
Abstract
Background
Accurate evaluation of valvular pathology is crucial in the timing of surgical intervention. Whilst transthoracic echocardiography is widely available and routinely used in the assessment of valvular heart disease, it is bound by several limitations. Although cardiovascular magnetic resonance (CMR) imaging can overcome many of the challenges encountered by echocardiography, it also has a number of limitations.
Main text
4D Flow CMR is a novel technique, which allows time-resolved, 3-dimensional imaging. It enables visualisation and direct quantification of flow and peak velocities of all valves simultaneously in one simple acquisition, without any geometric assumptions. It also has the unique ability to measure advanced haemodynamic parameters such as turbulent kinetic energy, viscous energy loss rate and wall shear stress, which may add further diagnostic and prognostic information. Although 4D Flow CMR acquisition can take 5–10 min, emerging acceleration techniques can significantly reduce scan times, making 4D Flow CMR applicable in contemporary clinical practice.
Conclusion
4D Flow CMR is an emerging CMR technique, which has the potential to become the new reference-standard method for the evaluation of valvular lesions. In this review, we describe the clinical applications, advantages and disadvantages of 4D Flow CMR in the assessment of valvular heart disease.
Similar content being viewed by others


Background
Transthoracic echocardiography (TTE) is the first line imaging modality for assessing patients with valvular heart disease (VHD) [1,2,3]. Although it is easily accessible, safe and inexpensive [4,5,6], it may be limited in cases of poor acoustic windows secondary to large body habitus [7] or in the presence of eccentric [8] or multiple regurgitant jets [9]. TTE assessment of heart valve function can also be challenging due to limited reproducibility [9], operator-dependence [10] and inaccuracy in quantification of regurgitant lesions in certain cases [11]. Although transoesophageal echocardiography overcomes some of these limitations and can be performed in patients with suboptimal quality TTE images [1], it is a moderately invasive procedure, can lead to potentially serious complications, [12] and increased patient discomfort.
Phase contrast magnetic resonance (PCMR) imaging offers several advantages over TTE and can clarify the severity and mechanism of VHD lesions in selected cases [7, 8, 13]. It enables detailed assessment of valvular flow and function with no geometric assumptions, and can therefore accurately assess lesions with multiple regurgitant jets or eccentric jets [8, 13]. Furthermore, assessment of left ventricular (LV) function and remodelling by cardiovascular magnetic resonance (CMR) imaging has been shown to be highly accurate and reproducible [14]. CMR is also the reference standard for evaluation of right ventricular (RV) morphology and function, and therefore can precisely assess the impact of right-sided valvular lesions on the ventricle [15]. However, despite all of its advantages, PCMR does not allow for accurate direct jet quantification in the atrio-ventricular valves as it does not account for valve plane motion during the cardiac cycle [13]. Also, flow quantification can be significantly affected by phase-offset errors [7, 16]. Furthermore, errors introduced in ventricular stroke volume calculations can lead to inaccurate quantification of atrio-ventricular regurgitant lesions [6].
Four-dimensional (4D) Flow CMR is a relatively novel CMR technique, which offers time-resolved 3-dimensional (3D) imaging and allows accurate and precise assessment of VHD. It overcomes a lot of the limitations present in TTE and PCMR. A typical 4D Flow whole heart acquisition has a temporal resolution of 30–40 ms, spatial resolution of < 3 mm × 3 mm × 3 mm and takes 5–10 min [16]. Available acceleration techniques, such as kt broad linear speed up technique (kt BLAST) with a 32-channel coil array allow shorter scan times, and make 4D Flow CMR more clinically applicable [17]. New acceleration techniques such as prospective undersampling in multiple dimensions (PROUD) [18], k-adaptive-t autocalibrating reconstruction for cartesian sampling (kat-ARC) [19] and SmartSpeed (compressed sensitivity encoding featuring artificial intelligence algorithm) [20] are emerging and hold promise for an even faster acquisition. Recommended sequence parameters for 4D Flow CMR imaging are based on the delicate balance between the ideal parameters to provide high quality data and what is clinically feasible in terms of, mainly scan time. The typical sequence parameters are as follows: field of view, which is sufficient to cover the region of interest; k-space segmentation factor of 2, which reduces scan time, but also decreases accuracy; retrospective electrocardiogram (ECG) gating, which allows coverage of the entire cardiac cycle, but requires complex reconstruction—this is preferred to prospective gating, where the data from end-diastole are not acquired, thus impairing accuracy of mitral valve and tricuspid valve forward flow quantification [21]; the use of respiratory navigator; elliptical k-space to reduce scan time; flip angle equivalent to at least the Ernst angle to provide optimal signal-to-noise ratio (SNR), but with negative effect on contrast; the use of acceleration techniques, if available, to reduce scan time, although this benefit is offset by reduction in signal-to-noise ratio; single velocity-encoding (VENC) set to 10% above the expected maximum velocity, which decreases scan time, but also negatively affects the velocity-to-noise ratio; and the application of phase-unwrapping algorithms as well as eddy current and Maxwell correction algorithms to improve accuracy [16].
When compared to standard imaging modalities, such as TTE and PCMR, 4D Flow CMR offers a number of advantages. It enables direct jet visualisation and quantification of regurgitant lesions, especially when complicated by eccentric or multiple jets [22,23,24]. This is possible as it can be visualised in a 3D dataset. When performed as a whole heart acquisition, it allows the evaluation of all four cardiac valves simultaneously within a single acquisition [25]. Simultaneous quantification of flow across all 4 valves in 4D Flow CMR provides a means of internal validation of flow measurements [16]. Studies which evaluated all four valves, showed strong agreement between net flow volumes across all valves [25], with small inter-valvular variation [26]. Consistency across modalities is significantly improved when retrospective valve tracking is used [27]. Furthermore, as all the measurements are obtained from the same acquisition, the impact of variability related to changes in heart rate, on consistency of measurements will be reduced [28]. Although blurring can occur as a result of irregular heart rate [29], recent study showed that measurements of flow volumes remain accurate and feasible even in the presence of atrial fibrillation [30]. Moreover, peak velocity measurements in stenotic lesions may be more accurate and precise than with PCMR [31]. Several novel markers, such as wall shear stress can also be measured, which may be helpful in the assessment of patients with bicuspid aortic valve (BAV) disease amongst other pathologies [32,33,34,35]. Finally, the acquisition itself requires only very simple planning [29].
There are, however, a number of challenges encountered in 4D Flow CMR. The main drawbacks of this technique include limited temporal and spatial resolution, long scan time [16] and the requirement for complex post-processing, which requires specialised knowledge and is time-consuming. Also, 4D Flow CMR imaging requires supplementary cine images, which serve as an anatomical framework for the phase images. This can potentially lead to misalignment between the anatomical reference and the phase images due to heart rate variability and patient movement during the scan. Although misalignment can often be corrected during post-processing, it adds an extra step to the analysis [28].
As with PCMR, appropriate VENC needs to be chosen and should be set to a value that is marginally higher (about 10%) than expected peak velocity in the region of interest. Inappropriately low VENC setting can lead to aliasing, whereas the higher the VENC, the lower the velocity-to-noise ratio. It is therefore advisable to apply a phase-unwrapping algorithm, especially in cases where it might be difficult to estimate the maximum velocity [16]. Mixed VHD can pose a further challenge to VENC setting, as a value appropriate for low velocities will not be optimal for a high velocity setting. Although this can be overcome by two separate acquisitions with different VENC settings, it is very time consuming [36]. Hence, clinically applicable dual- and multi-VENC sequences are emerging, which will be helpful when stenotic and regurgitant lesions co-exist [16, 36, 37].
Although peak velocity assessment in stenotic lesions may be complicated by signal dephasing secondary to turbulent flow and could potentially lead to imprecise measurements, the visualisation and identification of the highest velocity area may also allow more accurate assessment of velocity [38].
With regard to regurgitant lesions, visualisation of areas of turbulence and signal dephasing can help with accurate quantification, as these areas can be avoided [9]. Regurgitant lesions are also frequently complicated by multiple and/or eccentric jets, especially in the case of mitral valve [39]. Although direct jet quantification can be performed in these cases, it may be challenging [40] and time-consuming [41]. The indirect method can be advantageous in these cases and has been shown to have a better intra- and inter-technique reliability [42].
Furthermore, as with PCMR, phase offset errors may occur and must be corrected. Artefacts occurring due to Maxwell terms and non-linearity of the gradient field tend to be optimised easily, however, correction for eddy currents has to be performed manually and incorporated into data analysis [43]. The advantages and disadvantages of the various imaging modalities used in VHD assessment are shown in Table 1.
A number of cardiovascular 4D Flow CMR reviews were published in recent years. These focused on different aspects of 4D Flow CMR, such as kinetic energy assessment of LV blood flow [48], technical aspects of 4D Flow acquisition and application of 4D Flow CMR in various cardiac and vascular pathologies [49, 50], congenital heart disease applications [51] as well as structural heart disease [52] and peak velocity assessment [53]. Other reviews evaluated 4D Flow CMR in mitral valve disease [23, 54], left-sided VHD [22] and in various cardiovascular pathologies with a limited focus on VHD [32, 38, 55, 56]. Although a recent systematic review of 4D Flow CMR in the heart and great vessels evaluated current evidence for 4D Flow CMR in VHD in great detail, it did not provide illustrative examples of the different pathologies [27]. To our knowledge, there is no clinically focused 4D Flow CMR review, which is solely dedicated to acquired valvular heart disease.
As acquired VHD was not the emphasis of the majority of the above publications, the purpose of this review is to provide an educational overview of the rationale for 4D Flow CMR, its utility in the assessment of VHD in contemporary clinical practice and to provide illustrative examples of 4D Flow CMR evaluation of common valvular pathologies. Our aim was to provide a clinically focused and illustrative summary of 4D Flow CMR applications in VHD, in a manner that is approachable to both, a beginner 4D Flow CMR imager and an advanced specialist looking for a comprehensive summary of data.
Rationale and clinical applications of 4D Flow CMR in valve-specific pathologies
Mitral regurgitation
Mitral regurgitation and aortic stenosis (AS) are the most common valvular pathologies in the developed world. As the population is ageing significantly, the prevalence of VHD is expected to increase [57]. Mitral regurgitation accounts for almost 25% of VHD cases in contemporary practice and is the second most common pathology in Europe [58]. Furthermore, untreated severe mitral regurgitation is associated with a high burden of morbidity and mortality [59]. Current guidelines recommend surgery in symptomatic patients with severe chronic primary mitral regurgitation and those who are asymptomatic, but have evidence of LV or left atrial (LA) remodelling, such as impaired LV ejection fraction (LVEF) ≤ 60%, LV end-systolic diameter ≥ 45 mm, new-onset atrial fibrillation or pulmonary artery systolic pressures > 50 mmHg. In secondary mitral regurgitation, surgery is recommended in those with LVEF > 30% undergoing coronary artery bypass grafting, those with LVEF < 30%, but with viable myocardium and an option for revascularisation, and those who are considered at low surgical risk and failed a trial of optimal medical therapy [1]. These guidelines highlight the importance of accurate assessment of mitral regurgitation severity and LV cavity size and function, to guide surgical therapy decisions.
Quantification of mitral regurgitation, and therefore the indication for surgery or percutaneous intervention relies on TTE measurements in the majority of patients [1, 3]. In selected cases, however, further investigation, including the use of CMR may be indicated [3, 40, 60, 61]. CMR studies showed that PCMR reclassified a proportion of patients with mitral regurgitation into a different severity category, which in turn showed better association with prognosis. Uretsky et al. in 2015 demonstrated discordance between mitral regurgitation quantification by PCMR and TTE and showed that CMR had a superior correlation with post-operative LV remodelling [62]. The prognostic advantage of CMR was confirmed in several other studies [63,64,65]. However, studies have reported different thresholds for classifying ‘severe’ mitral regurgitation. A study by Myerson et al., showed that regurgitant volume (RVol) of more than 55 ml and regurgitant fraction (RF) of more than 40% was associated with adverse clinical outcomes [63], whereas a study by Aplin et al. proposed lower threshold values [66].
The above studies utilised indirect techniques for quantification of RVol and RF. This was performed by subtracting aortic forward flow volume (obtained from through-plane velocity mapping) from LV stroke volume (SV) derived from cine images. This decreased errors that could occur as a result of an eccentric jet, multiple jets or flow turbulence leading to signal void [6]. Although this standard PCMR assessment of mitral regurgitation is robust, it requires 2 types of acquisition and its accuracy may be limited by errors introduced in the process of SV calculation [9]. Furthermore, different centres may use different methods of LV segmentation including or excluding LV outflow tract (LVOT) [67] and/or papillary muscles [68], which can lead to discrepancy in mitral regurgitation quantification. In the absence of tricuspid regurgitation (TR), it is also possible to quantify mitral regurgitation by subtracting RV SV from LV SV [6], although this is less commonly used. Direct assessment of the regurgitant flow by PCMR is not typically performed in clinical practice as it is inaccurate due to through-plane motion of the valve plane during systole, which can lead to significant quantitation errors [68]. This is further challenged by the mitral valve’s complex anatomy [22]. Similarly to TTE, in the presence of eccentric jets, quantitation of mitral regurgitation by the direct approach may be imprecise due to signal void [9].
4D Flow CMR overcomes a lot of these limitations and offers several advantages in the assessment of mitral regurgitation [9, 54]. A summary of the main studies that evaluated 4D Flow CMR in the setting of mitral regurgitation and other valvular pathologies is presented in Table 2.
4D Flow CMR data are mostly analysed via retrospective valve tracking (RVT). RVT can be performed manually or by an automated process. In the case of the mitral valve, manual RVT is performed by first reformatting the mitral valve plane using the 4-chamber view and vertical long axis (VLA) of the LV. Manual placement of a line across the annulus in all the phases in the 4-chamber view marks the valve plane. This is cross-checked with the 2-chamber LV view to ensure correct positioning. This is subsequently performed manually in each phase. Once the valve is correctly tracked, a phase-contrast, valvular reformatted plane is created [69]. A study by Roes et al. showed good intra- and inter-observer reproducibility for this technique [25]. Automated valve tracking (Fig. 1) can be performed much more rapidly, and also with excellent intra- and inter-observer reproducibility [70]. Regurgitant flow can additionally be analysed by reformatting a plane, which is located above the annulus and is perpendicular to the regurgitant jet [26, 54]. Although most extensively studied in the setting of atrio-ventricular valves, retrospective valve tracking can also be applied to evaluation of semilunar valves. Recent studies showed, that aortic and pulmonary valve net forward flow and regurgitant flow can be directly quantified by RVT [26, 70]. Moreover, evaluation of valvular blood flow by automated RVT was shown to be reproducible and accurate for all valves, irrespective of scanner type and protocol [26].

4D Flow CMR visualisation and quantification of valvular flow by retrospective valve tracking. Step 1. Identification of valve plane from cines acquired in 2 orthogonal planes. Step 2. Valve plane is tracked in all phases in the first view and cross-checked with the second view. Arrow allows confirmation of flow in the correct direction. Step 3. Visualisation of flow enables accurate quantification of flow in phase-contrast images
Different studies have explored different methods of mitral regurgitant volume quantification by 4D Flow CMR. The main techniques included the indirect method (mitral regurgitant volume = 4D Flow CMR mitral inflow volume − 4D Flow CMR aortic outflow volume [Mitral RegurgitationMVAV], direct method, which quantified mitral regurgitation directly from 4D Flow phase contrast images and the 4D-CMR PISA method. These techniques are described below:
-
1.
4D flow CMR indirect method (MRMVAV)
A study by Fidock et al., showed that mitral regurgitatant volume assessed by the 4D Flow CMR derived aortic outflow-mitral inflow calculation, correlated well with standard PCMR in primary mitral regurgitation, secondary mitral regurgitation and even in patients with mitral valve replacement (MVR); and had the highest level of concordance with the standard PCMR measurements [54]. Another study of 54 patients with mitral regurgitation secondary to mitral valve prolapse (MVP), compared RVol and RF by 4D Flow CMR direct jet quantification and indirectly by 4D Flow derived difference in aortic SV and mitral inflow. The direct jet interrogation technique was shown to have a lower inter- and intra-technique consistency than the 4D Flow CMR indirect method. The indirect method agreed well with PCMR, whereas the direct technique yielded much lower regurgitant volumes. This was felt to be secondary to the physiology of mitral regurgitant jets, which tend to be multiple and eccentric in nature [42].
Although direct quantification at jet level can be reliable and accurate, even in the presence of multiple and eccentric regurgitant jets [41], the indirect method offers an advantage, especially in cases of very complex regurgitant jets, where the direct jet method can be challenging to perform and labour intensive [40, 54]. An example of 4D Flow CMR indirect assessment of moderate mitral regurgitation is shown in Fig. 2.
-
2.
Direct mitral regurgitation quantification

4D Flow CMR assessment of mitral regurgitation. a Shows four-dimensional mitral regurgitation flow streamline. b Demonstrates mitral forward flow visualised by 4D Flow CMR and c quantification of mitral forward flow by phase-contrast image obtained from 4D Flow CMR. d Shows aortic forward flow and e quantification of aortic forward flow by phase-contrast image obtained by 4D Flow CMR
An early study by Roes et al. showed that net flow through all valves can be assessed accurately with RVT and demonstrated good intra- and inter-observer consistency for regurgitant fraction in patients with mitral regurgitation [25]. A more recent study by Kamphuis et al. compared net forward flow and regurgitant fraction by automated RVT versus manual valve tracking, and demonstrated that automated RVT can be performed much more rapidly than manual valve tracking, but also with high intra- and inter-observer reproducibility for RF [70].
A small study of patients with ischaemic heart disease assessing LV diastolic parameters, found significantly lower transmitral flow rates and higher mitral valve RF when compared to PCMR [71]. Similarly, a study of healthy subjects and patients with mitral regurgitation showed that in healthy subjects, mitral valve flow was overestimated by 15% when assessed by PCMR [69]. However, when compared to TTE, the results were somewhat variable. Brandst et al. found an excellent correlation between 4D Flow CMR and TTE versus PCMR and TTE [71], whereas a study by Marsan et al. found that 2-dimensional (2D) TTE significantly underestimated mitral RVol in patients with functional mitral regurgitation as compared to 4D Flow CMR [72]. All studies mentioned so far mainly used RVT at the valve level to quantify mitral regurgitation.
Feneis et al. utilised direct jet analysis as well as the indirect method in the assessment of 21 patients with mitral regurgitation and/or TR and compared the results to conventional CMR. Direct jet assessment involved examination of the regurgitant flow at various anatomical locations, beginning at the valve plane and then with at least 5 mm intervals. Areas of signal dephasing and aliasing velocity were avoided. The authors showed, that there was a good correlation between the measurements for those 2 modalities, for both, the direct and the indirect method. The intraobserver and interobserver reproducibility also proved very good to excellent for the direct jet approach [9].
Direct jet interrogation was also used in a recent study by Fidock et al. of 35 patients with primary mitral regurgitation, secondary mitral regurgitation and MVR. Fidock et al. found that in cases of primary mitral regurgitation, direct jet interrogation overestimated mitral regurgitant volumes; this was not the case for secondary mitral regurgitation or MVR patients. The authors proposed that the inconsistency in delineating the analysis plane was most likely responsible for this finding. The concordance of results in secondary mitral regurgitation was most likely related to the central regurgitant jet and the particular cohort of patients in this study, as most patients with secondary mitral regurgitation had only a mild degree of regurgitation [54].
A recent study by Blanken et al. quantified mitral regurgitation by semi-automated flow tracking (SFT) and compared it to semi-automated valve tracking. In this retrospective study of 30 patients, the authors showed that flow tracking allowed superior assessment of mitral regurgitation, especially in cases of severe mitral regurgitation. This study showed that RVol assessed by flow tracking was higher than the volume quantified by valve tracking and it correlated better with the RVol assessed by the standard method (LV SV—aortic outflow). Mitral regurgitation volume was underestimated by the valve tracking technique in cases of severe mitral regurgitation. The interobserver reproducibility was superior for SFT versus semi-automated valve tracking. The authors proposed that the superiority of flow tracking may be related to the enhanced precision of quantification of flow by relocating the analysis plane above the annulus and thus avoiding areas of turbulence and dephasing; and improved differentiation of the mitral regurgitant jet and aortic forward flow. The authors noted, however, that there were several limitations, which may have been responsible for the findings, including different aetiologies of mitral regurgitation in the different valve severity groups [73].
-
3.
PISA method
Although this is not an actual 4D Flow method per se, Gorodisky et al. showed that CMR 4D-proximal isovelocity surface area (PISA) is feasible as a surrogate marker of mitral regurgitant volume quantification. In this method, 3D flow vectors are obtained from each 3 mm slice between the mitral valve annulus and the LV apex. Although the analysis is performed by automated software, the appropriate slices and time frames need to be chosen manually. CMR 4D-PISA excludes geometric assumptions that are invariably made by echocardiography with this method. When compared to TTE-PISA, the CMR-PISA was smaller. TTE-PISA frequently overestimates flow, as it is obtained at a single time-point and does not take into account variation of flow during systole. The shape of CMR-PISA was also noted to be a hemi-ellipsoid in contrast to the hemisphere on which the TTE-PISA assumptions are based. The authors suggested, that flow magnitude could be measured accurately, as 3D velocity encoding allowed for the true flow to be measured in each voxel, diminishing the errors caused by the angle between the flow direction and the imaging plane. However, one disadvantage of CMR-PISA method is the possibility of inaccurate localisation of the vena contracta, which can occur in some cases [74]. Of note, the accuracy of flow assessment may be influenced by the sequence used. A recent study showed, that accelerated echo-planar imaging sequence may lead to errors in flow and velocity measurements in certain cases [75].
Finally, novel markers such kinetic energy (KE) mapping by 4D Flow CMR can also be utilised to aid the assessment of mitral regurgitation [21]. One study showed that peak KE levels in the late diastolic period did not decline after mitral valve surgery, suggesting persistence of pathological blood flow after an intervention [76].
As 4D Flow CMR offers a lot of advantages in quantification of mitral regurgitation, it may help to correlate long-term outcomes of patients with significant regurgitation according to different thresholds of severity, and clarify what RVol and RF are associated with adverse LV remodelling and may benefit from earlier surgical treatment [9]. While there are advantages and disadvantages associated with all the aforementioned techniques, the indirect method (MRMVAV) has been shown to be most accurate and reproducible.
Mitral stenosis
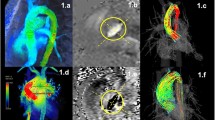
Although there are no studies of 4D Flow CMR in mitral stenosis, we have noted in our practice that mitral stenosis severity assessment by 4D Flow CMR-derived mean pressure drop correlates well with invasive measurement and mitral valve planimetry by CMR [77]. Mitral valve planimetry by TTE is the reference-standard in the assessment of mitral stenosis severity [1] and a good correlation between mitral valve planimetry by CMR and TTE has been previously shown [78]. An example of 4D Flow CMR and invasive assessment of moderate mitral stenosis is shown in Fig. 3.

Invasive and 4D Flow CMR assessment of moderate mitral stenosis. a Demonstrates invasive assessment of mitral stenosis with simultaneous recording of pulmonary artery wedge pressure and left ventricular pressure. The mean pressure gradient by this method was 6 mmHg. b–d CMR left ventricular outflow tract (LVOT) view, 4-chamber view and vertical long axis view, demonstrating reduced opening and thickening of the mitral valve leaflets and left atrial dilatation. e demonstrates quantification of peak velocity in the red areas of peak velocity zone on f–h. f–h In-plane velocities are superimposed on the above images, demonstrating increased forward flow velocity through the mitral valve
Aortic regurgitation
Evaluation of aortic regurgitation (AR) is primarily performed by TTE, and additionally with transesophageal echocardiography (TEE) and CMR in selected cases. TTE enables quantification of the severity of AR and its effect on LV cavity size and function [79], with indications for surgical timing in AR based on patient symptoms plus these aforementioned parameters [3]. Accurate assessment of regurgitation severity is crucial to allow optimal timing of intervention before irreversible LV remodelling occurs. As discussed, CMR provides the reference-standard evaluation of LV volume and function [14], with studies also showing that aortic RVol quantification by CMR correlates better with clinical outcomes than volumetric TTE measurements [80], and also has better prognostication than CMR assessment of LV volumes alone [81].
Assessment of AR by PCMR requires through-plane velocity encoded images. Although it is recommended to plan these images in a plane located 5 mm above the valve [82] and perpendicular to the vessel [83], in clinical practice this is frequently adjusted, as presence of turbulence and vortex formation secondary to eccentric jets may lead to inaccurate quantification of flow at this level and thus images are acquired at a level where flow appears more laminal. Care needs to be taken not to place the analysis plane too distally in the aorta, as this could lead to underestimation of regurgitation [84].
There are a number of advantages of 4D Flow CMR in the setting of AR when compared to PCMR. Functional and flow data are obtained from a single, free-breathing acquisition [85]. Furthermore, the annulus can be tracked accurately during the entire cardiac cycle [86].
In dilated aorta, we routinely see circular flow which makes it very challenging to quantify true forward flow through the vessel. In these challenging cases, 4D Flow allows to identify a plane with the most laminar flow in the ascending aorta to quantify forward flow. Therefore, 4D Flow CMR could potentially improve the accuracy of quantification of flow in the presence of a dilated aorta [79].
It is usually recommended, however to still cautiously segment the flow once a reformatted phase contrast plane is generated using the 4D Flow dataset.
A number of studies evaluated the feasibility of 4D Flow CMR in the assessment of AR (Table 2). A study by Ewe et al. of 32 patients compared RVol obtained from 2 and 3D TTE with 4D Flow CMR. This study demonstrated good correlation and agreement between AR severity assessed by 3D TTE and 4D Flow CMR; 2D TTE was less reliable. The correlation remained strong even in the presence of eccentric jets [86]. Another study of 54 patients compared 4D Flow CMR values against TTE. The concordance of these 2 methods was good, and more importantly 4D Flow CMR showed 100% sensitivity and 98% specificity for detection of more than mild AR [85]. A recent study by Alvarez et al. published in 2020 directly compared AR severity quantification by 4D Flow CMR versus PCMR. It evaluated 34 patients with AR RF of at least 5% as assessed by PCMR. The authors found an excellent agreement between the two techniques in terms of forward flow, regurgitant flow and RF [79]. An example of TTE and 4D Flow CMR assessment of moderate AR is shown in Fig. 4.

TTE and 4D Flow CMR assessment of moderate aortic regurgitation. a 4-chamber colour Doppler transthoracic echo (TTE) demonstrating aortic regurgitation jet and b TTE continuous wave Doppler demonstrating pressure half time consistent with moderate aortic regurgitation. c is a four-dimensional flow streamline visualisation of aortic regurgitation in left ventricular diastole. d is pathline visualization of flow reversal in the early diastole in the descending aorta. e is a reformatted c at aortic valve level flow quantification. f is the reformatted plane at the descending aorta level flow quantification
Aortic stenosis
Aortic stenosis (AS) is an increasingly common valvular pathology in the developed world [1]. Similar to other valvular lesions, the indications for intervention incorporate symptoms as well as timely and accurate assessment of AS severity [3]. Although TTE is the first-line investigation in most patients, PCMR provides a detailed and non-invasive option in challenging cases, where the severity of AS remains unclear. For accurate assessment of peak velocity, it is crucial to perform the through-plane velocity encoding by positioning the imaging plane parallel to the aortic valve and in a plane that corresponds to the highest velocity, characterised by turbulence in long-axis aortic valve cine views [82]. Appropriate VENC also needs to be chosen to avoid errors in peak velocity measurements [83]. Additionally, CMR can precisely assess LV function [6] and detect the presence and extent of fibrosis [46, 87, 88].
4D Flow CMR provides not only additional information related to valve severity and its impact on the LV, but it allows evaluation of consequences of pathological flow through the valve on the ascending aorta [22, 89]. It also has the potential to accurately assess peak velocities, even in the presence of multiple or eccentric jets [21]. Studies which evaluated 4D Flow CMR in AS are summarised in Table 2.
A study published by Garcia et al. proposed the use of 4D Flow jet shear layer detection method for measurement of the effective orifice area (EOA) in AS. This was validated against results based on the continuity equation method with values obtained from PCMR. 4D Flow CMR offered the advantage of 3D projection of the vena contracta, and thus allowed a more accurate localisation [90]. A recent study by Archer et al. assessed 18 patients with severe AS with TTE and 4D Flow CMR pre- and post-intervention. Patients undergoing transcatheter aortic valve replacement (TAVR) also underwent invasive pressure measurements. The authors showed that there was a good correlation between the invasive peak pressure gradient and the 4D Flow derived gradient. This study also demonstrated the prognostic advantage of 4D Flow derived pressure gradient versus TTE as shown by LV remodelling after the intervention [91].
As 4D-flow acquisitions can be time-consuming, several alternative k-space acquisition methods have been studied to optimise scan time. An in-vitro and in-vivo study of spiral k-space readout in patients with AS demonstrated shortening of echo time (TE) and the overall scan time. Peak velocity acquired with a spiral readout also correlated better with TTE Doppler measurements, than in the standard Cartesian acquisition [92]. A recent study by Callahan et al. evaluated dual VENC acquisition with a spiral readout. The authors showed that the spiral readout resulted in a reduction of flow-related artefacts due to lower TE, while dual VENC acquisition allowed better velocity resolution and reduction of noise [37]. An example of 4D Flow CMR assessment of severe AS is shown in Fig. 5.

4D Flow CMR assessment of severe aortic stenosis. a is a sagittal LVOT view and b coronal LVOT view demonstrating restrictive aortic valve opening with dephasing artefact demonstrating higher velocities through a narrow orifice. c and d further demonstrate increased velocity by superimposing in-plane velocity overlay onto the sagittal and coronal LVOT view. e shows four-dimensional flow streamline tracing through the aortic valve. f is a reformatted phase-contrast plane through the aortic valve demonstrating quantification of aortic valve forward flow and peak velocity. g is a zoomed in images of e demonstrating where the peak velocity through the aortic valve is (red ball). h Shows streamline visualisation of aortic regurgitation into the outflow tract
A novel marker that may be evaluated by 4D Flow imaging is turbulent kinetic energy (TKE). Turbulent blood flow in the presence of valvular lesions, such as AS, leads to energy loss by heat release, which can be quantified by TKE [21]. A small study of 4 healthy subjects and 14 AS patients, showed that there was a good agreement between the peak total TKE in the ascending aorta and pressure loss index based on standard assessment. Patients with AS also demonstrated much larger TKE in the ascending aorta as compared to healthy controls [93]. At present, TKE is only available as a research tool.
Low-flow low-gradient AS frequently poses a diagnostic challenge in clinical practice. Whereas there is a considerable amount of data supporting the use of 4D Flow CMR in the setting of high-gradient AS, data regarding 4D Flow CMR in the setting of low-flow low-gradient AS are scarce. Comprehensive assessment of advanced markers such as turbulent kinetic energy may be helpful in this cohort [94]. One study suggested that 4D Flow CMR-based turbulence production method of pressure drop assessment may be particularly useful in quantifying severity in low flow condition, such as paradoxical low-flow low-gradient AS, as it does not presume negligible viscosity [95].
Several studies evaluated bicuspid aortic valve disease with 4D Flow CMR and the associated changes in flow patterns. The altered haemodynamics have an adverse effect on the aorta and therefore may explain why BAV is frequently associated with an aortopathy [34, 96]. Although TTE and PCMR provide a comprehensive assessment of BAV, 4D Flow CMR offers a number of advantages in this particular pathology. These are briefly described below, as 4D Flow CMR assessment of pathological aortic flow patterns in BAV is beyond the scope of this review.
4D Flow CMR allows visualisation and interrogation of abnormal flow patterns in BAV, which may result in altered wall shear stress (WSS) and subsequently aortic dilation in certain cases [97]. Measurements of TKE losses, amongst other advanced parameters, may help in risk stratification [94]. A study of 111 patients with BAV demonstrated that in-plane rotational flow, systolic flow reversal ratio and right/non-coronary cusp fusion subtype were predictors of aortic dilatation, suggesting the need for closer monitoring in these subgroups [96].
Elbaz and colleagues proposed the use of a 4D-virtual catheter for the assessment of intra-aortic haemodynamics in patients with BAV. The authors showed that markers such as KE, viscous energy loss rate (VELR) and vorticity were reproducible. In this study, patients with severe AS demonstrated the highest levels of VELR and vorticity [98]. Bissell et al. examined changes in flow patterns following intervention in BAV patients. Interestingly, the authors showed that patients with mechanical aortic valve replacement (AVR) or Ross procedure had normalisation of in-plane wall shear stress and rotational flow versus those with bioprosthetic AV, who didn’t demonstrate a similar effect [34]. Pressure drop mapping is another parameter that can be measured by 4D Flow CMR in patients with BAV. Although pressure drop is present in healthy controls, a significantly higher pressure drop was observed in patients with BAV; and there was an association between pressure drop and severity of stenosis [99].
Tricuspid regurgitation
Tricuspid valve is often difficult to visualise by TTE, which renders the evaluation of tricuspid regurgitation (TR) potentially inaccurate with poor reproducibility. Similar to the mitral valve, direct assessment of TR by PCMR is imprecise due to through-plane valve motion. Although indirect assessment of TR volume by subtracting pulmonary valve (PV) outflow from RV SV is routinely used in clinical practice, it is also limited by potential errors, mainly in stroke volume calculation [100]. Accurate assessment is crucial, as the severity of TR guides treatment decisions [9].
There are only a small number of studies, that have evaluated the tricuspid valve by 4D Flow CMR (Table 2). Techniques used to quantify TR volume and fraction included the direct and indirect method, similar to assessment of mitral regurgitant severity [9, 25, 69]. Interestingly, the agreement between direct and indirect assessment by 4D Flow CMR was shown to be better for TR than mitral regurgitation. Interobserver agreement also compared favourably in cases of TR versus mitral regurgitation. This can possibly be explained by the nature of TR jet, which is characteristically more uniform and laminar [9].
Westenberg and colleagues showed, that not only there was a good agreement between 4D Flow CMR quantified tricuspid forward flow volume and aortic systolic flow volume in healthy subjects, but also that this agreement was better for 4D Flow CMR than PCMR. There was also a good agreement between mitral valve and tricuspid valve flow in both, the healthy subjects and patients with regurgitation; both of which can be overestimated with PCMR. 4D Flow CMR may therefore be particularly useful in the assessment of TR volume and fraction, as similar to mitral regurgitation, PCMR does not account for valve annulus through-plane motion during systole. The SNR was, however, lower with 4D Flow imaging, as acceleration techniques had to be utilised to reduce scan time. Although theoretically this could reduce the accuracy of results due to lower image quality, the authors felt that in this case SNR was adequate for precise flow assessment [69] Roes et al. also demonstrated high agreement between net flow volumes across all valves, including in patients with one or more regurgitant lesion [25].
TR in the setting of congenital heart disease (CHD) provides further diagnostic challenges. A study of 21 healthy subjects and 67 patients with RV pressure overload secondary to pulmonary hypertension, pulmonary stenosis, tetralogy of Fallot with PV stenosis or systemic RV found, that the effective flow volume across the TV quantified by 4D Flow CMR and the effective pulmonic valve flow assessed by PCMR correlated well. There was discordance between TR severity grades in almost 40% of cases when compared to TTE. Despite the difficult anatomy in this cohort, 4D Flow CMR was shown to have high reproducibility [100]. An example of 4D Flow CMR assessment of moderate TR is shown in Fig. 6.

4D Flow CMR assessment of tricuspid regurgitation. a shows 4D flow streamline of tricuspid regurgitation. b demonstrates tricuspid forward flow visualised by 4D Flow CMR and c quantification of tricuspid forward flow by phase-contrast image obtained by 4D Flow CMR. d Shows pulmonary forward flow and e quantification of pulmonary forward flow by phase-contrast image obtained by 4D Flow CMR
Pulmonary regurgitation
The pulmonary valve is less often assessed in routine adult cardiology practice. However, pulmonary regurgitation (PR) is common in the CHD population and a detailed assessment of the PV is standard practice. Although PCMR is a well-established method of PR evaluation, the acquisition may be difficult and requires careful planning. It is recommended that velocity encoded imaging plane should be placed about 5 mm above the valve [82] and positioned perpendicular to the vessel [83]. However, similar to AR quantification, this is frequently optimised in clinical practice to avoid areas of turbulence and dephasing.
4D Flow CMR offers many advantages in the assessment of PR, including a relatively simple acquisition and direct visualisation of the regurgitant flow [101]. Table 2 summarizes 4D Flow CMR studies in PR.
The main application of 4D Flow in PR is in patients with repaired tetralogy of Fallot [51]. In a recent publication, Jacobs and colleagues evaluated PR in a paediatric population by measuring pulmonary net flow (PNF). The closest concordance of PNF by 4D Flow CMR with aortic valve flow was found to be at the valve level. PV forward flow and RV stroke volume demonstrated more than moderate agreement. This study also found, that there was a slight overestimation of RV volumes and function by 4D Flow CMR as compared with PCMR. Importantly, the 4D Flow acquisition was significantly shorter than the acquisition of a complete, conventional PCMR scan protocol, which is crucial in a paediatric population [102]. A prospective study of 52 adult patients, mostly with various CHD pathologies demonstrated, that pulmonary flow and PR can be reliably assessed via 4D Flow CMR, although peak systolic velocity can be underestimated as compared to PCMR. This error can be minimised by measuring velocity in the pulmonary artery where it is likely to be the highest [101]. Comprehensive evaluation of PR also includes the assessment of peak diastolic WSS, which was shown to be associated with severity of PR [103]. An example of 4D Flow CMR assessment of significant PR in the setting of repaired tetralogy of Fallot is shown in Fig. 7.

Phase Contrast CMR and 4D Flow CMR assessment of pulmonary regurgitation post tetralogy of Fallot repair. a and b Show sagittal and coronal right ventricular outflow tract views used for planning of pulmonary through-plane flow. Red line demarcates the analysis plane. c and d Show quantifications of pulmonary flow by PCMR revealing significant regurgitant flow. e Shows significant pulmonary regurgitation by 4D Flow CMR. f Demonstrates quantification of pulmonary regurgitant flow by 4D Flow CMR
Limitations
Limited spatial and temporal resolution are significant drawbacks of 4D Flow CMR [16]. These can lead to underestimation of high-velocity regurgitant jets [9]. Long scan times may also limit the utility of this technique in a number of settings such as claustrophobic or unwell patients who may not tolerate such a lengthy scan [29, 51]. Newer acceleration techniques, however, enable faster acquisition without a compromise in terms of spatial or temporal resolution. Labour-intensive post-processing further limits the clinical applicability of 4D Flow [29]. Similar to PCMR, phase offset errors can cause substantial artefacts and need to be corrected. Although effects of eddy currents cannot be entirely removed, they can be minimised [16].
Current status and future perspective
In routine clinical practice, an experienced 4D Flow user can complete quantification of aortic and pulmonary flow in about 5 min. Careful segmentation of mitral valve flow adds 5–10 min. If direct jet approach is used, it adds a few minutes to the post-processing time.
Despite all the developments of 4D Flow CMR in the recent years, it has not become a routine component of CMR protocols. Expensive analysis software, time consuming post-processing and expert analysis required all hinder adoption of 4D Flow in everyday CMR practice. Development of an approachable, user-friendly software could encourage more imaging specialists to train in this novel technique, increasing its clinical utility.
Conclusions
Assessment of VHD by 4D Flow CMR is precise and reproducible. Although still a relatively novel technique and not routinely employed in contemporary clinical practice, it has the potential to become the new reference-standard method for the evaluation of valvular lesions. It overcomes a lot of the constraints of other imaging modalities, including TTE, TEE and PCMR. With new acceleration techniques and developments in automated post-processing methods, scan times and post-processing times are likely to be substantially shortened in the future, making this technique much more clinically applicable.
Availability of data and materials
All data presented in this review are available via online search using Ovid MEDLINE database and Google Scholar.
Abbreviations
- 2D:
-
Two-dimensional
- 3D:
-
Three-dimensional
- 4D:
-
Four-dimensional
- AF:
-
Atrial fibrillation
- Ao:
-
Aortic flow
- AR:
-
Aortic regurgitation
- AS:
-
Aortic stenosis
- AV:
-
Aortic valve
- AVR:
-
Aortic valve replacement
- BAV:
-
Bicuspid aortic valve
- CHD:
-
Congenital heart disease
- CMR:
-
Cardiovascular magnetic resonance
- C-SENSE:
-
Compressed sensitivity encoding
- ECG:
-
Electrocardiogram
- ECG:
-
Effective orifice area
- EROA:
-
Effective regurgitant orifice area
- KE:
-
Kinetic energy
- Kt-BLAST:
-
Kt broad linear speed up technique
- LA:
-
Left atrium/left atrial
- LV:
-
Left ventricle/left ventricular
- LVEF:
-
Left ventricular ejection fraction
- LVOT:
-
Left ventricular outflow tract
- MIP:
-
Maximum intensity projection
- MRI:
-
Magnetic resonance imaging
- MV:
-
Mitral valve
- MVP:
-
Mitral valve prolapse
- MVR:
-
Mitral valve replacement
- PCMR:
-
Phase contrast magnetic resonance
- PISA:
-
Proximal isovelocity surface area
- PNF:
-
Pulmonary net flow
- PR:
-
Pulmonary regurgitation
- PROUD:
-
Prospective undersampling in multiple dimensions
- PV:
-
Pulmonary valve
- RF:
-
Regurgitant fraction
- RV:
-
Right ventricle/right ventricular
- RVol:
-
Regurgitant volume
- RVT:
-
Retrospective valve tracking
- SAVR:
-
Surgical aortic valve replacement
- SFT:
-
Semi-automated flow tracking
- SNR:
-
Signal-to-noise ratio
- SV:
-
Stroke volume
- TAVR:
-
Transcatheter aortic valve replacement
- TE:
-
Echo time
- TEE:
-
Transesophageal echocardiography
- TKE:
-
Turbulent kinetic energy
- TR:
-
Tricuspid regurgitation
- TTE:
-
Transthoracic echocardiography
- TV:
-
Tricuspid valve
- VELR:
-
Viscous energy loss rate
- VENC:
-
Velocity encoding
- VHD:
-
Valvular heart disease
- VLA:
-
Ventricular long axis
- WSS:
-
Wall shear stress
References
Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–91.
Bax JJ, Delgado V. Advanced imaging in valvular heart disease. Nat Rev Cardiol. 2017;14(4):209–23.
Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143(5):e72–227.
Grant MD, Mann RD, Kristenson SD, Buck RM, Mendoza JD, Reese JM, et al. Transthoracic echocardiography: beginner’s guide with emphasis on blind spots as identified with CT and MRI. Radiographics. 2021;41(4):1022–42.
Malik SB, Chen N, Parker RA III, Hsu JY. Transthoracic echocardiography: pitfalls and limitations as delineated at cardiac CT and MR imaging. Radiographics. 2017;37(2):383–406.
Myerson SG. CMR in evaluating valvular heart disease: diagnosis, severity, and outcomes. JACC Cardiovasc Imaging. 2020;14:2020.
Gulsin GS, Singh A, McCann GP. Cardiovascular magnetic resonance in the evaluation of heart valve disease. BMC Med Imaging. 2017;17(1):67.
Chambers JB, Myerson SG, Rajani R, Morgan-Hughes GJ, Dweck MR. Multimodality imaging in heart valve disease. Open Heart. 2016;3(1).
Feneis JF, Kyubwa E, Atianzar K, Cheng JY, Alley MT, Vasanawala SS, et al. 4D flow MRI quantification of mitral and tricuspid regurgitation: reproducibility and consistency relative to conventional MRI. J Magn Reson Imaging. 2018;48(4):1147–58.
Steeds RP, Garbi M, Cardim N, Kasprzak JD, Sade E, Nihoyannopoulos P, et al. EACVI appropriateness criteria for the use of transthoracic echocardiography in adults: a report of literature and current practice review. Eur Heart J Cardiovasc Imaging. 2017;18(11):1191–204.
Lancellotti P, Tribouilloy C, Hagendorff A, Popescu BA, Edvardsen T, Pierard LA, et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2013;14(7):611–44.
Herbold T, Chon S-H, Grimminger P, Maus MK, Schmidt H, Fuchs H, et al. Endoscopic treatment of transesophageal echocardiography-induced esophageal perforation. J Laparoendosc Adv Surg Tech. 2018;28(4):422–8.
Mathew RC, Loffler AI, Salerno M. Role of cardiac magnetic resonance imaging in valvular heart disease: diagnosis, assessment, and management. Curr Cardiol Rep. 2018;20(11):119.
Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU, et al. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol. 2002;90(1):29–34.
Maceira AM, Prasad SK, Khan M, Pennell DJ. Reference right ventricular systolic and diastolic function normalized to age, gender and body surface area from steady-state free precession cardiovascular magnetic resonance. Eur Heart J. 2006;27(23):2879–88.
Dyverfeldt P, Bissell M, Barker AJ, Bolger AF, Carlhall CJ, Ebbers T, et al. 4D flow cardiovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson. 2015;17:72.
Zaman A, Motwani M, Oliver JJ, Crelier G, Dobson LE, Higgins DM, et al. 3.0T, time-resolved, 3D flow-sensitive MR in the thoracic aorta: Impact of k-t BLAST acceleration using 8- versus 32-channel coil arrays. J Magn Reson Imaging. 2015;42(2):495–504.
Blanken CPS, Gottwald LM, Westenberg JJM, Peper ES, Coolen BF, Strijkers GJ, et al. Whole-heart 4D flow MRI for evaluation of normal and regurgitant valvular flow: a quantitative comparison between pseudo-spiral sampling and EPI readout. J Magn Reson Imaging. 2021.
Vial J, Bouzerar R, Pichois R, Lhostis F, Raad O, Mathiron A, et al. MRI assessment of right ventricular volumes and function in patients with repaired tetralogy of fallot using kat-ARC accelerated sequences. AJR Am J Roentgenol. 2020;215(4):807–17.
Philips. Philips launches new AI-enabled MR portfolio of smart diagnostic systems, optimized workflow solutions and integrated clinical solutions at RSNA 2021 2021. Available from: https://www.philips.com/a-w/about/news/archive/standard/news/press/2021/20211123-philips-launches-new-ai-enabled-mr-portfolio-of-smart-diagnostic-systems-optimized-workflow-solutions-and-integrated-clinical-solutions-at-rsna-2021.html.
Demirkiran A, van Ooij P, Westenberg JJM, Hofman MBM, van Assen HC, Schoonmade LJ, et al. Clinical intra-cardiac 4D flow CMR: acquisition, analysis, and clinical applications. Eur Heart J Cardiovasc Imaging. 2021;23:154.
Blanken CPS, Farag ES, Boekholdt SM, Leiner T, Kluin J, Nederveen AJ, et al. Advanced cardiac MRI techniques for evaluation of left-sided valvular heart disease. J Magn Reson Imaging. 2018;48(2):318–29.
Fidock B, Barker N, Balasubramanian N, Archer G, Fent G, Al-Mohammad A, et al. A systematic review of 4D-flow MRI derived mitral regurgitation quantification methods. Front Cardiovasc Med. 2019;6:103.
Chowdhary A, Garg P, Das A, Nazir MS, Plein S. Cardiovascular magnetic resonance imaging: emerging techniques and applications. Heart. 2021;107(9):697–704.
Roes SD, Hammer S, van der Geest RJ, Marsan NA, Bax JJ, Lamb HJ, et al. Flow assessment through four heart valves simultaneously using 3-dimensional 3-directional velocity-encoded magnetic resonance imaging with retrospective valve tracking in healthy volunteers and patients with valvular regurgitation. Invest Radiol. 2009;44(10):669–75.
Juffermans JF, Minderhoud SCS, Wittgren J, Kilburg A, Ese A, Fidock B, et al. Multicenter consistency assessment of valvular flow quantification with automated valve tracking in 4D flow CMR. JACC Cardiovasc Imaging. 2021;14(7):1354–66.
Doyle CM, Orr J, Greenwood JP, Plein S, Tsoumpas C, Bissell MM. Four-dimensional flow magnetic resonance imaging in the assessment of blood flow in the heart and great vessels: a systematic review. J Magn Reson Imaging. 2021;55:1301.
van der Geest RJ, Garg P. Advanced analysis techniques for intra-cardiac flow evaluation from 4D flow MRI. Curr Radiol Rep. 2016;4:38.
Markl M, Schnell S, Barker AJ. 4D flow imaging: current status to future clinical applications. Curr Cardiol Rep. 2014;16(5):481.
Mills MT, Grafton-Clarke C, Williams G, Gosling RC, Al Baraikan A, Kyriacou AL, et al. Feasibility and validation of trans-valvular flow derived by four-dimensional flow cardiovascular magnetic resonance imaging in patients with atrial fibrillation. Wellcome Open Res. 2021;6:73.
Nordmeyer S, Riesenkampff E, Messroghli D, Kropf S, Nordmeyer J, Berger F, et al. Four-dimensional velocity-encoded magnetic resonance imaging improves blood flow quantification in patients with complex accelerated flow. J Magn Reson Imaging. 2013;37(1):208–16.
Corrias G, Cocco D, Suri JS, Meloni L, Cademartiri F, Saba L. Heart applications of 4D flow. Cardiovasc Diagn Ther. 2020;10(4):1140–9.
Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4D flow MRI. J Magn Reson Imaging. 2012;36(5):1015–36.
Bissell MM, Loudon M, Hess AT, Stoll V, Orchard E, Neubauer S, et al. Differential flow improvements after valve replacements in bicuspid aortic valve disease: a cardiovascular magnetic resonance assessment. J Cardiovasc Magn Reson. 2018;20(1):10.
Galian-Gay L, Rodriguez-Palomares J, Guala A, Michelena HI, Evangelista A. Multimodality imaging in bicuspid aortic valve. Prog Cardiovasc Dis. 2020;63(4):442–51.
Nett EJ, Johnson KM, Frydrychowicz A, Del Rio AM, Schrauben E, Francois CJ, et al. Four-dimensional phase contrast MRI with accelerated dual velocity encoding. J Magn Reson Imaging. 2012;35(6):1462–71.
Callahan S, Singam NS, Kendrick M, Negahdar MJ, Wang H, Stoddard MF, et al. Dual-Venc acquisition for 4D flow MRI in aortic stenosis with spiral readouts. J Magn Reson Imaging. 2020;52(1):117–28.
Demirkiran A, van Ooij P, Westenberg JJ, Hofman M, van Assen HC, Schoonmade LJ, et al. Clinical intra-cardiac 4D flow CMR: acquisition, analysis, and clinical applications. Eur Heart J-Cardiovasc Imaging. 2021;23:154.
Uretsky S, Argulian E, Narula J, Wolff SD. Use of cardiac magnetic resonance imaging in assessing mitral regurgitation: current evidence. J Am Coll Cardiol. 2018;71(5):547–63.
Garg P, Swift AJ, Zhong L, Carlhall CJ, Ebbers T, Westenberg J, et al. Assessment of mitral valve regurgitation by cardiovascular magnetic resonance imaging. Nat Rev Cardiol. 2020;17(5):298–312.
Calkoen EE, Westenberg JJ, Kroft LJ, Blom NA, Hazekamp MG, Rijlaarsdam ME, et al. Characterization and quantification of dynamic eccentric regurgitation of the left atrioventricular valve after atrioventricular septal defect correction with 4D Flow cardiovascular magnetic resonance and retrospective valve tracking. J Cardiovasc Magn Reson. 2015;17:18.
Spampinato RA, Jahnke C, Crelier G, Lindemann F, Fahr F, Czaja-Ziolkowska M, et al. Quantification of regurgitation in mitral valve prolapse with four-dimensional flow cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2021;23(1):87.
Stankovic Z, Allen BD, Garcia J, Jarvis KB, Markl M. 4D flow imaging with MRI. Cardiovasc Diagn Ther. 2014;4(2):173–92.
Jaidka A, Hobbs H, Koenig S, Millington SJ, Arntfield RT. Better with ultrasound: transesophageal echocardiography. Chest. 2019;155(1):194–201.
Kirkpatrick JN, Mitchell C, Taub C, Kort S, Hung J, Swaminathan M. ASE statement on protection of patients and echocardiography service providers during the 2019 novel coronavirus outbreak: endorsed by the American College of Cardiology. J Am Soc Echocardiogr. 2020;33(6):648–53.
Musa TA, Treibel TA, Vassiliou VS, Captur G, Singh A, Chin C, et al. Myocardial scar and mortality in severe aortic stenosis. Circulation. 2018;138(18):1935–47.
Bohbot Y, Renard C, Manrique A, Levy F, Marechaux S, Gerber BL, et al. Usefulness of cardiac magnetic resonance imaging in aortic stenosis. Circ Cardiovasc Imaging. 2020;13(5).
Kaur H, Assadi H, Alabed S, Cameron D, Vassiliou VS, Westenberg JJM, et al. Left ventricular blood flow kinetic energy assessment by 4D flow cardiovascular magnetic resonance: a systematic review of the clinical relevance. J Cardiovasc Dev Dis. 2020;7(3):37.
Azarine A, Garcon P, Stansal A, Canepa N, Angelopoulos G, Silvera S, et al. Four-dimensional flow MRI: principles and cardiovascular applications. Radiographics. 2019;39(3):632–48.
Soulat G, McCarthy P, Markl M. 4D flow with MRI. Annu Rev Biomed Eng. 2020;22:103–26.
Rizk J. 4D flow MRI applications in congenital heart disease. Eur Radiol. 2021;31(2):1160–74.
Jacobs K, Hahn L, Horowitz M, Kligerman S, Vasanawala S, Hsiao A. Hemodynamic assessment of structural heart disease using 4D flow MRI: how we do it. AJR Am J Roentgenol. 2021;217(6):1322–32.
Xu K, Wang X, Yang Z, Xu H, Xu R, Xie L, et al. Quantification of peak blood flow velocity at the cardiac valve and great thoracic vessels by four-dimensional flow and two-dimensional phase-contrast MRI compared with echocardiography: a systematic review and meta-analysis. Clin Radiol. 2021;76(11):863.
Fidock B, Archer G, Barker N, Elhawaz A, Al-Mohammad A, Rothman A, et al. Standard and emerging CMR methods for mitral regurgitation quantification. Int J Cardiol. 2021;331:316–21.
Zhuang B, Sirajuddin A, Zhao S, Lu M. The role of 4D flow MRI for clinical applications in cardiovascular disease: current status and future perspectives. Quant Imaging Med Surg. 2021;11(9):4193–210.
Crandon S, Elbaz MSM, Westenberg JJM, van der Geest RJ, Plein S, Garg P. Clinical applications of intra-cardiac four-dimensional flow cardiovascular magnetic resonance: a systematic review. Int J Cardiol. 2017;249:486–93.
Kodali SK, Velagapudi P, Hahn RT, Abbott D, Leon MB. Valvular heart disease in patients ≥80 years of age. J Am Coll Cardiol. 2018;71(18):2058–72.
Lung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24(13):1231–43.
Dziadzko V, Clavel M-A, Dziadzko M, Medina-Inojosa JR, Michelena H, Maalouf J, et al. Outcome and undertreatment of mitral regurgitation: a community cohort study. The Lancet. 2018;391(10124):960–9.
Gajjar K, Kashyap K, Badlani J, Williams RB, Biederman RWW. A review of the pivotal role of cardiac MRI in mitral valve regurgitation. Echocardiography. 2021;38(1):128–41.
Nikolou E, Bilkhu R, Kafil TS, Demetrescu C, Kotta PA, Lucchese G, et al. Multimodality imaging in transcatheter mitral interventions. Front Cardiovasc Med. 2021;8(92).
Uretsky S, Gillam L, Lang R, Chaudhry FA, Argulian E, Supariwala A, et al. Discordance between echocardiography and MRI in the assessment of mitral regurgitation severity: a prospective multicenter trial. J Am Coll Cardiol. 2015;65(11):1078–88.
Myerson SG, d’Arcy J, Christiansen JP, Dobson LE, Mohiaddin R, Francis JM, et al. Determination of clinical outcome in mitral regurgitation with cardiovascular magnetic resonance quantification. Circulation. 2016;133(23):2287–96.
Penicka M, Vecera J, Mirica DC, Kotrc M, Kockova R, Van Camp G. Prognostic implications of magnetic resonance-derived quantification in asymptomatic patients with organic mitral regurgitation: comparison with Doppler echocardiography-derived integrative approach. Circulation. 2018;137(13):1349–60.
Uretsky S, Shah DJ, Lasam G, Horgan S, Debs D, Wolff SD. Usefulness of mitral regurgitant volume quantified using magnetic resonance imaging to predict left ventricular remodeling after mitral valve “Correction.” Am J Cardiol. 2020;125(11):1666–72.
Aplin M, Kyhl K, Bjerre J, Ihlemann N, Greenwood JP, Plein S, et al. Cardiac remodelling and function with primary mitral valve insufficiency studied by magnetic resonance imaging. Eur Heart J Cardiovasc Imaging. 2016;17(8):863–70.
Suinesiaputra A, Bluemke DA, Cowan BR, Friedrich MG, Kramer CM, Kwong R, et al. Quantification of LV function and mass by cardiovascular magnetic resonance: multi-center variability and consensus contours. J Cardiovasc Magn Reson. 2015;17(1):63.
Krieger EV, Lee J, Branch KR, Hamilton-Craig C. Quantitation of mitral regurgitation with cardiac magnetic resonance imaging: a systematic review. Heart. 2016;102(23):1864–70.
Westenberg JJ, Roes SD, Ajmone Marsan N, Binnendijk NM, Doornbos J, Bax JJ, et al. Mitral valve and tricuspid valve blood flow: accurate quantification with 3D velocity-encoded MR imaging with retrospective valve tracking. Radiology. 2008;249(3):792–800.
Kamphuis VP, Roest AAW, Ajmone Marsan N, van den Boogaard PJ, Kroft LJM, Aben JP, et al. Automated cardiac valve tracking for flow quantification with four-dimensional flow MRI. Radiology. 2019;290(1):70–8.
Brandts A, Bertini M, van Dijk EJ, Delgado V, Marsan NA, van der Geest RJ, et al. Left ventricular diastolic function assessment from three-dimensional three-directional velocity-encoded MRI with retrospective valve tracking. J Magn Reson Imaging. 2011;33(2):312–9.
Marsan NA, Westenberg JJ, Ypenburg C, Delgado V, van Bommel RJ, Roes SD, et al. Quantification of functional mitral regurgitation by real-time 3D echocardiography: comparison with 3D velocity-encoded cardiac magnetic resonance. JACC Cardiovasc Imaging. 2009;2(11):1245–52.
Blanken CPS, Westenberg JJM, Aben JP, Bijvoet GP, Chamuleau SAJ, Boekholdt SM, et al. Quantification of mitral valve regurgitation from 4D flow MRI using semiautomated flow tracking. Radiol Cardiothorac Imaging. 2020;2(5).
Gorodisky L, Agmon Y, Porat M, Abadi S, Lessick J. Assessment of mitral regurgitation by 3-dimensional proximal flow convergence using magnetic resonance imaging: comparison with echo-Doppler. Int J Cardiovasc Imaging. 2018;34(5):793–802.
Westenberg JJM, van Assen HC, van den Boogaard PJ, Goeman JJ, Saaid H, Voorneveld J, et al. Echo planar imaging-induced errors in intracardiac 4D flow MRI quantification. Magn Reson Med. 2022;87(5):2398–411.
Al-Wakeel N, Fernandes JF, Amiri A, Siniawski H, Goubergrits L, Berger F, et al. Hemodynamic and energetic aspects of the left ventricle in patients with mitral regurgitation before and after mitral valve surgery. J Magn Reson Imaging. 2015;42(6):1705–12.
Wardley J, Swift A, Ryding A, Garg P. Four-dimensional flow cardiovascular magnetic resonance for the assessment of mitral stenosis. Eur Heart J Case Rep. 2021;5(12):ytab465.
Abdelaziz HM, Tawfik AM, Abd-Elsamad AA, Sakr SA, Algamal AM. Cardiac magnetic resonance imaging for assessment of mitral stenosis before and after percutaneous balloon valvuloplasty in comparison to two- and three-dimensional echocardiography. Acta Radiol. 2020;61(9):1176–85.
Alvarez A, Martinez V, Pizarro G, Recio M, Cabrera JA. Clinical use of 4D flow MRI for quantification of aortic regurgitation. Open Heart. 2020;7(1).
Harris AW, Krieger EV, Kim M, Cawley PJ, Owens DS, Hamilton-Craig C, et al. Cardiac magnetic resonance imaging versus transthoracic echocardiography for prediction of outcomes in chronic aortic or mitral regurgitation. Am J Cardiol. 2017;119(7):1074–81.
Myerson SG, d’Arcy J, Mohiaddin R, Greenwood JP, Karamitsos TD, Francis JM, et al. Aortic regurgitation quantification using cardiovascular magnetic resonance: association with clinical outcome. Circulation. 2012;126(12):1452–60.
Kramer CM, Barkhausen J, Bucciarelli-Ducci C, Flamm SD, Kim RJ, Nagel E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson. 2020;22(1):17.
Lotz J, Meier C, Leppert A, Galanski M. Cardiovascular flow measurement with phase-contrast MR imaging: basic facts and implementation. Radiographics. 2002;22(3):651–71.
Chatzimavroudis GP, Oshinski JN, Franch RH, Pettigrew RI, Walker PG, Yoganathan AP. Quantification of the aortic regurgitant volume with magnetic resonance phase velocity mapping: a clinical investigation of the importance of imaging slice location. J Heart Valve Dis. 1998;7(1):94–101.
Chelu RG, van den Bosch AE, van Kranenburg M, Hsiao A, van den Hoven AT, Ouhlous M, et al. Qualitative grading of aortic regurgitation: a pilot study comparing CMR 4D flow and echocardiography. Int J Cardiovasc Imaging. 2016;32(2):301–7.
Ewe SH, Delgado V, van der Geest R, Westenberg JJ, Haeck ML, Witkowski TG, et al. Accuracy of three-dimensional versus two-dimensional echocardiography for quantification of aortic regurgitation and validation by three-dimensional three-directional velocity-encoded magnetic resonance imaging. Am J Cardiol. 2013;112(4):560–6.
Everett RJ, Treibel TA, Fukui M, Lee H, Rigolli M, Singh A, et al. Extracellular myocardial volume in patients with aortic stenosis. J Am Coll Cardiol. 2020;75(3):304–16.
Kwak S, Everett RJ, Treibel TA, Yang S, Hwang D, Ko T, et al. Markers of myocardial damage predict mortality in patients with aortic stenosis. J Am Coll Cardiol. 2021;78(6):545–58.
Garcia J, Barker AJ, Markl M. The role of imaging of flow patterns by 4D flow MRI in aortic stenosis. JACC Cardiovasc Imaging. 2019;12(2):252–66.
Garcia J, Markl M, Schnell S, Allen B, Entezari P, Mahadevia R, et al. Evaluation of aortic stenosis severity using 4D flow jet shear layer detection for the measurement of valve effective orifice area. Magn Reson Imaging. 2014;32(7):891–8.
Archer GT, Elhawaz A, Barker N, Fidock B, Rothman A, van der Geest RJ, et al. Validation of four-dimensional flow cardiovascular magnetic resonance for aortic stenosis assessment. Sci Rep. 2020;10(1):10569.
Negahdar MJ, Kadbi M, Kendrick M, Stoddard MF, Amini AA. 4D spiral imaging of flows in stenotic phantoms and subjects with aortic stenosis. Magn Reson Med. 2016;75(3):1018–29.
Dyverfeldt P, Hope MD, Tseng EE, Saloner D. Magnetic resonance measurement of turbulent kinetic energy for the estimation of irreversible pressure loss in aortic stenosis. JACC Cardiovasc Imaging. 2013;6(1):64–71.
Hallett R, Moainie S, Hermiller J, Fleischmann D. CT and MRI of aortic valve disease: clinical update. Curr Radiol Rep. 2016;4(9).
Ha H, Kvitting JP, Dyverfeldt P, Ebbers T. Validation of pressure drop assessment using 4D flow MRI-based turbulence production in various shapes of aortic stenoses. Magn Reson Med. 2019;81(2):893–906.
Dux-Santoy L, Guala A, Teixido-Tura G, Ruiz-Munoz A, Maldonado G, Villalva N, et al. Increased rotational flow in the proximal aortic arch is associated with its dilation in bicuspid aortic valve disease. Eur Heart J Cardiovasc Imaging. 2019;20(12):1407–17.
Hope MD, Hope TA, Crook SE, Ordovas KG, Urbania TH, Alley MT, et al. 4D flow CMR in assessment of valve-related ascending aortic disease. JACC Cardiovasc Imaging. 2011;4(7):781–7.
Elbaz MSM, Scott MB, Barker AJ, McCarthy P, Malaisrie C, Collins JD, et al. Four-dimensional virtual catheter: noninvasive assessment of intra-aortic hemodynamics in bicuspid aortic valve disease. Radiology. 2019;293(3):541–50.
Fatehi Hassanabad A, Burns F, Bristow MS, Lydell C, Howarth AG, Heydari B, et al. Pressure drop mapping using 4D flow MRI in patients with bicuspid aortic valve disease: a novel marker of valvular obstruction. Magn Reson Imaging. 2020;65:175–82.
Driessen MMP, Schings MA, Sieswerda GT, Doevendans PA, Hulzebos EH, Post MC, et al. Tricuspid flow and regurgitation in congenital heart disease and pulmonary hypertension: comparison of 4D flow cardiovascular magnetic resonance and echocardiography. J Cardiovasc Magn Reson. 2018;20(1):5.
Chelu RG, Wanambiro KW, Hsiao A, Swart LE, Voogd T, van den Hoven AT, et al. Cloud-processed 4D CMR flow imaging for pulmonary flow quantification. Eur J Radiol. 2016;85(10):1849–56.
Jacobs KG, Chan FP, Cheng JY, Vasanawala SS, Maskatia SA. 4D flow vs. 2D cardiac MRI for the evaluation of pulmonary regurgitation and ventricular volume in repaired tetralogy of Fallot: a retrospective case control study. Int J Cardiovasc Imaging. 2020;36(4):657–69.
Rizk J, Latus H, Shehu N, Mkrtchyan N, Zimmermann J, Martinoff S, et al. Elevated diastolic wall shear stress in regurgitant semilunar valvular lesions. J Magn Reson Imaging. 2019;50(3):763–70.
Acknowledgements
Dr. Christopher Francois served as the JCMR Guest Editor for this manuscript.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
MG was responsible for review of relevant literature, drafting the manuscript and preparation of tables and figures. MMB, DMH, PG and SP were responsible for revision of the draft manuscript. JPG was responsible for revision and final approval of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gorecka, M., Bissell, M.M., Higgins, D.M. et al. Rationale and clinical applications of 4D flow cardiovascular magnetic resonance in assessment of valvular heart disease: a comprehensive review. J Cardiovasc Magn Reson 24, 49 (2022). https://doi.org/10.1186/s12968-022-00882-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12968-022-00882-0