
Abstract
Background
Reducing inequalities in physical activity (PA) and PA-associated health outcomes is a priority for public health. Interventions to promote PA may reduce inequalities, but may also unintentionally increase them. Thus, there is a need to analyze equity-specific intervention effects. However, the potential for analyzing equity-specific effects of PA interventions has not yet been sufficiently exploited. The aim of this study was to set out a novel equity-specific re-analysis strategy tried out in an international interdisciplinary collaboration.
Methods
The re-analysis strategy comprised harmonizing choice and definition of outcomes, exposures, socio-demographic indicators, and statistical analysis strategies across studies, as well as synthesizing results. It was applied in a collaboration of a convenience sample of eight European PA intervention studies in adults aged ≥45 years. Weekly minutes of moderate-to-vigorous PA was harmonized as outcome. Any versus no intervention was harmonized as exposure. Gender, education, income, area deprivation, and marital status were harmonized as socio-demographic indicators. Interactions between the intervention and socio-demographic indicators on moderate-to-vigorous PA were analyzed using multivariable linear regression and random-effects meta-analysis.
Results
The collaborative experience shows that the novel re-analysis strategy can be applied to investigate equity-specific effects of existing PA interventions. Across our convenience sample of studies, no consistent pattern of equity-specific intervention effects was found. Pooled estimates suggested that intervention effects did not differ by gender, education, income, area deprivation, and marital status.
Conclusions
To exploit the potential for equity-specific effect analysis, we encourage future studies to apply the strategy to representative samples of existing study data. Ensuring sufficient representation of ‘hard to reach’ groups such as the most disadvantaged in study samples is of particular importance. This will help to extend the limited evidence required for the design and prioritization of future interventions that are most likely to reduce health inequalities.
Similar content being viewed by others


Background
Reducing health inequalities - defined as socio-demographic differences in life-expectancy, morbidity, and mortality - has become an important public health priority [1]. Socio-demographic differences have also been shown in health behaviors, including physical activity (PA), an important determinant of healthy ageing [2,3,4]. The proportion of individuals with sufficient PA levels, however, declines with age, with particularly low levels of PA among middle-aged and older adults [5, 6]. Furthermore, lower leisure-time PA levels have been associated with low socio-economic position (SEP), being female, belonging to an ethnic minority group, living in a deprived neighborhood, and not having a spouse [7,8,9,10,11]. Because being physically active regularly has numerous beneficial effects on physical and mental wellbeing [12, 13], it is likely that inequalities in PA are an important contributor to health inequalities [14].
Public health interventions have the potential to reduce existing health inequalities, but in particular interventions that aim at changing individual behavior (‘downstream interventions’) may also unintentionally increase them (‘intervention-generated inequalities’; [15, 16]). One major reason for this is that downstream interventions in contrast to policy-change (‘upstream’) interventions usually require relatively more individual psychological, temporal, and material resources (‘individual agency’ [17];) to succeed. Such resources are unequally distributed between different population groups, favoring predominantly those at the upper end of the socio-economic spectrum [17,18,19]. In this regard, it has also been found that the links between psychosocial determinants of health behavior, such as attitudes and intentions, and health behavior are more pronounced and have stronger effects on behavior among high- than among low-SEP individuals [20, 21]. Thus, interventions based on these psychosocial determinants may unintentionally increase inequalities by benefiting high-SEP individuals disproportionally more. The relevance of individual agency for equity-specific effects of behavioral interventions is empirically supported by systematic reviews of interventions in different areas, including tobacco control [22], obesity prevention [23], and healthy eating [24]. Divergent perceptions between low-SEP individuals and health promoters regarding lifestyle, lifestyle change, and support for lifestyle change are a further possible explanation for interventions being less beneficial in low-SEP population groups [25].
The effects of PA interventions may not only differ by SEP but also by gender and other relevant socio-demographic indicators associated with inequalities and PA, such as ethnicity and marital status [26,27,28]. With regard to gender, there are differences between males and females in preferred PA domains and contexts, as well as in motivational factors and barriers to PA [29,30,31]. Compared with males, females appear to be more motivated by the social aspects of PA (e.g., spending time with others and meeting friends), by losing or managing weight, and by improving appearance. They tend to be less motivated than men to participate in physical activities that are vigorous, require skill and practice, involve some kind of competition, and are done outdoors [30]. Moreover, compared with males, females more often take over domestic and care responsibilities, not infrequently carried out in addition to paid work, leaving little time for leisure activities such as PA [31]. With regard to ethnicity, minority ethnic groups may face additional barriers to PA engagement, for example due to differing perceptions about and attitudes towards PA as well as cultural expectations [32].
Results of an equity-focused systematic review by Attwood and colleagues [27] indicate that the effects of primary-care-based PA interventions may differ by gender, but there was no consistent pattern regarding the direction of these differences. This is in line with the results of another equity-focused systematic review of interventions to promote PA among adults aged ≥50 years by Lehne & Bolte [28]. As reported by Humphreys & Ogilvie [26], the effects of environmental and policy interventions to promote PA may differ by ethnicity and gender, whereby members of the majority population seemed to benefit more from the interventions than members of ethnic minority populations. Like Attwood et al. [27] and Lehne & Bolte [28], this review also found no consistent pattern regarding the direction of gender-specific intervention effects. All three reviews concluded that, because of the paucity of studies that actually report equity-specific effect analyses, it is difficult to draw implications for the design of future interventions that could effectively reduce PA inequalities according to SEP, gender, and other relevant socio-demographic indicators (e.g., ethnicity, marital status) [26,27,28]. Such indicators are frequently measured in studies, but only a minority of studies explicitly analyze equity-specific intervention effects. The potential for assessing intervention effects on inequalities in PA has not yet been fully exploited [26,27,28].
Analyzing equity-specific intervention effects requires interaction or subgroup analyses that compare intervention effects across different population subgroups defined by socio-demographic characteristics [33]. A criticism of this approach is that few studies are designed with adequate sample sizes to run such interaction or subgroup analyses, so that many of the current findings are based on potentially underpowered post-hoc analyses with limited credibility [33, 34]. However, given the importance of better understanding whether, how, and why interventions affect health inequalities, and the plausibility of differential intervention effects, equity-specific re-analyses of data of existing intervention studies are arguably a valuable approach [35,36,37,38,39,40,41]. One particular reason is that the consistent conduct and reporting of such analyses allows for pooling effect estimates across studies, which increases statistical power and improves the credibility of the findings [42]. As re-analyses require access to complete primary data (including individual participant data) and detailed knowledge of the individual studies going beyond the information usually given in publications, a collaborative approach involving researchers from the primary studies seems necessary.
The aim of this study was to set out a novel strategy for re-analyzing equity-specific intervention effects and to try out its application in an international interdisciplinary collaboration between existing individual-level PA intervention studies in middle-aged and older adults.
Methods
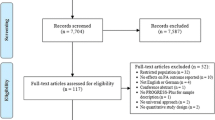
This study was conducted as part of the project “EQUAL - Equity impacts of interventions to increase physical activity”, a subproject within the prevention research network “AEQUIPA - Physical activity and health equity: primary prevention for healthy ageing” [43]. EQUAL aimed to develop and try out a strategy for re-analyzing equity-specific effects of PA interventions in an international interdisciplinary collaboration [44]. The collaboration was initiated based on researchers representing eight published European PA intervention studies in middle-aged and older adults [45,46,47,48,49,50,51,52] (a convenience sample of 20 eligible studies), as well as experts on equity-specific data analysis. In accordance with previous studies [53, 54], middle-aged and older adults were defined as individuals aged 45 years and older. As well as using the AEQUIPA intervention study PROMOTE [52], studies were identified through a literature search [44]. Inclusion criteria were: studies reporting the effects of individual-level PA interventions; targeted at community-dwelling adults aged ≥45 years; with a randomized or non-randomized controlled longitudinal study design in which the control group received no intervention; and reporting on participants’ age, gender, as well as on at least one measure of SEP (i.e., education, income, occupation, composite SEP). The collaborating researchers represent various disciplines, including (social) epidemiology, biostatistics, health psychology, primary care research, sport and human movement sciences.
Plenary and bilateral meetings (face-to-face and online) and e-mail correspondence were used to develop the re-analysis strategy and to define common criteria for adopting it to the sample of studies included in the collaboration. First, the EQUAL study team outlined ideas for the strategy to be developed, informed by: 1) available evidence about equity-specific effects of PA interventions; 2) concepts and theories of how interventions may affect health inequalities; and 3) existing approaches to equity-specific re-analysis. The outline was sent to the collaborating researchers via e-mail with a request for feedback and subsequently revised by the EQUAL study team according to the feedback received. In a next step, the collaborating researchers were invited to a one-day face-to-face workshop in Bremen, Germany, to find consensus about the individual steps of the strategy based on the revised outline as well as to discuss common criteria for adapting the strategy to the eight included studies. Based on the results of the discussion, the EQUAL study team developed draft criteria for re-analyzing equity-specific effects of the individual studies, which were revised after two rounds of iterative discussion by e-mail. These criteria were applied by members of the research group to their own data (i.e., there was no pooling of the studies’ individual participant data) with or without assistance from the EQUAL study team. Finally, criteria for combining the results from the individual studies were added. These criteria were developed by statistician colleagues of the collaboration working with the EQUAL study team and were agreed at an online meeting.
Characteristics of studies included in the collaboration
Details of the eight intervention studies are presented in Additional file 1. Three studies were conducted in the United Kingdom, three in the Netherlands, one in Belgium, and one in Germany. Seven studies were (cluster-)randomized controlled trials, and one was a controlled before and after study. Baseline sample sizes varied between 298 and 2140 participants. Two studies (GALM, PACE-UP) recruited exclusively physically inactive participants. Study participants were either recruited via the community (Active Plus I, Active Plus II, Every Step Counts!, GALM, PROMOTE) or through primary care (PACE-Lift, PACE-UP, ProAct65+). While all eight studies aimed to increase PA, three (PACE-Lift, PACE-UP, Every Step Counts!) had a particular focus on promoting walking, and one (GALM) on promoting recreational sports activities. Three studies (Every Step Counts!, PACE-Lift, PACE-UP) delivered individual-level pedometer-based walking programs, three personalized PA advices without (Active Plus I, Active Plus II) or with community-based group meetings (PROMOTE), one (GALM) group-based PA sessions in a gymnasium in the neighborhood, and one (ProAct65+) a home- or class-based exercise program. Intervention length ranged between 10 and 26 weeks.
Results
Equity-specific re-analysis strategy
The equity-specific re-analysis strategy comprises harmonizing the choice and definitions of outcomes (step 1), exposures (step 2), socio-demographic indicators (step 3), and statistical analysis strategies (step 4) across studies by defining common criteria; as well as synthesizing the results (step 5). The following sections provide detailed descriptions of the individual steps of the strategy and how to adopt them to existing study data. To do so, we present the criteria for harmonization and synthesizing results as defined for our convenience sample of PA intervention studies.
Step 1: harmonizing the choice and definition of outcome measures across studies
The first step includes choosing an outcome measure which adequately measures the objectives of the kind of intervention under study and which can be defined across studies as similar as possible. Health promoting behaviors such as PA need to be maintained for long-term health benefits [55, 56]. Moreover, it has been shown that inequalities may initially increase after implementation of new interventions before decreasing again as time passes [57]. Therefore, in order to make conclusions about inequalities in long-term health benefits, where data permit, both short-term and long-term outcomes of the interventions should be considered.
For our sample of PA intervention studies, we identified weekly minutes of moderate-to-vigorous PA (MVPA) at the post-intervention follow-up time point closest to the intervention end point (T1) as primary outcome because it could be defined in a similar manner across the studies and the beneficial effects of MVPA on health are well documented [58]. Considering the data of five studies, weekly minutes of MVPA at the next follow-up assessment (T2) was chosen as secondary outcome to investigate potential changes in equity-specific intervention effects over time. This was 8 months post-intervention for Active Plus I and Active Plus II, 9 months post-intervention for PACE-Lift and PACE-UP, and 6 months post-intervention for ProAct65+. Due to better precision and accuracy [59], we decided to prefer objective PA measures over subjective measures, when both were available in a study. In Active Plus I, Active Plus II, Every Step Counts!, GALM, and ProAct65+ that measured PA exclusively subjectively, physical activities of at least three metabolic equivalents (MET) were defined as MVPA, following recommendations by guidelines [60]. In PACE-Lift, PACE-UP, and PROMOTE that measured PA objectively, the standard Freedson cut-point of 1952 counts per minute [61], equivalent to three METs, was used to define MVPA. In addition to the main outcome total weekly minutes of MVPA, sensitivity analyses were conducted for PACE-Lift and PACE-UP using weekly minutes of MVPA in bouts of at least 10 min.
Step 2: harmonizing the choice and definition of exposure measures across studies
Studies of interventions may differ with regard to the number of intervention and control groups. Step two includes choosing an exposure measure which can be defined across studies as similar as possible.
For our sample of PA intervention studies, any versus no intervention was defined as exposure. In Active Plus I, Active Plus II, PACE-UP, ProAct65+, and PROMOTE which included several intervention groups, intervention groups were combined to create a single pair-wise comparison in order to avoid double-counting. The Cochrane Handbook for Systematic Reviews of Interventions recommends this approach for including studies with several intervention groups in a meta-analysis [62].
Step 3: harmonizing the choice and definition of socio-demographic indicators across studies
Step three includes harmonizing the choice and definition of socio-demographic indicators which should be based on existing theories and evidence of equity-specific intervention effects. There are several different socio-demographic indicators that might be relevant to consider. The PROGRESS-Plus framework [63], proposed by the Campbell and Cochrane Equity Methods Group, may help researchers in identifying socio-demographic indicators relevant for their specific research question. SEP should be considered a multidimensional construct comprising diverse socio-economic indicators at the individual, household, or contextual level [64,65,66,67]. Because different indicators of SEP operate through different causal pathways and may have different relevance among individuals of varying age and gender [64,65,66,67], the choice of SEP indicator may affect findings about the presence and extent of equity-specific intervention effects. It is therefore important to consider, and clearly differentiate between, various relevant SEP indicators instead of focusing on one indicator only or using several SEP indicators interchangeably. Moreover, potential intersections between several socio-demographic indicators [68, 69], such as gender and SEP, should be considered. Putting such an intersectionality lens to the re-analysis of data of intervention studies, where sample size and diversity permit, could yield even more comprehensive insights on the impact of these interventions on health inequalities.
For our sample of PA intervention studies, education as a measure of SEP [64,65,66,67] and gender (only defined as female versus male) as a social construct [70, 71] were selected as main socio-demographic indicators because both characteristics have previously been shown to moderate the effects of PA interventions [26,27,28], information on both were available in all collaborating studies, and both can be operationalized in a similar manner across studies from different countries. Education was defined according to the International Standard Classification of Education (ISCED) 2011 [72]. Based on the highest level of educational qualification or age at leaving full time education, individuals were grouped into the categories “Low” (at most lower secondary education (ISCED 0–2) or leaving full time education at ≤16 years), “Medium” (upper secondary and post-secondary non-tertiary education (ISCED 3–4) or leaving full time education at 17–18 years), or “High” (tertiary education (ISCED 5–8) or leaving full time education at ≥19 years).
In a secondary analysis, income and area deprivation as measures of SEP [64,65,66,67] were considered. Information on household income was available in two (ProAct65+, PROMOTE) and information on area deprivation (index of multiple deprivation [IMD] score [73]) was available in three studies (PACE-Lift, PACE-UP, ProAct65+). For both of these indicators, in each study, tertiles were defined in terms of the distribution in the study’s specific data set. This resulted in two variables with the categories “Low”, “Medium”, and “High” each for household income and area deprivation (see Additional file 2 for details). Additionally, marital status (defined as having versus not having a partner) was considered as a socio-demographic indicator because the presence or absence of a spouse has been shown to be associated with health inequalities and PA [10, 74].
Although the effects of PA interventions my also differ between individuals of different ethnic backgrounds, we did not consider ethnicity as a socio-demographic indicator due to differing ethnic compositions in the study populations and data availability. Potential intersections between several socio-demographic indicators were also not considered because of small sample size and insufficient diversity.
Step 4: harmonizing the choice and definition of statistical analysis strategies across studies
Step four comprises to specify the statistical methods and modeling strategies for the equity-specific effect analyses. Not only intervention effects, but also intervention reach, adherence, and dropout may also differ by socio-demographic characteristics and therefore should be considered for a comprehensive assessment of equity-specific intervention benefits [15, 75].
Equity-specific intervention reach
In our sample of PA intervention studies, the majority lacked information on socio-demographic indicators for non-participants. This precluded the calculation of socio-demographic group-specific response rates [76, 77], so it was not possible to investigate equity-specific intervention reach. We originally aimed to consult census data and to compare the study population with the targeted population of each study, considering the studies’ specific eligibility criteria. However, as no suitable census data could be identified, we decided to calculate an overall response percentage, defined as the number of persons who completed the baseline (T0) questionnaire and were assigned to the intervention conditions, divided by the number of persons invited to participate. For Every Step Counts! and PROMOTE, only estimations of response percentages could be made because the recruitment strategies comprised advertising. For each study, the distribution of gender, education, income, area deprivation, and marital status groups as well as the mean age in the intervention and control groups at T0 were calculated.
Equity-specific intervention adherence and dropout
We calculated percentages and means to describe adherence and dropout stratified by socio-demographic indicators. Information on intervention adherence was available in Active Plus II, GALM, PACE-UP, and PROMOTE, relating to the use of intervention materials and/or attendance at group meetings. We defined dropouts as individuals with valid information on MVPA at T0 but without valid information at T1. Additionally, we calculated mean values and corresponding standard deviations (SD) of weekly minutes of MVPA at T0 for each subgroup of interest, stratified by intervention and control group, as well as by completers and dropouts.
General and equity-specific intervention effects
The general intervention effect was defined as the difference between the intervention and control groups in minutes of MVPA per week at T1 (main analysis) or T2 (secondary analysis). For this purpose, post-intervention values of weekly minutes of MVPA were regressed on intervention versus control group and minutes of MVPA per week at T0 without (minimally adjusted model) and with adjustment for age in years, gender, and education (fully adjusted model). Due to the nature of the data, in four studies, the models were additionally (multilevel-)adjusted for practice (PACE-Lift, PACE-UP, ProAct65+); household (PACE-Lift, PACE-UP); or community, valid wear-time, and season (PROMOTE). All analyses were conducted by intention-to-treat, analyzing participants according to the group to which they were originally assigned, restricting the models to individuals with complete data on all variables included (i.e., complete case intention-to-treat analysis).
Equity-specific intervention effects were investigated by adding intervention*socio-demographic indicator interaction terms to the regression models. For analyzing equity-specific intervention effects by gender, for example, post-intervention values of weekly minutes of MVPA were regressed on intervention versus control group, MVPA per week at T0, age in years, gender, and the intervention*gender interaction without (minimally adjusted model) and with adjustment for education and the intervention*education interaction (fully adjusted model). Because age is associated with most of the socio-demographic indicators and with PA levels, we decided to include it as a covariate in all models. For each model, the p-values for the interaction terms and effect estimates with corresponding 95% confidence interval (CI) for each subgroup of interest were computed. Following Greenland et al. [78], precise p-values were reported.
Step 5: synthesizing the results
The last step includes synthesizing the results from the individual studies. Meta-analysis is the preferable method because it can increase the power for detecting equity-specific intervention effects which is often limited in post-hoc analysis [33, 34]. If the number of studies permit, meta-regression [79] should be used to investigate possible sources of heterogeneity (e.g. study quality, study design). If the sample of studies is highly heterogeneous and data can hardly be harmonized to enable meta-analysis, there are alternative approaches to synthesize and visualize the equity-specific results of individual studies, such as the harvest plot [80].
In our homogeneous sample of PA intervention studies, after data had been harmonized, the estimates for the regression coefficients of the intervention*socio-demographic indicator interactions from the individual studies were pooled using random-effects meta-analysis. To be able to assess the direction of these interaction effects, in particular for any disadvantage experienced by the most disadvantaged groups, regression models were slightly modified. Education, income, and area deprivation were considered as variables with two (low versus medium/high education and income, high versus medium/low deprivation) instead of three categories resulting in one regression coefficient for each intervention*socio-demographic indicator interaction. This means that for all studies, the socio-demographic indicators were comparable in measurement and levels.
Analyses were conducted in R using the metafor package [81]. As effect size, we chose the point estimates of the intervention*socio-demographic indicator interactions in minutes. A random effects model was fitted using the DerSimonian and Laird method. The extent of heterogeneity was measured by the I2 index. Following Higgins et al. [82], I2-values of 25, 50, and 75% were considered low, moderate, and high heterogeneity, respectively. The intervention*socio-demographic indicator interaction effect estimates and their corresponding 95% CI were presented in forest plots. Since some studies used different numbers of predictors, a sensitivity analysis was conducted estimating partial correlation coefficients [83]. Meta-regression was deemed inappropriate due to the low number of studies.
Risk of bias assessment
Whichever method to synthesize the results is chosen, a risk of bias assessment should be conducted. There is no specific tool for assessing the risk of bias in a result from equity-specific effect analysis. For our sample of studies, we therefore decided to assess the risk of bias regarding the general intervention effects, using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) [84] and the ROBINS-I risk-of-bias tool for non-randomized studies of interventions [85]. The assessment of each study was performed by at least one researcher from the contributing study (FB, TH, SI, RM, SM, DP, MS, JV) and one researcher from the EQUAL project team (GC) independently. Journal article(s), the published re-analysis strategy [44], and internal knowledge about the study were used to help inform the assessment. Any discrepancies were resolved through discussion and, where necessary, consulting the last author (GB).
Application of the equity-specific re-analysis strategy
The following sections illustrate the application of the equity-specific re-analysis strategy. To do so, we present the results from applying the criteria for adapting the strategy set out above to our convenience sample of PA intervention studies.
Risk of bias within studies
Regarding the general intervention effects, the randomized studies PACE-Lift and PACE-UP were judged to be at low risk of bias, and Active Plus I, Active Plus II, GALM, ProAct65+, and PROMOTE at high risk (Table 1). The non-randomized study Every Step Counts! was judged to be at serious risk (Table 2). The high/serious risks resulted from non-concealed randomization sequences, differing proportions of missing outcome data in the intervention and control groups, and/or participant-reported outcome measures. Further details are available in Additional file 3.
Response percentages and baseline socio-demographic characteristics
Calculated response percentages ranged from 6% in ProAct65+, over 10% in PACE-UP, 12% in GALM, 16% in Active Plus II, 23% in Active Plus I, to 30% in PACE-Lift. Response percentages of PROMOTE and Every Step Counts! were estimated to be 7 and 80%, respectively. Some differences existed between the studies regarding the socio-demographic composition of their baseline samples (Table 3). Most studies had slightly higher percentages of females, ranging from 51% in Active Plus I to 68% in Every Step Counts! (mean = 58%). There was a great variation in the proportion of low-educated participants, ranging from 2% in PROMOTE to 56% in Every Step Counts! (mean = 38%). The percentages of participants without a partner ranged from 18% in Active Plus II to 42% in ProAct65+ (mean = 26%).
Equity-specific intervention adherence
Results of Active Plus II, GALM, PACE-UP, and PROMOTE with information on intervention adherence indicated no or only slight differences across gender and education subgroups, with no consistent pattern regarding the direction of differences (Table 4). For example, in GALM, slightly higher mean attendance rates of the 15 intervention sessions were observed among low educated participants. In PACE-UP, PA diary return and pedometer use were slightly higher among medium educated individuals. In PROMOTE, females attended the group meetings more often than males. We also found only marginal differences across income, area deprivation, and marital status subgroups. Further details are available in Additional file 4.
Equity-specific intervention dropout
Dropout rates from T0 to T1 varied considerably between the studies, ranging from 6% in PACE-Lift to 45% in Active Plus II. In half of the studies (Active Plus I, Active Plus II, GALM, PROMOTE), intervention group participants were more likely to drop out of the study (Table 5). This bias was mainly the same across gender and education subgroups. In the other half of the studies (Every Step Counts!, PACE-Lift, PACE-UP, ProAct65+), dropout rates were comparable between intervention and control groups, for the total sample, as well as for the gender and education subgroups. Moreover, dropout rates in the intervention and control groups were generally comparable or differed only slightly across gender and education subgroups. For example, in GALM and PROMOTE, dropout rates in the control group slightly differed by gender, with a higher dropout among males (GALM) and females (PROMOTE), respectively.
Patterns of dropout in intervention and control groups were also similar across income, area deprivation, and marital status subgroups. Only slight differences in dropout rates in the intervention and control groups were found across these subgroups (Additional file 5).
Information on equity-specific dropout at T2 and baseline MVPA levels can be found in Additional files 5 and 6.
General and equity-specific intervention effects
The general intervention effects as well as the gender- and education-specific intervention effects at T1 derived from the fully adjusted models are shown in Table 6. Results of the minimally adjusted models are available in Additional file 7. In Active Plus II, Every Step Counts!, PACE-Lift, PACE-UP, and PROMOTE, the intervention groups did more weekly minutes of MVPA at T1 than the control groups. In Active Plus I, GALM, and ProAct65+, no differences between the groups were found.
Overall, we found no consistent pattern of differential intervention effects across the studies. For Active Plus I, an intervention*gender interaction was found, suggesting that the intervention was more effective in increasing weekly minutes of MVPA in females than in males. For PACE-UP, an intervention*education interaction was found, suggesting that the intervention was more effective among medium than high or low educated individuals.
There was no evidence of differential intervention effects by household income, area deprivation, and marital status (Additional file 7). For Active Plus II, at 8 months post-intervention, as well as for PACE-Lift and PACE-UP, at 9 months post-intervention, the intervention groups continued to have higher MVPA levels compared to the control groups, although the differences between the groups were less pronounced when compared to the main analysis (Additional file 7). For Active Plus I, at 8 months post-intervention, and ProAct65+, at 6 months post-intervention, the intervention groups tended to engage in more MVPA than the control groups. There was no evidence of differential intervention effects by any of the socio-demographic indicators examined. For PACE-Lift and PACE-UP, sensitivity analyses of MVPA in bouts of at least 10 min had little impact on the effect estimates and did not change the interpretation (Additional file 7).
Meta-analyses
Figures 1 and 2 show the estimates for the moderated effects of the interventions through gender and education at T1 for each study (fully adjusted models). The detailed results of the meta-analyses can be found in Additional file 8. The pooled estimates indicated no differences in intervention effects either by gender (5.1 (95% CI: − 20.7 to 31.0), 5321 participants, 8 studies) or by education (− 1.5 (95% CI: − 28.9 to 25.9), 5321 participants, 8 studies). Between study heterogeneity was moderate to high (I2 = 64%) for the moderated intervention effects through gender and low to moderate (45%) for the moderated intervention effects through education.

Forest plot of moderated intervention effects through gender at T1

Forest plot of moderated intervention effects through education at T1
The pooled estimates for the moderated intervention effects through income, area deprivation, and marital status at T1 indicated no differences in intervention effects by these indicators (income: 0.5 (95% CI: − 10.6 to 11.6), I2 = 0%, 933 participants, 2 studies); area deprivation: -27.9 (95% CI: − 58.5 to 2.7), I2 = 0%, 1802 participants, 3 studies); marital status: 6.9 (95% CI: − 3.3 to 17.1), I2 = 0%, 5341 participants, 8 studies).
At T2, the pooled estimates indicated no differences in intervention effects by gender (17.2 (95% CI: − 14.6 to 49.1); I2 = 18%; 4348 participants; 5 studies), education (− 13.4 (95% CI: − 54.3 to 27.5); I2 = 38%; 4348 participants; 5 studies), area deprivation (− 21.8 (95% CI: − 50.4 to 6.9); I2 = 0%; 1887 participants; 3 studies), and marital status (− 1.7 (95% CI: − 36.8 to 33.5), I2 = 15%; 4366 participants; 5 studies) (Additional file 8). The sensitivity analysis using partial correlation coefficients lead to comparable results (Additional file 9).
Discussion
This study sets out a novel equity-specific re-analysis strategy tried out in an international interdisciplinary collaboration. The collaborative experience shows that the novel strategy can be applied to investigate equity-specific effects of existing PA intervention studies in community-dwelling middle-aged and older adults. Across our convenience sample of eight studies, we found no consistent pattern of differential intervention adherence, dropout, and efficacy by gender, education, income, area deprivation, and marital status.
Strengths and limitations
By applying an equity lens to the analysis of data from PA intervention studies, our strategy offers an approach to filling the gap in knowledge about the impact of these interventions on health inequalities. In contrast to other approaches of equity-specific re-analysis, our strategy proposes the consideration of several SEP indicators instead of focusing on education only [40, 41] or using several SEP indicators interchangeably [38, 39]. Moreover, besides equity-specific intervention effects, the novel strategy includes investigating equity-specific intervention reach, adherence, and dropout, allowing for a comprehensive assessment of equity-specific intervention benefits. The strategy comprises harmonizing the choice and definition of outcomes, exposures, socio-demographic indicators, and statistical analysis strategies across studies as much as possible. Similar to an individual participant data meta-analysis with harmonized data [86], harmonizing each study’s individual participant data according to jointly developed criteria allows to examine interaction and subgroup effects in a setting that goes far beyond conventional meta-analyses of published data. Our experience shows that a collaborative approach bringing together researchers from primary studies and regular exchange within the collaboration is important as it allows discussing methodological issues and re-analysis findings in-depth. In this regard, the internal knowledge about the studies contributed by the responsible researchers is of particular importance as this far exceeds the information which can be extracted from publications.
A limitation of our study is that we applied the equity-specific re-analysis strategy to a convenience sample of studies. Therefore, our re-analysis results cannot be considered generalizable. To provide a comprehensive summary of the current evidence on equity-specific effects of individual-level PA interventions among middle-aged and older adults, it would be relevant to apply our strategy to a larger, representative sample of studies identified in a systematic literature search. The small sample of eight studies also prevented us from conducting meta-regression [79] which we would recommend to take into consideration when applying our strategy to a larger group of studies.
Our experience shows that there are certain limitations and challenges to using our strategy. First, data harmonization may result in a loss of data detail. For instance, in studies with several intervention groups, these groups were combined to create a single pair-wise comparison. Moreover, weekly minutes of MVPA was used as the outcome, without differentiating between different intensities, domains, or types of PA, and data transformations carried out in some studies’ original analysis were not used here. As a result, for some studies, the general intervention effects observed in the re-analysis diverged from the original study results. However, without data harmonization, no formal meta-analysis would be possible, thus losing the opportunity to gain precision in estimating effects of interest. It will be important for future studies to weigh the advantages against the disadvantages of data harmonization from a public health perspective.
A second issue relates to the fact that, because information on socio-demographic indicators for non-participants is often not available in studies of health promotion interventions, assessing inequalities in intervention reach is not straightforward. Instead, census data could be consulted and the study population could be compared with the targeted population of each study, considering the studies’ specific eligibility criteria. Our experience shows, however, that finding suitable census data can be complicated. We would recommend at least calculation (or estimation) of overall response rates and investigation of the socio-demographic characteristics of the study sample. In our convenience sample of eight intervention studies, most included rather equal numbers of females and males, with some studies reaching slightly more women than men. The percentage of individuals with low education, however, varied considerably between the studies, partly as a result of different recruitment procedures. In one study, the percentage was particularly low (2%), suggesting that the intervention reached predominantly those at the upper end of the socio-economic spectrum.
A third aspect involves the comprehensiveness with which equity-specific intervention effects can be analyzed. This depends particularly on the availability of information on relevant socio-demographic indicators, the comparability of socio-demographic indicators across studies, as well as the size and diversity of study samples. In our sample of PA intervention studies, information on gender, education, and marital status were available in all studies and could be defined in a similar manner, but information on income and area deprivation were available in only two and three studies, respectively. Ethnicity, which was assessed in three studies, was not considered as a socio-demographic indicator due to differing ethnic compositions in the study populations. The fact that not all studies were heterogeneous in terms of education might have limited the ability to identify education-specific intervention effects. Moreover, gender could be defined only as female versus male without further operationalizing gender according to gender theoretical concepts [71]. We were also only able to consider differential intervention effects with regard to a single dimension of inequalities, such as SEP, whereas potential differential intervention effects across intersections of multiple dimensions [68, 69], such as SEP and gender, were not considered.
A fourth issue concerns the handling of missing data. For our sample of PA intervention studies, we did not address the risk of attrition bias through sensitivity analyses using multiple imputation (MI) methods which future studies applying the strategy may consider. Because MI methods would have varied between the studies posing problems for interpretation, we decided to not impute missing outcome data. Moreover, in half the studies, MI sensitivity analyses were conducted in their original analyses providing evidence that their results were not biased by missing outcome data and dropout rates were found to be comparable across socio-demographic subgroups for most of the studies. In such cases, the risk of having under- or overestimated differential intervention effects due to differential dropout can be considered rather low. Fifth, in this regard, it also becomes clear that the high risk and serious risk of bias judgements of general intervention effect estimates, for example, due to differing proportions of missing outcome data in the intervention and control groups, must not necessarily apply to equity-specific intervention effect estimates. Existing risk of bias tools, such as the RoB 2.0 and the ROBINS-I, are designed to assess the risk of bias in estimates of general intervention effects, whereas estimates of equity-specific intervention effects are not considered. There is a need for tools that enable adequate assessments of the risk of bias in estimates of equity-specific intervention effects.
A sixth point is that the ability to investigate potential changes in equity-specific intervention effects over time may be limited because few studies of PA interventions have evaluated long-term intervention effects [56]. For our sample of PA intervention studies, we identified PA at the post-intervention follow-up time point closest to the intervention end point as the primary outcome as this criterion was met by all studies. Six, eight, or nine months post intervention, respectively, were used as a secondary outcome, considering the data of five studies. We strongly recommend, where sufficient data is available, to investigate equity-specific differences in intervention effects over a longer time period.
Finally, a collaborative procedure such as ours requires temporal, personnel, and financial resources. Future studies that aim to apply the strategy to existing study data must take these resources into account and should rate the costs against the expected benefit from a public health perspective.
Equity-specific re-analysis can help build the needed evidence base on the effects of public health interventions on health inequalities in the short term. However, there are some limitations of post-hoc analyses [33]. As discussed above, the comprehensiveness with which equity-specific intervention effects can be analyzed may be limited. Moreover, the probability of false-negative results (i.e., failing to detect a true differential intervention effect) may be increased due to insufficient statistical power [87]. Therefore, planning equity-specific effect analysis a-priori should be the long-term objective. Future studies should ideally consider inequalities already in the planning of data collection tools and sample size calculations. Particularly the latter is an ambitious goal which may not always be feasible because the increase in sample size required to detect differential intervention effects may be considerable [87].
Conclusions
The collaborative experience shows that the novel re-analysis strategy can be applied to investigate equity-specific effects of existing PA interventions. We encourage future studies to exploit the potential for equity-specific effect analysis by applying the strategy to representative samples of existing study data ensuring sufficient representation of ‘hard to reach’ groups. Ability to share individual participant data in line with open science principles and willingness to share detailed knowledge of study characteristics among primary study authors is of particular relevance. This will help extend the limited evidence required for the design and prioritization of future interventions that will be most likely to reduce health inequalities.
Availability of data and materials
Aggregated data supporting the conclusions of this article are included within the article and additional files. Individual participant data remain under ownership of the researchers from the contributing studies.
Change history
29 October 2021
The funding note was missing in the original publication. The article has been updated to rectify the error.
Abbreviations
- CI:
-
Confidence interval
- IMD:
-
Index of multiple deprivation
- ISCED:
-
International Standard Classification of Education
- MI:
-
Multiple imputation
- MVPA:
-
Moderate-to-vigorous physical activity
- PA:
-
Physical activity
- RoB 2.0:
-
Revised Cochrane risk-of-bias tool for randomized trials
- ROBINS-I:
-
Risk-of-bias tool for non-randomized studies of interventions
- SD:
-
Standard deviation
- SEP:
-
Socio-economic position
References
Commission on Social Determinants of Health (CSDH). Closing the gap in a generation - Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva: World Health Organisation; 2008.
Daskalopoulou C, Stubbs B, Kralj C, Koukounari A, Prince M, Prina AM. Physical activity and healthy ageing: a systematic review and meta-analysis of longitudinal cohort studies. Ageing Res Rev. 2017;38:6–17. https://doi.org/10.1016/j.arr.2017.06.003.
World Health Organisation (WHO). Strategy and action plan for healthy ageing in Europe, 2012–2020. Copenhagen: World Health Organization; 2012.
World Health Organisation (WHO). World report on ageing and health. Geneva: World Health Organization; 2015.
European Commission. Special Eurobarometer 472: sport and physical activity (wave EB88.4). Brussels: European Commission, Directorate-General for Education, Youth, Sport and Culture; 2018.
King AC, King DK. Physical activity for an aging population. Public Health Rev. 2010;32(2):401–26. https://doi.org/10.1007/BF03391609.
O’Donoghue G, Kennedy A, Puggina A, Aleksovska K, Buck C, Burns C, et al. Socio-economic determinants of physical activity across the life course : a “DEterminants of DIet and physical ACtivity” (DEDIPAC) umbrella literature review. PLoS One. 2018;13(1):e0190737. https://doi.org/10.1371/journal.pone.0190737.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077–e86. https://doi.org/10.1016/S2214-109X(18)30357-7.
Marshall SJ, Jones DA, Ainsworth BE, Reis JP, Levy SS, Macera CA. Race/ethnicity, social class, and leisure-time physical inactivity. Med Sci Sports Exerc. 2007;39(1):44–51. https://doi.org/10.1249/01.mss.0000239401.16381.37.
Pettee KK, Brach JS, Kriska AM, Boudreau R, Richardson CR, Colbert LH, et al. Influence of marital status on physical activity levels among older adults. Med Sci Sports Exerc. 2006;38(3):541–6. https://doi.org/10.1249/01.mss.0000191346.95244.f7.
Hillsdon M, Lawlor DA, Ebrahim S, Morris JN. Physical activity in older women: associations with area deprivation and with socioeconomic position over the life course: observations in the British women’s heart and health study. J Epidemiol Community Health. 2008;62(4):344–50. https://doi.org/10.1136/jech.2006.058610.
White RL, Babic MJ, Parker PD, Lubans DR, Astell-Burt T, Lonsdale C. Domain-specific physical activity and mental health: a meta-analysis. Am J Prev Med. 2017;52(5):653–66. https://doi.org/10.1016/j.amepre.2016.12.008.
Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet. 2017;390(10113):2643–54. https://doi.org/10.1016/S0140-6736(17)31634-3.
Petrovic D, de Mestral C, Bochud M, Bartley M, Kivimäki M, Vineis P, et al. The contribution of health behaviors to socioeconomic inequalities in health: a systematic review. Prev Med. 2018;113:15–31. https://doi.org/10.1016/j.ypmed.2018.05.003.
White M, Adams J, Heywood P. How and why do interventions that increase health overall widen inequalities within populations? In: Babones SJ, editor. Social inequality and public health. Bristol: Policy Press; 2009. p. 65–81. https://doi.org/10.2307/j.ctt9qgz3s.10.
Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health. 2013;67(2):190–3. https://doi.org/10.1136/jech-2012-201257.
McLaren L, McIntyre L, Kirkpatrick S. Rose’s population strategy of prevention need not increase social inequalities in health. Int J Epidemiol. 2010;39(2):372–7. https://doi.org/10.1093/ije/dyp315.
Adams J, Mytton O, White M, Monsivais P. Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLoS Med. 2016;13(4):e1001990. https://doi.org/10.1371/journal.pmed.1001990.
Backholer K, Beauchamp A, Ball K, Turrell G, Martin J, Woods J, et al. A framework for evaluating the impact of obesity prevention strategies on socioeconomic inequalities in weight. Am J Public Health. 2014;104(10):e43–50. https://doi.org/10.2105/AJPH.2014.302066.
Schüz B, Brick C, Wilding S, Conner M. Socioeconomic status moderates the effects of health cognitions on health behaviors within participants: two multibehavior studies. Ann Behav Med. 2020;54(1):36–48. https://doi.org/10.1093/abm/kaz023.
Hilz LK, Conner M, Schüz B. Social inequality, health behaviour determinants and health behaviour: a systematic review. Psychol Health. 2019. https://doi.org/10.31234/osf.io/te9uz.
Hill S, Amos A, Clifford D, Platt S. Impact of tobacco control interventions on socioeconomic inequalities in smoking: review of the evidence. Tob Control. 2014;23:e89–97.
Beauchamp A, Backholer K, Magliano D, Peeters A. The effect of obesity prevention interventions according to socioeconomic position: a systematic review. Obes Rev. 2014;15(7):541–54. https://doi.org/10.1111/obr.12161.
McGill R, Anwar E, Orton L, Bromley H, Lloyd-Williams F, O'Flaherty M, et al. Are interventions to promote healthy eating equally effective for all? Systematic review of socioeconomic inequalities in impact. BMC Public Health. 2015;15:457.
Bukman AJ, Teuscher D, Feskens EJ, van Baak MA, Meershoek A, Renes RJ. Perceptions on healthy eating, physical activity and lifestyle advice: opportunities for adapting lifestyle interventions to individuals with low socioeconomic status. BMC Public Health. 2014;14:1036. https://doi.org/10.1186/1471-2458-14-1036.
Humphreys DK, Ogilvie D. Synthesising evidence for equity impacts of population-based physical activity interventions: a pilot study. Int J Behav Nutr Phys Act. 2013;10(1):76. https://doi.org/10.1186/1479-5868-10-76.
Attwood S, van Sluijs E, Sutton S. Exploring equity in primary-care-based physical activity interventions using PROGRESS-Plus: a systematic review and evidence synthesis. Int J Behav Nutr Phys Act. 2016;13(1):60. https://doi.org/10.1186/s12966-016-0384-8.
Lehne G, Bolte G. Impact of universal interventions on social inequalities in physical activity among older adults: an equity-focused systematic review. Int J Behav Nutr Phys Act. 2017;14(1):20. https://doi.org/10.1186/s12966-017-0472-4.
Luten KA, Dijkstra A, Reijneveld SA, de Winter AF. Moderators of physical activity and healthy eating in an integrated community-based intervention for older adults. Eur J Pub Health. 2016;26(4):645–50. https://doi.org/10.1093/eurpub/ckw051.
van Uffelen JGZ, Khan A, Burton NW. Gender differences in physical activity motivators and context preferences: a population-based study in people in their sixties. BMC Public Health. 2017;17(1):624. https://doi.org/10.1186/s12889-017-4540-0.
The Lancet Public Health. Time to tackle the physical activity gender gap. Lancet Public Health. 2019;4(8):e360. https://doi.org/10.1016/S2468-2667(19)30135-5.
Koshoedo SA, Paul-Ebhohimhen VA, Jepson RG, Watson MC. Understanding the complex interplay of barriers to physical activity amongst black and minority ethnic groups in the United Kingdom: a qualitative synthesis using meta-ethnography. BMC Public Health. 2015;15(1):643. https://doi.org/10.1186/s12889-015-1893-0.
Petticrew M, Tugwell P, Kristjansson E, Oliver S, Ueffing E, Welch V. Damned if you do, damned if you don’t: subgroup analysis and equity. J Epidemiol Community Health. 2012;66(1):95–8. https://doi.org/10.1136/jech.2010.121095.
Inglis G, Archibald D, Doi L, Laird Y, Malden S, Marryat L, et al. Credibility of subgroup analyses by socioeconomic status in public health intervention evaluations: an underappreciated problem? SSM Pop Health. 2018;6:245–51. https://doi.org/10.1016/j.ssmph.2018.09.010.
De Bourdeaudhuij I, Simon C, De Meester F, Van Lenthe F, Spittaels H, Lien N, et al. Are physical activity interventions equally effective in adolescents of low and high socio-economic status (SES): results from the European Teenage project. Health Educ Res. 2011;26(1):119–30. https://doi.org/10.1093/her/cyq080.
Magnée T, Burdorf A, Brug J, Kremers SP, Oenema A, van Assema P, et al. Equity-specific effects of 26 Dutch obesity-related lifestyle interventions. Am J Prev Med. 2013;44(6):e57–66. https://doi.org/10.1016/j.amepre.2012.11.041.
Lien N, Haerens L, te Velde SJ, Mercken L, Klepp KI, Moore L, et al. Exploring subgroup effects by socioeconomic position of three effective school-based dietary interventions: the European TEENAGE project. Int J Public Health. 2014;59(3):493–502. https://doi.org/10.1007/s00038-013-0524-8.
Tinner L, Caldwell D, Hickman M, MacArthur GJ, Gottfredson D, Lana Perez A, et al. Examining subgroup effects by socioeconomic status of public health interventions targeting multiple risk behaviour in adolescence. BMC Public Health. 2018;18(1):1180. https://doi.org/10.1186/s12889-018-6042-0.
Love R, Adams J, van Sluijs EMF. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes Rev. 2019;20(6):859–70. https://doi.org/10.1111/obr.12823.
Coenen P, Robroek SJW, van der Beek AJ, Boot CRL, van Lenthe FJ, Burdorf A, et al. Socioeconomic inequalities in effectiveness of and compliance to workplace health promotion programs: an individual participant data (IPD) meta-analysis. Int J Behav Nutr Phys Act. 2020;17(1):112. https://doi.org/10.1186/s12966-020-01002-w.
Robroek SJW, Oude Hengel KM, van der Beek AJ, Boot CRL, van Lenthe FJ, Burdorf A, et al. Socio-economic inequalities in the effectiveness of workplace health promotion programmes on body mass index: an individual participant data meta-analysis. Obes Rev. 2020;21(11):e13101. https://doi.org/10.1111/obr.13101.
Moore GF, Littlecott HJ, Turley R, Waters E, Murphy S. Socioeconomic gradients in the effects of universal school-based health behaviour interventions: a systematic review of intervention studies. BMC Public Health. 2015;15(1):907.
Forberger S, Bammann K, Bauer J, Boll S, Bolte G, Brand T, et al. How to tackle key challenges in the promotion of physical activity among older adults (65+): the AEQUIPA network approach. Int J Environ Res Public Health. 2017;14(4):379.
Czwikla G, Boen F, Cook DG, de Jong J, Harris T, Hilz LK, et al. Equity-specific effects of interventions to promote physical activity among middle-aged and older adults: development of a collaborative equity-specific re-analysis strategy. Int J Environ Res Public Health. 2019;16(17):3195. https://doi.org/10.3390/ijerph16173195.
van Stralen MM, de Vries H, Mudde AN, Bolman C, Lechner L. Efficacy of two tailored interventions promoting physical activity in older adults. Am J Prev Med. 2009;37(5):405–17. https://doi.org/10.1016/j.amepre.2009.07.009.
Peels DA, van Stralen MM, Bolman C, Golsteijn RH, de Vries H, Mudde AN, et al. The differentiated effectiveness of a printed versus a Web-based tailored physical activity intervention among adults aged over 50. Health Educ Res. 2014;29(5):870–82. https://doi.org/10.1093/her/cyu039.
Pelssers J, Delecluse C, Opdenacker J, Kennis E, Van Roie E, Boen F. “Every step counts!”: effects of a structured walking intervention in a community-based senior organization. J Aging Phys Act. 2013;21(2):167–85. https://doi.org/10.1123/japa.21.2.167.
de Jong J, Lemmink KA, Stevens M, de Greef MH, Rispens P, King AC, et al. Six-month effects of the Groningen active living model (GALM) on physical activity, health and fitness outcomes in sedentary and underactive older adults aged 55-65. Patient Educ Couns. 2006;62(1):132–41. https://doi.org/10.1016/j.pec.2005.06.017.
Harris T, Kerry SM, Limb ES, Victor CR, Iliffe S, Ussher M, et al. Effect of a primary care walking intervention with and without nurse support on physical activity levels in 45- to 75-year-olds: the pedometer and consultation evaluation (PACE-UP) cluster randomised clinical trial. PLoS Med. 2017;14(1):e1002210. https://doi.org/10.1371/journal.pmed.1002210.
Harris T, Kerry SM, Victor CR, Ekelund U, Woodcock A, Iliffe S, et al. A primary care nurse-delivered walking intervention in older adults: PACE (pedometer accelerometer consultation evaluation)-Lift cluster randomised controlled trial. PLoS Med. 2015;12(2):e1001783. https://doi.org/10.1371/journal.pmed.1001783.
Iliffe S, Kendrick D, Morris R, Griffin M, Haworth D, Carpenter H, et al. Promoting physical activity in older people in general practice: ProAct65+ cluster randomised controlled trial. Br J Gen Pract. 2015;65(640):e731–8. https://doi.org/10.3399/bjgp15X687361.
Muellmann S, Buck C, Voelcker-Rehage C, Bragina I, Lippke S, Meyer J, et al. Effects of two web-based interventions promoting physical activity among older adults compared to a delayed intervention control group in northwestern Germany: results of the PROMOTE community-based intervention trial. Prev Med Rep. 2019;15:100958. https://doi.org/10.1016/j.pmedr.2019.100958.
Lee WC, Ory MG. The engagement in physical activity for middle-aged and older adults with multiple chronic conditions: findings from a community health assessment. J Aging Res. 2013;2013:152868.
Caban-Martinez AJ, Courtney TK, Chang WR, Lombardi DA, Huang YH, Brennan MJ, et al. Leisure-time physical activity, falls, and fall injuries in middle-aged adults. Am J Prev Med. 2015;49(6):888–901. https://doi.org/10.1016/j.amepre.2015.05.022.
Reiner M, Niermann C, Jekauc D, Woll A. Long-term health benefits of physical activity-a systematic review of longitudinal studies. BMC Public Health. 2013;13(1):813. https://doi.org/10.1186/1471-2458-13-813.
Hobbs N, Godfrey A, Lara J, Errington L, Meyer TD, Rochester L, et al. Are behavioral interventions effective in increasing physical activity at 12 to 36 months in adults aged 55 to 70 years? A systematic review and meta-analysis. BMC Med. 2013;11:75.
Tabuchi T, Iso H, Brunner E. Tobacco control measures to reduce socioeconomic inequality in smoking: the necessity, time-course perspective, and future implications. J Epidemiol. 2018;28(4):170–5. https://doi.org/10.2188/jea.JE20160206.
Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–29. https://doi.org/10.1016/S0140-6736(12)61031-9.
Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Beh Nutr Phys Act. 2008;5(1):56. https://doi.org/10.1186/1479-5868-5-56.
Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1423–34. https://doi.org/10.1249/mss.0b013e3180616b27.
Freedson PS, Melanson E, Sirard J. Calibration of the computer science and applications, inc. accelerometer. Med Sci Sports Exerc. 1998;30(5):777–81. https://doi.org/10.1097/00005768-199805000-00021.
Higgins JPT, Eldridge S, Li T. Chapter 23: Including variants on randomized trials. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., editors. Cochrane handbook for systematic reviews of interventions version 60 (updated September 2020): Cochrane; 2020. www.training.cochrane.org/handbook. Accessed 30 Nov 2020.
O'Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol. 2014;67(1):56–64. https://doi.org/10.1016/j.jclinepi.2013.08.005.
Galobardes B, Shaw BA, Lawlor DA, Lynch JW, Smith GD. Indicators of socioeconomic position (part1). J Epidemiol Community Health. 2006;60(1):7–12. https://doi.org/10.1136/jech.2004.023531.
Galobardes B, Shaw M, Lawlor DA, Lynch JW, Smith GD. Indicators of socioeconomic position (part 2). J Epidemiol Community Health. 2006;60(2):95–101. https://doi.org/10.1136/jech.2004.028092.
Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, et al. Socioeconomic status in health research. One size does not fit all. JAMA. 2005;294(22):2879–88. https://doi.org/10.1001/jama.294.22.2879.
Liberatos P, Link BG, Kelsey JL. The measurement of social class in epidemilogy. Epidemiol Rev. 1988;10(1):87–121. https://doi.org/10.1093/oxfordjournals.epirev.a036030.
Mena E, Bolte G, on behalf of the Advance Gender Study Group. Intersectionality-based quantitative health research and sex/gender sensitivity: a scoping review. Int J Equity Health. 2019;18(1):199.
Bauer GR. Incorporating intersectionality theory into population health research methodology: challenges and the potential to advance health equity. Soc Sci Med. 2014;110:10–7. https://doi.org/10.1016/j.socscimed.2014.03.022.
Krieger N. Genders, sexes, and health: what are the connections--and why does it matter? Int J Epidemiol. 2003;32(4):652–7. https://doi.org/10.1093/ije/dyg156.
Hammarström A, Johansson K, Annandale E, Ahlgren C, Aléx L, Christianson M, et al. Central gender theoretical concepts in health research: the state of the art. J Epidemiol Community Health. 2014;68(2):185–90. https://doi.org/10.1136/jech-2013-202572.
UNESCO Institute for Statistics. International standard classification of education: ISCED 2011. Montreal: UNESCO Institute for Statistics; 2012.
Noble M, McLennan D, Wilkinson K, Whitworth A, Barnes H. The English indices of deprivation 2007. London: Communities and Local Government; 2008.
Manzoli L, Villari P, Pirone GM, Boccia A. Marital status and mortality in the elderly: a systematic review and meta-analysis. Soc Sci Med. 2007;64(1):77–94. https://doi.org/10.1016/j.socscimed.2006.08.031.
Lehne G, Voelcker-Rehage C, Meyer J, Bammann K, Gansefort D, Brüchert T, et al. Equity impact assessment of interventions to promote physical activity among older adults: a logic model framework. Int J Environ Res Public Health. 2019;16(3):420. https://doi.org/10.3390/ijerph16030420.
Kerry SM, Morgan KE, Limb E, Cook DG, Furness C, Carey I, et al. Interpreting population reach of a large, successful physical activity trial delivered through primary care. BMC Public Health. 2018;18(1):170. https://doi.org/10.1186/s12889-018-5034-4.
Bayley A, Stahl D, Ashworth M, Cook DG, Whincup PH, Treasure J, et al. Response bias to a randomised controlled trial of a lifestyle intervention in people at high risk of cardiovascular disease: a cross-sectional analysis. BMC Public Health. 2018;18(1):1092. https://doi.org/10.1186/s12889-018-5939-y.
Greenland S, Senn SJ, Rothman KJ, Carlin JB, Poole C, Goodman SN, et al. Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol. 2016;31(4):337–50. https://doi.org/10.1007/s10654-016-0149-3.
Viechtbauer W, López-López JA, Sánchez-Meca J, Marín-Martínez F. A comparison of procedures to test for moderators in mixed-effects meta-regression models. Psychol Methods. 2015;20(3):360–74. https://doi.org/10.1037/met0000023.
Ogilvie D, Fayter D, Petticrew M, Sowden A, Thomas S, Whitehead M, et al. The harvest plot: a method for synthesising evidence about the differential effects of interventions. BMC Med Res Methodol. 2008;8(1):8. https://doi.org/10.1186/1471-2288-8-8.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Aloe AM, Thompson CG. The synthesis of partial effect sizes. J Soc Soc Work Res. 2013;4(4):390–405. https://doi.org/10.5243/jsswr.2013.24.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of individual participant data: rationale, conduct, and reporting. BMJ. 2010;340(feb05 1):c221. https://doi.org/10.1136/bmj.c221.
Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey SG. Subgroup analyses in randomised controlled trials: quantifying the risks of false positives and false negatives. Health Technol Assess. 2001;5(33):1–56. https://doi.org/10.3310/hta5330.
Acknowledgements
We are thankful to Christoph Buck, Elizabeth S. Limb, Birgit Reineke, and Steffen A. Schüle for their assistance in data analysis. Moreover, we are grateful to the German Federal Ministry of Education and Research for supporting this work.
Funding
This research is funded by the German Federal Ministry of Education and Research, funding number for University of Bremen: 01EL1822B. The funder had no role in the design of the study; in the collection, analysis, and interpretation of data; and in writing the manuscript. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
GC and GB designed the project. GC, FB, DGC, JdJ, TH, LKH, SI, RWM, SM, DAP, CRP, BS, MS, FJvL, JV, and GB developed the re-analysis strategy. FB, DGC, JdJ, TH, SI, LL, RWM, SM, DAP, CRP, MS, and JV contributed data of and/or knowledge on the primary studies. FB, DGC, JdJ, TH, SI, LL, RWM, SM, DAP, CRP, MS, and JV applied the re-analysis strategy to the data. GC assisted in applying the re-analysis strategy to the data. GC, FB, TH, SI, RWM, SM, DP, MS, JV, and GB performed the risk of bias assessment. BS and KT developed the meta-analytic approach. KT conducted the meta-analysis in R. All authors interpreted the results. GC and GB drafted the manuscript. All authors read, critically reviewed, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
For this study, ethical approval and consent to participate were not required because existing data were used and no primary data were collected.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Characteristics of intervention studies included in the collaboration. This file contains a table in which characteristics of the included intervention studies are summarized.
Additional file 2.
Definition of variables on income and area deprivation. This file contains details of how the variables on income and area deprivation were defined.
Additional file 3.
Results of Risk of Bias assessment. This file contains the detailed results of the risk of bias assessment.
Additional file 4.
Equity-specific intervention adherence. This file contains the detailed results of the equity-specific intervention adherence analyses (main and secondary analysis).
Additional file 5.
Equity-specific dropout. This file contains the results of the secondary analysis on equity-specific dropout.
Additional file 6.
Equity-specific baseline MVPA levels. This file contains information on equity-specific baseline MVPA levels (main and secondary analysis).
Additional file 7.
General and equity-specific intervention effects. This file contains the results of the general, gender-, and education-specific intervention effect analysis at T1 derived from the minimally adjusted models as well as the results of the secondary and sensitivity analyses on general and equity-specific intervention effects.
Additional file 8.
Detailed results of the meta-analyses using raw coefficients. This file contains the complete output of the random-effects meta-analysis (main and secondary analysis) using raw coefficients.
Additional file 9.
Detailed results of the meta-analyses using partial correlation coefficients. This file contains the complete output of the random-effects meta-analysis (main and secondary analysis) using partial correlation coefficients.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Czwikla, G., Boen, F., Cook, D.G. et al. Equity-specific effects of interventions to promote physical activity among middle-aged and older adults: results from applying a novel equity-specific re-analysis strategy. Int J Behav Nutr Phys Act 18, 65 (2021). https://doi.org/10.1186/s12966-021-01131-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-021-01131-w