
Abstract
Background
The acetabular fossa often showing the first signs of degeneration, Central acetabular osteophytes (CAO) have been increasingly recognized during hip arthroscopy. The purpose of this study was to investigate the condition of CAO in BDDH hips and compare cotyloid fossa size between the BDDH and the non-BDDH hips on CT images.
Methods
We performed a retrospective analysis of prospectively collected data of hip CT images of FAI or labral injury patients. A 1:2 propensity-score matched observational study comparing the linear length of cotyloid fossa was analyzed. Cotyloid fossa width (CFW) and cotyloid notch width (CNW) were measured on axial images, cotyloid fossa height (CFH) and cotyloid fossa depth (CFD) were measured on coronal images. Within the CAO patients, we performed central acetabular decompression (CAD) and then observed the morphology change in fossa.
Results
Propensity-score matching yielded 61 BDDH hips and 122 non-BDDH hips. BDDH hips had a higher prevalence of CAO and a decreased linear length of cotyloid fossa (CFW, CFH and CNW). In the BDDH group, 33 hips underwent CAD, postoperative CFW, CFH and CNW were significantly increased (p < .001 for all), and had no statistical difference compared with the non-BDDH hips (p = .193, p = .132, p = .421, respectively).
Conclusion
BDDH hips had a significantly higher prevalence of CAO than adequate acetabular coverage hips. After the procedure of CAD, BDDH hips were found to have acetabular parameters (CFW, CFH, CNW) and were restored to that of the control hips.
Similar content being viewed by others


Background
Developmental dysplasia of the hip (DDH) can lead to multiple conditions, such as labral lesions, chondral and ligamentum teres damage, which may contribute to the development of early osteoarthritis [1]. The severity of acetabular dysplasia can be classified into mild, moderate, and severe based on the lateral center edge angle (LCEA). Borderline developmental dysplastic hip (BDDH), with mild acetabular undercoverage, was first described by Fredensborg [2]. BDDH frequently coexists with intra-articular chondrolabral pathology and cam-type femora-acetabular impingement (FAI) [3]. The direct cause of symptoms in BDDH is soft tissue pathology rather than osseous structures abnormality [4]. With the recent advances in hip arthroscopy instrumentation and techniques, the surgical indications have gradually expanded, arthroscopic treatment of borderline dysplasia could provide satisfying benefits [5, 6], but the outcomes could be influenced by some risk factors [7,8,9], such as broken Shenton line, osteoarthritis, and Tӧnnis angle > 15°.
The contact stress distribution is an important role during the development of the human hip. The acetabulum has a cartilage void zone in its central and inferior part, creating the cotyloid fossa; this characteristic gives its articular surface a horseshoe shape and can optimize the contact stress distribution in the hip joint [10]. Despite this key role, the acetabular fossa receives relatively little attention in this discussion of hip pathology. The fossa is filled with the ligamentum teres, synovial membrane, and intra-articular adipose tissue(IAAT), which has adipocytes, fibroblasts, leucocytes, and abundant mast cells [11]. The acetabular fossa also contributes to the lubrication of the hip joint; the fossa is the only intra-articular tissue associated with fluid production, which is essential for cartilage nutrition and load transmission [12].
Lesions of the acetabular fossa are an uncommon cause of hip pain, of which the prevalence of central acetabular osteophytes(CAO) are as frequent as that of femoral head osteophytes in the degenerative changes [13]. CAO are thought to arise from the attachment of transverse acetabular ligament, progressing to involve the entire fossa [14]. CAO can create improper contact between the acetabular cartilage and femoral head by altering the congruency. CAO are significantly associated with the degree of chondral damage, which has been suggested as an early manifestation of osteoarthritis(OA) [15]. Sudsriluk et al. [16] found advanced stage of acetabular fossa change was statistically correlated with the advanced stage of acetabular cartilage degeneration. But CAO can also be seen in patients without advanced degeneration of the hip joint, central acetabular Impingement (CAI) can cause the formation of CAO in femoral-acetabular impingement (FAI) patients [17]. Cotyloid fossa lesions in the central compartment are increasingly being recognized and addressed at the time of routine hip arthroscopy [18, 19]. Arthroscopic acetabular notchplasty is a favorable method of decompressing the central acetabular region [15]. CAO patients treated with central acetabular decompression (CAD) had favorable outcomes at a minimum of 2 years follow-up [18].
At our center, we previously presenting the BDDH patients with labral tear observing that the incidence of cotyloid fossa hyperplasia and osteophyte formation is high. This precipitated an interest in whether hyperplasia of the cotyloid fossa or CAO, might have an association with BDDH. There is a paucity of literature on hyperplasia of cotyloid fossa and even less information on its relation with BDDH. The purpose of this study was to investigate the condition of CAO in the BDDH patients and compare cotyloid fossa size between the BDDH and the non-BDDH patients on CT images.
Methods
Patient selection
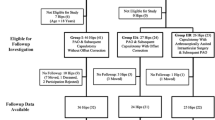
With the consent of the Ethics Committee at our institution, we performed a retrospective analysis of prospectively collected data between July 2019 and January 2020. FAI or labral injury patients, age 16–50 years, were included in this study. Exclusion criteria included: (1) revision surgery; (2) advanced osteoarthritis (Tӧnnis grade ≥ 2); (3) preoperative LCEA < 20° or > 40°; (4) sacroiliac joint disease; (5) history of hip operation; (6) inaccessible preoperative radiographs and incomplete medical record. Patients underwent preoperative anteroposterior (AP) pelvis and Dunn lateral radiography. The LCEA angle, Tӧnnis angle, and Sharp angle were measured on AP pelvis radiographs. The alpha angle was measured on Dunn lateral radiographs. The patients were classified into two groups based on the preoperative LCEA. The BDDH group had an LCEA between 20° and 25°, and the non-BDDH group had an LCEA between 25°and 40°(Fig. 1). The condition of cotyloid fossa hyperplasia and osteophyte formation was made intraoperatively and verified by surgical records and video records. In the BDDH group, patients were further classified into two groups based on the treatment of decompression of CAO.

CONSORT (Consolidated Standards of Reporting Trials) diagram indicating total patient population meeting inclusion and exclusion criteria. FAI: femoral acetabular impingement. BDDH: borderline developmental dysplastic hip
Surgical technique
All hip arthroscopies were performed by one senior author. The patient was placed in the modified supine position on standard hip traction. After the establishment of anterolateral (AL) portal and the midanterior portal (MAP), routine acetabuloplasty and labral repairing were performed. Then hips with CAO requiring CAD were performed in the central compartment. After identification of the morphology of cotyloid fossa, radiofrequency was used to expose the edge of hyperplastic osteophyte without disturbing ligamentum teres, and a long 4.5 mm 133 round bur (Smith & Nephew, Andover, MA) was introduced to remove the sclerotic CAI osteophyte. Capsular plication was performed for all hips after a routine femoroplasty. Figure 2 shows an arthroscopic view of the cotyloid fossa of a left hip with CAO. The intraoperative data were documented including the procedures of the ligamentum teres, labral repair, femoroplasty, and acetabuloplasty.

Intra-articular arthroscopic view of a central acetabular decompression (CAD). A Preoperative. B Postoperative. (A, acetabular cartilage; C, cotyloid fossa; F, femoral head)
CT measurement protocol
Compared to MRI, CT scan is a more accurate imaging modality for bone assessment. At our center, a preoperative CT scan was routinely performed. The GE Light speed 64 slice spiral CT (GE Medical System, Chalfont St Giles, UK) was used for CT examination. The collimator width was 0.625, the pitch was 1.0; the slice thickness of reconstruction was 3 mm, and the interlayer distance was 3 mm. Axial, coronary, and sagittal scanning were routinely performed.
Radiographic linear length measurements were performed using a picture archiving and communication system (PACS; GE Healthcare). The Cotyloid Fossa Width (CFW), Cotyloid Fossa Height (CFH), Cotyloid Fossa Depth (CFD), cotyloid notch Width (CNW) were measured on three or more adjacent CT scan images and the biggest value was selected for these paraments. CFW and CNW were measured on axial images. CFW was measured from the anterior extent to the posterior extent of the fossa. CNW was measured from the anterior extent to the posterior extent of the acetabular notch. CFH and CFD were measured on coronal images. CFH was measured from the top of the cotyloid fossa to the most inferior portion of the bony fossa. CFD was the longest perpendicular distance from the acetabular opening plane to the medial acetabular wall (Fig. 3). In the BDDH group, we further measured CFW, CFH, and CNW on the patient’s postoperative CT. Two orthopedic surgeons measured all parameters under the supervision of a senior radiologist. Both observers were blinded to all clinical data of patients. They performed two measurements one month apart to determine the reliability and obtain clinically meaningful results.

The measurement of the linear length of cotyloid fossa on CT images of the left hip. a and b CFW and CNW were measured on axial images; c CFH and CFD were measured on coronal images. CFW = Cotyloid Fossa Width; CFH = Cotyloid Fossa Height; CFD = Cotyloid Fossa Depth; CNW = cotyloid notch Width
Statistical analysis
A 1:2 propensity-score match based on age, gender, BMI, unilateral or bilateral symptoms was performed using RStudio to control for potential confounding variables in the BDDH group and non-BDDH group. Data for CFW, CFH, CFD, CNW were confirmed to be normal by the Kolmogorov–Smirnov test. The student’s unpaired t-test was performed to compare the differences in CFW, CFH, CFD, CNW between the 2 groups. C-squared test was used to compare categorical data in intraoperative procedures. Paired t-test was used to compare CFW, CFH, and CNW preoperative to postoperative in patients who underwent CAD in the BDDH group. All statistical analyses were performed using SPSS version 26 (IBM, Armonk, NY) with a statistical significance set at p < 0.05.
Results
A total of 471 patients underwent a hip arthroscopy during the study period. We identified 330 patients who met both our inclusion and exclusion criteria. among them, 66 hips with BDDH. Propensity score matching yielded 61 BDDH hips and 122 non-BDDH hips, their mean age was 36.5 years (range 16–50 years). After matching, there were no significant differences in age, sex, BMI, and laterality between the two groups. The preoperative radiographic findings for both groups were described in Table 1. The mean LCEA angle was 23.0° in the BDDH group and 33.2° in the non-BDDH group. The BDDH group also had a larger Tӧnnis angle and Sharp angle, indicating the deficient coverage of acetabular [20].
The BDDH group had a decreased absolute CFW size compared to the control group (29.31 ± 2.51 mm versus 31.15 ± 2.94 mm, p < 0.001). The BDDH group had lower CFH measurements compared with the control group (33.69 ± 3.21 mm versus 34.73 ± 3.14 mm, p = 0.037). There was a significant difference in the height-width ratio between the two groups (1.15 ± 0.11 versus 1.12 ± 0.10, p = 0.044). The BDDH group also had lower CNW measurements compared with the control group (24.96 ± 2.16 mm versus 26.17 ± 2.45 mm, p = 0.01) (Fig. 4). There was no difference in CFD measurements between the two groups (Table 2).

The comparison of the linear length of Cotyloid Fossa. a The white bar in the figure indicates the BDDH group, and the gray bar indicates the non-BDDH group; b. The white bar in the figure indicates preoperative in the BDDH group, and the white bar indicates postoperative in the BDDH group. CFW = Cotyloid Fossa Width; CFH = Cotyloid Fossa Height; CFD = Cotyloid Fossa Depth; CNW = cotyloid notch Width. CAD = central acetabular decompression. BDDH: borderline developmental dysplastic hip
Overall, most of the study population underwent labral repair, femoroplasty, and acetabuloplasty. The BDDH group had a significantly higher number of CAO (54.1% vs 30.3% p = 0.02) and ligamentum teres treatment (p = 0.01). There were no differences in other intraoperative procedures between the groups.
In the BDDH group, 33 hips with underwent CAD, postoperative CFW (31.87 ± 2.14 mm versus 29.29 ± 2.18 mm), CFH (36.27 ± 3.00 mm versus 33.68 ± 3.29 mm) and CNW (25.79 ± 2.15 mm versus 24.84 ± 2.14 mm, p < 0.001 for all) were significantly increased. Patients who underwent CAD also had increased postoperative CFW and CFH compared with non-CAD patients in the BDDH group (p = 0.01, p = 0.02, respectively) (Table 3). Moreover, after the procedure of CAD, the BDDH patients’ postoperative size of CFW, CFH, and CNW had no statistical difference compared with the non-BDDH group (p = 0.193, p = 0.132, p = 0.421, respectively). The intraobserver and interobserver reliability, evaluated by the ICC, was more than 0.85 (0.873–0.924) for each parameter, indicating an acceptable level of reliability.
Discussion
The results showed that the BDDH patients had a high prevalence of CAO. The BDDH group had a decreased linear length of Cotyloid Fossa Width (CFW), Cotyloid Fossa Height (CFH), and cotyloid notch Width (CNW) size compared to the non-BDDH group. In the BDDH group, CFW, CFH, and CNW were significantly increased after the decompression of CAO, the increase after CAD brought the measurements in line with the non BDDH group.
The acetabular fossa is a distinctive area in which osteophytes develops, CT is recommended for assessing the morphology of the acetabular fossa. On an anteroposterior pelvic radiograph, the acetabular fossa extends from the teardrop to an ill-defined area between the medial sourcil and the superior edge of the fovea capitis [11, 20], CAO in advanced osteoarthritis patients can be detected as saber-tooth bony excrescence on cross-sectional imaging, or cause the buttressing effect medial to the head of the femur and yield a double teardrop view in radiographs [21]. But the mild CAO may easily be neglected in the plain radiograph, they are more likely to lie inside the joint, not visible on conventional radiographs.
Previous studies focused mainly on the size of acetabulm and the result of the acetabular fossa size varied considerably. A three-dimensional (3D) CT study described that the dysplastic acetabula were elongated in females but the width was similar in both females and males [22]. Steppacher et al. [23] found dysplastic hips have a decreased size of the lunate surface, a decreased outer acetabular rim, but an increased acetabular fossa. Stephanie et al. [24] measured linear length dimensions of the cotyloid fossa in normal and dysplastic hips on MRI and CT, they found dysplastic acetabula had smaller CFH and CFW compared with normal acetabula. But the sample size was relatively small (20 hips) and they did not report if there were CAO formation in both groups. CAO progressing to involve cotyloid fossa circumferentially and may contribute to the smaller size of cotyloid fossa in the BDDH patients. Our result showed that the BDDH patients had a smaller size of CFW, CFH, and CNW compared with the control group. Moreover, after CAD, there is no statistical difference in CFW, CFH, and CNW size compared with the non-BDDH group.
Our result showed that the prevalence of CAO is high in the BDDH patients compared with the control group. Parth et al. [14] described CAI is associated with femoral head and ligamentum teres damage, they postulated CAI plays an important role in the formation of CAO. Different from FAI, the abnormal contact of CAI happens between cotyloid fossa and adjacent tissue (femoral head and the ligamentum teres), rather than the acetabular margin and the junction of the femoral head and neck. The ligamentum teres is thought to be an important hip stabilizer, especially in dysplasia hips [25]. Ippolito et al. [26] reported a thicker and longer ligamentum teres with wide areas of fibro-cartilaginous metaplasia in dysplastic hips, leading to anterosuperolateral migration of the femoral head, this migration causes distraction of the femoral head and increases the tension on ligamentum teres [14]. Our result showed that the BDDH patients had a significantly higher number of ligamentum teres treatment. Based on previous studies and our result, we conclude that the BDDH patients may have a higher incidence ligamentum teres damage.
The relationship between CAO and OA remains controversial, Varich et al. [27] used “the Saber tooth sign” to describe CAO and considered it as an early manifestation of OA. Asheesh [14] et al. described CAO are associated with degenerative ligamentum teres and femoral head damage arthroscopy. However, a systematic review concluded there is no association between the progression of hip OA and acetabular osteophytes [28]. Although our results showed that CAO is more prevalent in the BDDH patients, a CT study suggested that there is no association between BDDH and the pathogenesis of OA [29]. During the procedure of arthroscopy, we found inflammatory manifestation around IAAT tissue within the fossa. Sampatchalit et al. [16] found gradual acetabular fossa degenerative changes in cadaveric specimens with osteoarthritic changes, included a decrease volume of the adipose tissue, fibrocartilaginous metaplasia, and calcifications. Hence, we need a prognostic study focused on the comparison between patients undergoing CAD and those treated conservatively for CAO.
There are some limitations to our study. First, we did not analyze the differences in cotyloid fossa size between male and female hips. Male acetabula are larger in general; however, we controlled the effects of sex by including even numbers of male and female subjects in the two groups. Second, patient-reported outcomes (PROs) were not reported in this cross-sectional study. Although previous studies had reported the favorable outcomes of CAD at minimum 2-Year follow-up [18]. Markus et al. [17] reported that CAO are associated with an unfavorable outcome after arthroscopy in young FAI patients, and they considered hips with CAO as ‘‘hips at risk.’’ The long-term follow-up data and the long-term effect of CAD need to be further evaluated.
Conclusion
BDDH hips had a significantly higher prevalence of CAO than adequate acetabular coverage hips. After the procedure of CAD, BDDH hips were found to have acetabular parameters (CFW, CFH, CNW) and were restored to that of the control hips.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CAO:
-
Central acetabular osteophytes
- CAD:
-
Central acetabular decompression
- CFW:
-
Cotyloid fossa width
- CNW:
-
Cotyloid notch width
- CFH:
-
Cotyloid fossa height
- CFD:
-
Cotyloid fossa depth
- DDH:
-
Developmental dysplasia of the hip
- BDDH:
-
Borderline developmental dysplastic hip
- FAI:
-
Femoraacetabular impingement
References
Chandrasekaran S, Darwish N, Martin TJ, Suarez-Ahedo C, Lodhia P, Domb BG. Arthroscopic capsular plication and labral seal restoration in borderline hip dysplasia: 2-year clinical outcomes in 55 cases. Arthroscopy. 2017;33(7):1332–40.
Fredensborg N. The CE angle of normal hips. Acta Orthop Scand. 1976;47(4):403–5.
Ida T, Nakamura Y, Hagio T, Naito M. Prevalence and characteristics of cam-type femoroacetabular deformity in 100 hips with symptomatic acetabular dysplasia: a case control study. J Orthop Surg Res. 2014;9:93.
Jo S, Lee SH, Wang SI, Smith B, O’Donnell J. The role of arthroscopy in the dysplastic hip-a systematic review of the intra-articular findings, and the outcomes utilizing hip arthroscopic surgery. J Hip Preserv Surg. 2016;3(3):171–80.
Tang H-C, Dienst M. Surgical outcomes in the treatment of concomitant mild acetabular dysplasia and femoroacetabular impingement: a systematic review. Arthroscopy. 2020;36(4):1176–84.
Ding Z, Sun Y, Liu S, Chen J. Hip arthroscopic surgery in borderline developmental dysplastic hips: a systematic review. Am J Sports Med. 2019;47(10):2494–500.
Hatakeyama A, Utsunomiya H, Nishikino S, Kanezaki S, Matsuda DK, Sakai A, Uchida S. Predictors of poor clinical outcome after arthroscopic labral preservation, capsular plication, and cam osteoplasty in the setting of borderline hip dysplasia. Am J Sports Med. 2018;46(1):135–43.
Uchida S, Utsunomiya H, Mori T, Taketa T, Nishikino S, Nakamura T, Sakai A. Clinical and radiographic predictors for worsened clinical outcomes after hip arthroscopic labral preservation and capsular closure in developmental dysplasia of the hip. Am J Sports Med. 2016;44(1):28–38.
Cvetanovich GL, Levy DM, Weber AE, Kuhns BD, Mather RC, Salata MJ, Nho SJ. Do patients with borderline dysplasia have inferior outcomes after hip arthroscopic surgery for femoroacetabular impingement compared with patients with normal acetabular coverage? Am J Sports Med. 2017;45(9):2116–24.
Daniel M, Iglic A, Kralj-Iglic V. The shape of acetabular cartilage optimizes hip contact stress distribution. J Anat. 2005;207(1):85–91.
Slullitel PA, Coutu D, Buttaro MA, Beaule PE, Grammatopoulos G. Hip preservation surgery and the acetabular fossa. Bone Joint Res. 2020;9(12):857–69.
Field RE, Rajakulendran K. The labro-acetabular complex. J Bone Joint Surg Am. 2011;93(Suppl 2):22–7.
Varich L, Pathria M, Resnick D, Hodler J, Bruser D, Bosch E, Trudell D, Tyson R. Patterns of central acetabular osteophytosis in osteoarthritis of the hip. Invest Radiol. 1993;28(12):1120–7.
Lodhia P, Gui C, Martin TJ, Chandrasekaran S, Suarez-Ahedo C, Domb BG. Central acetabular impingement is associated with femoral head and ligamentum teres damage: a cross-sectional matched-pair analysis of patients undergoing hip arthroscopy for acetabular labral tears. Arthroscopy. 2018;34(1):135–43.
Gupta A, Redmond JM, Hammarstedt JE, Stake CE, Liu Y, Domb BG. Arthroscopic decompression of central acetabular impingement with notchplasty. Arthrosc Tech. 2014;3(5):e555–8.
Sampatchalit S, Chen L, Haghighi P, Trudell D, Resnick DL. Changes in the acetabular fossa of the hip: MR arthrographic findings correlated with anatomic and histologic analysis using cadaveric specimens. AJR Am J Roentgenol. 2009;193(2):W127–33.
Hanke MS, Steppacher SD, Anwander H, Werlen S, Siebenrock KA, Tannast M. What MRI findings predict failure 10 years after surgery for femoroacetabular impingement? Clin Orthop Relat Res. 2017;475(4):1192–207.
Lodhia P, Gui C, Martin TJ, Chandrasekaran S, Suárez-Ahedo C, Walsh JP, Domb BG. Arthroscopic central acetabular decompression: clinical outcomes at minimum 2-year follow-up using a matched-pair analysis. Arthrosc J Arthrosc related surgery. 2016;32(10):2092–101.
Brannon JK. Hip arthroscopy for space-occupying lesions within the acetabular cotyloid fossa. Orthopedics. 2014;37(7):461–5.
Tannast M, Hanke MS, Zheng G, Steppacher SD, Siebenrock KA. What are the radiographic reference values for acetabular under- and overcoverage? Clin Orthop Relat Res. 2015;473(4):1234–46.
Madadi F, Yazdanshenas H, Madadi F, Bazargan-Hejazi S. Double acetabular wall–a misleading point for hip arthroplasty: an anatomical, radiological, clinical study. Int Orthop. 2013;37(6):1007–11.
van Bosse H, Wedge JH, Babyn P. How are dysplastic hips different? A three-dimensional CT study. Clin Orthop Relat Res. 2015;473(5):1712–23.
Steppacher SD, Lerch TD, Gharanizadeh K, Liechti EF, Werlen SF, Puls M, Tannast M, Siebenrock KA. Size and shape of the lunate surface in different types of pincer impingement: theoretical implications for surgical therapy. Osteoarthritis Cartilage. 2014;22(7):951–8.
Pun SY, Hingsammer A, Millis MB, Kim Y-J. Is Increased acetabular cartilage or fossa size associated with pincer femoroacetabular impingement? Clin Orthop Relat Res. 2017;475(4):1013–23.
Philippon MJ, Rasmussen MT, Turnbull TL, Trindade CAC, Hamming MG, Ellman MB, Harris M, LaPrade RF, Wijdicks CA. Structural properties of the native ligamentum teres. Orthop J Sports Med. 2014;2(12):2325967114561962.
Ipplito E, Ishii Y, Ponseti IV. Histologic, histochemical, and ultrastructural studies of the hip joint capsule and ligamentum teres in congenital dislocation of the hip. Clin Orthop Relat Res. 1980;146:246–58.
Mofidi A, Shields JS, Stubbs AJ. Central acetabular osteophyte (saber tooth sign), one of the earliest signs of osteoarthritis of the hip joint. Eur J Orthop Surg Traumatol. 2011;21(2):71–4.
Wright AA, Cook C, Abbott JH. Variables associated with the progression of hip osteoarthritis: a systematic review. Arthritis Rheum. 2009;61(7):925–36.
Irie T, Takahashi D, Asano T, Arai R, Terkawi MA, Ito YM, Iwasaki N. Is There an association between borderline-to-mild dysplasia and hip osteoarthritis? analysis of CT osteoabsorptiometry. Clin Orthop Relat Res. 2018;476(7):1455–65.
Acknowledgements
We thank senior radiologist Wen Chen for her help in CT measurement.
Funding
This work was supported by grants from the National Natural Science Foundation of China (Grant Nos. 82072403, 81902205, 8187090401) and Beijing Natural Science Foundation (Grant No. 7192221).
Author information
Authors and Affiliations
Contributions
Fan Yang and Hong-Jie Huang drafted the manuscript, Zi-Yi He and Yan Xu analyzed and interpreted the patient data, Xin Zhang and Jian-Quan Wang conceived the idea for the article. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study and all experimental protocols were approved by the Ethics Committee of the Peking University Third Hospital (No.M2019193). All methods were carried out in accordance with relevant guidelines and regulations of the Institutional Review Board. Informed consent was obtained from all participants, and all of the radiological data were collected and analyzed anonymously in this study.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper and consent for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, F., Huang, HJ., He, ZY. et al. Central acetabular osteophytes (CAO) are more prevalent in the borderline developmental dysplastic hip (BDDH) patients: a propensity-score matched CT study. J Orthop Surg Res 17, 158 (2022). https://doi.org/10.1186/s13018-022-03056-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-022-03056-x