
Abstract
Background
Previous studies achieved low microbial detection rates in lymphoma patients with interstitial pneumonia (IP) after chemotherapy. However, the metagenomic next-generation sequencing (mNGS) is a comprehensive approach that is expected to improve the pathogen identification rate. Thus far, reports on the use of mNGS in lymphoma patients with chemotherapy-related IP remain scarce. In this study, we summarized the microbial detection outcomes of lymphoma patients with chemotherapy-related IP through mNGS testing of bronchoalveolar lavage fluid (BALF).
Methods
Fifteen lymphoma patients with chemotherapy-related IP were tested for traditional laboratory microbiology, along with the mNGS of BALF. Then, the results of mNGS and traditional laboratory microbiology were compared.
Results
Of the 15 enrolled patients, 11 received rituximab and 8 were administered doxorubicin hydrochloride liposome. The overall microbial yield was 93.3% (14/15) for mNGS versus 13.3% (2/15) for traditional culture methods (P ≤ 0.05). The most frequently detected pathogens were Pneumocystis jirovecii (12/15, 80%), Cytomegalovirus (4/15, 26.7%), and Epstein-Barr virus (3/15, 20%). Mixed infections were detected in 10 cases. Five patients recovered after the treatment with antibiotics alone without glucocorticoids.
Conclusion
Our findings obtained through mNGS testing of BALF suggested a high microbial detection rate in lymphoma patients with IP after chemotherapy. Notably, there was an especially high detection rate of Pneumocystis jirovecii. The application of mNGS in patients with chemotherapy-related IP was more sensitive.
Similar content being viewed by others

Introduction
Interstitial pneumonia (IP) is a severe adverse effect of chemotherapy in lymphoma patients. It may result in fever, dyspnea, respiratory failure, and death [1]. Additionally, patients who experience IP have more treatment delays and more frequent premature termination of chemotherapy [2]. According to the relevant research, the probability of IP after lymphoma chemotherapy is about 2-30%, and the incidence of IP in patients treated with rituximab-based chemotherapy is significantly higher than those treated with rituximab-free regimens [2,3,4,5]. The pathogenesis of chemotherapy-related IP is still unclear. At present, it is considered that the mechanism mainly involves drug allergic reactions and direct drug toxicity that damage endothelial cell membranes, causing diffuse alveolar damage and progressive pulmonary fibrosis [6,7,8]. However, some researchers have suggested that the occurrence of IP may be due to the increase of opportunistic infections after chemotherapy (especially rituximab-based regimens), as shown by the elevated serum beta-D-glucan (BDG) levels and the detection of certain pathogens (etiological tests are more common for Pneumocystis jirovecii (P. jirovecii) or fungi) [9, 10]. Many studies have reported that lymphoma patients treated with rituximab regimen are often infected with P. jirovecii [11,12,13]. Furthermore, preventing P. jirovecii is effective against P. jirovecii infection [14]. However, the pathogen detection rate of chemotherapy-related IP is low when traditional laboratory testing methods are used. Weiping Liu [2] retrospectively analyzed 83 lymphoma patients with IP after chemotherapy. Using traditional laboratory methods, only 6 cases were found to have evidence of pathogenic infection. However, physicians prescribed antibiotics to 53% of those patients with no proof of infection.
Despite less data on chemotherapy-related IP, the role of infection has been well-studied in other types of interstitial lung diseases. Research efforts thus far have shown that viruses are most associated with interstitial lung diseases. The most frequently identified virus appears to be Epstein-Barr virus (EBV), and other viruses including Cytomegalovirus (CMV), and hepatitis C virus [15]. Virus detection mainly relies on polymerase chain reaction (PCR) methods and antibody detection [15]. Bacteria have been less well studied in the area of IP. Richter et al [16] demonstrated positive bronchoalveolar lavage fluid(BALF) cultures for pathogens such as Streptococcus species, Haemophilus species and Pseudomonas species in eight of 22 stable patients with idiopathic pulmonary fibrosis. However, it is uncertain whether the IP caused by bacterial infection or the bacterial infection is secondary to IP. Other bacteria detected in BALF of idiopathic pulmonary fibrosis patients including Neisseria, and Veillonella [17]. Fungus including P. jirovecii and Aspergillus were detected as factors associated with IP [18,19,20]. P. jirovecii was usually identified by quantitative real-time PCR or toluidine blue ‘O’ staining on respiratory specimen [21]. Culture and histological-based methods remain central to the diagnosis of Aspergillus [22].
Metagenomic next-generation sequencing (mNGS) is a recently developed detection method that is independent of pathogen culture, which can help to provide rapid and objective pathogenic diagnosis. This technology can simultaneously detect known or unknown bacteria, fungi and viruses, and has been proven to significantly improve the pathogen detection rate in systemic infections, artificial joint infections, pleural infections and respiratory infections [23,24,25,26]. At present, many studies have confirmed that the analysis of BALF through mNGS can further improve the positive diagnosis rate of pneumonia patients compared with traditional microbiological detection methods [27, 28]. Moreover, mNGS has proven especially suitable for infected patients with negative traditional test results, immunodeficiency patients or critically ill infected patients [29,30,31]. Therefore, we believe that the application of mNGS to analyze the BALF of patients with IP after chemotherapy is a highly efficient method for the detection of respiratory pathogens.
Materials and methods
Ethics statement
The study protocol was approved by the Ethical Review Committee of Ningbo Medical Treatment Center Li Huili Hospital (approval number: KY2022PJ155). Informed consent to publish the information was obtained from the personal patient.
Case description
All lymphoma patients who were treated in Ningbo Medical Treatment Centre Li Huili Hospital between January 2016 to February 2022 were retrospectively reviewed. The included study participants were a consecutive series of all patients satisfying the inclusion criteria. The patient eligibility criteria were as follows: (I) ≥ 18 years of age; (II) had a histological diagnosis of lymphoma; (III) received at least one course of chemotherapy; (IV) developed IP after chemotherapy; (V)underwent bronchoscopy and mNGS test of BALF was performed when developed IP. Patients were excluded if they (I)had no BALF culture result; (II) had simultaneous infections of other parts other than the lung, such as blood infection and intestinal infection; (III) had previously received prophylactic anti-Pneumocystis treatment with trimethoprim-sulfamethoxazole (TMP-SMX); (IV) had incomplete documentation. IP was diagnosed based on radiologic findings, clinical symptoms, physical examination, laboratory tests, lung function, arterial gas analysis, bronchoalveolar lavage and pathologic results [32, 33]. Arterial gas analysis during the stable phase can show normal results or hypoxemia and respiratory alkalosis [34]. The necessary radiological findings of IP were diffuse pulmonary interstitial infiltration and other manifestations, including traction bronchiectasis, bilateral reticular opacities, loss of lobe volume, and opacity in the lower lungs on computed tomography (CT) scans [32, 33, 35]. The process of this study is shown in Fig. 1.

The process of this study
BALF collection
The collection of BALF was performed by experienced bronchoscopists according to standard procedures [36]: Prior to the examination, informed consent was obtained, and blood tests, coagulation function, electrocardiogram, and chest CT were used to evaluate the condition. Bronchoalveolar lavage was performed with the fiberoptic bronchoscope in a wedge position within the selected bronchopulmonary segment. Three aliquots of 50 ml normal saline (at room temperature) were instilled through the bronchoscope. After the instillation of each aliquot, instilled saline was retrieved using a negative suction pressure of less than 100 mm Hg. Finally, three aliquots of 20 mL BALF samples were retrieved. The first sample was discarded to avoid contamination, and the other two samples were separated into two aliquots. One was sent for conventional microbial culture in a clinical microbiology laboratory and the other was used for detection using mNGS.
Traditional microbiological methods
BALF samples from all patients were examined by traditional microbiological methods including smears and cultures for general bacteria and fungi and acid-fast staining for mycobacteria. The following microbiological methods were performed according to the clinician’s discretion: real-time PCR for EBV and CMV from the blood samples, serum BDG assay and serum galactomannan (GM) assay for fungi, serum antibodies for indirect immunofluorescence assay for respiratory syncytial virus, influenza A/B virus, parainfluenza virus, adenovirus, Legionella pneumophila, Mycoplasma pneumoniae and Chlamydia pneumoniae. Unfortunately, due to the limitations of our laboratory, toluidine blue ‘O’ staining on BALF or sputum cannot be performed.
mNGS of BALF
Total nucleic acid was extracted from 5 ml of BALF. DNA or RNA sequencing libraries were constructed for each patient. An Agilent 2100 instrument was used to assess the quality of the libraries. Then, DNA or RNA libraries were constructed through DNA-fragmentation, end-repair, adapter-ligation, reverse transcription (for RNA) and PCR amplification. High-quality sequencing data were generated by removing low-quality and short (length < 35 bp) reads, followed by computational subtraction of human host sequences mapped to the human reference genome (hg19) using Burrows-Wheeler Alignment. The remaining data by removal of low-complexity reads were classified by simultaneously aligning to four Microbial Genome Databases, consisting of viruses, bacteria, fungi, and parasites. The performers and readers of mNGS company were blinded to patient information, including the symptoms and diagnosis.
We used the following criteria to define clinically significant microbes in this study, which were derived and revised from prior literature [30, 37, 38]. Bacteria (mycobacteria excluded), viruses, fungi, and parasites: A microbe was considered a clinically significant microbe when its relative abundance at the species level was more than 30% and there was supportive literature evidence of its pulmonary pathogenicity. Mycobacterium: Given the low possibility of Mycobacterium contamination and low yield rate, Mycobacterium was considered a clinically significant microbe when the stringently mapped read number at the species level was more than 3.
Statistical analysis
SPSS 22.0 software was employed for data analysis. The categorical variables were presented as frequency and percentage, and the continuous variables were analyzed using descriptive statistical methods (median and range). The comparison between enumeration data was performed by the chi-square test. P < 0.05 was considered as indicative of statistical significance.
Results
Patient characteristics
During about 6-year study period, 659 lymphoma patients received at least one course of chemotherapy and 38 (5.77%) of these patients developed IP. In total, 15 patients were eligible for this study (Fig. 2). The clinical characteristics of the 15 patients, including sex, age, histology, the international prognostic index (IPI) score at the time of diagnosis of lymphoma, history of smoking, prior lung disease, and the chemotherapies before the onset of IP, were demonstrated in Table 1. The cohort comprised 4 females and 11 males, with a median age of 56 years (range, 30 to 64 years). Most patients (10/15, 66.7%) had a diagnosis of diffuse large B-cell lymphoma (DLBCL), and 66.7% (10/15) patients had IPI score ≥ 2. Few patients presented a history of smoking (4/15, 26.7%) or basic lung disease (1/15, 6.7%). 80% (12/15) of patients received rituximab-based chemotherapies and 53.3% (8/15) of patients received a chemotherapy regimen containing doxorubicin hydrochloride liposome. Only one patient received neither rituximab nor doxorubicin hydrochloride liposome, but they underwent allogeneic hematopoietic stem cell transplantation (allo-HSCT) and used prednisone for anti-rejection. The patients received a median of 4 cycles (1 to 20 cycles) of chemotherapy before they developed IP.

Schematic flow chart of patient selection in this study. IP: interstitial pneumonia; mNGS: metagenomic next-generation sequencing; BALF: bronchoalveolar lavage fluid
Symptoms, CT findings and laboratory test results
The patients’ clinical symptoms, characteristic CT findings and laboratory test results were listed in Table 2. Among the 15 patients, only one (P 10) had no obvious symptoms. The most frequent symptoms were fever (14/15, 93.3%) and dyspnea (10/15, 66.7%), and the less common symptoms were cough (2/15,13.3%) and sputum (1/15,6.7%).
The most common predominant CT patterns were diffuse ground-glass opacities (GGO) in 13 of 15 patients and most of them were symmetric and with no zonal predominance. The other CT manifestations included diffuse patchy exudation and thickening of the interlobular septa. The figures of these CT scans were uploaded as supplement materials.
All patients had elevated C-reactive protein (CRP) (median 64.6 mg/L, range 10.6–227 mg/L), and 40% (6/15) patients had elevated absolute neutrophils (median 2.9*10^9/L, range 0.6–20.8*10^9/L). Serum BDG and GM assays were performed in 13 patients. Four patients had elevated serum BDG assays, and the GM assays were negative in all 13 patients. PCR tests for EBV were performed in 11 patients and were all negative. PCR for CMV was performed in 9 patients, and 1 patient was positive (P 6). Serum antibodies for indirect immunofluorescence assay for respiratory pathogens were performed in 6 patients and were all negative.
Culture outcomes from BALF
The outcomes of BALF staining and culture were also listed in Table 2. Only two cases (2/15, 13.3%) had positive outcomes, withKlebsiella pneumoniae and Staphylococcus aureus detected, respectively.
mNGS results
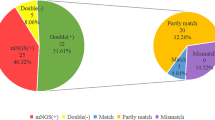
Pathogens were detected in 14 of 15 (93.3%) patients by mNGS (Table 2). It is worth noting thatP. jirovecii was detected in 12 patients (12/15, 80%) by this method. Among the patients with P. jirovecii, 4 patients had single P. jirovecii infection, while the other 8 patients had mixed infections of P. jirovecii with other pathogens. CMV and EBV were detected in 4 patients (4/15,26.7%) and 3 patients (3/15, 20%), respectively. Other infrequently detected pathogens were Campylobacter mucosa, Pseudostreptococcus pneumoniae, Candida albicans, Acinetobacter baumannii, Pseudomonas aeruginosa and Escherichia coli. The most common mixed infections were P. jirovecii together with CMV or EBV. The identified pathogens and copathogens were listed in Fig. 3.

Findings of pathogens of copathogens by mNGS
Pathogens detected by mNGS relative to conventional microbiologic methods
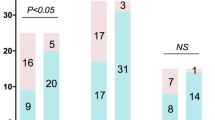
The overall microbial yield was 93.3% (14 of 15 patients) for mNGS versus 13.3% (2 of 15 patients) for traditional culture methods, with significant difference (Table 2;P ≤ 0.05). The pathogens detected by traditional culture methods were different from those detected by mNGS. Klebsiella pneumoniae and Staphylococcus aureus were respectively identified in P4 and P12 by culture of BALF, but not identified by mNGS. In the 4 patients with positive BDG assay, P. jirovecii was detected by mNGS, but no other fungal infection was identified.
Treatment of IP patients and outcomes
The treatments and outcomes of IP were also presented in Table 2. Treatments for IP included antimicrobial therapies and glucocorticoids. All patients were treated with antimicrobial drugs, and the most commonly used antimicrobial drug was TMP-SMX (14/15). Antibacterial drugs were used in 13 patients, while antifungal drugs were used in 8 patients. Of the 4 CMV-positive patients, 2 were treated with ganciclovir. Most of the enrolled patients (14 of 15) were treated with combinations of multiple antibiotics, and only 1 patient was treated with TMP-SMX alone. Three patients had severe hypoxemia and needed intubation (P5, P8, P15). It is worth noting that 5 patients recovered without the use of therapeutic doses of glucocorticoids (prednisone ≥ 20 mg daily). All of the patients with IP recovered after the applied treatments. Recovery of IP was considered when symptoms and > 75% of interstitial infiltrates disappeared. The recovery times varied between 5 days and 1 year.
Discussion
The main purpose of this study was to explore the pathogens of lymphoma patients with chemotherapy-related IP using the highly sensitive mNGS method. In previous studies on the etiology of chemotherapy-related IP, conventional microbiological methods are still the mainstream approach and with low detection rates [2, 10]. In this study, using mNGS, we found that the etiological detection rate of patients with chemotherapy-related IP was 93.3%. Moreover, P. jirovecii was detected in 80% of patients. The results suggested that detection of pathogens from BALF using mNGS was an extremely sensitive technique in this group of patients, especially for the detection of P. jirovecii.
P. jirovecii is a frequent opportunistic infection among immunocompromised patients. According to previous literature, Pneumocystis jirovecii pneumonia (PJP) occurred in 70–80% of AIDS patients [39]. A national study showed that the largest population associated with P. jirovecii were those suffering from underlying hematological malignancy [40]. The diagnosis of PJP include cytochemical or immunofluorescent staining and quantitative real-time PCR assay of respiratory specimen [41,42,43,44]. During the last years, the use of PCR has been increasingly investigated because of its high sensitivity. However, the PCR results are often difficult to interpret as they have various gene targets and sensitivities. To be able to differentiate between colonization and infection, standardized tests with data on interpreting low-level positives may be preferred [45]. Recently, mNGS was used for the diagnosis of pneumonia, and P. jirovecii was reported to be responsible for 61.2% of confirmed pneumonia in immunocompromised patients [30]. Meanwhile, in the study of pneumonia patients without immunosuppressed state, the detection rate of PJP was low even by mNGS [27, 46]. These results suggest that mNGS is a promising method for the accurate detection of P. jirovecii with high sensitivity and specificity. In this study, the enrolled patients suffered severe immunosuppression. It is reasonable to speculate that the P. jirovecii detected by mNGS was pathogen causing IP but not merely commensal.
Serum BDG assay and GM assay are helpful for the diagnosis of invasive fungal disease [47]. A meta-analysis showed that the sensitivity and specificity of the BDG assay for the diagnosis of invasive fungal disease were 50-90% and 70-100%, respectively [48]. Another meta-analysis showed the sensitivity and specificity of the BDG assay for invasive fungal disease were 76% and 85% respectively [49]. The BDG assay can also be used to diagnose PJP. Meta-analysis showed that the sensitivity and specificity of serum BDG assay for the diagnosis of PJP were 85% and 73% respectively in patients without human immunodeficiency virus infection [50]. In our study, 4 of 13 patients had elevated serum BDG assay, and P. jirovecii was detected by mNGS but no other fungal infection was identified in the 4 patients. This result suggests that BDG assay has good specificity in the detection of P. jirovecii in chemotherapy-related IP.
P. jirovecii infection is often associated with T cell dysfunction. Rituximab, on the other hand, can affect CD4 + T cell production by affecting B cells, leading to an increased risk of P. jirovecii infection [51, 52]. Several therapeutic options exist for the treatment of PJP and TMP-SMX is the first-line agent and drug of choice [21, 43]. No agent has been shown to have better outcomes than TMP-SMX. TMP-SMX is also the drug of choice for PJP prophylaxis. Daily or thrice weekly dosing is equally effective [53]. Jiang et al. [54] showed in a meta-analysis that lymphoma patients who received rituximab chemotherapy had a significantly increased risk of PJP, but that preventive therapy was highly effective in preventing PJP. Recently, several studies indicated that prophylactic anti-Pneumocystis treatment with TMP-SMX decreased the incidence of IP in patients with B-cell lymphoma and receiving chemotherapy [9, 55]. These findings suggested that P. jirovecii infection plays an important role in the pathogenesis of chemotherapy-related IP. In addition, the clinical manifestations of PJP patients are non-specific, so rapid and accurate diagnosis of PJP patients is very important for clinical prognosis. A recent retrospective study showed that in non-HIV-infected patients, the sensitivity of mNGS to diagnose PJP reached 100%, and the specificity of mNGS (96.3%) significantly exceeded that of BDG [56]. In this study, the detection rate of mNGS was also high (12/15, 80%). Therefore, we believe that mNGS has good performance in diagnosing PJP.
PJP and drug-induced IP may have a similar imaging presentation of diffuse pulmonary interstitial infiltration. Several studies tried to describe the different characteristics of them. Diffuse GGO or diffuse interstitial infiltration was frequent in patients with PJP [11, 57, 58]; in contrast, more than one focal alveolar pattern was observed in about half the patients with rituximab-induced interstitial lung disease [59]. Most PJPs (95%) show diffuse interstitial infiltration with nonzonal predominance and PJP showed a significant trend toward more severe disease [57]. In our study, 86.7% (13/15) of patients showed diffuse GGO. And in patients with P. jirovecii detected, diffuse GGO was observed in 92.3% (12/13) of cases, which met the characteristics of PJP.
CMV infections were the most frequently reported in patients after allo-HSCT [60], but they are less common in patients after conventional chemotherapy. In our study, the detection rate of CMV was also high (4/15,26.7%), suggesting that more research in this area is warranted in the future.
Cytomegalovirus infection is the most common in patients after allogeneic hematopoietic stem cell transplantation [52], but less common in patients after conventional chemotherapy. In addition, the lungs of PJP patients were often accompanied by CMV infection [61, 62]. In our study, the detection rate of CMV was also high (4/15,26.7%), with co-infection of CMV and P. jirovecii detected in 3 patients. In addition, of the four CMV-positive patients, only two patients received ganciclovir antiviral therapy, and the other two patients who did not receive treatment eventually recovered. This may be because CMV-specific T cell responses are intact when CMV is reactivated, and the host may eventually control viral replication without developing CMV pneumonia [61, 63]. For non-immunocompromised patients, CMV infection is generally considered benign and self-limiting [64]. Previous studies have shown that anti-CMV treatment does not affect the mortality and severity of PJP in HIV-infected people with interstitial pneumonia [65]. Similar results were found in non-HIV-infected patients [61]. The 4 CMV positive patients in this study were all detected by mNGS, while the conventional test was negative, which indicates that the mNGS test is more sensitive. However, critical readings for NGS used as markers of PJP and CMV have not yet been determined, and early bronchoscopy and mNGS are recommended for immunocompromised patients.
We also found some discordance between mNGS versus culture results. Klebsiella pneumoniae and Staphylococcus aureus were respectively identified in P4 and P12 by culture of BALF, but not identified by mNGS. One possible reason may be the contamination during culture. Another possible reason may be associated with the false negative of mNGS. Several reports suggested that the sensitivity of mNGS is not superior to that of culture for recognizing common bacteria (excluding MTB and anaerobes) [38, 66]. Therefore, it is necessary to combine mNGS and traditional microbiological methods to identify clinical infection.
Of the 15 enrolled patients, 5 patients recovered after receiving antimicrobial treatments alone without using glucocorticoids, indicating that the cause of interstitial pneumonia in these patients may be opportunistic infections instead of lung damage. From our results, we confer that the previous view of drug-induced lung injury rather than infection being the main pathogenesis of IP after lymphoma chemotherapy (especially rituximab-based chemotherapy) is debatable. Instead, opportunistic infections, especially P.jirovecii infection is potentially the major factor in the pathogenesis of IP.
This study has certain shortcomings. Firstly, as a retrospective study, there were selection bias and recall bias which was inevitable. Secondly, the toluidine blue ‘O’ staining and PCR assay for P.jirovecii and the BALF-GM or BALF-BGD tests were not performed. Thirdly, the sample size of the enrolled population was small and controls were lacking. Finally, it was difficult to distinguish pathogens from colonization to infection due to the unbiased detection of mNGS without a unified standard. In the future, we will conduct prospective studies and further expand the sample size, and explore the feasibility of guiding treatment options in line with the mNGS results.
Conclusion
In this study, we found that using mNGS test of BALF, the pathogen detection rate was much higher than that of traditional methods in lymphoma patients with chemotherapy-related IP. Notably, there was an especially high detection rate of P. jirovecii. We should be more alert to P. jirovecii infection in chemotherapy-related IP.
Data availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- IP:
-
interstitial pneumonia
- mNGS:
-
metagenomic next-generation sequencing
- BALF:
-
bronchoalveolar lavage fluid
- CMV:
-
cytomegalovirus
- EBV:
-
Epstein-Barr virus
- BDG:
-
beta-D-glucan
- GM:
-
galactomannan
- IPI:
-
international prognostic index
- CT:
-
computed tomography
- CRP:
-
C-reactive protein
- DLBCL:
-
diffuse large B-cell lymphoma
- MCL:
-
mantle cell lymphoma
- HL:
-
Hodgkin’s lymphoma, FL:follicular lymphoma
- ENKL:
-
extranodal NK/T cell lymphoma
- PTCL-NOS:
-
peripheral T-cell lymphoma-NOS
- allo-HSCT:
-
allogeneic hematopoietic stem cell transplantation
- GGO:
-
ground-glass opacities
- PJP:
-
Pneumocystis jirovecii pneumonia
- TMP-SMX:
-
trimethoprim sulfamethoxazole
References
Armitage JO, Gascoyne RD, Lunning MA, Cavalli F. Non-hodgkin Lymphoma. Lancet. 2017;390(10091):298–310.
Liu WP, Wang XP, Zheng W, Xie Y, Tu MF, Lin NJ, et al. Incidence, clinical characteristics, and outcome of interstitial Pneumonia in patients with Lymphoma. Ann Hematol. 2018;97(1):133–9.
Salmasi G, Li M, Sivabalasundaram V, Panzarella T, Tsang R, Kukreti V, et al. Incidence of pneumonitis in patients with non-hodgkin Lymphoma receiving chemoimmunotherapy with rituximab. Leuk Lymphoma. 2015;56(6):1659–64.
Zhou T, Shen Q, Peng H, Chao T, Zhang L, Huang L, et al. Incidence of interstitial pneumonitis in non-hodgkin’s Lymphoma patients receiving immunochemotherapy with pegylated liposomal doxorubicin and rituximab. Ann Hematol. 2018;97(1):141–7.
Meng YN, Wang S, Shi Q, Xu PP, Cheng S, Wang L, et al. [Interstitial Pneumonia in patients with diffuse large B-cell Lymphoma receiving RCHOP and RCDOP regimens]. Zhonghua Xue Ye Xue Za Zhi. 2019;40(12):1015–20.
Peerzada MM, Spiro TP, Daw HA. Pulmonary toxicities of biologics: a review. Anticancer Drugs. 2010;21(2):131–9.
Wu Y, Jia Y, Xu J, Shuai X, Wu Y. Fatal interstitial lung Disease induced by rituximab-containing chemotherapy, treatment with TNF-alpha antagonist and cytokine profiling: a case-report and review of the literature. J Clin Pharm Ther. 2013;38(3):249–53.
Tan J, Ni X. TNF-alpha antagonist may not be suitable for severe rituximab-induced interstitial lung Disease. J Clin Pharm Ther. 2015;40(3):249–50.
Li C, Lu F, Lei T, Yu H, Chen X, Peng S, et al. Prophylactic antibiotic treatment with TMP-SMX decreased the incidence of interstitial Pneumonia in patients with B-cell Lymphoma on chemotherapy. BMC Cancer. 2020;20(1):742.
Li C, Lu F, Lei T, Yu H, Yang H. Clinical features, treatment and risk factors for interstitial Pneumonia in B-cell non-hodgkin Lymphoma patients. Transl Cancer Res. 2020;9(9):5139–46.
Martin-Garrido I, Carmona EM, Specks U, Limper AH. Pneumocystis Pneumonia in patients treated with rituximab. Chest. 2013;144(1):258–65.
Jiang XQ, Fang L, Mei XD, Wang XJ, Bao MH. Pneumocystis Jiroveci Pneumonia in patients with Non-hodgkin’s Lymphoma after Rituximab-containing regimen: two cases of report and literature review. J Thorac Disease. 2013;5(4):E162–6.
Venhuizen AC, Hustinx WN, van Houte AJ, Veth G, van der Griend R. Three cases of Pneumocystis Jirovecii Pneumonia (PCP) during first-line treatment with rituximab in combination with CHOP-14 for aggressive B-cell non-hodgkin’s Lymphoma. Eur J Haematol. 2008;80(3):275–6.
Lee JY, Kang M, Suh KJ, Kim JW, Kim SH, Kim JW, et al. Pneumocystis Jirovecii Pneumonia in diffuse large B-cell Lymphoma treated with R-CHOP. Mycoses. 2021;64(1):60–5.
Azadeh N, Limper AH, Carmona EM, Ryu JH. The role of Infection in interstitial Lung Diseases: a review. Chest. 2017;152(4):842–52.
Richter AG, Stockley RA, Harper L, Thickett DR. Pulmonary Infection in Wegener granulomatosis and Idiopathic Pulmonary Fibrosis. Thorax. 2009;64(8):692–7.
Molyneaux PL, Cox MJ, Willis-Owen SA, Mallia P, Russell KE, Russell AM, et al. The role of bacteria in the pathogenesis and progression of Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2014;190(8):906–13.
Vidal S, de la Horra C, Martin J, Montes-Cano MA, Rodriguez E, Respaldiza N, et al. Pneumocystis jirovecii colonisation in patients with interstitial lung Disease. Clin Microbiol Infect. 2006;12(3):231–5.
Blivet S, Philit F, Sab JM, Langevin B, Paret M, Guerin C, et al. Outcome of patients with Idiopathic Pulmonary Fibrosis admitted to the ICU for Respiratory Failure. Chest. 2001;120(1):209–12.
Chioma OS, Drake WP. Role of Microbial Agents in Pulmonary Fibrosis. Yale J Biol Med. 2017;90(2):219–27.
Fishman JA, Gans H, Practice ASTIDC. Pneumocystis Jiroveci in solid organ transplantation: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transpl. 2019;33(9):e13587.
Douglas AP, Smibert OC, Bajel A, Halliday CL, Lavee O, McMullan B, et al. Consensus guidelines for the diagnosis and management of invasive aspergillosis, 2021. Intern Med J. 2021;51(Suppl 7):143–76.
Shiraishi Y, Kryukov K, Tomomatsu K, Sakamaki F, Inoue S, Nakagawa S, et al. Diagnosis of pleural empyema/parapneumonic effusion by next-generation sequencing. Infect Dis (Lond). 2021;53(6):450–9.
Chen Z, Cheng H, Cai Z, Wei Q, Li J, Liang J, et al. Identification of Microbiome Etiology Associated with Drug Resistance in Pleural Empyema. Front Cell Infect Microbiol. 2021;11:637018.
Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for Pathogen Detection. Annu Rev Pathol. 2019;14:319–38.
Duan H, Li X, Mei A, Li P, Liu Y, Li X, et al. The diagnostic value of metagenomic next rectanglegeneration sequencing in infectious Diseases. BMC Infect Dis. 2021;21(1):62.
Qi C, Hountras P, Pickens CO, Walter JM, Kruser JM, Singer BD, et al. Detection of respiratory pathogens in clinical samples using metagenomic shotgun sequencing. J Med Microbiol. 2019;68(7):996–1002.
Chen Y, Feng W, Ye K, Guo L, Xia H, Guan Y, et al. Application of Metagenomic Next-Generation sequencing in the diagnosis of pulmonary infectious pathogens from Bronchoalveolar Lavage Samples. Front Cell Infect Microbiol. 2021;11:541092.
Chen J, Zhao Y, Shang Y, Lin Z, Xu G, Bai B et al. The clinical significance of simultaneous detection of pathogens from bronchoalveolar lavage fluid and blood samples by metagenomic next-generation sequencing in patients with severe Pneumonia. J Med Microbiol. 2021;70(1).
Peng JM, Du B, Qin HY, Wang Q, Shi Y. Metagenomic next-generation sequencing for the diagnosis of suspected Pneumonia in immunocompromised patients. J Infect. 2021;82(4):22–7.
Casto AM, Fredricks DN, Hill JA. Diagnosis of infectious Diseases in immunocompromised hosts using metagenomic next generation sequencing-based diagnostics. Blood Rev. 2022;53:100906.
Travis WD, Costabel U, Hansell DM, King TE Jr., Lynch DA, Nicholson AG, et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–48.
Park SW, Baek AR, Lee HL, Jeong SW, Yang SH, Kim YH, et al. Korean guidelines for diagnosis and management of interstitial Lung Diseases: part 1. Introduction Tuberc Respir Dis (Seoul). 2019;82(4):269–76.
Park SW, Baek AR, Lee HL, Jeong SW, Yang SH, Kim YH, et al. Korean guidelines for diagnosis and management of interstitial Lung Diseases: part 1. Introduction Tuberculosis and Respiratory Diseases. 2019;82(4):269–76.
Lee SH, Yeo Y, Kim TH, Lee HL, Lee JH, Park YB, et al. Korean guidelines for diagnosis and management of interstitial Lung Diseases: part 2. Idiopathic Pulmonary Fibrosis. Tuberc Respir Dis (Seoul). 2019;82(2):102–17.
Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, du Bois RM, et al. An official American Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung Disease. Am J Respir Crit Care Med. 2012;185(9):1004–14.
Li Y, Sun B, Tang X, Liu YL, He HY, Li XY, et al. Application of metagenomic next-generation sequencing for bronchoalveolar lavage diagnostics in critically ill patients. Eur J Clin Microbiol Infect Dis. 2020;39(2):369–74.
Miao Q, Ma Y, Wang Q, Pan J, Zhang Y, Jin W, et al. Microbiological Diagnostic performance of Metagenomic Next-generation sequencing when Applied to Clinical Practice. Clin Infect Dis. 2018;67(suppl2):231–S40.
Avino LJ, Naylor SM, Roecker AM. Pneumocystis Jirovecii Pneumonia in the Non-HIV-Infected Population. Ann Pharmacother. 2016;50(8):673–9.
Maini R, Henderson KL, Sheridan EA, Lamagni T, Nichols G, Delpech V, et al. Increasing Pneumocystis Pneumonia, England, UK, 2000–2010. Emerg Infect Dis. 2013;19(3):386–92.
Esteves F, Gaspar J, de Sousa B, Antunes F, Mansinho K, Matos O. Pneumocystis jirovecii multilocus genotyping in pooled DNA samples: a new approach for clinical and epidemiological studies. Clin Microbiol Infect. 2012;18(6):E177–84.
Flori P, Bellete B, Durand F, Raberin H, Cazorla C, Hafid J, et al. Comparison between real-time PCR, conventional PCR and different staining techniques for diagnosing Pneumocystis Jiroveci Pneumonia from bronchoalveolar lavage specimens. J Med Microbiol. 2004;53(Pt 7):603–7.
Brakemeier S, Pfau A, Zukunft B, Budde K, Nickel P. Prophylaxis and treatment of Pneumocystis Jirovecii Pneumonia after solid organ transplantation. Pharmacol Res. 2018;134:61–7.
Lu Y, Ling G, Qiang C, Ming Q, Wu C, Wang K, et al. PCR diagnosis of Pneumocystis Pneumonia: a bivariate meta-analysis. J Clin Microbiol. 2011;49(12):4361–3.
Sasso M, Chastang-Dumas E, Bastide S, Alonso S, Lechiche C, Bourgeois N, et al. Performances of Four Real-Time PCR assays for diagnosis of Pneumocystis Jirovecii Pneumonia. J Clin Microbiol. 2016;54(3):625–30.
Wang J, Han Y, Feng J. Metagenomic next-generation sequencing for mixed pulmonary Infection diagnosis. BMC Pulm Med. 2019;19(1):252.
Huang XJ. [Promote laboratory methods to improve the diagnosis for invasive fungal Disease]. Zhonghua Xue Ye Xue Za Zhi. 2017;38(11):913–5.
Lamoth F, Cruciani M, Mengoli C, Castagnola E, Lortholary O, Richardson M et al. beta-Glucan antigenemia assay for the diagnosis of invasive fungal infections in patients with hematological malignancies: a systematic review and meta-analysis of cohort studies from the Third European Conference on Infections in Leukemia (ECIL-3). Clin Infect Dis. 2012;54(5):633 – 43.
Lu Y, Chen YQ, Guo YL, Qin SM, Wu C, Wang K. Diagnosis of invasive fungal Disease using serum (1–>3)-beta-D-glucan: a bivariate meta-analysis. Intern Med. 2011;50(22):2783–91.
Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 World Health Organization Classification of Lung Tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243–60.
Wei KC, Sy C, Wu SY, Chuang TJ, Huang WC, Lai PC. Pneumocystis Jirovecii Pneumonia in HIV-uninfected, rituximab treated non-hodgkin Lymphoma patients. Sci Rep. 2018;8(1):8321.
Lund FE, Hollifield M, Schuer K, Lines JL, Randall TD, Garvy BA. B cells are required for generation of protective effector and memory CD4 cells in response to Pneumocystis lung infection. Journal of immunology (Baltimore, Md: 1950). 2006;176(10):6147-54.
Stern A, Green H, Paul M, Vidal L, Leibovici L. Prophylaxis for Pneumocystis Pneumonia (PCP) in non-HIV immunocompromised patients. Cochrane Database Syst Rev. 2014(10):CD005590.
Jiang X, Mei X, Feng D, Wang X. Prophylaxis and Treatment of Pneumocystis Jiroveci Pneumonia in Lymphoma patients subjected to Rituximab-contained therapy: a systemic review and Meta-analysis. PLoS ONE. 2015;10(4):e0122171.
Park JW, Curtis JR, Jun KI, Kim TM, Heo DS, Ha J, et al. Primary Prophylaxis for Pneumocystis Jirovecii Pneumonia in patients receiving Rituximab. Chest. 2022;161(5):1201–10.
Jiang J, Bai L, Yang W, Peng W, An J, Wu Y, et al. Metagenomic next-generation sequencing for the diagnosis of Pneumocystis Jirovecii Pneumonia in Non-HIV-Infected patients: a retrospective study. Infect Dis Therapy. 2021;10(3):1733–45.
Park SY, Kim MY, Choi WJ, Yoon DH, Lee SO, Choi SH, et al. Pneumocystis Pneumonia versus rituximab-induced interstitial lung Disease in Lymphoma patients receiving rituximab-containing chemotherapy. Med Mycol. 2017;55(4):349–57.
Kim T, Choi SH, Kim SH, Jeong JY, Woo JH, Kim YS, et al. Point prevalence of Pneumocystis Pneumonia in patients with non-hodgkin Lymphoma according to the number of cycles of R-CHOP chemotherapy. Ann Hematol. 2013;92(2):231–8.
Liote H, Liote F, Seroussi B, Mayaud C, Cadranel J. Rituximab-induced lung Disease: a systematic literature review. Eur Respir J. 2010;35(3):681–7.
Li S, Shen ZH, Wan LP, Bao AH, Yang J, Tong Y, et al. [Cytomegalovirus Pneumonia after allogeneic hematopoietic stem cell transplantation]. Zhonghua Nei Ke Za Zhi. 2021;60(6):556–60.
Yu Q, Jia P, Su L, Zhao H, Que C. Outcomes and prognostic factors of non-HIV patients with pneumocystis jirovecii Pneumonia and pulmonary CMV co-infection: a retrospective cohort study. BMC Infect Dis. 2017;17(1):392.
Xie Y, Ruan B, Jin L, Zhu B. Case Report: next-generation sequencing in diagnosis of Pneumonia due to Pneumocystis Jirovecii and Cytomegalovirus in a patient with HIV Infection. Front Med. 2021;8:653294.
Kim T, Park SY, Lee HJ, Kim SM, Sung H, Chong YP, et al. Assessment of cytomegalovirus and cell-mediated immunity for predicting outcomes in non-HIV-infected patients with pneumocystis jirovecii Pneumonia. Medicine. 2017;96(30):e7243.
Yang A, Chen C, Hu Y, Zheng G, Chen P, Xie Z, et al. Application of Metagenomic Next-Generation sequencing (mNGS) using Bronchoalveolar Lavage Fluid (BALF) in diagnosing Pneumonia of children. Microbiol Spectr. 2022;10(5):e0148822.
Bower M, Barton SE, Nelson MR, Bobby J, Smith D, Youle M, et al. The significance of the detection of cytomegalovirus in the bronchoalveolar lavage fluid in AIDS patients with Pneumonia. AIDS. 1990;4(4):317–20.
Toma I, Siegel MO, Keiser J, Yakovleva A, Kim A, Davenport L, et al. Single-molecule long-read 16S sequencing to characterize the lung microbiome from mechanically ventilated patients with suspected Pneumonia. J Clin Microbiol. 2014;52(11):3913–21.
Acknowledgements
We thank the patients for cooperating with our investigation and acknowledge all investigators who participated in this study, including physicians, nurses, and laboratory technicians.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
D.J. and W.S. conceived the study and wrote the paper; J.L. revised the paper; Q.Y., L.L. and J.T. collected data; Q.C. and H.D. performed statistical analyses. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Ethics approval
The study protocol was approved by the Ethical Review Committee of Ningbo Medical Treatment Center Li Huili Hospital (approval number: KY2022PJ155).
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jin, D., Le, J., Yang, Q. et al. Pneumocystis jirovecii with high probability detected in bronchoalveolar lavage fluid of chemotherapy-related interstitial pneumonia in patients with lymphoma using metagenomic next-generation sequencing technology. Infect Agents Cancer 18, 80 (2023). https://doi.org/10.1186/s13027-023-00556-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13027-023-00556-1