
Abstract
Purpose
To assess whether the high metabolic region of fluorine-18-fluorode-oxyglucose (18F-FDG) in the primary lesion is the crux for recurrence in patients with nasopharyngeal carcinoma (NPC), to assess the feasibility and rationale for use of biological target volume (BTV) based on 18F-FDG positron emission tomography/computed tomography (18F-FDG-PET/CT).
Methods
The retrospective study included 33 patients with NPC who underwent 18F-FDG-PET/CT at the time of initial diagnosis as well as the time of diagnosis of local recurrence. Paired 18F-FDG-PET/CT images for primary and recurrent lesion were matched by deformation coregistration method to determine the cross-failure rate between two lesions.
Results
The median volume of the Vpri (primary tumor volume using the SUV thresholds of 2.5), the Vhigh (the volume of high FDG uptake using the SUV50%max isocontour), and the Vrecur (the recurrent tumor volume using the SUV thresholds of 2.5) were 22.85, 5.57, and 9.98 cm3, respectively. The cross-failure rate of Vrecur∩high showed that 82.82% (27/33) of local recurrent lesions had < 50% overlap volume with the region of high FDG uptake. The cross-failure rate of Vrecur∩pri showed that 96.97% (32/33) of local recurrent lesions had > 20% overlap volume with the primary tumor lesions and the median cross rate was up to 71.74%.
Conclusion
18F-FDG-PET/CT may be a powerful tool for automatic target volume delineation, but it may not be the optimal imaging modality for dose escalation radiotherapy based on applicable isocontour. The combination of other functional imaging could delineate the BTV more accurately.
Similar content being viewed by others

Introduction
Nasopharyngeal carcinoma (NPC) is a malignant head and neck cancer which is endemic in Southern China and Southeast Asia [1]. In the era of intensity-modulated radiotherapy (IMRT), definitive chemoradiotherapy remains the mainstay of treatment for NPC and results in excellent loco-regional control rates [2]. However, more than 10% patients develop local recurrence after primary treatment [3]. Aggressive salvage treatment for locally recurrent NPC (LR-NPC) may help achieve long-term survival [4]. However, salvage treatment for LR-NPC is complex and relatively limited [5]. Thus, the optimal solution for improving survival is to achieve adequate local control at primary treatment. One of the strategies for improving local control entails escalation of radiotherapy dose [6]. The bottleneck for this strategy is to determine the appropriate tumor volume to prescribe high radiation dose.
Traditional target volume delineation of nasopharyngeal tumors mainly relies on CT and MRI images, which are merely based on anatomical structure [7]. Functional imaging can help determine the biological characteristics and predict the radiotherapy sensitivity in different regions of the tumor; therefore, it has been gradually applied to contouring the gross target volume (GTV) [8, 9]. The development of functional imaging directly led to the emergence of the concepts of biological target volume (BTV) and biological IMRT. Fluorine-18-fluorode-oxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) has evolved from a diagnostic and staging tool to a powerful modality for guiding cancer treatment in radiation oncology, especially for head and neck tumors [10, 11]. Previous studies have suggested that metabolic tumor volume (MTV) based on 18F-FDG-PET/CT can provide supporting information to target volume delineation for dose escalation [12, 13]. PET/CT-guided escalated dose painting, i.e., contouring the BTV in target volume has been proven to confer a considerable survival benefit for patients with LR-NPC [14]. However, there is a paucity of research exploring whether the recurrent lesion is indeed in the PET/CT-guided target volume, which may be supposed to benefit from receiving dose escalation.
Thus, this retrospective cohort study aimed to assess whether the lesion of local recurrence in patients with NPC highly coincides with the volume of high FDG uptake in the primary lesion. In other words, we sought to confirm whether the high metabolic region in the primary lesion is the crux for recurrence or not, so as to retrospectively assess the feasibility and rationale for BTV based on 18F-FDG-PET/CT. We used paired 18F-FDG-PET/CT imaging for primary and recurrent lesion matched by image coregistration method to determine the cross-failure rate between the two lesions of patients with LR-NPC.
Methods and materials
Patient selection
We retrospectively analyzed the medical records of patients with LR-NPC at our cancer center between January 2012 and December 2019. The inclusion criteria were: (1) biopsy-proven primary NPC; (2) confirmed diagnosis of locally recurrent NPC; (3) whole-body 18F-FDG-PET/CT conducted at the time of primary diagnosis and recurrent diagnosis; (4) received radical radiotherapy; (5) availability of complete medical records. The exclusion criteria were: (1) distant metastasis at first diagnosis; (2) second primary carcinoma; (3) severe medical complications; 4) disruption of treatment. Finally, a total of 33 patients were enrolled in the study. The ethics committee of the Fujian Cancer Hospital approved the study (no. YKT2020-011-01).
18F-FDG-PET/CT imaging
All patients underwent 18F-FDG-PET/CT on a Gemini TF 64 PET/CT scanner (Philips, The Netherlands) according to a previously published protocol [12]. Radiochemical purity of 18F-FDG exceeded 95% when manufactured by HM-10 cyclotrons. All patients fasted ≥ 6 h before undergoing 18F-FDG-PET/CT scanning. Serum blood glucose level was 3.9 to 6.5 mmol/L before 18F-FDG was intravenously administered at a dose of 148 to 296 MBq. Patients rested for 40 to 60 min in a dimly lit room before PET/CT scan. CT scanning was performed from the head to the proximal thigh and the scan slice thickness was 4 mm. An iterative reconstruction algorithm based on ordered-subset expectation maximization was used to reconstruct the PET images following the CT-based attenuation correction.
The FDG standardized uptake value (SUV) was measured based on the region of interest (ROI) of tumor, which was calculated as [(decay-corrected activity/tissue volume)/(injected dose/body weight)]. Primary tumors and recurrent lesion were delineated using the SUV thresholds of 2.5 according to previous studies [15, 16]. Maximum SUV (SUVmax) was defined as the value of the most intense voxel within the region of interest. The volume of high FDG uptake was defined within the primary lesion as the 50% isocontour of the SUVmax (SUV50%max).
Treatment
All patients received radical IMRT. The radiotherapy dose and target volume delineation were conducted according to the institutional treatment protocol [17]. The GTV in the primary tumor (GTV-P) or in the involved lymph nodes (GTV-N) identified by clinical, imaging, and endoscopic results were prescribed to receive a total dose of 69.7–70.0 Gy administered in 33–35 fractions [17]. The planning target volume (PTV) was created with an additional 3 mm margin. Homogeneity Index (HI) is an objective tool for analyzing and quantifying the uniformity of dose distribution in the target volume. According to the International Commission on Radiation Units and Measurements (ICRU) report 83, the HI was calculated as \(\frac{D2-D98}{D50}\times 100\) (D2, D98 & D50 are the doses to 2%, 98%, & 50% volume of PTV).
Patients with stage II-IV disease received concurrent chemoradiotherapy based on platinum with or without neoadjuvant chemotherapy, based on the institutional protocol [17].
Follow-up and definition of recurrence
After treatment completion, follow-up was conducted once every 3 months for the first 2 years, once every 6 months in years 3 to 5, and annually thereafter until death or study end. Patients were assessed based on symptoms, physical examination, plasma Epstein-Barr virus (EBV)-DNA copy numbers, fiberoptic endoscopy, nasopharynx and neck contrast-enhanced MRI, chest CT, and abdominal ultrasound to monitor recurrence.
All patients with suspected local recurrence would receive fibreoptic endoscopy and biopsy. For patients without histological verification, the diagnosis of recurrence was confirmed by imaging signs of progression using 18F-FDG-PET/CT and MRI. The time to local recurrence was selected as the primary endpoint, defined as the duration from the date of diagnosis to the date of the first recurrence.
Image coregistration and recurrence mode
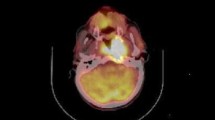
18F-FDG-PET/CT images at the time of primary diagnosis and recurrent diagnosis were registered. For patients with LR-NPC, the primary tumor volume (Vpri) was identified on primary 18F-FDG-PET/CT image (obtained at the time of diagnosis of primary NPC) using the SUV thresholds of 2.5 (Fig. 1-red line) [13]. The recurrent tumor volume (Vrecur) was identified on recurrent 18F-FDG-PET/CT image (obtained at the time when recurrence was first diagnosed) also using the SUV thresholds of 2.5 (Fig. 1-black line). The volume of high FDG uptake in primary tumor (Vhigh) was defined on primary 18F-FDG-PET/CT image using the SUV50%max isocontour (Fig. 1-green line). SUV50%max target was selected according to the definition of BTV based on 18F-FDG-PET/CT [14]. As shown in Fig. 1, the volumes for the primary lesions (Vpri), recurrent lesions (Vrecur) and high FDG uptake lesions (Vhigh) were automatically delineated, respectively, using the AccuContour 3.2 software (www.manteiatech.com).

A 18F-FDG-PET/CT image at the time of primary diagnosis: the red line delineates the volumes with the SUV thresholds of 2.5 and the green line delineates the volumes with 50% of the SUVmax. B 18F-FDG-PET/CT image at the time of diagnosis of recurrence: the black line delineates the volumes with the SUV thresholds of 2.5. C The deformation coregistration 18F-FDG-PET/CT image of primary and recurrent images. (A1,B1,C1) Patient 1: Cross-failure rate of Vrecur∩pri = 8.5%, out-field recurrence; Cross-failure rate of Vrecur∩high = 6.29%, out-side recurrence. (A2,B2,C2) Patient 2: Cross-failure rate of Vrecur∩pri = 47.76%, marginal-field recurrence; Cross-failure rate of Vrecur∩high = 9.68%, out-side recurrence. (A3,B3,C3) Patient 3: Cross-failure rate of Vrecur∩pri = 100%, in-field recurrence; Cross-failure rate of Vrecur∩high = 66.73%, in-side recurrence. (A4,B4,C4) Patient 4: Cross-failure rate of Vrecur∩pri = 97.15%, in-field recurrence; Cross-failure rate of Vrecur∩high = 32.36%, marginal-side recurrence
Using the deformation coregistration method, the ROIs in recurrent images were mapped to the primary images (Fig. 1C), and the volumes of the ROIs for recurrent and primary lesions were calculated. The exact site and extent of each recurrent tumor were then compared with the primary 18F-FDG-PET/CT image using Vpri and Vhigh, respectively, focusing on the superimposition of Vrecur to Vpri and Vhigh. The overlap volume of Vrecur and Vpri was defined as Vrecur∩pri, while the overlap volume of Vrecur and Vhigh was defined as Vrecur∩high.
For the purpose of this study, the percentage of overlap for Vpri (SUV = 2.5) and Vhigh (SUV50%max) to Vrecur (SUV = 2.5) was calculated. The cross-failure rate of Vrecur∩pri was calculated as (Vrecur∩pri/Vrecur)*100%. Analogously, the cross-failure rate of Vrecur∩high was calculated as (Vrecur∩high/Vrecur)*100%. The local recurrence was categorized as occurring inside or outside the Vpri, depending on the position of Vrecur and cross-failure rate of Vrecur∩pri: “in-field recurrence” if the rate was ≥ 95%, “marginal-field recurrence” if the rate was 20%–95%, or “out-field recurrence” if the rate was < 20%. Nevertheless, the cross-failure rate of Vrecur∩high were delimited as: “in-side recurrence” if the rate was ≥ 50%, “marginal-side recurrence” if the rate was 20%–50%, or”out-side recurrence” if the rate was < 20% [18,19,20]. Representative 18F-FDG-PET/CT images of 4 patients was shown in Fig. 1 to better display each category of recurrence.
Statistical analysis
Normality of distribution of continuous variables was assessed using the Shapiro–Wilk test. All normally distributed variables are expressed as mean ± standard deviation, whereas the skewed variables are expressed as median and range. The differences of SUVmax, Vrecur, Vpri and Vhigh between primary and recurrent 18F-FDG-PET/CT were evaluated using the paired t test (for normally distributed variables) or Wilcoxon signed-rank test (for skewed variables) (SPSS 22.0; IBM Corporation).
Results
A total of 33 patients with LR-NPC qualified the inclusion criteria after a median follow up of 50 months (range 18–102). The clinical characteristics of the study population are summarized in Table 1. The average SUVmax of primary tumor was 11.43 ± 5.17, whereas the average SUVmax of recurrent lesions was 7.73 ± 4.06. Vpri, the Vhigh, and Vrecur showed a skewed distribution, and the median volumes were 22.85 (range 4.16–105.09), 5.57 (0–43.07), and 9.98 (0.32–59.46) cm3, respectively.
The details of the TNM stage and dose distribution of the GTV-P for each of the enrolled patients are shown in Table 2. The median HI of the target volume was 0.07 (range 0.02–0.14), which indicated homogenous dose distribution among different radiotherapy plans. The GTV-P had sufficient dose coverage with only 0.39% (range 0–2.52) of the GTV-P obtaining < 95% of prescription dose. A greater part (95.74 ± 3.42%, range 87.98–100%) of GTV-P obtained ≥ 100% of prescription dose. The mean dose of GTV-P was 72.42 ± 0.89 Gy (range 69.34–74.16) while the minimum dose was 64.88 ± 4.12 Gy (range 55.09–69.38) and the maximum dose was 75.93 ± 1.69 Gy (range 71.45–78.38).
The volume of ROIs (include Vpri, Vhigh and Vrecur) and the cross-failure rate with corresponding recurrence mode for all patients are summarized in Table 3. The median percentage of Vhigh /Vpri was 34.14% (range 0–65.82).
Based on the cross-failure rate of Vrecur∩high, the in-side, marginal-side, and out-side recurrence rates were 18.18% (6/33), 42.42% (14/33), and 39.39% (13/33), respectively (Fig. 2A). In other words, approximately 82.82% (27/33) of local recurrent lesions had less than 50% (marginal-side and out-side) overlap volume with the region of high FDG uptake in primary lesions.

Pie chart of the cross-failure rate of Vrecur∩high and Vrecur∩pri. A Cross-failure rate of Vrecur∩high; B Cross-failure rate of Vrecur∩pri
As for the cross-failure rate of Vrecur∩pri, the in-field, marginal-field, and out-field recurrence rates accounted for 24.24% (8/33), 72.72% (24/33), and 3.03% (1/33), respectively (Fig. 2B). Approximately 96.97% (32/33) of local recurrent lesions had more than 20% (in-field and marginal-field) overlap volume with the primary tumor lesions. In addition, the median cross rate of Vrecur∩pri was up to 71.74%.
Discussion
Despite the application of IMRT and advances in treatment technology, local recurrence occurs in some patients with NPC, especially those with advanced disease. The reported local failure rate is up to 15–45% for T4 NPC, which remains an intractable problem [21, 22]. In comparison to the comprehensive treatment strategy involving chemotherapy, immunotherapy, and targeted therapy for patients with metastatic NPC, nasopharyngectomy and reirradiation remain the mainstay of salvage treatment for LR-NPC [21]. However, surgical salvage is only appropriate for early-stage recurrence. As for advanced LR-NPC, reirradiation is still the main treatment option. However, both surgery and reirradiation are associated with a high risk of early or late complications. Thus, exploring the mechanism of radiation resistance and improving the local control rate for primary NPC are key imperatives.
NPC is a highly radiosensitive and radiation dose-dependent disease, and the local control rate increases with improvement of irradiation dose, which is explained by a robust dose-tumor-control relationship [6, 23]. IMRT was shown to improve the dose and conformity of dose distributions in tumor volume by intensity-modulated radiation beams and iterative treatment plan optimization, which resulted in improved local control [24, 25]. However, due to the heterogeneity of biological characteristics and intratumoral radiation resistance, uniform radiotherapy dose may not kill all tumor cells. The inverse treatment planning system of IMRT enables the delivery of a small volume dose boost to target sites in tumor to increase the biologically effective dose (BED) [26]. Thus, identifying the region of high biological activity and resistance is the key to realize biology-guided radiotherapy (BgRT).
18F-FDG-PET/CT imaging can provide compositive information regarding anatomic site, receptor status, and metabolic processes. Currently, 18F-FDG is the most widely used radiopharmaceutical for PET, and its biological behavior is similar to that of glucose. One of the most distinctive biochemical features of malignant tumor cells is the high but inefficient metabolism of glucose, resulting in increased glycolysis [27]. FDG-6-PO4, the end product of FDG trapped in the metabolizing tissues, is a quantitative marker of the rate of glycolysis in the tumor. Compared with other positron-emitting radiotracers, FDG offers distinct advantages of long half-life and automated radiolabeling [27, 28]. In addition, Pisani et al. showed that the recurrence of head and neck carcinoma may originate from the volume with the highest FDG-signal [29]. Up to now, 18F-FDG-PET/CT has been used to identify biological target volumes for planning of radiation dose in non-small-cell lung cancer (NSCLC) and head and neck cancer (HNC) [10, 30].
In a prospective trial, PET/CT was shown to enhance the precision of the radiation therapy target volume definition using the SUV of 2.5 or greater (threshold value of 40%) as compared to CT in NSCLC [30,31,32]. Analogously, Sonay et al. assert that PET/CT can provide benefits in assessed target tumor volume for radiotherapy planning in patients with HNC [33]. In the present study, we also found that the SUV of 2.5 can reasonably guide the contouring of the GTV. Our results show that most of the local recurrent lesions had acceptable overlap volume (the median cross rate of Vrecur∩pri was up to 71.74%) with the primary tumor lesions at the SUV of 2.5. Therefore, 18F-FDG-PET/CT can be considered as a powerful tool for automatic target volume delineation.
The ultimate goal of dose escalation radiotherapy is to improve the local control rate and overcome radiation resistance. The most direct manifestation of radiation resistance is recurrence. Therefore, we infer that the location of local recurrence lesion can be used to define the delineation of the radiotherapy target volume with high biological activity and radiation resistance. Functional imaging modalities such as PET can be more intuitive than structural imaging in reflecting the region of biological malignancy, which also reflect the relationship of metabolism and radiation resistance. Thus, several recent studies have focused on PET/CT-guided dose escalation to delineate the BTV. For the treatment of locally advanced NPC, a randomized trial showed that PET/CT-guided dose escalation radiotherapy is well-tolerated with the SUV of 2.5 and appears to be superior to CT-guided chemoradiotherapy in volume delineation of the biological gross tumor [13]. In addition, in a retrospective study by Liu et al., PET/CT-guided dose-painting IMRT within the isocontour of SUV50%max was found to confer a significant survival benefit in patients with locoregionally advanced NPC [14].
In this study, we chose SUV50%max as the biological target volume because several ongoing clinical trials use the SUV50%max isocontour for dose painting [34, 35]. However, we found that adopting the SUV50%max for dose escalation radiotherapy is inappropriate, because only 18.18% (6/33) patients with LR-NPC showed more than 50% overlap volume with the region of high FDG uptake. We speculate that the treatment failure, especially local recurrence, may be attributable to the persistence of dormant tumor cells and residual tumor cells after local therapy [36]. While the dormant tumor cells are not exactly the region of high FDG uptake, the region of SUV50%max isocontour for dose escalation was not consistent with the local recurrent lesion in our research. In addition, functional imaging modalities include 18F-FDG-PET/CT and MRI-based functional imaging techniques such as diffusion-weighted imaging (DWI) and intravoxel incoherent motion DWI (IVIM-DWI) [7]. PET and DWI are both potential candidates for determining the BTV within the GTV for dose painting and escalation in HNC. For DWI, a low apparent diffusion coefficient (ADC) value indicated tumor presence, so that it was also arranged as a candidate for dose painting [37]. However, Antonetta et al. found that 18F-FDG-PET/CT and DWI provide different functional information, resulting in different biological targets with less overlap [38]. Thus, we believe that 18F-FDG-PET/CT may not be the optimal imaging for dose escalation radiotherapy.
Some limitations of the present study should be acknowledged. Firstly, this was a single-center retrospective study with a small sample size, which may have introduced an element of bias. Secondly, due to the difference of posture between the 18F-FDG-PET/CT examine images and the treatment position, the dose of GTV and possible bias in coregistration could not be directly evaluated; thus the inhomogeneity of the target was ignored. Further prospective trials are required to assess the discrepancy among various functional imaging-guided dose escalation strategies.
Conclusion
Our results suggest that 18F-FDG-PET/CT may be a powerful tool for automatic target volume delineation, but it may not be the optimal imaging modality for dose escalation radiotherapy based on applicable isocontour. The combination of other functional imaging could delineate the biological target volume more accurately.
Availability of data and materials
Data are available upon reasonable request. The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NPC:
-
Nasopharyngeal carcinoma
- IMRT:
-
Intensity-modulated radiotherapy
- LR-NPC:
-
Locally recurrent NPC
- GTV:
-
Gross target volume
- BTV:
-
Biological target volume
- 18F-FDG-PET/CT:
-
Fluorine-18-fluorode-oxyglucose positron emission tomography/computed tomography
- MTV:
-
Metabolic tumor volume
- SUV:
-
Standardized uptake value
- ROI:
-
Region of interest
- PTV:
-
Planning target volume
- HI:
-
Homogeneity Index
- ICRU:
-
International commission on radiation units and measurements
- EBV:
-
Epstein-Barr virus
- BED:
-
Biologically effective dose
- BgRT:
-
Biology-guided radiotherapy
- NSCLC:
-
Non-small-cell lung cancer
- HNC:
-
Head and neck cancer
- DWI:
-
Diffusion-weighted imaging
- ADC:
-
Apparent diffusion coefficient
References
Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80.
Ji MF, Sheng W, Cheng WM, Ng MH, Wu BH, Yu X, et al. Incidence and mortality of nasopharyngeal carcinoma: interim analysis of a cluster randomized controlled screening trial (PRO-NPC-001) in southern China. Ann Oncol. 2019;30(10):1630–7.
Lee AWM, Ng WT, Chan JYW, Corry J, Mäkitie A, Mendenhall WM, et al. Management of locally recurrent nasopharyngeal carcinoma. Cancer Treat Rev. 2019;79: 101890.
Yu KH, Leung SF, Tung SY, Zee B, Chua DT, Sze WM, et al. Survival outcome of patients with nasopharyngeal carcinoma with first local failure: a study by the Hong Kong Nasopharyngeal carcinoma study group. Head Neck. 2005;27(5):397–405.
Poh SS, Soong YL, Sommat K, Lim CM, Fong KW, Tan TW, et al. Retreatment in locally recurrent nasopharyngeal carcinoma: Current status and perspectives. Cancer Commun (Lond). 2021;41(5):361–70.
Teo PM, Leung SF, Tung SY, Zee B, Sham JS, Lee AW, et al. Dose-response relationship of nasopharyngeal carcinoma above conventional tumoricidal level: a study by the Hong Kong nasopharyngeal carcinoma study group (HKNPCSG). Radiother Oncol. 2006;79(1):27–33.
Li M, Zhang Q, Yang K. Role of MRI-based functional imaging in improving the therapeutic index of radiotherapy in cancer treatment. Front Oncol. 2021;27(11): 645177.
Ling CC, Humm J, Larson S, Amols H, Fuks Z, Leibel S, et al. Towards multidimensional radiotherapy (MD-CRT): biological imaging and biological conformality. Int J Radiat Oncol Biol Phys. 2000;47(3):551–60.
Van Baardwijk A, Baumert BG, Bosmans G, van Kroonenburgh M, Stroobants S, Gregoire V, et al. The current status of FDG-PET in tumour volume definition in radiotherapy treatment planning. Cancer Treat Rev. 2006;32(4):245–60.
Troost EG, Schinagl DA, Bussink J, Oyen WJ, Kaanders JH. Clinical evidence on PET-CT for radiation therapy planning in head and neck tumours. Radiother Oncol. 2010;96(3):328–34.
Acuff SN, Jackson AS, Subramaniam RM, Osborne D. Practical considerations for integrating PET/CT into radiation therapy planning. J Nucl Med Technol. 2018;46(4):343–8.
Fei Z, Chen C, Huang Y, Qiu X, Li Y, Li L, et al. Metabolic tumor volume and conformal radiotherapy based on prognostic PET/CT for treatment of nasopharyngeal carcinoma. Medicine (Baltimore). 2019;98(28): e16327.
Wang J, Zheng J, Tang T, Zhu F, Yao Y, Xu J, et al. A randomized pilot trial comparing position emission tomography (PET)-guided dose escalation radiotherapy to conventional radiotherapy in chemoradiotherapy treatment of locally advanced nasopharyngeal carcinoma. PLoS ONE. 2015;10(4): e0124018.
Liu F, Xi XP, Wang H, Han YQ, Xiao F, Hu Y, et al. PET/CT-guided dose-painting versus CT-based intensity modulated radiation therapy in locoregional advanced nasopharyngeal carcinoma. Radiat Oncol. 2017;12(1):15.
Hung GU, Wu IS, Lee HS, You WC, Chen HC, Chen MK. Primary tumor volume measured by FDG PET and CT in nasopharyngeal carcinoma. Clin Nucl Med. 2011;36(6):447–51.
Schwartz DL, Ford EC, Rajendran J, Yueh B, Coltrera MD, Virgin J, et al. FDG-PET/CT-guided intensity modulated head and neck radiotherapy: a pilot investigation. Head Neck. 2005;27(6):478–87.
Chen C, Fei Z, Pan J, Bai P, Chen L. Significance of primary tumor volume and T-stage on prognosis in nasopharyngeal carcinoma treated with intensity-modulated radiation therapy. Jpn J Clin Oncol. 2011;41(4):537–42.
Kong F, Ying H, Du C, Huang S, Zhou J, Chen J, et al. Patterns of local-regional failure after primary intensity modulated radiotherapy for nasopharyngeal carcinoma. Radiat Oncol. 2014;9:60.
Yang X, Ren H, Yu W, Zhang X, Sun Y, Shao Y, et al. Analysis of clinical target volume delineation in local-regional failure of nasopharyngeal carcinoma after intensity-modulated radiotherapy. J Cancer. 2020;11(7):1968–75.
Chen S, Yang D, Liao X, Lu Y, Yu B, Xu M, et al. Failure patterns of recurrence and metastasis after intensity-modulated radiotherapy in patients with nasopharyngeal carcinoma: results of a multicentric clinical study. Front Oncol. 2022;11: 693199.
Chan OS, Sze HC, Lee MC, Chan LL, Chang AT, Lee SW, et al. Reirradiation with intensity-modulated radiotherapy for locally recurrent T3 to T4 nasopharyngeal carcinoma. Head Neck. 2017;39(3):533–40.
Ng WT, Lee MC, Chang AT, Chan OS, Chan LL, Cheung FY, et al. The impact of dosimetric inadequacy on treatment outcome of nasopharyngeal carcinoma with IMRT. Oral Oncol. 2014;50(5):506–12.
Teo PM, Leung SF, Lee WY, Zee B. Intracavitary brachytherapy significantly enhances local control of early T-stage nasopharyngeal carcinoma: the existence of a dose-tumor-control relationship above conventional tumoricidal dose. Int J Radiat Oncol Biol Phys. 2000;46(2):445–58.
Hsiung CY, Yorke ED, Chui CS, Hunt MA, Ling CC, Huang EY, et al. Intensity-modulated radiotherapy versus conventional three-dimensional conformal radiotherapy for boost or salvage treatment of nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2002;53(3):638–47.
Lee N, Xia P, Quivey JM, Sultanem K, Poon I, Akazawa C, et al. Intensity-modulated radiotherapy in the treatment of nasopharyngeal carcinoma: an update of the UCSF experience. Int J Radiat Oncol Biol Phys. 2002;53(1):12–22.
Xiao WW, Huang SM, Han F, Wu SX, Lu LX, Lin CG, et al. Local control, survival, and late toxicities of locally advanced nasopharyngeal carcinoma treated by simultaneous modulated accelerated radiotherapy combined with cisplatin concurrent chemotherapy: long-term results of a phase 2 study. Cancer. 2011;117(9):1874–83.
Jerusalem G, Hustinx R, Beguin Y, Fillet G. PET scan imaging in oncology. Eur J Cancer. 2003;39(11):1525–34.
Gallagher BM, Fowler JS, Gutterson NI, MacGregor RR, Wan CN, Wolf AP. Metabolic trapping as a principle of oradiopharmaceutical design: some factors resposible for the biodistribution of [18F] 2-deoxy-2-fluoro-D-glucose. J Nucl Med. 1978;19(10):1154–61.
Pisani C, Vigna L, Mastroleo F, Loi G, Amisano V, Masini L, et al. Correlation of [18F] FDG-PET/CT with dosimetry data: recurrence pattern after radiotherapy for head and neck carcinoma. Radiat Oncol. 2021;16(1):57.
Bradley J, Thorstad WL, Mutic S, Miller TR, Dehdashti F, Siegel BA, et al. Impact of FDG-PET on radiation therapy volume delineation in non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2004;59(1):78–86.
Erdi YE, Rosenzweig K, Erdi AK, Macapinlac HA, Hu YC, Braban LE, et al. Radiotherapy treatment planning for patients with non-small cell lung cancer using positron emission tomography (PET). Radiother Oncol. 2002;62(1):51–60.
Miller TR, Grigsby PW. Measurement of tumor volume by PET to evaluate prognosis in patients with advanced cervical cancer treated by radiation therapy. Int J Radiat Oncol Biol Phys. 2002;53(2):353–9.
Arslan S, Abakay CD, Sen F, Altay A, Akpinar T, Ekinci AS, et al. Role of PET/CT in treatment planning for head and neck cancer patients undergoing definitive radiotherapy. Asian Pac J Cancer Prev. 2014;15(24):10899–903.
Madani I, Duthoy W, Derie C, De Gersem W, Boterberg T, Saerens M, et al. Positron emission tomography-guided, focal-dose escalation using intensity-modulated radiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;68(1):126–35.
Madani I, Duprez F, Boterberg T, Van de Wiele C, Bonte K, Deron P, et al. Maximum tolerated dose in a phase I trial on adaptive dose painting by numbers for head and neck cancer. Radiother Oncol. 2011;101(3):351–5.
Pantel K, Alix-Panabières C. Liquid biopsy and minimal residual disease - latest advances and implications for cure. Nat Rev Clin Oncol. 2019;16(7):409–24.
Wang J, Takashima S, Takayama F, Kawakami S, Saito A, Matsushita T, et al. Head and neck lesions: characterization with diffusion-weighted echo-planar MR imaging. Radiology. 2001;220(3):621–30.
Houweling AC, Wolf AL, Vogel WV, Hamming-Vrieze O, van Vliet-Vroegindeweij C, van de Kamer JB, et al. FDG-PET and diffusion-weighted MRI in head-and-neck cancer patients: implications for dose painting. Radiother Oncol. 2013;106(2):250–4.
Acknowledgements
None.
Funding
This work was supported by research projects for the Natural Science Foundation of Fujian Province (2020J011124) and Bethune-Translational Medicine Research Fund for Oncology radiotherapy (flzh202126).
Author information
Authors and Affiliations
Contributions
Study concept and design: ZD F, CB C. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: T X, Y F, HL H. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: T X, Y F, ZD F. Study supervision: CB C. All authors read and approved by the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethical Committee of Fujian Cancer Hospital (no. YKT2020-011-01). Patient identifiers such as names were not collected, instead patients were given a numerical identifier. Informed consent was obtained from all participants and for those under 18 years, from a parent or legal guardian. For confidentiality, the patients’ charts were used only within the confines of the records department and only the investigators and study assistant had access to the files.
Consent for publication
The authors affirm that human research participants provided informed consent for publication of the images in Figs. 1a, 1b and 1c.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, T., Feng, Y., Hong, H. et al. Biological target volume based on fluorine-18-fluorode-oxyglucose positron emission tomography/computed tomography imaging: a spurious proposition?. Radiat Oncol 18, 32 (2023). https://doi.org/10.1186/s13014-023-02225-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-023-02225-4