
Abstract
Background
IMP2 and IMP3 are mRNA binding proteins involved in carcinogenesis. We examined a large cohort of ovarian tumors with the aim to assess the value of IMP2 and IMP3 for differential diagnosis, and to assess their prognostic significance.
Methods
Immunohistochemical analyses with antibodies against IMP2 and IMP3 were performed on 554 primary ovarian tumors including 114 high grade serous carcinomas, 100 low grade serous carcinomas, 124 clear cell carcinomas, 54 endometrioid carcinomas, 34 mucinous carcinomas, 75 mucinous borderline tumors, and 41 serous borderline tumors (micropapillary variant). The associations of overall positivity with clinicopathological characteristics were evaluated using the chi-squared test or Fisher’s Exact test.
Results
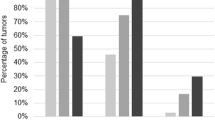
We found IMP2 expression (in more than 5% of tumor cells) in nearly all cases of all tumor types, so the prognostic meaning could not be analyzed. The positive IMP3 expression (in more than 5% of tumor cells) was most common in mucinous carcinomas (82%) and mucinous borderline tumors (81%), followed by high grade serous (67%) and clear cell carcinomas (67%). The expression was less frequent in endometrioid carcinomas (39%), low grade serous carcinomas (23%), and micropapillary variant of serous borderline tumors (20%). Prognostic significance of IMP3 could be evaluated only in low grade serous carcinomas in the case of relapse-free survival, where negative cases showed better RFS (p = 0.033).
Conclusion
Concerning differential diagnosis our results imply that despite the differences in expression in the different ovarian tumor types, the practical value for diagnostic purposes is limited. Contrary to other solid tumors, we did not find prognostic significance of IMP3 in ovarian cancer, with the exception of RFS in low grade serous carcinomas. However, the high expression of IMP2 and IMP3 could be of predictive value in ovarian carcinomas since IMP proteins are potential therapeutical targets.
Similar content being viewed by others


Background
The current WHO classification distinguishes between five major histological types of ovarian carcinomas with distinct histological features, immunophenotype, molecular abnormalities, precursors, risk factors, and responsiveness to therapy: high grade serous carcinoma (HGSC), low grade serous carcinoma (LGSC), endometrioid carcinoma (EC), clear cell carcinoma (CCC), and mucinous carcinoma (MC) [1, 2]. Although most ovarian carcinomas are relatively straightforward to diagnose, there may be overlapping histological features between some types, e.g. between HGSC and high-grade EC and ancillary immunohistochemical studies are often employed to aid in the diagnosis. Although diagnostic algorithms for immunohistochemistry based on large studies are available, some tumors may show an overlapping immunohistochemical profile, and additional novel immunohistochemical markers would be helpful [3,4,5,6].
The insulin-like growth factor 2 and 3 mRNA binding proteins (IMP2 and IMP3) are closely related members of a family of RNA-binding proteins. They are involved in various biological processes such as development and tumorigenesis, where they also play a role in ovarian carcinomas [7]. In particular, IMPs influence mRNA maturation, localization, translation, and stability via binding to RNA [7]. By these post-transcriptional regulations, IMPs can promote cell proliferation, invasion, and cell migration [7,8,9]. Overexpression of IMP2 has been described in esophageal, pancreatic, and hepatocellular carcinomas, where it serves as a marker of poor prognosis [10,11,12,13]. IMP3 protein is expressed in fetal tissues during embryogenesis, but it is either low or undetectable in adult tissues [9, 14]. Aberrant expression of IMP3 has been described in various malignant tumors, such as pancreatic, colorectal, lung, endocervical, endometrial, renal cell, gastric, urothelial, and breast cancers [8].
We studied a large cohort of ovarian tumors including HGSC, LGSC, CCC, EC, MC, mucinous borderline tumor (MBT) and micropapillary variant of serous borderline tumor (mSBT) with the aim to assess the value of IMP2 and IMP3 for the differential diagnosis. We further investigated the prognostic significance of IMP3 expression in ovarian tumors. IMP2 could not be analyzed because most cases were positive.
Methods
Samples
The archives of the pathology departments of the authors were searched for cases diagnosed as primary tubo-ovarian HGSC, LGSC, micropapillary variant of SBT (mSBT; synonymous with the term “noninvasive LGSC” used in the previous WHO classification), MC, MBT, EC, and CCC. In total, 542 cases were selected for immunohistochemical analysis, all of which were reviewed by two gynecological pathologists (PD and KN). The sample set included 114 HGSC, 100 LGSC, 124 CCC, 54 EC, 34 MC, 75 MBT and 41 SBT (only the micropapillary variant), which for the most part represents a dataset of ovarian tumors used in a previous study [15].
Patient’s clinical characteristics
Clinical data on patient and tumor characteristics at the time of diagnosis and other survival data were obtained retrospectively from medical records. The date of imaging, biopsy confirmation of recurrence or death from the disease was reported as the time of recurrence. If the patient died without determining the cause, the death was recorded as dead of unknown cause (DUC). The clinicopathological and survival characteristics of the 542 patients are summarized in Tables 1 and 2.
Immunohistochemical analysis
The immunohistochemical analysis was performed using tissue microarrays (TMAs) as described in our previous study [15]. The TMA technique was used based on previous studies which described IMP2 and IMP3 expression in ovarian tumors, in line with the recommendation of a review study designed by Burdeleski et al., which recommended the TMA as a convenient technique for evaluating IMP3 expression [8]. The expression of the following antibodies was analyzed in each case: IMP2, using two clones since the experience with these antibodies is rather limited (clone OTI3F9, dilution 1:200, Novus Biologicals, USA; clone EPR6741(B), dilution 1:200, Abcam, USA), and IMP3 (clone 69.1, dilution 1:200, Glostrup Denmark), with antigen retrieval HIER, and detection by EnVision FLEX, Dako. For both IMP2 clones the staining was performed by the Ventana BenchMark ULTRA instrument (Roche, Basel, Switzerland) with the OptiView detection kit. Normal ovarian surface epithelium served as negative control, while lymph follicles in lymph nodes were used as a positive control.
The expression of all markers was double-blindly evaluated by at least two of three pathologists in various combinations (KN, PD, MKB).
Cytoplasmic expression for all markers was assessed semiquantitatively (the overall percentage of positive cells). Cases were classified based on the overall percentage of positive cells as negative (entirely negative or arbitrarily set as ≤5% of positive tumor cells) or positive (more than 5% positive tumor cells).
Statistical analysis
The software R (version 4.0.2, https://www.r-project.org/) and Statistica (TIBCO Statistica 13.5.0, CA, USA) were used to perform the statistical analyses.
Associations of overall positivity (≤ 5% of positive tumor cells = negative, versus 6–100% of positive tumor cells = positive) with clinicopathological characteristics were evaluated using the chi-squared test or Fisher’s Exact test.
Overall survival (OS), relapse-free survival (RFS), local recurrence-free survival (LFS), and metastasis-free survival (MFS) analyses were performed. If the patient did not show any of the monitored events, the case was censored in the analysis to the date of the last follow-up. Survival analyses were plotted using Kaplan-Meier model and log-rank statistics were used to test for differences between positive and negative cases.
All tests were two-sided and a p-value of less than 0.05 was considered as significant.
Results
The clinicopathological and survival characteristics of the 542 patients are summarized in Tables 1 and 2. The immunohistochemical results in relation to the individual tumor types are summarized in Table 3. Overall, IMP2 (both clones) showed a higher percentage of positivity than IMP3 in all tumor types (Table 3). We also tried to use other different cut-offs (5, 10, and 50%) for differential diagnostic purposes between ovarian tumors, and the results are stated in Table 4.
IMP2
In all tumor types there was a strong positive correlation between the two clones (HGSC: R = 0.582, p < 0.001; LGSC: R = 0.867, p < 0.001; SBT: R = 0.828, p = 0.004; EC: R = 0.803, p < 0.001; CCC: R = 0.775, p < 0.001; MC: R = 0.507, p < 0.001, MBT: R = 0.658, p < 0.001).
All tumor types showed higher expression of IMP2 (for both antibodies) compared to IMP3 (Table 3).
IMP3
IMP3 expression in the various tumor types using 3 different cut-offs (5, 10, and 50%) is detailed in Table 3. The highest positivity of IMP3 according to the percentage of positive cells was found in MC (82% positive cases, 62% cases with expression in > 50% of tumor cells) and MBT (81% positive cases, 58% cases with expression in > 50% of tumor cells). IMP3 immunoreactivity was significantly higher in MC with expansile invasion compared to MC with infiltrative invasion (p = 0.015). High expression was also found in HGSC (67% positive cases, 42% cases with expression in > 50% of tumor cells), and CCC (67% positive cases, 42% cases with expression in > 50% of tumor cells). The lowest positivity was found in LGSC and mSBT with similar results (LGSC: 23% positive cases, 4% cases with expression in > 50% of tumor cells; mSBT: 20% positive cases, 7.5% cases with expression in > 50% of tumor cells). The EC group showed intermediate levels of IMP3 expression compared to the other tumor types (39% positive cases, 30% cases with expression in > 50% of tumor cells) (Fig. 1).

A – E Expression of IMP3: A - in HGSC (100x), B – in LGSC (100x), C – in CCC (200x), D – in EC (100x). F-G Expression of IMP2 (IGF2): F - in HGSC (100x), G – in LGSC (200x), H – in CCC (100x), I - in EC (200x), J – in MC (100x)
Prognostic analysis
Survival analysis was performed only for the tumor types with sufficient number of events of interest (see Supplementary Table S1 for a detailed overview of the sample size and results of time-to-event analyses in the individual subsets).
The only significant difference was detected in LGSC in case of relapse-free survival, where negative cases showed better RFS (p = 0.033, Fig. 2). None of the other clinicopathological correlations between the selected parameters and IMP2/IMP3 expression showed statistically significant results. In HGSC there was a trend towards a positive correlation between T stage and IMP3 expression, but it did not reach statistical significance (p = 0.054, Supplementary Table S2, note the limited sample size of the negative cases for both IMP2 clones).

Kaplan-Meier curves for RFS of LGSC patients in relation to expression of IMP3
Discussion
In the female genital tract, the expression of IMPs has, so far, been mostly investigated in ovarian and endometrial tumors. In endometrial lesions IMP3 expression has been found in benign endometrium, atypical endometrial hyperplasia, and endometrial carcinomas, with the highest expression in serous carcinomas [16,17,18,19,20,21]. Li et al. found IMP3 positivity in more than 50% of tumor cells in 93% of 42 serous carcinomas, and in only 7% of 8 endometrioid carcinomas and concluded that IMP3 may serve as a helpful biomarker in the distinction between these two tumor types (p < 0.001) [22]. Zheng et al. found IMP3 positivity in more than 50% of tumor cells in 94% of serous carcinomas and 49% of clear cell carcinomas compared to 3% of endometrioid carcinomas and complete negativity in 8 mucinous endometrial carcinomas [19]. They concluded that IMP3 is a highly sensitive marker for both endometrial serous and clear cell carcinomas. Mhawech-Fauceglia et al. found IMP3 positivity (in more than 5% of tumor cells) in 100 and 12% of serous and endometrioid endometrial carcinomas, respectively and suggested the combination of IMP3 and PTEN as a useful panel for distinguishing between these two tumor types (P < 0.001) [16]. In a subsequent study on 401 cases, the same authors found 78% of serous carcinomas, 57% of clear cell carcinomas and 15% of endometrioid carcinomas IMP3 positive by using a combined scoring system for intensity and percentage of expression [17]. Zaidi et al. found IMP3 positivity in 64% of endometrial serous carcinomas and 19% of grade 3 endometrioid carcinomas using 5% cut-off for positivity, and suggested a panel of p53, p16, IMP3, ER and PR as best for distinguishing serous from endometrioid carcinoma [18].
Concerning IMP3 expression in ovarian tumors, the published literature provides less clear evidence. Studies which have focused on IMP3 expression in HGSC have shown variable results. In 6 studies with a total of 526 cases of HGSC IMP3 positivity ranged from 23 to 68% (average 49%) [14, 23,24,25,26,27]. Three other studies found IMP3 expression in 45 to 93% of 110 “serous carcinoma cases”, but the type of serous carcinoma was not further specified [8, 28, 29]. Our data showed IMP3 expression in 67% of HGSC, which is consistent with studies that used the same cut-off for positivity and the same antibody clone [14, 28]; there is only one study which found a lower expression [25]. The explanation for such a wide range of IMP3 expression in the various studies is not clear but could be related to the different cut-offs for positivity used. Two studies used 10% of positive tumor cells as a cut off [8, 26], while the remaining studies used different scoring systems, mostly taking into account staining intensity as well as percentage of positive tumor cells [24, 27, 29, 30].
Unlike HGSC, expression of IMP3 in LGSC has not yet been studied in detail. One study analyzed the RNA expression levels in ovarian tumors including three cases of LGSC, but without correlation with immunohistochemical expression [31]. In our study, IMP3 expression was present in 23% of LGSC and 20% mSBT. We identified four studies analyzing IMP3 expression in SBT, with 125 cases in total, but only one of them mentions the mSBT subtype. In three of these studies all SBT cases were IMP3 negative [23, 24, 27, 28]. One study on 84 SBT, including 32 cases with a micropapillary pattern, reported absent or weak IMP3 expression in 34%, medium IMP3 expression in 57%, and strong IMP3 expression in 9% of cases [23]. Compared to previous studies, our study included only mSBT and, considering our results, expression of IMP3 in mSBT seems to differ from typical SBT.
IMP3 expression in ovarian EC has been investigated in 4 studies (comprising a total of 265 cases), but the data is equivocal with a wide range of positivity varying between 2 and 40% [8, 25,26,27]. However, the studies used different cut-offs for positivity; one study used a 5% cut-off (27% of positive cases), two a 10% cut-off (2 and 33% of positive cases), and the other combined scoring systems (40% of positive cases). In our study, IMP3 expression was found in 39% of cases of EC.
Four studies with a total of 337 cases investigated the expression of IMP3 in CCC and the expression ranged from 52 to 86%, which is in accordance with our result of 67% [25,26,27, 32]. These studies also used different cut-offs for positivity; one study used a 5% cut-off (52% of positive cases), two a 10% cut-off (63 and 86% of positive cases, respectively), and one study a combined scoring system (75% of positive cases).
We identified only three studies focusing on IMP3 expression in ovarian mucinous tumors, two of which included MC only [23, 25, 33]. In one study, the authors found IMP3 expression in 86% of 30 MC using a cut-off of 5% [25]. Another study on 250 ovarian mucinous tumors found any extent of IMP3 expression in 12% of benign tumors, 91% of MBT, and 100% of MC [33]. In another study on 140 MBT, moderate or strong expression was found in 66% of cases when using a combined immunoreactive score [23]. The results of our study showed a similar frequency of IMP3 expression in MBT and MC. IMP3 expression of any extent was found in 81% MBT and 82% MC, which is consistent with the above-mentioned results.
So far, only one study has examined the value of IMP3 expression in the differential diagnosis of ovarian carcinomas, and the authors suggested IMP3 to be an additional diagnostic marker for ovarian CCC [26]. The authors investigated 336 ovarian carcinomas (including 132 CCC, 103 HGSC, and 116 EC) and found IMP3 positivity in 86% of CCC, 23% of HGSC, and 2% of EC cases. IMP3 expression was significantly higher in CCC compared to HGSC and EC (p < 0.01) and, therefore, it was concluded that IMP3 is a useful marker to distinguish CCC from HGSC and EC. The study used a different antibody clone and a different cut-off for positivity (more than 10% of positive tumor cells) compared to ours, which did not find significant differences between CCC and HGSCs [26]. In our study, using the 5% cut-off, we did not find significant differences between CCC and HGSC. When using 3 different cut-offs (5, 10, and 50%), we found differences between CCC and EC for the cut-off 10% which is in concordance with the study just mentioned but there was no difference between HGSC and CCC (Table 4).
To date, only three studies have focused on the immunohistochemical expression of IMP2 in tumors of the female genital tract. Two of those studied endometrial tumors, while the other focused on ovarian tumors. Both endometrial studies suggested IMP2 as a marker which can be used in the differential diagnosis between endometrioid and serous carcinomas [34, 35]. One of these studies suggested the use of IMP2 in a diagnostic panel which would allow for the discrimination between endometrioid (G1 and G2) and serous carcinoma based on an H-score (IMP2 ≥ 115) [34]. However, using an H-score as a discriminator is not very feasible in diagnostic practice, and the sensitivity for differentiating grade 3 endometrioid carcinoma from serous carcinoma was lower. The other study investigated IMP2 expression in 227 endometrial carcinomas, and 93 cases of benign endometrium [35]. The authors found diffuse expression (in > 95% tumor cells) in all 27 cases of serous carcinomas, but all endometrioid carcinomas showed IMP2 expression in less than 75% of tumor cells (in 32% of tumors the expression was in < 5% of tumor cells). They concluded that IMP2 expression in < 75% of the tumor cells can help distinguish endometrioid from serous carcinomas.
Only one study examined the immunoreactivity of IMP2 in epithelial ovarian tumors and included ovarian transitional cell carcinoma, which is now considered a pattern of HGSC [36]. By using a combined score, they found a lower percentage of positive cells in Brenner tumors compared to transitional cell carcinomas. Two other studies examined protein expression profiling and found IMP2 expression in 89% (39/44) of HGSC and in 11% (2/18) of EC [37, 38].
The results of our study showed high IMP2 expression (of both clones) in all tumor types, which was higher compared to IMP3 expression. The highest IMP2 expression was detected in mSBT (showing 100% for both clones), and HGSC (both clones in the range of 98–100%). The expression was slightly lower, but still high, in EC (76–91%), LGSC (98%), and CCC (88–91%). In mucinous tumors the expression was 96% in MBT and 91–97% in MC. We did not find any statistically significant differences between the expression of IMP2 and IMP3 in MBT and MC, or in SBT and LGSC.
Although the expression of IMP3 showed statistically significant differences between some tumor types in our study, the value for differential diagnosis of ovarian tumors seems to be rather limited. In particular, the assessment of cut-offs for positivity seems to be problematic for most tumor types in diagnostic practice. The only exception seems to be the differences in expression between HGSC and LGSC, especially when considering a 50% cut-off, which was present in 42% of HGSC but only in 4% of LGSC. However, the practical value of this finding seems to be limited as the morphological distinction between HGSC and LGSC is usually straightforward and there are other useful antibodies such as p53, p16, and Ki67. Furthermore, IMP3 is not useful in the differential diagnosis between HGSC and grade 3 EC, which can also be problematic in some cases. Our study showed no practical use for IMP2 in the differential diagnosis of epithelial ovarian tumors.
Most studies of IMP3 and IMP2 expression in ovarian tumors have focused on its prognostic importance, but the results are not conclusive. The poor prognostic impact of IMP3 expression has been confirmed only in ovarian CCC [25, 32]. Our study showed no correlation between IMP3 expression and various clinicopathological parameters or patient outcomes (with respect to OS, RFS, LFS, and MFS), except for LGSC, which showed a significant difference in the case of RFS, seeing as negative cases had better RFS (p = 0.033). In mucinous tumors, high IMP2/EPR6741(B) expression was associated with favorable LFS, but the low number of events in our MC sample set limited the survival analyses. However, the high expression of IMP2 and IMP3 in ovarian carcinomas may gain further interest since IMP proteins are potential therapeutical targets [7]. One study focused on colorectal cancer reported that IMP3 directly regulates MEKK1 mRNA, and thus activates the MEK/ERK pathway [39]. The authors suggest that inhibiting IMP3, possibly in combination with a MEK1 inhibitor, may provide new potential therapeutic strategies for colorectal cancer treatment. Another study demonstrated that inhibition of IMP3 expression in cell lines of neuroendocrine tumors leads to downregulation of EGFR and Ki-67, proteins associated with cell proliferation, and these authors suggest IMP3 as a promising therapeutic target [40]. So far only one study described the inhibition of IMP2 in vitro and in vivo (in colorectal carcinoma and hepatocellular cell lines, zebrafish embryos) [7]. The results showed reduced growth of xenotransplanted tumor cells, which supports the theory that IMP2 represents a druggable target.
Conclusion
The results of our study suggest only a limited value of IMP2 and IMP3 for the differential diagnosis of ovarian epithelial tumors. Although we found differences in IMP3 expression between HGSC and LGSC, the practical value of this for differential diagnosis seems to be rather limited. We did not confirm the prognostic significance of IMP3 expression in ovarian epithelial tumors, with the exception of LGSC, where negative cases were associated with longer RFS. This is in contrast to other solid tumors. IMP2 could not be analyzed with respect to its prognostic impact due to the high levels of positivity in most cases. Nevertheless, IMP3 and IMP2 expression could be of predictive value, should inhibitors of the RNA-binding protein become therapeutic.
Availability of data and materials
All data generated or analyzed during this study is included in this published article (and its Supplementary information files).
References
Kurman RJ, Shih IM. Molecular pathogenesis and extraovarian origin of epithelial ovarian cancer--shifting the paradigm. Hum Pathol. 2011;42(7):918–31.
Singh N, McCluggage WG, Gilks CB. High-grade serous carcinoma of tubo-ovarian origin: recent developments. Histopathology. 2017;71(3):339–56.
Kobel M, Luo L, Grevers X, Lee S, Brooks-Wilson A, Gilks CB, et al. Ovarian carcinoma Histotype: strengths and limitations of integrating morphology with Immunohistochemical predictions. Int J Gynecol Pathol. 2019;38(4):353–62.
Kobel M, Rahimi K, Rambau PF, Naugler C, Le Page C, Meunier L, et al. An Immunohistochemical algorithm for ovarian carcinoma typing. Int J Gynecol Pathol. 2016;35(5):430–41.
McCluggage WG. Endometriosis-related pathology: a discussion of selected uncommon benign, premalignant and malignant lesions. Histopathology. 2020;76(1):76–92.
Rajendran S, McCluggage WG. WT1 positive ovarian Endometrioid tumors: observations from consult cases and strategies for distinguishing from serous neoplasms. Int J Gynecol Pathol. 2022;41(2):191–202.
Dahlem C, Abuhaliema A, Kessler SM, Krohler T, Zoller BGE, Chanda S, et al. First small-molecule inhibitors targeting the RNA-binding protein IGF2BP2/IMP2 for Cancer therapy. ACS Chem Biol. 2022;17(2):361–75.
Burdelski C, Jakani-Karimi N, Jacobsen F, Möller-Koop C, Minner S, Simon R, et al. IMP3 overexpression occurs in various important cancer types and is linked to aggressive tumor features: a tissue microarray study on 8,877 human cancers and normal tissues. Oncol Rep. 2018;39(1):3–12.
Gong Y, Woda BA, Jiang Z. Oncofetal protein IMP3, a new cancer biomarker. Adv Anat Pathol. 2014;21(3):191–200.
Barghash A, Golob-Schwarzl N, Helms V, Haybaeck J, Kessler SM. Elevated expression of the IGF2 mRNA binding protein 2 (IGF2BP2/IMP2) is linked to short survival and metastasis in esophageal adenocarcinoma. Oncotarget. 2016;7(31):49743–50.
Dahlem C, Barghash A, Puchas P, Haybaeck J, Kessler SM. The insulin-like growth factor 2 mRNA binding protein IMP2/IGF2BP2 is overexpressed and correlates with poor survival in pancreatic Cancer. Int J Mol Sci. 2019;20(13):3204.
Xing M, Li P, Wang X, Li J, Shi J, Qin J, et al. Overexpression of p62/IMP2 can promote cell migration in hepatocellular carcinoma via activation of the Wnt/β-catenin pathway. Cancers. 2019;12(1):7.
Xing M, Li P, Wang X, Li J, Shi J, Qin J, et al. Overexpression of p62/IMP2 can promote cell migration in hepatocellular carcinoma via activation of the Wnt/beta-catenin pathway. Cancers. 2019;12(1):7.
Mohanty SK, Tiwari A, Singh C, Walsh C, Chuang F, Kim E, et al. High-grade ovarian serous carcinomas: significant correlation of histologic patterns with IMP3 and E-cadherin predicting disease recurrence and survival. Ann Diagn Pathol. 2019;40:30–9.
Dundr P, Bazalova B, Bartu M, Bosse T, Drozenova J, Fabian P, et al. The cytokeratin 17 expression in primary ovarian tumors has diagnostic but not prognostic significance. Virchows Arch. 2022;481(2):201–12.
Mhawech-Fauceglia P, Herrmann FR, Rai H, Tchabo N, Lele S, Izevbaye I, et al. IMP3 distinguishes uterine serous carcinoma from endometrial endometrioid adenocarcinoma. Am J Clin Pathol. 2010;133(6):899–908.
Mhawech-Fauceglia P, Yan L, Liu S, Pejovic T. ER+ /PR+ /TFF3+ /IMP3- immunoprofile distinguishes endometrioid from serous and clear cell carcinomas of the endometrium: a study of 401 cases. Histopathology. 2013;62(7):976–85.
Zaidi A, Gupta P, Gupta N, Rajwanshi A, Rai B, Gainder S. Role of immunohistochemistry to distinguish grade 3 Endometrioid carcinoma and uterine serous carcinoma. Appl Immunohistochem Mol Morphol. 2020;28(1):42–8.
Zheng W, Yi X, Fadare O, Liang SX, Martel M, Schwartz PE, et al. The oncofetal protein IMP3: a novel biomarker for endometrial serous carcinoma. Am J Surg Pathol. 2008;32(2):304–15.
Li M, Zhao H, Zhao SG, Wei DM, Zhao YR, Huang T, et al. The HMGA2-IMP2 pathway promotes Granulosa cell proliferation in polycystic ovary syndrome. J Clin Endocrinol Metab. 2019;104(4):1049–59.
Fadare O, Liang SX, Crispens MA, Jones HW 3rd, Khabele D, Gwin K, et al. Expression of the oncofetal protein IGF2BP3 in endometrial clear cell carcinoma: assessment of frequency and significance. Hum Pathol. 2013;44(8):1508–15.
Li C, Zota V, Woda BA, Rock KL, Fraire AE, Jiang Z, et al. Expression of a novel oncofetal mRNA-binding protein IMP3 in endometrial carcinomas: diagnostic significance and clinicopathologic correlations. Mod Pathol. 2007;20(12):1263–8.
El-Balat A, Sänger N, Karn T, Becker S, Holtrich U, Muallem Z, et al. IMP3 expression in borderline tumors of the ovary. Anticancer Res. 2017;37(2):583–8.
Imamura H, Ohishi Y, Aman M, Shida K, Shinozaki T, Yasutake N, et al. Ovarian high-grade serous carcinoma with a noninvasive growth pattern simulating a serous borderline tumor. Hum Pathol. 2015;46(10):1455–63.
Köbel M, Xu H, Bourne PA, Spaulding BO, Shih Ie M, Mao TL, et al. IGF2BP3 (IMP3) expression is a marker of unfavorable prognosis in ovarian carcinoma of clear cell subtype. Mod Pathol. 2009;22(3):469–75.
Lu L, Wang S, Zhu Q, Qu Y, Gu W, Ning Y, et al. The expression of IMP3 in 366 cases with ovarian carcinoma of high grade serous, endometrioid and clear cell subtypes. Pathol Res Pract. 2018;214(8):1087–94.
Noske A, Faggad A, Wirtz R, Darb-Esfahani S, Sehouli J, Sinn B, et al. IMP3 expression in human ovarian cancer is associated with improved survival. Int J Gynecol Pathol. 2009;28(3):203–10.
Chisté M, Alexis J, Recine M. IMP3 expression in serous tumors of the ovary. Appl Immunohistochem Mol Morphol. 2014;22(9):658–62.
Zhang Y, Garcia-Buitrago MT, Koru-Sengul T, Schuman S, Ganjei-Azar P. An immunohistochemical panel to distinguish ovarian from uterine serous papillary carcinomas. Int J Gynecol Pathol. 2013;32(5):476–81.
Wang Y, Li L, Wang Y, Yuan Z, Zhang W, Hatch KD, et al. IMP3 as a cytoplasmic biomarker for early serous tubal carcinogenesis. J Exp Clin Cancer Res. 2014;33(1):60.
Hsu KF, Shen MR, Huang YF, Cheng YM, Lin SH, Chow NH, et al. Overexpression of the RNA-binding proteins Lin28B and IGF2BP3 (IMP3) is associated with chemoresistance and poor disease outcome in ovarian cancer. Br J Cancer. 2015;113(3):414–24.
Bi R, Shen X, Zhang W, Cheng Y, Feng Z, Cai X, et al. Clear cell carcinomas of the ovary: a mono-institutional study of 73 cases in China with an analysis of the prognostic significance of clinicopathological parameters and IMP3 expression. Diagn Pathol. 2016;11:17.
Zhu Q, Qu Y, Zhang Q, Lu L, Weng W, Zhang H, et al. IMP3 is upregulated in primary ovarian mucinous carcinoma and promotes tumor progression. Am J Transl Res. 2017;9(7):3387–98.
Santacana M, Maiques O, Valls J, Gatius S, Abó AI, López-García M, et al. A 9-protein biomarker molecular signature for predicting histologic type in endometrial carcinoma by immunohistochemistry. Hum Pathol. 2014;45(12):2394–403.
Zhang L, Liu Y, Hao S, Woda BA, Lu D. IMP2 expression distinguishes endometrioid from serous endometrial adenocarcinomas. Am J Surg Pathol. 2011;35(6):868–72.
Takeuchi T, Ohishi Y, Imamura H, Aman M, Shida K, Kobayashi H, et al. Ovarian transitional cell carcinoma represents a poorly differentiated form of high-grade serous or endometrioid adenocarcinoma. Am J Surg Pathol. 2013;37(7):1091–9.
Hiramatsu K, Yoshino K, Serada S, Yoshihara K, Hori Y, Fujimoto M, et al. Similar protein expression profiles of ovarian and endometrial high-grade serous carcinomas. Br J Cancer. 2016;114(5):554–61.
Gu L, Shigemasa K, Ohama K. Increased expression of IGF II mRNA-binding protein 1 mRNA is associated with an advanced clinical stage and poor prognosis in patients with ovarian cancer. Int J Oncol. 2004;24(3):671–8.
Zhang M, Zhao S, Tan C, Gu Y, He X, Du X, et al. RNA-binding protein IMP3 is a novel regulator of MEK1/ERK signaling pathway in the progression of colorectal Cancer through the stabilization of MEKK1 mRNA. J Exp Clin Cancer Res. 2021;40(1):200.
Er LM, Li Y, Wu ML, Li B, Tan BB, Gao Y, et al. Insulin-like growth factor II mRNA binding protein 3 regulates proliferation, invasion and migration of neuroendocrine cancer cells. Int J Clin Exp Pathol. 2017;10(10):10269–75.
Acknowledgements
The authors wish to extend their gratitude to Mgr. Zachary H.K. Kendall, B.A. (Institute for History of Medicine and Foreign Languages, First Faculty of Medicine, Charles University in Prague) for the English language editing.
Funding
This work was supported by the Ministry of Health, Czech Republic (MH CZ DRO-VFN 64165 and AZV NV19–03-00007), by Charles University (Project UNCE204065, SVV260516), and by the European Regional Development Fund (EF16_013/0001674) and BBMRI_CZ LM2018125.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. All authors participated on material preparation, data collection, and / or analyses. The first draft of the manuscript was written by KN. RM, IS provided statistical analysis. KN, PD, MKB provided immunohistochemical examination. DC gained clinical data. All authors commented on previous versions of the manuscript, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the General University Hospital in Prague in compliance with the Helsinki Declaration (No. 2140/19 S-IV). The Ethics Committee waived the requirement for informed consent as according to the Czech Law (Act. no. 373/11, and its amendment Act no. 202/17), it is not necessary to obtain informed consent in fully anonymized studies.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing financial and/or non-financial interests relevant to the content of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Overview of the sample size and results of survival analyses for each tumor type. Table S2. Correlations between the studied markers and the selected clinico-pathological parameters for different tumor types.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Němejcová, K., Bártů, M.K., Michálková, R. et al. A comprehensive immunohistochemical analysis of IMP2 and IMP3 in 542 cases of ovarian tumors. Diagn Pathol 18, 15 (2023). https://doi.org/10.1186/s13000-023-01300-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13000-023-01300-4