
Abstract
Background
There is no national representative and conclusive data regarding parent-young communication. Therefore, this study aimed to estimate the pooled prevalence of parent-young communication on sexual and reproductive health issues and its association with sex and perceptions of young people about its importance in Ethiopia, 2020.
Methods
The Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) was used during systematic review and meta-analysis. The study included both published and gray literatures which were searched using appropriate key terms. The articles were searched from different databases: PubMed, Cochrane Library, PsycINFO, CINAHL, Global Health, HINARI and Google scholar. Data were extracted in a Microsoft Excel sheet and STATA/SE 14 was used for meta-analysis. I2 and Egger test statistics were used to test heterogeneity and publication bias respectively.
Results
Twenty-nine articles were included in this systematic review and meta-analysis. The pooled prevalence of parent-young communication on sexual and reproductive health issues in Ethiopia was 42.96% [95% CI: (36.91, 49.02)]. Positive perception of young people towards parent-young communication [AOR = 3.72, 95% CI: (2.87, 4.86)] and female sex [AOR = 1.62, 95% CI: (1.12, 2.34)] were significantly associated with parent-young communication on sexual and reproductive health issues.
Conclusions
The prevalence of parent-young communication on sexual and reproductive health issues in Ethiopia was low as compared to other literatures conducted outside Ethiopia. Both perceptions of young people towards parent-young communication and sex were significantly associated with parent-young communication on sexual and reproductive health issues. Interventions targeting males and young who had negative perceptions regarding parent-young communication should be the primary focus of the government and their parents.
Review registration
The protocol of this systematic review and meta-analysis was registered in the PROSPERO International prospective of systematic reviews with a specific registration number: CRD42020161252.
Similar content being viewed by others


Background
According to the World Health Organization (WHO), young were populations aged from 10 to 24 years. Globally, the numbers of the young population were estimated to be 1.8 billion, of which 90% of them were lived in developing countries [1, 2]. Adolescent is the time of experimentation and in the course of such experimentation, they are often encountered in high-risk situations especially Human Immune Deficiency Virus (HIV) and unwanted pregnancy [3, 4]. The prevalence of parent-adolescent communication on reproductive health in Bangladesh was 65.6% [5] and ranged between 21 to 46.7% in Nigeria [6, 7]. Whereas, it was 53% in Kenya [8] and 60% in Zambia [9]. In Ethiopia, the prevalence of parent-young communication on sexual and reproductive health issues was ranged from 8.84 to 82.7% [10, 11].
The problem in parent-adolescent communication has been associate with an increase in a wide range of adolescent risk behaviors [8, 12,13,14,15,16]. Evidence showed that 29% of premarital sex was caused by improper parenting style [17]. Good parent-adolescent communication enables them to know their HIV status which would have an impact on HIV transmission [18]. Parental communication had an impact on the mental wellbeing of adolescents [19]. The other advantage of good parental communication was that it can delay early sexual initiation [20, 21].
Parent-young communication was associated with socio-demographic characteristics of young (age, sex, educational status) [9, 15, 22], parental characteristics (educational status and marital status) [5, 23, 24]. Improving sexual and reproductive health of young is one of the priorities of Sustainable Developmental Goals SDGs) [25]. In line with this, Ethiopia also develops strategies particularly for adolescents and youth which would apply to the end of 2020 [26]. Parent-young communication on sexual and reproductive health issues was a little bit investigated and studied in different parts of Ethiopia [27,28,29,30,31,32,33,34,35]. But, the finding of each study was highly varied and there is no single national representative estimate regarding it [11, 27,28,29, 36,37,38,39]. So, this study aimed to estimate the pooled prevalence of parent-young communication on sexual and reproductive health issues and its association with sex and perceptions of young people about its importance in Ethiopia, 2020.
Methods
Study design, search strategy and registration
The study was designed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-2009 Guidelines) [40]. It was conducted using published and unpublished articles and the articles were searched from different databases: (PubMed, Cochrane library, PsycINFO, CINAHL, Global Health, HINARI and Google scholar). All potential articles were accessed by using a combination of keywords/indices like; “prevalence”, “magnitude”, “parent adolescent”, “parent youth”, “parent young”, “communication”, “open communication”, “discussion”, “determinants”, “factors associated”, “associated factors”, “predictors”, “risk factors”, “sexual”, “sexuality”, “sexual issue”, “reproductive health” which were developed according to Medical Subject Headings (MeSH). All these key terms were searched by a combination of Boolean operators “AND” or “OR” as appropriate and the search was done by two authors independently (MY and BA). The protocol of this systematic review and meta-analysis was registered in the PROSPERO International prospective of systematic reviews with a specific registration number: CRD42020161252.
Study selection and eligibility criteria
Inclusion criteria
-
❖ Population: This systematic review included studies conducted among young and/or parents having young (aged 10 to 24 years) in Ethiopia.
-
❖ Exposure: Female young and young who had positive perception towards parent-young communication.
-
❖ Comparison: Male young and young who had negative perception towards parent-young communication.
-
❖ Outcome: Studies conducted parent-young communication as primary outcome.
-
❖ Study design: All observational studies were included
-
❖ Time frame: All studies irrespective of data collection and publication year until the end of November 1, 2020
-
❖ Publication: Either published in peer-reviewed journals or unpublished studies.
-
❖ Language: studies published only in English language were included in this systematic review and meta-analysis.
Exclusion criteria
-
❖ Studies in which the outcome did not clearly reported
-
❖ Studies in which the full texts were not available after 2 times authors request were excluded from systematic review and meta-analysis.
Variable measurements
Parent-young communication on sexual and reproductive health issues was measured in two ways. Thirteen articles used as having talked about at least one [11, 28, 30, 32, 34, 36, 38, 41,42,43,44,45,46] and the rest 16 articles were used at least two [10, 27, 29, 31, 33, 35, 37, 39, 47,48,49,50,51,52,53,54] of the following sexual and reproductive health related topics with their parents with in the past 6 months: a) body change during puberty, b) menstruation, c) abstinence, d) condom use and where to get condom, f) relationship with opposite sex, g) STI including HIV/AIDS, h) family planning, i) abortion, j) unplanned pregnancy and k) sexual organs.
Study quality appraisal and data extraction
Those articles identified in all databases were exported to Endnote X8 and duplicate files were excluded. The remaining articles and abstracts were independently screened by two groups (YD and BK) for inclusion in the full-text appraisal. It was assessed using Joanna Brigg’s Institute (JBI) critical appraisal checklist according to the study design of each article [55, 56]. Two independent authors (SW and AB) assessed the quality of the articles and the differences in the scales result was settled by taking the average result of both reviewers.
Data were extracted using Microsoft excel 2010 sheet and the sheet contained the following list of variables for the first objective: authors name followed by initials, year of study, year of publication, study setting, study design, sample size, response rate, quality score, sex of participants, region, study finding. For the second objective, in addition to the above mentioned, studies reported at least one of the above mentioned factors as predictors were identified and extracted. Two authors (MY and YW) extract the data for both objectives and any disagreements between the two authors during extractions were solved through discussion and consensus.
Data synthesis and statistical analysis
The data extracted in the Microsoft Excel sheet format was exported into STATA/SE 14 version statistical software for further analysis. The pooled effect of the point estimate of parent-young communication in Ethiopia was calculated by DerSimonian & Liard’s method of random effect model at P-value less than 0.05 [57]. Statistical significance for heterogeneity with I2 tests greater than 75% was taken as high heterogeneity and it was subjected to sub-group and sensitivity analysis. Finally, publication bias was assessed by using Egger’s weighted regression test method (p-value < 0.05) which was considered as statistically significant publication bias [58].
Results
Study selection
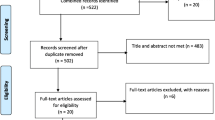
The review found a total of 780 articles. Sixty-four of them were removed due to duplication and 683 records also excluded after screening by title and abstract. The remaining 33 of them were screened for eligibility and appraised based on JBI checklist. Again 4 of them were excluded due to reason (outcome was not clearly reported or the authors couldn’t respond for full text request). A total of 29 full-text articles were included in systematic review and meta-analysis (Fig. 1).

PRISMA flow diagram of parent-young communication on sexual and reproductive health issues and its association with sex and perceptions of young people, a systematic review and meta-analysis, Ethiopia, 2020
Descriptive characteristics of included studies
All included articles were cross-sectional studies and the minimum and the maximum sample size was 262 and 2075 participants in a study conducted in Shambo and Nekemte town, Oromia respectively [43, 46]. A total of 16,721 young and/or parents had young were included and nearly half (48.28%) of the studies were from both preparatory and high school students [10, 30, 36, 38, 41, 42, 44, 45, 47,48,49,50,51,52] and six of them were community based [11, 28, 43, 46, 53, 54] (Table 1).
Prevalence of parent-young communication on sexual and reproductive health issues
Parent-young communication on sexual and reproductive health issues was ranged between 8.84 to 82.67% in unpooled estimate [10, 52]. The pooled prevalence of parent-young communication on sexual and reproductive health issues was 42.96% [95% CI: (36.91, 49.02)]. As it was illustrated in the figure, there was considerable heterogeneity (I2 = 98.6%, P value = 0.0001) among studies included in the analysis (Fig. 2). It was also 45.05% [95% CI: (34.97, 55.14)] and 41.27% [95% CI: (33.69, 48.85)] for those young who talked one and two sexual and reproductive health issues respectively. The sensitivity analysis indicated that there was no single influential estimate that could attributed to source of heterogeneity. The funnel plot of pooled prevalence was symmetrical (Fig. 3) and the Egger test revealed that there was no statistical evidence of publication bias (P = 0.112).

Forest plot of the pooled prevalence of parent-young communication on sexual and reproductive health issues, a systematic review and meta-analysis, Ethiopia, 2020

Funnel plot showing publication bias of parent-young communication on sexual and reproductive health issues and its association with sex and perceptions of young people, a systematic review and meta-analysis, Ethiopia, 2020
Subgroup analysis
Subgroup analysis was done by different parameters (region, study setting, study year, response rate and type of participants) to observe the possible sources of heterogeneity. Despite heterogeneity was not totally resolved in subgroup analysis, those studies conducted before 2011 had moderate heterogeneity (I2 = 61.8%, P value = 0.033) (Fig. 4). The highest and the lowest prevalence of parent-young communication were observed in Tigray and Benishangul Gumz respectively [52.82, 95% CI: (43.02, 62.61] and [28.88, 95% CI: (24.51, 33.26)]. Similarly, the prevalence of parent-young communication was significantly different among young [45.89, 95% CI: (40.76, 51.03)] and parents [24.56, 95% CI: (11.55, 37.57)].

Forest plot of subgroup analysis for prevalence of parent-young communication on sexual and reproductive health issues by study year using the random effect model, a systematic review and meta-analysis, Ethiopia, 2020
Factors associated with parent-young communication
The effect of perceptions of young people regarding parent-young communication on sexual and reproductive health issues was estimated by using seven articles. From those, only one of them was not significant [39] and the others were positively significant [31, 33, 35, 41, 47, 51]. The pooled odds of parent-young communication on sexual and reproductive health issues among young who had positive perception regarding parent-young communication was increased by 4 as compared to counterparts [AOR = 3.72, 95% CI: (2.87, 4.86)] (Fig. 5). The egger test showed that there was no statistical evidence of publication bias (P value = 0.334).

Forest plot of the pooled estimate of the effect of perceptions of young people on parent-young communication on sexual and reproductive health issues, a systematic review and meta-analysis, Ethiopia, 2020
The effect of sex on parent-young communication on sexual and reproductive health issues was estimated by using 11 articles. From those, only one of them was negatively significant [36], three of them were not significant [29, 37, 38] and the rest were positively significant [10, 27, 28, 35, 41, 47, 48]. Using the random effect model, the pooled odds of parent-young communication on sexual and reproductive health issue among females was 1.6 times high as compared to males [AOR = 1.62, 95% CI: (1.12, 2.34)] (I2 = 90.5%, P value = 0.000) (Fig. 6). The egger test shown that there was no statistical evidence of publication bias (P value = 0.073).

Forest plot of the pooled estimate of the effect of sex on parent-young communication on sexual and reproductive health issues, a systematic review and meta-analysis, Ethiopia, 2020
Discussion
The pooled prevalence of parent young communication on sexual and reproductive health issue in Ethiopia was 42.96% [95% CI: (36.91, 49.02)]. The pooled prevalence of parent-young communication was in line to a study conducted in Nigeria (46.7%) [6]. But, the result of this study was low as compared to a study conducted in Kenya (53%) [8] and Zambia (60%) [9]. Again the finding of this study was low as compared to a study in Bangladesh (65.6%) [5]. The possible explanation for this discrepancy may be due to socio-cultural difference related to parenting style [22]. In addition, traditional norms and religious beliefs of the countries may be another source of variation [24]. The highest and the lowest prevalence of parent young discussion were observed in Tigray and Benishangul Gumz respectively [52.82, 95% CI: (43.02, 62.61] and [28.88, 95% CI: (24.51, 33.26)]. The possible reason for this visible difference may be due to that Tigray region was relatively developed as compared to Benishangul Gumz. Moreover, the participants in Tigray region may be high possibility to have media exposure than that of Benishangul Gumz.
In addition, the highest prevalence of parent-young communication was observed in studies conducted among young as compared to studies conducted among parents. This may be due to the fact that parents had less exposure to education and information than young. Moreover, the parents might think it as a positive reinforcing factor for early sexual initiation.
The pooled odds of parent-young communication on sexual and reproductive health issues among young who had positive perception regarding parent-young communication were statistically high as compared to counterparts. The finding of this study was in agreement with a study conducted in Bangladesh [5]. It is also congruent with a study conducted in Myanmar [23]. The possible reason for this association may be their perception was highly affected by the culture what they were growing and sometimes they may also perceived as their parents have negative perception regarding parent-young communication [17].
The pooled odds of parent-young communication on sexual and reproductive health issues among females were high as compared to males. The finding was congruent to a study conducted in Nigeria [6]. The finding was also in agreement with a study conducted in Rwanda [15]. The possible reason for this association may be due to the fact that males were feeling ashamed and it is culturally unacceptable to talk about sexual matters. Even, they may wrongly perceived it as it would be interpreted as signs of sexual initiation [59]. Moreover, in the context of Ethiopia, females were wasting most of their times in the household which may increase the contact and possibilities of discussion than males.
Despite its strength, the study was not without limitation. The review was restricted to articles published in the English language and it may not be representative for articles published in other languages. Not only this, but also all the studies included in meta-analysis were cross-sectional and the pooled estimate may be influenced by study design.
Conclusions
The prevalence of parent-young communication on sexual and reproductive health issue in Ethiopia was low as compared to other literatures. Both positive perceptions of young people towards parent-young communication and female sex were significantly associated with parent-young communication on sexual and reproductive health issues. So, the government should focus on interventions that could change the perception of young on parent-young discussion. Interventions targeting male and young who had negative perception regarding parent-young communication should be the primary focus of the parents.
Availability of data and materials
All the data used and analyzed during this study are available from the corresponding author on reasonable request.
Abbreviations
- AIDS:
-
Acquired Immune Deficiency Syndrome
- HIV:
-
Human Immune Deficiency Virus
- JBI:
-
Joanna Brigg’s Institute
- WHO:
-
World Health Organization
References
World Health Organization. Engaging young people for health and sustainable development: strategic opportunities for the World Health Organization and partners. 2018.
Gupta MD. The Power of 1.8 Billion: Adolescents, Youth and the transformation of the future: United Nations Population Fund; 2014.
Kibangou E. Early sexual debut and human immunodeficiency virus infection in Central Africa; 2015.
Shrestha R, Karki P, Copenhaver M. Early sexual debut: a risk factor for STIs/HIV acquisition among a nationally representative sample of adults in Nepal. J Community Health. 2016;41(1):70–7.
Zakaria M, Xu J, Karim F, Cheng F. Reproductive health communication between mother and adolescent daughter in Bangladesh: a cross-sectional study. Reprod Health. 2019;16(1):114.
Abah VO. The Impact of Parent Adolescent Communication on Sexuality on Sexual Debut and Related Risk Behaviors among In School Adolescents in Benin City. J Dental Med Sci. 2018;17(4):06–14. www.iosrjournals.org.
Titiloye MA, Ajuwon AJ. Knowledge and quality of adolescents reproductive health communication between parents and their adolescents children in Ibadan, Nigeria. J Public Health Afr. 2017;8:688. https://doi.org/10.4081/jphia.2017.688.
Gathii N. The influence of parent -adolescent communication on sexual and reproductive behavior of adolescents: case study of Kibera slums; 2013.
Haakonde T, Chisumbe S, Chibwe M, Iwol K. An assessment of parents-adolescents communication on sexual and reproductive health matters between Evelyn hone college lecturers and their adolescent children. Lusaka, Zambia 2018:219–224.
Chane T, Cherie N. Parent–adolescent communication about sexual and reproductive health and associated factors among preparatory school students in Haiyk town, north East Ethiopia. Res Med Eng Sci. 2018;5(2):417–23.
Tegegne A, Ademasu E, Demewozu H. Parent to young communication on sexual and reproductive health and associated factors among parents living with young in Dera Woreda, north West Ethiopia 2018. J Community Med Health Educ. 2019;9(655):2.
Malcolm S, Huang S, Cordova D, Freitas D, Arzon M, Jimenez GL, et al. Predicting condom use attitudes, norms, and control beliefs in Hispanic problem behavior youth: the effects of family functioning and parent–adolescent communication about sex on condom use. Health Educ Behav. 2013;40(4):384–91.
Widman L, Choukas-Bradley S, Noar SM, Nesi J, Garrett K. Parent-adolescent sexual communication and adolescent safer sex behavior: a meta-analysis. JAMA Pediatr. 2016;170(1):52–61.
Rogers AA. Parent–adolescent sexual communication and adolescents’ sexual behaviors: a conceptual model and systematic review. Adolescent Research Review. 2017;2(4):293–313.
Bushaija E, Sunday F, Asingizwe D, Olayo R, Abong’o B. Factors that hinder parents from the communicating of sexual matters with adolescents in Rwanda. Rwanda J Health Sciences. 2013;2(2):13–9.
Maimunah S, Afiatin T, Helmi AF, editors. Parent-Adolescent Sexual Communication and Adolescent Sexual Behavior: A Meta-Analysis Review. 5th ASEAN Conference on Psychology, Counselling, and Humanities (ACPCH 2019); 2020: Atlantis Press.
Fajar NA, Etrawati F, Lionita W. Determinant of parents role in adolescent premarital sex behavior: an applicative model Determinan Peran orang Tua terhadap Perilaku Seks Pranikah Remaja: Sebuah model Aplikatif; 2018.
Balaji AB, Oraka E, Fasula AM, Jayne PE, Carry MG, Raiford JL. Association between parent–adolescent communication about sex-related topics and HIV testing, United States. 2006–2013. AIDS Care. 2017;29(3):344–9.
Walsh SD, Harel-Fisch Y, Fogel-Grinvald H. Parents, teachers and peer relations as predictors of risk behaviors and mental well-being among immigrant and Israeli born adolescents. Soc Sci Med. 2010;70(7):976–84.
Longmore MA, Eng AL, Giordano PC, Manning WD. Parenting and adolescents' sexual initiation. J Marriage Fam. 2009;71(4):969–82.
Nagamatsu M, Saito H, Sato T. Factors associated with gender differences in parent-adolescent relationships that delay first intercourse in Japan. J Sch Health. 2008;78(11):601–6.
Liu T, Fuller J, Hutton A, Grant J. Factors shaping parent–adolescent communication about sexuality in urban China. Sex Education. 2017;17(2):180–94.
Noe MTN, Saw YM, Soe PP, Khaing M, Saw TN, Hamajima N, et al. Barriers between mothers and their adolescent daughters with regards to sexual and reproductive health communication in Taunggyi township, Myanmar: what factors play important roles? PLoS One. 2018;13(12):e0208849.
Nundwe CS. Barriers to communication between parents and adolescents concerning sexual and reproductive health issues: a case study of Kinondoni municipality. Tanzania: Muhimbili University of Health and Allied Sciences; 2012.
GA U. Transforming our world: the 2030 Agenda for Sustainable Development. Division for Sustainable Development Goals: New York. 2015.
National Adolescent and Youth Health Strategy of Ethiopia. Federal Democratic Republic of Ethiopia, Ministry of Health. 2016.
Ayalew M, Mengistie B, Semahegn A. Adolescent-parent communication on sexual and reproductive health issues among high school students in Dire Dawa, Eastern Ethiopia: a cross sectional study. Reproductive Health. 2014;11(1):77.
Ayehu A, Kassaw T, Hailu G. Young people's parental discussion about sexual and reproductive health issues and its associated factors in Awabel woreda, Northwest Ethiopia. Reproductive Health. 2016;13(19):19.
Kinfe M. Getachew G/selassie.“assessment of communication on sexual and reproductive health issues among Gorro preparatory school students with their parents Gurage zone, southern Ethiopia, Ethiopia”. EC Gynaecology. 2018;7:95–103.
Kusheta S, Bancha B, Habtu Y, Helamo D, Yohannes S. Adolescent-parent communication on sexual and reproductive health issues and its factors among secondary and preparatory school students in Hadiya zone, southern Ethiopia: institution based cross sectional study. BMC Pediatr. 2019;19(1):9–11.
Mekie M, Taklual W, Melkie A, Addisu D. Parental communication on sexual and reproductive health issues and its associated factors among preparatory school students in Debre Tabor, Northcentral Ethiopia: institution based cross-sectional study. BMC Research Notes. 2019;12(1):598–6.
Melaku YA, Berhane Y, Kinsman J, Reda HL, Medicinska F, Institutionen för folkhälsa och klinisk m, et al. Sexual and reproductive health communication and awareness of contraceptive methods among secondary school female students, northern Ethiopia: a cross-sectional study. BMC Public Health. 2014;14(1):252.
Mekonen MT, Dagnew HA, Yimam TA, Yimam HN, Reta MA. Adolescent-parent communication on sexual and reproductive health issues and associated factors among high school students in Woldia town, Northeastern Ethiopia. Pan African Med J Article. 2018;31:35. doi: https://doi.org/10.11604/pamj.2018.31.35.13801.
Yowhanes Z, Berhe H, Hailu D. Assessment of Parent-Adolescent Communication about Sexual and Reproductive Health among High School Students in Mekelle Town, Northern Ethiopia. Global J Med Res. 2016;16(2).
Zewdu S. Assessment of Adolescent Parent Communication Concerning Sexual and Reproductive Health Issues among Ayer Tena Preparatory School Students [PhD Thesis]: Addis Ababa University; 2011.
Beyene D. Assessment of parent-adolescents communication on sexual and reproductive health matters and associated factors among secondary and preparatory schools students in ambo town. Ethiopia: Oromiya Region; 2015.
Fikre M, Betre M. Assessment of parent-adolescent communication on sexual and reproductive health matters in Hawasa town. Ethiopia: SNNPR; 2009.
Shewasinad S, Alelign Z, Yeshitla K, Bunga G, Negash S. Assessment of communication on sexual and reproductive health issues among Mizan secondary and preparatory school students with parents, Mizan town, Ethiopia, 2016. Am J Health Research. 2017;5(5):131–40.
Taddele M, Jara D, Hunie A. Level of parent adolescent communication on sexual and reproductive health issues and associated factors among debre markos preparatory school students, in debre markos town, east gojjam, zone, Ethiopia. Universal J Public Health. 2018;6(4):203–9. https://doi.org/10.13189/ujph.2018.060406.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews. 2015;4(1):1.
Feyisa M. Parent adolescent sexual and reproductive health communication and associated factors among secondary and preparatory school students in fiche town. North Shoa, Oromia Regional State, Ethiopia: Addis Ababa University; 2017.
Neme D, Dereje M. Adolescent Parent Communication Concerning Sexual and Reproductive Health Issues Among Sendafa High School and Preparatory Students. Age. 13(16):156.
Tesso DW, Fantahun MA, Enquselassie F. Parent-young people communication about sexual and reproductive health in E/Wollega zone, West Ethiopia: Implications for interventions. Reproductive Health. 2012;9(1):13.
Yohannes Z, Girma Y, Hussien S, Fekad B. Factors Associated with Parent-Adolescent Communication on Sexual and Reproductive Health Issues Among Secondary and Preparatory School Students in Mekelle City. North Ethiopia. 2015.
Yohannes Z, Tsegaye B. Barriers of parent-adolescent communication on sexual and reproductive health issues among secondary and preparatory school students in Yirgalem, town, South Ethiopia. Fam Med Med Sci Res. 2015;4(4):181.
Assebe T. Assessment of factors affecting parents in discussing reproductive health issue with their adolescent in Shambo town, Horo Guduru Wollega, Oromiya region, Ethiopia, May 2009: Addis Ababa University; 2009.
Fanta M, Lemma S, Gamo G, Meskele M. Factors associated with adolescent-parent communication of reproductive health issues among high school and preparatory students in Boditi town, southern Ethiopia: a cross-sectional study. Patient Intelligence. 2016;8:57–70.
Habte NM, Melku AT, Alemayehu MT. Parent-adolescent communication on sexual and reproductive health matters and associated factors among secondary and preparatory school students in robe town, bale zone, Southeast Ethiopia, 2017. J Public Health Int. 2019;1(4):1.
Masresha SA, Alen GD, Aberra IA, Dender DK, Mamo ZA, Girma AD, et al. Parent-Adolescent Communication about Sexual and Reproductive Health and Its Association with Gender and Pre-Marital Sex Among Secondary and Preparatory School Students in Woldia Town, North East Ethiopia, 2019. 2019.
Mengistu T. Assessment of parent-adolescent communication and associated factors on sexual and reproductive health issues at Fagita Lokoma District in Awi Zone, Northwest Ethiopia [PhD Thesis]. 2012.
Shiferaw K, Getahun F, Asres G. Assessment of adolescents' communication on sexual and reproductive health matters with parents and associated factors among secondary and preparatory schools' students in Debremarkos town, North West Ethiopia. Reproductive Health. 2014;11(1):2.
Yesus DG, Fantahun M. Assessing communication on sexual and reproductive health issues among high school students with their parents, Bullen Woreda, Benishangul Gumuz Region, North West Ethiopia. Ethiopian J Health Development. 2010;24(2):89–95.
Yadeta TA, Bedane HK, Tura AK. Factors affecting parent-adolescent discussion on reproductive health issues in Harar, Eastern Ethiopia: a crosssectional study. J Environ Public Health. 2014;2014:102579. https://doi.org/10.1155/2014/102579.
Bekele D, Deksisa A, Abera W, Megersa G. Parent-adolescent communication on sexual and reproductive health issues and affecting factors in Asella town, Arsi zone, Ethiopia; a community based cross-sectional study; 2020.
Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: systematic reviews of etiology and risk. Joanna Briggs Institute Reviewer's Manual The Joanna Briggs Institute 2017:2019–2005.
Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evidence-Based Healthcare. 2015;13(3):147–53.
DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemporary Clinical Trials. 2015;45:139–45.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Bmj. 1997;315(7109):629–34.
Motsomi K, Makanjee C, Basera T, Nyasulu P. Factors affecting effective communication about sexual and reproductive health issues between parents and adolescents in zandspruit informal settlement, Johannesburg, South Africa. Pan Afr Med J. 2016;25:120. https://doi.org/10.11604/pamj.2016.25.120.9208.
Acknowledgments
Our special thanks go to all public health staff for their help when needed.
Funding
No fund was received.
Author information
Authors and Affiliations
Contributions
MY, BA and BK: Analyzed the data and wrote the result, YD and MA: Drafted the manuscript, SW, AB and YW: Edited and revised the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All the authors declared that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yalew, M., Adane, B., Kefale, B. et al. Parent-young communication on sexual and reproductive health issues and its association with sex and perceptions of young people in Ethiopia, 2020: a systematic review and meta-analysis. Arch Public Health 78, 133 (2020). https://doi.org/10.1186/s13690-020-00515-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-020-00515-x