
Abstract
Background
Serum cholinesterase (ChE) is positively associated with incident diabetes and dyslipidemia. We aimed to investigate the relationship between ChE and the incidence of diabetic retinopathy (DR).
Methods
Based on a community-based cohort study followed for 4.6 years, 1133 participants aged 55–70 years with diabetes were analyzed. Fundus photographs were taken for each eye at both baseline and follow-up investigations. The presence and severity of DR were categorized into no DR, mild non-proliferative DR (NPDR), and referable DR (moderate NPDR or worse). Binary and multinomial logistic regression models were used to estimate the risk ratio (RR) and 95% confidence interval (CI) between ChE and DR.
Results
Among the 1133 participants, 72 (6.4%) cases of DR occurred. The multivariable binary logistic regression showed that the highest tertile of ChE (≥ 422 U/L) was associated with a 2.01-fold higher risk of incident DR (RR 2.01, 95%CI 1.01-4.00; P for trend < 0.05) than the lowest tertile (< 354 U/L). The multivariable binary and multinomial logistic regression showed that the risk of DR increased by 41% (RR 1.41, 95%CI 1.05–1.90), and the risk of incident referable DR was almost 2-fold higher than no DR (RR 1.99, 95%CI 1.24–3.18) with per 1-SD increase of loge-transformed ChE. Furthermore, multiplicative interactions were found between ChE and elderly participants (aged 60 and older; P for interaction = 0.003) and men (P for interaction = 0.044) on the risk of DR.
Conclusions
In this study, ChE was associated with the incidence of DR, especially referable DR. ChE was a potential biomarker for predicting the incident DR.
Similar content being viewed by others


Introduction
Diabetic retinopathy (DR) is a highly specific microvascular complication of diabetes [1]. DR reached the top 5 leading causes of blindness in adults aged 50 years and above in 2020 according to the report of the vision loss expert group of the Global Burden of Disease Study [2]. While great progress has been made in the treatment of DR in recent years, these treatments are costly, and the related side effects (such as infection, vitreous hemorrhage, etc.) are concerning [3]. With the aging population and the worldwide diabetes epidemic, DR has become and will continue to be a severe public health issue shared globally in the following decades.
Although glycemia, blood pressure, and lipids are traditional modifiable risk factors for DR [3], only 9% of DR progression and 10% of proliferative DR (PDR) incidence could be attributed to these factors reported in the Wisconsin Epidemiology Study of Diabetic Retinopathy (WESDR) [4]. Therefore, it is imperative to actively explore new and reliable biomarkers that can predict DR.
Serum cholinesterase (ChE) is an α glycoprotein synthesized by the liver and has two main forms: acetylcholinesterase (AChE) and butyrylcholinesterase (BChE) [5], and the majority found in human plasma is the latter (BChE: AChE = 412.5: 1) [6]. Clinically, the level of ChE sensitively reflects the synthetic function of the liver [5]. Previous case-control studies reported that serum or plasma ChE levels were significantly higher in participants with diabetes [7], hypertension [7], or diabetic peripheral neuropathy [8]. As for prospective cohort studies, serum BChE increased the risk of incident diabetes among Japanese men [9], and the risk of incident dyslipidemia in participants in a medical check-up center [10].
However, to the best of our knowledge, there have been no prospective population-based cohort studies exploring the relationship between serum ChE and incident DR. Based on a community-based cohort study, we prospectively (1) evaluated the association between baseline serum ChE and the risk of incident DR, including the severity of DR, (2) explored the potential interactions between ChE and metabolic disorders on the incidence of DR, and (3) compared the performances of the known DR predictive models with or without ChE.
Materials and methods
Participants and study design
The Shanghai Nicheng Cohort Study was a community-based cohort study. It has been well-documented in previous literature [11]. In brief, the purpose of this cohort was to evaluate the epidemiological characteristics of cardiovascular metabolic diseases in the Chinese population. The baseline survey was launched between April 2013 and August 2014. Individuals aged 55–70 years old at baseline were invited to the follow-up survey in 2018.
The inclusion criteria were met if the participants were 55–70 years old, were diagnosed with diabetes, and had complete fundus photos and ChE data at baseline. The exclusion criteria for the participants included having retinopathy at baseline (including DR, retinitis pigmentosa, hypertensive retinopathy, glaucoma, macular degeneration, and white dot syndrome); taking drugs that affected ChE (including ChE inhibitors, lipid-lowering treatments, and liver-protecting drugs) two weeks before the baseline survey; severe impairment of liver function (alanine aminotransferase [ALT] or aspartate aminotransferase [AST] exceeded 2 times the upper limit of the detection range); having histories of a cardiovascular or malignant tumor at baseline; missing fundus photographs in the follow-up survey. To sum up, we included 2442 participants in this study. 1753 participants finished the follow-up investigation (the follow-up rate was 71.8%). Finally, 1133 participants with diabetes were analyzed in this study (Additional file 1).
Anthropometric and biochemical indicators
During the baseline and follow-up investigation, the standard questionnaire was used to collect data regarding demographics, lifestyles, disease histories, and other information. The collection of biochemical and anthropometric indicators (including height, weight, and blood pressure) has been described in detail [11]. Current smokers were defined as people who have smoked at least one cigarette a day in the past year. Current drinkers were defined as individuals who had consumed at least 1 g of alcohol per week in the last 1 year. Body mass index (BMI) was the ratio of weight (kg) to the square of height (m).
After at least 10 h of overnight fasting, blood samples were obtained from each participant. The serum ChE was detected using the L-type ChE assay kit (produced by the FUJIFILM Wako Pure Chemical Corporation), with the methylthiophenecarbonylthiocholine as the substrate. The lowest detectable level was 203 U/L and the range of interassay variation was 0.58–1.11%. Fasting plasma glucose (FPG) and 2-h plasma glucose (2-h PG) were tested by the glucose oxidase method. Hemoglobin A1c (HbA1c) was tested by high-performance liquid chromatography. Fasting insulin (FINS) was measured by electrochemiluminescence immunoassay. Triglyceride (TG) and total cholesterol (TC) were determined using the enzymatic colorimetric method. Low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) were assessed by the direct method. Urine creatinine and urine albumin were tested by the sarcosine oxidase-PAP method and rate nephelometry assay, respectively. ALT, AST, and γ-glutamine transferase (GGT) were determined using the ultraviolet-lactate dehydrogenase method, ultraviolet-malic dehydrogenase method, and γ-glutamyl-p-nitroaniline method, respectively. The calculation formula of homeostasis model assessment-insulin resistance (HOMA-IR) was FINS (mU/L) × FPG (mmol/L) /22.5 [12]. The estimated glomerular filtration rate (eGFR) was computed by the Chronic Kidney Disease Epidemiology Collaboration equation [13].
Assessment and definition of the outcome
Before the fundus photography, participants were required to rest in a dark room for a moment to allow their pupils to dilate naturally. Non-mydriatic cameras (baseline: Canon CR6 45NM; follow-up: TOPCON TRC-NW400) were used to take photographs of each eye. The photographs were evaluated by two experienced and qualified ophthalmologists who were masked regarding the health status of participants, and inconsistent results were verified by a third ophthalmologist. The DR score was based on their worse eye.
Based on the diagnosis criteria of the American Diabetes Association, participants who had a history of diabetes, FPG ≥ 126 mg/dL, 2-h PG ≥ 200 mg/dL, and/or HbA1c ≥ 6.5% were diagnosed with diabetes [14]. The presence and severity of DR were graded according to the International Clinical Diabetic Retinopathy Disease Severity Scales [15]. Referable DR was defined as moderate non-proliferative DR (NPDR) or worse [16].
Statistical analysis
The Kolmogorov-Smirnov test showed that the distribution of all continuous variables were skewed. Thus, the continuous variables were shown as median (25th-75th percentile), and the categorical variables were shown as numbers (proportions). The comparisons of the distributions of continuous variables were using the Wilcoxon rank test or Kruskal-Wallis test, and for categorical variables, the chi-square test or Fisher exact test was used as appropriate. To compare the ChE levels among different DR severity groups, least squares mean and standard errors of loge-transformed ChE were calculated using the analysis of covariance adjusted for related factors, and the trend was tested using linear regression. The Spearman and partial correlation analyses were used to estimate the correlations between ChE and baseline clinical measurements, respectively. Multivariable binary logistic regression was used to evaluate the risk ratios (RR) and 95% confidence intervals (CI) for the risk of DR with the ChE tertiles. The linear trend between ChE levels and incident DR was tested using the median of ChE in each tertile group as a continuous variable with the binary logistic regression analysis. Meanwhile, we evaluated the effect of per 1-SD increase of loge-transformed ChE using both the binary and multinomial logistic regression models. The selection of confounders in the regression models was based on: risk factors of DR; factors related to ChE or DR; biological interests (ALT, reflecting the liver function; HbA1c, directly affecting ChE level). Moreover, We separately conducted the stratified analyses by sex, family history of diabetes, and the cut-off points of age (60 and 65 years old), BMI (24 kg/m2), HbA1c (6.5%), TG (150 mg/dL), and LDL-C (100 mg/dL). We also simultaneously included ChE, the aforementioned categorical variables, and their product term in the logistic regression to estimate the multiplicative interaction.
In addition, we evaluated the area under the receiver operating characteristic curve (AUC), integrated discrimination improvement (IDI), relative IDI (rIDI), and net reclassification improvement (NRI) to assess the predictive ability of the models with or without ChE. Both IDI and rIDI could measure the discrimination value of the predictive models and NRI could assess the improvement in the disease reclassification after the addition of ChE [17, 18]. We used two predictive models established previously [19, 20]. Model 1 included sex, diabetes duration, HbA1c, systolic blood pressure (SBP), albuminuria, creatinine clearance, and glucose-lowering treatment [19]. Model 2 included age, diabetes duration, 2-h PG, HbA1c, urine creatinine, albuminuria, and SBP [20].
All the statistical analyses were performed using the SAS software (vision 9.4). A two-tailed P < 0.05 was considered statistically significant.
Results
Among the 1133 individuals with diabetes, the median age was 61.8 years old (25th-75th percentile, 58.9–65.3), and 60.1% were women. Of them, 32.2% had known diagnosed diabetes, and 15.4% had diabetes duration over 5 years (Table 1). Participants in the highest ChE tertile group were younger, and had higher glycemia levels, FINS, HOMA-IR, lipid levels, eGFR, UCAR, ALT, GGT, BMI, and blood pressure levels. Moreover, they had higher proportions of women and glucose-lowering treatment, but a lower proportion of current smokers (Additional file 2: Table S1). Furthermore, the Spearman partial correlation analyses between baseline serum ChE and clinical characteristics showed that after adjustment for age and sex, ChE was moderately correlated with TG, HOMA-IR, and FINS (range of r from 0.34 to 0.43). In contrast, ChE was negatively correlated with HDL-C (r = -0.16, P < 0.001) (Additional file 3: Table S2).
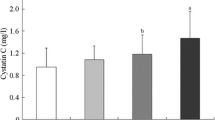
After a mean 4.6-year follow-up, 72 (6.4%) were diagnosed with incident DR, of which 45 were mild NPDR (4.0%) and 27 were referable DR (2.4%). The baseline ChE level was significantly higher in the participants with incident DR (P = 0.036), particularly in individuals with referable DR (P for trend = 0.012) (Fig. 1). In addition, the multivariable logistic regression analyses showed that baseline serum ChE was positively associated with incident DR, particularly referable DR (Fig. 2). In the binary logistic regression analyses, compared with the lowest ChE tertile group, the highest ChE tertile group had a 2.01-fold higher risk of incident DR (RR 2.01, 95%CI 1.01-4.00). A linear association was found between ChE and DR risk (P for trend < 0.05). In addition, each 1-SD increase of loge-transformed ChE was associated with a 41% higher risk of incident DR (RR 1.41, 95%CI 1.05–1.90) (Fig. 2A). Furthermore, in the multinomial logistic regression analyses, the higher level of ChE was associated with a higher risk of referable DR (RR 1.99, 95%CI 1.24–3.18) compared with the no DR group, but not significant in the mild NPDR group (RR 1.22, 95% CI 0.84–1.76) (Fig. 2B).

The least-square means of ChE by the presence and severity of DR groups. The least-square means of loge-transformed ChE with standard errors were presented as dot and error bars after adjustment for age, sex, BMI, SBP, smoking and drinking status, family history of diabetes, duration of diabetes, glucose-lowering treatment, HbA1c, ALT, TG, LDL-C, and eGFR. Abbreviations: DR, diabetic retinopathy; ChE, cholinesterase; RR, risk ratio; CI, confidence interval; BMI, body mass index; SBP, systolic blood pressure; HbA1c, hemoglobin A1c; ALT, alanine aminotransferase; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate

ChE and risks of incidence and severity of DR. (A) ChE and incidence of DR using the binary logistic regression. (B) ChE and severity of DR using the multinomial logistic regression. *P for trend was tested using the median of each group as a continuous variable in the logistic regression. All P for trend was < 0.05. † Model 1 was adjusted for age and sex. ‡ Model 2 was adjusted for age, sex, BMI, SBP, smoking and drinking status, family history of diabetes, diabetes duration, and glucose-lowering treatment. § Model 3 was adjusted for age, sex, BMI, SBP, smoking and drinking status, family history of diabetes, duration of diabetes, glucose-lowering treatment, HbA1c, ALT, TG, LDL-C, and eGFR. ¶ The effect was scaled by the 1-SD increase of loge-transformed ChE. Abbreviations: DR, diabetic retinopathy; ChE, cholinesterase; RR, risk ratio; CI, confidence interval; BMI, body mass index; SBP, systolic blood pressure; HbA1c, hemoglobin A1c; ALT, alanine aminotransferase; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate
Stratified analyses of two strata showed that the associations between ChE and incident DR were significantly positive in the strata of men, with a family history of diabetes, with age ≥ 65 years old, BMI ≥ 25 kg/m2, HbA1c ≥ 6.5%, or TG ≥ 150 mg/dL, but not significant in their corresponding other strata. However, significant multiplicative interactions of ChE with sex and ageing (cutoff point: 60) on incident DR were found (Ps for interaction: 0.044 and 0.003) (Fig. 3).

Stratified analyses of the risk of incident DR according to per 1-SD increase of loge-transformed ChE. Models were adjusted for age, sex, BMI, SBP, smoking and drinking status, family history of diabetes, duration of diabetes, glucose-lowering treatment, HbA1c, ALT, TG, LDL-C, and eGFR. Abbreviations: DR, diabetic retinopathy; ChE, cholinesterase; RR, risk ratio; CI, confidence interval; BMI, body mass index; SBP, systolic blood pressure; HbA1c, hemoglobin A1c; ALT, alanine aminotransferase; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate
Finally, there were no significant differences in the AUCs of the models before or after adding ChE to the established models (model 1: 0.65 [95% CI 0.59–0.71], model 1 + ChE: 0.67 [95% CI 0.60–0.73], P = 0.320; model 2: 0.65 [95% CI 0.60–0.71], model 2 + ChE: 0.66 [95% CI 0.60–0.72], P = 0.686). However, with additional ChE in the two models, IDI, rIDI, and NRI were improved: both IDI in the two models increased by 0.01; model 1, rIDI (0.36, P = 0.024) and NRI (0.31, P = 0.010); model 2, rIDI (0.54, P = 0.019) and NRI (0.27, P = 0.025) (Table 2).
Discussion
To our knowledge, this was the first prospective observational cohort study to investigate the serum ChE levels and incident DR. After a mean 4.6-year follow-up, in the middle-aged and older Chinese people with diabetes, higher ChE levels were associated with higher risks of incident DR and referable DR: a 2.01-fold higher risk of DR in the highest tertile versus the lowest tertile, 1.41-fold higher DR risk and an almost 2-fold higher risk of referable DR per 1-SD increase of loge-transformed ChE. Moreover, both the male sex and the elderly aged 60 and over had significantly stronger associations between ChE and incident DR than their counterparts. Furthermore, ChE improved the IDI, rIDI, and NRI of the established predictive models, thus, the predictive models with the addition of ChE had better discrimination and significant improvement in diabetic retinopathy reclassification.
The WESDR study indicated that only 9% of the development of DR and 10% of the incidence of PDR were attributed to HbA1c, blood pressure, and TC [4]. Our study demonstrated that when ChE was taken into account with traditional risk factors in the two established models, the predictive abilities improved, with both the IDI improving by 0.01, rIDI improving by 0.36 and 0.54, and the NRI improving by 0.31 and 0.27, respectively [19, 20]. The incremental predictive ability possessed by ChE may be explained by both metabolic and neurological aspects. Consistent with several previous population-based studies [21, 22], we observed that higher ChE was accompanied by worse metabolic profiles: TG, HOMA-IR, and FINS were moderately correlated with ChE. Meanwhile, it has been proposed that DR is not only regarded as a microvascular but also a neurodegenerative disease [23]. Interestingly, recent research revealed that ChE was involved in the process of neurological diseases [24]. Hence, ChE could be regarded as an integrative factor that reflects both the metabolic status and the function of the nervous system.
In particular, another important finding was that elevated ChE was associated with referable DR. As stated by some organizations, including the Chinese Diabetes Society, the presence of referable DR required interventions from professional ophthalmologists [16, 25]. However, with the global epidemic of diabetes, ophthalmology services are overwhelmed. Although the technologies of artificial intelligence have developed in detecting DR in recent years, it still takes time to be widely promoted [26, 27]. Also, the current treatments are mainly for those with advanced stages of DR, and they may not be effective for everyone [3]. Therefore, our study suggested that the testing of ChE, a clinically easily detectable indicator, could facilitate the early identification of people at high risk of developing referable DR. The sooner an individual with high risk is identified, the sooner interventions can be made, and the less likely it is the person will face the dilemma of blindness. Further observational studies with larger samples are still needed to explore the relationship between ChE and more severe DR stages, like vision-threatening DR (severe NPDR or worse) or even PDR.
The association between ChE and DR did not attenuate even after adjustment for TG, LDL-C, and HbA1c in the regression model, which indicated that there were other possible mechanisms independent of glucose and lipid profiles. The substrates of ChE may be used to explain related mechanisms. ChE could hydrolyze acetylcholine (ACh), and BChE could hydrolyze ghrelin specifically [28, 29]. By hydrolyzing ACh, ChE may influence retinal neuron function [30], blood flow conditions [31, 32], and retinal inflammation [33,34,35]. Moreover, by hydrolyzing ghrelin, BChE could lessen its retinal protective effects, like inhibiting hyperglycemia-induced cell death, reducing the production of reactive oxygen species, and protecting retinal function and structure [36]. On the other hand, in animal experiments, the application of ChE inhibitors could prevent the decrease in retinal thickness and significantly improve retinal blood flow [30, 32]. Nonetheless, the potential mechanisms between ChE and DR have not been fully elaborated. Further interventional trials should be actively conducted to target ChE on preventing or delaying DR, which should be expected to relieve the burdens from both the personal perspective and the social perspective.
The causal role of hyperglycemia in DR has been demonstrated by numerous large-scale cohort studies [1]. Besides, some population-based observational studies reported that ChE was positively correlated with glucose profiles [21, 22]. Also, an in vitro study using the serum from healthy controls showed that the ChE activity elevated with increasing glucose gradients [7]. These all suggested that higher ChE often accompanied higher blood glucose levels. A randomized control trial revealed that the ChE inhibitor galantamine could lower the level of TNF, a molecule that contributed to insulin resistance, and also significantly lower plasma insulin and HOMA-IR in patients with metabolic syndrome [37]. This trial suggested that ChE might be involved in insulin resistance. However, the multiplicative interaction was not statistically significant. This was probably due to the small cases in each subgroup. Further studies are needed to evaluate how metabolic indicators including HbA1c interact with ChE in developing DR.
Although age was reported to not be associated with cholinesterase levels [38], aging itself could lead to changes in the retina, such as reduced blood flow and retinal thinning [39]. In this study, the interaction between ChE and age was only observed in participants aged 60 and older, but not in those aged 65 and older. The small cases may contribute to this result. More studies are needed to elaborate on our results.
Besides, this study revealed that men had statistically significant multiplicative interaction with the association between ChE and incident DR. Intriguingly, consistent with previous studies, among participants with age over 55, ChE was higher in women than men [40]. However, our results showed that men had higher FPG and diastolic blood pressure, lower FINS, worse renal function, and had less healthy lifestyles with respect to smoking, drinking, and physical activity (Additional file 4: Table S3). These adverse factors were reported to be correlated with DR [3]. Meanwhile, men seemed to be more susceptible to DR than women. In individuals with diabetes but without DR, women had significantly lower concentrations of inflammation-associated proteins in aqueous humor than men [41]. Moreover, a case-control study based on 70 adults with type 2 diabetes found that characteristics of neuroretinal function were more abnormal in men than women, like the delayed implicit time of the retinal locations [42]. All in all, the variation in the pathophysiological mechanism of DR between women and men remains an essential area for future research.
This is the first community-based cohort study to explore the association between ChE and incident DR. Fundus photographs were reviewed by professional and experienced ophthalmologists, so the diagnosis of DR was objective and reliable. Our limitations in this study are as follows: first, our study was conducted on Chinese middle-aged and elderly people, so the extrapolation of the findings is limited. Second, we did not identify sufficient cases of DR because of the relatively short follow-up period. Consequently, our results should be interpreted with caution.
In this study, we found that higher levels of serum ChE increased the risk of DR. ChE may be a promising biomarker for DR prevention, particularly referable DR. We could better pinpoint the population at high risk for DR when ChE was taken into account. Further studies are needed to further validate the causality between serum ChE of DR, and confirm whether ChE could be a potential therapeutic target for DR.
Data availability
The datasets analysed during the current study are not publicly available due the privacy constraints, but are available from the corresponding author on reasonable request.
Abbreviations
- ChE:
-
cholinesterase
- DR:
-
diabetic retinopathy
- PDR:
-
proliferative diabetic retinopathy
- NPDR:
-
non-proliferative diabetic retinopathy
- AChE:
-
acetylcholinesterase
- BChE:
-
butyrylcholinesterase
- ALT:
-
alanine aminotransferase
- AST:
-
aspartate aminotransferase
- BMI:
-
body mass index
- FPG:
-
fasting plasma glucose
- 2-h PG:
-
2-h plasma glucose
- HbA1c:
-
hemoglobin A1c
- FINS:
-
fasting insulin
- TG:
-
triglyceride
- TC:
-
total cholesterol
- LDL-C:
-
low-density lipoprotein cholesterol
- HDL-C:
-
high-density lipoprotein cholesterol
- GGT:
-
γ-glutamine transferase
- HOMA-IR:
-
homeostasis model assessment-insulin resistance
- eGFR:
-
estimated glomerular filtration rate
- UACR:
-
urinary albumin creatinine ratio
- SBP:
-
systolic blood pressure
- RR:
-
risk ratios
- CI:
-
confidence intervals
- AUC:
-
area under the receiver operating characteristic curve
- rIDI:
-
relative integrated discrimination improvement
- NRI:
-
net reclassification improvement
- SBP:
-
systolic blood pressure.
References
Solomon SD, Chew E, Duh EJ, Sobrin L, Sun JK, VanderBeek BL, et al. Diabetic Retinopathy: A position Statement by the American Diabetes Association. Diabetes Care. 2017;40(3):412–418. https://doi.org/10.2337/dc16-2641.
GBD 2019 Blindness and Vision Impairment Collaborators. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to Sight: an analysis for the global burden of Disease Study. Lancet Glob Health. 2021;9(2):e144–e160. https://doi.org/10.1016/s2214-109x(20)30489-7.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Diabet Retinopathy Preferred Pract Pattern®. Ophthalmol. 2020;127(1):p66–p145. https://doi.org/10.1016/j.ophtha.2019.09.025.
Klein R. The Epidemiology of Diabetic Retinopathy. In: Duh, Elia, editors. Diabetic Retinopathy. Totowa: Humana Press; 2008. pp. 67–107.
Santarpia L, Grandone I, Contaldo F, Pasanisi F. Butyrylcholinesterase as a prognostic marker: a review of the literature. J Cachexia Sarcopenia Muscle. 2013;4(1):31–39. https://doi.org/10.1007/s13539-012-0083-5.
Brimijoin S, Hammond P. Butyrylcholinesterase in human brain and acetylcholinesterase in human plasma: trace enzymes measured by two-site immunoassay. J Neurochem. 1988;51(4):1227–1231. https://doi.org/10.1111/j.1471-4159.1988.tb03091.x.
Inácio Lunkes G, Stefanello F, Sausen Lunkes D, Maria Morsch V, Schetinger MR, Gonçalves JF. Serum cholinesterase activity in diabetes and associated pathologies. Diabetes Res Clin Pract. 2006;72(1):28–32. https://doi.org/10.1016/j.diabres.2005.08.009.
Sykam A, Gutlapalli VR, Tenali SP, Meena AK, Chandran P, Suneetha S, et al. Anticeramide antibody and butyrylcholinesterase in peripheral neuropathies. J Clin Neurosci. 2017;42:204–208. https://doi.org/10.1016/j.jocn.2017.04.023.
Sato KK, Hayashi T, Maeda I, Koh H, Harita N, Uehara S, et al. Serum butyrylcholinesterase and the risk of future type 2 diabetes: the Kansai Healthcare Study. Clin Endocrinol (Oxf). 2014;80(3):362–367. https://doi.org/10.1111/cen.12171.
Oda E. Associations between serum cholinesterase and incident hyper-LDL cholesterolemia, hypertriglyceridemia and hypo-HDL cholesterolemia as well as changes in lipid levels in a health screening population. Atherosclerosis. 2015;241(1):1–5. https://doi.org/10.1016/j.atherosclerosis.2015.04.804.
Chen P, Hou X, Hu G, Wei L, Jiao L, Wang H, et al. Abdominal subcutaneous adipose tissue: a favorable adipose depot for diabetes? Cardiovasc Diabetol. 2018;17(1):93. https://doi.org/10.1186/s12933-018-0734-8.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. https://doi.org/10.1007/bf00280883.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12. https://doi.org/10.7326/0003-4819-150-9-200905050-00006.
American Diabetes Association Professional Practice Committee. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Suppl 1):s17–s38. https://doi.org/10.2337/dc22-S002.
Wilkinson CP, Ferris FLr, Klein RE, Lee PP, Agardh CD, Davis M, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110(9):1677–1682. https://doi.org/10.1016/s0161-6420(03)00475-5.
Draznin B, Aroda VR, Bakris G, Benson G, Brown FM, Freeman R, et al. 12. Retinopathy, Neuropathy, and Foot Care: Standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Suppl 1):s185–s194. https://doi.org/10.2337/dc22-S012.
Pencina MJ, D’Agostino RB, Sr DARB Jr, Vasan RS. Comments on ‘Integrated discrimination and net reclassification improvements—practical advice’. Stat Med. 2008;27(2):207–212. https://doi.org/10.1002/sim.3106.
Kennedy KF, Pencina MJ, editors. A SAS ® Macro to Compute Added Predictive Ability of New Markers Predicting a Dichotomous Outcome2010.
Semeraro F, Parrinello G, Cancarini A, Pasquini L, Zarra E, Cimino A, et al. Predicting the risk of diabetic retinopathy in type 2 diabetic patients. J Diabetes Complications. 2011;25(5):292–297. https://doi.org/10.1016/j.jdiacomp.2010.12.002.
Mo R, Shi R, Hu Y, Hu F. Nomogram-Based prediction of the risk of Diabetic Retinopathy: a retrospective study. J Diabetes Res. 2020;2020:7261047. https://doi.org/10.1155/2020/7261047.
Iwasaki T, Yoneda M, Nakajima A, Terauchi Y. Serum butyrylcholinesterase is strongly associated with adiposity, the serum lipid profile and insulin resistance. Intern Med. 2007;46(19):1633–1639. https://doi.org/10.2169/internalmedicine.46.0049.
Randell EW, Mathews MS, Zhang H, Seraj JS, Sun G. Relationship between serum butyrylcholinesterase and the metabolic syndrome. Clin Biochem. 2005;38(9):799–805. https://doi.org/10.1016/j.clinbiochem.2005.04.008.
Simó R, Stitt AW, Gardner TW. Neurodegeneration in diabetic retinopathy: does it really matter? Diabetologia. 2018;61(9):1902–1912. https://doi.org/10.1007/s00125-018-4692-1.
Hampel H, Mesulam MM, Cuello AC, Farlow MR, Giacobini E, Grossberg GT, et al. The cholinergic system in the pathophysiology and treatment of Alzheimer’s disease. Brain. 2018;141(7):1917–1933. https://doi.org/10.1093/brain/awy132.
Jia W, Weng J, Zhu D, Ji L, Lu J, Zhou Z, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158. https://doi.org/10.1002/dmrr.3158.
Ting DSW, Cheung CY, Lim G, Tan GSW, Quang ND, Gan A, et al. Development and validation of a Deep Learning System for Diabetic Retinopathy and Related Eye Diseases using retinal images from multiethnic populations with diabetes. JAMA. 2017;318(22):2211–2223. https://doi.org/10.1001/jama.2017.18152.
Dai L, Wu L, Li H, Cai C, Wu Q, Kong H, et al. A deep learning system for detecting diabetic retinopathy across the disease spectrum. Nat Commun. 2021;12(1):3242. https://doi.org/10.1038/s41467-021-23458-5.
De Vriese C, Gregoire F, Lema-Kisoka R, Waelbroeck M, Robberecht P, Delporte C. Ghrelin degradation by serum and tissue homogenates: identification of the cleavage sites. Endocrinology. 2004;145(11):4997–5005. https://doi.org/10.1210/en.2004-0569.
Mesulam MM, Guillozet A, Shaw P, Levey A, Duysen EG, Lockridge O. Acetylcholinesterase knockouts establish central cholinergic pathways and can use butyrylcholinesterase to hydrolyze acetylcholine. Neuroscience. 2002;110(4):627–639. https://doi.org/10.1016/s0306-4522(01)00613-3.
Zaitone SA, Alshaman R, Alattar A, Elsherbiny NM, Abogresha NM, El-Kherbetawy MK, et al. Retinoprotective effect of donepezil in diabetic mice involves mitigation of excitotoxicity and activation of PI3K/mTOR/BCl(2) pathway. Life Sci. 2020;262:118467. https://doi.org/10.1016/j.lfs.2020.118467.
Gericke A, Sniatecki JJ, Goloborodko E, Steege A, Zavaritskaya O, Vetter JM, et al. Identification of the muscarinic acetylcholine receptor subtype mediating cholinergic vasodilation in murine retinal arterioles. Invest Ophthalmol Vis Sci. 2011;52(10):7479–7484. https://doi.org/10.1167/iovs.11-7370.
Almasieh M, MacIntyre JN, Pouliot M, Casanova C, Vaucher E, Kelly ME, et al. Acetylcholinesterase inhibition promotes retinal vasoprotection and increases ocular blood flow in experimental glaucoma. Invest Ophthalmol Vis Sci. 2013;54(5):3171–3183. https://doi.org/10.1167/iovs.12-11481.
Egea J, Buendia I, Parada E, Navarro E, León R, Lopez MG. Anti-inflammatory role of microglial alpha7 nAChRs and its role in neuroprotection. Biochem Pharmacol. 2015;97(4):463–472. https://doi.org/10.1016/j.bcp.2015.07.032.
Patel H, McIntire J, Ryan S, Dunah A, Loring R. Anti-inflammatory effects of astroglial α7 nicotinic acetylcholine receptors are mediated by inhibition of the NF-κB pathway and activation of the Nrf2 pathway. J Neuroinflammation. 2017;14(1):192. https://doi.org/10.1186/s12974-017-0967-6.
Stitt AW, Curtis TM, Chen M, Medina RJ, McKay GJ, Jenkins A, et al. The progress in understanding and treatment of diabetic retinopathy. Prog Retin Eye Res. 2016;51:156–186. https://doi.org/10.1016/j.preteyeres.2015.08.001.
Bai J, Yang F, Wang R, Yan Q. Ghrelin ameliorates Diabetic Retinal Injury: potential therapeutic avenues for Diabetic Retinopathy. Oxid Med Cell Longev. 2021;2021:8043299. https://doi.org/10.1155/2021/8043299.
Consolim-Colombo FM, Sangaleti CT, Costa FO, Morais TL, Lopes HF, Motta JM, et al. Galantamine alleviates inflammation and insulin resistance in patients with metabolic syndrome in a randomized trial. JCI Insight. 2017;2(14):e93340. https://doi.org/10.1172/jci.insight.93340.
Abou-Hatab K, O’Mahony MS, Patel S, Woodhouse K. Relationship between age and plasma esterases. Age Ageing. 2001;30(1):41–45. https://doi.org/10.1093/ageing/30.1.41.
Leley SP, Ciulla TA, Bhatwadekar AD. Diabetic Retinopathy in the Aging Population: a perspective of Pathogenesis and Treatment. Clin Interv Aging. 2021;16:1367–1378. https://doi.org/10.2147/cia.S297494.
Lepage L, Schiele F, Gueguen R, Siest G. Total cholinesterase in plasma: biological variations and reference limits. Clin Chem. 1985;31(4):546–550.
Haq Z, Yang D, Psaras C, Stewart JM. Sex-based analysis of potential inflammation-related protein biomarkers in the aqueous humor of patients with diabetes Mellitus. Transl Vis Sci Technol. 2021;10(3):12. https://doi.org/10.1167/tvst.10.3.12.
Ozawa GY, Bearse MA Jr, Bronson-Castain KW, Harrison WW, Schneck ME, Barez S, et al. Neurodegenerative differences in the retinas of male and female patients with type 2 diabetes. Invest Ophthalmol Vis Sci. 2012;53(6):3040–3046. https://doi.org/10.1167/iovs.11-8226.
Acknowledgements
Not applicable.
Funding
This work was supported by the Shanghai Key Clinical Center for Metabolic Disease (No. 2017ZZ01013), Shanghai Municipal Key Clinical Specialty, National Science Foundation of China-National Health and Medical Research Council joint research grant (No. 81561128016), and the Shanghai Natural Science Foundation (No. 18ZR1429000).
Author information
Authors and Affiliations
Contributions
R.Y. and X.Y. performed the literature search, analyzed and interpreted the data, and drafted the manuscript. X.W., Q.W., and L.J. collected, verified, and interpreted the data reported. K.D. and Z.Z. contributed to the data collection. Y.B. contributed to the design of this study and data interpretation. W.P. and X.H. designed this study, interpreted the data, revised the manuscript. All authors reviewed and approved the final version of the manuscript. W.J. and X.H. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the Shanghai Sixth People’s Hospital, China (approval number: 2015-27).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yu, R., Ye, X., Wang, X. et al. Serum cholinesterase is associated with incident diabetic retinopathy: the Shanghai Nicheng cohort study. Nutr Metab (Lond) 20, 26 (2023). https://doi.org/10.1186/s12986-023-00743-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12986-023-00743-2