
Abstract
Background
Healthy eating by primary school-aged children is important for good health and development. Schools can play an important role in the education and promotion of healthy eating among children. The aim of this review was to: 1) perform a systematic review of randomised controlled, quasi-experimental and cluster controlled trials examining the school-based teaching interventions that improve the eating habits of primary school children; and 2) perform a meta-analysis to determine the effect of those interventions.
Methods
The systematic review was limited to four healthy eating outcomes: reduced food consumption or energy intake; increased fruit and vegetable consumption or preference; reduced sugar consumption or preference (not from whole fruit); increased nutritional knowledge. In March 2014, we searched seven electronic databases using predefined keywords for intervention studies that were conducted in primary schools which focused on the four healthy eating outcomes. Targeted internet searching using Google Scholar was also used. In excess of 200,000 possible citations were identified. Abstracts and full text of articles of potentially relevant papers were screened to determine eligibility. Data pertaining to teaching strategies that reported on healthy eating outcomes for primary school children was extracted from the 49 eligible papers.
Results
Experiential learning strategies were associated with the largest effects across the reduced food consumption or energy intake; increased fruit and vegetable consumption or preference; and increased nutritional knowledge outcomes. Reducing sugar consumption and preference was most influenced by cross-curricular approaches embedded in the interventions.
Conclusions
As with most educational interventions, most of the teaching strategies extracted from the intervention studies led to positive changes in primary school children’s healthy eating behaviours. However, given the finite resources, increased overcrowding of school curriculum and capacity of teachers in primary schools, a meta-analysis of this scope is able to provide stakeholders with the best evidence of where these resources should be focused.
Similar content being viewed by others

Introduction
Rationale
The Australian National Health and Medical Research Council (2013) [1] states that optimum nutrition is essential for the healthy growth and development of children. Healthy eating contributes to achieving and maintaining a healthy weight, and provides protection against chronic disease and premature mortality. Conversely, unhealthy eating early in life, in particular the over-consumption of energy-dense, nutrient-poor foods and drinks, as well as physical inactivity and a sedentary lifestyle, are predictors of overweight and obesity [2,3]. There is good evidence that many other non-communicable diseases (such as diabetes, osteoporosis, and hypertension) are also related to unhealthy eating habits and patterns formed during childhood [4]. As such, it is important to establish healthy eating behaviours early, as evidence shows that eating habits and patterns track into adulthood [5,6]. Therefore, childhood is a period where education about healthy eating is essential for establishing healthy eating practices in later years. Schools have been a popular setting for the implementation of health promotion and prevention interventions, as they offer continuous, intensive contact with children and that lifelong health and wellbeing begins with promoting healthy behaviours early in life [7]. School infrastructure, physical environment, policies, curricula, teaching and learning, and staff all have the potential to positively influence child health. Whilst schools have remained a popular infrastructure for health promotion initiatives, teachers will remain the key agent of promoting health and nutrition within schools post-2015 [8]. No systematic review or meta-analysis have been undertaken to date which ascertain the strategies teachers should employ in order to yield maximum effect from their teaching interventions when it comes to fostering healthy eating behaviours in primary school-aged children.
Objectives
Our aim was to systematically review the evidence related to interventions designed to improve healthy eating habits and patterns of primary school students. Our objectives were to: 1) describe the nature of the interventions that had been conducted (i.e., theories and teaching strategies and approaches); and 2) conduct meta-analyses to determine the effectiveness of these interventions.
Methods
Design
This systematic review and meta-analyses report on data extracted and synthesised in 2014 as part of a review project undertaken for the New South Wales (NSW) Department of Education and Communities and the NSW Ministry of Health. The PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) Statement [9] was followed to ensure the transparent reporting of the study.
Eligibility criteria
Interventions types
We included teaching and school-based elementary school interventions delivered by teachers or teacher substitutes that sought to bring about positive nutritional consumption, preference or knowledge change in elementary school children. The following types of teaching and school-based interventions included:
-
1.
Curriculum initiatives or evaluations
-
2.
Nutrition-friendly school initiatives
-
3.
Community programs linked to curricula or delivered by schools (e.g. community gardens)
-
4.
Health/nutrition education programs related to improving dietary habits
-
5.
Environmental school change strategies implemented by classroom teachers
-
6.
Environmental interventions/industry partnerships focused on point-of-purchase consumption linked through classroom based education; this might include campaigns to draw attention to healthier products in school canteens or school lunch choices
-
7.
Social marketing campaigns
-
8.
Policies that seek to improve dietary habits of elementary school children (i.e. school board level, provincial/national level).
Acceptable designs for this review included randomised, quasi-experimental and cluster controlled studies conducted in elementary schools (Grades K-6) whereby the primary change agent in the intervention was the classroom teacher (or their teaching substitute). Relevant clusters within studies included individual students, classrooms, schools or communities as the unit of analysis.
Locations
Intervention locations had to include elementary schools and/or their immediate community settings. We excluded programs or strategies delivered solely through homes, religious institutions other than schools, non-governmental organisations, primary health care settings, universities, hospitals, outpatient clinics located within hospital settings, commercial programs and metabolic or weight loss clinics.
Outcomes of interest (Healthy eating behaviours)
Our primary outcomes included student consumption, preference and knowledge of nutrient dense foods. Evidence of intervention effects included measures at individual, family, school or community levels. They also included measures of food consumption, preference or knowledge and change in food environments, food disappearance, and food sales (in school cafeterias). Measures of consumption included: diet and food intake records, self-reported and/or reported by parents, teachers or both; food frequency questionnaires/balance sheets; food wastage and plate waste; and micronutrient measures (i.e., biomarkers of exposure to food). Measures of preference included: questionnaires, surveys or self-report instruments that included Likert scales, pairing activities, or self-reported preferences. Measures of knowledge included: questionnaires or tests on food-related knowledge (i.e., Recommended Dietary Intakes, ingredients, nutritional knowledge).
These primary outcomes were then grouped into four dominant healthy eating outcomes that the authors determined aligned with the National Health and Medical Research Council (NHMRC) and their Healthy Eating for Children [10] Guidelines. Our outcomes were therefore;
-
1.
Food Consumption and Energy Intake–NHMRC Guideline 1 (Limiting energy intake to meet energy needs)
-
2.
Fruit and Vegetable (FV) Consumption or Preference–NHMRC Guideline 2 (Enjoy a wide variety of nutritious foods)
-
3.
Reduced Sugar Consumption or Preference (Not from whole fruit)–NHMRC Guideline 3 (Limit intake of foods containing added sugar)
-
4.
Nutritional Knowledge–NHMRC Guideline 5 (Care for food)
Note: The instruments used and the number studies included in the review and meta-analysis did not allow for segregation of consumption and preference of fruit and vegetables or sugar. We acknowledge that preference for certain food types may have a greater affect on long-term consumption habits.
Outcomes of interest (Teaching strategies)
The primary outcomes of interest included any recognised teaching strategy or articulated approach to teaching that has a known effect on student learning and behaviour. The categorisation for these teaching strategies and approaches to curricula were largely derived from (but not limited to) those articulated in Hattie’s synthesis of meta-analysis relating to teaching, learning and student achievement [11].
Search
Our search strategy included: electronic bibliographic databases; grey literature databases; reference lists of key articles; targeted internet searching via Google Scholar; and targeted internet searching of key organisation websites.
We searched the following databases, adapting search terms according to the requirements of individual databases in terms of subject heading terminology and syntax: PUBMED; MEDLINE; the Cochrane Central Register of Controlled Trials (CENTRAL); PsycINFO; ERIC; ScienceDirect; and A + Education. These search terms were based on; 1) participants (e.g. child* OR young people OR youth OR pediatric OR paediatric OR primary school-age* OR elementary school-age* OR primary student* OR elementary student* OR primary school* OR elementary school*); 2) delivery (e.g. teach* OR class* OR health* ed* teach* OR learn* OR teach* polic* OR nutrition ed* OR health* eat*); 3) strategies (e.g. phys* edu* OR health* edu* OR curricul* OR outdoor* OR cook* OR food* OR fruit* OR veg* OR know* OR test*); 4) design (e.g. RCT OR randomi* OR control* OR trial* OR evaluat* OR quasi-exper* OR cluster*). The dates range for search were from database inception to 31st May, 2014.
The search results were then refined to include the full text copies retrieved from these databases and Google Scholar that were published after 1970. These citations were then cross-referenced electronically with 15 reference lists from scoping and systematic review papers in the field of nutrition, education, and health promotion published between 1997 and 2012. A final database and internet search was then conducted to identify studies published between January 2010 (year prior to publication of most recent systematic review) and May 2014.
Screening of citations
Initially duplicate citations were removed from the search by the lead author. The abstract of each citation was then reviewed by a single researcher (DAD) to determine whether it would be included in the systematic review. The full-text articles of all potentially relevant citations were obtained and saved as Adobe-PDF files. Whenever it was uncertain as to whether a citation was appropriate, the full-text copy was obtained. The lead author then screened the citation list. Citations that were deemed ineligible were reviewed by the remaining two authors (WGC, LRP) to determine if any potentially relevant citations were missed, and full-text copies of these citations were then obtained.
Study selection
Following the screening process, full-text articles were then reviewed by the three researchers against the inclusion criteria; if uncertain as whether or not to include an article, the article in question was reviewed again until a final decision was made by majority consensus.
Data extraction
Data was initially extracted from the included studies by the lead researcher from full-text articles and placed in tabulated form (see Table 1). This data included:
-
1.
Study authors;
-
2.
Year of publication;
-
3.
Country (s) of study;
-
4.
Funding agency of study;
-
5.
Study design;
-
6.
Dominant Theoretical Framework used to inform study design
-
7.
Study sample (Size, Grade, Mean age of participants);
-
8.
Intervention length;
-
9.
Whether the intervention was coupled with a physical activity or specially resourced teacher;
-
10.
Relevant outcome categories
-
11.
Statistical significance (p value/95%CI)
-
12.
The effect size of different teaching strategies on each outcome (Cohen’s d). Note: If these were not reported in the study and Mean and Standard Deviations could be extracted either directly or indirectly, the Cohen’s d was calculated by the lead researcher and verified by the co-authors.
These data were tabulated by the lead author and shared with co-authors for feedback and review. Changes to these interpretations were decided by majority consensus by all three researchers.
The three researchers then reviewed each of the articles independently and each identified the teaching approaches employed in the intervention phase of the studies. Researchers met and cross-referenced their identification of each teaching approach and decided though consensus how each approach would be classified as a wider teaching strategy (if appropriate) that would allow for comparison between studies.
Assessment of methodological quality
Included articles were also assessed for methodological quality using a 10-item quality assessment scale derived from van Sluijs and colleagues [12] (see Table 2). For each included article, three reviewers independently assessed whether the assessed item was present or if the assessed item was absent. Where an item was insufficiently described it was allocated an absent score. Agreement between reviewers for each article was set a priori at 80% [12]. That is, for each article, reviewers were required to agree that the items were either present or absent for 8 of the 10 items. In the case of less than 80% agreement, consensus was reached by further discussion. Results for the assessment of methodological quality are reported in Table 3.
Synthesis of results
Effect sizes are the preferred metric for estimating the magnitude of effect of an intervention because they make possible between study as well as within study comparisons [13]. Cohen’s d, the effect-size metric constituting the focus of this meta-analysis, is one of the most widely used measures of magnitude of effect and commonly used in educational meta-analyses [11]. The formula for calculating Cohen’s d is:
where M 1 is the mean of one group of study participants, M 2 is the mean of a second group of study participants, and SD P is the pooled standard deviation for both groups of study participants.
In instances where the groups have been given different learning experiences (e.g. an intervention), d is a measure of the magnitude of effect of the experience on the group receiving the enhanced teaching and learning experience. In cases where SD was not reported but SE (Standard Error) was, SE was converted to SD using the following formula:
As Cohen’s d accounts for sample size, mean effect sizes for the purposes of the meta-analysis were calculated as follows:
where
M d is the mean Cohen’s d calculated by the sum of all d values and divided by the number of studies (N s ) from which a d value could be extracted for that outcome.
Data pertaining to each study were initially collated and described in a narrative summary (see Table 1). To facilitate comparison between the effect of teaching strategies/approaches, studies were divided according to their outcome measure as follows: Decreased food consumption/energy intake, increased FV consumption/preference, decreased sugar consumption/preference, and increased nutritional knowledge. Meta-analyses were conducted using the standardised mean difference approach (Cohen’s d) regardless of their statistical significance where at least two studies existed for a particular outcome measure and sufficient statistical data were reported to allow such synthesis to occur.
Studies incorporated into the meta-analyses included a comparison between teaching strategies/approaches and reported post-test/follow-up values or change scores along with measures of distribution (i.e. mean and standard deviation). For studies that included post-test and follow-up assessments, the assessments completed at the end of the study period (i.e., follow-up) were included in the meta-analyses. The standardized effect sizes were interpreted as minimal (<.02), small (0.2), medium (0.5), and large (0.8) [14]. Analyses also considered whether they represented an effective investment in education given the average effect size of most educational interventions is d = 0.4 [11].
Results
Study selection
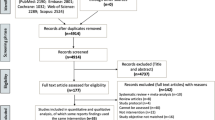
The study selection process is shown in Figure 1. It initially retrieved in excess of 200,000 possible citations. We refined searches to include only full text copies available online and published after 1970 in each of the databases and in Google Scholar reducing this to 18,100 possible citations. These citations were then cross-referenced electronically with reference lists from scoping and systematic review papers published in the field of nutrition, education, and health promotion (n = 15) [15-29] published between 1997 and 2012 that yielded 454 likely studies. A final database and internet search was then conducted to identify studies published between January 2010 (year prior to publication of most recent systematic review) and May 2014. This revealed an additional 23 possible citations totalling 487 publications that were considered for review.

Flowchart of study selection.
These 487 publications were then reviewed based on abstract and excluded if they were not conducted in primary schools or on primary school-aged children. This reduced the number of studies to 233. Studies were then excluded if they were not: a) randomised controlled trials; b) quasi-experimental studies; or c) cluster-controlled trials. This left 55 studies. On review of the full-text paper, another 6 studies were excluded for not meeting the inclusion criteria (i.e. conducted in a laboratory setting) or being a duplicate study. The final 49 studies were all in the form of peer-reviewed journal publications.
To ensure a complete review of the relevant literature is given, all 49 of the included articles are presented in Table 1. Specifically, the table outlines the details of the studies, including author(s), title, year, location, design and stated dominant theoretical framework, target population, and types of outcomes measured. The year of publication for included articles ranged from 1973 to 2011.
Study and intervention characteristics
The final 49 studies included one randomised controlled trial, 13 quasi-experiential studies and 35 cluster-controlled trials. These studies captured data from 38001 primary school children in 13 different countries. Data capable for inclusion in the meta-analyses came from 20234 (53%) participants. All but one country (Trinidad and Tobago) included in these studies were member nations of the Organization for Economic Co-operation and Development (OECD). Only 27 of the 49 studies reported the theoretical frameworks used to inform their intervention design. Whilst some studies reported multiple theoretical approaches (see Table 1), Social Cognitive Theory was the most frequently used theoretical framework and was reported in 16 of 27 studies.
Teaching strategies/approaches
There were eight dominant teaching strategies or approaches to teaching exhibited across the 49 studies that addressed the pre-determined areas of healthy eating for primary school students (i.e. food consumption/energy intake, fruit and vegetable consumption or preference, sugar consumption or preference, and nutritional knowledge). Some studies included more than one of these teaching strategies/approaches in their intervention group. The dominant teaching strategies/approaches were: 1) Enhanced curriculum approaches (i.e. speciality nutrition education programs beyond existing health curricula delivered by teachers or specialists) (n = 29); 2) cross-curricular approaches (i.e. nutrition education programs that were delivered across two or more traditional primary school subjects) (n = 11); 3) parental involvement (i.e. programs requiring active participation or assistance from a parent within or outside the school environment) (n = 10); 4) experiential learning approaches (i.e. school/community garden, cooking and food preparation activities) (n = 10); 5) contingent reinforcement approaches (i.e. rewards or incentives given to students in response to desired behaviours) (n = 7); 6) literary abstraction approaches (i.e. literature read by/to children whereby a character promotes/exemplifies positive behaviours) (n = 3); 7) games-based approaches (i.e. board/card games played by students at school designed to promote positive behaviour and learning of new knowledge) (n = 2); and 8) web-based approaches (i.e. internet-based resources or feedback mechanisms that could be accessed by students at home or school) (n = 2).
The results of the systematic review indicate that several dominant evidence-based approaches to teaching healthy eating in the randomised controlled trial, quasi-experimental and cluster controlled trial literature. In order to determine the strength of the evidence for these approaches, they are analysed against each of the major outcomes used to determine healthy eating and if the study achieved p-values of p < .05 for 50% of the studies, the magnitude of M d (i.e. minimal, small, medium, large) and/or if M d > .40. The decision to use an effect size of M d > .40 is based on Hattie’s Zone of Desired Effects reside above this hinge point [11] and therefore have the greatest influence and represent the best investment for improving educational outcomes.
Food consumption and energy intake
Eleven studies reported on outcomes of food consumption and the overall energy intake of primary school-aged children. Curriculum-based approaches were the most popular (seven studies) and reported achieving statistical significance of p < .05 or better across nine studies reducing food consumption or energy intake outcomes. However, researchers were able to calculate effect sizes across six of the reported outcomes and found that four showed minimal or no effect, one had a negative effect and one reported a small effect size. The mean effect size of curriculum-based approaches is minimal (M d = 0.12) and would suggest that curriculum-based approaches alone are not the best influence on reducing food consumption or energy intake.
Three studies utilising experiential learning approaches (i.e., school/community gardens, cooking lessons and food preparation) reported on outcomes associated with reducing food consumption and energy intake. Two of these studies reported achieving statistical significance of p < .05 or better for at least one food consumption or energy intake variable. Effect sizes could be calculated on three of the reported outcomes from two studies. Two large effect sizes were recorded and the other showed no effect. Whilst there were only a small number of effect sizes that were able to be calculated based on the reporting method in these studies, the mean effect size was M d = 1.31 and within the Zone of Desired Effects. These approaches warrant greater investigation to reduce the amount of variance in the calculated effect but show promise in their ability to reduce food consumption and energy intake.
Fruit and vegetable (FV) consumption or preference
In terms of FV consumption or preference, curriculum-based approaches were again the most popular. 60% of curriculum-based approaches found statistically significant (p < .05) improvements in FV consumption or preference among primary school-aged children. However, it is important to note that many of the studies that used curriculum-based approaches (especially those with stronger p values) also coupled their interventions with secondary approaches (e.g., experiential-learning, parental-involvement). Given the way in which data was reported in these studies, it is difficult at this stage to determine the degree to which curriculum-based approaches alone contributed to statistical significance.
Of the 30 effect sizes that were calculated by the researchers, 33% had a medium to large effect and a further 23% had a small effect size. The mean effect size for curriculum-based approaches was M d = 0.45 indicating that having a nutrition curriculum delivered in primary schools makes an important investment in improving FV consumption or preference based on the educational hinge-point of effect sizes described by Hattie [11]. All but one study that was included in the analysis appeared to be based on behavioural, mastery, or didactic approaches and curricula models. The study driven by a socio-cultural perspective of health [30] had only 33 participants and effect sizes ranging from-0.26 to 1.04 for a range of different FV consumption or preference behaviours.
Experiential-learning approaches were used in eight studies to improve FV consumption or preference in primary school children and proved to be very effective with 75% of these types of studies yielding statistical significance at p < .05 or better. Of the 11 effect sizes that were calculated by the researchers, 45% had a large effect and the remaining 55% had a minimal effect size. However, the mean effect size for experiential-learning approaches that included school/community gardens, cooking skills, or food preparation was M d = 0.68, indicating experiential-learning approaches were within the Zone of Desired Effects [11] for improving FV consumption or preference in primary school children.
Cross-curricular approaches (i.e., learning experiences taught across two or more learning areas/subjects) to improving FV consumption or preference in primary school children also proved to very effective. Of the 10 studies using cross-curricular approaches, 90% of these yield statistical significance at p < .05 or better and of the 6 effect sizes calculated by the researchers, 50% had large effect sizes and the remaining 50% had a small or medium effect size. Whilst there were only a small number of effect sizes that were able to be calculated based on the reporting method in these studies, the mean effect size was M d = 0.63, which was within the Zone of Desired Effects.
Four studies used a contingent reinforcement (i.e., reward for behaviour) approach in promotion of FV consumption or preference among primary school children. All four (100%) of these studies reported achieving statistical significance of at least p < .05. There were six effect sizes reported across only two studies [31,32] and four of these effect sizes (67%) were considered large and two (33%) were considered minimal. Based on these two studies, the average effect size for contingent reinforcement in promoting FV consumption or preference is M d = 1.34. More studies are needed in order to ascertain an average effect size with less variance, however, based on available data this approach is well above M d = 0.4 with strong statistical significance in every study indicates it is a worthwhile investment strategy in improving FV consumption or preference among primary school children.
Parental involvement was incorporated into 10 studies that reported against 23 FV consumption or preference outcomes in primary school children. 91% of the outcomes reported against were statistically significant at the p < .05 level. The researchers were able to calculate 14 effect sizes in five of the studies. The results were varied with three large, two medium, three small, two minimal and four negative effect sizes being calculated. The mean effect was M d = 0.39 that was just below the Zone of Desired effects however it is worthwhile noting that no parent involvement approach was ever ‘stand-alone’. They all included elements of enhanced curriculum, cross-curricular, experiential learning or web-based support.
Sugar consumption or preference (not from whole fruit)
Enhanced curriculum approaches (mainly based on behavioural or social cognitive theories) in primary schools provided 10 studies for reducing sugar consumption or preference in students however only three yielded statistical significance of p < .05 or better for reducing any sugar-laden beverage (SLB), fruit juice or carbohydrate consumption. Six effect sizes were calculated from these studies that showed one large, one small and four minimal effect sizes. The mean effect size of curriculum approaches for reducing sugar consumption however was only M d = 0.28 suggesting that greater investment beyond curriculum is required to make a substantial difference in reducing the sugar consumption of primary school children.
Cross-curricular approaches were reported in two studies [33,34] in reducing SLB or fruit juice consumption. Both studies reported statistically significant reductions in both SLB and fruit juice consumption at p < .05 or better. Taylor et al. [34] reported two minimal effect sizes whilst James et al. [35] reported a large effect size. The mean effect size for cross-curricular approaches at reducing SLB or fruit juice consumption was M d = 0.42. This was within the Zone of Desired Effects [11], but more investigation may be required given the small number of studies included in the analysis.
Nutritional knowledge
There were 12 studies that adopted enhanced curricula approaches to improving the nutritional knowledge of primary school children. There were 13 nutritional knowledge outcomes that achieved a statistically significant improvement of p < .05 or better. In fact, 8 of the 13 studies reported statistical significance of p < .001. Researchers were able to calculate 7 effect sizes (3 × large, 1 × medium, 3 × minimal) with the mean effect size being M d = 0.75. This indicates that quality curriculum interventions (largely based on behavioural or social cognitive learning theory) are capable of achieving improvements in student nutritional knowledge with the Zone of Desired Effects [11].
An experiential learning-approach was adopted in four studies and all reported achieving statistical significance of p < .05 across seven nutritional knowledge-related outcomes. The researchers were able to calculate effect sizes for six of them and found five large and one minimal effect size. The mean effect size for the experiential learning approaches to nutritional knowledge was M d = 1.35 indicating this approach is a particularly strong evidence-based strategy for improving the nutritional knowledge of primary school-aged children
Discussion
This meta-analysis of school-based teaching interventions that have focused on improving the eating habits of primary school children found that experiential learning approaches had the greatest effect on reducing the food consumption, energy intake and nutritional knowledge of primary school children, and a smaller effect on primary school children’s FV consumption or preference. The other strategies that had a smaller effect on improving primary school children’s nutritional knowledge and reducing sugar consumption or preferences were cross-curricular approaches and quality curriculum interventions, respectively. In regards with improving primary school children’s FV consumption or preferences, both cross-curricular and quality curriculum interventions were effective.
In light of these findings, it is important to note that the high levels of heterogeneity among the included primary school healthy eating programs, does not make it possible to make firm conclusions. However, the findings have been supported in other literature, with experiential learning strategies, such as garden-enhanced learning strategies, positively influencing vegetable preferences and consumption among primary school children, which has been found to be the strongest predictor of future consumption [36-39]. Similar to this review, Langellotto & Gupta [39], who used meta-analytic techniques, found that school gardens and associated teaching strategies increased vegetable consumption in children, whereas the impacts of nutrition education programs were marginal or non-significant. There are two possible reasons for these findings: 1) school gardens increase access to vegetables; and 2) gardening decreases children’s reluctance to try new foods. Birch and colleagues [38] have also stated that in order to improve primary school children’s healthy food preferences, experiences and strategies need to increase availability and accessibility to increase exposure to those foods that will then affect their willingness to taste.
Whilst some studies report FV consumption or preference independently of each other, this tends to be the exception rather than the rule of reporting FV consumption or preference in primary school-based studies. Future studies should seek to promote, analyse and report vegetable consumption independent of fruit consumption to ascertain what physiological and behavioural effects this may have on students and findings of the study. This is because excessive consumption of fruit-based sugars (i.e. consuming fructose >50 g/d) may be one of the underlying aetiologies of Metabolic Syndrome and Type 2 Diabetes [35].
This study has some important considerations with regard to its generalizability. The target population were the students attending primary schools from any country around the world but all the studies bar one [40] were conducted in nations of the OECD. As such, they represent some of the most developed and advanced economies on the planet and should be taken into serious consideration when seeking to generalise these findings. Of the 49 studies analysed, more than half (n = 28) were conducted in the United States followed by the United Kingdom (n = 7). This may be attributed of the growing percentage of children in the USA and UK with non-communicable diseases attributed to diet-related factors [4,41]. It may also be indicative of the capacity of advanced economies, such as the USA and UK, to conduct empirically robust studies in primary school settings [42].
Strengths and limitations
There are several strengths of this systematic review and meta-analysis. First, this is the first known paper to systematically extract specific teaching strategies and approaches that facilitate the healthy eating of primary school children. As such, we conducted a systematic review using broad search terms to increase the probability of identifying all eligible publications, which yielded a well-sized (k = 49) evidence base. Second, the method of meta-analysis allowed for these strategies to be considered against other nutritional as well as the educational meta-analytic literature. Third, teaching strategies and approaches were reliably coded using schema of existing evidence of ‘what works’ in educational settings [11].
There were a few limitations associated with this review. The heterogeneity of primary school healthy eating interventions is large. This fact alone limited our ability to measure the effectiveness of each teaching strategy in the multi-faceted nutrition education programs. Moreover, it is possible that some strategies are commonly clustered with others, thus our findings should be considered carefully in terms of these strategies having similar effects when implemented on their own. Given that all the articles were identified from the peer-reviewed literature, there is some possibility of publication bias on the nature of evidence available to inform the review. Publication bias by particular journals, or more specifically the inability and discouragement of publishing articles that report negative results, may distort conclusions reached. Further, due to all but one study were conducted in OECD countries, findings from this systematic review and meta-analyses should be limited to informing decision making of stakeholders in those of similar nations.
Conclusion
Most teaching strategies extracted from intervention studies lead to positive changes in primary school children’s nutritional knowledge and behaviours. However, the most effective strategies for facilitating healthy eating in primary school children are enhanced curricula, cross-curricula and experiential learning approaches. Other strategies that showed some promising effect, but need to be further investigated include contingent reinforcement and parental involvement approaches.
Complete citations of the studies included in the systematic review and meta analyses are listed as the following in the reference list [30-34,36,40,43-84].
References
National Health and Medical Research Council. Australian Dietary Guidelines. Canberra: Australian Government; 2013.
Gill T, King L, Webb K. Best options for promoting healthy weight and preventing weight gain in NSW. Sydney: NSW Centre for Public Health Nutrition; 2005.
Khambalia AZ, Dickinson S, Hardy LL, Gill T, Baur LA. A synthesis of existing systematic reviews and meta-analyses of school-based behavioural interventions for controlling and preventing obesity. Obes Rev. 2012;13(3):214–33.
Popkin BM, Gordon-Larsen P. The nutrition transition: Worldwide obesity dynamics and their determinants. Int J Obes Relat Metab Disord. 2004;28:S2–9. Doi:10.1038/sj.ijo.0802804.
Neumark-Sztainer D, Wall M, Larson NI, Eisenberg ME, Loth K. Dieting and disordered eating behaviors from adolescence to young adulthood: findings from a 10-year longitudinal study. J Am Diet Assoc. 2011;111(7):1004–11.
Nicklaus S, Remy E. Early origins of overeating: tracking between early food habits and later eating patterns. Curr Obes Rep. 2013;2(2):179–84.
Lee A. Health-promoting schools: evidence for a holistic approach to promoting health and improving health literacy. Appl Health Econ Health Policy. 2009;7(1):11–7.
United Nations Educational, Scientific and Cultural Organization. Making Education a Priority in the Post-2015 Development Agenda. Paris: UNESCO; 2013.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(6):e1000097.
National Health and Medical Research Council. Healthy eating for children. Teach your child healthy habits for a healthy life. Canberra: Australia: Australian Government Department of Health and Ageing; 2014.
Hattie JA. Visible Learning: A synthesis of over 800 Meta-Analyses Relating to Achievement. London: Routledge; 2009.
Van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ. 2007;335(7622):703.
Rosenthal R. Parametric measures of effect size. In: Cooper H, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation; 1994. p. 231–44.
Cohen J. A power primer. Psyc Bul. 1992;112(1):155–9.
Roe L, Hunt P, Bradshaw H, Rayner M. Health promotion interventions to promote healthy eating in the general population: a review. Health Promot Eff Rev. 1997;6:198.
Campbell K, Waters E, O’Meara S, Summerbell C. Interventions for preventing obesity in childhood: a systematic review. Obes Rev. 2001;2(3):149–57.
Ammerman AS, Lindquist CH, Lohr KN, Hersey J. The efficacy of behavioural interventions to modify dietary fat and fruit and vegetable intake: a review of the evidence. Prev Med. 2002;35(1):25–41.
Burchett H. Increasing fruit and vegetable consumption among British primary school children: a review. Health Educ. 2003;103(2):99–109.
Berti PR, Krasevec J, FitzGerald S. A review of the effectiveness of agriculture interventions in improving nutrition outcomes. Public Health Nutr. 2004;7:599–609.
Knai C, Pomerleau J, Lock K, McKee M. Getting children to eat more fruit and vegetables: a systematic review. Prev Med. 2006;42(2):85–95.
Rasmussen M, Krolner R, Klepp KI, Lytle L, Brug J, Bere E, et al. Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature: Part I: quantitative studies. J Behav Nutr Phys Act. 2006;3(22):1–19.
Sahay TB, Ashbury FD, Roberts M, Rootman I. Effective components for nutrition interventions: a review and application of the literature. Health Promot Pract. 2006;7(4):418–27.
Howerton MW, Bell BS, Dodd KW, Berrigan D, Stolzenberg-Solomon R, Nebeling L. School-based nutrition programs produced a moderate increase in fruit and vegetable consumption: Meta and pooling analyses from 7 studies. J Nutr Educ Behav. 2007;39(4):186–96.
Oldroyd J, Burns C, Lucas P, Haikerwal A, Waters E. The effectiveness of nutrition interventions on dietary outcomes by relative social disadvantage: a systematic review. J Epidemiol Community Health. 2008;62(7):573–9.
Perez-Escamilla R, Hromi-Fiedler A, Vega-Lopez S, Bermudez-Millan A, Segura-Perez S. Impact of peer nutrition education on dietary behaviors and health outcomes among Latinos: a systematic literature review. J Nutr Educ Behav. 2008;40(4):208–25.
Robinson-O’Brien R, Story M, Heim S. Impact of garden-based youth nutrition intervention programs: a review. J Am Diet Assoc. 2009;109(2):273–80.
Hingle MD, O’Connor TM, Dave JM, Baranowski T. Parental involvement in interventions to improve child dietary intake: a systematic review. Prev Med. 2010;51(2):103–11.
Delgado-Noguera M, Tort S, Martinez-Zapata MJ, Bonfill X. Primary school interventions to promote fruit and vegetable consumption: a systematic review and meta-analysis. Prev Med. 2011;53(1–2):3–9.
Ganann R, Fitzpatrick-Lewis D, Ciliska D, Peirson L. Community-based interventions for enhancing to or consumption of fruit and vegetable among five to 18-year olds: a scoping review. BMC Pub Health. 2012;12:711.
Govula C, Kattelman K, Ren C. Culturally appropriate nutrition lessons increased fruit and vegetable consumption in American Indian children. Topics in Clin Nutr. 2007;22(3):239–45.
Horne PJ, Tapper K, Lowe CF, Hardman CA, Jackson MC, Woolner J. Increasing children’s fruit and vegetable consumption: a peer-modelling and rewards-based intervention. Eur J Clin Nutr. 2004;58(12):1649–60.
Baranowski T, Davis M, Resnicow K, Baranowski J, Doyle C, Lin LS, et al. Gimme 5 fruit, juice, and vegetables for fun and health: outcome evaluation. Health Educ Behav. 2000;27(1):96–111.
James J, Thomas P, Cavan D, Kerr D. Preventing childhood obesity by reducing consumption of carbonated drinks: cluster randomised controlled trial. BMJ. 2005;328(1):1237–9.
Taylor RW, McAuley KA, Barbezat W, Strong A, Williams SM, Mann JI. APPLE Project: 2-y findings of a community-based obesity prevention program in primary school age children. Am J Clin Nutr. 2007;86(3):735–42.
Johnson RJ, Perez-Pozo SE, Sautin YY, Manitius J, Sanchez-Lozada LG, Feig DI, et al. Could excessive fructose intake and uric acid cause type 2 diabetes? Endocr Rev. 2009;30(1):96–116.
McAleese J, Rankin L. Garden-based nutrition education affects fruit and vegetable consumption in sixth-grade adolescents. J Am Diet Assoc. 2007;107:662–5.
Blanchette L, Brug J. Determinants of fruit and vegetable consumption among 6–12-year-old children and effective interventions to increase consumption. J Hum Nutr Diet. 2005;18:431–43.
Birch LL, McPhee L, Shoba BC, Pirok E, Steinberg L. What kind of exposure reduces children’s food neophobia? Looking vs tasting. Appetite. 1987;9:171–8.
Langellotto GA, Gupta A. Gardening increases vegetable consumption in school-aged children: a meta-analytical synthesis. Hort Tech. 2012;22(4):430–45.
Francis M, Nichols SSD, Dalrymple N. The effects of a school-based intervention programme on dietary intakes and physical activity among primary-school children in Trinidad and Tobago. Public Health Nutr. 2010;13(5):738–47.
Organization of Economic Cooperation and Development. Health at a Glance 2013: OECD Indicators. Paris: OECD; 2013.
Organization of Economic Cooperation and Development. Equity and Quality in Education: Supporting Disadvantaged Students and Schools. Paris: OECD; 2012.
Auld GW, Romaniello C, Heimendinger J, Hambidge C, Hambidge M. Outcomes from a school-based nutrition education program using resource teachers and cross-disciplinary models. J Nutr Educ. 1998;30(5):268–80.
Bell CG, Lamb MW. Nutrition education and dietary behavior of fifth graders. J Nutr Educ. 1973;5:196–9.
Edwards CS, Hermann JR. Piloting a cooperative extension service nutrition education program on first-grade children’s willingness to try foods containing legumes. J Ext. 2011;49(1):1–4. Article 1IAW3 (Epublication).
Fahlman MM, Dake JA, McCaughtry N, Martin J. A pilot study to examine the effects of a nutrition intervention on nutrition knowledge, behaviors, and efficacy expectations in middle school children. J Sch Health. 2008;78(4):216–22.
Friel S, Kelleher C, Campbell P, Nolan G. Evaluation of the Nutrition Education at Primary School (NEAPS) programme. Public Health Nutr. 1999;2(4):549–55.
Gortmaker SL, Cheung LWY, Peterson KE, Chomitz G, Cradle JH, Dart H, et al. Impact of a school-based interdisciplinary intervention on diet and physical activity among urban primary school children: eat well and keep moving. Arch Pediatr Adolesc Med. 1999;153(9):975–83.
Liquori T, Koch PD, Contento IR, Castle J. The cookshop program: outcome evaluation of a nutrition education program linking lunchroom food experiences with classroom cooking experiences. J Nutr Educ. 1998;30(5):302–13.
Manios Y, Moschandreas J, Hatzis C, Kafatos A. Health and nutrition education in primary schools of Crete: changes in chronic disease risk factors following a 6-year intervention programme. Br J Nutr. 2002;88:315–24.
Morgan PJ, Warren JM, Lubans DR, Saunders KL, Quick GI, Collins CE. The impact of nutrition education with and without a school garden on knowledge, vegetable intake and preferences and quality of school life among primary-school students. Public Health Nutr. 2010;13(11):1931–40.
Simons-Morton BG, Parcel GS, Baranowski T, Forthofer R, O’Hara NM. Promoting physical activity and a healthful diet among children: results of a school-based intervention study. Am J Public Health. 1991;81(8):986–91.
Agozzino E, Esposito D, Genovese S, Manzi E, Russo KP. Evaluation of the effectiveness of a nutrition education intervention performed by primary school teachers. Ital J Public Health. 2007;4(4):131–7.
Amaro S, Viggiano A, Di Costanzo A, Madeo I, Baccari ME, Marchitelli E, et al. Kaledo, a new educational board-game, gives nutritional rudiments and encourages healthy eating in children: a pilot cluster randomized trial. Eur J Pediatr. 2006;165(9):630–5.
Anderson AS, Porteous LE, Foster E, Higgins C, Stead M, Hetherington M, et al. The impact of a school-based nutrition education intervention on dietary intake and cognitive and attitudinal variables relating to fruits and vegetables. Public Health Nutr. 2005;8(6):650–6.
Bere E, Veierod MB, Bjelland M, Klepp KI. Outcome and process evaluation of a Norwegian school-randomized fruit and vegetable intervention: Fruits and Vegetables Make the Marks (FVMM). Health Educ Res. 2006;21(2):258–67.
Cooke LJ, Chambers LC, Anez EV, Croker HA, Boniface D, Yeomans MR, et al. Eating for pleasure or profit: the effect of incentives on children’s enjoyment of vegetables. Psychol Sci. 2011;22(2):190–6.
Day ME, Strange KS, McKay HA, Naylor P. Action schools! BC–healthy eating: effects of a whole-school model to modifying eating behaviours of elementary school children. Can J Public Health. 2008;99(4):328–31.
Domel SB, Baranowski T, Davis H, Thompson WO, Leonard SB, Riley P, et al. Development and evaluation of a school intervention to increase fruit and vegetable consumption among 4th and 5th grade students. J Nutr Educ. 1993;25(6):345–9.
Duncan S, McPhee JC, Schluter PJ, Zinn C, Smith R, Schofield G. Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Int J Behav Nutr Phys Act. 2011;8:127.
Foster GD, Sherman S, Borradaile KE, Grundy KM, Vander Veur SS, Nachmani J, et al. A policy-based school intervention to prevent overweight and obesity. Pediatrics. 2008;121(4):e794–802.
Gorely T, Nevill ME, Morris JG, Stensel DJ, Nevill A. Effect of a school-based intervention to promote healthy lifestyles in 7–11 year old children. Int J Behav Nutr Phys Act. 2009;6:5.
Head MK. A nutrition education program at three grade levels. J Nutr Educ. 1974;6(56):59.
Hendy HM, Williams KE, Camise TS. Kid’s Choice Program improves weight management behaviors and weight status in school children. Appetite. 2011;56(2):484–94.
Hoffman JA, Franko DL, Thompson DR, Power TJ, Stallings VA. Longitudinal behavioral effects of a school-based fruit and vegetable promotion program. J Pediatr Psychol. 2010;35(1):61–71.
Kipping RR, Jago R, Lawlor DA. Diet outcomes of a pilot school-based randomised controlled obesity prevention study with 9–10 year olds in England. Prev Med. 2010;51(1):56–62.
Kristjansdottir AG, Johannsson E, Thorsdottir I. Effects of a school-based intervention on adherence of 7-9-year-olds to food-based dietary guidelines and intake of nutrients. Public Health Nutr. 2010;13(8):1151–61.
Luepker RV, Perry CL, McKinlay SM, Nader PR, Parcel GS, Stone EJ, et al. Outcomes of a field trial to improve children’s dietary patterns and physical activity: the child and adolescent trial for cardiovascular health CATCH collaborative group. JAMA. 1996;275(10):768–76.
Mangunkusumo RT, Brug J, De Koning HJ, Van Der Lei J, Raat H. School-based internet-tailored fruit and vegetable education combined with brief counselling increases children’s awareness of intake levels. Public Health Nutr. 2007;10(3):273–9.
Muth ND, Chatterjee A, Williams D, Cross A, Flower K. Making an IMPACT: effect of a school-based pilot intervention. N C Med J. 2008;69(6):432–40.
Panunzio MF, Antoniciello A, Pisano A, Dalton S. Nutrition education intervention by teachers may promote fruit and vegetable consumption in Italian students. Nutr Res. 2007;27(9):524–8.
Parcel GS, Simons-Morton B, O’Hara NM, Baranowski T, Wilson B. School promotion of healthful diet and physical activity: impact on learning outcomes and self-reported behavior. Health Educ Q. 1989;16(2):181–99.
Parmer SM, Salisbury-Glennon J, Shannon D, Struempler B. School gardens: an experiential learning approach for a nutrition education program to increase fruit and vegetable knowledge, preference, and consumption among second-grade students. J Nutr Educ Behav. 2009;41(3):212–7.
Perry CL, Bishop DB, Taylor G, Murray DM, Mays RW, Dudovitz BS, et al. Changing fruit and vegetable consumption among children: the 5-a-Day Power Plus Program in St. Paul, Minnesota. Am J Public Health. 1998;88(4):603–9.
Perry CL, Mullis R, Maile M. Modifying eating behavior of children: a pilot intervention study. J Sch Health. 1985;55(10):399–402.
Powers AR, Struempler BJ, Guarino A, Parmer SM. Effects of a nutrition education program on the dietary behavior and nutrition knowledge of second-grade and third-grade students. J Sch Health. 2005;75(4):129–33.
Quinn LJ, Horacek TM, Castle J. The impact of COOKSHOP on the dietary habits and attitudes of fifth graders. Top Clin Nutr. 2003;18(1):42–8.
Resnicow K, Davis M, Smith M, Baranowski T, Lin LS, Baranowski J, et al. Results of the TeachWell worksite wellness program. Am J Public Health. 1998;88(2):250–7.
Reynolds KD, Franklin FA, Binkley D, Raczynski JM, Harrington KF, Kirk KA, et al. Increasing the fruit and vegetable consumption of fourth graders: results from the high 5 project. Prev Med. 2000;30(4):309–19.
Sahota P, Rudolf MC, Dixey R, Hill AJ, Barth JH, Cade J. Randomised controlled trial of primary school based intervention to reduce risk factors for obesity. BMJ. 2001;323(7320):1029–32.
Shannon B, Chen AN. A three-year school-based nutrition education study. J Nutr Educ. 1988;20(34):114–24.
Smolak L, Levine MP, Schermer F. A controlled evaluation of an elementary school primary prevention program for eating problems. J Psychosom Res. 1998;44(3–4):339–53.
Spiegel SA, Foulk D. Reducing overweight through a multidisciplinary school-based intervention. Obesity (Silver Spring, Md). 2006;14(1):88–96.
Te Velde SJ, Brug J, Wind M, Hildonen C, Bjelland M, Perez-Rodrigo C, et al. Effects of a comprehensive fruit-and vegetable-promoting school-based intervention in three European countries: the Pro children study. Br J Nutr. 2008;99(4):893–903.
Funding
This study was brokered by the Sax Institute for the NSW Department of Education and Communities and the NSW Ministry of Health. The funding agencies instigated the research questions but had no influence (either directly or indirectly) over the search strategy, included studies, data analysis or findings.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
DAD, WGC and LRP conceptualized and designed the study. DAD, WGC and LRP collected the data. DAD conducted the statistical analyses. DAD, WGC and LRP contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Dudley, D.A., Cotton, W.G. & Peralta, L.R. Teaching approaches and strategies that promote healthy eating in primary school children: a systematic review and meta-analysis. Int J Behav Nutr Phys Act 12, 28 (2015). https://doi.org/10.1186/s12966-015-0182-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-015-0182-8