, thereby deeply influencing tumor cell behavior [46]. Moreover, the increased tissue stiffness, derived from a dense and abundant tumor ECM, promotes the development of a physical barrier that could hamper the diffusion of anti-cancer drugs and essential nutrients and oxygen, fostering the establishment of a hypoxic environment [45, 47]. These mechanisms further increase the malignant behavior of tumor cells, due to the activation of several pathways involved in tumor cell proliferation, plasticity, and invasion [45, 47].
In the last years, increasing attention has been focused on tumor extracellular vesicles (EVs), as critical mediators of cell-to-cell communication within the TME [48]. These small membrane-bound vesicles, released by both tumor cells and stromal cells, transport proteins, nucleic acids, lipids, and several signaling molecules to neighboring or distant cells, promoting cell proliferation, angiogenesis, immune escape, and metastasis [49]. Furthermore, EVs are employed by sensitive cells to transfer drug resistance to chemosensitive cells, by delivering multi-drug resistance proteins [50, 51].
In such a scenario, great efforts are focused on developing advanced culture models, such as organ-on-chips (specifically, cancer-on-chips). The main goal is to reproduce the key in vivo TME interactions, provide a deep understanding of the underlying molecular pathways, and identify new targeted therapeutic strategies [17, 52].
Organ-on-chip technology: microengineering joins biology
Definition and key characteristics
An organ-on-chip “is a fit-purpose fabricated micro-fluidic-based device, containing living engineered organ substructures in a controlled micro- or nanoenvironment, that recapitulate one or more aspects of the dynamics, functionalities and (patho)physiological response of an organ in vivo, in real-time monitoring mode” [53]. Indeed, these tiny devices host living cells in microchambers perfused thanks to the presence of hollow microchannels. The “chip” word derives from the adaptation of the photolithographic techniques used in the computer microchips, which allow features at micro and nanoscale. These small dimensions permit obtaining highly controlled environments that resemble those of human cells [54]. Three key features characterize this technology [55]:
-
1.
the organization of the cells in an in vivo-like arrangement;
-
2.
the choice to culture multiple cell types to better replicate the human conditions;
-
3.
the implementation of biochemical and biophysical stimuli to resemble the organs’ or tissues’ functions.
OoCs’ environment
The micro- and nanoenvironments are responsible for the precise tuning of the fluids inside the OoCs’ channels as well as for the spatiotemporal control of gradients (e.g., chemical or nutrients). These peculiar characteristics are one of the major contributions to the success of OoC technology. Indeed, OoCs allow replicating and controlling of similar-human physiological cues, such as perfusion (laminar, pulsatile, and interstitial flow), physical forces (compression and tension), fluid shear stress, cyclic strain, and biochemical gradients of specific compounds [56]. Laminar flow is present in small vessels of organs and tissues and has a pivotal role in reproducing their physiology and pathophysiology. In the microfluidic systems, luminal fluid shear stress is controlled allowing the study of their role in different biological peculiarities, such as the reorganization of the actin cytoskeleton [57], the translocation of proteins [58], and the modulation of angiogenesis [59]. Studies were also performed to assess how capillary laminar fluid flow can impact the metastatic cells in their cycle progression, motility, and phenotypic changes [60, 61]. Laminar flow is usually generated using gravity-driven devices, pressure regulators, and syringe pumps [62]. Pulsatile flow is applied to microfluidic systems that aim to reproduce the human vessels and the pulsatile blood flow [63, 64]. Reproducing the physiological nature of the human vascular system is important when the connection between organs is established [65] and when studying the properties of endothelial cells in normal or diseased conditions [66]. This type of flow is typically actuated thanks to peristaltic pumps (also embedded in the chips [67]), syringes, and pneumatic pumps [62]. Interstitial flow happens inside or around a 3D ECM and has important effects on different aspects of cells’ functions, like their motility [68]. This type of flow has a role in the cancer cells’ metastasis and how they access and shape other environments [69]. Hydrostatic pressure-driven flow is the most used to reproduce this kind of flow [62]. Compression is a physical cue indispensable for many tissues and organs, such as the skin and heart. Pressure devices have been implemented with microfluidic devices to reproduce the compressive stimuli and help in the formation of specific tissue and organ [70]. Vacuum and syringe pumps are also applied to reproduce the cyclic strain that specific organs experience in the human body [62]. Connective tissue and lungs are just an example where this stimulus is necessary [71]. Organ and tissue microarchitectures (physiological or not) are simulated in the organ-on-chips thanks to the use of ECM coatings or hydrogels in which cells are seeded to resemble the human biological 3D structures [72, 73]. Indeed, organ-on-chips integrate with or enhance other 3D models, such as those based on scaffolds (hydrogels, porous scaffolds) [74,75,76] and on cells (spheroids, organoids) [77, 78]. Table 1 provides an overview of the main characteristics of these 3D systems [79, 80]. ECM-like hydrogels work as a 3D cell culture framework when inside an OoC. They provide mechanical support thanks to their porosity, water retention, and stiffness [81]. Natural (e.g., collagen, fibrin) and synthetic (e.g., poly(ethylene glycol), polyacrylamide) hydrogels are both used in combination with OoCs [82, 83]. Natural hydrogels have different cell binding sites and growth factors that influence cellular behaviors. However, they usually show poor mechanical properties. On the other side, synthetic hydrogels' mechanical and chemical properties can be easily tuned, but they lack bioactive molecules to support specific cell functions [81]. Another scaffold technology used in the OoC application is that obtained with electrospun fibers. Specific electrospinning techniques have been developed to introduce the polymeric fibers at micro- or nanometric scale inside organ-on-chip models [84] to have adequate support for cell growth [85]. Spheroids and organoids are the most common cell-based options to obtain the cell-ECM interactions needed in the OoCs [79]. Spheroids are the simplest 3D culture method coming from the spontaneous aggregation of differentiated cells, while organoids have a specific development process starting from either embryonic stem cells, induced pluripotent stem cells, or adult stem cells [79, 80]. The replica of the physiological micro- and nanoenvironments comprises also the tissue interfaces and endothelialized vascular channels [86, 87]. The implementation of these last biological features in the OoCs can also be achieved through the implementation of the 3D structures described above [88, 89].
OoCs’ technology
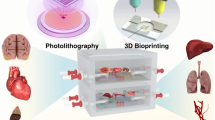
The production of these microsystems mainly relies on silicon rubber polydimethylsiloxane (PDMS), an easy-to-use material that paved the way for the application of OoC technology by many research groups. PDMS characteristics, such as high gas permeability, optical transparency, and high flexibility, make it suitable for cell culture. Microfabrication techniques (photolithography, soft lithography, and replica molding) are easily applied to PDMS to generate patterns and structures relevant to physiological conditions (Fig. 2A and B) [54, 56]. Indeed, OoCs’ features shapes and sizes (e.g., hollow channels) on the scale of nm or μm are obtained thanks to photo- and soft lithography. Such dimensions are in the same range as those sensed by the living cells in the human body [56]. Other techniques are also employed to produce OoCs with the use of different materials. Bioprinting is one of the most promising fabrication approaches, where a cell-laden bioink is printed with supporting materials to construct functional tissues and organs [90, 91]. Different bioprinting methods are available, from the simplest nozzle-based approaches to the most sophisticated optical-based techniques (Fig. 2C) [92, 93]. Notwithstanding the production methods, OoCs can be more biologically functional thanks to the introduction of micro- and biosensors. Some examples are the transepithelial/endothelial resistance (TEER) sensors for analyzing barrier model integrity [94], multielectrode arrays to monitor neuronal networks and cardiac tissues [95, 96], and optochemical sensors to study cell metabolism [97]. Various OoCs were produced in the last years, starting from those replicating the key physiological functional units of whole human organs or tissues, such as the lung [98, 99], liver [100, 101], gut [102, 103], heart [104, 105], skin [106, 107], kidney [108], muscle [109, 110] and the blood–brain barrier [111, 112]. OoCs mimicked also diseased and pathologic conditions like acute SARS-CoV-2 [113, 114], asthma [115], ischemia [116, 117], cardiac fibrosis [118, 119], inflammatory bowel disease (IBD) [120], fatty liver disease (FLD) [121, 122], diabetes [123, 124], Alzheimer’s disease [125] and CoC platforms, recapitulating specific primary tumors with their metastatic site.

The two main microfabrication techniques used to generate organs-on-chip. a Photolithography is the core microfabrication technique used to transfer micro- and nanoscale patterns to photosensitive materials by optical radiation. A silicon wafer is used as support for the photo-sensitive material, which is generally called photoresist. After its application on the wafer’s surface, the wafer is spin-coated to obtain a thin uniform film of the photoresist, which is then brought in contact with a photomask that reproduces the desired pattern. The photoresist crosslink in the parts exposed to high-intensity ultraviolet (UV) light; while the covered photoresist is removed by a chemical agent. The negative design of the mask is now reproduced on the silicon master. b Soft lithography allows the fabrication of elastomeric molds using a replica molding technique. The PDMS is cast against the bas-relief pattern of the silicon master photoresist. After a thermal phase, the resulting substrate is peeled off showing the 3D pattern of the original master. The microfluidic device is then generated by creating the needed features, e.g., the inlets, and by bonding it to a PDMS or glass slab. c 3D bioprinting constructs microfluidic devices using a fast and automated process. In the bioprinting nozzle-based approach, the bioink is extruded through a nozzle moved by a computer-controlled arm to create 3D shapes. Superior resolutions are obtained using optical-based approaches where laser exposure solidifies the bioink through a crosslinking reaction
Cancer-on-chip to study primary tumors and the associated metastatic sites
In recent years, there has been a significant advancement in the development of various models of cancer-on-chip (CoC) systems, which aim to closely resemble the primary and metastatic tumor microenvironment (TME) in an in vivo-like manner. These models have primarily focused on studying specific stages of carcinogenesis, ranging from tumor growth to the metastatic process. Among these models, microfluidic systems have been demonstrated to be able to mimic the in vivo tumor conditions than traditional 2D systems [126, 127].
CoC and the primary tumor
The role of extracellular vesicles (EVs) in influencing primary tumor behavior and growth is of great interest. To investigate their release within a solid tumor model, researchers have developed an intriguing organ-on-chip platform called EV microbioreactors (EVμBRs) [128]. The EVμBRs have demonstrated the ability to replicate cellular physiology and heterogeneity, providing a valuable in vitro tool for investigating the implications of EVs in tumor behavior. Tumor angiogenesis, the formation of new blood vessels in the TME, is another important process in carcinogenesis. Microfluidic devices have been employed to gain deeper insights into this complex mechanism, enabling the study of early stages of tumor growth and the development of the tumor microvascular network [129, 130]. Noteworthy, the spread of tumor cells is closely associated with a phenomenon called epithelial-to-mesenchymal transition (EMT), in which epithelial cells undergo changes and acquire a more mesenchymal phenotype. In one study, researchers generated an EMT index using tumor-derived EVs isolated in a microfluidic chip to evaluate metastatic risk [131]. Other factors involved in promoting EMT have been investigated using organ-on-chip systems, including the influence of mechanical stimuli such as flow-induced hydrodynamic shear stress and the role of hypoxia, in more reliable in vivo conditions [132,133,134].
CoC and the metastatic process
Recently, increasing interest has been in deciphering the mechanisms underlying the metastatic process and investigating the specific organs where tumor cells prefer to metastasize. Several multi-organ microfluidic chips were developed to investigate metastatic events. In a pilot study using a metastasis-on-a-chip, it was observed that primary colorectal cancer cells tend to preferentially metastasize to the lung and liver constructs when fluidically linked to them, consistent with observations in humans [135]. Similar results were obtained when studying lung cancer metastasis using a multi-organs-on-a-chip, considering the liver, lung, and brain as potential metastatic sites [136]. After the settlement of metastatic cells in these organs, specific factors associated with cellular damage were released. These findings align with the “seed and soil” theory, which suggests that tumor cells (the “seed”) can colonize and establish secondary tumors in specific organs or tissues (the “soil”) [137]. The preference of tumor cells for specific organs or tissues is influenced by the molecular characteristics of the cells and the microenvironmental factors of the target site, such as extracellular matrix composition, immune cell presence, and molecular signaling molecules [138].
CoC for the most common cancers
The aforementioned examples highlight the ability of these innovative microfluidic devices to recapitulate crucial aspects of different tumor processes, including development, growth, and metastasis and their applicability to better elucidate these processes. A deeper understanding of tumor cell characteristics and the microenvironments within CoCs holds the potential to provide valuable insights into the factors that either promote or hinder metastatic spread. This knowledge can contribute to the development of more effective strategies for the treatment of metastatic diseases.
A comprehensive review was undertaken to examine CoC models developed for the most common cancers worldwide, such as breast, lung, pancreas, colon, and liver [139, 140]. This review critically discusses the strengths and limitations of these CoC platforms, while also exploring their potential future applications in advancing our understanding of tumor mechanisms.
Breast cancer
Framework
In 2020, 2.3 million women were diagnosed with breast cancer and more than half a million died globally [141]. Breast cancer develops both in the duct and in the lobule of the glandular tissue of the breast. The treatment of primary breast cancer can be highly effective, but there are difficulties with the metastasis sites [141]. Indeed, breast cancer tends to metastasize in the brain, lungs, bones, and liver, leading to the death of many patients [142]. There are several breast cancer subtypes among which triple-negative breast cancer is the most challenging to treat. Intensive efforts are focused on developing new treatments for this tumor type as well as patient-specific therapeutic applications.
CoCs to study the breast primary tumor
In a study, triple-negative breast cancer cell lines were cultured in an organ-on-chip platform based on the standard 384-well plate. The goal was to test breast cancer therapies [143]. Characterization in terms of seeding densities, ECM composition, and biochemical conditions was performed for three distinct breast-cancer cell lines. These cells were exposed to a series of anticancer agents (paclitaxel, olaparib, and cisplatin) and compared to 2D models treated with the same drugs. The executed tests showed a different behavior between 2D and organ-on-chip models. Especially, the response to cisplatin was more like the physiological one in the cell lines treated inside the organ-on-chips. This result was confirmed using primary tumor cells. Therefore, this technology could be a promising tool for personalized medicine and/or could help in the selection of suitable therapies. A lot was done to understand the mechanisms of tumor cell invasiveness and aggressiveness. For example, acidification of the primary tumor environment is considered one of the causes that induce an invasive behavior in cells [144]. The TME acidification and its possible neutralization using CaCO3 nanoparticles (nanoCaCO3) were the main core of a study using a bifurcated chip, with the experimental and control conditions on the same cancer-on-chip [144]. Moreover, hydrostatic pressure was highly controlled so to generate physiological flow inside the channels. Indeed, it was shown that tumor growth and migration were inhibited thanks to a constant buffering of nanoCaCO3 (Fig. 3A). NanoCaCO3 particles induced tumor cell reprogramming by altering the TME pH. Coupling this methodology with drugs that are effective in an acid environment can open the door to new therapeutic strategies.

Examples of breast cancer-on-chips. a Bifurcated chip to study a possible solution for the acidification of the primary tumor environment. (i) Design of the microfluidic device: the upper chambers are loaded with CaCO3 nanoparticles able to neutralize the acidification of the TME. (ii) Chip setup. Pipette tips are used to feed the upper and lower chambers, while the middle channel (which ensures the separation between the control and experimental compartments) is connected to a syringe pump. Adapted from [144] with permissions from Scientific Reports. b Organ-on-chip model to analyze the tissue-specific breast cancer extravasation. (i) Schematic illustration of the extravasation chip with the Side 2 view highlighted. (ii) Z-stack projection images of Side 2 view showing HUVEC-C endothelial monolayers (green), extravasated (arrowhead), and associated (arrow) human breast cancer cells (MDA-MB-231, red) into the lung, liver, or breast microenvironments. Adapted from [145] with permissions from Biotechnology & Bioengineering. c Miniaturized bone-on-a-chip to study breast cancer bone metastasis. (i) Schematic of the simultaneous-growth-and-dialysis mechanism. Low-molecular-weight nutrients and metabolic waste move continuously through the dialysis membrane. While large bone matrix-building proteins accumulate in the bottom chamber contributing to the spontaneous formation of the osteoblastic tissue. (ii) Exploded view of the bone-on-a-chip. (iii) Injected inks highlight the central circular area of the assembled chip. Dialysis occurs in this space. Adapted from [146] with permissions from Small
Breast CoCs for the metastatic behavior
Important aspects of breast cancer metastasis are intravasation and extravasation events. Intravasation refers to tumor cells entering the blood circulation, while extravasation refers to tumor cells exiting from the bloodstream and creating a new colony. The interactions between metastatic tumor cells and the blood vasculature were studied in an engineered 3D vasculature. This structure was generated through rapid multilayer microfabrication, where subpopulations of triple-negative breast cancer cells were seeded surrounded by osteoblasts, bone marrow-derived mesenchymal stem cells, or lung fibroblasts [147]. Experiments were performed mimicking the lung or the bone microenvironment. The obtained results highlighted that the osteoblasts play a crucial role in the selective extravasation of bone MDA-231, a specific breast tumor subpopulation. Therefore, this technology proved to be useful in the investigation of organotrophic metastasis and a helpful tool in identifying targets and treatment strategies to benefit patients. Another study was performed by developing two novel cancer-on-chips to analyze the tissue-specific breast cancer invasion/chemotaxis and extravasation [145]. Liver, lung, and breast microenvironments were mimicked to distinguish invasion/chemotaxis toward these different tissues. It was observed that metastatic breast cancer cells tend to invade the lung and liver more than the breast tissue. Moreover, the lung-specific metastatic cell subpopulation had a higher invasion behavior in the lung microenvironment than other metastatic cell subpopulations, like the bone one. Finally, an extravasation model was implemented, which comprised also an intact endothelial monolayer. It was shown that metastatic breast cancer cells are prone to cross the endothelial barrier when the lung microenvironment is simulated (Fig. 3B). These results could help to improve cancer diagnosis and select the best therapeutic option. Other factors can play an important role in breast cancer metastasis. For example, a study analyzed the role of the sympathetic nervous system (SNS) in the modulation of breast cancer metastasis [148]. In this research, a human metastasis-on-chip platform was developed to reproduce the effect of sympathetic activation on the dynamic crosstalk between bone tropic breast cancer cells and osteoclasts. It was shown that bone tropic breast cancer cells received synergistic inputs from neurons and osteoclasts. The osteoclasts increased pro-inflammatory cytokines that are important for the progression of breast cancer bone metastasis and osteoclastogenesis. This finding proved the importance of correctly reproducing the interactions of the specific metastatic microenvironment. Moreover, this microfluidic model allowed stopping communications among the three different compartments, bone tropic breast cancer cells, sympathetic neurons, and osteoclasts. In particular, the above-described effects on breast cancer bone metastasis and osteoclasts were not present when the interaction between bone and neuron compartment was interrupted, even if the levels of the studied pro-inflammatory cytokines remained quite stable. Bone metastasis generated by metastatic breast cancer cells was also studied using a miniaturized bone-on-a-chip (Fig. 3C) [146]. A naturally thick mineralized 3D tissue was generated by applying the principle of simultaneous growth dialysis. The resulting bone tissue provided the necessary microenvironment for the colonization of metastatic breast cancer cells. Both metastatic and metastasis-suppressed breast cancer cells were introduced into the developed osteoblastic tissue. The metastasis-suppressed breast cancer cells showed the expected dormant behavior with limited metastases. On the other hand, the metastatic cells replicated key features and characteristics usually observed in vivo, such as the invasion of the mineralized tissue apical layer, invadopodia protrusion, and formation of the so-called “Indian files” formed by the invading cancer cells. Therefore, the developed bone-on-a-chip proved to be a physiologically relevant model for the study of breast cancer bone metastasis in vitro.
Breast CoCs’ advantages and limitations
In summary, the described breast cancer models have advantages in terms of more suitable therapies’ selection in the context of personalized medicine [143], in the study of the mechanisms behind tumor cells’ invasive behavior [144], in the analysis of the intravasation and extravasation events [145, 147], and in the replication of the metastatic microenvironment to identify the key phenomena [146, 148]. Organotropism, the non-random process where distant metastases are distributed to specific organs, can be elucidated thanks to the use of CoCs giving hints to identify better therapies for patients [138, 145]. However, these studies were not always able to replicate the 3D structure of the tumor microenvironment [143] and the associated stromal cells that are pivotal for the correct representation of the TME [144].
Lung cancer
Framework
Lung cancer is one of the most diagnosed cancers worldwide with a high mortality rate [149]. Public health measures have been implemented in industrialized countries to reduce smoking, which is the main cause of such cancer. However, a high smoking incidence is still present in low-income nations. On the other hand, the lung cancer subtype adenocarcinoma continues to occur in people that have never smoked [149]. Lung cancer often metastasizes in the liver, brain, bones, breast, and kidney, with a very low survival rate for patients with metastasis. Therefore, the high and aggressive progression and the well-known resistance to chemotherapy have led to a search for better methods to investigate the mechanisms of lung cancer development and metastasis [150]. In this context, organ-on-chips represent a promising option to elucidate the underlying processes of lung cancer.
CoCs to study the lung primary tumor
A study was performed to reproduce human orthotopic models of non-small cell lung cancer (NSCLC) in vitro [151]. The aim was to recapitulate the in vivo-like TME and investigate tumor growth using a lung-on-chip device made of two parallel channels separated by a porous membrane. Epithelial cells and a low density of NSCLC cells were cultured in one channel on the porous membrane, while human lung microvascular endothelial cells were cultured on all four walls of the facing channel, forming a hollow vascular lumen. A mechanical suction was applied to mimic normal breathing. Indeed, it was found that this mechanism significantly suppressed lung cancer growth. Resistance to tyrosine kinase inhibitor (TKI) therapy of patients showing specific mutations was successfully reproduced in this orthotopic device. This mechanism was never observed in the conventional 2D in vitro models. The simulation of the alveolar microenvironment to study lung cancer was achieved by implementing a poly(lactic-co-glycolic acid) (PLGA) electrospinning nanofiber membrane as the cell scaffold of a lung-on-chip [152]. A human NSCLC (A549) and a human fetal lung fibroblast (HFL1) cell lines were co-cultured in the chip device on the upper and lower sides of the membrane, respectively. This study evaluated the effect of gefitinib, a selective inhibitor of the epidermal growth factor receptor (EGFR)-tyrosine kinase. Significant resistance to drug treatment was observed in A549 and HFL1 cell co-culture, thus confirming the role of HFL1 cells in decreasing tumor cells’ sensitivity to chemotherapy. Moreover, A549 and HFL1 cells were co-cultured with endothelial cells (HUVEC). This experiment showed how A549 cells became strongly invasive destroying the endothelial barrier and starting the metastatic invasion process. Therefore, reproducing the TME is pivotal to obtaining a pathophysiological model. A 3D microfluidic lung cancer model was developed to investigate the role of the stromal cells in lung tumorigenesis and to resemble as much as possible the in vivo TME [153]. This in vitro lung cancer platform was established by tri-culturing endothelial cells, fibroblasts, and lung cancer cells within a 3D collagen matrix (Fig. 4A). The presence of fibroblasts allowed the formation of the tumor environment by regulating the biophysical and biochemical properties of the TME. Moreover, the vasculogenesis induced by fibroblasts was confirmed thanks to the establishment of a stable in vitro tumor model with a complex structure.

Examples of lung cancer-on-chips. a Microfluidic chip for the study of the role of the stromal cells in tumorigenesis. (i) An in vivo-simulating representation of the TME was achieved by integrating into the same microfluidic device stromal cells, fibroblasts, and endothelial cells surrounded by a 3D collagen matrix with a channel for the continuous flow of the culture medium. (ii) Overview of the main components interacting with the microfluidic device. Adapted from [153] with permissions from Scientific Reports. b Microfluidic device to recapitulate the metastatic brain niche. (i) Representation of the bTME composed of BM-NSCLC, cerebral microvascular endothelial cells, and primary human brain astrocytes. (ii) Configuration of the seven-channel microfluidic device with its cross-section showing where each cell type is cultured. Adapted from [154] with permissions from Advanced Science. c Multi-organs-on-a-chip for the study of different metastatic sites. (i) Schematic illustration of the multi-organs-on-a-chip comprising the primary site of cancer (the lung, in purple) and the three distant organs (inlet 3, inlet 4, and inlet 5). (ii) Representation of the chip lung structure, where a membrane divides the air compartment from the blood one. Lung cancer cells are co-cultured with human bronchial epithelial cells on the upper side of the membrane, while stromal cells (microvascular endothelial cells, fibroblasts, and macrophages) are seeded on the lower side. Metastatic lung cancer cells move along the blood channel to reach distant organs, the brain, bone, and the liver. (iii) Overview of the chip structure composed of three main layers and two microporous membranes. Adapted with permission from [136]. Copyright 2016 American Chemical Society
Lung CoCs for the metastatic behavior
A lot was done to elucidate the mechanisms of the lung cancer metastasis process and to investigate the characteristics of the metastatic sites. In a seven-channel 3D microfluidic platform, brain metastatic non-small cell lung carcinoma (BM-NSCLC), cerebral microvascular endothelial cells, and primary human brain astrocytes were cultured together to reconstitute the brain tumor microenvironment (bTME) (Fig. 4B) [154]. The enhanced cancer cells’ survival was studied revealing the activation of specific pathways against the anti-cancer drugs. Moreover, cytokine-related intracellular pathways were discovered to be responsible for the acquired drug resistivity. This model elucidated the communication mechanisms among the different components of the bTME. A multi-organs-on-a-chip was developed including the primary site of cancer (the lung) and three different metastatic organs (the brain, bone, and liver) (Fig. 4C) [136]. Changes in lung cancer cells and expression of specific epithelial and stromal markers were identified as clear signals of tumor growth and cell invasive capacity. Cell–cell interactions during metastasis have been elucidated thanks to this microfluidic device.
Lung CoCs’ advantages and limitations
In conclusion, the described lung cancer-on-chip models highlight the potential of these systems in studying tumor growth and its response to specific therapies [151, 152]. They confirm the important role of TME reproduction to resemble as much as possible the in vivo conditions [154] and describe the communication mechanisms and interactions among the different TME components in the metastatic organs [136, 154]. Better pathophysiological models could be obtained by introducing specific TME components that play a role in tumor progression [151, 152] and cancer-associated immune cells [154].
Pancreatic cancer
Framework
There are two main types of pancreatic cancer: exocrine and rare endocrine cancer. Exocrine Pancreatic Ductal Adenocarcinoma (PDAC) has one of the lowest survival rates [155]. Failure of current chemotherapeutics is reasonably due to the high molecular heterogeneity of PDAC and its intricate tumor microenvironment [156, 157]. A specific system is pivotal for drug discovery and personalized medicine in such cancer.
CoCs to study the pancreatic primary tumor
Few successful attempts have been published so far, notwithstanding a pancreas-on-a-chip was generated for the first time in 2015 [158]. This model was inflated with isolated patient-derived pancreatic ductal organoids mimicking pancreatic cell function and interface in situ (Fig. 5A). Even if this model didn´t recapitulate the pancreatic TME, it represents the first physiologic-like model of the pancreas. A study was carried out to develop a platform useful in the diagnosis and prognosis of PDAC, the so-called HepaChip® [159]. The obtained results demonstrate the feasibility of PDAC cell cultures in a microfluidic chamber under continuous and controlled perfusion (Fig. 5B). Moreover, the chemotherapeutic drug cisplatin was tested in the organ-on-chip model giving consistent responses with what is observed in vivo. Pancreatic patient-derived organoids were cultured in a microfluid scaffold platform called InVADE. This study aimed to elucidate the evolution of the PDAC stroma and its effects on drug bioavailability. The resulting vascularized human PDAC model also captured the hallmarks of an evolving TME thanks to a co-culture with human fibroblasts [160].

Examples of pancreatic cancer-on-chips. a Pancreas-on-a-chip to model fibrosis-related disorders. (i) Pancreatic ductal epithelial cells (PDCEs) were cultured inside the single-channel chip (ii) together with pancreatic islets (iii) to monitor the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) function. Adapted from [158] with permissions from Nature Communications. b HepaChip® for the diagnosis and prognosis of PDAC. (i) Image of the chip with the 8 culture chambers. The electrodes and ridges present in each chamber are shown together with flow velocity and trajectory simulation. (ii) Live/Dead of the PDAC cells after 146 h of culture inside the HepaChip®. Adapted from [159] with permissions from Scientific Reports. c Organ-on-chip to model the invasion of PDAC tumor cells to blood vessels. (i) Two hollow cylindrical channels in the microfluidic device mimic the blood vessel and the pancreatic cancer duct, respectively. Endothelial cells (HUVEC) were seeded in the perfusable vessel, while pancreatic cells were cultured in the cancer duct. (ii) Representation of the average invasion distance of the PDAC cell line PD7591 when an FBS gradient is established and with/without the HUVEC cells. Speed migration is increased when the HUVECs are present. Adapted from [161] with permissions from Science Advances
Pancreatic CoCs for the metastatic behavior
The most frequent pancreatic cancer metastasis occurs in the liver, peritoneum, and lung (80%, 48%, and 45%, respectively) [162]. Indeed, pancreatic cancer expresses and secretes a plethora of proangiogenic factors [163], even if it is poorly vascularized [164]. In 2019, a 3D organotypic model helped to shed light on this mechanism (Fig. 5C). This model was able to recapitulate the invasion of PDAC tumor cells to blood vessels, showing how these cells can rapidly penetrate the lumen of blood vessels and ablate the endothelial cells [161].
Pancreatic CoCs’ advantages and limitations
The reported examples show how these models can reproduce the main physiological features of the pancreas in vitro [158], the major characteristics of the PDAC TME, and its response to drug therapy [159, 160]. Moreover, pancreas cancer-on-chip models help better understand this cancer type's metastasis mechanisms [161]. However, still, too few studies have been published to better investigate this type of cancer and the related metastasis mechanisms, and the described ones lack important TME components and cancer-associated stromal cells [159].
Colorectal cancer
Framework
Colorectal cancer (CRC) represents the second leading cause of cancer-related death and the third most diagnosed cancer worldwide [165]. CRC is largely asymptomatic until it progresses to advanced stages characterized by distant metastasis and poor overall survival [166, 167]. The liver represents the most common CRC metastatic site: 25–30% of patients present colorectal liver metastasis (CLM) at the time of diagnosis or develop it after the primary tumor resection [168, 169]. Furthermore, most of these patients are not eligible for curative surgery at the time of diagnosis and they usually have a 5-year survival rate (< 15%) [170, 171]. This highlights the urgent need to improve drug treatments along with a deeper understanding of the biological mechanisms of CRC. In such a scenario, several OoCs were developed in the last years aimed to elucidate in depth the CRC molecular pathways, perform drug testing and understand the metastatic steps of this disease [135, 172,173,174,175].
CoCs to study the colorectal primary tumor
A vascularized micro-tumor (VMT) device composed of three tissue chambers was co-cultured with different human cell types: endothelial colony-forming cell-derived endothelial cells (ECFC-EC), normal lung fibroblasts (NHLF), and colorectal cancer cells (HCT116 and SW480) (Fig. 6A) [172]. Once the cells were seeded in each tissue compartment, they were exposed to a physiological flow. This mechanical stimulus led to complex self-organization from day 5 in culture. To better characterize this innovative platform, transcriptomic analysis was performed on HCT116 cells grown in the VMT, implanted as a xenograft tumor, and cultured in the conventional 2D culture system. The results showed that gene expression of HCT116 cells from the VMT closely resembled that grown in vivo while differing from the same cells cultured in the 2D system. Indeed, several pathways were found to be enriched in the VMT and xenograft-derived cells compared to 2D monocultures, such as MAPK signaling, PI3K-Akt signaling, and microsatellite instability. Furthermore, the same comparison was performed to evaluate the response to FOLFOX (5-fluorouracil, leucovorin, and oxaliplatin), the first-line treatment for CLM patients [176]. HCT116 and SW480 cells derived from VMT or xenograft tumors showed a significant reduction in drug sensitivity compared to the cells grown in 2D. These findings suggest that the VMT system can recapitulate the in vivo CRC features, such as tumor drug response. Due to the increasing attention to the TME and its relationship with tumor progression and response to drug treatments, the interaction between CRC cells and fibroblasts was studied in a microfluidic device fabricated with seven channels: three to host colorectal adenocarcinoma cell line (HT-29) and normal colon fibroblasts (CCD-18Co), and four to provide nutrients with the medium (Fig. 6B) [177]. In this device, a significant increase in HT-29 spheroid size was observed when co-cultured with CCD-18Co compared with the monoculture spheroids suggesting the growth-promoting role of fibroblasts for tumor cells. At the same time, CCD-18Co showed an increase in the levels of αSMA and F-actin in the co-culture with tumor cells, highlighting the established crosstalk between the two cell types. Furthermore, the treatment with paclitaxel revealed that tumor cells in co-culture with fibroblasts were less sensitive to this drug treatment compared with HT-29 monoculture. This result suggests the importance of developing culture systems able to mimic the in vivo TME and its role in chemotherapeutic resistance.

Examples of colon cancer-on-chips. a The vascularized micro-tumors (VMTs) are composed of 3 tissue chambers (T1-3), hosting CRC cells, fibroblasts, and endothelial cells. There is also a pressure regulator (PR) to prevent the gel rupture, two loading ports (L1-2), and two medium inlets and outlets (M1-2). The entire structure is bonded onto a bottomless 96-well plate. Reproduced from [172] with permission from The Royal Society of Chemistry. b Schematic representation of the microfluidic device for tumor and fibroblast cells co-culture composed of seven channels: three to host cells and four for the media. Reproduced with permission [177] Copyright 2016, Jeong et al. c The CRC-on-chip (image courtesy of Emulate, Inc.) is composed of two channels: at the top, the epithelial channel (1), hosting epithelial and CRC cells (3); at the bottom, the endothelial channel (2), hosting HUVEC cells (4). The two channels are divided by a porous membrane (5). Reproduced with permission [174]. Copy-right Strelez et al., 2021. d Metastasis-on-a-chip (MOC). To provide an equal flow into all device chambers, the media was perfused from the colorectal compartment and then bifurcated twice to the endothelial (E), lung (Lu), and liver (Li) constructs. Reproduced with permission [135]. Copyright 2019, John Wiley and Sons
Colorectal CoCs for the metastatic behavior
Intense efforts were focused on reproducing CoC models to investigate the metastatic process of CRC cells and their dissemination to the metastatic site. To this scope, a CRC-on-chip was developed by incorporating key features of the TME (e.g., shear force mimicking peristalsis) in a two compartments device. Intestinal epithelial cells (Caco2, C2BBe1) were seeded in the upper chamber and left to generate a complete functional barrier. The lower chamber hosted endothelial cells (HUVEC). After a few days in culture, CRC cells (HC116 or HT29) were injected into the intestinal compartments and exposed to constant flow and stretch conditions, which led to the formation of CRC cell clusters on the top of the 3D structure of the intestinal cells (Fig. 6C) [174]. HCT116 cells showed a significant invasion ability compared to HT29 cells and several metabolic pathways were identified to be greatly enriched in the most invasive cell type. Furthermore, these cells were more heterogeneous in the endothelial chamber compared to the same cells on 2D plastic. In particular, the invasive characteristics of HCT116 were found to be pronounced when a fluid flow, mimicking the physiological peristalsis, was applied to the device or in the presence of cancer-associated fibroblasts. These results showed the fundamental role of each TME component in the behavior of tumor cells. A multi-organs-on-chip was developed to elucidate the mechanisms of cells spreading to different organs. The metastasis-on-chip (MOC) was designed to host the primary tumor construct and three target tissues (liver, lung, and endothelial compartments) (Fig. 6D) [135]. After ten days in culture, the cancer HTC116 cells, originally seeded in the CRC chamber, started to disseminate in the circulating flow reaching the downstream target tissues and showing a different localization between lung and liver sites. In the lung, HCT116 cells were mainly found around lung cells, while they showed higher engraftment in the liver site. Therefore, the tumor cell dissemination process and the phenomena underlying the preferential metastatic site could be understood thanks to the reproduction of a more in vivo-like environment in the multi-organs-on-chip model.
Colorectal CoCs’ advantages and limitations
In summary, the described CRC chips represent a superior alternative to the current in vitro models. In vivo-like responses are obtained using the material and data from CRC organ-on-chip platforms [172, 176]. TME features are successfully reproduced to study how the tumor grows and reacts to pharmacological treatments [177]. Moreover, the study of the factors driving metastatic behaviors is also possible thanks to the implementation of such models [135, 174]. Notwithstanding, some important TME features are still missing, like the immune component [172, 177]. Another limit is the use of immortalized cell lines instead of patient-derived cells [172]. Indeed, the use of patient-derived cell populations is the best way to represent the heterogeneity of human cancer biology.
Liver cancer
Framework
Primary liver cancer is the sixth most diagnosed cancer worldwide, accounting for almost 900.000 new cases per year [178]. Hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (iCCA) represent the two major histological types, resulting in 75% and 15% of all liver cases, respectively [178, 179]. Primary liver cancers are characterized by poor 5-year survival rates and few therapeutic strategies are available. Indeed, surgery still represents the main curative option for these patients [140, 180]. In the last years, intense efforts were dedicated to developing cutting-edge culture systems to mimic in vivo liver tumors and elucidate the molecular mechanisms.
CoCs to study the liver primary tumor
A biomimetic liver tumor-on-chip was designed by seeding HepG2 cells, an HCC immortalized cell line, in a decellularized liver matrix enriched with gelatin methacryloyl (GelMa). This structure closely mimics the 3D complexity of the hepatic microenvironment, thanks to the presence of essential ECM proteins, growth factors, shear stress, and matrix stiffness [181]. This perfusion-based platform observed a dose-dependent response after treatment with acetaminophen and sorafenib. This result evidences that specific matrix proteins are needed to better emulate cancer biophysical properties and have an accurate platform for drug screening. A microfluidic platform was co-cultured with hepatoma cells (Hepa1-6) and hepatic stellate cells (JS-1) to study the role of hypoxia in the anticancer effect of paclitaxel (PTX) and tirapazamine (TPZ) in a more reliable microenvironment (Fig. 7A). Hepa1-6 and JS-1 cells showed a decrease in the viability after treatment with both drugs in monoculture and normoxic conditions. Instead, increased drug resistance was observed when Hepa1-6 cells were co-cultured with JS-1 cells. This effect was enhanced after PTX treatment in the hypoxic condition compared to the normoxic one. These results suggested that the activation of hepatic stellate cells could interfere with the resistance to PTX of the hepatoma cells in hypoxia and co-culture conditions [182]. This liver tumor-on-chip model demonstrated its ability to replicate the tumor niche and represents a useful platform for drug screening. Only one microfluidic system is reported in the literature for the study of CCA. This system was developed as a diagnostic tool to detect the circulating tumor cells (CTCs) in human bile (Fig. 7B) [183]. In this micrometric platform, composed of different modules, the cells isolated from the human bile are loaded and incubated with magnetic beads targeted against the EpCAM, an epithelial cell molecule, to isolate the cellular complexes (upper module of the chip). Subsequently, an immunofluorescence staining is performed with two specific anti-cytokeratin for CCA cells and, finally, the CTCs are detected and quantified in the sample (lower module of the chip). This different use of microfluidic technology underlines its potential role in the medical and biological fields.

Examples of liver cancer-on-chips. a Schematic design of the microfluidic device. (i) The left channel was used to generate the hypoxic gradient (red fluorescent image), flanked by the culture compartment composed of three adjacent channels. (ii) Image of the co-culture compartments. Reproduced from [182] with permission from the Chinese Journal of Analytical Chemistry. b Cholangiocarcinoma-on-chip to detect the CTCs in the human bile. (i) Image of the chip with its compartments. Upper module: A, sample loading chamber; B, membrane-type micromixers/micropumps; P, PBS chamber; W, waste outlet. Lower module: C, membrane-type micromixers/micropumps; D, paraformaldehyde chamber; E, Triton X-100 chamber; F - G, first and secondary antibody chambers, respectively; H, DAPI/Hoechst stain chamber; P, PBS chamber; W, waste outlet. (ii) Schematic representation of the cell capture, washing, collection, and immunofluorescence (IF) staining and analysis on-chip. Reproduced from [183] Copyright Hung et al., 2017
Liver CoCs’ advantages and limitations
In conclusion, on the one hand, liver tumor-on-chips prove to have clear advantages concerning conventional in vitro models. Biophysical properties and TME features can be recapitulated in these platforms providing better results in terms of drug screening [181, 182]. On the other hand, even if models that reproduce the CCA tumors are still undiscovered, applications studying the characteristics of these cancer cells start to appear in the scenario of microfluidic systems [183]. In general, studies that focus on elucidating metastatic behavior are still absent and more efforts are necessary to better understand and replicate the main TME components of this cancer type.
Cancer-on-chip: pros & cons and future perspectives
Cancer-on-chip has been identified as a promising technology for studying the environment and the development of different cancers. It is becoming a possible powerful tool for different oncology applications (Fig. 8).

Overview of the possible cancer-on-chips applications. In general, these microfluidic devices can be used to study all cancer features and stages, to perform anti-cancer drug screening in terms of safety and efficacy, and to implement personalized medicine using patient-derived cells
These tiny devices can mimic the physiology and the pathophysiology of a target human organ, resembling human body conditions [151]. Compared to the in vivo models, the lower cost, and the possibility to have animal-free approaches should lead to extensive use of these devices, especially in the study of cancer and the possible therapies [184]. These models are considered superior to the 2D in vitro counterparts [185]. In the organ-on-chips, the implemented cell constructs are often in three dimensions, better recapitulating the cell–cell interactions by regulating key important factors such as nutrients, cytokines, and hormones. Anyway, most of the developed cancer-on-chip models still rely on the use of cell lines. Indeed, the implementation of primary cells, especially patient-derived, could be an important step to obtain a superior reproduction of the in vivo conditions. Different organs and tissues can be represented within the same platform, having a better model to study a specific phenomenon or structure [136]. The microenvironment could also be recapitulated with the flow key component. Indeed, important mechanical and chemical stimuli are generated thanks to the movement of the medium inside the designed channels, like shear stress and specific factors’ gradients, thus reproducing the in vivo conditions. The implementation of the flow and the perfused endothelial-lined vessels allow the study of several processes such as cancer cell intravasation, extravasation, and dissemination [132, 186]. Moreover, drug delivery studies are better modeled than in conventional in vitro systems thanks to the samples collected from compartments dedicated to a specific organ [143]. In the OoCs, sensors with different outputs (e.g., temperature, pH, and oxygenation) can be added to control the microenvironment and perform measurements in real-time [187]. For example, sensors have been implemented for the control and measurement of physical features, such as flow [188], temperature [189], and pH [190]. Specific sensors have been used for cancer-on-chips: an electrical cell-substrate impedance sensing (ECIS) was implemented for the monitoring of single cancer cells [191]; an electrical biosensor based on nano roughened poly(methyl methacrylate) (PMMA) was used to detect the metastatic cells [192]; and a surface plasmon resonance imaging (SPRI)-impedance sensor was applied to analyze the status of living cancer cells in real-time [193]. On one hand, this versatility represents a strong driver in the adoption of the technology, and it is essential to have trustworthy and robust organ-on-chip models. On the other hand, such sensor implementation makes organ-on-chip complex systems often not easily exploitable by people without the required expertise. In general, OoCs are more difficult to implement than other 3D models, like spheroids, which usually show a higher throughput [194]. PDMS is the most widely used material for organ-on-chip production due to its high biocompatibility, transparency, and oxygen permeability. However, the major drawback of PDMS is its nonspecific absorption of small hydrophobic molecules, including some drugs [195]. Therefore, new materials should be developed and implemented for organ-on-chip production by retaining the same important characteristics of PDMS, in terms of biocompatibility and optical clarity, but with low or null drug absorption. Solutions can be found using for example additives [196], coatings [197, 198], and completely other materials [199,200,201]. High pressure is put on the users to find materials that fit the purpose and the aim of the device’s application. For this reason, several manuals have appeared [202, 203] to guide users to make a more informed and correct choice. Technical robustness is another challenge that should be overcome. The small scale and the high complexity of these systems make them sensible to simple factors, like bubbles, that can impair the interplay of the implemented controls and features with the loss of organ-on-chip functionality [204]. Studies have been performed trying to prevent the formation of bubbles by providing hints about channel structuring and characteristics [205] or strategies to efficiently remove the bubbles [206]. Finally, organ-on-chip devices should be manufactured according to Good Manufacturing Practices (GMP), and the tests conducted following the in-force Good Laboratory Practices (GLP) and the Good In Vitro Method Practices (GIVIMP) [207]. These are the requirements to be recognized as pre-clinical tools. Indeed, even if most of the OoCs are tested for reproducibility, the variability due to the user-to-user component is still difficult to control. Fabrication and cell culturing methods are developed by each user mostly without any guidance. This leads to OoCs that differ in technological and biological aspects [55]. The passage from the results obtained in the micron-scale to a possible application at the macro-scale (scalability) is therefore hampered due to the lack of standardization [55]. These limitations get worse if complex multi-organ interactions are implemented. To summarize, organ-on-chip technology is still in its young phase and several challenges must be overcome as well as improvements adopted (Fig. 9). But the technological advancement of these platforms keeps on increasing. Table 2 provides an overview of some implemented solutions to reduce the impact of the described challenges. Regarding CoCs, future development relies on personalized medicine [208]. Patient-derived cells could be directly cultured within the platform providing a precise tool to better investigate the biological mechanisms underlying cancer development and to investigate the most suitable patient-specific drug therapy during the clinical trials. However, obtaining patient-specific cells is often challenging [209]. A possible solution relies on the use of stem cells. But this cellular model shows limitations in terms of technical reprogramming, increased genetic instability, especially of the induced pluripotent stem cells (iPSC), and the highly variable (but typically low) efficiency of stem cell differentiation across cell lineages [210]. Another limitation of cancer-on-chips is the simplicity of these devices, since only the essential components are usually recapitulated, missing some important chemical and physical characteristics inherent to the TME. Help is coming from the increased awareness of cancer microenvironment physiology, which is leading to more representative and even modular devices [211]. Moreover, the development of a cancer-on-chip that reproduces the entire body (body-on-chip) or multiple organs fluidically connected is aiding in a better understanding of the cancer pathophysiology, the structure, the hidden mechanisms, and the metastatic process [212].

Summary of pros and cons of cancer-on-chips. Many pros are identified for the cancer-on-chip technology when compared to the conventional in vitro and in vivo models. However, acceptance of cancer-on-chip as a pre-clinical tool has several drawbacks that must be solved
Conclusion
The current in vitro and in vivo models show evident limitations in reproducing the complexity of the TME and studying cancer progression and metastasis. Cancer-on-chips could provide the necessary complexity to express the pathophysiology and the cell–cell crosstalk within the TME and allow for studying tumor development and progression in a more in vivo-like environment. This new technology represents an advanced and unique way to reveal underlined molecular, chemical, and cellular mechanisms with a key role in cancer progression. Furthermore, the development of these platforms using patient-specific cells could help obtain a more realistic tool to faithfully recapitulate the main characteristics of the TME. The possibility to integrate multiple organs in the same platform has the huge potential to reproduce in vitro realistic models of invasiveness and metastatic tumors, thus better mimicking the intricate pathologic conditions. However, intense efforts are needed from academic researchers, manufacturers, and regulators to push the adoption of organ-on-chip technology as an alternative to the 2D in vitro and in vivo models. Indeed, the establishment of good practices as well as shared and approved standard protocols could guarantee the fundamental required quality allowing the use of organ- and cancer-on-chip as a keystone to close the gap between the pre-clinical and clinical studies.
Availability of data and materials
Not applicable.
Abbreviations
- 2D:
-
Two-dimensional
- 3D:
-
Three-dimensional
- BBB:
-
Blood-brain barrier
- BM-NSCLC:
-
Brain metastatic non-small cell lung carcinoma
- bTME:
-
Brain tumor microenvironment
- CAFs:
-
Cancer-associated fibroblasts
- CCA:
-
Cholangiocarcinoma
- CCL2:
-
Chemokine (C–C motif) ligand 2
- CCL5:
-
Chemokine (C–C motif) ligand 5
- CCL7:
-
Chemokine (C–C motif) ligand 7
- CFTR:
-
Cystic Fibrosis Transmembrane Conductance Regulator
- CLM:
-
Colorectal liver metastasis
- CoC:
-
Cancer-on-chip
- CRC:
-
Colorectal cancer
- CSE:
-
Cigarette smoke extracts
- CTC(s):
-
Circulating tumor cell(s)
- CXCL12:
-
Chemokine (C-X-C motif) ligand 1
- dT-MOC:
-
Ductal tumor-microenvironment-on-chip
- EB(s):
-
Embryoid body(ies)
- EC(s):
-
Endothelial cell(s)
- ECFC-EC:
-
Endothelial colony-forming cell-derived endothelial cells
- ECIS:
-
Electrical cell-substrate impedance sensing
- ECM:
-
Extracellular matrix
- EGFR:
-
Epidermal growth factor receptor
- EMT:
-
Epithelial-to-mesenchymal transition
- EV(s):
-
Extracellular vesicle(s)
- EVμBR(s):
-
Microfluidic
- EV:
-
Microbioreactor(s)
- FGF:
-
Fibroblast growth factors
- FLD:
-
Fatty liver disease
- FOLFOX:
-
5-Fluorouracil, leucovorin, and oxaliplatin
- GelMa:
-
Gelatin methacryloyl
- GIVIMP:
-
Good In Vitro Method Practices
- GLP:
-
Good Laboratory Practices
- GMP:
-
Good Manufacturing Practices) and the
- HCC:
-
Hepatocellular carcinoma
- HFL1:
-
Human fetal lung fibroblasts
- IBD:
-
Inflammatory bowel disease
- iCCA:
-
Intrahepatic cholangiocarcinoma
- IL-8:
-
Interleukin-8
- IORT:
-
Intraoperative radiotherapy
- MOC:
-
Metastasis-on-chip
- MMP2:
-
Matrix metalloproteinases 2
- MMP9:
-
Matrix metalloproteinases 9
- NanoCaCO3 :
-
CaCO3 nanoparticles
- NHLF:
-
Normal lung fibroblasts
- NSCLC:
-
Non-small cell lung cancer
- OoC:
-
Organ-on-chip
- PTX:
-
Paclitaxel
- PDAC:
-
Pancreatic ductal adenocarcinoma
- PDCE(s):
-
Pancreatic ductal epithelial cell(s)
- PDGF:
-
Platelet-derived growth factors
- PDMS:
-
Polydimethylsiloxane
- pH:
-
Power of hydrogen
- PLGA:
-
Poly(lactic-co-glycolic acid)
- PMMA:
-
Poly(methyl methacrylate)
- SDF-1:
-
Stromal cell-derived factor 1
- SNS:
-
Sympathetic nervous system
- SPRI:
-
Surface plasmon resonance imaging
- TEER:
-
Transepithelial/endothelial resistance
- TGFβ:
-
Transforming growth factor beta
- TKI:
-
Tyrosine kinase inhibitor
- TME:
-
Tumor microenvironment
- TPZ:
-
Tirapazamine
- TS(s):
-
Tumor spheroid(s)
- UV:
-
Ultraviolet (light)
- VMT(s):
-
Vascularized micro-tumor(s)
- μ-CCD:
-
Microfluidic hanging drop-based spheroid co-culture device
References
Kocarnik JM, Compton K, Dean FE, Fu W, Gaw BL, Harvey JD, Henrikson HJ, Lu D, Pennini A, Xu R, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: a systematic analysis for the global burden of disease study 2019. JAMA Oncol. 2022. https://doi.org/10.1001/jamaoncol.2021.6987.
Soerjomataram I, Bray F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nat Rev Clin Oncol. 2021. https://doi.org/10.1038/s41571-021-00514-z.
Winkle M, El-Daly SM, Fabbri M, Calin GA. Noncoding RNA therapeutics - challenges and potential solutions. Nat Rev Drug Discov. 2021. https://doi.org/10.1038/s41573-021-00219-z.
Davis-Marcisak EF, Deshpande A, Stein-O’Brien GL, Ho WJ, Laheru, D, Jaffee EM, Fertig EJ, Kagohara LT. From bench to bedside: single-cell analysis for cancer immunotherapy. Cancer Cell. 2021. https://doi.org/10.1016/j.ccell.2021.07.004.
Propper DJ, Balkwill FR. Harnessing Cytokines and Chemokines for Cancer Therapy. Nat Rev Clin Oncol. 2022. https://doi.org/10.1038/s41571-021-00588-9.
Law AMK, Rodriguez de la Fuente L, Grundy TJ, Fang G, Valdes-Mora F, Gallego-Ortega D. Advancements in 3D cell culture systems for personalizing anti-cancer therapies. Front Oncol. 2021. https://doi.org/10.3389/fonc.2021.782766.
Jensen C, Teng Y. Is it time to start transitioning from 2D to 3D cell culture? Front Mol Biosci. 2020. https://doi.org/10.3389/fmolb.2020.00033.
Paradiso F, Serpelloni S, Francis LW, Taraballi F. Mechanical studies of the third dimension in cancer: from 2D to 3D model. Int J Mol Sci. 2021. https://doi.org/10.3390/ijms221810098.
Habanjar O, Diab-Assaf M, Caldefie-Chezet F, Delort L. 3D cell culture systems: tumor application, advantages, and disadvantages. Int J Mol Sci. 2021. https://doi.org/10.3390/ijms222212200.
Conrad C, Moore K, Polacheck W, Rizvi I, Scarcelli G. Mechanical modulation of ovarian cancer tumor nodules under flow. IEEE Trans Biomed Eng. 2022. https://doi.org/10.1109/TBME.2021.3092641.
Fuh KF, Shepherd RD, Withell JS, Kooistra BK, Rinker KD. Fluid Flow exposure promotes epithelial-to-mesenchymal transition and adhesion of breast cancer cells to endothelial cells. Breast Cancer Res. 2021. https://doi.org/10.1186/s13058-021-01473-0.
Pagnotti GM, Thompson WR, Guise TA, Rubin CT. suppression of cancer-associated bone loss through dynamic mechanical loading. Bone. 2021. https://doi.org/10.1016/j.bone.2021.115998.
Yang G, Guan W, Cao Z, Guo W, Xiong G, Zhao F, Feng, M, Qiu J, Liu Y, Zhang MQ, et al. Integrative genomic analysis of gemcitabine resistance in pancreatic cancer by patient-derived xenograft models. Clin Cancer Res. 2021. https://doi.org/10.1158/1078-0432.CCR-19-3975.
Boughey JC, Suman VJ, Yu J, Santo K, Sinnwell JP, Carter JM, Kalari KR, Tang X, McLaughlin SA, Moreno-Aspitia A, et al. Patient-derived xenograft engraftment and breast cancer outcomes in a prospective neoadjuvant study (BEAUTY). Clin Cancer Res. 2021. https://doi.org/10.1158/1078-0432.CCR-21-0641.
Gould SE, Junttila MR, de Sauvage FJ. Translational value of mouse models in oncology drug development. Nat Med. 2015. https://doi.org/10.1038/nm.3853.
Anderson NM, Simon MC. The tumor microenvironment. Curr Biol. 2020. https://doi.org/10.1016/j.cub.2020.06.081.
Imparato G, Urciuolo F, Netti PA. Organ on chip technology to model cancer growth and metastasis. Bioeng (Basel, Switzerland). 2022: doi: https://doi.org/10.3390/bioengineering9010028.
Del Piccolo N, Shirure VS, Bi Y, Goedegebuure SP, Gholami S, Hughes CCW, Fields RC, George SC. Tumor-on-chip modeling of organ-specific cancer and metastasis. Adv Drug Deliv Rev. 2021. https://doi.org/10.1016/j.addr.2021.05.008.
Sontheimer-Phelps A, Hassell BA, Ingber DE. Modeling cancer in microfluidic human organs-on-chips. Nat Rev Cancer. 2019. https://doi.org/10.1038/s41568-018-0104-6.
Portillo-Lara R, Annabi N. Microengineered cancer-on-a-chip platforms to study the metastatic microenvironment. Lab Chip. 2016. https://doi.org/10.1039/c6lc00718j.
Stewart BW. Mechanisms of carcinogenesis: from initiation and promotion to the hallmarks. In: Baan RA, Stewart BW, Straif K, editors. Tumour Site Concordance and Mechanisms of Carcinogenesis. Lyon: International Agency for Research on Cancer; 2019.
Lambert AW, Pattabiraman DR, Weinberg RA. Emerging biological principles of metastasis. Cell. 2017. https://doi.org/10.1016/j.cell.2016.11.037.
Eslami-S Z, Cortés-Hernández LE, Alix-Panabières C. The metastatic cascade as the basis for liquid biopsy development. Front Oncol. 2020. https://doi.org/10.3389/fonc.2020.01055.
Whiteside TL. The tumor microenvironment and its role in promoting tumor growth. Oncogene. 2008. https://doi.org/10.1038/onc.2008.271.
Li X, Yang Y, Huang Q, Deng Y, Guo F, Wang G, Liu M. Crosstalk between the tumor microenvironment and cancer cells: a promising predictive biomarker for immune checkpoint inhibitors. Front cell Dev Biol. 2021. https://doi.org/10.3389/fcell.2021.738373.
Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev. 2018. https://doi.org/10.1101/gad.314617.118.
Farc O, Cristea V. An overview of the tumor microenvironment, from cells to complex networks (Review). Exp Ther Med. 2021. https://doi.org/10.3892/etm.2020.9528.
Jackute J, Zemaitis M, Pranys D, Sitkauskiene B, Miliauskas S, Vaitkiene S, Sakalauskas R. Distribution of M1 and M2 macrophages in tumor islets and stroma in relation to prognosis of non-small cell lung cancer. BMC Immunol. 2018. https://doi.org/10.1186/s12865-018-0241-4.
Alvisi G, Termanini A, Soldani C, Portale F, Carriero R, Pilipow K, Costa G, Polidoro M, Franceschini B, Malenica I, et al. Multimodal single-cell profiling of intrahepatic cholangiocarcinoma defines hyperactivated tregs as a potential therapeutic target. J Hepatol. 2022. https://doi.org/10.1016/j.jhep.2022.05.043.
Lv Y, Lv D, Lv X, Xing P, Zhang J, Zhang Y. Immune cell infiltration-based characterization of triple-negative breast cancer predicts prognosis and chemotherapy response markers. Front Genet. 2021. https://doi.org/10.3389/fgene.2021.616469.
Pagès F, Mlecnik B, Marliot F, Bindea G, Ou F.-S, Bifulco C, Lugli A, Zlobec I, Rau TT, Berger MD, et al. International validation of the consensus immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet (London, England). 2018. https://doi.org/10.1016/S0140-6736(18)30789-X.
LeBleu VS, Kalluri R. A peek into cancer-associated fibroblasts: origins, functions and translational impact. Dis Model Mech. 2018. https://doi.org/10.1242/dmm.029447.
Cadamuro M, Morton SD, Strazzabosco M, Fabris L. Unveiling the role of tumor reactive stroma in cholangiocarcinoma: an opportunity for new therapeutic strategies. Transl Gastrointest Cancer. 2013. https://doi.org/10.3978/j.issn.2224-4778.2013.04.02.
Gascard P, Tlsty T.D. Carcinoma-associated fibroblasts: orchestrating the composition of malignancy. Genes Dev. 2016. https://doi.org/10.1101/gad.279737.116.
Kalluri R. The biology and function of fibroblasts in cancer. Nat Rev Cancer. 2016. https://doi.org/10.1038/nrc.2016.73.
Han Y, Zhang Y, Jia T, Sun Y. Molecular mechanism underlying the tumor-promoting functions of carcinoma-associated fibroblasts. Tumour Biol. 2015. https://doi.org/10.1007/s13277-015-3230-8.
Chen Y, Yu Z, Lv M, Cai Z, Zou Y, Lan P, Wu X, Gao F. Cancer-associated fibroblasts impact the clinical outcome and treatment response in colorectal cancer via immune system modulation: a comprehensive genome-wide analysis. Mol Med. 2021. https://doi.org/10.1186/s10020-021-00402-3.
Min KW, Kim DH, Noh YK, Son BK, Kwon MJ, Moon JY. Cancer-associated fibroblasts are associated with poor prognosis in solid type of lung adenocarcinoma in a machine learning analysis. Sci Rep. 2021. https://doi.org/10.1038/s41598-021-96344-1.
Raskov H, Orhan A, Gaggar S, Gögenur I. Cancer-associated fibroblasts and tumor-associated macrophages in cancer and cancer immunotherapy. Front Oncol. 2021. https://doi.org/10.3389/fonc.2021.668731.
Peng H, Xue R, Ju Z, Qiu J, Wang J, Ya W, Gan X, Tian Y, Shen H, Wang X, et al. Cancer-associated fibroblasts enhance the chemoresistance of CD73(+) hepatocellular carcinoma cancer cells via HGF-Met-ERK1/2 pathway. Ann Transl Med. 2020. https://doi.org/10.21037/atm-20-1038.
Yang D, Guo P, He T, Powell CA. Role of endothelial cells in tumor microenvironment. Clin Transl Med. 2021. https://doi.org/10.1002/ctm2.450.
Hida K, Maishi N, Annan DA, Hida Y. Contribution of tumor endothelial cells in cancer progression. Int J Mol Sci. 2018. https://doi.org/10.3390/ijms19051272.
Nagl L, Horvath L, Pircher A, Wolf D. Tumor Endothelial Cells (TECs) as potential immune directors of the tumor microenvironment - new findings and future perspectives. Front Cell Dev Biol. 2020. https://doi.org/10.3389/fcell.2020.00766.
Hida K, Maishi N, Takeda R, Hida Y. The Roles of Tumor Endothelial Cells in Cancer Metastasis. In: Sergi CM, editor. Metastasis. Brisbane: Exon Publications; 2022.
Henke E, Nandigama R, Ergün S. Extracellular matrix in the tumor microenvironment and its impact on cancer therapy. Front Mol Biosci. 2020. https://doi.org/10.3389/fmolb.2019.00160.
Jang I, Beningo KA. Integrins, CAFs and mechanical forces in the progression of cancer. Cancers (Basel). 2019. https://doi.org/10.3390/cancers11050721.
Huang J, Zhang L, Wan D, et al. Extracellular matrix and its therapeutic potential for cancer treatment. Signal Transduct Target Ther. 2021. https://doi.org/10.1038/s41392-021-00544-0.
Tao SC, Guo SC. Role of extracellular vesicles in tumour microenvironment. Cell Commun Signal. 2020. https://doi.org/10.1186/s12964-020-00643-5.
Cavallari C, Camussi G, Brizzi MF. Extracellular vesicles in the tumour microenvironment: eclectic supervisors. Int J Mol Sci. 2020. https://doi.org/10.3390/ijms21186768.
Corcoran C, Rani S, O’Brien K, et al. Docetaxel-resistance in prostate cancer: evaluating associated phenotypic changes and potential for resistance transfer via exosomes. PLoS ONE. 2012. https://doi.org/10.1371/journal.pone.0050999.
Zhang FF, Zhu YF, Zhao QN, et al. Microvesicles mediate transfer of P-glycoprotein to paclitaxel-sensitive A2780 human ovarian cancer cells, conferring paclitaxel-resistance. Eur J Pharmacol. 2014. https://doi.org/10.1016/j.ejphar.2014.05.026.
Roma-Rodrigues C, Mendes R, Baptista PV, Fernandes AR. Targeting tumor microenvironment for cancer therapy. Int J Mol Sci. 2019. https://doi.org/10.3390/ijms20040840.
Mastrangeli M, Millet S, Orchid Partners T, Van den Eijnden-van RJ. Organ-on-chip in development: towards a roadmap for organs-on-chip. Altex. 2019. https://doi.org/10.14573/altex.1908271.
Huh D, Hamilton GA, Ingber DE. From 3D cell culture to organs-on-chips. Trends Cell Biol. 2011. https://doi.org/10.1016/j.tcb.2011.09.005.
Ko J, Park D, Lee S, Gumuscu B, Jeon NL. Engineering organ-on-a-chip to accelerate translational research. Micromachines (Basel). 2022. https://doi.org/10.3390/mi13081200.
Bhatia SN, Ingber DE. Microfluidic organs-on-chips. Nat Biotechnol. 2014. https://doi.org/10.1038/nbt.2989.
Tovar-Lopez F, Thurgood P, Gilliam C, et al. A microfluidic system for studying the effects of disturbed flow on endothelial cells. Front Bioeng Biotechnol. 2019. https://doi.org/10.3389/fbioe.2019.00081.
Jang KJ, Cho HS, Kang DH, Bae WG, Kwon TH, Suh KY. Fluid-shear-stress-induced translocation of aquaporin-2 and reorganization of actin cytoskeleton in renal tubular epithelial cells. Integr Biol (Camb). 2011. https://doi.org/10.1039/c0ib00018c.
Buchanan CF, Verbridge SS, Vlachos PP, Rylander MN. Flow shear stress regulates endothelial barrier function and expression of angiogenic factors in a 3D microfluidic tumor vascular model. Cell Adh Migr. 2014. https://doi.org/10.4161/19336918.2014.970001.
Taïeb HM, Herment G, Robinson T, Cipitria A. Effect of capillary fluid flow on single cancer cell cycle dynamics, motility, volume and morphology. Lab Chip. 2022. https://doi.org/10.1039/d2lc00322h.
Calibasi Kocal G, Güven S, Foygel K, et al. Dynamic microenvironment induces phenotypic plasticity of esophageal cancer cells under flow. Sci Rep. 2016. https://doi.org/10.1038/srep38221.
Kaarj K, Yoon JY. Methods of delivering mechanical stimuli to organ-on-a-chip. Micromachines (Basel). 2019. https://doi.org/10.3390/mi10100700.
Mohammed M, Thurgood P, Gilliam C, et al. Studying the response of aortic endothelial cells under pulsatile flow using a compact microfluidic system. Anal Chem. 2019. https://doi.org/10.1021/acs.analchem.9b03247.
Chen H, Cornwell J, Zhang H, et al. Cardiac-like flow generator for long-term imaging of endothelial cell responses to circulatory pulsatile flow at microscale. Lab Chip. 2013. https://doi.org/10.1039/c3lc50123j.
Truskey GA, Achneck HE, Bursac N, et al. Design considerations for an integrated microphysiological muscle tissue for drug and tissue toxicity testing. Stem Cell Res Ther. 2013. https://doi.org/10.1186/scrt371.
Chu PY, Hsieh HY, Chung PS, et al. Development of vessel mimicking microfluidic device for studying mechano-response of endothelial cells. iScience. 2023. https://doi.org/10.1016/j.isci.2023.106927
Xiu MX, Liu ZT, Tang J. Screening and identification of key regulatory connections and immune cell infiltration characteristics for lung transplant rejection using mucosal biopsies. Int Immunopharmacol. 2020. https://doi.org/10.1016/j.intimp.2020.106827.
Haessler U, Teo JC, Foretay D, Renaud P, Swartz MA. Migration dynamics of breast cancer cells in a tunable 3D interstitial flow chamber. Integr Biol (Camb). 2012. https://doi.org/10.1039/c1ib00128k.
Shieh AC, Rozansky HA, Hinz B, Swartz MA. Tumor cell invasion is promoted by interstitial flow-induced matrix priming by stromal fibroblasts. Cancer Res. 2011. https://doi.org/10.1158/0008-5472.CAN-10-1513.
Park SH, Sim WY, Min BH, Yang SS, Khademhosseini A, Kaplan DL. Chip-based comparison of the osteogenesis of human bone marrow- and adipose tissue-derived mesenchymal stem cells under mechanical stimulation. PLoS ONE. 2012. https://doi.org/10.1371/journal.pone.0046689.
Kumar V, Madhurakkat Perikamana SK, Tata A, et al. An in vitro microfluidic alveolus model to study lung biomechanics. Front Bioeng Biotechnol. 2022. https://doi.org/10.3389/fbioe.2022.848699.
Wan L, Yin J, Skoko J, Schwartz R, Zhang M, LeDuc PR, Neumann CA. 3D collagen vascular tumor-on-a-chip mimetics for dynamic combinatorial drug screening. Mol Cancer Ther. 2021. https://doi.org/10.1158/1535-7163.MCT-20-0880.
Verbruggen SW, Thompson CL, Duffy MP, Lunetto S, Nolan J, Pearce OMT, Jacobs CR, Knight MM. Mechanical stimulation modulates osteocyte regulation of cancer cell phenotype. Cancers (Basel). 2021. https://doi.org/10.3390/cancers13122906.
Marhuenda E, Villarino A, Narciso M, Elowsson L, Almendros I, Westergren-Thorsson G, Farré R, Gavara N, Otero J. Development of a Physiomimetic model of acute respiratory distress syndrome by using ECM hydrogels and organ-on-a-chip devices. Front Pharmacol. 2022. https://doi.org/10.3389/fphar.2022.945134.
Ortiz-Cárdenas JE, Zatorski JM, Arneja A, Montalbine AN, Munson JM, Luckey CJ, Pompano RR. Towards spatially-organized organs-on-chip: photopatterning Cell-Laden Thiol-Ene and methacryloyl hydrogels in a microfluidic device. Organs-on-a-chip. 2022. https://doi.org/10.1016/j.ooc.2022.100018.
Bhusal A, Dogan E, Nieto D, Mousavi Shaegh SA, Cecen B, Miri AK. 3D Bioprinted hydrogel microfluidic devices for parallel drug screening. ACS Appl bio Mater. 2022. https://doi.org/10.1021/acsabm.2c00578.
Hospodiuk-Karwowski M, Chi K, Pritchard J, Catchmark JM. Vascularized pancreas-on-a-chip device produced using a printable simulated extracellular matrix. Biomed Mater. 2022. https://doi.org/10.1088/1748-605X/ac8c74.
Hiratsuka K, Miyoshi T, Kroll KT, Gupta NR, Valerius MT, Ferrante T, Yamashita M, Lewis JA, Morizane R. Organoid-on-a-chip model of human ARPKD reveals mechanosensing pathomechanisms for drug discovery. Sci Adv. 2022. https://doi.org/10.1126/sciadv.abq0866.
Heinrich MA, Mostafa AMRH, Morton JP, Hawinkels LJAC, Prakash J. Translating complexity and heterogeneity of pancreatic tumor: 3D in vitro to in vivo models. Adv Drug Deliv Rev. 2021. https://doi.org/10.1016/j.addr.2021.04.018.
de Jongh D, Massey EK, Bunnik EM. Organoids: a systematic review of ethical issues. Stem Cell Res Ther. 2022. https://doi.org/10.1186/s13287-022-02950-9.
Massidda M, Flore L, Kikuchi N, et al. Influence of the MCT1-T1470A polymorphism (rs1049434) on repeated sprint ability and blood lactate accumulation in elite football players: a pilot study. Eur J Appl Physiol. 2021. https://doi.org/10.1007/s00421-021-04797-z.
Meng Q, Wang Y, Li Y, Shen C. Hydrogel microfluidic-based liver-on-a-chip: mimicking the mass transfer and structural features of liver. Biotechnol Bioeng. 2021. https://doi.org/10.1002/bit.27589.
Huang D, Liu T, Liao J, et al. Reversed-engineered human alveolar lung-on-a-chip model. Proc Natl Acad Sci U S A. 2021. https://doi.org/10.1073/pnas.2016146118.
Terrell JA, Jones CG, Kabandana GKM, Chen C. From cells-on-a-chip to organs-on-a-chip: scaffolding materials for 3D cell culture in microfluidics. J Mater Chem B. 2020. https://doi.org/10.1039/d0tb00718h.
Chen C, Mehl BT, Sell SA, Martin RS. Use of electrospinning and dynamic air focusing to create three-dimensional cell culture scaffolds in microfluidic devices. Analyst. 2016. https://doi.org/10.1039/c6an01282e.
Park S, Kim TH, Kim SH, You S, Jung Y. Three-dimensional vascularized lung cancer-on-a-chip with lung extracellular matrix hydrogels for in vitro screening. Cancers (Basel). 2021. https://doi.org/10.3390/cancers13163930.
Si L, Bai H, Rodas M, Cao W, Oh CY, Jiang A, Moller R, Hoagland D, Oishi K, Horiuchi S, et al. A human-airway-on-a-chip for the rapid identification of candidate antiviral therapeutics and prophylactics. Nat Biomed Eng. 2021. https://doi.org/10.1038/s41551-021-00718-9.
Nie J, Gao Q, Wang Y, et al. Vessel-on-a-chip with hydrogel-based microfluidics. Small. 2018. https://doi.org/10.1002/smll.201802368.
Kim JA, Kim HN, Im SK, Chung S, Kang JY, Choi N. Collagen-based brain microvasculature model in vitro using three-dimensional printed template. Biomicrofluidics. 2015. https://doi.org/10.1063/1.4917508.
Yi HG, Lee H, Cho DW. 3D Printing of Organs-On-Chips. Bioeng (Basel, Switzerland). 2017. https://doi.org/10.3390/bioengineering4010010.
Miri AK, Mostafavi E, Khorsandi D, Hu SK, Malpica M, Khademhosseini A. Bioprinters for organs-on-chips. Biofabrication. 2019. https://doi.org/10.1088/1758-5090/ab2798.
Kolesky DB, Homan KA, Skylar-Scott MA, Lewis JA. Three-dimensional bioprinting of thick vascularized tissues. Proc Natl Acad Sci U S A. 2016. https://doi.org/10.1073/pnas.1521342113.
Torgersen J, Ovsianikov A, Mironov V, Pucher N, Qin X, Li Z, Cicha K, Machacek T, Liska R, Jantsch V, et al. Photo-sensitive hydrogels for three-dimensional laser microfabrication in the presence of whole organisms. J Biomed Opt. 2012. https://doi.org/10.1117/1.JBO.17.10.105008.
van der Helm MW, Odijk M, Frimat JP, van der Meer AD, Eijkel JCT, van den Berg A, Segerink LI. Fabrication and validation of an organ-on-chip system with integrated electrodes to directly quantify transendothelial electrical resistance. J Vis Exp. 2017. https://doi.org/10.3791/56334.
Kundu A, McCoy L, Azim N, Nguyen H, Didier CM, Ausaf T, Sharma AD, Curley JL, Moore MJ, Rajaraman S. Fabrication and characterization of 3D printed, 3D microelectrode arrays for interfacing with a peripheral nerve-on-a-chip. ACS Biomater Sci Eng. 2021. https://doi.org/10.1021/acsbiomaterials.0c01184.
Caluori G, Pribyl J, Pesl M, Jelinkova S, Rotrekl V, Skladal P, Raiteri R. Non-invasive electromechanical cell-based biosensors for improved investigation of 3D cardiac models. Biosens Bioelectron. 2019. https://doi.org/10.1016/j.bios.2018.10.021.
Dornhof J, Kieninger J, Muralidharan H, Maurer J, Urban GA, Weltin A. Microfluidic organ-on-chip system for multi-analyte monitoring of metabolites in 3D cell cultures. Lab Chip. 2022. https://doi.org/10.1039/d1lc00689d.
Baptista D, Moreira Teixeira L, Barata D, Tahmasebi Birgani Z, King J, van Riet S, Pasman T, Poot AA, Stamatialis D, Rottier RJ, et al. 3D lung-on-chip model based on biomimetically microcurved culture membranes. ACS Biomater Sci Eng. 2022. https://doi.org/10.1021/acsbiomaterials.1c01463.
Cao T, Shao C, Yu X, Xie R, Yang C, Sun Y, Yang S, He W, Xu Y, Fan Q, et al. Biomimetic Alveolus-on-a-Chip for SARS-CoV-2 Infection Recapitulation. Research (Washington, D.C.). 2022. https://doi.org/10.34133/2022/9819154.
Ya S, Ding W, Li S, Du K, Zhang Y, Li C, Liu J, Li F, Li P, Luo T, et al. On-Chip construction of liver lobules with self-assembled perfusable hepatic sinusoid networks. ACS Appl Mater Interfaces. 2021. https://doi.org/10.1021/acsami.1c00794.
Kulsharova G, Kurmangaliyeva A, Darbayeva E, Rojas-Solórzano L, Toxeitova G. Development of a hybrid polymer-based microfluidic platform for culturing hepatocytes towards liver-on-a-chip applications. Polymers (Basel). 2021. https://doi.org/10.3390/polym13193215.
Jeon MS, Choi YY, Mo SJ, Ha JH, Lee YS, Lee HU, Park SD, Shim JJ, Lee JL, Chung BG. Contributions of the microbiome to intestinal inflammation in a gut-on-a-chip. Nano Converg. 2022. https://doi.org/10.1186/s40580-022-00299-6.
Fois CAM, Schindeler A, Valtchev P, Dehghani F. Dynamic flow and shear stress as key parameters for intestinal cells morphology and polarization in an organ-on-a-chip model. Biomed Microdevices. 2021. https://doi.org/10.1007/s10544-021-00591-y.
Visone R, Occhetta P, Rasponi M. Electromechanical stimulation of 3D cardiac microtissues in a heart-on-chip model. Methods Mol Biol. 2022. https://doi.org/10.1007/978-1-0716-1693-2_9.
Tamargo MA, Nash TR, Fleischer S, Kim Y, Vila OF, Yeager K, Summers M, Zhao Y, Lock R, Chavez M, et al. MilliPillar: a platform for the generation and real-time assessment of human engineered cardiac tissues. ACS Biomater Sci Eng. 2021. https://doi.org/10.1021/acsbiomaterials.1c01006.
Varone A, Nguyen JK, Leng L, Barrile R, Sliz J, Lucchesi C, Wen N, Gravanis A, Hamilton GA, Karalis K, et al. A novel organ-chip system emulates three-dimensional architecture of the human epithelia and the mechanical forces acting on it. Biomaterials. 2021. https://doi.org/10.1016/j.biomaterials.2021.120957.
Zhang J, Chen Z, Zhang Y, Wang X, Ouyang J, Zhu J, Yan Y, Sun X, Wang F, Li X, et al. Construction of a high fidelity epidermis-on-a-chip for scalable in vitro irritation evaluation. Lab Chip. 2021. https://doi.org/10.1039/d1lc00099c.
Roye Y, Bhattacharya R, Mou X, Zhou Y, Burt MA, Musah S. A personalized glomerulus chip engineered from stem cell-derived epithelium and vascular endothelium. Micromachines. 2021. https://doi.org/10.3390/mi12080967.
Ortega MA, Fernández-Garibay X, Castaño AG, De Chiara F, Hernández-Albors A, Balaguer-Trias J, Ramón-Azcón J. Muscle-on-a-chip with an on-site multiplexed biosensing system for in situ monitoring of secreted IL-6 and TNF-α. Lab Chip. 2019. https://doi.org/10.1039/c9lc00285e.
Nagashima T, Hadiwidjaja S, Ohsumi S, Murata A, Hisada T, Kato R, Okada Y, Honda H, Shimizu K. In vitro model of human skeletal muscle tissues with contractility fabricated by immortalized human myogenic cells. Adv Biosyst. 2020. https://doi.org/10.1002/adbi.202000121.
Zakharova M, do Carmo MAP, van der Helm MW, Le-The H, de Graaf MNS, Orlova V, van den Berg A, van der Meer AD, Broersen K, Segerink LI. Multiplexed blood-brain barrier organ-on-chip. Lab Chip. 2020. https://doi.org/10.1039/d0lc00399a
Noorani B, Bhalerao A, Raut S, Nozohouri E, Bickel U, Cucullo L. A quasi-physiological microfluidic blood-brain barrier model for brain permeability studies. Pharmaceutics. 2021. https://doi.org/10.3390/pharmaceutics13091474.
Zhang M, Wang P, Luo R, Wang Y, Li Z, Guo Y, Yao Y, Li M, Tao T, Chen W, et al. Biomimetic human disease model of SARS-CoV-2-induced lung injury and immune responses on organ chip system. Adv Sci (Weinheim, Baden-Wurttemberg, Ger). 2021. https://doi.org/10.1002/advs.202002928.
Buzhdygan TP, DeOre BJ, Baldwin-Leclair A, Bullock TA, McGary HM, Khan JA, Razmpour R, Hale JF, Galie PA, Potula R, et al. The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood-brain barrier. Neurobiol Dis. 2020. https://doi.org/10.1016/j.nbd.2020.105131.
Nawroth JC, Lucchesi C, Cheng D, Shukla A, Ngyuen J, Shroff T, Varone A, Karalis K, Lee HH, Alves S, et al. A microengineered airway lung chip models key features of viral-induced exacerbation of asthma. Am J Respir Cell Mol Biol. 2020. https://doi.org/10.1165/rcmb.2020-0010MA.
Budhathoki S, Graham C, Sethu P, Kannappan R. Engineered aging cardiac tissue chip model for studying cardiovascular disease. Cells Tissues Organs. 2022. https://doi.org/10.1159/000516954.
Nemcovsky Amar D, Epshtein M, Korin N. Endothelial cell activation in an embolic ischemia-reperfusion injury microfluidic model. Micromachines. 2019. https://doi.org/10.3390/mi10120857.
Kong M, Lee J, Yazdi IK, Miri AK, Lin YD, Seo J, Zhang YS, Khademhosseini A, Shin SR. Cardiac fibrotic remodeling on a chip with dynamic mechanical stimulation. Adv Healthc Mater. 2019. https://doi.org/10.1002/adhm.201801146.
Mastikhina O, Moon BU, Williams K, Hatkar R, Gustafson D, Mourad O, Sun X, Koo M, Lam AYL, Sun Y, et al. Human cardiac fibrosis-on-a-chip model recapitulates disease hallmarks and can serve as a platform for drug testing. Biomaterials. 2020. https://doi.org/10.1016/j.biomaterials.2019.119741.
Beaurivage C, Kanapeckaite A, Loomans C, Erdmann KS, Stallen J, Janssen RAJ. Development of a human primary gut-on-a-chip to model inflammatory processes. Sci Rep. 2020. https://doi.org/10.1038/s41598-020-78359-2.
Wang Y, Wang H, Deng P, Tao T, Liu H, Wu S, Chen W, Qin J. Modeling Human Nonalcoholic Fatty Liver Disease (NAFLD) with an organoids-on-a-chip system. ACS Biomater Sci Eng. 2020. https://doi.org/10.1021/acsbiomaterials.0c00682.
Kostrzewski T, Cornforth T, Snow SA, Ouro-Gnao L, Rowe C, Large EM, Hughes DJ. Three-dimensional perfused human in vitro model of non-alcoholic fatty liver disease. World J Gastroenterol. 2017. https://doi.org/10.3748/wjg.v23.i2.204.
Tanataweethum N, Trang A, Lee C, Mehta J, Patel N, Cohen RN, Bhushan A. Investigation of insulin resistance through a multiorgan microfluidic organ-on-chip. Biomed Mater. 2022. https://doi.org/10.1088/1748-605X/ac4611.
Bauer S, Wennberg Huldt C, Kanebratt KP, Durieux I, Gunne D, Andersson S, Ewart L, Haynes WG, Maschmeyer I, Winter A, et al. Functional coupling of human pancreatic islets and liver spheroids on-a-chip: towards a novel human ex vivo type 2 diabetes model. Sci Rep. 2017. https://doi.org/10.1038/s41598-017-14815-w.
Shin Y, Choi SH, Kim E, Bylykbashi E, Kim JA, Chung S, Kim DY, Kamm RD, Tanzi RE. Blood-brain barrier dysfunction in a 3D in vitro model of alzheimer’s disease. Adv Sci (Weinheim, Baden-Wurttemberg, Ger.) 2019. https://doi.org/10.1002/advs.201900962.
Russo A, Yang Z, Heyrman GM, Cain BP, Lopez Carrero A, Isenberg BC, Dean MJ, Coppeta J, Burdette JE. Versican secreted by the ovary links ovulation and migration in fallopian tube derived serous cancer. Cancer Lett. 2022. https://doi.org/10.1016/j.canlet.2022.215779.
Jeibouei S, Hojat A, Mostafavi E, Aref AR, Kalbasi A, Niazi V, Ajoudanian M, Mohammadi F, Saadati F, Javadi SM, et al. Radiobiological effects of wound fluid on breast cancer cell lines and human-derived tumor spheroids in 2D and microfluidic culture. Sci Rep. 2022. https://doi.org/10.1038/s41598-022-11023-z.
Rima XY, Zhang J, Nguyen LTH, Rajasuriyar A, Yoon MJ, Chiang CL, Walters N, Kwak KJ, Lee LJ, Reátegui E. Microfluidic harvesting of breast cancer tumor spheroid-derived extracellular vesicles from immobilized microgels for single-vesicle analysis. Lab Chip. 2022. https://doi.org/10.1039/d1lc01053k.
Li C, Li S, Du K, Li P, Qiu B, Ding W. On-chip replication of extremely early-stage tumor behavior. ACS Appl Mater Interfaces. 2021. https://doi.org/10.1021/acsami.1c03740.
Ko J, Ahn J, Kim S, Lee Y, Lee J, Park D, Jeon NL. Tumor spheroid-on-a-chip: a standardized microfluidic culture platform for investigating tumor angiogenesis. Lab Chip. 2019. https://doi.org/10.1039/c9lc00140a.
Gwak H, Park S, Kim J, Lee JD, Kim IS, Kim SI, Hyun KA, Jung HI. Microfluidic chip for rapid and selective isolation of tumor-derived extracellular vesicles for early diagnosis and metastatic risk evaluation of breast cancer. Biosens Bioelectron. 2021. https://doi.org/10.1016/j.bios.2021.113495.
Mani V, Lyu Z, Kumar V, Ercal B, Chen H, Malhotra SV, Demirci U. Epithelial-to-Mesenchymal Transition (EMT) and drug response in dynamic bioengineered lung cancer microenvironment. Adv Biosyst. 2019. https://doi.org/10.1002/adbi.201800223.
Li E, Xu Z, Liu F, Wang H, Wen J, Shao S, Zhang L, Wang L, Liu C, Lu J, et al. Continual exposure to cigarette smoke extracts induces tumor-like transformation of human nontumor bronchial epithelial cells in a microfluidic chip. J Thorac Oncol. 2014. https://doi.org/10.1097/JTO.0000000000000219.
Jin X, Luan H, Chai H, Yan L, Zhang J, Wang Q, Cao L. Netrin-1 interference potentiates epithelial-to-mesenchymal transition through the PI3K/AKT pathway under the hypoxic microenvironment conditions of non-small cell lung cancer. Int J Oncol. 2019. https://doi.org/10.3892/ijo.2019.4716.
Aleman J, Skardal A. A multi-site metastasis-on-a-chip microphysiological system for assessing metastatic preference of cancer cells. Biotechnol Bioeng. 2019. https://doi.org/10.1002/bit.26871.
Xu Z, Li E, Guo Z, Yu R, Hao H, Xu Y, Sun Z, Li X, Lyu J, Wang Q. Design and construction of a multi-organ microfluidic chip mimicking the in vivo microenvironment of lung cancer metastasis. ACS Appl Mater Interfaces. 2016. https://doi.org/10.1021/acsami.6b08746.
Liu Q, Zhang H, Jiang X, Qian C, Liu Z, Luo D. Factors involved in cancer metastasis: a better understanding to “seed and soil” hypothesis. Mol Cancer. 2017. https://doi.org/10.1186/s12943-017-0742-4.
Gao Y, Bado I, Wang H, Zhang W, Rosen JM, Zhang XH. Metastasis organotropism: redefining the congenial soil. Dev Cell. 2019. https://doi.org/10.1016/j.devcel.2019.04.012.
Ferlay J, Colombet M, Soerjomataram I, et al. Cancer statistics for the year 2020: an overview [published online ahead of print, 2021 Apr 5]. Int J Cancer. 2021. https://doi.org/10.1002/ijc.33588
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021. https://doi.org/10.3322/caac.21660
Lei S, Zheng R, Zhang S, Wang S, Chen R, Sun K, Zeng H, Zhou J, Wei W. Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020. Cancer Commun (London, England). 2021. https://doi.org/10.1002/cac2.12207.
Park M, Kim D, Ko S, Kim A, Mo K, Yoon H. Breast cancer metastasis: mechanisms and therapeutic implications. Int J Mol Sci. 2022. https://doi.org/10.3390/ijms23126806.
Lanz HL, Saleh A, Kramer B, Cairns J, Ng CP, Yu J, Trietsch SJ, Hankemeier T, Joore J, Vulto P, et al. Therapy response testing of breast cancer in a 3D high-throughput perfused microfluidic platform. BMC Cancer. 2017. https://doi.org/10.1186/s12885-017-3709-3.
Lam SF, Bishop KW, Mintz R, Fang L, Achilefu S. Calcium carbonate nanoparticles stimulate cancer cell reprogramming to suppress tumor growth and invasion in an organ-on-a-chip system. Sci Rep. 2021. https://doi.org/10.1038/s41598-021-88687-6.
Firatligil-Yildirir B, Bati-Ayaz G, Tahmaz I, Bilgen M, Pesen-Okvur D, Yalcin-Ozuysal O. On-chip determination of tissue-specific metastatic potential of breast cancer cells. Biotechnol Bioeng. 2021. https://doi.org/10.1002/bit.27855.
Hao S, Ha L, Cheng G, Wan Y, Xia Y, Sosnoski DM, Mastro AM, Zheng SY. A spontaneous 3D bone-on-a-chip for bone metastasis study of breast cancer cells. Small. 2018. https://doi.org/10.1002/smll.201702787.
Kwak TJ, Lee E. Rapid multilayer microfabrication for modeling organotropic metastasis in breast cancer. Biofabrication. 2020. https://doi.org/10.1088/1758-5090/abbd28.
Conceição F, Sousa DM, Loessberg-Zahl J, Vollertsen AR, Neto E, Søe K, Paredes J, Leferink A, Lamghari M. A metastasis-on-a-chip approach to explore the sympathetic modulation of breast cancer bone metastasis. Mater today Bio. 2022. https://doi.org/10.1016/j.mtbio.2022.100219.
Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet (London, England). 2021. https://doi.org/10.1016/S0140-6736(21)00312-3.
Ruzycka M, Cimpan MR, Rios-Mondragon I, Grudzinski IP. Microfluidics for studying metastatic patterns of lung cancer. J Nanobiotechnology. 2019. https://doi.org/10.1186/s12951-019-0492-0.
Hassell BA, Goyal G, Lee E, Sontheimer-Phelps A, Levy O, Chen CS, Ingber DE. Human organ chip models recapitulate orthotopic lung cancer growth, therapeutic responses, and tumor dormancy in vitro. Cell Rep. 2017. https://doi.org/10.1016/j.celrep.2017.09.043.
Yang X, Li K, Zhang X, Liu C, Guo B, Wen W, Gao X. Nanofiber membrane supported lung-on-a-chip microdevice for anti-cancer drug testing. Lab Chip. 2018. https://doi.org/10.1039/c7lc01224a.
Lee SW, Kwak HS, Kang MH, Park YY, Jeong GS. Fibroblast-associated tumour microenvironment induces vascular structure-networked tumouroid. Sci Rep. 2018. https://doi.org/10.1038/s41598-018-20886-0.
Kim H, Sa JK, Kim J, Cho HJ, Oh HJ, Choi DH, Kang SH, Jeong DE, Nam DH, Lee H, et al. Recapitulated crosstalk between cerebral metastatic lung cancer cells and brain perivascular tumor microenvironment in a microfluidic co-culture chip. Adv Sci (Weinheim, Baden-Wurttemberg, Ger.). 2022. https://doi.org/10.1002/advs.202201785.
Rawla P, Sunkara T, Gaduputi V. Epidemiology of pancreatic cancer: global trends, etiology and risk factors. World J Oncol. 2019. https://doi.org/10.14740/wjon1166.
Liffers ST, Godfrey L, Frohn L, Haeberle L, Yavas A, Vesce R, Goering W, Opitz FV, Stoecklein N, Knoefel WT, et al. Molecular heterogeneity and commonalities in pancreatic cancer precursors with gastric and intestinal phenotype. Gut. 2022. https://doi.org/10.1136/gutjnl-2021-326550.
Group Young Researchers In Inflammatory Carcinogenesis, et al. The heterogeneity of the tumor microenvironment as essential determinant of development, progression and therapy response of pancreatic cancer. Cancers. 2021. https://doi.org/10.3390/cancers13194932
Shik Mun K, Arora K, Huang Y, Yang F, Yarlagadda S, Ramananda Y, Abu-El-Haija M, Palermo JJ, Appakalai BN, Nathan JD, et al. Patient-derived pancreas-on-a-chip to model cystic fibrosis-related disorders. Nat Commun. 2019. https://doi.org/10.1038/s41467-019-11178-w.
Beer M, Kuppalu N, Stefanini M, Becker H, Schulz I, Manoli S, Schuette J, Schmees C, Casazza A, Stelzle M, et al. A novel microfluidic 3D platform for culturing pancreatic ductal adenocarcinoma cells: comparison with in vitro cultures and in vivo xenografts. Sci Rep. 2017. https://doi.org/10.1038/s41598-017-01256-8.
Lai Benjamin FL, Lu Rick X, Hu Y, Davenport HL, Dou W, Wang EY, Radulovich N, Tsao MS, Sun Y, Radisic M. Recapitulating pancreatic tumor microenvironment through synergistic use of patient organoids and organ-on-a-chip vasculature. Adv Funct Mater. 2020. https://doi.org/10.1002/adfm.202000545.
Nguyen DHT, Lee E, Alimperti S, Norgard RJ, Wong A, Lee JJK, Eyckmans J, Stanger BZ, Chen CS. A biomimetic pancreatic cancer on-chip reveals endothelial ablation via ALK7 signaling. Sci Adv. 2019. https://doi.org/10.1126/sciadv.aav6789.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015. https://doi.org/10.3322/caac.21254.
Korc M. Pathways for aberrant angiogenesis in pancreatic cancer. Mol Cancer. 2003. https://doi.org/10.1186/1476-4598-2-8.
Olive KP, Jacobetz MA, Davidson CJ, Gopinathan A, McIntyre D, Honess D, Madhu B, Goldgraben MA, Caldwell ME, Allard D, et al. Inhibition of hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science. 2009. https://doi.org/10.1126/science.1171362.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018. https://doi.org/10.3322/caac.21492.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet (London, England). 2019. https://doi.org/10.1016/S0140-6736(19)32319-0.
Simon K. Colorectal cancer development and advances in screening. Clin Interv Aging. 2016. https://doi.org/10.2147/CIA.S109285.
Misiakos EP, Karidis NP, Kouraklis G. Current treatment for colorectal liver metastases. World J Gastroenterol. 2011. https://doi.org/10.3748/wjg.v17.i36.4067.
Chow FCL, Chok KSH. Colorectal liver metastases: an update on multidisciplinary approach. World J Hepatol. 2019. https://doi.org/10.4254/wjh.v11.i2.150.
Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020. https://doi.org/10.3322/caac.21601.
Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 2019. https://doi.org/10.5114/pg.2018.81072.
Hachey SJ, Movsesyan S, Nguyen QH, Burton-Sojo G, Tankazyan A, Wu J, Hoang T, Zhao D, Wang S, Hatch MM, et al. An: in vitro vascularized micro-tumor model of human colorectal cancer recapitulates in vivo responses to standard-of-care therapy. Lab Chip. 2021. https://doi.org/10.1039/d0lc01216e.
Carvalho MR, Barata D, Teixeira LM, Giselbrecht S, Reis RL, Oliveira JM, Truckenmüller R, Habibovic P. Colorectal tumor-on-a-chip system: a 3D tool for precision onco-nanomedicine. Sci Adv. 2019. https://doi.org/10.1126/sciadv.aaw1317.
Strelez C, Chilakala S, Ghaffarian K, Lau R, Spiller E, Ung N, Hixon D, Yoon AY, Sun RX, Lenz HJ, et al. Human colorectal cancer-on-chip model to study the microenvironmental influence on early metastatic spread. iScience. 2021. https://doi.org/10.1016/j.isci.2021.102509.
Shirure VS, Bi Y, Curtis MB, Lezia A, Goedegebuure MM, Goedegebuure SP, Aft R, Fields RC, George SC. Tumor-on-a-chip platform to investigate progression and drug sensitivity in cell lines and patient-derived organoids. Lab Chip. 2018. https://doi.org/10.1039/c8lc00596f.
Lu W, Fu D, Kong X, Huang Z, Hwang M, Zhu Y, Chen L, Jiang K, Li X, Wu Y, et al. FOLFOX treatment response prediction in metastatic or recurrent colorectal cancer patients via machine learning algorithms. Cancer Med. 2020. https://doi.org/10.1002/cam4.2786.
Jeong SY, Lee JH, Shin Y, Chung S, Kuh HJ. Co-culture of tumor spheroids and fibroblasts in a collagen matrix-incorporated microfluidic chip mimics reciprocal activation in solid tumor microenvironment. PLoS One. 2016. https://doi.org/10.1371/journal.pone.0159013.
Dasgupta P, Henshaw C, Youlden DR, Clark PJ, Aitken JF, Baade PD. Global trends in incidence rates of primary adult liver cancers: a systematic review and meta-analysis. Front Oncol. 2020. https://doi.org/10.3389/fonc.2020.00171.
Komuta M. Histological heterogeneity of primary liver cancers: clinical relevance, diagnostic pitfalls and the pathologist’s role. Cancers (Basel). 2021. https://doi.org/10.3390/cancers13122871.
Feng M, Pan Y, Kong R, Shu S. Therapy of primary liver cancer. Innov (Cambridge). 2020. https://doi.org/10.1016/j.xinn.2020.100032.
Lu S, Cuzzucoli F, Jiang J, Liang LG, Wang Y, Kong M, Zhao X, Cui W, Li J, Wang S. Development of a diomimetic liver tumor-on-a-chip model based on decellularized liver matrix for toxicity testing. Lab Chip. 2018. https://doi.org/10.1039/C8LC00852C.
Sun W, Chen YQ, Wang MF, Wang YR, Zhang M, Zhang HY, Hu P. Study on drug resistance to tumor cell in oxygen gradient and co-culture microfluidic chip. Chinese J Anal Chem. 2020. https://doi.org/10.1016/S1872-2040(19)61214-4.
Hung LY, Chiang NJ, Tsai WC, Fu CY, Wang YC, Shan YS, Lee GB. A microfluidic chip for detecting cholangiocarcinoma cells in human bile. Sci Rep. 2017. https://doi.org/10.1038/s41598-017-04056-2.
Nahak BK, Mishra A, Preetam S, Tiwari A. Advances in organ-on-a-chip materials and devices. ACS Appl bio Mater. 2022. https://doi.org/10.1021/acsabm.2c00041.
Joseph X, Akhil V, Arathi A, Mohanan PV. Comprehensive development in organ-on-a-chip technology. J Pharm Sci. 2022. https://doi.org/10.1016/j.xphs.2021.07.014.
Collins T, Pyne E, Christensen M, Iles A, Pamme N, Pires IM. Spheroid-on-chip microfluidic technology for the evaluation of the impact of continuous flow on metastatic potential in cancer models in vitro. Biomicrofluidics. 2021. https://doi.org/10.1063/5.0061373.
Lopez-Muñoz GA, Mugal S, Ramón-Azcón J. Sensors and biosensors in organs-on-a-chip platforms. Adv Exp Med Biol. 2022. https://doi.org/10.1007/978-3-031-04039-9_3.
Kim J, Cho H, Kim J, Park JS, Han KH. A disposable smart microfluidic platform integrated with on-chip flow sensors. Biosens Bioelectron. 2021. https://doi.org/10.1016/j.bios.2020.112897.
Zhao X, Gao W, Yin J, Fan W, Wang Z, Hu K, Mai Y, Luan A, Xu B, Jin Q. A high-precision thermometry microfluidic chip for real-time monitoring of the physiological process of live tumour cells. Talanta. 2021. https://doi.org/10.1016/j.talanta.2021.122101.
Meghani N, Kim KH, Kim SH, Lee SH, Choi KH. Evaluation and live monitoring of PH-responsive HSA-ZnO nanoparticles using a lung-on-a-chip model. Arch Pharm Res. 2020. https://doi.org/10.1007/s12272-020-01236-z.
Nguyen TA, Yin TI, Reyes D, Urban GA. Microfluidic chip with integrated electrical cell-impedance sensing for monitoring single cancer cell migration in three-dimensional matrixes. Anal Chem. 2013. https://doi.org/10.1021/ac402761s.
Nikshoar MS, Khosravi S, Jahangiri M, Zandi A, Miripour ZS, Bonakdar S, Abdolahad M. Distinguishment of populated metastatic cancer cells from primary ones based on their invasion to endothelial barrier by biosensor arrays fabricated on nanoroughened poly(Methyl Methacrylate). Biosens Bioelectron. 2018. https://doi.org/10.1016/j.bios.2018.07.036.
Yanase Y, Yoshizaki K, Kimura K, Kawaguchi T, Hide M, Uno S. Development of SPR imaging-impedance sensor for multi-parametric living cell analysis. Sensors (Basel). 2019. https://doi.org/10.3390/s19092067.
Bassi G, Grimaudo MA, Panseri S, Montesi M. Advanced multi-dimensional cellular models as emerging reality to reproduce in vitro the human body complexity. Int J Mol Sci. 2021. https://doi.org/10.3390/ijms22031195.
Shakeri A, Khan S, Didar TF. Conventional and emerging strategies for the fabrication and functionalization of pdms-based microfluidic devices. Lab Chip. 2021. https://doi.org/10.1039/d1lc00288k.
Mair DB, Williams MAC, Chen JF, et al. PDMS-PEG block copolymer and pretreatment for arresting drug absorption in microphysiological devices. ACS Appl Mater Interfaces. 2022. https://doi.org/10.1021/acsami.2c10669.
Yao J, Guan Y, Park Y, Choi YE, Kim HS, Park J. Optimization of PTFE coating on PDMS surfaces for inhibition of hydrophobic molecule absorption for increased optical detection sensitivity. Sensors (Basel). 2021. https://doi.org/10.3390/s21051754.
Esch MB, Prot JM, Wang YI, et al. Multi-cellular 3D human primary liver cell culture elevates metabolic activity under fluidic flow. Lab Chip. 2015. https://doi.org/10.1039/c5lc00237k.
Sønstevold L, Czerkies M, Escobedo-Cousin E, Blonski S, Vereshchagina E. Application of polymethylpentene, an oxygen permeable thermoplastic, for long-term on-a-chip cell culture and organ-on-a-chip devices. Micromachines (Basel). 2023. https://doi.org/10.3390/mi14030532.
Gencturk E, Mutlu S, Ulgen KO. Advances in microfluidic devices made from thermoplastics used in cell biology and analyses. Biomicrofluidics. 2017. https://doi.org/10.1063/1.4998604.
Domansky K, Inman W, Serdy J, Dash A, Lim MH, Griffith LG. Perfused multiwell plate for 3D liver tissue engineering. Lab Chip. 2010. https://doi.org/10.1039/b913221j.
Cao UMN, Zhang Y, Chen J, Sayson D, Pillai S, Tran SD. Microfluidic organ-on-a-chip: a guide to biomaterial choice and fabrication. Int J Mol Sci. 2023. https://doi.org/10.3390/ijms24043232.
Leung CM, de Haan P, Ronaldson-Bouchard K et al. A guide to the organ-on-a-chip. Nat Rev Methods Primers 2. 2022. https://doi.org/10.1038/s43586-022-00118-6
Pereiro I, Fomitcheva Khartchenko A, Petrini L, Kaigala GV. Nip the bubble in the bud: a guide to avoid gas nucleation in microfluidics. Lab Chip. 2019. https://doi.org/10.1039/c9lc00211a.
He X, Wang B, Meng J, Zhang S, Wang S. How to prevent bubbles in microfluidic channels. Langmuir. 2021. https://doi.org/10.1021/acs.langmuir.0c03514.
Zhao X, Ma C, Park DS, Soper SA, Murphy MC. Air bubble removal: Wettability contrast enabled microfluidic interconnects. Sens Actuators B Chem. 2022. https://doi.org/10.1016/j.snb.2022.131687.
Piergiovanni M, Leite SB, Corvi R, Whelan M. Standardisation needs for organ on chip devices. Lab Chip. 2021. https://doi.org/10.1039/d1lc00241d.
Caballero D, Reis RL, Kundu SC. Engineering patient-on-a-chip models for personalized cancer medicine. Adv Exp Med Biol. 2020. https://doi.org/10.1007/978-3-030-36588-2_4.
Regmi S, Poudel C, Adhikari R, Luo KQ. Applications of microfluidics and organ-on-a-chip in cancer research. Biosensors (Basel). 2022. https://doi.org/10.3390/bios12070459.
Zhu D, Kong CSL, Gingold JA, Zhao R, Lee DF. Induced pluripotent stem cells and induced pluripotent cancer cells in cancer disease modeling. Adv Exp Med Biol. 2018. https://doi.org/10.1007/5584_2018_257.
Liu Y, Yang Q, Zhang H, et al. Construction of cancer-on-a-chip for drug screening. Drug Discov Today. 2021. https://doi.org/10.1016/j.drudis.2021.03.006.
Skardal A, Shupe T, Atala A. Organoid-on-a-chip and body-on-a-chip systems for drug screening and disease modeling. Drug Discov Today. 2016. https://doi.org/10.1016/j.drudis.2016.07.003.
Kim Y, Ko J, Shin N, Park S, Lee SR, Kim S, Song J, Lee S, Kang KS, Lee J, et al. All-in-one microfluidic design to integrate vascularized tumor spheroid into high-throughput platform. Biotechnol Bioeng. 2022. https://doi.org/10.1002/bit.28221.
Koch EV, Ledwig V, Bendas S, Reichl S, Dietzel A. Tissue barrier-on-chip: a technology for reproducible practice in drug testing. Pharmaceutics. 2022. https://doi.org/10.3390/pharmaceutics14071451.
Vivas A, van den Berg A, Passier R, Odijk M, van der Meer AD. Fluidic circuit board with modular sensor and valves enables stand-alone, tubeless microfluidic flow control in organs-on-chips. Lab Chip. 2022. https://doi.org/10.1039/d1lc00999k.
Kann SH, Shaughnessey EM, Coppeta JR, Azizgolshani H, Isenberg BC, Vedula EM, Zhang X, Charest JL. Measurement of oxygen consumption rates of human renal proximal tubule cells in an array of organ-on-chip devices to monitor drug-induced metabolic shifts. Microsystems Nanoeng. 2022. https://doi.org/10.1038/s41378-022-00442-7.
Acknowledgements
This work was supported by the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement n° 860715.
Funding
The present work was founded by the Associazione Italiana per la Ricerca sul Cancro (IG AIRC 2019 – ID 23408 to A.L.) and by the Italian Ministry of Health (Ricerca Finalizzata 2016 GR-2016–02364990 to S.M.).
Author information
Authors and Affiliations
Contributions
Both E.C. and M.A.P. researched and compiled the data from the literature and drafted the first draft of the manuscript. S.M., C.B., M.R., and A.L. revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cauli, E., Polidoro, M.A., Marzorati, S. et al. Cancer-on-chip: a 3D model for the study of the tumor microenvironment. J Biol Eng 17, 53 (2023). https://doi.org/10.1186/s13036-023-00372-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13036-023-00372-6