
Abstract
Background
Sexual and reproductive health (SRH) is at the base of young people's living and wellbeing. A significant number of young peoples are affected by avoidable SRH problems due to a lack of appropriate knowledge regarding SRH. Parent-young communication on SRH is critical in informing them about risk and protective behaviors which in turn decrease the likelihood of involvement in risky sexual behaviors. Therefore, the purpose of this study was to evaluate the parent-young communication on SRH issues and associated factors among secondary and preparatory school students at Agaro town, Southwestern Ethiopia.
Methods
School based cross-sectional study was conducted from April 13 to April 20, 2019 using stratified random sampling technique. A total of 315 students were included to the study. Data were collected using pretested interviewer-administered structured questionnaire entered into Epi data version 3.1; and analyzed using SPSS version 20. A variable having a p-value of < 0.25 in the bivariable logistic regression model was subjected to multivariable logistic regression analysis to avoid the confounding variable’s effect. Adjusted odds ratios were calculated at the 95% confidence interval and considered significant with a p-value of < 0.05.
Results
The mean age of the respondents was 20.2 ± 2.6 years. The study finding showed that 61.3% of the participants were discussed on SRH issues with their parents. According to multivariate analysis; educational status of mother [primary education (AOR = 3.67; 95%CI = 1.93, 6.97),secondary education(AOR:2.86; 95%CI = 1.20, 6.80)],educational status of father[primary education (AOR = 5.8;95%CI = 2.8, 12.3,secondary education (AOR = 3.21; 95%CI = 1.55, 6.59)],having family size of < 5 (AOR = 6.4; 95%CI = 3.36, 12.37) and having boy/girlfriend(AOR = 1.99; 95%CI = 1.0, 3.8) were significantly associated with parent-young people communication.
Conclusion
About two third of the participants communicate with their parents about SRH issues and parents’ educational status, family size of < 5 and having boy/girlfriend were significantly associated with it. The main reasons for not communicated was cultural taboos, shame and parents lack of knowledge. Therefore, it is necessary to educate and equip students and parents to address the identified problems.
Plain English summary
Sexual and reproductive health (SRH) is at the base of young people's living and wellbeing. A significant number of young peoples are affected by avoidable SRH problems. Parent-young communication on SRH is critical in informing them about risk and protective behaviors which in turn decrease the likelihood of involvement in risky sexual behaviors. This study was intended to assess this issue on students learning at Agaro town, Ethiopia during April 13 to April 20, 2019 using pretested interviewer-administered structured questionnaire with sample size of 315.
The study finding showed that 61.3% of the participants were discussed on SRH issues with their parents. According to multivariable logistic regression analysis educational status of parents, having family size of < 5 and boy/girlfriend were significantly associated with parent adolescent communication. Cultural taboos, shame and parents lack of knowledge were the major barriers for communication. Thus, it is necessary to educate students and parents to address the identified problems thereby prevent young population from risky sexual behaviors.
Similar content being viewed by others


Introduction
Globally, there are 1.8 billion young people (age 10–24 years) and 90% of them live in developing countries [1, 2]. Young age is a critical stage of rapid biological and psychosocial changes that affect all aspects of life, and it is also an important period to lay the foundations of good health in adulthood [3]. Unsafe abortion, early pregnancy, high rates of sexually transmitted infections (STIs), difficulty accessing contraception, cultural factors and socio-economic are some of the challenges faced by young people [4].
Each year around the globe sixteen million late adolescent girls give birth, in which 95 percent of them occur in developing countries [5]. Young people usually engage in risky sexual behaviors and highly affected by the burden of unwanted pregnancy, HIV/AIDS, STIs and other reproductive ill health due to lack of awareness about risky sexual behaviors [6,7,8]. Globally greater than 60% of young people were living with HIV, and they also account for 58% of newly acquired HIV infections [9]. Unplanned and unwanted pregnancy for unmarried young women results in dropout of school, rejection from family and community. The main cause for the above situation is the gap in promoting the sexual and reproductive health (SRH) agenda and young population health is usually ignored area in health priority [10].
One of the priorities of the Sustainable Development Goals is improving the SRH of the young population [11]. To this end, Ethiopia has also developed a strategy specifically targeting young people [12]. However, There are only few national programs specifically targeted to addressing the needs of this group and the problem of SRH among young people remains a challenge [13]. Moreover, lack of integration and shortage of young-friendly services are common problems in most developing countries, including our country [4].
Parent-young population communication on SRH issues is vital in reducing risky sexual behaviors and negative its consequences [14]. It is fundamental process through which parents transmit sexual values, information, beliefs, and expectations to their children with the purpose of influencing sexual behaviours, attitudes and decision-making of their children [15]. Parent-young population communication is one potential source of SRH information for young people [16]. Evidence revealed that 29% of premarital sex is due to inappropriate parenting [17]. The Ethiopian government has established a strategic goal to encourage parental participation, but little is known about parental participation [18] and the role and current status of parent-young population discussions on SRH issues have not been well addressed yet [19].
Reasons for not discussing with parents include sociocultural norms, lack of knowledge and parental fear [20]. As a result, most of the young people attempts regarding sexual matters is generally misguided by their peer group of the same sex and many teenagers do not have access to reliable information regarding their SRH needs. A significant number of young peoples are affected by avoidable SRH problems due to a lack of appropriate knowledge regarding SRH. Parent-young communication on SRH is critical in informing them about risk and protective behaviors [6, 21]. According to previous studies, the factors associated with the parent-young people communication about SRH were parental education, adolescent’s age and living arrangements, type of parents, and parents’ SRH knowledge and attitude [20, 22, 23] (Additional file 1).
Generally, there is inadequate evidence about the proportion of parent-young people communication in Ethiopia [24], point prevalence varies among the studies and there is no established evidence at the study area. Moreover, there are inconsistent findings with regard to proportion and factors associated with parent and young people communication on SRH issues. For instance, according to study finding gender had a positive relationship with communication on SRH [22, 25] while other studies showed no association [6].
Hence, this study was aimed at assessing the proportion and associated factors of parent young communication on SRH among secondary and preparatory school students for risk minimization and better health at the study area. This study will help to provide information regarding the proportion of parent young people communication on SRH and its determinants which helps as an input to design appropriate intervention programs. Furthermore, this study was attempted to generate evidence based information for concerned government bodies and policy makers to consider the situation and to design an appropriate intervention strategy.
Methods and materials
Study area
The study was conducted at Agaro town, Jimma Zone, Southwest Ethiopia. It is located 45 km from Jimma town and 391 km from Addis Ababa. There are educational services from kindergarten to university in the town and it has two health centers and one primary hospital. There are 2 secondary and preparatory schools and 4 secondary schools in the town. According to the data obtained from school directors, the school had 2818 total regular secondary and preparatory students during the study period.
Study period
The study was conducted from April 13 to April 20, 2019.
Study design
A descriptive facility based cross-sectional study was conducted among secondary and preparatory school students at Agaro town.
Study population
The source population comprised of all Agaro secondary and preparatory school students whose age was 10–24 years during the academic year of 2019, while the study population comprised all Agaro secondary and preparatory school students who fulfilled the inclusion criteria.
Eligibility criteria
Regular students were included in the study, whereas students absent from class on data collection days live alone, orphans or live with guardian who are not their biological parents, deaf, dumb students, sick and married students were excluded.
Sample size determination
The sample size was determined using single population proportion formula considering the following assumptions: P = 28.9% [26], significance level 5% and margin of error 5%.
where n = required sample size, Z = Percentiles of the standard normal distribution corresponding to 95% confidence level assumption, \(z \alpha \left/ 2 \right.\)= Coefficient at level of significance = 1.96, p = 28.9% proportion of parent young communication (according to study done in Mizan), d = Margin of error = 0.05.
Accordingly it gives initial sample size of 317. Since the source population is less than 10,000, (2818), we employed population correction formula for a finite population.
where: N = sample size. N = total population (2818). nf = final sample size.
By taking into consideration 10% non-response rate, the final sample size was 286 + 28.6 = 315.
Sampling procedure
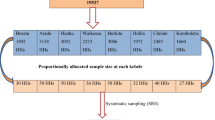
Stratified random sampling technique was employed to select study participants. First the sampling frame was prepared by having lists of students from grade 9 to 12 and then the sample population was proportionally assigned to each grade. Proportional allocation was done by allocating sampling proportional to the total population of each unit, using the formula:
where ni = sample size of students from each grade, n = total sample size of students, N = total population of students, and Ni = total population of students at each grade. Finally samples were selected from each class by simple random sampling technique using students’ roster (Fig. 1).

Schematic diagram representation of sampling procedure for selecting participants at Agaro secondary and preparatory school, Southwest Ethiopia 2021
Operational definition
Parents: in this study mean biological parents, step parents or foster parents but does not include elder siblings [27].
Parent-young communication on SRH: Students open discussion on at least two SRH issues (STIs/ HIV/AIDS, condom, sexual intercourse, premarital sex, puberty, menstrual cycle, unwanted pregnancy and contraception) with their parents in the last 12 months initiated by the young population or both [28].
Secondary school students: students who were in grade 9 and 10.
Preparatory school students: students who were in grade 11 and 12.
Regular students: students who were assigned on working day (from Monday to Friday) on regular working hour.
Young people: In this study context are peoples who are between 10–24 year olds.
Ever got SRH information = in this study context participants who had SRH information on at least two SRH issues during their life time.
Residence: In our study context place where students live for at least 6 months.
Ethnicity: nation of the study participant they belongs.
Data collection instrument
Data were collected using pretested, validated, self-administered structured questionnaire which was developed through reviewing different related scientific literatures [6, 25, 26, 29] and it was pre-tested before collecting data to ensure data quality. The data were collected by six diploma graduate nurses under the supervision of two supervisors and principal investigator. Data collectors were supervised by two diploma midwives.
Data quality control
Data quality was ensured through standardized data collection materials and the English version questionnaire was translated to local language (Oromic) version for appropriateness and easiness by language experts in both cases. The Oromic version was again translated back to English language to verify the content validity of the original version.
Two days of training was given for data collectors about the aim of the study, how to approach the study subjects, sampling procedure and the content of the questionnaire. The questionnaires were pre-tested on 5% of participants at the Jiren secondary and preparatory school one week ahead of actual data collection and further modified based on the results. Continuous follow-up and supervision were made by the two supervisors and principal investigator and collected data were reviewed and checked daily for clarity, completeness and consistency.
Data entry, processing and analysis
The collected data was compiled, reviewed, coded and entered in to Epidata version 3.1 and exported to SPSS version 20 for analysis. Data was checked and cleaned for its completeness and errors in coding and entering before analysis. Descriptive statistical analysis was used to compute frequency and a percentage of independent and dependent variables. A logistic regression model was computed to see the association of independent variables and dependent variables. Variables with p ≤ 0.25 on bivariable logistic regression were considered as candidates for multivariable regression and P-values of < 0.05 were considered to be statistically significant in the multivariable analysis. Crude and adjusted odds ratios with their 95% confidence intervals were calculated. The Hosmer and Lemeshow goodness-of-fit test were checked and gave a p value of 0.704, indicating evidence of fitness of the model. The variance inflation factor was used to verify the multico-llinearity between the independent variables, and no findings were found.
Results
Socio demographic characteristics of the study population
A total of 315 students were included to the study. The mean age of the respondents was 20.2 ± 2.6 years. Regarding religion most of the respondents 263(83.5%) were muslim. One hundred forty one (44.7%) was grade nine students followed by grade ten students who account 105 (33.3%). Most of young students lives with both parents 279(88.6%). Almost half (53.3%) of the participants had ever got SRH information (Table 1).
Communication on sexual and reproductive health issues
Although 92% of the respondents reported that it was important to discuss SRH issues with parents, only 61.3% had communicated with their parents on at least two SRH topics. The major topics discussed among participants were premarital sex (40%) followed puberty (37.8%) (Table 2).
Only hundred twelve (35.6%) of the students had discussed about STIs/HIV/AIDS because of parents’ lack of knowledge (49.5%) and shame (35.9%). Similarly only 23.8% of the students discussed with their parents about unwanted pregnancy due to shame (46%) and parents lack of (24.8%) (Table 3).
Factors associated with parent-young communications on SRH issues
Bivariable logistic regression analysis was performed to assess association between each independent variable and outcome variable. Results of bivariable analysis showed that sex of student, mother education status, father education status, age, having ever got SRH information, having boy/girlfriend, residence, occupation of family and family size show association with parent-young communication. All of them were entered to multivariable analysis to control effect of confounding. The result of multivariable logistic regression model revealed that educational status of biological parents, family size of < 5 and having boy/girlfriend were significantly associated with parent adolescent communication.
The odds of parent-young communication were 6.4 times [AOR = 6.4; 95% CI: 3.36, 12.37] higher among students of family size of < 5 than their counter parts. The odds of parent-young communication were 1.99 times [AOR = 1.99; 95% CI: 1.3.0, 8.0] higher among students who had boy/girlfriend than those who had no boy/girlfriend.
Young students, whose mothers had primary education, were 3.67 times more likely to communicate on SRH issues with their parents than those students whose mothers were illiterate (AOR = 3.67; 95%CI:1.93–6.97). Similarly, young students whose mothers had secondary education were 2.86 times more likely to communicate on SRH issues with their parents than those students whose mothers were illiterate (AOR = 2.86; 95%CI: 1.2, 6.8).This study also revealed fathers’ education [primary education (AOR = 5.8 95%CI: 2.8, 12.3),secondary education (AOR = 3.21 95%CI:1.55, 6.59)]were significantly associated with parent-young communication after controlling for confounders (Table 4).
Discussion
This study has attempted to assess the proportion of parent-young communication on SRH issues and its associated factors in Agaro secondary and preparatory school students, Southwest Ethiopia. The magnitude of parental communication on SRH issues was reported to be only 61.3% (193) [95% CI: 55.6, 66.7]. This finding was in line with two independent studies done in Ethiopia, 59.1% in Yergalem, South Ethiopia [29] and 57.6% in Mekelle, Northern Ethiopia [30]. However, this result was higher than three independent studies done in Ethiopia: 48.5% in Dabat, Northwest Ethiopia [31], 47% in Robe, Southeast Ethiopia [32] and 37% in Dire Dewa, Eastern Ethiopia [6]. Those differences might be due to the difference in socio-demographic, cultural difference and accessing sexual reproductive health information. For example, the possible explanation of higher prevalence in our study could be due to home to home, school and mass health education and information by Jimma University health science students during community based team training program every year.
In contrast, the finding of the current study was lower than that of a study conducted in Hayik and Wolaita Sodo, Ethiopia were 83% [25] and 85%, respectively [33]. The possible reason for the difference in our finding and the one from Wolaita Sodo could be due to the difference in the study population, i.e., the study from Wolaita Sodo included only female university students with large sample size who have better information. Similarly in the study conducted in Hayk, more than three-quarters of the participants lived in urban areas with adequate access to reproductive health services, and all participants were from preparatory schools. Moreover, the study from Ghana reported 82.3% [34]. The difference might be related to difference in sample size used, sampling technique and culture related to openness related to SRH issues.
The major topics discussed among participants were premarital sex, puberty and STIs/HIV/AIDS, while topics like contraception was discussed less among participants. The possible justification might be as majority of the participants were Muslim followers and their religion did not encourage them to use contraception including condoms which might affect their discussion. Thus, we recommend future study supported with qualitative findings to explore on this issue.
Regarding challenges for not discussing SRH issues shame, cultural taboos, embarrassments and parents' lack of knowledge were mentioned by the majority of participants. For instance, almost three quarters of participants were not discussed regarding unwanted pregnancy due to shame and parents’ lack of knowledge 46% and 24.8%, respectively. This was consistent with previous studies [25, 27]. This might be due to the fact that sexual conversations are deemed a taboo subject in many African communities, including our country. Moreover, parent-young communication on SRH issues in Ethiopia is believed to be socially disgraceful and parents are not open and uncomfortable to discuss these issues with their young children [35].
In agreement with earlier studies, in this study educational status of father and mother showed statistical significance with parent adolescent communication about SRH issues [25, 36, 37]. This could be due to educated parents have better access to health service information, improved perceptions of SRH issue and better skill of communication.
In the same manner, the study showed that those students whose family size was less than five were more likely to communicate which agreed with previous study [38]. This result demonstrated that those parents with small family size had better chance of discussing SRH issues with their children. Finally, the present study revealed that there were significant association between parent adolescent’s sexual and reproductive issues and having boy/girlfriend. The possible reason for this association might be students who enter to relationship might raise about SRH issues with each other and they may discuss with their parents for more information.
Limitation of the study
1st due to cross-sectional nature of the study, it was difficult to imply cause–effect relationship. 2nd this study was done to assess parent young-people communication were based on young population perceptions, which may not reflect what parents were actually doing. 3rd, since it was based on self-reporting, it might be affected by social desirability bias because of sensitive nature and cultural barrier for open discussion and finally additional qualitative study should be done to explore more on young and parents communication.
Conclusion
This study showed about two third of young population had discussion on SRH issues with their parents on at least two SRH issues. Educational level of parents, having family size of < 5 and having boy/girlfriend were significantly associated with communication. The main reasons for not communicated was cultural taboos, shame and parents lack of knowledge. Thus, it is necessary to educate and equip students and parents to address the identified problems.
Students and their parents should receive health education on the significance of talking about SRH issues and related consequences of risky sexual behaviors. To promote and support school sex education, teachers should receive SRH training. Moreover, more research is required to identify barriers especially with regard to parents.
In order to build a supportive atmosphere for parent-young people communication regarding SRH, policy makers will need to design tailored action to create supportive environment for parent young people communication concerning SRH.
Availability of data and materials
The data used to support the findings of this study can be available from the corresponding author upon reasonable request.
References
World Health Organization. Engaging young people for health and sustainable development: strategic opportunities for the World Health Organization and partners. 2018.
Gupta MD. The Power of 1.8 Billion: Adolescents, Youth and the transformation of the future: United Nations Population Fund; 2014.
Organization, W.H., Health for the world’s adolescents: a second chance in the second decade: summary. 2014.
Morris JL, Rushwan H. Adolescent sexual and reproductive health: the global challenges. Int J Gynecol Obstet. 2015;131:S40–2.
Braine T. Adolescent pregnancy: a culturally complex issue. World Health Organization. Bull World Health Organiza. 2009;87(6):410.
Ayalew M, Mengistie B, Semahegn A. Adolescent-parent communication on sexual and reproductive health issues among high school students in Dire Dawa, Eastern Ethiopia: a cross sectional study. Reprod Health. 2014;11(1):1–8.
World Health Organization Executive Board. Early marriages, adolescent and young pregnancies. Geneva: WHO; 2011.
Mekonen MT, Dagnew HA, Yimam TA, Yimam HN, Reta MA. Adolescent-parent communication on sexual and reproductive health issues and associated factors among high school students in Woldia town, Northeastern Ethiopia. Pan Afr Med J. 2018;31(1).
WHO Consolidated guideline on sexual and reproductive health and rights of women living with HIV. Geneva. 2017
Singh NS, Aryasinghe S, Smith J, Khosla R, Say L, Blanchet K. A long way to go: a systematic review to assess the utilisation of sexual and reproductive health services during humanitarian crises. BMJ Global Health. 2018;3(2).
GA U. Transforming our world: the 2030 Agenda for Sustainable Development. Division for Sustainable Development Goals: New York. 2015.
National Adolescent and Youth Health Strategy of Ethiopia. Federal Democratic Republic of Ethiopia, Ministry of Health. 2016.
Federal Democratic Republic of Ethiopia (FDROE), Ministry of Health (MOH). National adolescent and youth Reproductive Health Strategy (2007–2015) https://extranet.who.int/countryplanningcycles/sites/default/files/planning_cycle_repository/ethiopia/ayrh_strategy.pdf
Yang H, Stanton B, Li X, Cottrel L, Galbraith J, Kaljee L. Dynamic association between parental monitoring and communication and adolescent risk involvement among African–American adolescents. J Natl Med Assoc. 2007;99(5):517.
Jerman P, Constantine NA. Demographic and psychological predictors of parent–adolescent communication about sex: A representative statewide analysis. J Youth Adolesc. 2010;39(10):1164–74.
United Nations Population Fund Global sexual and reproductive health package for men and adolescent boys. 2017
Fajar NA, Etrawati F, Lionita W. Determinant of parents role in adolescent premarital sex behavior: an applicative model. Media Kesehatan Masyarakat Indonesia. 2019;15(2):143–9.
Federal Democratic Republic of Ethiopia Minstry of Health (2006) National adolescent and youth reproductive health strategy 2006–2015. Available from https://www.exemplars.health/-/media/files/egh/resources/underfive-mortality/ethiopia/ethiopia-fmoh_national-reproductive-health-strategy.pdf?la=en
Federal Democratic Republic of Ethiopia, Ministry of Health. National Reproductive Health Strategy, (2006–2015) Addis Ababa: FMOH; 2006. Available from https://www.exemplars.health/-/media/files/egh/resources/underfive-mortality/ethiopia/ethiopia-fmoh_national-reproductive-health-strategy.pdf?la=en
Yadeta TA, Bedane HK, Tura AK. Factors affecting parent-adolescent discussion on reproductive health issues in Harar, Eastern Ethiopia: a cross-sectional study. J Environ Public Health. 2014;29:2014.
Ayehu A, Kassaw T, Hailu G. Young people’s parental discussion about sexual and reproductive health issues and its associated factors in Awabel woreda, Northwest Ethiopia. Reprod Health. 2016;13(1):19.
Tesso DW, Fantahun MA, Enquselassie F. Parent-young people communication about sexual and reproductive health in E/Wollega zone, West Ethiopia: implications for interventions. Reprod Health. 2012;9(1):13.
Melaku YA, Berhane Y, Kinsman J, Reda HL. Sexual and reproductive health communication and awareness of contraceptive methods among secondary school female students, northern Ethiopia: a cross-sectional study. BMC Public Health. 2014;14(1):252.
Yalew M, Adane B, Kefale B, Damtie Y, Arefaynie M, Wedajo S, Bitew A, Wasihun Y. Parent-young communication on sexual and reproductive health issues and its association with sex and perceptions of young people in Ethiopia, 2020: a systematic review and meta-analysis. Arch Public Health. 2020;78(1):1–1.
Chane T, Cherie N. Parent-adolescent communication about sexual and reproductive health and associated factors among preparatory school students in Haiyk Town, North East Ethiopia. Res Med Eng Sci. 2018;5(2):417–23.
Shewasinad S, Alelign Z, Yeshitla K, Bunga G, Negash S. Assessment of Communication on Sexual and Reproductive Health Issues among Mizan Secondary and Preparatory School Students with Parents, Mizan Town, Ethiopia, 2016. Am J Health Res. 2017;5(5):131–40.
Adu-Mireku S. Family communication about HIV/AIDS and sexual behaviour among senior secondary school students in Accra, Ghana. Afr Health Sci. 2003;3(1):7–14.
Shiferaw K, Getahun F, Asres G. Assessment of adolescents’ communication on sexual and reproductive health matters with parents and associated factors among secondary and preparatory schools’ students in Debremarkos town, North West Ethiopia. Reprod Health. 2014;11(1):1.
Yohannes Z, Tsegaye B. Barriers of parent-adolescent communication on sexual and reproductive health issues among secondary and preparatory school students in Yirgalem, Town, South Ethiopia. Fam Med Med Sci Res. 2015;4(181):2.
Yowhanes Z, Berhe H, Hailu D. Assessment of parent-adolescent communication about sexual and reproductive health among high school students in Mekelle Town, Northern Ethiopia. Global J Med Res. 2016;16(2).
Dagnachew Adam N, Demissie GD, Gelagay AA. Parent–Adolescent communication on sexual and reproductive health issues and associated factors among preparatory and secondary school students of Dabat Town, Northwest Ethiopia. J Environ Public Health. 2020;25:2020.
Habte NM, Melku AT, Alemayehu MT. Parent–adolescent communication on sexual and reproductive health matters and associated factors among secondary and preparatory school students in Robe Town, Bale Zone, Southeast Ethiopia, 2017. J Public Health Int. 2019;1(4):1.
Tsegay M. Assessment of sexual and reproductive health communication practice and associated factors among female undergraduate students of Wolaita Sodo University, Southern Ethiopia (Doctoral dissertation, Addis Ababa University).
Manu AA, Mba CJ, Asare GQ, Odoi-Agyarko K, Asante RK. Parent–child communication about sexual and reproductive health: evidence from the Brong Ahafo region, Ghana. Reprod Health. 2015;12(1):16.
Taffa N, Bjune G, Sundby J, Gaustad P, Alestrøm A. Prevalence of gonococcal and chlamydial infections and sexual risk behavior among youth in Addis Ababa, Ethiopia. Sexually Transmit Dis. 2002;29(12):828–33.
Musa OI, Akande TM, Salaudeen AG, Soladoye OM. Family communication on HIV/AIDS among secondary school students in a northern state of Nigeria. Afr J Infect Dis. 2008;2(1):46–50.
Fanta M, Lemma S, Sagaro GG, Meskele M. Factors associated with adolescent–parent communication of reproductive health issues among high school and preparatory students in Boditi town, Southern Ethiopia: a cross-sectional study. Patient Intell. 2016;14(8):57–70.
Mekie M, Taklual W, Melkie A, Addisu D. Parental communication on sexual and reproductive health issues and its associated factors among preparatory school students in Debre Tabor, Northcentral Ethiopia: institution based cross-sectional study. BMC Res Notes. 2019;12(1):598.
Acknowledgements
We want to acknowledge our study participants and data collectors.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
DA participated in the design of the study, performed the statistical analysis and helped to revise the manuscript. WS conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from the Institutional Review Board of the Jimma University (Ref. No. IHRPGn/153/). A formal letter of cooperation was written to the school administration Agaro District Education Office for permission and support. After ethical approval, the objective of the study was described and oral informed consent was obtained from study participants aged ≥ 18 years and parental informed consent was obtained for those who were aged ≥ 15 years after explaining the purpose of the study. Information was recorded anonymously and confidentiality and beneficence were assured throughout the process.
Consent for publication
Not applicable.
Competing interests
The authors of this study declare that have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abdissa, D., Sileshi, W. Parent-young communication on sexual and reproductive health issues and its associated factors: experience of students in Agaro Town, Ethiopia. Reprod Health 20, 11 (2023). https://doi.org/10.1186/s12978-022-01553-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-022-01553-0