
Abstract
Background
Our team has developed a decision aid to help pregnant women and their partners make informed decisions about Down syndrome prenatal screening. However, the decision aid is not yet widely available in Quebec’s prenatal care pathways.
Objective
We sought to identify knowledge translation strategies and develop an implementation plan to promote the use of the decision aid in prenatal care services in Quebec, Canada.
Methods
Guided by the Knowledge-to-Action Framework and the Theoretical Domains Framework, we performed a synthesis of our research (11 publications) on prenatal screening in Quebec and on the decision aid. Two authors independently reviewed the 11 articles, extracted information, and mapped it onto the Knowledge-to-Action framework. Using participatory action research methods, we then recruited pregnant women, health professionals, managers of three prenatal care services, and researchers to (a) identify the different clinical pathways followed by pregnant women and (b) select knowledge translation strategies for a clinical implementation plan. Then, based on all the information gathered, the authors established a consensus on strategies to include in the plan.
Results
Our knowledge synthesis showed that pregnant women and their partners are not sufficiently involved in the decision-making process about prenatal screening and that there are numerous barriers and facilitators of the use of the decision aid in clinical practice (e.g., low intention to use it among health providers). Using a participatory action approach, we met with five pregnant women, three managers, and six health professionals. They informed us about three of Quebec’s prenatal care pathways and helped us identify 20 knowledge translation strategies (e.g., nurse discusses decision aid with women before they meet the doctor) to include in a clinical implementation plan. The research team reached a consensus about the clinical plan and also about broader organizational strategies, such as training healthcare providers in the use of the decision aid, monitoring its impact (e.g., measure decisional conflict) and sustaining its use (e.g., engage key stakeholders in the implementation process).
Conclusion
Next steps are to pilot our implementation plan while further identifying global strategies that target institutional, policy, and systemic supports for implementation.
Similar content being viewed by others

Background
Screening for Down syndrome is becoming a part of routine prenatal care in a growing number of countries worldwide. In the province of Quebec, Canada, the provincial Trisomy 21 Prenatal Screening Program covers maternal serum screening tests and amniocentesis diagnostic tests for all pregnant women with public health insurance [1]. Other tests, such as nuchal translucency ultrasounds, are publicly covered in some circumstances [1]. Participation in this program is voluntary and pregnant women must decide whether or not to take these tests.
To help women and their partners make informed decisions consistent with the best available evidence and their preferences and values, health professionals can engage them in shared decision making (SDM) [2, 3]. One effective way to facilitate SDM is through the use of decision aids [4, 5]. Decision aids are tools (printed or digital) that can be used at point-of-care to provide information about a health condition, treatment options, and probabilities about possible benefits and harms [6, 7]. They help patients actively engage in decisions about their care and make choices that better match their values and preferences [5, 8]. In the context of genetic testing, pregnant women experience less decisional conflict [5, 9] and decisional regret [5] after using a decision aid. Yet, despite the proven benefits of decision aids, their use in routine clinical practice is limited [10, 11] and particularly rare in the context of prenatal care and screening for Down syndrome [12, 13].
Recently, our team developed and validated a decision aid for decisions about Down syndrome prenatal screening that respects the 16 criteria of the International Patient Decision Aid Standards (IPDAS) [14,15,16]. However, this decision aid has not yet been implemented in prenatal care settings. Given the many professional, patient-related, and contextual barriers to implementing SDM in routine clinical practice [17, 18], we felt it was necessary to develop a robust plan to promote adoption of the decision aid by the province’s prenatal services. Implementation planning is an important but understudied part of the process of implementing evidence-based practices [19]. The aim of this study was thus to create a theory-informed approach to developing an implementation plan to support the adoption of a patient decision aid for Down syndrome prenatal screening. Building on our previous work in this area and in consultation with stakeholders, we planned to identify the knowledge translation (KT) strategies needed to overcome barriers to implementing the decision aid in three of Quebec’s prenatal care pathways.
Methods
Conceptual framework
We used two conceptual frameworks from the field of implementation science: the Knowledge-to-Action (KTA) Framework [20, 21] and the Theoretical Domains Framework [22]. The KTA Framework describes the knowledge translation (KT) process as iterative, complex, and made up of two distinct but related components: knowledge creation and knowledge application (the action cycle). Knowledge creation is the production of knowledge that can be synthesized, refined, and converted into useful tools for end-users. The action cycle is based on planned action theories and consists of seven main phases: (1) identifying, reviewing, and selecting the knowledge to implement; (2) adapting or customizing the knowledge to the local context; (3) assessing the determinants of knowledge use; (4) selecting, tailoring, and implementing KT strategies; (5) monitoring KT strategies and knowledge uptake: (6) evaluating outcomes: and (7) determining strategies for sustained knowledge use [20, 23].
The Theoretical Domains Framework (TDF) provides a theoretical lens through which to understand factors influencing implementation and the determinants of behavior [24]. It represents a synthesis of 33 theories of behavior and behavioral change and features 84 theoretical constructs clustered into 14 domains. It has been used to explore barriers and facilitators to the adoption of evidence-based practices and to identify strategies to support implementation [24, 25]. Taken together, these theoretical frameworks provide guidance on the elements and strategies to include in an implementation plan.
Study design and context
We performed a synthesis of our previous research on Down syndrome prenatal screening in Quebec. The synthesis included a review of articles related to several research projects, notably the CanGenTest and PEGASUS (PErsonalized Genomics for prenatal Aneuploidy Screening USing maternal blood) projects. The latter was an independent study to validate the performance and utility of this new genetic screening in Quebec’s public clinical laboratories and to enable pregnant women and their partners together with health professionals to make informed decisions about prenatal screening choices [26]. The funding for these projects was provided by a variety of federal and provincial agencies from 2008 until 2017.
We identified stakeholders involved in any aspect of the prenatal screening process: pregnant women, prenatal service health professionals and managers, and PEGASUS prenatal care researchers. Using the Participatory Action Research (PAR) approach, we asked the stakeholders to identify strategies and co-design an implementation plan specifically for the clinical context of prenatal care. PAR is a systematic inquiry, in collaboration of those affected by the issue being studied, for the purposes of education and taking action or effecting social change [27]. The stakeholders provided us with information not collected in our previous studies on the current organization of prenatal services in Quebec and on how our KT interventions could be tailored to the different clinical pathways. The stakeholders helped us identify the types of prenatal service in which most pregnant women in Quebec receive their care. Ethics approval for the PAR phase of the study was obtained from the research ethics boards of the Centre de Santé et de Services Sociaux de la Vieille-Capitale (#2013-2014-29) and the CHU de Quebec (#B14-02-1929).
We used the Standards for Reporting Implementation Studies (StaRI) checklist to report this study [28].
Data collection
For the knowledge synthesis, two authors (TTA, MM) selected 11 articles published as part of our previous research. Articles were eligible if they related to decision-making or the implementation of SDM or decision aids in decisions about Down syndrome prenatal screening. The articles described results from: (a) a systematic review of the decisional needs of participants in Down syndrome prenatal testing [29], (b) a cross-sectional study examining the levels of SDM and decisional conflict during routine consultations about Down syndrome prenatal testing [13, 30, 31], (c) an environmental scan of decision aids for Down syndrome prenatal screening [32], (d) two mixed-methods studies examining pregnant women’s [33,34,35] and health professionals’ [36, 37] intentions to use a decision aid for Down syndrome prenatal screening, and (e) a theory-based qualitative study examining women’s perceptions of strategies to enhance the use of a decision aid for Down syndrome prenatal screening [38].
For the PAR phase of the study, we recruited managers knowledgeable about the organization of prenatal services in the province, end-users of our decision aid (pregnant women and health professionals), and researchers with expertise in Down syndrome prenatal screening. Prenatal service managers were recruited from three clinical sites in Quebec City: an academic family medicine clinic, a university hospital obstetrics/gynecology department, and a birthing center. One manager from each site was asked to provide details about the clinical pathways of pregnant women in their service. Meetings lasted 30 min and were conducted at the managers’ places of work.
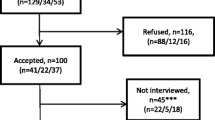
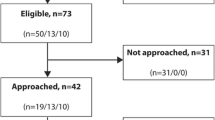
With support from these managers, we then recruited pregnant women who had experience with each clinical pathway. Women were eligible if they were at least 18 years old, were no less than 16 weeks pregnant or had just given birth, had already made their decision about Down syndrome prenatal screening for their current pregnancy, and were able to read and speak French. We excluded women who had participated in previous phases of the PEGASUS project related to SDM, who presented a high-risk pregnancy (e.g., preeclampsia, gestational diabetes, multiple pregnancy), and whose delivery date corresponded with the dates of data collection. We drafted an initial list of 15 women recruited from each location and purposely selected five women to be partners in our study. The women were consulted individually at our research center during meetings lasting 30–45 min. This consultation focused on validating results of our previous study on strategies to enhance decision aid use by pregnant women [38], cross-checking their personal clinical pathway with the clinical pathways described by prenatal service managers, and eliciting their ideas for generating knowledge KT strategies.
We next approached health professionals who were staff members of the same three clinical sites. Two family physicians, a gynecologist, a midwife, a nurse, and a neonatologist agreed to participate. Meetings with the professionals focused on their perceptions of the appropriate strategies for promoting decision aid adoption in the different prenatal care pathways. Finally, we consulted four prenatal care researchers with longstanding involvement in the PEGASUS to explore their views on the KT strategies. The consultations with health professionals and researchers took place individually at their places of work and lasted approximately 30 min.
All consultations were conducted by one of the authors who was trained in public health and had experience in conducting qualitative research and who took detailed notes during meetings with stakeholders.
Data analysis
Two authors (TTA, MM) reviewed the articles included in the knowledge synthesis. MM extracted barriers and facilitators from the 11 studies and categorized them in the TDF domains. Extraction and categorization were then verified by TTA. We chose to proceed in this way because both authors had prior knowledge of the studies and indeed had been involved in conducting several of them. Also, categorization was facilitated by the fact that five of the 11 studies used the TDF or a conceptual framework related to it. Following this, the two authors met to discuss any differences in interpretation, validated categorization, and established a consensus on the most relevant strategies for addressing barriers and facilitators, drawing on strategies found in our environmental scan and suggested in our stakeholder consultations.
For the PAR, TTA transcribed notes taken during interviews with stakeholders (pregnant women, health professionals, researchers, and clinical managers). Transcripts were categorized into themes according to the type of information sought (portrait of the clinical pathway, KT strategies generated, and views on KT strategies) and analyzed manually. TTA drafted a summary of the feedback from meetings with stakeholders. Then, authors discussed the summary and established a consensus on information that should be taken into account in the selection of KT strategies for the design of the implementation plan.
Results
In the sections that follow, we use the elements of the KTA framework to describe what we learned about implementing a decision aid for prenatal screening from our knowledge synthesis and from our PAR study, and present the KT strategies identified. First, the “Knowledge Creation” section describes the knowledge we have acquired (through primary studies and reviews) and tools/products we have developed over the past 10 years. Second, we identify strategies for a plan to implement the decision aid in three clinical prenatal care contexts (steps 1–4 of the Action Cycle). Third, we identify broader-scale strategies for expanding/scaling up the implementation plan throughout the province of Quebec (steps 5–7 of the Action Cycle).
Knowledge creation
Knowledge inquiry
Primary studies conducted by our team helped us generate valuable knowledge about the nature of decision-making about prenatal screening for Down syndrome and about the factors that influence decision aid adoption by pregnant women and health professionals. In particular, an initial cross-sectional study examining SDM for prenatal screening decisions in routine consultations revealed that women were rarely involved in these decisions and that any fears or concerns they may have had were rarely discussed [13, 31]. However, both women and health professionals were willing to engage in SDM, especially when they had a positive outlook on SDM and it was valued by significant others [31]. Subsequent mixed-methods and qualitative studies revealed that most pregnant women showed a similarly strong willingness to use decision aids to support their prenatal care decisions, though about a third (≈30%) were ambivalent [34]. Using the Theoretical Domains Framework as a guide, our team found that women’s intentions to use decision aids were influenced by a range of factors, including their attitudes and beliefs, their knowledge and skill levels, the nature of the decision aid itself, and the context in which they encountered it [34, 35]. Health professionals also generally showed strong intentions to use decision aids but this varied by type of professional, with midwives having the highest intentions and obstetrician/gynecologists having the lowest [37]. Professionals’ intentions to use decision aids were similarly influenced by many factors, including their attitudes and beliefs about the decision aidand their own professional identity, the compatibility and availability of the decision aid within their practice, and the use of decision aids by their peers [36, 37]. These studies thus reinforced the need for a multifaceted implementation approach that targeted pregnant women, their care providers, and the decision-making environments. The studies also shed light on potential facilitators and barriers to decision aid adoption that could be taken into consideration in the implementation plan (see below).
Knowledge synthesis
Our team had also conducted two knowledge syntheses to aggregate existing evidence on topics related to Down syndrome prenatal screening. From a first systematic review on the decisional needs of pregnant women, their partners, and health professionals [29], we learned that in some cases participants found prenatal screening decisions to be difficult because of anxiety or fear, lack of information available about risks and benefits, and the possibility that they would have to make decisions that contradicted their personal values. In other cases, prenatal screening had not been presented to the women as a topic to discuss but rather as a part of routine care without any decision needed. Decision-making was made easier when women had better access to information, personal or professional support, and were clear about their personal values around pregnancy and childbirth. This review also highlighted the important role of women’s partners, who often participate in decisions and can be important sources of support or pressure in decision-making. In a second knowledge synthesis, an environmental scan was performed to identify publically available decision aids that focus on prenatal screening or diagnosis of Down syndrome [32]. We identified 20 decision aids, including five for prenatal screening only, three for prenatal diagnosis, and 12 that covered both screening and diagnosis. However, none of them met all the IPDAS criteria to qualify as high-quality, effective decision aids, indicating a clear need for new knowledge tools on these topics.
Knowledge tools/products
Following the environmental scan, we developed a decision aid to help pregnant women and their partners make screening decisions [32]. This decision aid was adapted from another identified in the scan that had scored relatively well on the IPDAS criteria (10 out of 16 criteria) and that seemed relevant to the Quebec context. The new decision aid met all minimal IPDAS criteria and was available in French and English. It was also the foundation for two other products, namely a video illustrating the use of an SDM approach in the context of Down syndrome prenatal screening (in which the decision aid appears) and an online training program for health professionals to improve their SDM skills in this context.
Strategies for a clinical implementation plan
Action cycle step 1: identify the problem and the knowledge to be implemented
Making decisions about Down syndrome screening can be challenging given its important consequences for the child and family. Yet pregnant women and their partners may not be involved in the decision-making process, may lack information to help inform their decisions, or in some cases may not even be informed there is a decision to make. In 2017, the Quebec government published an evaluation that confirmed the findings of our research projects [39]. Among women participating in the provincial Trisomy 21 Prenatal Screening Program, only 61% of women received written materials about the tests, 34% received no information about the diagnostic amniocentesis test and its risks, and 50% received no information on the options of pursuing or terminating their pregnancy in the event of prenatal diagnosis of Down syndrome [39]. When women lack information about the options, not only are they deprived of their right to informed consent [39], but there is a high risk that they will experience decisional conflict [40] and decisional regret [30]. We thus identified the main problem as an absence of SDM and decision support for people facing Down syndrome screening decisions, prompting us to develop the new decision aid for use in prenatal services. The barriers to decision aid adoption in routine care identified in our research also highlighted the need for a multi-faceted plan for supporting implementation that would take environmental context, policies, training, and health system organization into account.
Action cycle step 2: adapt knowledge to local context
Our consultations with managers, health professionals, researchers, and pregnant women during the PAR process shed important light on the contexts of prenatal care in Quebec and the different clinical pathways followed by pregnant women (Table 1). The stakeholders from the various prenatal care services helped us understand how to adapt knowledge to these different clinical contexts. Implementation of the decision aid would be more straightforward in birthing centers because midwives expressed the highest intention to use it, their consultations were generally longer, and there was more flexibility in the care pathway to allow women and their partners to reflect on the decision. In contrast, implementing the decision aid among obstetrician/gynecologists in a hospital setting would take more finely tuned strategies as they had less favorable attitudes towards decision aids, their consultations were shorter, and they were less surrounded by other professionals who could assist with decision support (Fig. 1).

General training on SDM and decision aid use for all prenatal care providers. Selecting and training a decision coach in each prenatal care service. Shared decision making in the context of Down syndrome
Action cycle step 3: assess barriers/facilitators to knowledge use
Barriers and facilitators to the adoption of decision aids in prenatal care were initially identified through the knowledge synthesis and through the PAR consultations. We categorized them in our implementation plan according to their TDF domains (Table 2). We selected KT strategies that might be taken to address them, identified in the next step, to these domains. For instance, for women dealing with anxiety, in the TDF domain “emotion,” the strategy might be to have a decision coach accompany women when they use the decision aid and be reassured that their questions will be answered by a health professional.
Action cycle step 4: select, tailor, and implement interventions
The selection of further KT strategies was informed by both the knowledge synthesis and the PAR consultations. Among the studies in our knowledge synthesis was a qualitative study that explored pregnant women’s views on strategies for promoting the use of a decision aid for Down syndrome prenatal screening [38]. This study revealed several strategies that women perceived as relevant and acceptable for supporting decision aid adoption, including (1) using credible sources (e.g., receiving it directly from their prenatal care providers or retrieving it from hospital or government websites), (2) goal setting around the use of the decision aid (e.g., having professionals clearly explain its purpose), (3) ensuring decisional and social support (e.g., supporting women through the decision-making process, answering their questions, including women’s partners in the decision), (4) demonstrating the use of the decision aid (e.g., showing women the video illustrating its use), (5) modifying the environment in which it is to be used (e.g., ensuring its availability for clinicians and placing posters and messages on screens in the waiting rooms of clinics encouraging its use).
We selected an initial set of KT strategies, including those from step 3. We then invited our stakeholders (pregnant women partners, healthcare professionals, and PEGASUS project members) for a second round of consultation during which they gave their feedback on the strategies and proposed implementation plan. Some of the strategies applied to all three prenatal contexts while others were tailored to each of the different prenatal care contexts. The final set of KT strategies is presented in Table 2 and the final plan is presented in Fig. 1. Based on the Effective Practice and Organisation of Care (EPOC) taxonomy, we used the strategies to propose an implementation plan for shared decision making in the context of Down syndrome prenatal screening (Table 3) [41].
While our initial focus was on strategies appropriate for an implementation plan at the organizational level of clinical prenatal care pathways, the following strategies identified in our knowledge synthesis are also appropriate for a long-term province-wide implementation plan.
Strategies for a long-term province-wide implementation plan
Action cycle step 5: monitor knowledge use
Monitoring knowledge use in real time will be critical in order to determine whether our KT strategies are sufficient to bring about desired changes, i.e., whether women and their prenatal care providers are adopting the decision aid and engaging in SDM. As a research team, we identified several low-cost monitoring strategies to integrate into the clinical implementation plan, including (1) monitoring the distribution of paper copies of the decision aid and the number of online downloads of the decision aid, (2) monitoring the distribution of posters to the different clinical settings, and (3) tracking the number of professionals completing the online and in-person training on SDM and decision aids. In select pilot implementation sites, clinician-patient encounters could be video recorded to examine the adoption and fidelity of decicion aid use. Using multiple data sources over longer time periods is also necessary to explore the sustainability of their use in different clinical care contexts (Table 4).
Action cycle step 6: evaluate outcomes
In Quebec, more than 80,000 births were registered for the year 2018 [42]. Reliable statistics on the number of women who undergo Down syndrome prenatal screening each year are not available, likely because of the mix of public and private testing options. However, integration of the prenatal screening decision aid into clinical practice is not intended to change screening rates but rather to increase women’s involvement in decision-making and support them in achieving informed, shared decisions that reflect their values and preferences. Our previous studies in this area shed light on a variety of relevant outcomes for evaluating the success of our KT strategies: first, assessing behavioral intentions regarding adoption among women and healthcare providers [31, 34, 37]; second, measuring the influence of decision aid adoption on women’s involvement in prenatal screening decisions and in their experiences of decisional conflict [43]; third, measuring women’s knowledge of their options, their satisfaction with their decision and the extent to which it aligns with their values and preferences [44,45,46]; and finally, assessing the involvement of women’s partners in prenatal care decisions [46]. In a pilot phase, we will measure all these outcomes and demonstrate the impact of the implementation plan on adoption of the prenatal screening decision aid at the organizational level, see Table 4.
Action cycle step 7: sustain knowledge use
The notion of sustaining evidence-based practices over time has received growing attention in recent years [47,48,49], and we conceived our implementation plan with sustainability in mind. It includes six sustainability strategies. First, engagement of key stakeholders in the implementation process so that they share responsibility for increasing the involvement of women and their partners in their prenatal care. Second, the decision aid will be permanently and freely available through multiple platforms and its content and design will be repeatedly reviewed and updated to ensure it continues to be relevant. Third, our project steering committee plans to work with policymakers to promote the decision aid as an integral part of the province’s prenatal screening program. Fourth, our training strategies use low-cost existing online training modules that have been tested in a variety of clinical contexts. Fifth, our team continues to work with health organizations to provide training on interprofessional approaches to SDM, including on the use of this decision aid. Sixth, we plan to work with partners in hospital settings to train practising professionals as prenatal decision coaches, including in the use of this decision aid, using train-the-trainer models to mitigate potential staff turnover. Finally, to ensure ongoing and sustainable outcomes evaluation, we will work with stakeholders to embed further measures and indicators within the clinical and information systems used by providers (Table 4).
Discussion
The use of decision aids to support shared decisions about Down syndrome prenatal screening is not a widespread practice in Quebec. Our team aimed to change this. Using two conceptual frameworks drawn from implementation science, we developed tailored KT strategies and a plan for implementing the new decision aid in three common prenatal care settings. To our knowledge, our paper is among the first to describe in detail the process used to develop such an implementation plan, a critical step in the process of implementing SDM.
Our plan addresses clinic-level organizational change at every stage, i.e., from training health professionals and raising patient awareness to following up with women post-decision. Though there is now extensive literature on SDM and decision aids, there is still uncertainty about how to implement them as sustainable practices in routine care [50, 51]. Passive dissemination strategies fail to address challenges stemming from professional attitudes and identities, lack of training, and organizational inertia [52], resulting in low levels of implementation and sustainability [52]. Several authors now argue that multi-faceted interventions targeting multiple levels (e.g., service users, providers, teams, organizations, systems) and addressing a range of facilitators and barriers are likely to be more successful [52,53,54,55]. For example, a robust attempt to implement SDM in routine care took place in the UK with the MAGIC program, a 3-year-quality improvement initiative (2010–2013) seeking to embed SDM within multiple clinical areas across a range of primary and secondary care settings [56, 57]. Investigators spent over 15 months designing and testing strategies and interventions to support the dissemination, adoption, and sustainability of SDM using the following strategies: (a) training and performance feedback activities, (b) support through the use of decision aids, (c) marketing campaigns, (d) facilitation and peer support, (e) increasing patient awareness and involvement, and (f) institutional supports for implementation [56, 57]. The result was improvements in care providers’ SDM-related knowledge and skills and increased use of decision support materials. The program also led some clinical teams to integrate SDM into their clinical routines, although results were not consistent in all clinical settings and some providers remained ambivalent about the need to share decisions with patients [56, 57]. The MAGIC study underscores the complexity of the implementation process, the diversity of potential barriers, and the need for bundles of KT interventions working together holistically to achieve broad and sustainable practice changes [54]. It also underscores how iterative the process of planning and implementation needs to be in real-world clinical settings.
Our process of establishing a clear and comprehensive user-designed implementation plan before moving to implementation itself may improve the effectiveness and efficiency of the change process. However, there is little guidance available on what the components of implementation plans should be, the steps involved in their development, and how to select the most appropriate KT strategies [19, 58]. Meyers and colleagues’ implementation plan involves needs assessments and readiness assessments, adapting the innovation to context, obtaining buy-in from key stakeholders, building organizational capacity, providing effective training, and creating implementation teams [59]. For their part, Damschroder et al. [19] suggest assessing stakeholders’ needs and perspectives, tailoring strategies, delivering information and education, establishing communication channels, tracking progress, and preparation with simulations or trial sessions. While studies of SDM implementation are rarely theory-informed [52], Damschroder et al. also propose basing their plan on behavioral or organizational theory. In the present study, stakeholder assessments using the PAR approach as well as the KTA and TDF frameworks helped us identify key strategies for our plan. The details of the plan were informed by our team’s work since 2008 in exploring attitudes around Down syndrome prenatal care screening, intentions to use decision aids, and facilitators and barriers to their use. We also developed contacts with key stakeholders who will facilitate its future adoption in prenatal care contexts in Quebec.
Another distinguishing feature of our process was our efforts to understand the clinical contexts and pathways associated with DS prenatal screening and care. The importance of understanding context has been cited frequently in the literature on implementation [60,61,62] and other work on decision aid implementation emphasizes taking clinicians’ workflows into account [57]. Using the PAR approach, we learned that hospital-based settings were likely to be the most challenging for decision aid implementation. We thus included five KT strategies tailored to the hospital context that target professional identities, attitudes, competencies, and capabilities. We expect that buy-in from senior hospital leaders and champions will be critical to the success of our implementation plan and will improve SDM with women cared for by gynecologists.
The present study has several strengths and limitations. Among the strengths was adoption of a theory-informed and participatory approach to developing our implementation plan, which included in-depth knowledge of the three main prenatal care pathways in the province. One limitation may be that our knowledge synthesis did not include studies beyond those conducted by our research team. This likely limited our access to information and lessons learned from other investigations into the implementation of decision aids in the context of prenatal care or screening practices. However, our research team has been an international leader in this area and we were able to draw on 11 articles representing over a decade’s work on this topic, which provided our team with useful and context-specific knowledge to inform our plan. With respect to our PAR study, we had a limited number of participants and did not gather the perspectives of community-based nurses, who are also involved in supporting prenatal screening decisions in primary care and other community settings. In preparation for a province-wide implementation plan, a broader coalition of stakeholders will be sought for the pilot phase of the study, which will involve operationalizing the implementation plan and its interventions, determining which sites will participate, and timelines for implementation activities.
Conclusion
In this study, we propose KT strategies and a clinical implementation plan for promoting use of a decision aid by pregnant women for the decision to undergo or not DS prenatal screening. Tailored for use in three clinical prenatal care settings, this theory-informed and user-designed implementation plan is intended to help institutionalize the practice of shared decision making for the difficult decision of DS prenatal screening. It ultimately aims to improve the way clinicians engage pregnant women and their partners in the decision-making process, and ensure that decisions better reflect their values and preferences. Our implementation plan could be integrated into the Quebec government’s DS Prenatal Screening Program and, with adaptations, to that of other governments. Next steps are to pilot our implementation plan while further developing global strategies that target institutional, policy, and systemic supports for implementation.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DS:
-
Down syndrome
- DA:
-
Decision aid
- SDM:
-
Shared decision making
- KTA framework:
-
Knowledge to action framework
- TDF:
-
Theoretical domains framework
- BCT:
-
Behaviour change techniques
- PEGASUS:
-
Personalized Genomics for Prenatal Aneuploidy Screening Using Maternal Blood
- KT:
-
Knowledge translation
References
Gouvernement du Québec. Trisomy 21 Prenatal Screening Program of Québec. Retrieved at https://www.quebec.ca/en/health/advice-and-prevention/screening-and-carrier-testing-offer/trisomy-21-prenatal-screening-program-of-quebec/ on 17 december 2019. 2019.
Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–7. https://doi.org/10.1007/s11606-012-2077-6.
Elwyn G, Edwards A, Kinnersley P. Shared decision-making in primary care: the neglected second half of the consultation. Br J Gen Pract. 1999;49(443):477–82.
Barry MJ, Edgman-Levitan S. Shared decision making—the pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–1. https://doi.org/10.1056/NEJMp1109283.
Stacey D, Légaré F, Lewis K, Barry MJ, Bennett CL, Eden KB, Holmes-Rovner M, Llewellyn-Thomas H, Lyddiatt A, Thomson R, Trevena L. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;12;4(4):CD001431. https://doi.org/10.1002/14651858.CD001431.pub5.
Graham ID, Logan J, Bennett CL, Presseau J, O'Connor AM, Mitchell SL, et al. Physicians’ intentions and use of three patient decision aids. BMC Med Inform Decis Mak. 2007;7(1):20. https://doi.org/10.1186/1472-6947-7-20.
Knops AM, Legemate DA, Goossens A, Bossuyt PM, Ubbink DT. Decision aids for patients facing a surgical treatment decision: a systematic review and meta-analysis. Ann Surg. 2013;257(5):860–6. https://doi.org/10.1097/SLA.0b013e3182864fd6.
Bekker HL, Hewison J, Thornton JG. Understanding why decision aids work: linking process with outcome. Patient Educ Couns. 2003;50(3):323–9. https://doi.org/10.1016/S0738-3991(03)00056-9.
Hunter A, Cappelli M, Humphreys L, Allanson J, Chiu T, Peeters C, et al. A randomized trial comparing alternative approaches to prenatal diagnosis counseling in advanced maternal age patients. Clin Genet. 2005;67(4):303–13. https://doi.org/10.1111/j.1399-0004.2004.00405.x.
Woolf S, Chan ECY, Harris R, Sheridan S, Braddock C, Kaplan R, et al. Promoting informed choice: transforming health care to dispense knowledge for decision making. Ann Intern Med. 2005;143(4):293–300. https://doi.org/10.7326/0003-4819-143-4-200508160-00010.
Légaré F. Le partage des décisions en santé entre patients et médecins. Recherches Sociographiques. 2009;50(2):283–99. https://doi.org/10.7202/037958ar.
Légaré F, Kearing S, Clay K, Gagnon S, D’Amours D, Rousseau M, et al. Are you SURE? Can Fam Physician. 2010;56(8):e308–e14.
Gagnon S, Labrecque M, Njoya M, Rousseau F, St-Jacques S, Légaré F. How much do family physicians involve pregnant women in decisions about prenatal screening for Down syndrome? Prenat Diagn. 2010;30(2):115–21. https://doi.org/10.1002/pd.2421.
Elwyn G, O’Connor A, Stacey D, Volk R, Edwards A, Coulter A, et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. Br Med J. 2006;333(7565):417.
International Patient Decision Aid Standards (IPDAS) Collaboration. IPDAS 2005: criteria for judging the quality of patient decison aids. Repéré à http://ipdas.ohri.ca/ipdas_checklist.pdf, le 14-03-2018. 2013.
Canada research chair in shared decision making and knowledge translation. The Chair. Promoting Shared Decision-Making in Healthcare. Repéré à http://www.decision.chaire.fmed.ulaval.ca/en/the-chair/, le 14-03-2018. 2018.
Légaré F, Ratté S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals’ perceptions. Patient Educ Couns. 2008;73(3):526–35. https://doi.org/10.1016/j.pec.2008.07.018.
Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: a systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns. 2014;94(3):291–309. https://doi.org/10.1016/j.pec.2013.10.031.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. https://doi.org/10.1186/1748-5908-4-50.
Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, et al. Lost in knowledge translation: time for a map? J Continuing Educ Health Prof. 2006;26(1):13–24. https://doi.org/10.1002/chp.47.
Field B, Booth A, Ilott I, Gerrish K. Using the Knowledge to Action Framework in practice: a citation analysis and systematic review. Implement Sci. 2014;9(1):172. https://doi.org/10.1186/s13012-014-0172-2.
Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37. https://doi.org/10.1186/1748-5908-7-37.
Straus SE, Brouwers M, Johnson D, Lavis JN, Légaré F, Majumdar SR, et al. Core competencies in the science and practice of knowledge translation: description of a Canadian strategic training initiative. Implement Sci. 2011;6(1):127. https://doi.org/10.1186/1748-5908-6-127.
Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. https://doi.org/10.1186/s13012-017-0605-9.
Mosavianpour M, Sarmast HH, Kissoon N, Collet J-P. Theoretical domains framework to assess barriers to change for planning health care quality interventions: a systematic literature review. J Multidiscip Healthc. 2016;9:303.
PErsonalized Genomics for prenatal Aneuploidy Screening USing maternal blood (PEGASUS). Moving towards implementing the next generation of prenatal screening. n. y. http://pegasus-pegase.ca/ Accessed September 27, 2019.
Green L, George M, Daniel M, Frankish C, Herbert C, Bowie W. Study of participatory research in health research promotion: review and recommendations for the development of participatory research in health promotion in Canada. Vancouver, BC: Institute of Health Promotion Research, University of British …; 1995.
Pinnock H, Barwick M, Carpenter CR, Eldridge S, Grandes G, Griffiths CJ, et al. Standards for reporting implementation studies (StaRI) statement. BMJ. 2017;356:i6795. https://doi.org/10.1136/bmj.i6795.
St Jacques S, Grenier S, Charland M, Forest J-C, Rousseau F, Légaré F. Decisional needs assessment regarding Down syndrome prenatal testing: a systematic review of the perceptions of women, their partners and health professionals. Prenat Diagn. 2008;28(13):1183–203. https://doi.org/10.1002/pd.2059.
Légaré F, Kearing S, Clay K, Gagnon S, D’Amours D, Rousseau M, et al. Are you SURE?: Assessing patient decisional conflict with a 4-item screening test. Can Fam Physician. 2010;56(8):e308–e14.
Légaré F, St-Jacques S, Gagnon S, Njoya M, Brisson M, Frémont P, et al. Prenatal screening for Down syndrome: a survey of willingness in women and family physicians to engage in shared decision-making. Prenat Diagn. 2011;31(4):319–26. https://doi.org/10.1002/pd.2624.
Leiva Portocarrero ME, Garvelink MM, Becerra Perez MM, Giguère A, Robitaille H, Wilson BJ, et al. Decision aids that support decisions about prenatal testing for Down syndrome: an environmental scan. BMC Med Inform Decis Mak. 2015;15(1):76. https://doi.org/10.1186/s12911-015-0199-6.
Delanoë A, Lépine J, Turcotte S, Leiva Portocarrero MA, Robitaille H, Giguère AMC, et al. Role of health literacy and psychosocial factors on the intention to use a decision aid for the Down syndrome prenatal screening: a theory-based online survey. JMIR. 2016;18(10):e283. https://doi.org/10.2196/jmir6362.
Delanoë A, Lépine J, Portocarrero MEL, Robitaille H, Turcotte S, Lévesque I, et al. Health literacy in pregnant women facing prenatal screening may explain their intention to use a patient decision aid: a short report. BMC Res Notes. 2016;9(1):339. https://doi.org/10.1186/s13104-016-2141-0.
Portocarrero MEL, Giguère AM, Lépine J, Garvelink MM, Robitaille H, Delanoë A, et al. Use of a patient decision aid for prenatal screening for Down syndrome: what do pregnant women say? BMC Pregnancy Childbirth. 2017;17(1):90. https://doi.org/10.1186/s12884-017-1273-0.
Lépine J, Leiva Portocarrero ME, Delanoë A, Robitaille H, Lévesque I, Rousseau F, et al. What factors influence health professionals to use decision aids for Down syndrome prenatal screening? BMC Pregnancy Childbirth. 2016;16(1):262. https://doi.org/10.1186/s12884-016-1053-2.
Rahimi SA, Lépine J, Croteau J, Robitaille H, Giguere AM, Wilson BJ, et al. Psychosocial factors of health professionals’ intention to use a decision aid for Down Syndrome screening: cross-sectional quantitative study. J Med Internet Res. 2018;20(4):e114. https://doi.org/10.2196/jmir.9036.
Agbadjé TT, Menear M, Dugas M, Gagnon M-P, Rahimi SA, Robitaille H, et al. Pregnant women’s views on how to promote the use of a decision aid for Down syndrome prenatal screening: a theory-informed qualitative study. BMC Health Serv Res. 2018;18(1):434. https://doi.org/10.1186/s12913-018-3244-1.
Ministère de la santé et des services sociaux (MSSS). Faits saillants de l’enquête sur l’offre du programme québécois de dépistage prénatal de la trisomie 21 – information pour les professionnels du Réseau de la santé et des services sociaux. Programme québécois de dépistage prénatal de la trisomie 21. https://www.oiiq.org/sites/default/files/uploads/pdf/sondage-trisomie-21-faits-saillants-2017.pdf. Accessed 29 Apr 2020. 2017.
O’Connor AM, Jacobsen MJ, Stacey D. An evidence-based approach to managing women’s decisional conflict. J Obstet Gynecol Neonatal Nurs. 2002;31(5):570–81. https://doi.org/10.1111/j.1552-6909.2002.tb00083.x.
Cochrane Effective Practice and Organisation of Care. Effective Practice and Organisation of Care (EPOC). EPOC Taxonomy. epoc.cochrane.org/epoc-taxonomy; Accessed 24 july 2020. 2015.
Institut de la statistique du Québec. Births and fertility. http://www.stat.gouv.qc.ca/statistiques/population-demographie/naissance-fecondite/index_an.html on 17 decembre 2019. 2015.
O'Connor AM. Validation of a decisional conflict scale. Med Decis Making. 1995;15(1):25–30. https://doi.org/10.1177/0272989X9501500105.
Brehaut JC, O'Connor AM, Wood TJ, Hack TF, Siminoff L, Gordon E, et al. Validation of a decision regret scale. Med Decis Making. 2003;23(4):281–92. https://doi.org/10.1177/0272989X03256005.
Holmes-Rovner M, Kroll J, Schmitt N, Rovner DR, Breer ML, Rothert ML, et al. Patient satisfaction with health care decisions: the satisfaction with decision scale. Med Decis Making. 1996;16(1):58–64. https://doi.org/10.1177/0272989X9601600114.
Michie S, Dormandy E, Marteau TM. The multi-dimensional measure of informed choice: a validation study. Patient Educ Couns. 2002;48(1):87–91. https://doi.org/10.1016/S0738-3991(02)00089-7.
Proctor E, Luke D, Calhoun A, McMillen C, Brownson R, McCrary S, et al. Sustainability of evidence-based healthcare: research agenda, methodological advances, and infrastructure support. Implement Sci. 2015;10(1):88. https://doi.org/10.1186/s13012-015-0274-5.
Lennox L, Maher L, Reed J. Navigating the sustainability landscape: a systematic review of sustainability approaches in healthcare. Implement Sci. 2018;13(1):27. https://doi.org/10.1186/s13012-017-0707-4.
Moore JE, Mascarenhas A, Bain J, Straus SE. Developing a comprehensive definition of sustainability. Implement Sci. 2017;12(1):110. https://doi.org/10.1186/s13012-017-0637-1.
Siyam T, Shahid A, Perram M, Zuna I, Haque F, Archundia-Herrera MC, et al. A scoping review of interventions to promote the adoption of shared decision-making (SDM) among health care professionals in clinical practice. Patient Educ Couns. 2019;102(6):1057–66. https://doi.org/10.1016/j.pec.2019.01.001.
Kuppermann M, Sawaya GF. Shared decision-making: easy to evoke, challenging to implement. JAMA Intern Med. 2015;175(2):167–8. https://doi.org/10.1001/jamainternmed.2014.4606.
Elwyn G, Scholl I, Tietbohl C, Mann M, Edwards AG, Clay C, et al. “Many miles to go…”: a systematic review of the implementation of patient decision support interventions into routine clinical practice. BMC Med Inform Decis Mak. 2013;13(S2):S14.
Scholl I, LaRussa A, Hahlweg P, Kobrin S, Elwyn G. Organizational-and system-level characteristics that influence implementation of shared decision-making and strategies to address them—a scoping review. Implement Sci. 2018;13(1):40. https://doi.org/10.1186/s13012-018-0731-z.
Joseph-Williams N, Lloyd A, Edwards A, Stobbart L, Tomson D, Macphail S, et al. Implementing shared decision making in the NHS: lessons from the MAGIC programme. Bmj. 2017;357:j1744.
Elwyn G, Frosch DL, Kobrin S. Implementing shared decision-making: consider all the consequences. Implement Sci. 2015;11(1):114. https://doi.org/10.1186/s13012-016-0480-9.
Lloyd A, Joseph-Williams N, Edwards A, Rix A, Elwyn G. Patchy ‘coherence’: using normalization process theory to evaluate a multi-faceted shared decision making implementation program (MAGIC). Implement Sci. 2013;8(1):102. https://doi.org/10.1186/1748-5908-8-102.
The Health Foundation. The MAGIC programme: evaluation. An independent evaluation of the MAGIC (Making good decisions in collaboration) improvement programme. https://www.health.org.uk/publications/the-magic-programme-evaluation. Accessed April 30, 2020. 2013.
Powell BJ, Beidas RS, Lewis CC, Aarons GA, McMillen JC, Proctor EK, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. 2017;44(2):177–94. https://doi.org/10.1007/s11414-015-9475-6.
Meyers DC, Durlak JA, Wandersman A. The quality implementation framework: a synthesis of critical steps in the implementation process. Am J Community Psychol. 2012;50(3-4):462–80. https://doi.org/10.1007/s10464-012-9522-x.
Squires JE, Aloisio LD, Grimshaw JM, Bashir K, Dorrance K, Coughlin M, et al. Attributes of context relevant to healthcare professionals’ use of research evidence in clinical practice: a multi-study analysis. Implement Sci. 2019;14(1):52. https://doi.org/10.1186/s13012-019-0900-8.
Li S-A, Jeffs L, Barwick M, Stevens B. Organizational contextual features that influence the implementation of evidence-based practices across healthcare settings: a systematic integrative review. Syst Rev. 2018;7(1):72. https://doi.org/10.1186/s13643-018-0734-5.
May CR, Johnson M, Finch T. Implementation, context and complexity. Implement Sci. 2016;11(1):141. https://doi.org/10.1186/s13012-016-0506-3.
Acknowledgements
We are grateful to stakeholders who participated in our study.
Funding
This project was funded through Genome Canada’s PEGASUS Project, the Canadian Institutes for Health Research, Génome Quebec, the Ministère de l’enseignement supérieur, de la recherche, de la science et de la technologie du Québec, Genome Alberta, and Genome BC.
Author information
Authors and Affiliations
Contributions
The study was led by TTA supervised by FL, Chairholder of the Tier 1 Canada Research Chair in Shared Decision Making and Knowledge Translation. All authors contributed to the conception and writing of this study. ATT and MM reviewed the articles and extracted information relevant to the KTA framework. ATT and MD interviewed stakeholders. ATT and MM established a consensus on the most relevant elements to include in the implementation plan. ATT and MM drafted the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was obtained from the research ethics boards of the Centre de Santé et de Services Sociaux de la Vieille-Capitale (#2013-2014-29) in Quebec, and the CHU de Quebec (#B14-02-1929).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Standards for Reporting Implementation Studies (StaRI) checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Agbadjé, T.T., Menear, M., Gagnon, MP. et al. Theory-based approach to developing an implementation plan to support the adoption of a patient decision aid for Down syndrome prenatal screening. Implementation Sci 16, 56 (2021). https://doi.org/10.1186/s13012-021-01103-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13012-021-01103-5