
Abstract
Background
Few patients with pancreatic cancer may be candidates for immediate surgical resection at the initial diagnosis. Even if patients with borderline resectable pancreatic cancer (BRPC), micrometastases may occur before surgery. Therefore, neoadjuvant therapy is vital for improved survival, which has been confirmed in previous studies that neoadjuvant chemotherapy with or without radiotherapy provides superior overall compared with upfront surgery. However, question of whether the addition of radiotherapy to neoadjuvant chemotherapy can improve prognosis compared with chemotherapy alone is a challenging matter. Moreover, most of previous studies only adopted conventional radiotherapy as the neoadjuvant modality though stereotactic body radiation therapy (SBRT) has been proven effective and commonly employed in pancreatic cancer. Also, no studies have evaluated the efficacy of S-1 as the neoadjuvant chemotherapy regimen for BRPC albeit similar prognosis has been found between S-1 and gemcitabine in advanced pancreatic cancer. Hence, the aim of this study is to investigate whether neoadjuvant chemotherapy plus SBRT results in better outcomes compared with neoadjuvant chemotherapy alone and also compare the efficacy of gemcitabine plus nab-paclitaxel with SBRT and S-1 plus nab-paclitaxel with SBRT.
Methods
Patients with biopsy and radiographically confirmed BRPC, no prior treatment and severe morbidities are enrolled. They will be randomly allocated into three groups: neoadjuvant gemcitabine plus nab-paclitaxel, neoadjuvant gemcitabine plus nab-paclitaxel with SBRT and neoadjuvant S-1 plus nab-paclitaxel with SBRT. Standard doses of gemcitabine and nab-paclitaxel are used. The radiation dose of SBRT is 7.5-8Gy/f for 5 fractions. Surgical resection will be performed 3 weeks after SBRT. Artery first approach pancreaticoduodenectomy or radical antegrade modular pancreatosplenectomy will be used for the tumor in the head or body and tail of the pancreas, respectively. The primary endpoint is overall survival. The secondary outcomes are disease free survival, pathological complete response rate, R0 resection rate and incidence of adverse effects.
Discussion
If results show the survival benefits of neoadjuvant chemotherapy plus SBRT and similar outcomes between S-1 and gemcitabine, it may provide evidence of clinical practice of this modality for BRPC.
Trial registration
The study has been registered in ClinicalTrial.gov (NCT03777462).
Similar content being viewed by others

Introduction
Pancreatic cancer has been the fourth cause of cancer mortality in the US with a 5-year survival rate of 3% [1]. In the recent release of cancer statistics of GLOBALCAN database, pancreatic cancer is the seventh leading cause of cancer death in both males and females worldwide [2], and it has been projected that pancreatic cancer will surpass breast cancer as the third cause of cancer death in the European Union [3]. Slightly increasing incidences and cancer mortality of pancreatic cancer were also found in China [4].
Though surgical resection is considered as the only curative intent treatment, the 5-year survival rate of patients with upfront surgery is less than 20% [5]. Therefore, it may be implied that patients could not benefit from surgery alone even with early stage pancreatic cancer at the initial diagnosis, which might be attributable to the micrometastases invisible in the imaging examinations before surgery. As a result, optimal multimodality is in demand for reducing the risk of micrometastases before operations and the incidences of positive or narrow margins, especially for borderline resectable pancreatic cancer (BRPC). Although it has still remained controversial whether neoadjuvant treatment should be performed for BRPC in the guidelines, a recent study has shown survival benefits with neoadjuvant chemoradiation compared with upfront surgery [6].
Due to high intolerance and incidences of adverse effects of FOLFIRINOX in Chinese, other regimens with mild toxicities may be the alternatives. It has been proven that gemcitabine plus nab-paclitaxel contributed to increased survival in pancreatic cancer [7]. And this modality has been included as an option for neoadjuvant chemotherapy in the guideline though there is limited evidence to recommend specific regimens. Moreover, nab-paclitaxel has been confirmed to bind secreted protein acidic and rich in cysteine in the tumor, which resulted in accumulation of chemotherapy drugs and degradation of mesenchymal tissues, thus probably improving the efficacy of chemotherapy. In addition to gemcitabine and nab-paclitaxel, S-1, the prodrug of 5-fluorouracil comprising of tegafur, gimeracil and oteracil, was also an option as the regimen. Previous studies have proven that S-1 was not inferior to gemcitabine in terms of overall survival (OS) rates and disease free survival (DFS) rates with tolerable effects [8, 9]. Hence, nab-paclitaxel based chemotherapy may contribute to synergic effects with S-1.
Furthermore, compared with conventional radiotherapy, the advantages of stereotactic body radiation therapy (SBRT), precise treatment delivery by motion compensation strategies with high doses to target volumes, abrupt dose fall-off outside target volumes, shorter durations and real-time tracking, has rendered SBRT as an appealing technique of radiotherapy, which has been widely employed for pancreatic cancer with high rates of local control and acceptable toxicities. Nevertheless, only conventional radiotherapy was employed in the neoadjuvant treatment in the previous studies.
Therefore, the aim of the study is to compare and evaluate the efficacy of neoadjuvant gemcitabine plus nab-paclitaxel versus gemcitabine plus nab-paclitaxel with SBRT versus S-1 plus nab-paclitaxel with SBRT for BRPC.
Methods
Objectives
The primary objective is to compare the OS of patients receiving neoadjuvant gemcitabine plus nab-paclitaxel versus gemcitabine plus nab-paclitaxel with SBRT versus S-1 plus nab-paclitaxel with SBRT for BRPC. The secondary objective is to compare DFS, pathological complete response rates and adverse effects of the three groups.
Hypothesis
Neoadjuvant chemotherapy plus SBRT is superior to neoadjuvant chemotherapy alone regarding OS, while no significant difference is found between gemcitabine plus nab-paclitaxel with SBRT and S-1 plus nab-paclitaxel with SBRT.
Study design, setting and participants
This is a randomized, prospective, single center and phase III trial. Patients aged above 18, with radiographically and biopsy proven BRPC and without any prior treatment will be screened for eligibility. Therefore, all potential patients would receive fine needle aspirations guided by endoscopic ultrasound. Details about the inclusion and exclusion criteria are shown in Table 1. Additionally, though there are difficulties in defining this borderline resectable pancreatic cancer due to heterogeneity of definitions of this disease entity proposed by different institutions, it is likely that most of studies would employ the definition demonstrated in the NCCN guideline. Therefore, the definition of BRPC is referred to that clarified in the NCCN guideline (Table 2).
Eligible participants would receive personal interviews with physicians for a detailed explanation of the whole study and related treatment. It is mandatory to acquire the written informed consents before the study. Afterwards, patients are required to complete the pretreatment evaluations, including blood routine tests, liver and renal function tests, coagulation function tests, serum tumor marker (CA19–9) tests, enhanced CT and MRI, circulating cell free DNA (cfDNA), circulating tumor cells (CTC), DNA sequences of the specimens from fine-needle aspirations and pancreatic cancer-derived organoid cultures with specimens. In each group, participants will be randomized with a 1:1:1 allocation to receive gemcitabine plus nab-paclitaxel or gemcitabine plus nab-paclitaxel and SBRT or S-1 plus nab-paclitaxel and SBRT. Randomizations will be performed by a computer-generated random numbers table. After completion of the whole chemotherapy, patients will first receive PET-CT to exclude distant metastases and then undergo SBRT. Those with distant metastases will be precluded from the study and receive chemotherapy continuously. Likewise, patients confirmed with distant metastases after chemotherapy and SBRT will receive other aggressive chemotherapy regimens rather than surgical resections (Fig. 1).

Flow diagram of the study
Ethics
The study is performed in accordance with the Declaration of Helsinki. All patients will be enrolled only after comprehensive information concerning the nature, scope, and possible consequences of the clinical trial has been provided to them in an understandable way by the physicians. Written informed consent will be obtained from each patient before the enrolment. During the study, details about the procedures, benefits and risks of chemotherapy, SBRT and surgery will be elucidated for those patients.
All physicians and patients involved in the study will be blinded to the allocations. Only researchers not involved in the study will be responsible for the randomization procedures. Additionally, patients could withdraw from the study at any time for any reason without any consequences. Clinicians are also required to record any adverse effects promptly in case that the treatment may be stopped temporarily or patients may be excluded from the study due to chemotherapy or radiotherapy induced toxicities at the physicians’ discretion. Those dropping out of the study would receive other alternative treatment based on multidisciplinary approaches.
The protocol has been reviewed and approved by the institutional review board of our hospital (CHEC2018–176). The study has also been registered in ClinicalTrial.gov (NCT03777462).
Intervention
All participants are allocated into the three groups randomly. Intravenous administration of gemcitabine (1000 mg/m2) or nab-paclitaxel (125 mg/m2) is initiated on day 1, 8 and 15 during each 4-week cycle, which will repeat for 3 cycles. S-1 is orally administrated at a dose of 80 mg/m2 for 18 days followed by a 10-day rest, which also continues for 3 cycles.
SBRT is performed after completion of the chemotherapy. The protocol of SBRT is similar to our previous studies [10,11,12,13]. Patients are required to be on fasting for 4–6 h before CT simulation. Vacuum bags are used for immobilization during SBRT. SBRT is delivered via Cyberknife, an image-guided frameless stereotactic robotic radiosurgery system (Accuray Corporation, Sunnyvale, California, USA). Before the simulation, fiducials should be implanted adjacent to the tumor guided by endoscopic ultrasound. Therefore, motion management during treatment would be performed by Synchrony® Respiratory Tracking System. A plain CT and an enhanced pancreatic parenchymal CT are performed for radiation treatment planning and target delineations. The scan range includes the whole pancreas, at least 10 cm above and below the tumor, with a slice thickness of 1 .5mm. Gross tumor volume (GTV) is delineated as a radiographically evident gross disease by the enhanced CT acquired from the portal-venous phase. At the discretion of the physician, clinical target volume (CTV) encompassing areas of the potential subclinical disease spread is also designated. In most cases, the CTV equals to GTV. A 2–5 mm expansion margin is included to determine the planning target volume (PTV). When tumors are adjacent to the critical organs, the expansion of GTV should be avoided at this direction. At least 90 % of PTV should be covered by the prescription dose. The prescribed dose is 7.5-8Gy/f for 5 fractions. Dose constraints of normal tissues are referred to the American Association of Physicists in Medicine guidelines in TG-101 [14].
Surgical resection is performed 3 weeks after SBRT. For the surgical approach of the tumor in the head of the pancreas, artery first approach pancreaticoduodenectomy is employed [15,16,17]. Regarding the tumor in the body or tail of the pancreas, radical antegrade modular pancreatosplenectomy (RAMPS) is used [17, 18].
Data collection
The schematic diagram for the timeline of data collections and evaluations of efficacy and safety is shown in Table 3. Pretreatment assessment will be performed and recorded by physicians. After randomizations, efficacy and toxicity of chemotherapy and SBRT and post-operative complications will also be evaluated and recorded by the clinicians. Furthermore, all information about the randomizations and data about the pretreatment assessment and follow-up will be firstly carefully checked by the physicians and re-checked by the researchers not involved in the study to promote data accuracy and completeness. And data entry into the database will be performed by the researchers.
The investigators will not assume any demands, including publishing or reporting of individual patient’s data, especially data required for this clinical trial, until a valid consent has been obtained. Patients’ data would be kept strictly confidential within the study, but their pseudonymous medical records and information would be extracted from the database and reviewed for trial purposes by authorized individuals other than their treating physicians.
Follow-up
Patients are required to receive regular follow-up 1 month, 3 months, 6 months, 1 year and 2 years after surgery. In each follow-up, patients will undergo physical examinations (ECOG, evaluations of symptoms and weight) and laboratory tests (including blood tests, liver and kidney functions, serum tumor biomarker). Imaging examinations will be performed 3 months, 6 months, 1 year and 2 years after surgery to evaluate efficacy. Post-operative complications would be evaluated 1 month and 3 months after surgical resection. Adverse effects of chemotherapy will be assessed according to The Common Terminology Criteria for Adverse Events version 4.03 (CTCAE v4.03). Radiation-induced acute toxicities are adverse effects that occur within 90 days after treatment, and determined by the Radiation Therapy Oncology Group, ‘Acute radiation morbidity scoring criteria’. If patients experience disease progression during follow-up, cfDNA and CTC would be performed to evaluate the tumor burden and identify genetic differences of the tumor cells before and after treatment as far as possible. Disease progression is determined by the Response Evaluation Criteria in Solid Tumors (RECIST) criteria (v1.1).
Outcomes
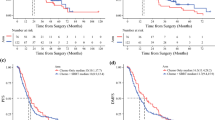
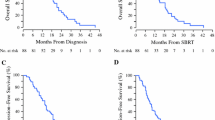
The primary outcome is OS and 1-year and 2-year OS rate. OS is defined as the time interval from the time of surgical resection to the date of all-cause death or the last follow-up.
The secondary outcomes are DFS, pathological complete response rate, R0 resection rate, incidence of adverse effects. DFS is determined as the time interval from the date of surgery to the confirmation of recurrence at any sites or death from any cause, if this occurs before disease progression, or the last follow-up. The definition of pathological complete response is ypT0N0M0, which is no evidence of invasive tumor in the pancreas and the draining lymph nodes at the time of surgery. R0 resection is defined as both clear macroscopic and microscopic margins (≥1 mm).
Sample size and statistical analysis
Assuming, for the gemcitabine plus nab-paclitaxel group, a median 2-year OS rate of about 20%, we target a 10 and 15% relative improvement in 2-year OS rate for the group allocated to S-1 plus nab-paclitaxel with SBRT and gemcitabine plus nab-paclitaxel with SBRT over the gemcitabine plus nab-paclitaxel group, respectively. This would provide approximately 80% power with one-sided α of 0.025. Hence, the maximum number of required patients in each group is 73. Thereafter, when a 10% dropout rate is taken into account, the number of participants in each group is 81.
For the continuous variables, statistical normality will be assessed firstly. Comparisons between these main effects of the three groups will be then performed by analysis of variance or its’2 non-parametric equivalents as appropriate. Categorical data will be compared by Chi-square tests or Fisher’s Exact tests. The OS and DFS curves will be conducted by Kaplan-Meier method. Log-rank test will be employed for comparisons of OS and DFS. Proportional hazard Cox regression adjusted for variables will be used when necessary. Data analysis will be performed on both intention-to-treat and per-protocol basis. All P values will be reported using a significance level of 0.05.
Discussion
It has been long suggested that upfront surgery is given first priority for patients with BRPC or resectable pancreatic cancer based on NCCN guidelines. However, recent studies have clarified the possibility of employment of neoadjuvant chemotherapy with or without radiotherapy, which may provide potential survival benefits. For resectable pancreatic cancer, systemic reviews indicated that neoadjuvant therapy was associated with improved OS [19,20,21]. Likewise, a recent study also identified that total neoadjuvant FOLFIRINOX followed by chemoradiotherapy brought about high rates of R0 resection and prolonged OS and DFS for patients with BRPC [22]. Furthermore, a meta-analysis has shown that neoadjuvant chemoradiotherapy appeared to improve OS compared with upfront surgery [23]. Therefore, it might be implied that neoadjuvant chemoradiotherapy could be an alternative to the surgery-first paradigm for BRPC albeit without high-level evidence. And in 2018 ASCO meeting, a randomized trial reported that preoperative chemoradiotherapy resulted in high rates of R0 resection, longer disease free survival, distant metastases free survival and locoregional recurrence free survival and a trend of superior OS compared with immediate surgery.
Additionally, in most of previous studies, conventional radiotherapy was used as the modality. Usually, radiation doses of 45-54Gy in 1.8–2.0Gy fractions are prescribed leading to a long treatment period, which may result in micrometastases during neoadjuvant therapy. For patients with BRPC, relatively small tumor volumes without obvious invasions of adjacent vessels may provide opportunities for dose-escalation. Hence, SBRT may be an appropriate choice due to its delivery of high biological effective doses within a short period and quick dose fall-off, which may not delay subsequent treatment and provide high pathological complete response rates with acceptable toxicities simultaneously, combined with chemotherapy. Though it might be implied from the previous studies that neoadjuvant chemotherapy with or without radiotherapy could be an alternative to the surgery-first paradigm for BRPC, potential benefits from neoadjuvant chemoradiotherapy still need to be confirmed in prospective studies. Therefore, the BRPCNCC-1 trial, a randomized and prospective study, investigates whether neoadjuvant chemotherapy plus SBRT can prolong survival for BRPC compared with neoadjuvant chemotherapy alone.
Though S-1 has been confirmed effective in pancreatic cancer, especially for Asians, most of studies have only adopted S-1 in advanced pancreatic cancer. No studies have evaluated the efficacy of S-1 in neoadjuvant therapy. Besides, only FOLFIRINOX or gemcitabine plus nab-paclitaxel is recommended in guidelines. As a result, it is necessary to assess whether neoadjuvant S-1 plus nab-paclitaxel with SBRT could be an alternative to neoadjuvant gemcitabine plus nab-paclitaxel with SBRT regarding OS.
Another concern about the trial is the definition of resectability status. Recently, a new international consensus on the definition and criteria of BRPC has been proposed [24]. It has been advocated that tumor biomarker, CA19–9, and performance status should be taken into account in addition to anatomical definition. In this consensus, CA19–9 level of less than 500 U/ml was also a pivotal prerequisite for BRPC. Moreover, patients with resectable pancreatic cancer and ECOG of 2 or more were defined as BRPC. In our study, all included patients have ECOG of less than 2. Additionally, CA19–9 may be a potential factor predictive of OS albeit no inclusion criteria about determinations of the CA19–9 level in our study. Therefore, regarding the two factors, prognosis would be compared between different levels of these factors in the subgroup analyses based on the new biological criteria for BRPC.
In summary, this pilot study, BRPCNCC-1, will investigate whether the addition of SBRT to neoadjuvant chemotherapy results in superior survival compared with neoadjuvant chemotherapy alone and compare the efficacy of S-1 plus nab-paclitaxel combined with SBRT and gemcitabine plus nab-paclitaxel combined with SBRT. The results may provide sufficient evidence for clinical practice of neoadjuvant therapy for BRPC.
Abbreviations
- BRPC:
-
Borderline resectable pancreatic cancer
- cfDNA:
-
Circulating cell free DNA
- CTC:
-
Circulating tumor cells
- CTV:
-
Clinical target volume
- DFS:
-
Disease free survival
- GTV:
-
Gross tumor volume
- OS:
-
Overall survival
- PTV:
-
Planning target volume
- RAMPS:
-
Radical antegrade modular pancreatosplenectomy
- SBRT:
-
Stereotactic body radiation therapy
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018. https://doi.org/10.3322/caac.21492.
Ferlay J, Partensky C, Bray F. More deaths from pancreatic cancer than breast cancer in the EU by 2017. Acta Oncol. 2016;55:1158–60.
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–32.
Winter JM, Brennan MF, Tang LH, D'Angelica MI, Dematteo RP, Fong Y, et al. Survival after resection of pancreatic adenocarcinoma: results from a single institution over three decades. Ann Surg Oncol. 2012;19:169–75.
Jang JY, Han Y, Lee H, Kim SW, Kwon W, Lee KH, et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: a prospective, randomized, open-label, multicenter phase 2/3 trial. Ann Surg. 2018;268:215–22.
Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369:1691–703.
Ueno H, Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Boku N, et al. Randomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST study. J Clin Oncol. 2013;31:1640–8.
Sudo K, Yamaguchi T, Nakamura K, Denda T, Hara T, Ishihara T, et al. Phase II study of S-1 in patients with gemcitabine-resistant advanced pancreatic cancer. Cancer Chemother Pharmacol. 2011;67:249–54.
Zhu X, Li F, Shi D, Ju X, Cao Y, Shen Y, et al. Health-related quality of life for gemcitabine and nab-paclitaxel plus radiotherapy versus gemcitabine and S-1 plus radiotherapy in patients with metastatic pancreatic cancer. Cancer Manag Res. 2018;10:4805–15.
Zhu X, Li F, Ju X, Shen Y, Cao Y, Cao F, et al. Prediction of overall survival after re-irradiation with stereotactic body radiation therapy for pancreatic cancer with a novel prognostic model (the SCAD score). Radiother Oncol. 2018;129:313–8.
Zhu X, Shi D, Li F, Ju X, Cao Y, Shen Y, et al. Prospective analysis of different combined regimens of stereotactic body radiation therapy and chemotherapy for locally advanced pancreatic cancer. Cancer Med. 2018. https://doi.org/10.1002/cam4.1553.
Zhu X, Li F, Liu W, Shi D, Ju X, Cao Y, et al. Stereotactic body radiation therapy plus induction or adjuvant chemotherapy for early stage but medically inoperable pancreatic cancer: a propensity score-matched analysis of a prospectively collected database. Cancer Manag Res. 2018;10:1295–304.
Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, et al. Stereotactic body radiation therapy: the report of AAPM task group 101. Med Phys. 2010;37:4078–101.
Hirono S, Kawai M, Okada KI, Miyazawa M, Shimizu A, Kitahata Y, et al. Mesenteric approach during pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. Ann Gastroenterol Surg 2017;1:208–218.
Hirono S, Kawai M, Okada KI, Fujii T, Sho M, Satoi S, et al. MAPLE-PD trial (mesenteric approach vs. conventional approach for pancreatic Cancer during Pancreaticoduodenectomy): study protocol for a multicenter randomized controlled trial of 354 patients with pancreatic ductal adenocarcinoma. Trials. 2018;19:613.
Chun YS. Role of radical antegrade modular pancreatosplenectomy (RAMPS) and pancreatic cancer. Ann Surg Oncol. 2018;25:46–50.
Strasberg SM, Drebin JA, Linehan D. Radical antegrade modular pancreatosplenectomy. Surgery. 2003;133:521–7.
Stessin AM, Meyer JE, Sherr DL. Neoadjuvant radiation is associated with improved survival in patients with resectable pancreatic cancer: an analysis of data from the surveillance, epidemiology, and end results (SEER) registry. Int J Radiat Oncol Biol Phys. 2008;72:1128–33.
Gillen S, Schuster T, Meyer Zum Büschenfelde C, Friess H, Kleeff J. Preoperative/neoadjuvant therapy in pancreatic cancer: a systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010;7(4):e1000267.
Artinyan A, Anaya DA, McKenzie S, Ellenhorn JD, Kim J. Neoadjuvant therapy is associated with improved survival in resectable pancreatic adenocarcinoma. Cancer. 2011;117:2044–9.
Murphy JE, Wo JY, Ryan DP, Jiang W, Yeap BY, Drapek LC, et al. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: a phase 2 clinical trial. JAMA Oncol. 2018;4:963–9.
Versteijne E, Vogel JA, Besselink MG, Busch ORC, Wilmink JW, Daams JG, et al. Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer. Br J Surg. 2018;105:946–58.
Isaji S, Mizuno S, Windsor JA, Bassi C, Fernández-Del Castillo C, Hackert T, et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology. 2018;18:2–11.
Acknowledgements
We appreciate Dr. Jiuhong Chen for her precise comments on the revisions of the protocol and article.
Funding
None.
Availability of data and materials
Not applicable.
Author information
Authors and Affiliations
Contributions
JG, ZHJ and GSW designed the study and revised the manuscript. GSZ and ZXF drafted the manuscript. ZXF is responsible for treatment plans of radiotherapy. GSZ, ZXF and SHX perform the follow-up. GSZ, GSW, SHX and JG perform the surgery. CK and BY are responsible for patients’ imaging examinations. JH carry out the pathological examinations. WKX perform the fine needle aspirations guided by endoscopic ultrasound. GSZ and GSW perform the statistical analyses. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The protocol has been reviewed and approved by the institutional review board of our hospital (CHEC2018–176). The study has also been registered in ClinicalTrial.gov (NCT03777462).
Consent for publication
The consents for publication of data have been obtained from patients.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Gao, S., Zhu, X., Shi, X. et al. Comparisons of different neoadjuvant chemotherapy regimens with or without stereotactic body radiation therapy for borderline resectable pancreatic cancer: study protocol of a prospective, randomized phase II trial (BRPCNCC-1). Radiat Oncol 14, 52 (2019). https://doi.org/10.1186/s13014-019-1254-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-019-1254-8