
Abstract
Background
The relationship between cerebrospinal fluid (CSF) biomarkers and the clinical features of idiopathic normal pressure hydrocephalus (iNPH) has been inconclusive. We aimed to evaluate CSF biomarkers reflecting Alzheimer’s disease (AD)-related amyloid β (Aβ) aggregation, tau pathology, neuroinflammation and axonal degeneration in relation to the clinical features of pre- and post-shunt surgery in iNPH patients.
Methods
Mini Mental State Examination (MMSE) scores and gait velocity were evaluated pre- and postoperatively in cohorts of 65 Finnish (FIN) and 82 Swedish (SWE) iNPH patients. Lumbar CSF samples were obtained prior to shunt surgery and analysed for soluble amyloid precursor protein alpha (sAPPα) and beta (sAPPβ); amyloid-β isoforms of 42, 40 and 38 (Aβ42, Aβ40, Aβ38); total tau (T-tau); phosphorylated tau (P-tau181); neurofilament light (NfL) and monocyte chemoattractant protein 1 (MCP1).
Results
Preoperative patient characteristics showed no significant differences between patients in the FIN and SWE cohorts. Patients in both cohorts had significantly improved gait velocity after shunt surgery (p < 0.0001). Low CSF T-tau and absence of apolipoprotein E ε4 predicted over 20% gait improvement postoperatively (p = 0.043 and p = 0.008). Preoperative CSF T-tau, P-tau181 and NfL correlated negatively with MMSE scores both pre- (p < 0.01) and post-surgery (p < 0.01). Furthermore, T-tau, NfL and Aβ42 correlated with MMSE outcomes (p < 0.05). Low preoperative CSF P-tau181 (p = 0.001) and T-tau with NfL (p < 0.001 and p = 0.049) best predicted pre- and postoperative MMSE scores greater than or equal to 26.
Conclusions
CSF biomarkers of neurodegeneration appeared to correlate with pre- and postoperative cognition, providing a window into neuropathological processes. In addition, preoperative CSF neurodegeneration biomarkers may have potential in the prediction of gait and cognitive outcomes after shunt surgery.
Similar content being viewed by others


Background
Idiopathic normal pressure hydrocephalus (iNPH) is characterized by a symptom triad of gait dysfunction, dementia and incontinence, accompanied by enlarged ventricles [1, 2]. Symptom progression can be reversed with CSF shunt surgery [3, 4]. The common symptom triad and shunt-surgery outcomes are usually quantified by symptom domain classifying grading scales. Regardless of careful patient selection, not all patients have favourable surgical outcomes [5, 6]. It has been suggested that poor shunt surgery outcomes are derived from commonly coexisting neurodegenerative diseases, such as Alzheimer’s disease (AD) or vascular degeneration [7, 8].
There are several CSF biomarkers assessed for diagnostic and predictive purposes in the field of neurodegenerative diseases. For iNPH patients, it has been shown that the lumbar CSF composition of low tau and APP-derived proteins together with high MCP1 can distinguish iNPH patients from cognitively intact individuals and patients with other neurodegenerative diseases [9]. However, the association of a wider repertoire of AD biomarkers with postsurgery clinical features in iNPH are still somewhat inconclusive [10,11,12,13].
In the current literature, postoperative gait velocity has been found to be associated with lumbar CSF T-tau and P-tau181 collected preoperatively [11, 13]. Regarding cognitive decline, studies have shown the predictive value of P-tau181, the Aβ42/P-tau181 ratio and the Aβ38/Aβ42 ratio [12, 13], with a higher P-tau181 correlating with a poorer cognitive outcome. In another study [14], CSF Aβ42 was shown to correlate with postoperative MMSE values.
The role of the axonal degeneration biomarker neurofilament-light (NfL) as a symptom predictor in iNPH patients has not been studied widely either. In AD patients, higher plasma NfL levels have been shown to be associated with poorer Mini Mental State Examination (MMSE) scores [15], and plasma Nfl and CSF NfL levels are the best single predictors of cognition in AD patients [16]. On the other hand, a recent study found no significant correlation between neuropsychiatric symptoms and CSF NfL in AD [17]. For vascular dementia, however, there was a negative correlation between CSF NfL and neuropsychiatric performance [17].
Since there are tendencies for biomarkers to enhance the accuracy of diagnosis and prediction of outcome in iNPH, establishing a more precise, specific preoperative biomarker combination able to predict a favourable shunt surgery outcome would be highly beneficial.
Objective
In this study, we aimed to evaluate preoperatively-obtained CSF biomarkers reflecting AD-related Aβ aggregation, tau pathology, neuroinflammation and axonal degeneration and their associations with pre- and postoperative clinical features in Finnish and Swedish iNPH cohorts.
Methods
Study populations
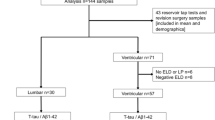
In all, 65 and 82 consecutive shunted patients with probable iNPH diagnosed by the Relkin criteria [18] at Kuopio University Hospital and the Hydrocephalus Research Unit, Sahlgrenska University Hospital in Gothenburg were included (Fig. 1). The requirement for ventriculoperitoneal CSF shunt surgery was assessed using previously described protocols [9, 19]. The clinical features of cohorts were evaluated pre- and postoperatively using Mini Mental State Examination (MMSE) and gait velocity (m/s) along with the iNPH grading scale (NPHGS, 0–12) [20] for Finnish patients and the iNPH scale (NPHS, 0–100) [21] for Swedish patients. A favourable shunt surgery outcome was defined as a decrease of ≥ 1 point in iNPHGS and an increase of > 5 points in iNPH scale. Comorbidities of type 2 diabetes mellitus (DM2), hypertension and cardiac diseases were also registered preoperatively. The diagnostic protocols and CSF sampling were executed 3 months prior to shunt surgery. The postsurgery evaluation was performed 3 and 12 months postoperatively in the Finnish cohort where the 3-month value was used if the 12-month visit was missing. In the Swedish cohort, postsurgery evaluation was performed approximately 6 months postoperatively. The mean follow-up times were 11.5 months for the Finnish cohort and 10.9 months for the Swedish cohort. During the follow-up, 7 participants withdrew or died (5 from the Finnish cohort and 2 from the Swedish cohort). In addition, venous blood samples were obtained for APOE genotyping, and DNA was isolated using a commercial kit according to the manufacturer’s protocol (Illustra Blood GenomicPrep Mini Spin Kit, GE Healthcare, Little Chalfont, UK). The extracted samples were analysed by the standard PCR method [22].

Flow chart. Flow chart presenting the cohorts and participants. Baseline represents the presurgery examination and Postoperative the visits after surgery. INPH: idiopathic normal pressure hydrocephalus; n: number; post-op: postoperative; pre-op: preoperative
Biomarker analysis
Preoperative CSF samples were obtained by lumbar puncture in both cohorts and retained in 10 ml polypropylene tubes. Samples were centrifuged, aliquoted and frozen in a temperature-controlled − 80 °C freezer. There was no blood contamination seen in the samples obtained.
The CSF biomarker measurements were performed at the Clinical Neurochemistry Laboratory at Sahlgrenska University Hospital, Mölndal, Sweden. The laboratory technicians were board-certified and blinded to the clinical data. All experiments were executed on the same plate in one round of experiments and using the same batch of reagents. Commercial kits were used to perform the biomarker concentration analysis. CSF T-tau and P-tau181 were measured by INNOTEST ELISAs using the kit manufacturer’s protocol (Fujirebio, Ghent, Belgium). For Aβ38, Aβ40, Aβ42, sAPPα, sAPPβ and MCP1 analysis, electrochemiluminescence (ECL) assays were used, as described by the manufacturer [23] (Meso Scale Discovery Rockville, MD, USA). The NfL concentration was measured with an in-house ELISA, as previously described [24].
Statistics
The group comparisons performed for mean values and frequencies were performed by t tests for continuous variables and x2 or Wilcoxon’s signed ranks test for discrete variables. Pearson correlation coefficients (r) were assessed for linear dependency analyses. Since CSF concentrations of T-tau, P-tau181, NfL, Aβ38, Aβ40, Aβ42, sAPPα, sAPPβ and MCP1 were concordant in both cohorts, we pooled the cohorts for correlation analysis. For pre- and postoperative comparisons, we used analysis of covariance (ANCOVA) with the confounding covariates of age, sex and APOE genotype. Receiver operating characteristics (ROC curves) and binary logistic regression were used to model MMSE performance and gait outcome. Pre- and postoperative MMSE with gait outcome were dichotomized by cut-offs of 26 by the mild dementia value commonly used and 20% improvement in gait. ROC analysis of biomarkers, dichotomized MMSE and gait was performed. We aimed to identify optimal biomarker cut-offs by estimating Youden’s indices and favouring balanced sensitivity and specificity. Univariate modelling was performed, and significant variables with age, sex and APOE genotype were used in the multiple regression model. Multicollinearity diagnostics were used for variables included in the multiple regression model. All tests calculated were two-sided and considered significant with a p value less than 0.05. The statistical analyses were performed in IBM SPSS Statistics 27.00 for IOS.
Results
The patient demographic and clinical characteristics, APOE genotype and mean CSF biomarker values are presented in Table 1. No significant differences were seen in demographic or clinical characteristics or APOE genotype between the Finnish and Swedish cohorts. In addition, CSF concentrations of T-tau, P-tau181, NfL, Aβ38, Aβ40, Aβ42, sAPPα, sAPPβ and MCP1 were concordant in both cohorts. Correlation analysis was assessed for pooled cohorts (Fig. 2, Table 2). Preoperative MMSE results correlated negatively with T-tau (r = − 0.36, p < 0.0001, Fig. 2A), P-tau181 (r = − 0.26, p = 0.002, Fig. 2C) and NfL (r = − 0.23, p = 0.006, Fig. 2E). Comparable results were seen between the postoperative MMSE values and biomarkers of T-tau (r = − 0.37, p < 0.0001, Fig. 2B), P-tau181 (r = − 0.30, p < 0.0001, Fig. 2D) and NfL (r = − 0.23, p = 0.006, Fig. 2F). The postsurgery MMSE outcome correlated negatively with T-tau (r = − 0.18, p = 0.046, Fig. 3A) and NfL (r = − 0.17, p = 0.045, Fig. 3B) and positively with Aβ42 (r = 0.18, p = 0.38, Fig. 3C). We compared MMSE results between P-tau181 cut-off 27.5 ng/l derived groups and a 4.0% increase (mean score 24.8–25.8) was seen in low P-tau181 group during the follow-up whereas the high P-tau181 group remained similar (mean score 21.8) (Fig. 4). Both pre- and postsurgery MMSE values differed between patients in the P-tau181-derived groups (Pre, p < 0.001; Post, p < 0.001). In addition, the P-tau181 groups showed divergent Aβ42 concentrations of 321 ng/l in the low P-tau181 group and 415 ng/l in the high P-tau181 group (p < 0.001). The APOE genotype correlated only with Aβ42 (r = − 0.27, p = 0.003, Table 2).

Pre- and postoperative correlation of Mini Mental State Examination and biomarkers. Graphs of concentration of lumbar CSF biomarkers of T-tau (A, B), P-tau181 (C, D) and NfL (E, F): preoperative—(A, C, E) and postoperative (B, D, F) MMSE values. Significant results are highlighted with asterisk (*p < 0.01, **p < 0.0001). Linear trendlines are drawn to visualize the correlations. T-tau: total tau protein; P-tau: phosphorylated at threonine 181 tau protein; NfL: neurofilament-light; MMSE: mini mental state examination

Correlation of Mini Mental State Examination outcome and biomarkers. Graphs of preoperatively obtained lumbar CSF biomarkers of T-tau (A), NfL (B) and Aβ42 (C) correlated with MMSE outcomes (T-tau r = − 0.18, NfL r = − 0.17, Aβ42 r = 0.18). Negative outcome is presented as a decrease in X-axis. Significant results are highlighted with asterisk (*p < 0.05). Linear trendlines are drawn to visualize the correlations. T-tau: total tau protein; NfL: neurofilament-light; Aβ42: Amyloid-β 42; MMSE: mini mental state examination

Pre-and postoperative Mini Mental State Examination results grouped by P-tau181 concentrations. Longitudinal change of pooled MMSE results with CSF P-tau181 derived grouping presented in chart. Cutoff used for grouping was 27.5 ng/l. Low P-tau181 group presented as triangles and high P-tau181 group as circles. Significant results are presented by asterisk (*p < 0.001). MMSE, mini mental state examination; Pre-op: preoperative; Post-op: postoperative; P-tau: phosphorylated at threonine 181 tau protein
In gait velocity, both cohorts improved significantly after surgery (by 38% FIN, 33% SWE) (p < 0.0001) (Table 1). In the pooled cohort, only NfL showed a negative correlation with preoperative gait velocity (r = − 0.25, p = 0.003, Table 2), whereas for postoperative gait velocity, this correlation was seen for T-tau (r = − 0.33, p < 0.001, Fig. 5A), P-tau181 (r = − 0.25, p = 0.005, Fig. 5B) and NfL (r = − 0.25, p = 0.003, Fig. 5C).

Chart of postoperative correlation of biomarkers with gait velocity. Preoperatively obtained lumbar CSF biomarkers of T-tau (A), P-tau181 (B) and NfL (C) correlated negatively (T-tau r = − 0.33, P-tau r = − 0.25, NfL r = − 0.25) with postoperative gait velocity (m/s) and presented in XY-chart. Significant correlations are highlighted with asterisk (*p < 0.01). Linear trendlines are drawn to visualize the correlations. T-tau: total tau protein; P-tau: phosphorylated at threonine 181 tau protein; NfL: neurofilament-light
Regression modelling was utilized for dichotomized biomarker concentration variables with MMSE performance and gait velocity outcomes as dependent variables (Table 3). Low CSF P-tau181 (cut-off 27.5 ng/l, OR 3.4) and T-tau (cut-off 211 ng/l, OR 3.7) patients were more likely to have MMSE above 26 preoperatively (p < 0.05). Comparable results were seen for postoperative MMSE results: patients in the low CSF P-tau181 (cut-off 27.5 ng/l, OR 4.5), T-tau (213.5 ng/l, OR 8.1), NfL (1045 ng/l, OR 3.7), Aβ38 (1710 ng/l, OR 2.5) and Aβ40 (3714 ng/l, OR 2.2) groups were more likely to have MMSE scores above 26 (p < 0.05), respectively compared to the scores of patients in the high concentration groups. Favourable outcome of 20% increase in gait velocity was 2.8-, 2.7-, 0.4- and 0.4-times more likely for low CSF T-tau (cut-off 206 ng/l), NfL (1050 ng/l), Aβ42 (301 ng/l) and sAPPβ (239 ng/l) concentration patients compared to high (p < 0.05). The most significant multivariate model for evaluating preoperative MMSE included P-tau181, NfL, APOE, sex and age (Nagelkerke R2 = 0.18, 69.8% accuracy). In this model, low CSF P-tau181 patients were 3.4 times more likely to have MMSE above 26 (CI (1.3–8.7), p = 0.01). For postoperative MMSE, the combination of T-tau, NfL, Aβ38, age and sex best predicted the performance (Nagelkerke R2 = 0.32, 72.9% accuracy). The low CSF T-tau and NfL patients were 13.6 (CI 3.4–55.0) and 2.4 (1.0–5.8) times more likely to have MMSE above 26 (p < 0.05). The model with a more specific CSF T-tau cut-off (306 ng/l) predicted MMSE to be below 26 postoperatively by 96.7% specificity, 37.0% sensitivity and 63.9% overall accuracy. In this model, high T-tau patients had a 17.0-fold (CI 3.8–75.3, p < 0.001) greater risk of having MMSE below 26 postsurgery. Gait improvement over 20% postoperatively was best predicted by T-tau, sAPPβ, APOE, age and sex (Nagelkerke R2 = 0.22, 75.8% accuracy). The patients with low CSF T-tau and absence of APOE ε4-allele were 3.1 (1.0–9.4) and 3.9 (1.4–10.4) times more likely to improve their gait by 20% postsurgery (p < 0.05).
In the follow-up from pre- to postsurgery, both cohorts improved in NPHGS (p = 0.025) and NPHS (p < 0.0001). In the subdomains of both NPHGS and NPHS, a significant change was seen in gait (p = 0.01 FIN, p < 0.0001 SWE), along with cognition (p < 0.0001). In the Swedish cohort, P-tau181 was the only biomarker to correlate with the NPHS outcome (r = − 0.25, p = 0.028). In the Finnish cohort, MCP1 (r = − 0.28, p = 0.030) correlated with postoperative outcome. Interestingly, MCP1 was found to negatively correlate with the incontinence outcome of NPHGS in the Finnish cohort (r = − 0.34, p = 0.009).
Discussion
To our knowledge, this is the first study to report this broad preoperatively-collected CSF biomarker profile of iNPH patients in comparison with their MMSE scores and gait velocity. Our data showed that T-tau, P-tau181 and NfL are associated with cognitive and gait performance in iNPH patients. Furthermore, T-tau and NfL were able to predict postoperative MMSE results, and T-tau was able to predict an improvement of 20% or more in postoperative gait velocity.
The role of biomarkers in defining clinical symptoms has not been established previously with iNPH patients. Nonetheless, our findings verify previous results of the ability of preoperatively obtained lumbar CSF P-tau181 to predict postoperative MMSE values and thus support the ability of T-tau and P-tau181 to predict postoperative cognition [12,13,14]. Contrary to Nakajima et al. [13], who reported that P-tau181 correlated only to the postoperative MMSE, we found P-tau181 to correlate with both pre- and postoperative MMSE values. This difference may be due to the larger number of patients within our study. Additionally, we performed CSF P-tau181-derived group comparison (27.5 ng/l cut-off) against the pre- and postoperative MMSE values. The results were similar to those previously found [13], as the MMSE performance of patients in the groups differed significantly, with a higher P-tau181 group resulting in significantly worse postoperative MMSE score (Fig. 4). In logistic regression modelling, we found similar results using ROC curve-derived cut-offs (P-tau181 27.5 ng/l, T-tau 213.5 ng/l), where the low CSF P-tau181 and T-tau groups had a significantly increased chance of MMSE above 26 postoperatively (Table 3). In previous studies [11, 13], T-tau and P-tau181 could predict gait outcome measured with NPHGS. Since the gait domain of NPHGS is derived mostly from gait velocity, we consider our results to partly support these earlier findings.
For amyloid precursor protein-derived biomarkers, we found no direct association with shunt response, corroborating the results of a previous study [25]. However, our postoperative MMSE values did not show a correlation with CSF Aβ42, as previously reported [14]. Interestingly, in our data, the MMSE outcome was found to correlate positively with preoperative Aβ42 (Fig. 3C). Regarding the APOE genotype, we found a weak association with CSF Aβ42, as expected. In regression modelling, the absence of the APOE ε4 allele predicted gait improvement of 20% postsurgery. The correlation seen for CSF MCP1 to outcome and incontinence in the Finnish cohort was interesting as well, evoking the question of whether underlying inflammatory mechanisms are frequently seen amongst Finnish iNPH patients. This finding was not seen in the Swedish cohort contesting this result to occur by coincidence.
The NfL concentrations showed similar associations with MMSE and gait velocity values as T-tau and P-tau181. In logistic regression modelling, patients with low CSF NfL were significantly more likely to have postoperative MMSE scores above 26 (Table 3). Furthermore, the correlations of NfL to T-tau and especially to P-tau181 (Table 2) were notably lower than those between T-tau and P-tau181. We consider this difference to derive from the different origins of NfL being a large calibre myelinated axon protein [26]. Thus, reinforcing the role of NfL as reflecting changes in neurodegeneration independently from T-tau and P-tau181. In previous studies, NfL has been stated to be elevated in several neurodegenerative diseases, including iNPH, when compared to healthy individuals, mirroring both acute and subacute changes in brain metabolism [26,27,28]. Consequently, we believe that our baseline concentrations of lumbar CSF NfL are able to reflect symptoms seen both pre- and postoperatively.
A possible explanation for the prognostic features of T-tau, P-tau181 and NfL reported is their ability to reflect acute and subacute neuropathologic processes [28, 29]. The natural course of iNPH is reported to be progressive and potentially lethal [3, 30]. The associations between increased T-tau, P-tau181 and NfL CSF concentrations and more severe symptomatology probably represent ongoing damage to the brain parenchyma. More precisely, the progressive neurodegeneration seen in iNPH might derive from reported impaired CSF circulation [2, 31]. With shunt surgery accomplished, disease progression is restricted, but the damage to the parenchyma occurring presurgery remains to some extent, leading to lower MMSE values and slower gait velocity.
The other, more frequently discussed hypothesis for the negative correlation of CSF tau proteins, especially P-tau181, with the MMSE and gait velocity observed postoperatively is potentially caused by other underlying neuropathological processes, such as AD. Low Aβ42 and elevated P-tau181 concentrations of CSF are characteristics of comorbid AD in iNPH [32]. This hypothesis is supported by the results presenting the high prevalence of AD comorbidity in iNPH patients [7]. In addition, the CSF P-tau181-derived group comparison (Fig. 4) visualizes the varying outcome of MMSE with higher P-tau181 concentrations obtained presurgery. When comparing the Aβ42 compositions between the P-tau181 groups, a consistently lower concentration of Aβ42 was seen in the high-P-tau181 group. On the other hand, the improvement of MMSE in the low-P-tau181 group might present the established hypothesis of pure iNPH pathophysiology with reversible cognitive impairment since the low CSF tau proteins are stated to be a characteristic domain for iNPH [9, 33]. Regarding these hypotheses and results obtained here, we consider the biomarkers of neurodegeneration to have prognostic features that emerge during the postoperative follow-up.
Our second intent was to determine plausible differences between two separate cohorts of iNPH patients from different populations of Sweden and Finland. Our data showed that both cohorts were comparable in baseline characteristics and had equivalent shunt surgery outcomes despite the diverse diagnostic protocols (Table 1, Fig. 6). Moreover, the preoperatively obtained CSF biomarker concentrations and distributions were similar (Table 1, Fig. 7). These results add support to the notion that diagnostic guidelines and standardized clinical diagnostic procedures lead to the identification of patients with iNPH in a similar and reproducible way, which is of importance in the clinical setting but also for the generalization of results in research studies. Intriguing differences were seen when comparing the subdomains of NPHGS and NPHS from pre- to postsurgery. The Swedish cohort improved significantly in subdomains of gait and cognition, whereas significant improvement was only seen in gait for the Finnish cohort. This variety seen between different diagnostic tools might originate from the wider measurement range of the iNPH scale. Nevertheless, this comparison provides insight into how the positive shunt surgery outcome is mainly derived from gait and cognition improvements.

Pre- and Postoperative Mini Mental State Examination & Gait velocity distributions between cohorts. Pre- and post-operative MMSE results with gait velocity distributions of Finnish and Swedish cohorts are presented as violin plots. Violin plots including Kernel density plot and box plot combined. No significant differences were seen between the cohorts. MMSE: mini mental state examination; Pre-op: preoperative; Post-op: postoperative; Fin: Finnish cohort; Swe: Swedish cohort

CSF biomarkers of neurodegeneration distributions in cohorts of Finnish and Swedish patients. Pre-operatively obtained CSF biomarker distributions presented as violin plot from Finnish and Swedish cohorts. Violin plots including Kernel density plot and box plot combined. No significant differences were seen between the groups. T-tau: total tau protein; P-tau: phosphorylated at threonine 181 tau protein; NfL: neurofilament-light; Aβ38: Amyloid-β 38; Aβ40: Amyloid-β 40; Aβ42: Amyloid-β 42; sAPPα: soluble amyloid precursor protein α; sAPPβ: soluble amyloid precursor protein β, MCP1: monocyte chemoattractant protein 1; Fin: Finnish cohort; Swe, Swedish cohort
Our challenge in this study was the various measures for symptoms since the Kuopio University Hospital patients were graded using iNPHGS and the Sahlgrenska University Hospital patients were graded using the iNPH scale although the diagnostic tools of MMSE and gait velocity used in both centres were comparable. However, using the MMSE only most likely fails to consider all the cognitive dimensions seen with iNPH patients [34]. Furthermore, symptom validation using gait velocity can include confounding components since the measurement with metres per second does not take into account assistant devices used during the walk test. Nonetheless, we consider this not to notably influence our results, since the gait velocity outcomes were similar in both cohorts, and we had a relatively large study population as a whole. Another challenge we found, was not to be able to provide distinct biomarker thresholds below which MMSE improvements do not occur due the overlap of CSF biomarker concentrations between responders and non-responders. We also note that our follow-up times varied between the patients. Nonetheless, the variation seen between follow-up times was rather small.
We performed univariate and multivariate logistic regression modelling with ROC curve-derived biomarker cut-offs to validate the best predictive CSF biomarker combination for pre- and postoperative MMSE among patients with over 20% improvement in postoperative gait velocity (Table 3). To our surprise, P-tau181 was the best predictor of preoperative MMSE scores. NfL and T-tau combined with Aβ38 predicted postoperative MMSE results with the highest accuracy. The notable finding was also that a higher T-tau cut-off of 306 ng/l could predict at least mildly demented patients postoperatively by a specificity of 96.7%. In gait improvement, T-tau and APOE genotype were found to be the only significant variables in the multivariate model to have the ability to predict 20% postoperative gait improvement. These results highlight the usefulness of NfL- and tau-derived CSF biomarkers. Moreover, a better prognostic value is achieved by using the combination of CSF biomarkers that are reflecting different components of neurodegenerative processes. However, we cannot rule out shunt operations based on this study and further research is still needed for the clinical applications of these biomarkers.
Conclusions
The patients in the study cohorts were comparable in baseline characteristics and showed equivalent shunt surgery outcomes. CSF biomarkers of neurodegeneration appeared to correlate with pre- and postoperative cognition, providing a window into neuropathological processes. CSF T-tau and P-tau181 appear to be the best predictors both for pre- and postoperative MMSE scores. In addition, preoperative T-tau may have potential for the prediction of gait velocity outcomes after shunt surgery.
Availability of data and materials
All data supporting the findings within this article will be shared anonymized by request of any qualified investigator.
Abbreviations
- iNPH:
-
Idiopathic normal pressure hydrocephalus
- AD:
-
Alzheimer’s disease
- CSF:
-
Cerebrospinal fluid
- DM2:
-
Diabetes mellitus type 2
- MMSE:
-
Mini mental state examination
- Pre-op:
-
Preoperative
- Post-op:
-
Postoperative
- APOE :
-
Apolipoprotein E
- NPHGS:
-
Idiopathic normal pressure hydrocephalus grading scale (0–12)
- NPHS:
-
Idiopathic normal pressure hydrocephalus scale (0–100)
- T-tau:
-
Total tau protein
- P-tau181 :
-
Phosphorylated at threonine 181 tau protein
- NfL:
-
Neurofilament-light
- Aβ38 :
-
Amyloid-β 38
- Aβ40 :
-
Amyloid-β 40
- Aβ42 :
-
Amyloid-β 42
- sAPPα:
-
Soluble amyloid precursor protein α
- sAPPβ:
-
Soluble amyloid precursor protein β
- MCP1:
-
Monocyte chemoattractant protein 1
- r:
-
Pearson correlation coefficient
- OR:
-
Odds ratio
References:
Hakim S, Adams RD. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure: observations on cerebrospinal fluid hydrodynamics. J Neurol Sci. 1965;2(4):307–27.
Eide PK, Valnes LM, Pripp AH, Mardal K-A, Ringstad G. Delayed clearance of cerebrospinal fluid tracer from choroid plexus in idiopathic normal pressure hydrocephalus. J Cereb Blood Flow Metab. 2020;40(9):1849–58.
Andrén K, Wikkelsø C, Hellström P, Tullberg M, Jaraj D. Early shunt surgery improves survival in idiopathic normal pressure hydrocephalus. Eur J Neurol. 2021;28(4):1153–9.
Kazui H, Miyajima M, Mori E, Ishikawa M, Hirai O, Kuwana N, et al. Lumboperitoneal shunt surgery for idiopathic normal pressure hydrocephalus (SINPHONI-2): an open-label randomised trial. Lancet Neurol. 2015;14(6):585–94.
Toma AK, Papadopoulos MC, Stapleton S, Kitchen ND, Watkins LD. Systematic review of the outcome of shunt surgery in idiopathic normal-pressure hydrocephalus. Acta Neurochir. 2013;155(10):1977–80.
Sundström N, Malm J, Laurell K, Lundin F, Kahlon B, Cesarini KG, et al. Incidence and outcome of surgery for adult hydrocephalus patients in Sweden. Br J Neurosurg. 2017;31(1):21–7.
Leinonen V, Koivisto AM, Alafuzoff I, Pyykk OT, Rummukainen J, Von Und Zu Fraunberg M, et al. Cortical brain biopsy in long-term prognostication of 468 patients with possible normal pressure hydrocephalus. Neurodegener Dis. 2012;10(1–4):166–9.
Hamilton R, Patel S, Lee EB, Jackson EM, Lopinto J, Arnold SE, et al. Lack of shunt response in suspected idiopathic normal pressure hydrocephalus with Alzheimer disease pathology. Ann Neurol. 2010;68(4):535–40.
Jeppsson A, Wikkelsö C, Blennow K, Zetterberg H, Constantinescu R, Remes AM, et al. CSF biomarkers distinguish idiopathic normal pressure hydrocephalus from its mimics. J Neurol Neurosurg Psychiatry. 2019;90:1117–23.
Schirinzi T, Sancesario GM, Ialongo C, Imbriani P, Madeo G, Toniolo S, et al. A clinical and biochemical analysis in the differential diagnosis of idiopathic normal pressure hydrocephalus. Front Neurol. 2015;6:86.
Craven CL, Baudracco I, Zetterberg H, Lunn MPT, Chapman MD, Lakdawala N, et al. The predictive value of T-tau and AB1-42 levels in idiopathic normal pressure hydrocephalus. Acta Neurochir. 2017;159(12):2293–300.
Nakajima M, Miyajima M, Ogino I, Akiba C, Sugano H, Hara T, et al. Cerebrospinal fluid biomarkers for prognosis of long-term cognitive treatment outcomes in patients with idiopathic normal pressure hydrocephalus. J Neurol Sci. 2015;357(1–2):88–95.
Nakajima M, Miyajima M, Ogino I, Akib C, Kawamura K, Kamohara C, et al. Preoperative phosphorylated tau concentration in the cerebrospinal fluid can predict cognitive function three years after shunt surgery in patients with idiopathic normal pressure hydrocephalus. J Alzheimer’s Dis. 2018;66(1):319–31.
Elobeid A, Laurell K, Cesarini KG, Alafuzoff I. Correlations between mini-mental state examination score, cerebrospinal fluid biomarkers, and pathology observed in brain biopsies of patients with normal-pressure hydrocephalus. J Neuropathol Exp Neurol. 2015;74(5):470–9.
Mattsson N, Cullen NC, Andreasson U, Zetterberg H, Blennow K. Association between longitudinal plasma neurofilament light and neurodegeneration in patients with Alzheimer disease. JAMA Neurol. 2019;76(7):791–9.
Van Hulle C, Jonaitis EM, Betthauser TJ, Batrla R, Wild N, Kollmorgen G, et al. An examination of a novel multipanel of CSF biomarkers in the Alzheimer’s disease clinical and pathological continuum. Alzheimer’s Dement. 2021;17(3):431–45.
Bloniecki V, Zetterberg H, Aarsland D, Vannini P, Kvartsberg H, Winblad B, et al. Are neuropsychiatric symptoms in dementia linked to CSF biomarkers of synaptic and axonal degeneration? Alzheimer’s Res Ther. 2020;12(1):1–10.
Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57(suppl_3):S2-4.
Junkkari A, Luikku AJ, Danner N, Jyrkkänen HK, Rauramaa T, Korhonen VE, et al. The Kuopio idiopathic normal pressure hydrocephalus protocol: initial outcome of 175 patients. Fluids Barriers CNS. 2019;16(1):21.
Kubo Y, Kazui H, Yoshida T, Kito Y, Kimura N, Tokunaga H, et al. Validation of grading scale for evaluating symptoms of idiopathic normal-pressure hydrocephalus. Dement Geriatr Cogn Disord. 2007;25(1):37–45.
Hellström P, Klinge P, Tans J, Wikkelsø C. A new scale for assessment of severity and outcome in iNPH. Acta Neurol Scand. 2012;126(4):229–37.
Pyykkö OT, Helisalmi S, Koivisto AM, Mölsä JAA, Rummukainen J, Nerg O, et al. APOE4 predicts amyloid-β in cortical brain biopsy but not idiopathic normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry. 2012;83(11):1119–24.
Zetterberg H, Andreasson U, Hansson O, Wu G, Sankaranarayanan S, Andersson ME, et al. Elevated cerebrospinal fluid BACE1 activity in incipient alzheimer disease. Arch Neurol. 2008;65(8):1102–7.
Gaetani L, Höglund K, Parnetti L, Pujol-Calderon F, Becker B, Eusebi P, et al. A new enzyme-linked immunosorbent assay for neurofilament light in cerebrospinal fluid: Analytical validation and clinical evaluation. Alzheimer’s Res Ther. 2018;10(1):1–13.
Hamdeh SA, Virhammar J, Sehlin D, Alafuzoff I, Cesarini KG, Marklund N. Brain tissue Aβ42 levels are linked to shunt response in idiopathic normal pressure hydrocephalus. J Neurosurg. 2019;130(1):121–9.
Bridel C, Van Wieringen WN, Zetterberg H, Tijms BM, Teunissen CE, Alvarez-Cermeño JC, et al. Diagnostic value of cerebrospinal fluid neurofilament light protein in neurology: a systematic review and meta-analysis. JAMA Neurol. 2019;76(9):1035–48.
Jeppsson A, Zetterberg H, Blennow K, Wikkelsø C. Idiopathic normal-pressure hydrocephalus pathophysiology and diagnosis by CSF biomarkers. Neurology. 2013;80(15):1385–92.
Lukkarinen H, Tesseur I, Pemberton D, Van Der Ark P, Timmers M, Slemmon R, et al. Time trends of cerebrospinal fluid biomarkers of neurodegeneration in idiopathic normal pressure hydrocephalus. J Alzheimer’s Dis. 2021;80:1–14.
Clarke CJ, Skandsen T, Zetterberg H, Einarsen CE, Feyling C, Follestad T, et al. One-year prospective study of plasma biomarkers from CNS in mild traumatic brain injury patients. Front Neurol. 2021;12:568.
Andrén K, Wikkelsø C, Tisell M, Hellström P. Natural course of idiopathic normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry. 2014;85(7):806–10.
Lindstrøm EK, Ringstad G, Mardal KA, Eide PK. Cerebrospinal fluid volumetric net flow rate and direction in idiopathic normal pressure hydrocephalus. NeuroImage Clin. 2018;20:731–41.
Vanninen A, Nakajima M, Miyajima M, Rauramaa T, Kokki M, Musialowicz T, et al. Elevated CSF LRG and decreased Alzheimer’s disease biomarkers in idiopathic normal pressure hydrocephalus. J Clin Med. 2021;10(5):1105.
Espay AJ, Da Prat GA, Dwivedi AK, Rodriguez-Porcel F, Vaughan JE, Rosso M, et al. Deconstructing normal pressure hydrocephalus: Ventriculomegaly as early sign of neurodegeneration. Ann Neurol. 2017;82(4):503–13.
Nerg O, Junkkari A, Hallikainen I, Rauramaa T, Luikku A, Hiltunen M, et al. The CERAD neuropsychological battery in patients with idiopathic normal pressure hydrocephalus compared with normal population and patients with mild Alzheimer’s disease. J Alzheimers Dis. 2021;81(3):1117–30.
Acknowledgements
We would like to acknowledge Marita Parviainen, RN, for assistance and cognitive testing. HZ is a Wallenberg Scholar supported by Grants from the Swedish Research Council (#2018-02532), the European Research Council (#681712), Swedish State Support for Clinical Research (#ALFGBG-720931), the Alzheimer Drug Discovery Foundation (ADDF), USA (#201809-2016862), the AD Strategic Fund and the Alzheimer's Association (#ADSF-21-831376-C, #ADSF-21-831381-C and #ADSF-21-831377-C), the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden (#FO2019-0228), the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie Grant agreement No. 860197 (MIRIADE), and the UK Dementia Research Institute at UCL. MT is supported by grants from the Rune and Ulla Amlöv foundation, the Edit Jacobson foundation, the foundation Hjalmar Svenssons forskningsfond and the Swedish state under the agreement between the Swedish government and the County Councils, the ALF-agreement (#ALFGBG 720121). KB is supported by the Swedish Research Council (#2017-00915), the Alzheimer Drug Discovery Foundation (ADDF), USA (#RDAPB-201809-2016615), the Swedish Alzheimer Foundation (#AF-742881), Hjärnfonden, Sweden (#FO2017-0243), the Swedish state under the agreement between the Swedish government and the County Councils, the ALF-agreement (#ALFGBG-715986), the European Union Joint Program for Neurodegenerative Disorders (JPND2019-466-236), the National Institute of Health (NIH), USA, (grant #1R01AG068398-01), and the Alzheimer’s Association 2021 Zenith Award (ZEN-21-848495). HL is supported by grants from Maire Taponen Foundation and The Finnish Medical Foundation.
Funding
The study was funded by Kuopio University Hospital VTR (#5252614) fund, Academy of Finland (#339767) and Sigrid Juselius Foundation.
Author information
Authors and Affiliations
Contributions
All authors discussed the results and contributed to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the regional ethics committee in Kuopio/Finland and Gothenburg/Sweden. Written informed consent was signed by all included participants. The implementation and governance of this study was performed in agreement with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
HZ has served at scientific advisory boards and/or as a consultant for Alector, Eisai, Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, Nervgen, AZTherapies, CogRx and Red Abbey Labs, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure and Biogen, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). KB has served as a consultant, at advisory boards, or at data monitoring committees for Abcam, Axon, Biogen, JOMDD/Shimadzu. Julius Clinical, Lilly, MagQu, Novartis, Prothena, Roche Diagnostics, and Siemens Healthineers, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program. CW and MT have received support from Codman/Integra for lecturing.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lukkarinen, H., Jeppsson, A., Wikkelsö, C. et al. Cerebrospinal fluid biomarkers that reflect clinical symptoms in idiopathic normal pressure hydrocephalus patients. Fluids Barriers CNS 19, 11 (2022). https://doi.org/10.1186/s12987-022-00309-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12987-022-00309-z