
Abstract
Background
Spasticity is defined as “a motor disorder characterised by a velocity dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks”. It is a highly prevalent condition following stroke and other neurological conditions. Clinical assessment of spasticity relies predominantly on manual, non-instrumented, clinical scales. Technology based solutions have been developed in the last decades to offer more specific, sensitive and accurate alternatives but no consensus exists on these different approaches.
Method
A systematic review of literature of technology-based methods aiming at the assessment of spasticity was performed. The approaches taken in the studies were classified based on the method used as well as their outcome measures. The psychometric properties and usability of the methods and outcome measures reported were evaluated.
Results
124 studies were included in the analysis. 78 different outcome measures were identified, among which seven were used in more than 10 different studies each. The different methods rely on a wide range of different equipment (from robotic systems to simple goniometers) affecting their cost and usability. Studies equivalently applied to the lower and upper limbs (48% and 52%, respectively). A majority of studies applied to a stroke population (N = 79). More than half the papers did not report thoroughly the psychometric properties of the measures. Analysis identified that only 54 studies used measures specific to spasticity. Repeatability and discriminant validity were found to be of good quality in respectively 25 and 42 studies but were most often not evaluated (N = 95 and N = 78). Clinical validity was commonly assessed only against clinical scales (N = 33). Sensitivity of the measure was assessed in only three studies.
Conclusion
The development of a large diversity of assessment approaches appears to be done at the expense of their careful evaluation. Still, among the well validated approaches, the ones based on manual stretching and measuring a muscle activity reaction and the ones leveraging controlled stretches while isolating the stretch-reflex torque component appear as the two promising practical alternatives to clinical scales. These methods should be further evaluated, including on their sensitivity, to fully inform on their potential.
Similar content being viewed by others

Background
The definition of spasticity has long been debated in published studies and amongst clinicians. This definition has sometime encompassed any increase in muscle tone of various physiological origins, whether they are constant (and then referred to simply as “tone”, “hyper-resistance” or “hyper-tonicity”) or are only velocity-dependent (and in which case are due to an exaggerated stretch-reflex) [1]. Still, the more commonly used definition—adopted in this work—remains the more specific one proposed by Lance in 1980: “a motor disorder characterised by a velocity dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one component of the upper motor neuron syndrome” [2]. This definition has been recently confirmed and updated by a European consensus, stating that “spasticity refers to velocity dependent stretch hyperreflexia as part of hyper-resistance” [3]. These definitions should still be taken with care when considering the measurement modality and procedure used. Indeed, Lance’s definition was primarily derived from muscle activity observations, while today clinical practices rely on the measure of an exaggerated force or torque response (e.g. a catch angle). In addition, a continuous velocity-dependent torque response has also been recently demonstrated for the elbow joint by McPherson et al. [4]. Overall, past the phenomenon definition, it remains unclear as to which modality is appropriate to characterise spastic responses.
Significance of spasticity and its assessment
Spasticity is a highly prevalent symptom in people suffering a neurological injury, with estimates ranging from 30 to 80% after stroke [5]. Upper limb spasticity following a stroke affects a large number of individuals in the chronic phase [6] and is strongly correlated with post-stroke pain [7] and limitation of patient’s engagement in rehabilitation [8, 9]. The socioeconomic burden for those with post-stroke spasticity is estimated to be four times greater than for stroke survivors without spasticity [10]. Therefore, effective management of post-stroke spasticity remains a critical issue of importance in the field of neurological rehabilitation [11]. However, measuring effectiveness of treatments requires sensitive, valid and reliable assessment tools.
The Modified Ashworth Scale (MAS) and Modified Tardieu Scale (MTS) are the more commonly used measures of spasticity in clinical practice [12]. These measures have important limitations, especially the limited ability to distinguish between spasticity—velocity dependent and of neural origin, as per Lance’s definition—on one hand and tone or stiffness—of non-neural origin—on the other hand. The importance of this differentiation has been recently stressed by a European consensus [3].
Specifically, the MAS rates the reaction of the assessed muscle to stretch using a six point scale [13]. The measure evaluates the resistance torque at a single, approximately defined stretching velocity, so it cannot capture the velocity-dependent component of spasticity. The MAS has also been shown to have only moderate intra-rater and inter-rater reliabilities, leading to questions regarding the overall validity of this tool in the measurement of spasticity [14]. The MTS [15] has been recommended as a more appropriate measurement of spasticity [16]. Like the MAS, this tool rates the reaction of the affected muscle using a Likert scale from 0—no resistance to 4—unfatigable clonus. The primary difference between the two measures is that the MTS explicitly considers velocity-dependent characteristics by requiring the clinicians to stretch the joint at two different velocities, “as slow as possible” and “as fast as possible” [17]. However, the MTS does not fully reflect the variation of the intensity of the stretch induced by the velocity as the scale is only based on the angles at which the muscle reaction occurs. Its sensitivity is also limited by the ability of the rater to evaluate the reflex torques accurately and its inter-rater reliability is dependent on the experience of the clinician [15].
Technology assisted assessments
Given the importance of spasticity evaluation and its relevance to motor impairment and rehabilitation, together with the stated limitations of the existing clinical scales, many attempts have been made to offer efficient and reliable technological solutions to this evaluation. Two main classes of systems have been developed since the late 1980s [18, 19]: passive instruments, where the goal is to accurately measure the resistance force and/or muscle activity at a given joint which is manually stretched by a clinician; and active (i.e. robotic) devices which produce a controlled movement of a specific joint at several possible velocities while measuring the resistance force or muscle activity.
These techniques use a variety of different apparatus and propose a variety of different outcome measures but have often been individually evaluated, for different populations, different joints and often relatively low number of subjects, making it challenging to define and compare their clinical relevance. Many of these measures have not been adopted into clinical practice, possibly due to the complexity of their apparatus, amongst other factors. Indeed, studies have found that perceived ease of use and perceived usefulness are strong predictors of clinician likelihood to adopt such devices in practice [20]. It is to note that despite the aforementioned limitations, the MAS and MTS are simple and quick assessments to administer, potentially explaining their predominance against instrumented measures with lower usability.
Although two recent dedicated reviews [21, 22] investigated robotic-assisted methods for spasticity, the restriction of their scope to robotic systems does not allow for a full picture and comparison of existing methods. A more complete picture of the field is provided in a review of systematic reviews encompassing all assessment methods [23]. This review shows the overall limited evaluation of the existing assessments but does not propose a specific categorisation—and thus comparison—of the methods used. Additionally, none of these previous reviews address the question of the usability of the assessment methods which is a critical point for clinical adoption, especially in comparison to the widely used existing clinical scales which have the benefit of being cost-effective and easy to administer.
This systematic review thus proposes to identify existing technology-assisted methods aiming to assess the level of spasticity. A classification based on the method characteristics is then proposed, allowing for a usability comparison. Finally the psychometric properties of the different outcome measures are analysed. The review scope encompasses any limb and joint (or muscle) and any condition leading to spasticity, as the underlying mechanism of spasticity and its manifestation are expected to remain consistent across these conditions.
Methodology
Search and screening
A systematic literature review search was performed on the Medline, Embase and IEEEXplore databases. The search query was constructed to identify papers of which title or abstract contain at least one keyword of each of the three following groups: (1) spasticity, (2) assessment and (3) technology. The keywords of each group were defined as follows:
-
1
spastic* (spastic, spasticity), muscle tone, muscular tone, hyperton* (hypertonia, hypertonic, hypertonicity);
-
2
assess* (assess, assessment), measure* (measure, measurement), quanti* (quantify, quantification, quantitative);
-
3
technolog* (technology, technological), instrument* (instrument, instrumental, instrumented), mechatronic, mechanical, muscle activity measurement, electromyography, EMG, sEMG, inertial measurement unit, IMU, force sensor, dynamometer, ergometer, robot* (robot, robotic, robotics), kinematic* (kinematic, kinematics, kinematical).
Note that the key terms of group (1) deliberately included terms that may not be specific to spasticity as per Lance’s definition. These terms were included to ensure to not exclude valid studies using an inappropriate terminology. The construct validity of each measure was then evaluated in a second time, as explained below. The technology group (3) was constructed to include any mechatronic and/or sensor based systems.
The search was restricted to papers published after January 2000 to exclude older results leveraging outdated technology. Both journal articles and full-text conference proceedings written in English were included. Additional papers identified outside of the search were also included.
Eligibility was assessed based on the paper abstract to ensure that the reported study was specific to spasticity, or more generally to muscle tone, and applied to a neurologically injured population. Only papers directly aiming at the assessment of spasticity were considered. As such papers only reporting spasticity treatments or management methods were not included. Finally, it was ensured that the papers were using or proposing a technology-assisted measure. Typically, studies assessing psychometric properties of non-instrumented clinical measures (such as MAS or MTS) were excluded. Abstracts of identified papers were then screened independently by two reviewers (XG and RW) for eligibility. In case of disagreement, inclusion decision was made by a third reviewer (VC).
The PRISMA methodology [24] was used to report the literature review.
Data extraction and analysis
The full texts of the included papers were then analysed. The first objective was to characterise the spasticity assessment method used (or proposed). This step consisted of identifying the type of sensor(s) and device(s) used, the type of physiological measure(s), procedure, outcome measure and joint being assessed. When multiple outcome measures were proposed in the same study, only the one(s) claimed to be specific to spasticity by the authors were reported. When a paper presented several distinct assessment methodologies, these were considered independently. Conversely, when several papers were relative to the same assessment method, those were reported together.
The information extracted was used to populate a first table and further used to provide a full picture of technology-assisted assessments of spasticity.
The second step aimed at extracting, for each study, the relevant psychometric properties of the assessment and other information relative to its evaluation with the targeted population. When a study used more than one method, those were considered independently. Methods only tested with non-neurologically impaired populations were not considered at this stage. Specifically, information were sought regarding:
-
the targeted population;
-
the spasticity severity of the targeted population (in terms of a clinical score);
-
the sample size, assessed here as number of limbs tested and either belonging to the test population or control (including own control);
and on the reporting of the following five psychometric properties.
-
1
The construct validity, evaluating the specificity of the measure based on Lance’s and the European consensus definitions. Two aspects were sought for evaluation: (1) is the measure (and/or procedure) accounting for the velocity dependent aspect of the phenomenon (independently of the type of the outcome measure); and (2) is the measure (and/or procedure) attempting to isolate the stretch reflex from any voluntary muscle component and other joint passive resistance? This was thus rated from 0 to 2.
-
2
The discriminant validity, based on the existence of a control group/limb and ability of the measure to discriminate between these groups. This was rated as Significant, Conditionally Significant (under specific conditions) or Non-Significant.
-
3
The clinical (concurrent) validity, based on its correlation with the clinical measures reported as a Kappa, Spearman or Pearson correlation coefficients and rated from Very Weak to Very Strong [25, 26].
-
4
The reliability, based on a rating of the repeatability from Poor to Excellent (ICC [27]).
-
5
The sensitivity evaluation, reporting the Minimal Detectable Change (MDC) or similar measures.
The information, when available, was used to populate a second extraction table. This extraction was performed by one of the authors (XG) and discussed among all the authors in case of doubt.
Due to the heterogeneity of the data, no quality appraisal of the studies was performed but this information was further used to analyse how the different assessment methods—and outcome measure(s)—have been investigated along the different psychometric properties.
For the assessment methods with a construct validity of two out of two (thus specifically evaluating spasticity as a velocity-dependent increase of the stretch reflex) a usability evaluation was performed. The administration time, equipment cost and portability of the equipment necessary to these methods were estimated. The administration time was estimated by the authors based on the procedure description, the required instrumentation (such as EMG sensors placement or exoskeleton adjustment) and the number of movements/actions required (see Appendix, Table 5). The administration time was then classified as either:
-
comparable administration time to a MAS or MTS: less than 10 min;
-
equivalent to a typical intervention session: 10 to 30 min;
-
length of an extended session: 30 to 60 min or;
-
longer than an extended session: more than 60 min.
The equipment cost was estimated using the cost of a standard equivalent equipment (see Appendix, Table 6) and classified as either:
-
a disposable expense: less than $1000 USD;
-
an expense requiring a departmental funding: $1000 to $10,000 USD;
-
an expense requiring an institutional funding: $10,000 to $50,000 USD or;
-
an expense requiring a grant or special funding: more than $50,000 USD.
Portability was estimated based on the less portable piece of equipment and classified as either:
-
easily transportable (e.g. EMG sensors);
-
transportable from room-to-room (e.g. Ultra-Sound system on wheels) or;
-
not movable (e.g. BIODEX system).
Results

PRISMA diagram of the literature review
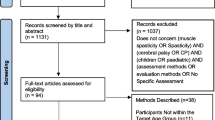
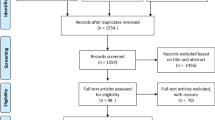
The search conducted in May 2021 identified 491 papers and six were added from other sources by the authors (see Fig. 1), 310 papers were excluded based on their abstract and 20 additional ones were excluded after a full-text review, leading to a total of 124 papers included in the analysis. During the screening phase, there was an agreement among the two reviewers on 384 papers whereas 70 required an arbitration.
Available assessment methods
In total, 120 different assessments were identified. The extraction table summarising the assessment methodologies presented in each paper is available as a supplementary material (Additional file 1).

Distributions of studies by a types of measurement (some studies use more than one type of measurement); b types of stretch used and breakdown of measurements for the two main stretch categories; c joint(s) on which the methods have been applied to; and d most commonly encountered outcome measures (some studies have several outcome measures). KI kinematic measure, MA muscle activity measure, FT force/torque measure, MP muscle property measure
Physiological measures
Four categories of physiological measures—and their combinations—used to produce the outcome measure were identified. They are summarised in Table 1.
A majority of studies used Kinematic measures (KI, N = 105), then Muscle Activity measures (MA, N = 83), then Force/Torque (FT, N = 64), and a few studies used intrinsic Muscle Properties (MP, N = 8) (see Fig. 2a). The most common combinations were Kinematic with Muscle Activity (N = 63), and Kinematic with Force/Torque (N = 56).
Stretching methods
Studies were further categorised based on the type of movement used defined in Table 2.
Most studies relied either on Manual stretching of the limb (N = 60) or on Controlled stretching movements (N = 45). Only a small number of studies (N = 14) relied on Voluntary movements. This last option has the disadvantage of not providing a standard movement velocity—and its variations—but has the advantage of being more directly representative of the spasticity effect on patients function.
These stretches were applied at several different velocities in 69 studies—either in a randomised or increasing velocity order (N = 48 and N = 21 respectively)—which demonstrate how most methods tackle the velocity dependence aspect of spasticity. Still, in 44 studies, only one stretching velocity was used and 23 did not clearly report the number of velocities used or did not use any stretching (NS).
Joints of application
The different methods were equally applied to the upper or lower limb joints (52% vs 48%) but much more frequently to the more distal joints with only two studies relative to the shoulder and four to the hip (see Fig. 2c). Only four studies were applied to the fingers joints.
Devices used
Ten categories of technological devices could be identified in the different studies. Most of the studies used two or more types of devices. Fifty studies relied on active systems, either a robotic end-effector system (REE, N = 34) or a robotic exoskeleton (REXO, N = 16), among which they were coupled with EMG measurements in 23 cases. Electrical stimulation (STI) was used in four studies. Passive orthoses (ORT) were used to guide or stabilise the movement and measure either kinematic or kinetic data in 20 cases.
Purely in terms of measurement devices, EMG is the most commonly used system (N = 83), followed by goniometers (GON, N = 26) and IMUs (N = 17), dynamometers (DYN, N = 8) and finally Ultra-Sound or mechanomyography (US or MMG, N = 7).
Outcome measures
Seventy-eight different outcome measures were identified with only a few recurrent ones and multiple studies reporting several outcome measures. The largest category encompasses the Force/Torque level outcomes (N = 51), either resistive torques measured in varying conditions or the Force/Torque evolution over stretching angle or velocity. Thirty-six studies reported a Muscle Activity level, 19 reported a catch angle, 16 the presence of an EMG onset and 15 the Tonic Stretch Reflex Threshold (TSRT), sometimes with the associated Tonic Stretch Reflex Slope (TSRS). Figure 2d presents the most commonly encountered measures and a full list is available in the Additional file 1. Among the variety of other outcome measures reported, it is noted that six studies aimed at estimating a MAS score equivalent, either by reproducing the MAS procedure using technological equipment or by using machine learning techniques on a set of recorded features.
Types of measurement
When comparing the main stretching categories (Fig. 2b), not surprisingly, all methods using Controlled stretching relied on Kinematic measures—as it is directly provided and controlled by the stretching system. Quite naturally, Controlled methods also more commonly relied on Force/Torque measurements than Manual methods, as this measure can be directly provided by the mechatronics system. Instead, Manual methods tend to use Muscle Activity measures more frequently as an alternative to Force/Torque.
Psychometric properties
The detailed data extraction table with the characteristics of each study, and for each outcome measure, is provided as a Supplementary material (Additional file 2). Six studies [28,29,30,31,32,33] were excluded from the psychometric properties analysis as they only recruited healthy subjects.
There is quite a large variety of study designs, which do not all aim at formally assessing the psychometric properties of the used—or proposed—assessment methods. As such, not surprisingly, no study reported all the expected items and six studies reported four of the five properties [34,35,36,37,38,39]. When psychometric items were reported, they also were commonly evaluated only for some of the outcome measures proposed.
Overall, more than half of the studies (N = 76) proposed or evaluated a method which scores less than two on the construct validity criterion, showing that it is either not velocity-dependent or does not attempt to isolate the stretch reflex component.
For 42 studies, at least one outcome measure was able to discriminate between the test and control populations, whereas this discrimination was not possible, or only under specific conditions, in 10 studies. 78 studies did not report any discriminant validity evaluation.
A Strong or Very Strong correlation of the evaluated measure with clinical measures of spasticity was found in 28 studies, out of the 62 reporting such evaluation. It is to note that in most of these studies (N = 33) the concurrent validity was evaluated against the MAS. Given the limited properties and limited specificity of the MAS, this raises the question of relevance of these correlations.
The repeatability of the proposed measures was reported in only 29 cases and was found excellent in 25 cases.
Sensitivity was evaluated in only three studies, either using a Minimal Detectable Change (MDC), a Smallest Real Difference (SRD) or a Smallest Detectable Difference (SDD).
The targeted population was well specified in a large majority of studies with only two studies missing this information. A majority of studies applied to the Stroke population (N = 79), followed by CP population (N = 30) and SCI population (N = 15). The spasticity severity of the test group was provided in 108 studies.
Assessment methods comparison
In order to estimate which of the main assessment method categories (defined in the previous section) benefit from the more positive evaluation across the different psychometric properties, Table 3 reports the percentage of studies in each method, with what is considered a good psychometric property: a fully valid construct (\(=2\)), a Significant discriminant validity, a Strong or Very Strong correlation with clinical scales, an Excellent repeatability and any evaluation of the sensitivity.
None of the different assessment methods demonstrate a good or even systematic validation across the five psychometric properties. Among the methods relying on Manual stretching, the ones using the larger set of measurements (M-MA+KI+FT) have an overall better validation. The simpler approach (M-KI), requiring the simpler equipment, has a good validation overall even if its construct validity remains low. Similarly, among methods relying on a Controlled stretching, the ones with the larger set of measurements (C-MA+KI+FT) demonstrate the best overall properties. Approaches relying on either Voluntary movements (V-) or on a static measurement (NS-) have a low construct validity score and generally suffer from an absence of repeatability evaluation.
Outcome measures comparison
The same analysis was performed based on the studies outcome measure(s). The results for the most commonly used measures are presented in Table 4.
A more detailed analysis accounting only for studies reporting on a specific property is presented on Fig. 3. When evaluated, most outcomes demonstrate an Excellent repeatability and a positive discriminant validity. It is to note still, that the use of TSRT and the presence of EMG onset are very rarely evaluated along these properties. Overall, across the spectrum, only the Force/Torque measure, either as a whole (i.e. resistive) or isolating the neural component, and the Work measure demonstrate good properties in a majority of studies. This similar behaviour is not surprising, as these two outcome measures are relatively similar, the Work being the integration of the Force (or Torque) along the stretching movement.

Response on the different psychometric properties for the more commonly adopted outcome measures (in 10 or more studies). Sensitivity being reported in only three studies is not presented. Note that this does account only for studies reporting the given property and as such leads to a very inequal total number across the different properties (and different vertical scales)
Only one study reported properties of a good level across the first four psychometric properties (Additional file 1), and this for the MA level outcome measure when applied at the knee joint with subjects with CP [38]. The same authors, in a different study with the same population at the ankle, were the only ones to also report good construct validity, discriminant validity and repeatability (but without assessing clinical validity) [77]. This applied to the overall Work, specific Neural Work and Torque outcome measures.
Usability analysis of valid approaches
Usability was evaluated and analysed for 54 studies which specifically evaluated spasticity and so had a construct validity of 2/2.
Usability comparison by method approaches
Less than half of the studies’ procedures (N = 19) could be administered in less than 10 mins, making them comparable to the MAS or MTS. It is of note that most of these 19 studies were in the Manual Stretch method category which generally required minimal time for equipment setup. In contrast, the majority of studies had an administration time as much as a typical intervention session (10–30 mins, N = 21) or an extended intervention session (30–60 mins, N = 14).
In terms of equipment cost, nearly half of the studies (N = 26) had a cost between $1000 and $10,000 USD. Meanwhile, six studies had a cost of $10,000–50,000 USD and 21 studies had a cost more than $50,000 USD, where most of these studies used a robotic device (REE or REXO) to perform Controlled stretching. A relatively low cost (less than $1000 USD) was only found in one study, which combined a musculoskeletal model and Kinematic measurements from three IMUs during Manual stretching to predict the velocity-dependent TSRT [79].
The portability analysis showed the assessment equipment was not movable in nearly half of the studies (N = 26). Only 11 studies used a device which could be transportable from room-to-room, and 17 studies (all in the Manual Stretch category) used easily transportable equipment.
Usability comparison by outcome measures
In order to compare which validated assessment methods and their associated outcome measures have advantages in practicality, the usability for the most commonly used outcome measures (used in 10 or more studies) is presented in Fig. 4.

Usability analysis on the equipment cost, administration time and portability for the more commonly adopted outcome measures
MA level approaches had an overall good usability across administration time, equipment cost and portability. More than half of the studies measuring MA level had an administration time of less than 10 mins, which is thus comparable to a MAS or MTS, they required an equipment costing between $1000 and $10,000 USD and scored high on portability.
Overall, the good usability of MA level relied on simple equipment used (e.g. EMG) and a relatively small number of Manual stretches in most of these studies.
Although TSRT demonstrated a similar performance on equipment cost and portability as MA level, its administration time was longer, more commonly of more than 30 mins as it requires a larger number of stretches. Indeed, a larger number of stretches is required to elicit sufficient Dynamic Strectch Reflex Thresholds (DSRT) data points to obtain a reliable TSRT value.
In contrast with MA level and TSRT, most FT (neural) studies had an equipment cost over $50,000 USD and lacked equipment movability as these assessment methods were generally performed on a robotic system (REE or REXO). Additionally, more than half of the FT (neural) studies required more than 10 mins for measurement.
Discussion
The diversity of outcome measures shows that there is no clear agreement on efficient method for such assessment. The psychometric properties of the different measures are not well explored.
A very large spectrum of methods and outcome measures have been developed and used in studies with various methodology approaches. This development seems to be at the expense of limited formal evaluation of the proposed methods. Many studies neglect the evaluation of important psychometric properties of the measures. This is evident for the sensitivity (present in only three studies) and also repeatability which is not evaluated in a majority of studies. Clinical validity is more often present. If it appears important to provide a benchmark against accepted scales, its significance remains limited given the low specificity and inter/intra rater properties of the MAS and MTS (the most frequently encountered). This correlation cannot be considered alone to characterise an appropriate measure of spasticity. It would thus appear more appropriate to evaluate proposed methods against relatively well established ones such as Muscle Activity approaches (MA level) or ones properly isolating the stretch reflex in Controlled stretches (FT neural).
Measures specificity to spasticity
The diversity of proposed methods and the limited construct validity (<2) in more than half the studies show the limited specificity of the methods evaluated. This is illustrated by the wide use of catch angles measures considered only at a single velocity, or the use of a MAS equivalent, also known to not be velocity-dependent. It was noted that, as suggested by McPherson et al. [4], catch angles may be used to construct a valid outcome measure (representing the stretch-reflex sensitivity) but only when their velocity dependence is considered. This lack of specificity in the literature is in agreement with a conclusion of a previous systematic review which found that a “majority of studies rely on methods that assess resistance to passive movement rather than spasticity” [23].
Still, the importance of specificity might be relative for clinical use. Typically, Botulinum toxin type A injection decisions can be made on the basis of static postures [151] or MAS scores [152] to address both hypertonicity and spasticity all-together. As such, when a specific measure is not required, it appears that simple instrumented methods relying on a manual stretching and a simple kinematic measurement [35,36,37, 79,80,81,82] could be favoured.
Lack of repeatability and sensitivity evaluation
Overall, most outcome measures demonstrate an excellent repeatability when reported but with the notable exception of the TSRT and the presence of EMG onset (Fig. 3). This absence of repeatability evaluation is especially problematic given that these two measures are the ones with the higher construct validity overall—because they take advantage of a Muscle Activity measure—and are such very relevant approaches.
In general, repeatability, which is a fundamental property relatively straightforward to evaluate is very much lacking for most methods and outcome measures, and care should be taken to fill in this gap.
The sensitivity of the outcome measures is even more critically lacking from the literature, with only three studies proposing such evaluation. This confirms and extends a previous finding about robotic assessments of spasticity by van der Velden et al. [22]. The recommendation of the authors to invest more effort “in studying diagnostic accuracy” and its “added value for clinical care” can be extended to all existing instrumented measures.
Usability and clinical implications
One of the main objectives of the different methodology developments in the literature is to provide alternatives to the MAS and MTS scales in clinical practice. These scales are criticised for their limited repeatability, specificity and sensitivity but have the major advantage of not requiring a specific equipment and being quick to administer with minimal training. As such, usability considerations are important when looking at possible alternatives.
A number of existing methods address this issue and have an estimated administration time of less than 10 minutes. Those mostly include instrumented Manual stretching methods measuring a Muscle Activity reaction and the Kinematics (e.g. [55]) or Force/Torque reaction (e.g. [77]). Lower cost alternatives relying only on a kinematic measure, provided by either a goniometer [80] or an IMU [35, 36, 79] have been proposed but have reported relatively poor psychometric properties, except for [79] and [80] (see Additional file 1).
It is also to note that, if TSRT is an interesting approach quite well explored, it can only be recommended as a comparison point in research studies as it requires a large number of stretches to be efficient, thus increasing its administration time.
Another, less specific alternatives to the MAS and MTS are static methods not relying on any stretching movements (NS-) and measuring either intrinsic Muscle Properties using Ultra-Sound [132, 144,145,146] or measuring the H-reflex using EMG and electrical stimulation [70, 81]. These approaches, past their low construct validity, have a good discriminant validity and a Moderate to Very Strong clinical validity, but no repeatability nor sensitivity evaluation.
Overall, Muscle Activity measures (using EMG) of Manual stretches seem to constitute the go-to alternative to existing clinical scales, given their short administration time but also relative low-cost (<$10,000 for most of them). These Manual methods tend to have a lower equipment cost than their Controlled counterparts which require a robotic system but this additional cost is often defrayed given that when robotic systems are used for spasticity assessment, this is generally not their only—or even primary—use, as discussed in [21]. In addition, Muscle Activity based methods require an appropriate placement of EMG electrodes which may require specific experience. The choice between Controlled-Torque methods and Manual-Muscle Activity one is thus still open depending on the equipment available and clinicians experience.
Limitations
The diversity of outcome measures and variety of objectives of the studies make it difficult to draw specific conclusions. As such, one limitation of this review is the lack of analysis for every different joint and pathology. It is clear that practical considerations may not allow a straightforward translation of one method from one joint to another (e.g. sEMG placement or robotic devices fitting and adaption to the joints morphology) but such analysis would require a more narrow scope. Similarly regarding the different pathologies, the assessment needs, and limbs presentation, might vary slightly for the different pathologies and so affect each method differently.
In addition, the construct validity considered in this review intentionally does not characterise the physiological mechanisms of spasticity specifically: no distinction is made between methods estimating an increased sensitivity of the stretch reflex and methods estimating an increase of the reaction amplitude. This approach thus assumes that both effects may exist and can potentially characterise spasticity. This is expected to be aligned with current clinical definitions of spasticity.
The usability of the different methods in clinical practice is based on estimations of the equipment cost and administration time. It is acknowledged that the cost does not include the expertise that may be required by some methods and that the cost of the equipment itself can significantly vary. As such this remains only an approximation used for comparisons between methods. Similarly, the estimated administration time can highly depend on the patient presentation but also expertise of the assessor. It is only relevant here as a comparison between methods and against the commonly used clinical scales, MAS and MTS, which have the advantage of being fast to administer.
Finally, the choice to include conference proceedings within the scope appeared important given the importance of such publications in the engineering field which contributes to the development of the assessment methods. Nevertheless, this may have introduced a bias when analysing the validation of the methods, given that some preliminary publication may not provide a full validation, complemented in a different publication. This approach also tends to aggregate studies which aim to introduce new evaluation methods with ones focusing on a more careful analysis of the psychometric properties.
Conclusions
The review found a large variety of technology assisted methods and associated outcome measures to assess spasticity. These methods generally lack systematic evaluation of their psychometric properties. It thus appears that some consolidation of knowledge around existing approaches is required and that no ready-to-use alternative to existing clinical scales (MAS and MTS) is yet fully validated. Nevertheless, methods measuring a Muscle Activity reaction to manual stretches appear as promising practical method to be investigated further. Similarly, and when robotic systems are readily available, measures relying on a specific Torque (or Work) reaction to a controlled stretching can also be recommended.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its Additional files.
Abbreviations
- MAS:
-
Modified Ashworth Scale
- MTS:
-
Modified Tardieu Scale
- EMG:
-
ElectroMyoGraphy
- sEMG:
-
Surface ElectroMyoGraphy
- IMU:
-
Inertial Measurement Unit
- US:
-
Ultra-Sound
- ICC:
-
Intraclass Correlation Coefficient
- TSRT:
-
Tonic Stretch Reflex Threshold
- CP:
-
Cerebral Palsy
- SCI:
-
Spinal Cord Injury
- KI:
-
Kinematic
- MA:
-
Muscle Activity
- FT:
-
Force/Torque
- MP:
-
Muscle Property
- M:
-
Manual (stretch)
- C:
-
Controlled (stretch)
- V:
-
Voluntary (stretch)
- NS:
-
No Stretch
References
Pandyan A, Gregoric M, Barnes M, Wood D, Wijck F.v., Burridge J, Hermens H, Johnson G. Spasticity: clinical perceptions, neurological realities and meaningful measurement. Disabil Rehabil. 2005;27(1–2):2–6.
Lance JW. Symposium synopsis. In Feldman RG, Young RR, Koella WP, editors. Spasticity: disordered motor control. Yearbook Medical, Chicago; 1980, pp. 485–494.
Noort JCVD, Bar-On L, Aertbeliën E, Bonikowski M, Braendvik SM, Broström EW, Buizer AI, Burridge JH, Campenhout AV, Dan B, Fleuren JF, Grunt S, Heinen F, Horemans HL, Jansen C, Kranzl A, Krautwurst BK, Krogt MVD, Lara SL, Lidbeck CM, Lin J-P, Martinez I, Meskers C, Metaxiotis D, Molenaers G, Patikas DA, Rémy-Néris O, Roeleveld K, Shortland AP, Sikkens J, Sloot L, Vermeulen RJ, Wimmer C, Schröder AS, Schless S, Becher JG, Desloovere K, Harlaar J. European consensus on the concepts and measurement of the pathophysiological neuromuscular responses to passive muscle stretch. Eur J Neurol. 2017. https://doi.org/10.1111/ene.13322.
McPherson JG, Stienen AHA, Schmit BD, Dewald JPA. Biomechanical parameters of the elbow stretch reflex in chronic hemiparetic stroke. Exp Brain Res. 2019;237(1):121–35. https://doi.org/10.1007/s00221-018-5389-x.
Kuo C-L, Hu G-C. Post-stroke spasticity: a review of epidemiology, pathophysiology, and treatments. Int J Gerontol. 2018;12(4):280–4. https://doi.org/10.1016/j.ijge.2018.05.005.
Wissel JM, Manack A, Brainin M. Toward an epidemiology of poststroke spasticity. Neurology. 2013. https://doi.org/10.1212/WNL.0b013e3182762448.
Wissel J, Schelosky LD, Scott J, Christe W, Faiss JH, Mueller J. Early development of spasticity following stroke: a prospective, observational trial. J Neurol. 2010;257(7):1067–72. https://doi.org/10.1007/s00415-010-5463-1.
Welmer A-K, Arbin MV, Holmqvist LW, Sommerfeld DK. Spasticity and its association with functioning and health-related quality of life 18 months after stroke. Cerebrovasc Dis. 2006. https://doi.org/10.1159/000091222.
Chen C, Leys D, Esquenazi A. The interaction between neuropsychological and motor deficits in patients after stroke. Neurology. 2013;80(3 Suppl 2):27–34. https://doi.org/10.1212/WNL.0b013e3182762569.
Lundström E, Smits A, Borg J, Terént A. Four-fold increase in direct costs of stroke survivors with spasticity compared with stroke survivors without spasticity: the first year after the event. Stroke. 2010;41(2):319–24. https://doi.org/10.1161/STROKEAHA.109.558619.
Francisco GE, McGuire JR. Poststroke spasticity management. Stroke. 2012. https://doi.org/10.1161/STROKEAHA.111.639831.
Cusick A, Lannin N, Kinnear BZ. Upper limb spasticity management for patients who have received Botulinum Toxin A injection: Australian therapy practice. Aust Occup Therapy J. 2015. https://doi.org/10.1111/1440-1630.12142.
Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987;67(2):206–7. https://doi.org/10.1093/ptj/67.2.206.
Ansari NN, Naghdi S, Arab TK, Jalaie S. The interrater and intrarater reliability of the Modified Ashworth Scale in the assessment of muscle spasticity: Limb and muscle group effect. NeuroRehabilitation. 2008;23(3):231–7. https://doi.org/10.3233/NRE-2008-23304.
Ansari NN, Naghdi S, Hasson S, Azarsa MH, Azarnia S. The Modified Tardieu Scale for the measurement of elbow flexor spasticity in adult patients with hemiplegia. Brain Inj. 2008;22(13–14):1007–12. https://doi.org/10.1080/02699050802530557.
Sheean G, Lannin NA, Turner-Stokes L, Rawicki B, Snow BJ. Cerebral Palsy Institute: Botulinum toxin assessment, intervention and after-care for upper limb hypertonicity in adults: international consensus statement. Eur J Neurol. 2010;17(Suppl 2):74–93. https://doi.org/10.1111/j.1468-1331.2010.03129.x.
Patrick E, Ada L. The Tardieu Scale differentiates contracture from spasticity whereas the Ashworts Scale is confounded by it. Clin Rehabil. 2006;20(2):173–81. https://doi.org/10.1191/0269215506cr922oa.
Powers RK, Marder-Meyer J, Rymer WZ. Quantitative relations between hypertonia and stretch reflex threshold in spastic hemiparesis. Ann Neurol. 1988;23(2):115–24. https://doi.org/10.1002/ana.410230203.
Katz RT, Rovai GP, Brait C, Rymer WZ. Objective quantification of spastic hypertonia: correlation with clinical findings. Arch Phys Med Rehabil. 1992;73(4):339–47. https://doi.org/10.1016/0003-9993(92)90007-J.
Alaiad A, Zhou L. The determinants of home healthcare robots adoption: an empirical investigation. Int J Med Inform. 2014;83(11):825–40. https://doi.org/10.1016/j.ijmedinf.2014.07.003.
De-la-Torre R, Ona ED, Balaguer C, Jardon A. Robot-aided systems for improving the assessment of upper limb spasticity: a systematic review. Sensors (Basel, Switzerland). 2020;20(18):5251. https://doi.org/10.3390/s20185251.
van der Velden LL, de Koff MAC, Ribbers GM, Selles RW. The diagnostic levels of evidence of instrumented devices for measuring viscoelastic joint properties and spasticity; a systematic review. J Neuroeng Rehabil. 2022;19(1):1–8.
Aloraini SM, Alyosuf EY, Aloraini LI, Aldaihan MM. Assessment of spasticity: an overview of systematic reviews. Physical Therapy Rev. 2022;0(0):1–14. https://doi.org/10.1080/10833196.2022.2059942.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. Prisma 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372.
Evans JD. Straightforward statistics for the behavioral sciences. Pacific Grove: Brooks/Cole Publishing Company; 1996.
Altman DG. Practical statistics for medical research. London: Chapman and Hall; 1991.
Fleiss JL. The design and analysis of clinical experiments. New York: John Wiley and Sons; 1986.
Averta G, Abbinante M, Orsini P, Felici F, Lippi P, Bicchi A, Catalano MG, Bianchi M. A novel mechatronic system for evaluating elbow muscular spasticity relying on Tonic Stretch Reflex Threshold estimation. In: 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), pp. 2020:3839–3843. https://doi.org/10.1109/EMBC44109.2020.9176011
Erden MS, McColl W, Abassebay D, Haldane S. Hand exoskeleton to assess hand spasticity. In: 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), pp. 2020:1004–1009. https://doi.org/10.1109/BioRob49111.2020.9224329
Falzarano V, Petrella G, Marini F, Holmes MWR, Masia L, Morasso P, Zenzeri J. Preliminary evaluation of a robotic measurement system for the assessment of wrist joint spasticity. In: 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), pp. 2020:539–544. https://doi.org/10.1109/BioRob49111.2020.9224343
Seth N, Johnson D, Abdullah HA. Spasticity assessment system for elbow flexors/extensors: healthy pilot study. In: 2014 IEEE Symposium on Computational Intelligence in Robotic Rehabilitation and Assistive Technologies (CIR2AT), pp. 2014:36–41 . https://doi.org/10.1109/CIRAT.2014.7009739
Misgeld BJE, Lueken M, Kim S, Leonhardt S. Body sensor network-based spasticity detection. In: 2014 4th International Conference on Wireless Mobile Communication and Healthcare - Transforming Healthcare Through Innovations in Mobile and Wireless Technologies (MOBIHEALTH), pp. 2014:291–295. https://doi.org/10.1109/MOBIHEALTH.2014.7015968
Simon D, Foulds R. Developing a quantitative measure of muscle spasticity. In: IEEE 30th Annual Northeast Bioengineering Conference, pp. 2004:196–197. https://doi.org/10.1109/NEBC.2004.1300062
Cetin N, Dilek A, Aytar A, Akman MN. Reproducibility of isokinetic test findings for assessment of wrist spasticity in stroke patients. Isokinet Exerc Sci. 2008;16(1):61–7. https://doi.org/10.3233/ies-2008-0297.
Bui HT, Gagnon C, Audet O, Mathieu J, Leone M. Measurement properties of a new wireless electrogoniometer for quantifying spasticity during the pendulum test in ARSACS patients. J Neurol Sci. 2017;375:181–5. https://doi.org/10.1016/j.jns.2017.01.065.
Sterpi I, Caroli A, Meazza E, Maggioni G, Pistarini C, Colombo R. Lower limb spasticity assessment using an inertial sensor: a reliability study. Physiol Meas. 2013;34(11):1423–34. https://doi.org/10.1088/0967-3334/34/11/1423.
Bohannon RW, Harrison S, Kinsella-Shaw J. Reliability and validity of pendulum test measures of spasticity obtained with the Polhemus tracking system from patients with chronic stroke. J Neuroeng Rehabil. 2009;6(1):30–6. https://doi.org/10.1186/1743-0003-6-30.
Bar-On L, Aertbelien E, Wambacq H, Severijns D, Lambrecht K, Dan B, Huenaerts C, Bruyninckx H, Janssens L, Van Gestel L, Jaspers E, Molenaers G, Desloovere K. A clinical measurement to quantify spasticity in children with cerebral palsy by integration of multidimensional signals. Gait Posture. 2013;38(1):141–7. https://doi.org/10.1016/j.gaitpost.2012.11.003.
Wang H, Huang P, Li X, Samuel OW, Xiang Y, Li G. Spasticity assessment based on the maximum isometrics voluntary contraction of upper limb muscles in post-stroke hemiplegia. Front Neurol. 2019. https://doi.org/10.3389/fneur.2019.00465.
Sorinola IO, White CM, Rushton DN, Newham DJ. Electromyographic response to manual passive stretch of the hemiplegic wrist: accuracy, reliability, and correlation with clinical spasticity assessment and function. Neurorehabil Neural Repair. 2009;23(3):287–94. https://doi.org/10.1177/1545968308321778.
Malhotra S, Cousins E, Ward A, Day C, Jones P, Roffe C, Pandyan A. An investigation into the agreement between clinical, biomechanical and neurophysiological measures of spasticity. Clin Rehabil. 2008;22(12):1105–15. https://doi.org/10.1177/0269215508095089.
Alves CM, Rezende AR, Marques IA, Martins Naves EL. SpES: a new portable device for objective assessment of hypertonia in clinical practice. Comput Biol Med. 2021. https://doi.org/10.1016/j.compbiomed.2021.104486.
Frenkel-Toledo S, Solomon JM, Shah A, Banina MC, Berman S, Soroker N, Liebermann DG, Levin MF. Tonic stretch reflex threshold as a measure of spasticity after stroke: reliability, minimal detectable change and responsiveness. Clin Neurophysiol. 2021;132(6):1226–33. https://doi.org/10.1016/j.clinph.2021.02.390.
Yu S, Chen Y, Cai Q, Ma K, Zheng H, Xie L. A novel quantitative spasticity evaluation method based on surface electromyogram signals and adaptive neuro fuzzy inference system. Front Neurosci. 2020;14:462. https://doi.org/10.3389/fnins.2020.00462.
Zhang X, Tang X, Zhu X, Gao X, Chen X, Chen X. A regression-based framework for quantitative assessment of muscle spasticity using combined EMG and inertial data from wearable sensors. Front Neurosci. 2019;13:398. https://doi.org/10.3389/fnins.2019.00398.
Marques IA, Silva MB, Silva AN, Luiz LMD, Soares AB, Naves ELM. Measurement of post-stroke spasticity based on tonic stretch reflex threshold: implications of stretch velocity for clinical practice. Disabil Rehabil. 2019;41(2):219–25. https://doi.org/10.1080/09638288.2017.1381183.
Hu B, Zhang X, Mu J, Wu M, Zhu Z, Liu Z, Wang Y. Spasticity measurement based on the HHT marginal spectrum entropy of sEMG using a portable system: a preliminary study. IEEE Trans Neural Syst Rehabil Eng. 2018;26(7):1424–34. https://doi.org/10.1109/TNSRE.2018.2838767.
Silva MB, Silva AN, Naves ELM, Palomari ET, Soares AB. An improved approach for measuring the tonic stretch reflex response of spastic muscles. Comput Biol Med. 2017;80:166–74. https://doi.org/10.1016/j.compbiomed.2016.12.001.
Ewoldt JK, Lazzaro EC, Roth EJ, Suresh NL. Quantification of a single score (1+) in the Modified Ashworth Scale (MAS), a clinical assessment of spasticity. In: 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), pp. 2016:1737–1740. https://doi.org/10.1109/EMBC.2016.7591052
Ferreira J, Moreira V, Machado J, Soares F. Improved biomedical device for spasticity quantification. In: 2013 IEEE 3rd Portuguese Meeting in Bioengineering (ENBENG) 2013. https://doi.org/10.1109/ENBENG.2013.6518417
Ferreira J, Moreira V, Machado J, Soares F. Biomedical device for spasticity quantification based on the velocity dependence of the Stretch Reflex threshold. In: ETFA 2011, pp. 2011:1–4 . https://doi.org/10.1109/ETFA.2011.6059225
Ferreira J, Moreira V, Machado J, Soares F. A mechatronic device for spasticity quantification. In: 2011 9th IEEE International Conference on Industrial Informatics, pp. 2011:257–262. https://doi.org/10.1109/INDIN.2011.6034884
McGibbon CA, Sexton A, Jones M, O’Connell C. Elbow spasticity during passive stretch-reflex: clinical evaluation using a wearable sensor system. J Neuroeng Rehabil. 2013;10(1):1–14. https://doi.org/10.1186/1743-0003-10-61.
Calota A, Feldman AG, Levin MF. Spasticity measurement based on tonic stretch reflex threshold in stroke using a portable device. Clin Neurophysiol. 2008;119(10):2329–37. https://doi.org/10.1016/j.clinph.2008.07.215.
Schless S-H, Desloovere K, Aertbelien E, Molenaers G, Huenaerts C, Bar-On L. The intra- and inter-rater reliability of an instrumented spasticity assessment in children with cerebral palsy. PLoS ONE. 2015;10(7):1–23. https://doi.org/10.1371/journal.pone.0131011.
Kristinsdottir K, Magnusdottir G, Chenery B, Gudmundsdottir V, Gudfinnsdottir HK, Karason H, Ludvigsdottir GK, Helgason T. Comparison of spasticity in spinal cord injury and stroke patients using reflex period in pendulum test. Eur J Transl Myol. 2020;30(1):154–8.
Choi S, Kim J. Improving modified tardieu scale assessment using inertial measurement unit with visual biofeedback. In: 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), United States, pp. 4703–4706. https://doi.org/10.1109/EMBC.2016.7591777
Yeh CH, Young HWV, Wang CY, Wang YH, Lee PL, Kang JH, Lo MT. Quantifying spasticity with limited swinging cycles using pendulum test based on phase amplitude coupling. IEEE Trans Neural Syst Rehabil Eng. 2016;24(10):1081–8. https://doi.org/10.1109/TNSRE.2016.2521612.
Fleuren JFM, Snoek GJ, Voerman GE, Hermens HJ. Muscle activation patterns of knee flexors and extensors during passive and active movement of the spastic lower limb in chronic stroke patients. J Electromyogr Kinesiol. 2009;19(5):301–10. https://doi.org/10.1016/j.jelekin.2008.04.003.
Sloot LH, Bar-On L, van der Krogt MM, Aertbelien E, Buizer AI, Desloovere K, Harlaar J. Motorized versus manual instrumented spasticity assessment in children with cerebral palsy. Dev Med Child Neurol. 2017;59(2):145–51. https://doi.org/10.1111/dmcn.13194.
Arami A, Tagliamonte NL, Tamburella F, Huang H-Y, Molinari M, Burdet E. A simple tool to measure spasticity in spinal cord injury subjects. In: 2017 International Conference on Rehabilitation Robotics (ICORR), United States, pp. 1590–1596. https://doi.org/10.1109/ICORR.2017.8009475
Choi S, Shin YB, Kim S-Y, Kim J. A novel sensor-based assessment of lower limb spasticity in children with cerebral palsy. J Neuroeng Rehabil. 2018;15(1):1–16. https://doi.org/10.1186/s12984-018-0388-5.
van den Noort JC, Scholtes VA, Becher JG, Harlaar J. Evaluation of the catch in spasticity assessment in children with cerebral palsy. Arch Phys Med Rehabil. 2010;91(4):615–23. https://doi.org/10.1016/j.apmr.2009.12.022.
Cousins E, Ward AB, Roffe C, Rimington LD, Pandyan AD. Quantitative measurement of poststroke spasticity and response to treatment with botulinum toxin: a 2-patient case report. Phys Ther. 2009;89(7):688–97. https://doi.org/10.2522/ptj.20080040.
Pandyan AD, Van Wijck FMJ, Stark S, Vuadens P, Johnson GR, Barnes MP. The construct validity of a spasticity measurement device for clinical practice: an alternative to the Ashworth scales. Disabil Rehabil. 2006. https://doi.org/10.1080/09638280500242390.
Wu Y-N, Park HS, Ren Y, Gaebler-Spira D, Chen J-J, Zhang L-Q. Measurement of elbow spasticity in stroke patients using a manual spasticity evaluator. In: 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, United States, pp. 3974–3977
Bar-On L, Van Campenhout A, Desloovere K, Aertbelien E, Huenaerts C, Vandendoorent B, Nieuwenhuys A, Molenaers G. Is an instrumented spasticity assessment an improvement over clinical spasticity scales in assessing and predicting the response to integrated botulinum toxin type a treatment in children with cerebral palsy? Arch Phys Med Rehabil. 2014;95(3):515–23. https://doi.org/10.1016/j.apmr.2013.08.010.
Bar-On L, Aertbelien E, Molenaers G, Van Campenhout A, Vandendoorent B, Nieuwenhuys A, Jaspers E, Hunaerts C, Desloovere K. Instrumented assessment of the effect of Botulinum Toxin-A in the medial hamstrings in children with cerebral palsy. Gait Posture. 2014;39(1):17–22. https://doi.org/10.1016/j.gaitpost.2013.05.018.
Lebiedowska MK, Fisk JR. Knee resistance during passive stretch in patients with hypertonia. J Neurosci Methods. 2009;179(2):323–30. https://doi.org/10.1016/j.jneumeth.2009.02.005.
Chen B, Sangari S, Lorentzen J, Nielsen JB, Perez MA. Bilateral and asymmetrical contributions of passive and active ankle plantar flexors stiffness to spasticity in humans with spinal cord injury. J Neurophysiol. 2020;124(3):973–84. https://doi.org/10.1152/jn.00044.2020.
Lynn B-O, Erwin A, Guy M, Herman B, Davide M, Ellen J, Anne C, Kaat D. Comprehensive quantification of the spastic catch in children with cerebral palsy. Res Dev Disabil. 2013;34(1):386–96. https://doi.org/10.1016/j.ridd.2012.08.019.
Wang S-J, Park J-H, Park H-S, Nanda D, Albert MV. Wearable spasticity estimation and validation using machine learning. In: 2020 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), pp. 2020:2109–2112 . https://doi.org/10.1109/BIBM49941.2020.9313130
Wu Y-N, Park H-S, Chen J-J, Ren Y, Roth EJ, Zhang L-Q. Position as well as velocity dependence of spasticity-four-dimensional characterizations of catch angle. Front Neurol. 2018;9:863. https://doi.org/10.3389/fneur.2018.00863.
Kumar R, Pandyan A, Sharma A. Biomechanical measurement of post-stroke spasticity. Age Ageing. 2006;35(4):371–5. https://doi.org/10.1093/ageing/afj084.
Pandyan AD, Price CIM, Rodgers H, Barnes MP, Johnson GR. Biomechanical examination of a commonly used measure of spasticity. Clin Biomech. 2001. https://doi.org/10.1016/S0268-0033(01)00084-5.
Hughes TAT, Westem BJ, Thomas M, van Deursen RWM, Griffiths H. An instrument for the bedside quantification of spasticity: a pilot study. In: 2001 Conference Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, vol. 2, pp. 2001:1228–1231. https://doi.org/10.1109/IEMBS.2001.1020415
Bar-On L, Desloovere K, Molenaers G, Harlaar J, Kindt T, Aertbelien E. Identification of the neural component of torque during manually-applied spasticity assessments in children with cerebral palsy. Gait Posture. 2014;40(3):346–51. https://doi.org/10.1016/j.gaitpost.2014.04.207.
Peng Q, Park H-S, Shah P, Wilson N, Ren Y, Wu Y-N, Liu J, Gaebler-Spira DJ, Zhang L-Q. Quantitative evaluations of ankle spasticity and stiffness in neurological disorders using manual spasticity evaluator. J Rehabil Res Dev. 2011;48(4):473–81. https://doi.org/10.1682/JRRD.2010.04.0053.
Ang WS, Geyer H, Chen I-M, Ang WT. Objective assessment of spasticity with a method based on a human upper limb model. IEEE Trans Neural Syst Rehabil Eng. 2018;26(7):1414–23. https://doi.org/10.1109/TNSRE.2018.2821197.
Le Cavorzin P, Hernot X, Bartier O, Allain H, Carrault G, Rochcongar P, Chagneau F. A computed model of the pendulum test of the leg for routine assessment of spasticity in man. ITBM-RBM. 2001;22(3):170–7. https://doi.org/10.1016/S1297-9562(01)90028-2.
Manella KJ, Roach KE, Field-Fote EC. Temporal indices of ankle clonus and relationship to electrophysiologic and clinical measures in persons with spinal cord injury. J Neurol Phys Ther. 2017;41(4):229–38. https://doi.org/10.1097/NPT.0000000000000197.
Banky M, Clark RA, Mentiplay BF, Olver JH, Kahn MB, Williams G. Toward accurate clinical spasticity assessment: validation of movement speed and joint angle assessments using smartphones and camera tracking. Arch Phys Med Rehabil. 2019;100(8):1482–91. https://doi.org/10.1016/j.apmr.2018.11.026.
Hu B, Zhang X, Mu J, Wu M, Wang Y. Spasticity assessment based on the Hilbert-Huang transform marginal spectrum entropy and the root mean square of surface electromyography signals: a preliminary study. Biomed Eng Online. 2018;17(1):1–20. https://doi.org/10.1186/s12938-018-0460-1.
Wang H, Wang L, Xiang Y, Zhao N, Li X, Chen S, Lin C, Li G. Assessment of elbow spasticity with surface electromyography and mechanomyography based on support vector machine. In: 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), United States, pp. 3860–3863. https://doi.org/10.1109/EMBC.2017.8037699
Wang L, Guo X, Fang P, Wei Y, Samuel OW, Huang P, Geng Y, Wang H, Li G. A new EMG-based index towards the assessment of elbow spasticity for post-stroke patients. In: 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), United States, pp. 3640–3643. https://doi.org/10.1109/EMBC.2017.8037646
Jun SW, Yong SJ, Jo M, Kim YH, Kim SH. Brief report: preliminary study on evaluation of spasticity in patients with brain lesions using mechanomyography. Clin Biomech (Bristol, Avon). 2018;54:16–21. https://doi.org/10.1016/j.clinbiomech.2018.02.020.
Sherwood AM, Graves DE, Priebe MM. Altered motor control and spasticity after spinal cord injury: subjective and objective assessment. J Rehabil Res Dev. 2000;37(1):41–52.
Cooper A, Musa IM, van Deursen R, Wiles CM. Electromyography characterization of stretch responses in hemiparetic stroke patients and their relationship with the Modified Ashworth scale. Clin Rehabil. 2005;19(7):760–6. https://doi.org/10.1191/0269215505cr888oa.
Kim J, Shin M, Min Y, Cho K, Paik N, Park H. Intercontinental bilateral teleoperation applied to remote elbow assessment of patients post stroke. In: 2013 13th International Conference on Control, Automation and Systems (ICCAS 2013), pp. 2013:1447–1449 . https://doi.org/10.1109/ICCAS.2013.6704113
Chino N, Muraoka Y, Ishihama H, Ide M, Ushijima R, Basford JR. Measurement of ankle plantar flexor spasticity following stroke: assessment of a new quantitative tool. J Rehabil Med. 2015;47(8):753–5. https://doi.org/10.2340/16501977-1991.
Salazar-Torres Jd, Pandyan AD, Price CIM, Davidson RI, Barnes MP, Johnson GR. Biomechanical characterization of the stretch reflex activity as an approach to spasticity measurement and modeling-a pilot study. In: Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No.03CH37439), vol. 2, pp. 2003:1491–1494 . https://doi.org/10.1109/IEMBS.2003.1279622
Germanotta M, Gower V, Papadopoulou D, Cruciani A, Pecchioli C, Mosca R, Speranza G, Falsini C, Cecchi F, Vannetti F, Montesano A, Galeri S, Gramatica F, Aprile I, Falsini C, Aprile I, Group tFRR. Reliability, validity and discriminant ability of a robotic device for finger training in patients with subacute stroke. J Neuroeng Rehabil. 2020;17(1):1–10. https://doi.org/10.1186/s12984-019-0634-5.
Ranzani R, Viggiano F, Engelbrecht B, Held JPO, Lambercy O, Gassert R. Method for muscle tone monitoring during robot-assisted therapy of hand function: a proof of concept. In: 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), pp. 957–962. NLM (Medline), United States. https://doi.org/10.1109/ICORR.2019.8779454
Salehi Dehno N, Kamali Sarvestani F, Shariat A, Jaberzadeh S. Test-retest reliability and responsiveness of isokinetic dynamometry to assess wrist flexor muscle spasticity in subacute post-stroke hemiparesis. J Bodyw Mov Ther. 2020;24(3):38–43. https://doi.org/10.1016/j.jbmt.2020.02.011.
Leng Y, Lo WLA, Hu C, Bian R, Xu Z, Shan X, Huang D, Li L. The effects of extracorporeal shock wave therapy on spastic muscle of the wrist joint in stroke survivors: evidence from neuromechanical analysis. Front Neurosci. 2020;14. https://doi.org/10.3389/fnins.2020.580762.
Leng Y, Wang Z, Bian R, Lo WLA, Xie X, Wang R, Huang D, Li L. Alterations of elastic property of spastic muscle with its joint resistance evaluated from shear wave elastography and biomechanical model. Front Neurol. 2019;10:736. https://doi.org/10.3389/fneur.2019.00736.
Gaverth J, Sandgren M, Lindberg PG, Forssberg H, Eliasson A-C. Test-retest and inter-rater reliability of a method to measure wrist and finger spasticity. J Rehabil Med. 2013;45(7):630–6. https://doi.org/10.2340/16501977-1160.
Pennati GV, Plantin J, Borg J, Lindberg PG. Normative NeuroFlexor data for detection of spasticity after stroke: a cross-sectional study. J NeuroEng Rehabil. 2016. https://doi.org/10.1186/s12984-016-0133-x.
Lindberg PG, Gaverth J, Islam M, Fagergren A, Borg J, Forssberg H. Validation of a new biomechanical model to measure muscle tone in spastic muscles. Neurorehabil Neural Repair. 2011;25(7):617–25. https://doi.org/10.1177/1545968311403494.
Seth N, Johnson D, Allen B, Abdullah HA. Upper limb robotic assessment: pilot study comparing velocity dependent resistance in individuals with acquired brain injury to healthy controls. J Rehabil Assist Technol Eng. 2020;7:1–10. https://doi.org/10.1177/2055668320929535.
Seth N, Johnson D, Abdullah HA. Transverse forces versus modified ashworth scale for upper limb flexion/extension in para-sagittal plane. In: 2017 International Conference on Rehabilitation Robotics (ICORR), United States, pp. 765–770. https://doi.org/10.1109/ICORR.2017.8009340
Seth N, Johnson D, Taylor GW, Allen OB, Abdullah HA. Robotic pilot study for analysing spasticity: clinical data versus healthy controls. J Neuroeng Rehabil. 2015;12(1):1–13. https://doi.org/10.1186/s12984-015-0103-8.
Posteraro F, Crea S, Mazzoleni S, Berteanu M, Ciobanu I, Vitiello N, Cempini M, Gervasio S, Mrachacz-Kersting N. Technologically-advanced assessment of upper-limb spasticity: a pilot study. Eur J Phys Rehabil Med. 2018;54(4):536–44. https://doi.org/10.23736/S1973-9087.17.04815-8.
Dehem S, Gilliaux M, Lejeune T, Detrembleur C, Galinski D, Sapin J, Vanderwegen M, Stoquart G. Assessment of upper limb spasticity in stroke patients using the robotic device reaplan. J Rehabil Med. 2017;49(7):565–71. https://doi.org/10.2340/16501977-2248.
Lee DJ, Bae SJ, Jang SH, Chang PH. Design of a clinically relevant upper-limb exoskeleton robot for stroke patients with spasticity. In: 2017 International Conference on Rehabilitation Robotics (ICORR), United States, pp. 622–627 (2017). https://doi.org/10.1109/ICORR.2017.8009317
Ardabili NS, Abdollahi I, Khorramymehr S, Shirzad H, Bahadorany H. Quantitative evaluation of spasticity at the elbow of stroke patients. In: 2011 18th Iranian Conference of Biomedical Engineering (ICBME), pp. 2011:131–136 . https://doi.org/10.1109/ICBME.2011.6168540
Mirbagheri MM, Tsacr C-C, Rymer WZ. Abnormal intrinsic and reflex stiffness related to impaired voluntary movement. In: The 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, vol. 2, pp. 2004:4680–4683 . https://doi.org/10.1109/IEMBS.2004.1404296
: Mirbagheri MM, Chen D, Harvey RA, Rymer WZ. Quantification of spasticity: identification of reflex and intrinsic mechanical properties. In: First International IEEE EMBS Conference on Neural Engineering, 2003., pp. 2003:313–315 . https://doi.org/10.1109/CNE.2003.1196823
Engsberg JR, Ross SA, Hollander KW, Park TS. Hip spasticity and strength in children with spastic diplegia cerebral palsy. J Appl Biomech. 2000;16(3):221–33. https://doi.org/10.1123/jab.16.3.221.
Gholami S, Ansari NN, Naghdi S, Tabatabaei A, Jannat D, Senobari M, Dadgoo M. Biomechanical investigation of the modified Tardieu Scale in assessing knee extensor spasticity poststroke. Physiother Res Int. 2018;23(1):1–7. https://doi.org/10.1002/pri.1698.
Engsberg JR, Ross SA, Olree KS, Park TS. Ankle spasticity and strength in children with spastic diplegic cerebral palsy. Dev Med Child Neurol. 2000;42(1):42–7. https://doi.org/10.1017/S0012162200000086.
Baniasad MA, Farahmand M, Ansari NN. Wrist-RoboHab: a robot for treatment and evaluation of brain injury patients. In: 2011 IEEE International Conference on Rehabilitation Robotics Rehabilitation Robotics (ICORR), United States, p. 5975506. https://doi.org/10.1109/ICORR.2011.5975506
Pisano F, Miscio G, Del Conte C, Pianca D, Candeloro E, Colombo R. Quantitative measures of spasticity in post-stroke patients. Clin Neurophysiol. 2000;111(6):1015–22. https://doi.org/10.1016/S1388-2457(00)00289-3.
Sin M, Kim WS, Cho K, Paik NJ. Isokinetic robotic device to improve test-retest and inter-rater reliability for stretch reflex measurements in stroke patients with spasticity. J Vis Exp. 2019. https://doi.org/10.3791/59814.
Sin M, Kim W-S, Cho K, Cho S, Paik N-J. Improving the test-retest and inter-rater reliability for stretch reflex measurements using an isokinetic device in stroke patients with mild to moderate elbow spasticity. J Electromyogr Kinesiol. 2018;39:120–7. https://doi.org/10.1016/j.jelekin.2018.01.012.
McPherson JG, Stienen AHAA, Schmit BD, Dewald JPAA. Biomechanical parameters of the elbow stretch reflex in chronic hemiparetic stroke. Exp Brain Res. 2019;237(1):121–35.
Sung J, Choi S, Kim J, Kim J. A Simplified Estimation of Abnormal Reflex Torque due to Elbow Spasticity Using Neuro-musculoskeletal Model. In: 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), pp. 5076–5079. NLM (Medline), United States. https://doi.org/10.1109/EMBC.2019.8856613
Condliffe EG, Clark DJ, Patten C. Reliability of elbow stretch reflex assessment in chronic post-stroke hemiparesis. Clin Neurophysiol. 2005;116(8):1870–8. https://doi.org/10.1016/j.clinph.2005.02.030.
Grippo A, Carrai R, Hawamdeh Z, Falsini C, Aito S, Pinto F, de Scisciolo G, Pizzi A. Biomechanical and electromyographic assessment of spastic hypertonus in motor complete traumatic spinal cord-injured individuals. Spinal cord. 2011;49(1):142–8. https://doi.org/10.1038/sc.2010.56.
Pierce SR, Johnston TE, Shewokis PA, Lauer RT. Examination of spasticity of the knee flexors and knee extensors using isokinetic dynamometry with electromyography and clinical scales in children with spinal cord injury. J Spinal Cord Med. 2008;31(2):208–14. https://doi.org/10.1080/10790268.2008.11760714.
Pierce SR, Lauer RT, Shewokis PA, Rubertone JA, Orlin MN. Test-retest reliability of isokinetic dynamometry for the assessment of spasticity of the knee flexors and knee extensors in children with cerebral palsy. Arch Phys Med Rehabil. 2006;87(5):697–702. https://doi.org/10.1016/j.apmr.2006.01.020.
Xu D, Wu Y-N, Gaebler-Spira D, Gao F, Clegg NJ, Delgado MR, Zhang L-Q. Neural and non-neural contributions to ankle spasticity in children with cerebral palsy. Dev Med Child Neurol. 2020;62(9):1040–6. https://doi.org/10.1111/dmcn.14506.
Kim DY, Park C-I, Chon JS, Ohn SH, Park TH, Bang IK. Biomechanical assessment with electromyography of post-stroke ankle plantar flexor spasticity. Yonsei Med J. 2005;46(4):546–54. https://doi.org/10.3349/ymj.2005.46.4.546.
Rabita G, Dupont L, Thevenon A, Lensel-Corbeil G, Perot C, Vanvelcenaher J. Quantitative assessment of the velocity-dependent increase in resistance to passive stretch in spastic plantarflexors. Clin Biomech (Bristol, Avon). 2005;20(7):745–53. https://doi.org/10.1016/j.clinbiomech.2005.04.002.
Woolacott AJ, Burne JA. The tonic stretch reflex and spastic hypertonia after spinal cord injury. Exp Brain Res. 2006;174(2):386–96. https://doi.org/10.1007/s00221-006-0478-7.
Jobin APT, Levin MF. Regulation of stretch reflex threshold in elbow flexors in children with cerebral palsy: a new measure of spasticity. Dev Med Child Neurol. 2000;42(8):531–40. https://doi.org/10.1017/S0012162200001018.
Chow JW, Yablon SA, Stokic DS. Knee muscle stretch reflex responses after an intrathecal baclofen bolus in neurological patients with moderate-to-severe hypertonia. Neuromodul J Int Neuromodul Soc. 2020;23(7):1018–28. https://doi.org/10.1111/ner.13112.
Tuzson AE, Granata KP, Abel MF. Spastic velocity threshold constrains functional performance in cerebral palsy. Arch Phys Med Rehabil. 2003;84(9):1363–8. https://doi.org/10.1016/S0003-9993(03)00199-0.
Germanotta M, Taborri J, Rossi S, Frascarelli F, Palermo E, Cappa P, Castelli E, Petrarca M. Spasticity measurement based on tonic stretch reflex threshold in children with cerebral palsy using the PediAnklebot. Front Hum Neurosci. 2017;11:277. https://doi.org/10.3389/fnhum.2017.00277.
Rabita G, Dupont L, Thevenon A, Lensel-Corbeil G, Perot C, Vanvelcenaher J. Differences in kinematic parameters and plantarflexor reflex responses between manual (Ashworth) and isokinetic mobilisations in spasticity assessment. Clin Neurophysiol. 2005;116(1):93–100. https://doi.org/10.1016/j.clinph.2004.07.029.
Centen A, Lowrey CR, Scott SH, Yeh T-T, Mochizuki G. KAPS (kinematic assessment of passive stretch): a tool to assess elbow flexor and extensor spasticity after stroke using a robotic exoskeleton. J Neuroeng Rehabil. 2017;14(1):59. https://doi.org/10.1186/s12984-017-0272-8.
Hong MJ, Park JB, Lee YJ, Kim HT, Lee WC, Hwang CM, Lim HK, Lee DH. Quantitative evaluation of post-stroke spasticity using neurophysiological and radiological tools: a pilot study. Ann Rehabil Med. 2018;42(3):384–95. https://doi.org/10.5535/arm.2018.42.3.384.
Misgeld BJE, Luken M, Heitzmann D, Wolf SI, Leonhardt S. Body-sensor-network-based spasticity detection. IEEE J Biomed Health Inform. 2016;20(3):748–55. https://doi.org/10.1109/JBHI.2015.2477245.
Voerman GE, Fleuren JFM, Kallenberg LAC, Rietman JS, Snoek GJ, Hermens HJ. Patient ratings of spasticity during daily activities are only marginally associated with long-term surface electromyography. J Neurol Neurosurg Psychiatry. 2009;80(2):175–81. https://doi.org/10.1136/jnnp.2008.147090.
Winslow J, Martinez A, Thomas CK. Automatic identification and classification of muscle spasms in long-term EMG recordings. IEEE J Biomed Health Inform. 2015;19(2):464–70. https://doi.org/10.1109/JBHI.2014.2320633.
Albani G, Cimolin V, Galli M, Vimercati S, Bar D, Campanelli L, Gandolfi R, Lombardi R, Mauro A. Use of surface EMG for evaluation of upper limb spasticity during botulinum toxin therapy in stroke patients. Funct Neurol. 2010;25(2):103–8.
Lasek A-K, von Werder SCAF, Werner CJ, Disselhorst-Klug C. Introduction of a procedure to objectively quantify spastic movement impairment during freely performed voluntary movements. J Electromyogr Kinesiol. 2019;48:44–52. https://doi.org/10.1016/j.jelekin.2019.06.001.
Tirosh O, Rutz E. Quantifying the velocity-dependent muscle response during gait of children with Cerebral Palsy. J Electromyogr Kinesiol. 2019;48:76–83. https://doi.org/10.1016/j.jelekin.2019.06.007.
van der Krogt MM, Doorenbosch CAM, Becher JG, Harlaar J. Dynamic spasticity of plantar flexor muscles in cerebral palsy gait. J Rehabil Med. 2010;42(7):656–63. https://doi.org/10.2340/16501977-0579.
Turpin NA, Feldman AG, Levin MF. Stretch-reflex threshold modulation during active elbow movements in post-stroke survivors with spasticity. Clin Neurophysiol. 2017;128(10):1891–7. https://doi.org/10.1016/j.clinph.2017.07.411.
Barden HLH, Nott MT, Baguley IJ, Heard R, Chapparo C. Test-retest reliability of computerised hand dynamometry in adults with acquired brain injury. Aust Occup Ther J. 2012;59(4):319–27. https://doi.org/10.1111/j.1440-1630.2012.01016.x.
Mochizuki G, Centen A, Resnick M, Lowrey C, Dukelow SP, Scott SH. Movement kinematics and proprioception in post-stroke spasticity: assessment using the Kinarm robotic exoskeleton. J Neuroeng Rehabil. 2019;16(1):1–13. https://doi.org/10.1186/s12984-019-0618-5.
Diserens K, Perret N, Chatelain S, Bashir S, Ruegg D, Vuadens P, Vingerhoets F. The effect of repetitive arm cycling on post stroke spasticity and motor control: repetitive arm cycling and spasticity. J Neurol Sci. 2007;253(1):18–24. https://doi.org/10.1016/j.jns.2006.10.021.
Askin A, Kalayci OT, Bayram KB, Tosun A, Demirdal US, Atar E, Kalayci OT, Inci MF. Strain sonoelastographic evaluation of biceps muscle intrinsic stiffness after botulinum toxin-A injection. Top Stroke Rehabil. 2017;24(1):12–7. https://doi.org/10.1080/10749357.2016.1183865.
Illomei G. Muscle elastography in multiple sclerosis spasticity. Neurodegener Dis Manag. 2016;6(6 s):13–6. https://doi.org/10.2217/nmt-2016-0048.
Picelli A, Tamburin S, Cavazza S, Scampoli C, Manca M, Cosma M, Berto G, Vallies G, Roncari L, Melotti C, Santilli V, Smania N. Relationship between ultrasonographic, electromyographic, and clinical parameters in adult stroke patients with spastic equinus: an observational study. Arch Phys Med Rehabil. 2014;95(8):1564–70. https://doi.org/10.1016/j.apmr.2014.04.011.
Dash A, Dutta A, Lahiri U. Quantification of grip strength with complexity analysis of surface electromyogram for hemiplegic post-stroke patients. NeuroRehabilitation. 2019;45(1):45–56. https://doi.org/10.3233/NRE-192734.
Pizzi A, Carlucci G, Falsini C, Verdesca S, Grippo A. Evaluation of upper-limb spasticity after stroke: a clinical and neurophysiologic study. Arch Phys Med Rehabil. 2005;86(3):410–5. https://doi.org/10.1016/j.apmr.2004.10.022.
Aarestad DD, Williams MD, Fehrer SC, Mikhailenok E, Leonard CT. Intra- and interrater reliabilities of the myotonometer when assessing the spastic condition of children with cerebral palsy. J Child Neurol. 2004;19(11):894–901. https://doi.org/10.1177/08830738040190110801.
Carlyle JK, Mochizuki G. Influence of post-stroke spasticity on EMG-force coupling and force steadiness in biceps brachii. J Electromyogr Kinesiol. 2018;38:49–55. https://doi.org/10.1016/j.jelekin.2017.11.005.
Simpson DM, Patel AT, Alfaro A, Ayyoub Z, Charles D, Dashtipour K, Esquenazi A, Graham GD, McGuire JR, Odderson I. Onabotulinumtoxina injection for poststroke upper-limb spasticity: guidance for early injectors from a delphi panel process. PM &R. 2017;9(2):136–48.
Sandrini G, Baricich A, Cisari C, Paolucci S, Smania N, Picelli A. Management of spasticity with onabotulinumtoxina: practical guidance based on the italian real-life post-stroke spasticity survey. Funct Neurol. 2018;33(1):37.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the design of the review. XG and RW performed the screening of the papers. XG performed the data extraction. XG and VC did the data analysis and drafted the manuscript. All the authors revised, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Assessment methods extraction table.
Additional file 2: Table S2.
Psychometric properties extraction table.
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, X., Wallace, R., Tan, Y. et al. Technology-assisted assessment of spasticity: a systematic review. J NeuroEngineering Rehabil 19, 138 (2022). https://doi.org/10.1186/s12984-022-01115-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-022-01115-2