
Abstract
Background
Fruit and vegetable (FV) consumption in children in the United States (US) is very low. Adequate FV consumption is required for proper development during childhood, and dietary habits are established during preschool-age and tend to persist into adulthood. As most U.S. preschool-aged children attend childcare or preschool, this may be an opportune time and setting to conduct interventions to improve FV intake. These interventions should be based in theory and use behavior change techniques (BCTs) to explain mechanisms for expected change. To date, no published reviews have examined the effectiveness of childcare- or preschool-based FV interventions in preschoolers and their use of theoretical frameworks and BCTs.
Methods
This systematic review was completed adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Inclusion criteria were randomized controlled trials (RCTs) published between 2012 and 2022 of interventions to improve diet or FV intake in preschoolers (aged 2–5 years) in childcare or preschool-settings. A search of four databases was conducted between in September 2022 using search terms pertaining to the study’s primary aim (FV consumption), age group (preschool-aged), settings (US childcare or preschool settings), and study design (RCT). Additional criteria were objective measures of FV consumption or skin carotenoids, as a proxy for FV intake. Included studies were narratively synthesized based on intervention type, measured effect, and use of theory and BCTs.
Results
The search resulted in six studies that reported on nine interventions. Overall, six interventions increased FV intake, of which five used nutrition education and one manipulated the feeding environment. Among the three interventions with no measured effect, two manipulated the feeding environment and one used peer modeling. Effective studies used at least three BCTs, though no pattern was observed between use of theory or BCTs and intervention effect.
Conclusions
While several studies have shown promising results, the limited number of studies identified in this review highlights key gaps in this field: there is a need for studies to test FV interventions in US childcare settings that use objective measures of FV intake, directly compare intervention components and BCTs, are theory-based, and assess long-term behavior change.
Similar content being viewed by others


Introduction
Promoting fruit and vegetable (FV) intake in children is critical to support proper brain and body development [1,2,3] and to establish healthy dietary habits that persist over the life course [4, 5]. Despite the long-standing explicit guidelines and evidence regarding the importance of FV intake, average FV consumption amongst all US children (2–18 years old) remains low: only 40% and 7% meet the recommended intake for fruits and vegetables, respectively [6]. The current average intake for children is only 0.9 cup equivalents of each (60% of recommended), with consumption levels that decline with age and are restricted in variety relative to recommended guidelines [7]. Thus, in support of public health, it is important to develop strategies to improve FV intake in children.
Preschool age children begin developing their own dietary habits by gaining autonomy over their food choice [4, 5], evident in the decline in FV intake as children transition from preschool age to school age [8,9,10]. Thus, preschool age (2–5 years old) may be an optimal time for a dietary intervention to promote FV intake throughout the lifespan. However, there are key gaps and inconsistencies present in diet research that will be discussed below.
Consideration of the measurement tool in diet research is particularly important in young children because they are unable to accurately report their own intake [11, 12]. Parent-reported measures, while most frequently used in research [13,14,15], have been repeatedly shown to be subjective and prone to recall and reporting bias [16, 17]; this is especially problematic when parents are asked to report on periods of time for which they are not directly responsible for child feeding, such as during childcare hours [18, 19]. As such, use of objective observation measures is critical with this age group [20, 21]. An additional objective measure specific to FV intake is the skin carotenoid level [22,23,24,25,26]. When FVs are consumed, the carotenoids in the FVs are absorbed and then deposited in various tissues including the skin [27], which can be quantified using reflection spectroscopy [17] to objectively measure FV intake within the previous two to four weeks [26, 28, 29]. Due to the discrepancies associated with the different techniques used to measure dietary intake, reviews should distinguish between studies with subjective and objective measures to adequately evaluate the validity of a large proportion of this body of work.
The setting of dietary interventions in children is another significant consideration. In 2019, nearly two-thirds (64%) of 3–5 year old children in the US were enrolled in childcare or preschool with 64.7% of all enrollments being full-time [30]. Thus, childcare services have a large influence on children’s development in the US [31], and this may be an efficient avenue to effectively influence children’s behavior, namely dietary behavior [32,33,34]. In evaluating intervention effectiveness, it is therefore vital to consider the setting of the interventions to avoid extrapolating evidence for intervention effectiveness to other contexts.
Behavior change techniques (BCTs) are the intervention components regarded as the “active ingredients” within behavior change interventions. It is often helpful to examine the use of BCTs within interventions aimed at changing dietary behaviors to assess the mechanism by which interventions may be effective at causing the behavior change [35]. Given the heterogeneity in intervention techniques used in dietary interventions, evaluation of BCTs in reviews and meta-analyses may provide important insight on the underlying intervention components that may be at play [35,36,37].
Use of theory in developing an intervention is another metric that can be examined within interventions that target behavior change. This metric evaluates how exactly a specific theory and its concepts are utilized to tailor intervention techniques and components and allows for a better understanding of why an intervention is effective or ineffective. This knowledge may then be evaluated in systematic reviews and applied to the refinement of an interventions to better target the tenets of the theory [38, 39].
A recent systematic literature review by Hodder et al. [40] of FV intake in children five years and younger identified 80 trials reporting a large variety of interventions to promote FV intake in preschool-aged children globally. This review included interventions conducted in all settings and using various intervention methods, though it did not distinguish between subjective and objective measurements of food intake or evaluate BCTs and use of theory in the included studies. The main implications drawn from these findings is that more pragmatic studies are needed to test the interventions, and that these interventions should be based on BCTs and theoretical frameworks that may explain the mechanism by which these interventions may change children’s dietary behaviors related to FV intake [41].
In 2012, Hendrie et al. [42] published a systematic review to explore the use of BCTs in home- and school-based interventions for the prevention of childhood obesity involving children and parents. More specifically, they compared the number and type of BCTs used in effective and ineffective studies and reported that effective studies incorporated more BCTs than ineffective studies (median of 10 versus 6.5). However, this review was not specific to interventions aimed at improving FV intake, so we are unable to determine whether these findings are applicable to FV interventions specifically.
In 2017, Hendrie et al. [43] used a similar technique to evaluate interventions to improve vegetable intake in children and found that the BCTs “Repeated exposure”, “Provision of staff training,” and “Planning for social support or change,” were associated with effective behavior change. This review only examined interventions conducted in home or community settings and, therefore, these results may not be extrapolated to interventions conducted in other settings, such as childcare centers [53]. Similar to the review by Hodder et al., these two reviews are limited by their inclusion of subjective measures of dietary change, and lack of evaluation of use of theory within the included studies.
To our knowledge, there are currently no published reviews that evaluate both the effectiveness of FV interventions specifically in childcare- or preschool-based settings in the US, and the use of theoretical frameworks and BCTs within these studies. This is a critical gap as comparing different types of interventions, exploring whether use of theory and BCTs moderate effectiveness, and summarizing the level of evidence is critically needed to develop effective interventions in the future. Therefore, the purpose of this review was to systematically identify published randomized controlled trials (RCTs) evaluating childcare- or preschool-based interventions designed to increase objectively measured intake of fruits, vegetables, or both, in preschool children (aged 2–5 years) in the US and to summarize their methods and results. This review also aimed to identify the use of theoretical models and BCTs in each study and to assess their effectiveness in improving FV intake.
Methods
Search strategy
This systematic review utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was pre-registered with PROSPERO International Prospective Register of Systematic Reviews (ID: CRD42022350953). Studies were identified using CINAHL, PubMed, Web of Science, and MEDLINE (Ovid) between August 15 and September 4, 2022. The following search terms, using Boolean operators and MeSH terms (PubMed), were used: (fruit OR vegetable) AND (intake OR consumption) AND (“young children” OR preschool OR pre-kindergarten) AND (preschool OR center* OR childcare* OR daycare*) AND (intervention* OR program OR “nutrition education”). Additional search hedges included in the search were designed to include only randomized-controlled trials and studies conducted within the US. The search was restricted to articles published in English between January 2012 and September 2022. The reference list of included articles were reviewed to identify additional relevant articles. Search strategies were reviewed by a university librarian.
Grey literature
The risk of publication bias was evaluated by examining preprints and unpublished studies from clinical trial registries and dissertation/theses, using a google search tool to limit results to “.gov,” “.org”, and “.edu” sources, ClinicalTrials.gov, ProQuest Dissertations and Theses Global database (unpublished theses), and MedRxiv (pre-prints of relevant studies). The search terms used for the grey literature search were “fruit and vegetable interventions in preschoolers in the United States.” The search using the ProQuest Dissertations and Theses database was limited to scholarly journals and dissertations and theses, only English and in the US, and within the last 10 years. The search using the MedRxiv database used the previously stated Boolean search terms and was also limited to the last 10 years.
The risk of outcome reporting bias was assessed by comparing planned outcomes in the Methods section with reported outcomes to identify any missing outcomes. Two researchers (FH and AVN) independently screened the titles and abstracts of all articles based on the inclusion and exclusion criteria stated below. Any discrepancies between reviewers were resolved by discussion until consensus was reached. If necessary, a third reviewer (SK) was consulted.
Eligibility criteria
Eligible studies were randomized controlled trials (RCTs) conducted in the US that utilized an intervention to improve fruit and/or vegetable intake in preschoolers (children 2–5 years old), were conducted in preschool or childcare settings, and examined the magnitude of change from baseline (between an intervention and control group) of the number of servings, portions, or grams of FVs consumed or changes in skin carotenoid levels used as a proxy for FV intake. We restricted our inclusion criteria study reports to interventions in the US to allow for comparison between studies that are based on the uniform national recommendations/guidelines, similar food supply, similar access to federal nutrition programs (WIC and SNAP) and known cultural differences in dietary patterns. For instance, the United Kingdom National Health Services (NHS) dietary guidelines for two- to five-year old children are: “should gradually move to eating the same foods as the rest of the family in the proportions shown in the Eatwell Guide [44],” with no specific consumption amount or type of FV specified during childhood. The Eatwell Guide specification for which FV to consume is different from the US guidance, for example, potatoes are not counted as vegetables. Only studies published within the previous 10 years were considered for inclusion to ensure recency of data and to reflect changes in early childhood education approaches. For example, the Mere Exposure hypothesis, first developed in 1968 and later applied to the context of children’s dietary behavior, was considered the cornerstone method of improving children’s diet until relatively recent studies found that it may not be applicable to all children [45] and results may not be sustainable [46] and researchers modified their approach. Only studies in which FV intake was measured objectively were included, and FV intake or diet must have been measured as one of the primary aims. Studies that reported only subjective measures of FV intake were excluded due to the lower validity of subjective dietary measures. Hence, those that used self-reported measures, such as dietary recalls or caregiver questionnaires, were excluded. Interventions that aimed to improve overall diet quality with fruit and/or vegetables as a component were also included; interventions whose primary aim were not diet related, such as those aiming to produce weight loss, were excluded due to the potential for confounding.
The population being studied included preschool children, parents, guardians, caregivers, and professionals responsible for the care of preschool children. Studies were included if they combined both child- and parent-targeted interventions. Studies were excluded if the interventions only targeted parents or caregivers of preschoolers, such as only parent-focused nutrition education interventions. Studies focused on populations with special developmental considerations, such as autism spectrum disorder, were also excluded because these children have been shown to respond differently to dietary interventions [47,48,49].
Data extraction and synthesis
Data selection and extraction were conducted with the use of Covidence, a program developed for conducting systematic reviews and meta-analyses. Studies were independently reviewed by two reviewers (FH and AVN) and selected for inclusion using a pre-specified form with the inclusion and exclusion criteria explicitly stated and reviewed by a professional expert in childhood nutrition (SK). Disagreements about article classifications between reviewers were resolved by discussion and consensus between the two reviewers (FH and AVN). A third reviewer (SK) was consulted, if necessary. A data extraction form was developed under supervision of an expert in the topic (WY) and piloted on five randomly selected studies that met inclusion criteria. Data was then extracted in duplicate by the first author (FH) and two additional authors (AVN and ARR) to ensure duplicity.
Outcome data were extracted using mean difference in fruit and/or vegetable intake, where outcomes were reported in grams, and standardized mean difference, where outcomes were reported using a different method (grams per kilogram of body weight, grams per total energy intake, servings). The results of statistical analyses were extracted including, but not limited to, t-tests, analysis of variance, analysis of covariance, and linear and mixed-model regressions. For studies that reported multiple timepoints for fruit and/or vegetable intake, the data for each timepoint was extracted separately. For studies that did not report effect size, effect size estimates (Cohen’s d) were calculated by the first author using either means/standard deviations of each group or reported t-test values. We were unable to estimate effect size for two interventions due to lack of reported standard deviations [50]. We also coded for additional study characteristics, if applicable to the study, including: 1) information pertaining to the study design, setting, length, frequency, description and length of interventions, outcomes measured and measurement tools used to obtain these measurements, 2) sample size, mean age of participants or proportion of children within provided age groups, sex of participants, 3) identification and classification of behavioral or cognitive theories and/or models used, 4) identification and classification of BCTs used, 5) predictors and/or confounders of response to the FV intervention, and 6) cost-effectiveness of the intervention, if applicable. The additional variables were evaluated on a case-by-case basis and compared to the usual care and/or comparator(s) defined within the intervention.
The use of BCTs were identified within studies and coded accordingly using a standardized taxonomy of behavior change techniques [36]. This taxonomy consists of 93 unique BCTs grouped into 16 domains. BCTs used within studies were coded in duplicate by the first author (FH) and two independent reviewers (AVN and ARR). Interclass correlation coefficient was used to establish intercoder reliability of BCTs present and absent, as well as number of BCTs used in each study. Any discrepancies were then resolved by consensus amongst all three coders.
The use of theory within studies was also evaluated by the first author (FH) using a Theory Coding Scheme developed by Michie and Prestwich in 2010 [38]. This taxonomy consists of 19 items; items 1–6 evaluate if theory is mentioned, whether it was used to select participants, and whether it was tailored to participants, items 7–11 evaluate whether the relevant theoretical constructs were explicitly targeted and all intervention techniques are linked to a specific construct, and items 12–19 assess whether the theory was adequately measured within the intervention and explains the changes observed, and whether the theory was refined based on the intervention’s outcomes. This review aimed to identify the use of theory in the development of interventions, rather than how well the specific theories were able to yield results. Hence, items 12–19 were not evaluated in this review [39]. Items 1–11 were scored based on whether they were present within the paper and were summed to yield a Use of Theory score ranging from 0 to 11, with higher scores indicating greater use of theory [39]. For studies for which a separate publication was available to describe the intervention development or methodology, we used that publication to assess the intervention’s Use of Theory score.
The included studies were organized into subgroups by type of intervention (e.g. repeated exposure, nutrition education). Although intervention types were not directly compared to one another due to heterogeneity between studies, each subgroup was evaluated as a group based on the level of evidence, patterns in the measured effect (mean difference in fruit and/or vegetable intake), and any adverse effects unique to that intervention type. Information regarding the maintenance or sustainability of the behavior change was evaluated by assessing data of a post-intervention follow-up period, if applicable, within each included study. Following narrative synthesis of the results, the additional outcomes were evaluated in the context of the intervention and its overall desired effect.
Quality assessment
Risk of bias within studies was examined using the Cochrane risk of bias assessment tool [51]. This tool evaluates randomization, deviations from the intended interventions, outcome data, measurement of outcome, and selection of the reported results. Two researchers (FH and AVN) individually assessed the included studies for risk of bias using this tool. The risk of bias was judged within each domain and overall risk-of-bias as 'low risk', 'some concerns', 'high risk', or 'unclear risk'. Any discrepancies between reviewers were resolved by consensus between the two reviewers.
Results
Search results
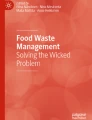
A total of 70 studies was identified during the initial search. After removing duplicates, 53 remained and were screened by title and abstract using the inclusion and exclusion criteria. No additional studies were identified using backward and forward snowballing. No studies were identified in the grey literature. After title and abstract screening, 14 studies were screened as full text, and eight were excluded for various reasons, such as not measuring FV intake objectively (ie. using self-reported measures of dietary intake), not being conducted in the US, and not RCTs. The final review included six papers that reported on nine unique interventions from 2012 to 2022 (Fig. 1). Studies that reported on multiple intervention groups were analyzed as separate interventions.

PRISMA flow diagram of literature search
Study characteristics
Study designs included cluster- (six interventions), crossover- (two interventions) and individual- (one intervention) RCTs. Interventions ranged from a single day to 12 weeks, with a frequency of two to five days per week. The mean total intervention days across all interventions was 20.33 days, with a range of 1 to 40 days. Only two studies (two interventions) included a follow-up period, which included seven days [52] and three months [53] post-intervention. The remaining four studies (seven interventions) only assessed FV intake immediately post-intervention [50, 54,55,56]. All interventions were conducted in preschool settings; three studies (five interventions) specified the use of Head Start programs for the intervention [50, 55, 56]. Only four of nine studies reported the mean age of the participants, which ranged from 4.1 to 4.9 years. The remaining studies reported the proportion of 2–3 and 4–5 year olds [50, 56] or were not permitted to record the children’s ages [53].
Intervention components used across studies were nutrition education [53,54,55,56], changing the feeding environment [50, 56], peer modeling [52], and repeated exposure to FVs [53, 56]. Two interventions were classified as multi-component as they included more than one of the intervention components: Witt et al. [53] included nutrition education and repeated exposure and Smith et al. [56] included nutrition education, changing the food environment, and repeated exposure. Additionally, three interventions elicited parent involvement by sending home newsletters [56] or education materials [53] to families of participating children. No included study reported cost-effectiveness of the intervention.
Seven studies reported on directly measured fruit and/or vegetable consumption using direct observation methods of visual observation [50, 54], photo-assisted [55], or plate-waste method [52, 53] during either snack [52,53,54] or lunch [50, 55]. The remaining two, both by Smith and colleagues [56], estimated FV intake by measuring skin carotenoid levels using resonance Raman spectroscopy. Four interventions measured only vegetables [52, 54, 55], three interventions measured both fruits and vegetables separately [50, 53], and two interventions measured combined fruits and vegetable intake [56].
Intervention effectiveness and study quality assessment
Overall, six out of nine interventions were able to significantly increase fruit and/or vegetable intake. Of these six, half of them were conducted in Head Start programs. Two (out of three) interventions observed an increase in fruit consumption. Four (out of seven) interventions observed an increase in vegetable consumption. One of the two interventions that measured skin carotenoids was effective at improving FV consumption. Two of the studies with no FV improvement used changing the feeding environment [50, 56] and one used peer modeling [52] as their intervention method. Unexpectedly, one intervention led to a significant decrease in FV consumption [50]. Two of these three ineffective studies were conducted in Head Start programs. The characteristics of all included studies are described in Additional file 1.
We were unable to estimate effect size for two interventions due to lack of reported standard deviations [50]. Amongst the studies with statistically significant effects, two studies [54, 55] had small effect sizes (d < 0.50), one [54] had a medium effect size (d is 0.50 to < 0.80), and the remaining two [52, 53, 56] had large effect sizes (d > 0.80). Amongst the studies with no statistically significant effects, both had large effect sizes (d > 0.80) [52, 56].
Three of the six studies (which reported on five of nine interventions) were rated as low risk of bias and the remaining four were rated as having some concerns for bias. The reasons for were no mention of pre-specified analysis plan [54] and no information regarding concealment of allocation sequence (to both researchers and subjects) prior to assignment of the intervention [53, 55]. A table reporting the risk of bias assessments is provided in Additional file 2.
Behavior-change techniques
Intercoder reliability determined by inter-rater intraclass correlation coefficient (ICC) was “moderate” for BCTs present and absent (ICC = 0.70) and “good” for the number of BCTs used in each study (ICC = 0.77). Overall, 23 of the 93 BCTs were used in at least one intervention. Interventions used between one and ten BCTs, spanning between one and seven domains, with an average of 4.44 techniques used.
The most commonly used BCTs were “Adding objects to the environment” and “Framing/reframing”, which were both used in five of the nine interventions. The most commonly used domains (ie. used at least once within an intervention) were “Antecedents” and “Identity”, both of which were used by five interventions. The most frequently used domains (ie. total number of BCTs within this domain used within studies) were “Antecedents” and “Repetition and substitution”, whose BCTs were used nine and seven times across interventions, respectively. Two domains, “Feedback and monitoring” and “Regulation” were not used by any studies.
The BCTs and domains used in studies that did and did not effectively increase FV intake are described in Table 1. Effective studies used at least three BCTs and covered at least two domains. Two of the ineffective interventions used only the “Antecedents” domain [50, 56] and the remaining used only “Covert learning” domain [52]. No domains or BCTs were exclusive to effective or ineffective interventions.
Theoretical frameworks
Two studies [54, 56] cited separate methodology publications that were used for the Use of Theory score [57, 58]. Overall, the average Use of Theory score across interventions was 2.33 (out of 11) and ranged from 0 to 8. Four interventions [52, 53, 55, 56] mentioned a theory or model of behavior and only two of these [53, 55] linked the theory or its constructs to their intervention techniques. While the limited number of studies prohibits an empirical investigation, a narrative comparison reveals no pattern in the Use of Theory score and intervention effectiveness; the average score amongst effective and ineffective interventions was 2.17 and 2.67, respectively. In fact, the intervention with the highest Use of Theory score was ineffective [52]. The Use of Theory scoring of included interventions is described in Additional file 3.
Discussion
We identified nine childcare- or preschool-based RCTs, reported in six different publications, that objectively measured FV intake in 2–5 year old children. Six of the nine achieved their goal of improving FV intake using the three following intervention methods: nutrition education, repeated exposure, and change in feeding environment. Two of the nine interventions had large effect sizes [55, 57], one had a moderate effect size [53], and two had small effect sizes [52, 53].
Even beyond the effect size heterogeneity, some studies reported substantial imprecision in effect size estimates. For example, in two of the studies reporting large effect sizes (d > 2.5), the standard errors were large and the differences did not reach the threshold for statistical significance at p < 0.05 [55, 56]. Therefore, the nonsignificant findings in these two studies may be due to small sample sizes rather than an ineffective intervention.
Five of the six effective interventions incorporated the use of nutrition education. Importantly, all nutrition education interventions were interactive for children and improved FV intake even if children were not instructed to consume FVs; merely the knowledge of the importance of FVs led to increases in consumption. These findings are in line with similar reviews that found that interventions related to “experiential learning” of nutritional concepts and healthy eating were highly effective at improving FV preference and intake in young children, compared to those relying on parental involvement or contingent reinforcement [59], and especially if they contain multiple components or strategies [60, 61].
Repeated exposure was used alongside nutrition education in two interventions, both of which were effective at improving FV intake. The use of repeated exposure to achieve behavior change stems from the Theory of Mere Exposure [62], which predicts that repeatedly exposing children to certain things, including eating healthy foods, will make them more likely to engage in that behavior in the future [63, 64]. What this theory fails to account for is that dietary behaviors are not dictated solely by liking of foods. Rather, they are driven by the complex interaction of food preferences, appetite, and external influences including, but not limited to, peer influence and pressure from a caregiver [65]. Unfortunately, as with nutrition education, no intervention in this review solely used repeated exposure, so it cannot be determined whether this intervention method is able to increase FV intake when utilized without additional components.
Based on our narrative synthesis, changing the feeding environment was not consistently effective. The only manipulation of the feeding environment that was effective at improving fruit, but not vegetable, intake was serving FV five minutes before the rest of the meal [50]. Conversely, neither providing pre-portioned meals [50], nor providing FVs for children to take home were able to improve FV intake [56]. This suggests that the low FV intake amongst preschoolers is likely not improved solely by making them more available; rather, as suggested by these findings, an additional component, such as nutrition education, may be required to improve intake [56]. In summary, these findings support the notion that many different forms of FV interventions may be effective at improving intake in preschoolers, although additional research is needed to confirm the findings.
The observation that studies with no significant improvement in FV intake used fewer BCTs is similar to the findings of other reviews evaluating BCTs and obesity-related behaviors in children [42, 66]. The BCTs used in the studies that effectively improved FV intake are similar with those reported in the review by Hendrie et al. [42]. We also observed the use of the “Framing/reframing” BCT within effective studies in this review, possibly due to different age groups (preschoolers versus all children) or the use of different versions of the BCT taxonomy. Finally, while “Restructuring the physical environment” and “Adding objects to the environment” were used in studies that both did and did not observe improvements in FV intake, the studies that exclusively used one or both of these BCTs observed no increase in FV intake, suggesting that using these two BCTs alone or in tandem is insufficient and that solely manipulating the food environment should be used with caution. Overall, our findings suggest both that no single BCT or domain must be included and no single BCT identified will certainly lead to observed improvements in FV intake in preschoolers.
The lack of association between the use of theory within interventions and their effectiveness is in line with the findings of some reviews [67,68,69], but opposed the findings of other reviews [70, 71]. The differences observed in the Use of Theory scores between studies likely lie in the expertise of the researchers publishing the data; the researchers with psychological backgrounds will likely be more inclined to base interventions on theory, whereas those primarily in the dietetics or physiology field may not. Regardless, most intervention studies inherently target constructs of behavioral theories, even if they are not explicitly linked, evidenced by the use of similar methods. Hence, although interventions may have been informed by theory, the authors may not have explicitly reported the theory used, and therefore received a lower Use of Theory score. Amongst the included studies, Social Cognitive Theory was the most commonly mentioned theory, in line with a similar review of obesity-preventing interventions in children [72]. Nonetheless, although rarely practiced, designing a behavior change intervention that is comprehensively informed by behavior change theory is agreed on to be a valuable factor in designing interventions aimed at changing behavior [38, 67, 68, 70].
This review differs from similar reviews in the number of included studies. This is primarily due to its narrow inclusion criteria for studies; we only included RCTs that objectively measured FV intake and were conducted in the US. This distinction was intentional to highlight the need for objectively measured outcomes in evaluating dietary interventions [18, 19]. Importantly, the findings of this review pertain only to studies in the US and may not be generalizable to other countries. The small number of studies fulfilling the inclusion criteria, and the heterogeneity in measured outcomes, precluded this review from meta-analysis. Heterogeneity in effect sizes was likely partially due to the difference in the selected outcome measures; the two largest effect sizes were observed in studies that measured skin carotenoid levels [55], and the third study measured grams of vegetable intake of a snack of bell peppers and cheerios [56]. The remainder of the studies measured pieces of FV [53] or grams [54] of FVs consumed during lunch or percent of FVs consumed (of total amount served) during lunch [57]. Hence, comparison of the effect sizes in these studies should be conducted with caution. Another consequence of a limited number of studies is the lack of inferential testing of the role of theory and BCT. As observed in larger reviews that were able to empirically test the role of theory and BCTs, this information is valuable to understanding children’s eating behavior in the US. Additionally, the evaluation of theory and BCT use is limited by the use of only published materials; authors were not contacted for additional information regarding their use of theoretical frameworks and the relevant constructs. Finally, while this review aimed to examine the cost-effectiveness of included studies, no studies provided this information. These limitations should be considered within the strengths of this systematic review, including the inclusion of only study designs that objectively measure the effects of interventions within a very specific setting and population. Importantly, this review highlights the need for further research in this field to allow for a more pragmatic evaluation in future reviews.
Implications for future research
In addition to the need for future studies to address the limitations of this systematic review, the reviewed FV interventions and studies also highlight several opportunities for future research. Firstly, although it was not one of our primary outcomes, we found that only one study included an acclimation period to familiarize children with the research staff, methods, and changes to the eating environment. The lack of run-in time in the remaining studies may have increased the risk of the Hawthorne and placebo effects, which suggest that behavior may be altered due to the knowledge of being observed [73], particularly in studies that were implemented by unfamiliar researchers. To overcome this limitation, future studies should include an acclimation period to introduce researchers to the children and establish familiarity with equipment and methods, unless FV intake data is collected covertly. This suggestion may also mitigate any changes in eating behavior caused by the novelty of certain FVs or just novelty of being part of an intervention. Similar to studies in adults, children may be more inclined to consume FVs immediately following a nutrition education intervention on the benefits of FVs or have experienced associative conditioning from characters or books [74]. There is also need for studies with longer-term outcome measurements (ie. follow-up) to evaluate whether an intervention effect is sustainable beyond the time of direct exposure [53, 75], a critical component of all public health improvement [76]. Only two of the identified studies in this review included a follow-up period (one week and three months) [52, 53], thus, it is unknown whether the reported short-term changes in eating behavior continued [76]. This is an important aspect because only behavior changes that are maintained over time and after the children have returned to their usual environment are meaningful contributors to the effort to improve children’s diet quality. Future studies should also consider different levels of FV influence across the socioecological model (e.g. peers, family members) and potential moderators of FV intake (e.g. race, SES) to provide a more comprehensive understanding of FV intake behaviors [40, 77,78,79]. It is also important to consider study feasibility, acceptability, and risk of unintended impacts on children, staff, or families [80, 81], as only four of the included studies reported these effects [55, 82,83,84]. Evaluation of these effects in future studies may elucidate the factors associated with these undesirable or unintended effects to mitigate their impact.
Future research may also benefit from using a factorial study design that compares both different intervention components and different BCTs. These BCTs should also be placed in various contexts, such as within different intervention components, to ascertain whether the BCT or the intervention component is at play, and in heterogenous populations to explore whether different populations, or different characteristics, may respond differently to BCTs or intervention components.
Conclusion
In conclusion, this systematic review highlights the existing evidence on RCT interventions implemented in preschools and childcare centers to improve FV intake in preschool-age children in the United States. Although only nine interventions were identified, the most consistent evidence observed is that inclusion of nutrition education components were consistently effective at improving FV intake. Studies that manipulated the feeding environment, by providing pre-portioned meals at preschool or sent FVs for children to take home, but did not directly educate children, produced inconsistent results including decreases in FV intake. Further, there was no observable pattern between the use of theoretical frameworks or BCTs and effectiveness of the studies. While several studies have shown promising results, this review highlights key gaps in this field: there is a need for more studies to test FV interventions in US childcare settings that 1) use robust designs, such as RCTs that use objective measures of dietary intake, 2) directly compare intervention components and BCTs using a factorial model, 3) explicitly report their use of theoretical frameworks, and 4) include follow-up measures to assess long-term behavior change, to determine the most effective methods to reduce the deficiency in FV intake amongst young children in the United States.
Availability of data and materials
Not applicable.
Abbreviations
- FV:
-
Fruit and vegetable
- US:
-
United States
- BCT:
-
Behavior change technique
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT:
-
Randomized controlled trial
- ICC:
-
Intraclass correlation coefficient
- SCT:
-
Social Cognitive Theory
- CACFP:
-
Child and Adult Care Food Program
References
Wachs TD, Georgieff M, Cusick S, McEwen BS. Issues in the timing of integrated early interventions: contributions from nutrition, neuroscience, and psychological research. Ann N Y Acad Sci. 2014;1308:89–106.
Prynne CJ, Mishra GD, O’Connell MA, Muniz G, Laskey MA, Yan L, et al. Fruit and vegetable intakes and bone mineral status: a cross sectional study in 5 age and sex cohorts. Am J Clin Nutr. 2006;83(6):1420–8.
Maynard M, Gunnell D, Emmett P, Frankel S, Davey SG. Fruit, vegetables, and antioxidants in childhood and risk of adult cancer: the Boyd Orr cohort. J Epidemiol Community Health. 2003;57(3):218–25.
Lioret S, Campbell KJ, McNaughton SA, Cameron AJ, Salmon J, Abbott G, et al. Lifestyle patterns begin in early childhood, persist and are socioeconomically patterned, confirming the importance of early life interventions. Nutrients. 2020;12(3):724.
Singer MR, Moore LL, Garrahie EJ, Ellison RC. The tracking of nutrient intake in young children: the Framingham Children’s Study. Am J Public Health. 1995;85(12):1673–7.
Control CfD, Prevention. Children eating more fruit, but fruit and vegetable intake still too low. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services. 2014.
Services UDoHaH. 2020–2025 Dietary Guidelines for Americans. In: Agriculture UDo, editor. 9 ed. Washington, DC: US Dept of Health and Human Services; 2020.
Albani V, Butler LT, Traill WB, Kennedy OB. Fruit and vegetable intake: change with age across childhood and adolescence. Br J Nutr. 2017;117(5):759–65.
Demory-Luce D, Morales M, Nicklas T, Baranowski T, Zakeri I, Berenson G. Changes in food group consumption patterns from childhood to young adulthood: the Bogalusa Heart Study. J Am Diet Assoc. 2004;104(11):1684–91.
Magarey A, Mauch C, Mallan K, Perry R, Elovaris R, Meedeniya J, et al. Child dietary and eating behavior outcomes up to 3.5 years after an early feeding intervention: The NOURISH RCT. Obesity (Silver Spring). 2016;24(7):1537–45.
Livingstone M, Robson P. Measurement of dietary intake in children. Proceedings of the Nutrition Society. 2000;59(2):279–93.
Livingstone MB, Robson PJ, Wallace JM. Issues in dietary intake assessment of children and adolescents. Br J Nutr. 2004;92(Suppl 2):S213–22.
Foster E, Bradley J. Methodological considerations and future insights for 24-hour dietary recall assessment in children. Nutr Res. 2018;51:1–11.
Treiber FA, Leonard SB, Frank G, Musante L, Davis H, Strong WB, et al. Dietary assessment instruments for preschool children: reliability of parental responses to the 24-hour recall and a food frequency questionnaire. J Am Diet Assoc. 1990;90(6):814–20.
Pérez Rodrigo C, Aranceta J, Salvador G, Varela-Moreiras G. Food frequency questionnaires. Nutr Hosp. 2015;31(Suppl 3):49–56.
Livingstone MB, Prentice AM, Coward WA, Strain JJ, Black AE, Davies PS, et al. Validation of estimates of energy intake by weighed dietary record and diet history in children and adolescents. Am J Clin Nutr. 1992;56(1):29–35.
Wallace A, Kirkpatrick SI, Darlington G, Haines J. Accuracy of parental reporting of Preschoolers' dietary intake using an online self-administered 24-h recall. Nutrients. 2018;10(8):987.
Wilson AM, Lewis RD. Disagreement of energy and macronutrient intakes estimated from a food frequency questionnaire and 3-day diet record in girls 4 to 9 years of age. J Am Diet Assoc. 2004;104(3):373–8.
Linneman C, Hessler K, Nanney S, Steger-May K, Huynh A, Haire-Joshu D. Parents are accurate reporters of their preschoolers’ fruit and vegetable consumption under limited conditions. J Nutr Educ Behav. 2004;36(6):305–8.
Burrows TL, Martin RJ, Collins CE. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labeled water. J Am Diet Assoc. 2010;110(10):1501–10.
Xu Y, Duan R, Feng P, Gao W, Xing D, Cheng G. Comparison of the diet photograph record to weighed dietary record and 24 h dietary recall for estimating energy and nutrient intakes among Chinese preschoolers. Front Nutr. 2021;8: 755683.
Aguilar SS, Wengreen HJ, Lefevre M, Madden GJ, Gast J. Skin carotenoids: a biomarker of fruit and vegetable intake in children. J Acad Nutr Diet. 2014;114(8):1174–80.
Nguyen LM, Scherr RE, Linnell JD, Ermakov IV, Gellermann W, Jahns L, et al. Evaluating the relationship between plasma and skin carotenoids and reported dietary intake in elementary school children to assess fruit and vegetable intake. Arch Biochem Biophys. 2015;572:73–80.
Seguin-Fowler RA, Hanson KL, Marshall GA, Belarmino EH, Jilcott Pitts SB, Kolodinsky J, et al. Fruit and vegetable intake assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, is associated with skin carotenoid measurements in children. Nutrients. 2021;13(3):980.
Jahns L, Johnson LK, Conrad Z, Bukowski M, Raatz SK, Jilcott Pitts S, et al. Concurrent validity of skin carotenoid status as a concentration biomarker of vegetable and fruit intake compared to multiple 24-h recalls and plasma carotenoid concentrations across one year: a cohort study. Nutr J. 2019;18(1):78.
Jahns L, Johnson LK, Mayne ST, Cartmel B, Picklo MJ Sr, Ermakov IV, et al. Skin and plasma carotenoid response to a provided intervention diet high in vegetables and fruit: uptake and depletion kinetics. Am J Clin Nutr. 2014;100(3):930–7.
Tsuruoka H, Khovidhunkit W, Brown BE, Fluhr JW, Elias PM, Feingold KR. Scavenger receptor class B type I is expressed in cultured keratinocytes and epidermis. Regulation in response to changes in cholesterol homeostasis and barrier requirements. J Biol Chem. 2002;277(4):2916–22.
Scarmo S, Henebery K, Peracchio H, Cartmel B, Lin H, Ermakov IV, et al. Skin carotenoid status measured by resonance Raman spectroscopy as a biomarker of fruit and vegetable intake in preschool children. Eur J Clin Nutr. 2012;66(5):555–60.
Mayne ST, Cartmel B, Scarmo S, Jahns L, Ermakov IV, Gellermann W. Resonance Raman spectroscopic evaluation of skin carotenoids as a biomarker of carotenoid status for human studies. Arch Biochem Biophys. 2013;539(2):163–70.
Cui J, Natzke L. Early Childhood Program Participation: 2019. First Look. NCES 2020–075. National center for education statistics. 2020.
Hasnin S, Saltzman JA, Dev DA. Correlates of children’s dietary intake in childcare settings: a systematic review. Nutr Rev. 2022;80(5):1247–73.
Larson N, Ward DS, Neelon SB, Story M. What role can child-care settings play in obesity prevention? A review of the evidence and call for research efforts. J Am Diet Assoc. 2011;111(9):1343–62.
Stacey FG, Finch M, Wolfenden L, Grady A, Jessop K, Wedesweiler T, et al. Evidence of the potential effectiveness of centre-based childcare policies and practices on child diet and physical activity: Consolidating evidence from systematic reviews of intervention trials and observational studies. Current Nutrition Reports. 2017;6:228–46.
Nicklas TA, Baranowski T, Baranowski JC, Cullen K, Rittenberry L, Olvera N. Family and child-care provider influences on preschool children’s fruit, juice, and vegetable consumption. Nutr Rev. 2001;59(7):224–35.
Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27(3):379–87.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95.
Michie S, Wood CE, Johnston M, Abraham C, Francis JJ, Hardeman W. Behaviour change techniques: the development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol Assess. 2015;19(99):1–188.
Michie S, Prestwich A. Are interventions theory-based? Development of a theory coding scheme. Health Psychol. 2010;29(1):1–8.
Webb TL, Joseph J, Yardley L, Michie S. Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res. 2010;12(1): e4.
Hodder RK, O'Brien KM, Stacey FG, Wyse RJ, Clinton-McHarg T, Tzelepis F, et al. Interventions for increasing fruit and vegetable consumption in children aged five years and under. Cochrane Database Syst Rev. 2018;5(5):Cd008552.
Matwiejczyk L, Mehta K, Scott J, Tonkin E, Coveney J. Characteristics of effective interventions promoting healthy eating for Pre-Schoolers in Childcare Settings: an umbrella review. Nutrients. 2018;10(3):293.
Hendrie GA, Brindal E, Corsini N, Gardner C, Baird D, Golley RK. Combined home and school obesity prevention interventions for children: what behavior change strategies and intervention characteristics are associated with effectiveness? Health Educ Behav. 2012;39(2):159–71.
Hendrie GA, Lease HJ, Bowen J, Baird DL, Cox DN. Strategies to increase children's vegetable intake in home and community settings: a systematic review of literature. Matern Child Nutr. 2017;13(1):e12276.
Service UKNH. The Eatwell Guide: NHS; 2022. [updated 2022 Nov 29; cited 2023 Apr 10]. Available from: www.nhs.uk/live-well/eat-well/food-guidelines-and-food-labels/the-eatwell-guide/.
Hausner H, Olsen A, Møller P. Mere exposure and flavour-flavour learning increase 2–3 year-old children’s acceptance of a novel vegetable. Appetite. 2012;58(3):1152–9.
Cravener TL, Schlechter H, Loeb KL, Radnitz C, Schwartz M, Zucker N, et al. Feeding strategies derived from behavioral economics and psychology can increase vegetable intake in children as part of a home-based intervention: results of a pilot study. J Acad Nutr Diet. 2015;115(11):1798–807.
Adams JB, Audhya T, Geis E, Gehn E, Fimbres V, Pollard EL, et al. Comprehensive nutritional and dietary intervention for autism spectrum disorder-a randomized, controlled 12-month trial. Nutrients. 2018;10(3):369.
Cermak SA, Curtin C, Bandini LG. Food selectivity and sensory sensitivity in children with autism spectrum disorders. J Am Diet Assoc. 2010;110(2):238–46.
Chistol LT, Bandini LG, Must A, Phillips S, Cermak SA, Curtin C. Sensory sensitivity and food selectivity in children with autism spectrum disorder. J Autism Dev Disord. 2018;48(2):583–91.
Harnack LJ, Oakes JM, French SA, Rydell SA, Farah FM, Taylor GL. Results from an experimental trial at a Head Start center to evaluate two meal service approaches to increase fruit and vegetable intake of preschool aged children. Int J Behav Nutr Phys Act. 2012;9:51.
Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Assessing risk of bias in a randomized trial. Cochrane handbook for systematic reviews of interventions. 2019:205–28.
Staiano AE, Marker AM, Frelier JM, Hsia DS, Martin CK. Influence of screen-based peer modeling on preschool children’s vegetable consumption and preferences. J Nutr Educ Behav. 2016;48(5):331-5.e1.
Witt KE, Dunn C. Increasing fruit and vegetable consumption among preschoolers: evaluation of color me healthy. J Nutr Educ Behav. 2012;44(2):107–13.
Gripshover SJ, Markman EM. Teaching young children a theory of nutrition: conceptual change and the potential for increased vegetable consumption. Psychol Sci. 2013;24(8):1541–53.
Nicklas T, Lopez S, Liu Y, Saab R, Reiher R. Motivational theater to increase consumption of vegetable dishes by preschool children. Int J Behav Nutr Phys Act. 2017;14(1):16.
Smith E, Sutarso T, Kaye GL. Access with education improves fruit and vegetable intake in preschool children. J Nutr Educ Behav. 2020;52(2):145–51.
Izumi BT, Eckhardt CL, Hallman JA, Herro K, Barberis DA. Harvest for healthy kids pilot study: associations between exposure to a Farm-to-Preschool intervention and willingness to try and liking of target fruits and vegetables among low-income children in head start. J Acad Nutr Diet. 2015;115(12):2003–13.
Dunn C, Thomas C, Pegram L, Ward D, Schmal S. Color me healthy, preschoolers moving and eating healthfully. J Nutr Educ Behav. 2004;36(6):327–8.
Dudley DA, Cotton WG, Peralta LR. Teaching approaches and strategies that promote healthy eating in primary school children: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2015;12:28.
Charlton K, Comerford T, Deavin N, Walton K. Characteristics of successful primary school-based experiential nutrition programmes: a systematic literature review. Public Health Nutr. 2021;24(14):4642–62.
Varman SD, Cliff DP, Jones RA, Hammersley ML, Zhang Z, Charlton K, et al. Experiential learning interventions and healthy eating outcomes in children: a systematic literature review. Int J Environ Res Public Health. 2021;18(20):10824.
Birch LL, Marlin DW. I don’t like it; I never tried it: effects of exposure on two-year-old children’s food preferences. Appetite. 1982;3(4):353–60.
Cooke L. The importance of exposure for healthy eating in childhood: a review. J Hum Nutr Diet. 2007;20(4):294–301.
de Wild VW, de Graaf C, Jager G. Effectiveness of flavour nutrient learning and mere exposure as mechanisms to increase toddler’s intake and preference for green vegetables. Appetite. 2013;64:89–96.
DeCosta P, Møller P, Frøst MB, Olsen A. Changing children’s eating behaviour - A review of experimental research. Appetite. 2017;113:327–57.
Anselma M, Chinapaw MJM, Kornet-van der Aa DA, Altenburg TM. Effectiveness and promising behavior change techniques of interventions targeting energy balance related behaviors in children from lower socioeconomic environments: a systematic review. PLoS One. 2020;15(9):e0237969.
Prestwich A, Sniehotta FF, Whittington C, Dombrowski SU, Rogers L, Michie S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014;33(5):465–74.
Sediva H, Cartwright T, Robertson C, Deb SK. Behavior change techniques in digital health interventions for Midlife Women: systematic review. JMIR Mhealth Uhealth. 2022;10(11): e37234.
An RP, Li DY, Xiang XL. Role of theories in school-based diabetes care interventions: a critical review. World J Clin Cases. 2021;9(18):4709–20.
Armaou M, Araviaki E, Dutta S, Konstantinidis S, Blake H. Effectiveness of digital interventions for deficit-oriented and asset-oriented psychological outcomes in the workplace: a systematic review and narrative synthesis. Eur J Investig Health Psychol Educ. 2022;12(10):1471–97.
Liu MG, Davis GM, Kilbreath SL, Yee J. Physical activity interventions using behaviour change theories for women with breast cancer: a systematic review and meta-analysis. J Cancer Survivor. 2022;16(5):1127–48.
Waters E, de Silva-Sanigorski A, Hall BJ, Brown T, Campbell KJ, Gao Y, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2011(12):Cd001871.
Sedgwick P, Greenwood N. Understanding the Hawthorne effect. BMJ. 2015;351: h4672.
Gniß S, Kappesser J, Hermann C. Placebo effect in children: the role of expectation and learning. Pain. 2020;161(6):1191–201.
Klesges LM, Dzewaltowski DA, Glasgow RE. Review of external validity reporting in childhood obesity prevention research. Am J Prev Med. 2008;34(3):216–23.
Kopelman P, Jebb SA, Butland B. Executive summary: foresight “Tackling obesities: Future choices” project. Obes Rev. 2007;8(Suppl 1):vi–ix.
de Jong E, Visscher TL, HiraSing RA, Seidell JC, Renders CM. Home environmental determinants of children’s fruit and vegetable consumption across different SES backgrounds. Pediatr Obes. 2015;10(2):134–40.
Lioret S, Campbell KJ, McNaughton SA, Cameron AJ, Salmon J, Abbott G, et al. Lifestyle patterns begin in early childhood, persist and are socioeconomically patterned, confirming the importance of early life interventions. Nutrients. 2020;12(3):724.
Wolfenden L, Barnes C, Jones J, Finch M, Wyse RJ, Kingsland M, et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst Rev. 2020;2(2):Cd011779.
John J. Economic perspectives on pediatric obesity: impact on health care expenditures and cost-effectiveness of preventive interventions. Nestle Nutr Workshop Ser Pediatr Program. 2010;66:111–24.
Bowen DJ, Kreuter M, Spring B, Cofta-Woerpel L, Linnan L, Weiner D, et al. How we design feasibility studies. Am J Prev Med. 2009;36(5):452–7.
Cepni AB, Taylor A, Crumbley C, Thompson D, Moran NE, Olvera N, et al. Feasibility and efficacy of the “FUNPALs Playgroup” intervention to improve toddler dietary and activity behaviors: a pilot randomized controlled trial. Int J Environ Res Public Health. 2021;18(15):7828.
Kong A, Buscemi J, Stolley MR, Schiffer LA, Kim Y, Braunschweig CL, et al. Hip-Hop to Health Jr. Randomized effectiveness trial: 1-year follow-up results. Am J Prev Med. 2016;50(2):136–44.
Galloway AT, Fiorito LM, Francis LA, Birch LL. “Finish your soup”: counterproductive effects of pressuring children to eat on intake and affect. Appetite. 2006;46(3):318–23.
Acknowledgements
We acknowledge the help of librarian Kate Joshua for helping to develop the search terms and criteria used to obtain articles for this review.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
FH and SK developed this study. FH defined the search terms, conducted the literature search, reviewed the studies, extracted data, coded articles according to the BCT and Use of Theory coding schemes, and drafted the manuscript, under supervision of SK. AVN reviewed the studies, extracted data, assessed studies for risk of bias, and coded articles according to the BCT coding schemes. ARR extracted data and coded articles according to the BCT coding schemes. JZ and SK contributed to the development of the inclusion and exclusion criteria. JZ encouraged the evaluation of BCTs and use of theory in this review and supervised the findings of this work. AJN aided in development of the search terms and interpreting the findings related to use of BCTs and use of theoretical frameworks. WY aided in the development of the data extraction form and interpretation of the findings. DS and JZ contributed to the interpretation and implication of the findings. SK, DS, AJN and WY contributed significant intellectual content and substantially contributed to the conception of this review, design of the review, and revisions to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hasan, F., Nguyen, A.V., Reynolds, A.R. et al. Preschool- and childcare center-based interventions to increase fruit and vegetable intake in preschool children in the United States: a systematic review of effectiveness and behavior change techniques. Int J Behav Nutr Phys Act 20, 66 (2023). https://doi.org/10.1186/s12966-023-01472-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-023-01472-8