
Abstract
Background
Axial neck pain is one of the complications of posterior cervical surgeries such as laminoplasty. This study aimed to investigate the efficiency of the PainVision apparatus for axial neck pain assessment by comparing it with other methods.
Methods
This prospective study included 118 patients (90 men and 28 women; average age: 66.9 (32–86) years) with cervical myelopathy who underwent open-door laminoplasty at our medical center between April 2009 and August 2019. Pain degree (PD) measured by PainVision, visual analog scale (VAS), and bodily pain (BP), a subitem of the MOS 36-Item Short-Form Health Survey (SF36), were used to evaluate axial neck pain, which was investigated preoperatively and at 3, 6, 12, 18, and 24 months postoperatively.
Results
Comparison of the scores at each evaluation time point found significant improvement between the pre- and post-operative values for all assessment methods. Further, on comparing the amounts of change between pre- and post-operative scores in each pain assessment method, we found significant differences in PD and VAS but not in BP. We also found significant positive correlations between PD and VAS at each time point (all p < 0.001) and significant negative correlations between PD and BP (all p < 0.05) and between VAS and BP (all p < 0.01) at each time point.
Conclusions
In this study, we demonstrated that PD and VAS are more sensitive indicators of changes in axial neck pain than BP and also that PD has an excellent correlation with VAS. These results suggest that the PainVision apparatus may be an effective instrument for quantifying axial neck pain after cervical laminoplasty, though its superiority over VAS needs to be verified in future studies.
Similar content being viewed by others


Background
Cervical myelopathy is a progressive degenerative disease that causes sensory disturbance in the extremities, dysfunction of hand movement, gait disturbance, and dysuria [1]. Laminoplasty was developed as a surgical method for cervical myelopathy and is widely performed. However, one of the complications of laminoplasty is neck and shoulder pain, referred to as axial symptoms. It is also defined as axial neck pain [2], which significantly affects quality of life [3]. It is reported that axial neck pain has improved due to various improvements in surgical methods, rehabilitation, and orthosis [4,5,6,7]; however, the evaluation criteria of axial neck pain vary across reports, and it is notoriously difficult to evaluate pain in an objective and robust manner. This is in part due to the wide variability in pain thresholds and pain tolerance between individuals.
The PainVision PS-2100 (Nipro, Osaka, Japan), a quantitative pain analyzer, has been clinically applied to low back pain disorders, herpes zoster, and cancer pain [8,9,10]. However, to the best of our knowledge, no study has reported on assessment of axial neck pain after cervical laminoplasty. Therefore, this study aimed to investigate the efficacy of the PainVision apparatus for axial neck pain assessment by comparing it with other assessment methods.
Methods
Study population
This prospective study included a total of 118 patients with cervical myelopathy (110 patients with cervical spondylotic myelopathy; 8 with ossification of the posterior longitudinal ligament; 90 men and 28 women, with an average age of 66.9 years (32–86 years)) who underwent open-door laminoplasty at our medical center between April 2009 and August 2019. The cervical vertebral level at which laminoplasty was performed was C3–6 in 17 patients, C3–7 in 8, C4–6 in 87, and C4–7 in 6.
Patients with a history of cervical spine surgery, cervical radiculopathy, and those who received spinal fusion surgery together with laminoplasty were excluded from this study. This study was approved by the Ethics Committee of the local university. All patients were given an overview of the study either orally or in writing, and informed consent was obtained.
Surgical technique
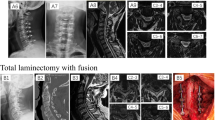
In this study, a single surgeon performed open-door laminoplasty using a slightly modified version of the Ito-Tsuji technique [7]. A posterior midline incision was performed, followed by an incision of the ligamentum nuchae. The detachment of muscle was performed slightly lateral to the lamina-facet junction. When the cervical vertebral levels at which laminoplasty was performed were C4–6, the muscles from the C3 to C6 were detached. However, the muscles attached to C2 and C7 were preserved. When the laminoplasty range included C3, the semispinalis cervicis muscle insertion at C2 was dissected. On the other hand, when the laminoplasty range included C7, the muscle attached to C7 was dissected. Gutters were fashioned on the inner edges of the facet joints on both the open and hinge sides. Following creation of the gutters, the lamina was opened and the ligamentum flavum as well as the epidural adhesion tissue on the open side was severed when necessary. Suture material was passed through a small burr hole that was created on the open side, and a hydroxyapatite spacer was placed to keep the lamina open (Fig. 1). A closed drain was inserted, and the wound was closed by suturing the ligamentum nuchae. On post-operative day 2, patients were allowed to leave their beds. Use of cervical collars was avoided where possible. During the early post-operative period, cervical spine range of motion training and isometric muscle strengthening were initiated.

Post-operative X-rays and computed tomography images. Hydroxyapatite spacers were used for open-door laminoplasty in the present study
Outcome measures
The PainVision generated a superficial pulsed current (50 Hz; 0–150 μA; pulse amplitude, 0.3 ms) that gradually increased in intensity and measured the participant’s perception thresholds and current producing pain compatible with their axial neck pain (i.e., the current producing pain of the same intensity as the axial neck pain reported by the patient). We defined axial neck pain as pain or stiffness around the posterior neck or scapular areas in line with previous studies [4, 5]. The electrode of the PainVision was patched onto the surface of the patients’ forearm. The pain degree (PD) was automatically calculated (pain degree = 100 × (current producing pain comparable with axial neck pain—current at perception threshold) / current at perception threshold) (Fig. 2).

Photograph of the PainVision PS-2100 unit. The PainVision generated a superficial pulsed current that gradually increased in intensity and measured the participant’s perception thresholds and currently producing pain compatible with their axial neck pain were measured
In addition to PD measured by the PainVision, visual analog scale (VAS) (score of 0 indicated no pain and 100 indicated worst pain) and bodily pain (BP) (the Japanese national standard was set at 50), a subitem of the MOS 36-Item Short-Form Health Survey (SF36), were used to evaluate axial neck pain and investigated preoperatively and at 3, 6, 12, 18, and 24 months postoperatively. The main analyses performed were as follows:
-
(1)
The axial neck pain scores preoperatively and at 3, 6, 12, 18, and 24 months postoperatively were compared using three pain assessment methods (PD, VAS, and BP).
-
(2)
The amounts of change between pre- and post-operative scores in three pain assessment methods were compared. The amount of change was defined as ( (scores at each assessment point) − (preoperative scores)) and evaluated at 3, 6, 12, 18, and 24 months postoperatively.
-
(3)
Correlation analyses between three types of pain assessment methods were evaluated.
Statistical analysis
Statistical analyses were performed using SPSS, version 25.0 for Windows (IBM Japan, Tokyo, Japan). All values are expressed as mean ± standard deviation or as median and interquartile range (IQR). The Friedman test was used for intragroup comparisons after confirming the normality of the data beforehand. The Bonferroni method was used for post-tests. Spearman's rank correlation coefficient test was used for correlation analysis of the three pain assessment methods (PD, VAS, and BP). P values < 0.05 were considered statistically significant.
Results
The median scores preoperatively and at 3, 6, 12, 18, and 24 months postoperatively in each assessment method were as follows (Table 1): PD, 82.5, 63.5, 52, 47, 43, and 31, respectively; VAS scores (mm), 43.5, 23.5, 20, 20, 20, and 16, respectively; and BP, 35.4, 40.3, 40.3, 40.3, 40.3, and 44.7, respectively.
Comparison of the pre- and post-operative scores in each pain assessment method
Comparison of the pre- and post-operative scores using the Friedman test showed significant differences in all assessment methods (p < 0.001; Table 1). The post-test results using the Bonferroni method are shown in Table 2. For PD, significant differences were observed between scores preoperatively and 3 months postoperatively (p = 0.023), preoperatively and 6 months postoperatively (p = 0.004), preoperatively and 12 months postoperatively (p < 0.001), preoperatively and 18 months postoperatively (p < 0.001), and preoperatively and 24 months postoperatively (p < 0.001; Table 2). VAS scores showed significant differences between preoperatively and 12 months postoperatively (p = 0.013), preoperatively and 18 months postoperatively (p = 0.002), preoperatively and 24 months postoperatively (p < 0.001), and 6 months postoperatively and 24 months postoperatively (p = 0.024; Table 2). BP showed significant differences between preoperatively and 3 months postoperatively (p = 0.010), preoperatively and 6 months postoperatively (p = 0.005), preoperatively and 12 months postoperatively (p < 0.001), preoperatively and 18 months postoperatively (p < 0.001), and preoperatively and 24 months postoperatively (p < 0.001; Table 2).
Comparison of the amounts of change between pre- and post-operative scores in each pain assessment method
Comparison of the amounts of change between pre- and post-operative scores using the Friedman test showed significant differences in PD and VAS scores but not in BP (Table 3). The results of the post-test using the Bonferroni method are shown in Table 4.
For PD, a significant difference was noted between the amount of change at 3 months postoperatively and that at 18 months postoperatively (p = 0.022) and between that at 3 months postoperatively and that at 24 months postoperatively (p = 0.025; Table 4). For VAS scores, significant differences were observed at 3 months and 24 months postoperatively (p = 0.004) and at 6 months and 24 months postoperatively (p = 0.028; Table 4).
Correlation analyses between the three pain assessment methods (PD, VAS, and BP)
Correlation analyses (Table 5) revealed significant positive correlations between PD and VAS scores at each time point (all p < 0.001) and significant negative correlations between PD and BP (all p < 0.05) and between VAS and BP at each time point (all p < 0.01).
Discussion
This study aimed to investigate the utility of PD, which was measured using the PainVision apparatus, as a pain assessment method by comparing it with VAS and BP. Through the prospective study of 118 patients with cervical myelopathy who underwent open-door laminoplasty at our medical center, we investigated axial neck pain preoperatively and at 3, 6, 12, 18, and 24 months postoperatively. We found PD and VAS to be more sensitive indicators of changes in axial neck pain than BP because comparing the amounts of change between pre- and post-operative scores in each pain assessment method showed significant differences in PD and VAS scores but not in BP. In addition, significant correlations were found in each pain assessment method, with robust positive correlations between PD and VAS.
Axial neck pain may increase after cervical posterior surgeries such as laminoplasty [11]. In a previous study, during the period when no preventive measures were taken, the incidence of axial pain after laminoplasty was 60%, and 25% of patients had severe pain that persisted for > 3 months after surgery [11]. In another study, laminoplasty and anterior cervical fusion were compared and the occurrence of axial pain after laminoplasty was found to be higher [12, 13].
Some preoperative factors and patient selection can influence outcomes following laminoplasty. For example, patients with a low mental state, potentially before surgery, are at a high risk of post-operative axial neck pain [14].
Many studies on preventive measures for axial neck pain have been reported [2, 4, 15,16,17,18,19,20]. A meta-analysis evaluating the presence of axial symptoms after posterior cervical decompression found that preservation of the posterior muscles and structures, stabilization of cervical vertebrae, and reduction in external cervical immobilization time were associated with reduced axial symptoms postoperatively [21]. The occurrence of axial neck pain, one of the complications after cervical laminoplasty, is likely to be decreasing due to the various modifications described above.
According to previous reports, different pain assessment methods were used for axial neck pain. There is no one method that can be termed the gold standard, probably because all methods have advantages and disadvantages. Hosono et al. [15] used a self-designed pain assessment method, wherein axial neck pain was graded according to previously published criteria, as follows: severe (pain killer or local injection regularly required), moderate (physiotherapy or compress regularly required), or mild (no treatment needed). Sakaura et al. also used this grading system [22], which is limited by the fact that the type and frequency of pain medications used varied between each patient. In a study by Mori et al. [16], VAS grades were used (I–IV): Grade I, 0–2.5 points; Grade II, 2.6–5.0 points; Grade III, 5.1–7.5 points; and Grade IV, 7.6–10.0 points, also limited by the arbitrary and artificial grade groupings. Takeuchi et al. described a self-designed pain assessment tool [4], which was graded as follows: no axial symptoms (no symptoms), occasional symptoms but no problems in activities of daily living (mild symptoms), and some problems in activities of daily living or work due to the symptoms (severe symptoms); however, the words ‘occasional’ and ‘some’ used in the gradings are subjective and open to differences in interpretation between individuals; for example, ‘occasional’ for one person will not be same as for another. Kimura et al. [3] rated axial neck pain on an 11-point scale from 0 to 10 using a numeric rating scale, and Yoshida et al. [6] described a self-designed pain assessment method graded 0–V: grade 0 = never, grade I = rarely, grade II = mild, grade III = moderate, grade IV = severe, and grade V = intolerable; this latter scale is also limited by the lack of precision in what would constitute ‘rarely,’ ‘mild,’ ‘moderate,’ ‘severe,’ and ‘intolerable,’ which would differ between individuals.
Pain assessment is essential for determining the effectiveness of treatment, and a method with scientific reliability and validity is ideal. However, pain is a purely subjective complaint and is impossible to evaluate in a truly objective manner. To this end, the goal should be the development of reliable and reproducible assessments of pain. In this study, three pain assessment methods, PD, VAS, and BP, were selected, and no obvious difference was noted in the sensitivity of the three methods when comparing scores at the time of each assessment. However, on comparing the change in scores of each evaluation method, significant differences were found in PD and VAS but not in BP. These results suggest that PD and VAS are more sensitive indicators of changes in axial neck pain than BP. It was difficult to establish relative superiority between PD and VAS. However, although VAS is useful for evaluating pain before and after treatment in the same case, it is difficult to use it to compare pain across cases [23]. On the other hand, PD is an evaluation method that applies perception thresholds; hence, there is a possibility that pain can be compared across cases [23]. Therefore, PD may be the preferred technique for studies comparing pain between different populations. VAS is also limited by ceiling effects that restrict the ability of patients to quantify worsening pain reliably [24] and conceal variation in the intensity of severe pain [25]; more specifically, the ceiling effect results in compression of all intensity ratings [26], and VAS anchors are poorly defined, thereby increasing the risk of misinterpretation, bias, and confusion [27].
PD has been measured using the PainVision in patients with low back pain previously, showing consistency with repeated calculations [23]. In another study that assessed low back pain, PD also showed a moderate correlation with the numeric rating scale scores at each time point [9]. Moreover, a previous study showed that the PainVision was also useful for the quantitative assessment of sensory disturbance [28, 29].
This study has some limitations. First, the PainVision is expensive (approximately 1,500,000 JPY or 11,500 USD) that hinders widespread use, particularly in resource-limited settings. Second, the lack of evaluation within the first 3 months following surgery. This was due to the fact that most patients in our medical center are transferred to other hospitals for rehabilitation after surgery.
Conclusions
In this study, we demonstrated that PD and VAS are more sensitive indicators of changes in axial neck pain than BP and also that PD has an excellent correlation with VAS. These results suggest that the PainVision apparatus may be an effective instrument for quantifying axial neck pain after cervical laminoplasty, though its superiority over VAS needs to be verified in future studies.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
24 October 2023
A Correction to this paper has been published: https://doi.org/10.1186/s13018-023-04277-4
Abbreviations
- PD:
-
Pain degree
- BP:
-
Bodily pain
- VAS:
-
Visual analog scale
- IQR:
-
Interquartile range
References
Nouri A, Tetreault L, Singh A, Karadimas SK, Fehlings MG. Degenerative cervical myelopathy: epidemiology, genetics, and pathogenesis. Spine (Phila Pa 1976). 2015;40(12):E675-93.
Wang SJ, Jiang SD, Jiang LS, Dai LY. Axial pain after posterior cervical spine surgery: a systematic review. Eur Spine J. 2011;20(2):185–94.
Kimura A, Endo T, Inoue H, Seichi A, Takeshita K. Impact of axial neck pain on quality of life after laminoplasty. Spine (Phila Pa 1976). 2015;40(24):E1292-8.
Takeuchi K, Yokoyama T, Aburakawa S, Saito A, Numasawa T, Iwasaki T, et al. Axial symptoms after cervical laminoplasty with C3 laminectomy compared with conventional C3–C7 laminoplasty: a modified laminoplasty preserving the semispinalis cevicis inserted into axis. Spine (Phila Pa 1976). 2005;30(22):2544–9.
Kato M, Nakamura H, Konishi S, Dohzono S, Toyoda H, Fukushima W, et al. Effect of preserving paraspinal muscles on postoperative axial pain in the selective cervical laminoplasty. Spine (Phila Pa 1976). 2008;33(14):E455-9.
Yoshida M, Tamaki T, Kawakami M, Nakatani N, Ando M, Yamada H, et al. Does reconstruction of posterior ligamentous complex with extensor musculature decrease axial symptoms after cervical laminoplasty? Spine (Phila Pa 1976). 2002;27(13):1414–8.
Itoh T, Tsuji H. Technical improvements and results of laminoplasty for compressive myelopathy in the cervical spine. Spine (Phila Pa 1976). 1985;10(8):729–36.
Wang D, Zhang K, Han S, Yu LZ. PainVision apparatus for assessment of efficacy of pulsed radiofrequency combined with pharmacological therapy in the treatment of postherpetic neuralgia and correlations with measurements. BioMed Res Int. 2017;2017:5670219.
Ohtori S, Kawaguchi H, Takebayashi T, Orita S, Inoue G, Yamauchi K, et al. PainVision apparatus is effective for assessing low back pain. Asian Spine J. 2014;8(6):793–8.
Katims JJ. Electrodiagnostic functional sensory evaluation of the patient with pain: a review of the neuroselective current perception threshold and pain tolerance threshold. Pain Digest. 1998;8:219–30.
Hosono N, Yonenobu K, Ono K. Neck and shoulder pain after laminoplasty. A noticeable complication. Spine (Phila Pa 1976). 1996;21(17):1969–73.
Wada E, Suzuki S, Kanazawa A, Matsuoka T, Miyamoto S, Yonenobu K. Subtotal corpectomy versus laminoplasty for multilevel cervical spondylotic myelopathy: a long-term follow-up study over 10 years. Spine (Phila Pa 1976). 2001;26(13):1443–7.
Seng C, Tow BP, Siddiqui MA, Srivastava A, Wang L, Yew AK, et al. Surgically treated cervical myelopathy: a functional outcome comparison study between multilevel anterior cervical decompression fusion with instrumentation and posterior laminoplasty. Spine J. 2013;13:723–31.
Oshima Y, Matsubayashi Y, Taniguchi Y, Hayakawa K, Fukushima M, Oichi T, et al. Mental state can influence the degree of postoperative axial neck pain following cervical laminoplasty. Glob Spine J. 2019;9(3):292–7.
Hosono N, Sakaura H, Mukai Y, Yoshikawa H. The source of axial pain after cervical laminoplasty-C7 is more crucial than deep extensor muscles. Spine (Phila Pa 1976). 2007;32:2985–8.
Mori E, Ueta T, Maeda T, Yugué I, Kawano O, Shiba K. Effect of preservation of the C6 spinous process and its paraspinal muscular attachment on the prevention of postoperative axial neck pain in C3–6 laminoplasty. J Neurosurg Spine. 2015;22(3):221–9.
Qi Q, Chen Y, Ling Z, Hu H, Ma J, Guo W, et al. Modified laminoplasty preserving the posterior deep extensor insertion into C2 improves clinical and radiologic results compared with conventional laminoplasty: a meta-analysis. World Neurosurg. 2018;111:157–65.
Umeda M, Sasai K, Kushida T, Wakabayashi E, Maruyama T, Ikeura A, et al. A less-invasive cervical laminoplasty for spondylotic myelopathy that preserves the semispinalis cervicis muscles and nuchal ligament. J Neurosurg Spine. 2013;18(6):545–52.
Kotani Y, Abumi K, Ito M, Sudo H, Takahata M, Nagahama K, et al. Impact of deep extensor muscle-preserving approach on clinical outcome of laminoplasty for cervical spondylotic myelopathy: comparative cohort study. Eur Spine J. 2012;21(8):1536–44.
Kawaguchi Y, Matsui H, Ishihara H, Gejo R, Yoshino O. Axial symptoms after en bloc cervical laminoplasty. J Spinal Disord. 1999;12(5):392–5.
Wang M, Luo XJ, Deng QX, Li JH, Wang N. Prevalence of axial symptoms after posterior cervical decompression: a meta-analysis. Eur Spine J. 2016;25(7):2302–10.
Sakaura H, Hosono N, Mukai Y, Iwasaki M, Yoshikawa H. Medium-term outcome of C3–6 laminoplasty for cervical myelopathy. A prospective study with a minimum 5-year follow-up. Eur Spine J. 2011;20(6):928–33.
Kim J, Lee KS, Kong SW, Kim T, Kim MJ, Park SB, et al. Correlations between electrically quantified pain degree, subjectively assessed visual analogue scale, and the McGill pain questionnaire: a pilot study. Ann Rehabil Med. 2014;38(5):665–72.
González-Fernández M, Ghosh N, Ellison T, McLeod JC, Pelletier CA, Williams K. Moving beyond the limitations of the visual analog scale for measuring pain: novel use of the general labeled magnitude scale in a clinical setting. Am J Phys Med Rehabil. 2014;93(1):75–81.
Bartoshuk LM. Comparing sensory experiences across individuals: recent psychophysical advances illuminate genetic variation in taste perception. Chem Senses. 2000;25(4):447–60.
Prutkin J, Fisher EM, Etter L, Fast K, Gardner E, Lucchina LA, et al. Genetic variation and inferences about perceived taste intensity in mice and men. Physiol Behav. 2000;69(1–2):161–73.
Torrance GW, Feeny D, Furlong W. Visual analog scales: do they have a role in the measurement of preferences for health states? Med Decis Mak. 2001;21(4):329–34.
Inoue T, Soshi S, Kubota M, Marumo K. New method for the quantitative assessment of sensory disturbances in cervical myelopathy: application for neurological level diagnosis. Spine Surg Relat Res. 2020;4(3):216–22.
Inoue T, Soshi S, Kubota M, Marumo K. Efficacy of laminoplasty in improving sensory disturbances in patients with cervical spondylotic myelopathy: a prospective study. World Neurosurg. 2020;134:e581–8.
Acknowledgements
Editorial support in the form of English proofreading was provided by Editage (available at: www.editage.com), a Division of Cactus Communications.
Funding
None.
Author information
Authors and Affiliations
Contributions
SS and MS designed the study; TI and SY collected the data; SY analyzed the data; SS and MS supervised the study; TI wrote the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of The Jikei University School of Medicine (Approval code. 19-076:5007, 19-077:5008, 30-402:9423). All patients were given an overview of the study either orally or in writing, and informed consent was obtained.
Consent for publication
All the patients provided written consent to publish their data in this manuscript.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Inoue, T., Soshi, S., Yamamoto, S. et al. Efficacy of the PainVision apparatus for assessment of axial neck pain after cervical laminoplasty: a prospective study. J Orthop Surg Res 18, 473 (2023). https://doi.org/10.1186/s13018-023-03904-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03904-4