
Abstract
Background
Policymakers in sub-Saharan Africa (SSA) face challenging decisions regarding the allocation of health resources. Economic evaluations can help decision makers to determine which health interventions should be funded and or included in their benefits package. A major problem is whether the evaluations incorporated data from sources that are reliable and relevant to the country of interest. We aimed to review the quality of the data sources used in all published economic evaluations for cardiovascular disease and diabetes in SSA.
Methods
We systematically searched selected databases for all published economic evaluations for CVD and diabetes in SSA. We modified a hierarchy of data sources and used a reference case to measure the adherence to reporting and methodological characteristics, and descriptively analysed author statements.
Results
From 7,297 articles retrieved from the search, we selected 35 for study inclusion. Most were modelled evaluations and almost all focused on pharmacological interventions. The studies adhered to the reporting standards but were less adherent to the methodological standards. The quality of data sources varied. The quality level of evidence in the data domains of resource use and costs were generally considered of high quality, with studies often sourcing information from reliable databases within the same jurisdiction. The authors of most studies referred to data sources in the discussion section of the publications highlighting the challenges of obtaining good quality and locally relevant data.
Conclusions
The data sources in some domains are considered high quality but there remains a need to make substantial improvements in the methodological adherence and overall quality of data sources to provide evidence that is sufficiently robust to support decision making in SSA within the context of UHC and health benefits plans. Many SSA governments will need to strengthen and build their capacity to conduct economic evaluations of interventions and health technology assessment for improved priority setting. This capacity building includes enhancing local infrastructures for routine data production and management. If many of the policy makers are using economic evaluations to guide resource allocation, it is imperative that the evidence used is of the feasibly highest quality.
Similar content being viewed by others

Introduction
Sub-Saharan Africa (SSA) has a high burden of non-communicable diseases (NCD) which include cardiovascular disease (CVD), diabetes, cancer, respiratory disease, and mental health conditions [1]. Despite a population of over one billion people, less than 1% of the world’s financial resources for health are spent in SSA; it has only 3% of the global health workforce, while having 24% of the global burden of disease [2]. The rising impact of NCDs in Africa have led to predictions that associated deaths would exceed those linked to maternal, perinatal, nutritional, and communicable diseases combined by 2030 [3].
Many African countries are seeking to achieve Universal Health Coverage (UHC), one of the Sustainable Development Goals (SDG), as part of ambitions to improve access to health services for their citizens [4]. However, due to economic challenges linked to a changing aid environment, a fragmented and inefficient structure of domestic and international health financing, and a lack of regulation or oversight of the private health sector, notwithstanding also the ongoing impact of the COVID-19 pandemic on health systems, achieving meaningful UHC will likely be difficult [5, 6].
Achieving UHC will in part depend on ensuring that available resources are used to maximise health benefits where possible. This can be achieved by building sustainable and locally relevant evidence-informed priority-setting systems utilising approaches such as health technology assessment (HTA) [7]. HTA aims to synthesise evidence from several disciplines to inform policy and clinical decision making around the introduction of health technologies, such as medicines, devices, and diagnostic approaches. It is a globally accepted approach for bringing together evidence on costs and clinical effectiveness, whilst also considering broader social values including equity, and is usually embedded in a well-defined multi-stakeholder process [8]. The benefits of HTA have been demonstrated in many high and upper-middle income countries by informing resource allocation decisions [9].
There are many aspects to consider when establishing HTA systems, but a core input is the availability of locally relevant data and evidence; this is especially challenging in the absence of strong health information systems [10]. For effective HTA, there is a need for high-quality data covering a number of key informational domains: epidemiology (such as prevalence and incidence of disease), clinical effectiveness, health outcomes (such as health related quality of life), resource use and costs, and equity [11]. Many SSA countries lack comprehensive and robust locally-generated data [12]. They may not have guidelines for undertaking economic evaluations within an established HTA system nor adequate capacity to conduct and assess relevant HTA studies [13]. Also lacking in most African countries are independent institutions or institutional processes to conduct HTA assessments [8]. Despite these challenges, economic evaluations focused on African settings have been undertaken, with many of these in relation to communicable disease. While fewer in number, there are published economic evaluations of NCD-related interventions in African settings but there are some concerns about their quality [14]. This has highlighted questions regarding the underpinning data sources informing key parameters in the analyses.
Methods
We aimed to explore the sources and quality of data used in economic evaluations of interventions to prevent or treat CVD and diabetes in SSA since 2000. Furthermore, we examined the content, assessed the reporting and methodological standards, and ranked the quality of evidence of the included studies.
Literature search
We conducted a systematic literature search to identify economic evaluations pertaining to SSA. We searched PubMed, Embase, Scopus, and CINAHL from 1 January 2000 to 14 August 2021. The main search terms were economic evaluations, costs, Sub-Saharan Africa, and non-communicable diseases. The studies were screened in two stages – firstly the title and abstract, and secondly the full text. We excluded evaluations published before 2000, those concerning communicable diseases, not pertaining to SSA, or not in English. We only included articles that were full economic evaluations (i.e. with both costs and outcomes of two or more interventions), peer reviewed, and in cardiovascular disease or diabetes.
Evaluation of data sources
We developed an extraction template to record four aspects: (a) general study characteristics; (b) methodological and reporting characteristics relative to an economic evaluation Reference Case developed by international experts [15]; (c) quality of data sources covering the six data domains of HTA [11, 16]; and (d) author comments on data sources and quality. Firstly, the study characteristics included general information such as the first author, institution of first author, journal, type of economic evaluation, study perspective, source of funding, discount rate, time horizon, type of model (empirical [trial-based] or model), currency, and the type of sensitivity analysis used [17, 18]. Secondly, we used the International Decision Support Initiative (iDSI) reference case [15, 19, 20] to create a checklist of 40 questions for methodological and reporting standards. Each question was assigned a 1 (yes), 0 (no or unclear). Thirdly, we ranked the quality of data sources used for six domains of data - clinical effectiveness, costs, epidemiology, quality of life (outcomes), resource use, and equity [11] - adapted from a hierarchy of evidence [16]. We ranked each individual data source within the six domains for each of the studies (where applicable) where the rankings ranged from one to six levels. For ranking of effectiveness, there may be two levels within a rank to distinguish between evidence from a meta-analysis of trials (denoted by +) and a single trial [16]. We modified the ranked order of two domains (resources and service use, and costs) to better reflect the higher ranking of expert opinion in Sub-Saharan Africa given the sparsity of data. For some domains – especially epidemiology, resource use and costs - multiple data sources were included within a data domain. We calculated the proportion of sources in each of three levels of evidence – high (ranks 1 and 2), medium (rank 3), and low (ranks 4 to 6). Lastly, we extracted information from the Discussion section of each study to examine any comments from the authors about data sources and quality [8]. We descriptively analysed the main themes from those papers that discussed the issues. We used Microsoft Excel to record data.
Results
Search results
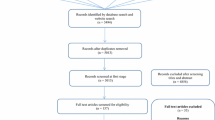
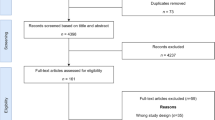
The systematic search yielded 7,297 articles but after removing duplicates there were 4,121 studies remaining (Fig. 1). Screening of titles and abstracts led to 65 full text reviews; ultimately 35 evaluations were selected [17, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54].

PRISMA flow chart
General characteristics of studies
The evaluations were published between 2000 and 2021 (Table 1, Additional File 1) and most were exclusively concerned with SSA settings, except for two: one study included South-East Asia, and another included all LMICs (only data for SSA were extracted). There were 28 (80%) cost-effectiveness analyses (CEA) where non-monetary measures of health outcomes were used, two cost-consequence analyses (6%), and four (11%) cost benefit analyses. One study modelled the impact of a tax on sugar sweetened beverages in Zambia on deaths averted, life years gained, and revenues generated [36]. The outcomes measures in the studies included: DALYs (n = 14, 40%), QALYs (n = 6, 17%), and currency (n = 4, 11%; further information on other outcomes is available in Additional File 1). Most evaluations were models (71%), the rest were empirical. Markov was the most common model type (n = 13) followed by retrospective (n = 5) and microsimulation (n = 4). The perspective of the evaluations was predominantly from the healthcare sector (n = 21, 60%), followed by society (n = 7, 20%). The interventions in the evaluations were targeted at cardiovascular disease (n = 13, 37%), non-communicable disease generally (n = 8, 23%), hypertension (n = 7, 20%), and diabetes (n = 7, 20%).
Adherence to iDSI reference case reporting standards
All the evaluations (100%) stated their intervention, outcome, and parameter sources (Table 2). Most evaluations stated the population of interest and cited parameter sources (97%), general limitations (94%), the comparator [transparency] (91%) and time horizon (91%). Most evaluations (> 80%) included a conflict-of-interest statement, funding source, clearly stated the comparator [comparators], stated the costs in local and US dollars, and stated the perspective. The weaker elements included providing budget impact estimates (54%), considerations of equity (51%), and subgroup analysis (46%, Table 2).
Three out of four evaluations indicated the use of a discount rate, and 22 studies applied a 3% discount rate for both inputs and outputs (some studies used more than one discount rate). Three of the selected studies used discount rates in sensitivity analysis that were greater than 3%; two studies applied a discount rate of 10% [22, 54]. For those six studies that did not apply discounting, in only two the stated time horizon of the analysis was short (1 year). Four in five evaluations stated a time horizon.
Adherence to iDSI reference case methodological standards
All the economic evaluations characterised the decision problem (100%), and all but one characterised the limitations and reported costs that were consistent with the perspective (97%, Table 3). Many studies (> 80%) included a declaration of interest statement, used the standard of care as the comparator, used a limited societal perspective, and reported direct health costs.
Fewer than half of the studies (< 50%) stated whether a lifetime horizon was used, performed a sensitivity analysis of parameter sources, included a budget impact assessment, or used a systematic review to identify relevant evidence. In terms of exploring uncertainty in the economic evaluation, 19 studies (54%) undertook sensitivity analysis on model structure. In terms of parameter uncertainty, 16 studies (46%) applied deterministic sensitivity analysis and 18 studies (51%) undertook probabilistic sensitivity analyses; nine studies conducted both (Table 3).
Quality of data sources
The data domains with data sourced from the pre-defined highest levels of evidence were epidemiology (34 studies; 80% high, 16% medium) and effectiveness (35 studies; 85% high, 4% medium). For epidemiological data, 46% of relevant parameters were based on data sourced from reliable databases specifically conducted for the study covering patients solely from the jurisdiction of interest. For instance, Manyema et al., (2016) identified Statistics South Africa as the primary source for population estimates by age and sex for 2012 [55] and Basu et al. (2016) used the World Health Organization Study on Global Ageing and adult health to determine population projections by age, sex and urban versus rural residence in each country [56]. In the case of effectiveness estimates, data were mostly drawn from meta-analyses and randomised controlled trials, although often from higher income settings. Notably the level of evidence in the data domains of resource use and costs were generally considered of high quality: resources and service use (35 studies; 74% high, 25% low) and costs (35 studies; 78% high, low 20%). Studies often sourced information from reliable databases that were within the same jurisdiction. These included the National Health Insurance Scheme and International Drug Price Indicator Guide in Nigeria [21]. The weakest data domains were outcome utilities (24 studies, 43% high) and equity (12 studies, 67% high).
Descriptive analysis of author comments on sources and quality
Three of four studies (n = 26, 74%) referred to data sources in the Discussion section of the publications, in many cases highlighting the challenges of obtaining good quality and locally relevant data (Additional File 1). Many of the ‘global’ or 'regional’ papers (e.g. from WHO) used regional estimates instead of country level estimates, for example [27, 29, 37]. There was often the need to use estimates from high income countries (HIC) and apply them to LMIC, particularly effectiveness estimates from trials. Authors highlighted concerns that there was an absence of rigorous data in the epidemiology domain especially with respect to risk factors, disease progression, prevalence of complications, and disease sequelae. Several authors noted that the perspective of the economic evaluation was important particularly for costs in the context of LMIC where there is high out of pocket expenditure [26, 35, 51]. Six studies made specific recommendations mostly covering empirical data collection [24, 26, 31, 32, 38, 53]. Only three studies said they explored data limitations in uncertainty analyses [36, 39, 43].
Discussion
Statement of principal findings
While authors highlighted concerns around the availability of good quality local evidence, most of the studies, particularly with respect to the domains of effectiveness and epidemiology, sourced data that were categorised as ‘high level’ in the domain-specific hierarchies of evidence applied [21, 24, 51]. Data sources within the domains of resource use and costs were generally obtained from reliable sources such as the relevant national statistics authority in the country of interest, or the International Drug Price Indicator Guide [21].
Although the reporting standards of the evaluations were high, adherence to methodological standards appeared uneven. For instance, three of five studies applied a 3% discount rate for both inputs and outputs as recommended by the iDSI Reference Case (some studies used more than one discount rate) [15]. While 3% has been adopted as a global health standard, there have been concerns that this does not reflect the economic context of LMICs, and over-values the future costs and benefits of interventions [57]. While most evaluations stated a time horizon, only 30% used a lifetime horizon as recommended by the iDSI Reference Case [15]. Typically, a lifetime horizon should be applied in economic evaluations (unless there are good reasons not to) and this is particularly relevant for NCDs given their chronic nature. It is usually appropriate to apply a time horizon that captures all relevant costs and outcomes pertaining to the decision problem.
Some studies used a Markov modelling approach to estimate benefits and costs over a longer period. Modelling approaches are more common in economic evaluations, especially for those involving the extrapolation of evidence beyond the duration of many trials [17]. Modelling analyses, compared to trial-based or empirical evaluations, generally apply longer time horizons, include more comparators, and are less restricted to generalisability issues in different settings or countries [17, 58, 59]. Furthermore, modelling approaches allow researchers to account for final patient-relevant endpoints, such as death or a cardiovascular event (e.g. stroke, myocardial infarction) rather than relying on surrogate or intermediate outcomes often measured in randomised controlled trials, such as a reduction in blood pressure or cholesterol levels [58]. We note, however, that modelling approaches are only as good as the assumptions on which they are based.
Many of the studies did not adequately explore uncertainty in their analyses. For example, only about half of the studies undertook probabilistic sensitivity analysis (PSA) despite recommendations that it should be routinely used to reflect the uncertainty in multiple parameters, and is especially important for evaluations characterised by non-linearities such as Markov models where PSA provides the best estimates of the mean costs and benefits [60]. Typically, Markov models are used in the evaluation of NCD interventions [61] and as such, the expectation is that PSA would be applied in every instance unless there are good reasons not to.
For most of the cost-effectiveness studies included, DALYs were used as the main outcome measure. Some studies included both an outcome in natural health units and a generic preference-based measure. The appropriateness or otherwise of the use of DALYs in the evaluation of NCD interventions has been debated elsewhere [62]. Nevertheless, DALYs are the most used metric in LMIC settings due to the lack of locally relevant data required to translate outcomes from clinical trials and other studies for the calculation of QALYs [15]. Increasing interest in the use of QALYs for HTA assessment in Africa has recently led to several health state valuation studies in Ethiopia and Uganda - a necessary precursor for the more widespread use of this metric [63,64,65].
The published economic evaluations we reviewed were relatively weak with respect to the quality of their reporting and methodological adherence to the iDSI Reference Case in the areas of budget impact analysis and equity. This is broadly consistent with the findings of an earlier review of cost-per DALY averted studies and their adherence to the iDSI Reference Case, which found very low levels of consideration of these aspects by the authors of included studies [19].
Strengths and weaknesses of this study
This is the first study, to our knowledge, to examine the quality of data sources across six domains in economic evaluations in SSA focused on the NCDs using a comprehensive and systematic search combined with reputable scoring systems across four aspects of economic evaluations. This study outlines as a novel approach to assessing the quality of data sources with a combination of a methods/reporting checklist (based on the iDSI Reference Case [19]) with six data domain-specific hierarchies derived from earlier studies [16].
There were some limitations with our study. Firstly, we will likely have missed studies not published in journals that were indexed in the selected databases or present in the grey literature. This may have reduced the yield as some economic evaluations conducted in LMICs are not published due to uncontrollable factors such as economic constraints [66]. Furthermore, evaluations from LMICs which are published generally reflect those of higher quality so we may have overestimated the quality of the data sources used. Secondly, the method of scoring the quality of the data sources had the potential to be skewed by one or two very good quality studies, particularly those with more sources of data. Generally, the economic evaluations which scored poorly would use only single or limited data sources for each data domain. There are other checklists for economic evaluations, such as CHEERS and Drummond [67, 68]; we reviewed these checklists and ascertained that the important elements were captured in the general characteristics and iDSI reference case standards [15].
There remains an issue regarding the applicability of evidence in a given jurisdiction when sourced from another setting, even when that evidence is judged as high quality, such as a meta-analysis of randomised controlled trials. Authors in the reviewed studies noted concerns regarding the use, for example, of trial evidence from high income settings. In our analysis, we did not explore the broader issue of evidence transferability, although we recognise this is also arguably a component of any ‘quality’ assessment. Checklists to support evidence transfer for the purpose of HTA are available, although it has been argued that more guidance may be warranted in settings with limited capacity to undertake HTA [69]. Although not specifically analysed in this study, we anecdotally noted that the overall quality of the economic evaluations improved over the twenty-year time frame. The studies ranged from rudimentary in a single setting to sophisticated and extensive economic evaluations across many countries and regions (often with many data sources). We speculate that important publications and guidance (e.g. WHO-CHOICE and the publication of guides for HTA methods including the iDSI Reference Case [15]) may have contributed to the evolution of better quality evaluations.
Strengths and weaknesses relating to other studies
The findings of this review are consistent with those found in other studies focused on LMICs. Teerawattananon et al., reported that data sources used for costs were from high quality sources (prospectively collected from reliable and local databases), and the evidence used for clinical effectiveness was of lower quality primarily obtained from single placebo-controlled clinical trials in another jurisdiction [70]. Furthermore, Prinja et al. (2015) encountered similar issues regarding the availability of evidence in India; there was a lack of locally available evidence on disability or quality of life weights, hence most cost utility analyses used utility weights from non-Indian settings [71]. In terms of the reporting and methodological results, there was a common trend seen amongst the studies. In India, it was found that the areas which required the most improvement was the perspective, justification on the type of economic evaluation used, discount rates, costing methodologies, and approaches to exploring uncertainty, especially in model-based evaluations [71]. A major weakness in the methodological and reporting standards for studies from Thailand was the lack of an incremental cost effectiveness ratio and the limited use of uncertainty (sensitivity) analyses. Overall, our results are very similar to what others have found in LMIC.
Implications for practice
Many of the problems we identified in relation to the quality of the data sources used and the reporting and methodological standards stem from a lack of robust and comprehensive local data. The lack of good quality data ultimately limits countries in SSA from generating quality evidence to support decision making. By using data of poorer quality, policy makers risk making decisions that are not suited to their local context. This becomes particularly problematic when a decision is made to fund one health intervention over another given the opportunity costs involved [15].
This study highlights the importance for SSA countries to establish effective data governance frameworks to improve the production, processing, protection, ownership, quality, openness, timeliness, relevance, accessibility, and interoperability of different types of data [72]. This can be achieved through significant investments in data technologies, platforms, and tools such as internet and mobile digital technologies. LMICs are starting to implement such systems. For instance, India has analysed the cost-effectiveness of utilising a cloud-based emergency health care information system through the use of palm vein pattern recognition [73]. It avoided misinterpretations of data amongst collectors and participants and reduced errors, physical storage issues, and security and privacy concerns [73]. The use of mobile phone-based applications to collect data in the primary care context in Ethiopia significantly improved the quality, timeliness, and processing of data [74]. Biometric fingerprint scanning in Bangladesh reduced the gap in identification by advancing the civil registration and vital statistics systems thereby enhancing epidemiological data and the monitoring of service delivery [75].
Furthermore, there needs to be greater collaboration and coordination among data collectors (government, private-sector, and civil society) to reduce duplication of results by increasing the availability and accessibility of data [72]. Both policymakers and researchers (i.e. those generating economic evaluations) need to commit to improving the production and use of data. This can be achieved by building the research capacity of those conducting economic evaluations; and creating an enabling environment for more research efforts that are locally relevant and of good quality [17]. Currently, researchers are hindered in producing high-quality research due to budget restrictions and policymakers are reluctant to use evidence derived from poorer-quality data [17]. Policymakers are encouraged to acknowledge the contribution which economic evaluations can make towards better priority setting and resource allocation.
Ongoing efforts are needed to address the political and economic issues surrounding data; there has been suboptimal engagement with policymakers to appreciate the importance of data [76]. While this study only identified whether studies declared a conflict of interest and the funding source, Glassman et al. (2012) emphasises the detrimental impact that international donors have on the quality of data in LMIC, especially when there are incentives present [9]. Misinterpretations and systematic bias have been found, where countries are reporting slower rates of growth and poverty reduction to maintain international financing [9]. This significantly impacts the quality of data produced, and future efforts will need to minimise the political interference.
Future research
As economic evaluations seek to provide evidential and analytical support for decision making, more funding for conducting research, developing technical capacity, and creating evidence related specifically to the SSA setting is required [77]. An ideal starting point would be growing data communities and investing in the primary data collectors. There are two main priorities for future research. Firstly, a major area is to review the training and level of investment of SSA countries to build the technical capacity of their researchers conducting economic evaluations; it will improve the reporting and methodological adherence. Secondly, given the dearth of locally relevant data on clinical effectiveness, we could enhance the transferability of data across jurisdictions and explore techniques combining randomised and non-randomised (‘real world’ evidence) [78]. The adaptation of evidence and evaluations from high income countries to LMICs is a possibility, but will be challenging and need resources [79]. Some studies have reviewed the existing approaches for assessing the geographic transferability of data sources [80, 81]. Goeree et al., (2011) reviewed seven unique systems for assessing transferability where there was high variability among the proposed approaches. Overall, due to the complexities in identifying appropriate weights, it still remains uncertain as to whether data sources were appropriate to be transferred [80]. We note ongoing research on the quality of reporting and data sources used in economic evaluations [82].
Conclusion
We examined the quality of data sources used in published economic evaluations in SSA in the areas of CVD and diabetes using a novel approach to rank and describe data quality. The data sources in some domains are considered high quality but there remains a need to make substantial improvements in the methodological adherence and overall quality of data sources to provide evidence that is sufficiently robust to support decision making in SSA within the context of UHC and health benefits plans. Many SSA governments will need to strengthen and build their capacity to conduct economic evaluations of interventions and health technology assessment for improved priority setting. This capacity building includes enhancing local infrastructures for routine data production and management. If many of the policy makers are using economic evaluations to guide resource allocation, it is imperative that the evidence used is of the feasibly highest quality.
Data Availability
All data necessary for interpretation of this study are contained in the manuscript and additional files.
Abbreviations
- CEA:
-
cost effectiveness analysis
- CUA:
-
cost utility analysis
- CVD:
-
cardiovascular disease
- DALY:
-
disability adjusted life year
- HTA:
-
health technology assessment
- iDSI:
-
International Decision Support Initiative
- LMIC:
-
low and middle income countries
- NCD:
-
non-communicable diseases
- PSA:
-
probabilistic sensitivity analysis
- QALY:
-
quality adjusted life year
- SDG:
-
sustainable development goals
- SSA:
-
Sub-Saharan Africa
- UHC:
-
universal health coverage
- WHO:
-
World Health Organization
References
Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-saharan Africa. Lancet Glob Health. 2019;7:e1295–6.
Anyangwe SC, Mtonga C. Inequities in the global health workforce: the greatest impediment to health in sub-saharan Africa. Int J Environ Res Public Health. 2007;4:93–100.
Global Burden of Disease Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the global burden of Disease Study 2017. Lancet. 2018;392:1684–735.
World Health Organization. : SDG Target 3.8 | Achieve universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all. 2023.
Russo G, Bloom G, McCoy D. Universal health coverage, economic slowdown and system resilience: Africa’s policy dilemma. BMJ Glob Health. 2017;2:e000400.
Verguet S, Hailu A, Eregata GT, Memirie ST, Johansson KA, Norheim OF. Toward universal health coverage in the post-COVID-19 era. Nat Med. 2021;27:380–7.
Hollingworth S, Gyansa-Lutterodt M, Dsane-Selby L, Nonvignon J, Lopert R, Gad M, Ruiz F, Tunis S, Chalkidou K. Implementing health technology assessment in Ghana to support universal health coverage: building relationships that focus on people, policy, and process. Int J Technol Assess Health Care. 2020;36:8–11.
Hollingworth S, Fenny AP, Yu SY, Ruiz F, Chalkidou K. Health technology assessment in sub-saharan Africa: a descriptive analysis and narrative synthesis. Cost Eff Resour Alloc. 2021;19:39.
Glassman A, Chalkidou K, Giedion U, Teerawattananon Y, Tunis S, Bump JB, Pichon-Riviere A. Priority-setting institutions in health: recommendations from a center for global development working group. Glob Heart. 2012;7:13–34.
Wiseman V, Mitton C, Doyle-Waters MM, Drake T, Conteh L, Newall AT, Onwujekwe O, Jan S. Using economic evidence to Set Healthcare Priorities in Low-Income and Lower-Middle-Income Countries: a systematic review of methodological frameworks. Health Econ. 2016;25(Suppl 1):140–61.
Downey L, Rao N, Guinness L, Asaria M, Prinja S, Sinha A, Kant R, Pandey A, Cluzeau F, Chalkidou K. Identification of publicly available data sources to inform the conduct of Health Technology Assessment in India. F1000Res. 2018;7:245.
Fraser HS, Blaya J. Implementing medical information systems in developing countries, what works and what doesn’t. AMIA Annu Symp Proc. 2010;2010:232–6.
Hollingworth SA, Ruiz F, Gad M, Chalkidou K. Health technology assessment capacity at national level in sub-saharan Africa: an initial survey of stakeholders. F1000Res. 2020;9:364.
Mulligan JA, Walker D, Fox-Rushby J. Economic evaluations of non-communicable disease interventions in developing countries: a critical review of the evidence base. Cost Eff Resour Alloc. 2006;4:7.
Wilkinson T, Sculpher MJ, Claxton K, Revill P, Briggs A, Cairns JA, Teerawattananon Y, Asfaw E, Lopert R, Culyer AJ. Walker DG: the international decision support Initiative Reference Case for economic evaluation: an aid to Thought. Value Health. 2016;19:921–8.
Cooper N, Coyle D, Abrams K, Mugford M, Sutton A. Use of evidence in decision models: an appraisal of health technology assessments in the UK since 1997. J Health Serv Res Policy. 2005;10:245–50.
Aminde LN, Takah NF, Zapata-Diomedi B, Veerman JL. Primary and secondary prevention interventions for cardiovascular disease in low-income and middle-income countries: a systematic review of economic evaluations. Cost Eff Resour Alloc. 2018;16:22.
Jiang S, Ma X, Desai P, Yang L, Rascati K. A systematic review on the extent and quality of Pharmacoeconomic Publications for China. Value Health Reg Issues. 2014;3:79–86.
Emerson J, Panzer A, Cohen JT, Chalkidou K, Teerawattananon Y, Sculpher M, Wilkinson T, Walker D, Neumann PJ, Kim DD. Adherence to the iDSI reference case among published cost-per-DALY averted studies. PLoS ONE. 2019;14:e0205633.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, Augustovski F, Briggs AH, Mauskopf J, Loder E, Force CT. Consolidated Health Economic evaluation reporting Standards (CHEERS) statement. Cost Eff Resour Alloc. 2013;11:6.
Adibe MO, Aguwa CN, Ukwe CV. Cost-utility analysis of Pharmaceutical Care intervention Versus Usual Care in Management of nigerian patients with type 2 diabetes. Value Health Reg Issues. 2013;2:189–98.
Anderson AN, Moodley I, Kropman K. A south african pharmaco-economic analysis of the Acute lnfarction Ramipril Efficacy (AIRE) Study. Cardiovasc J S Afr. 2000;11:89–94.
Anderson AN, Wessels F, Moodley I, Kropman K. AT1 receptor blockers–cost-effectiveness within the south african context. S Afr Med J. 2000;90:494–8.
Basu S, Shankar V, Yudkin JS. Comparative effectiveness and cost-effectiveness of treat-to-target versus benefit-based tailored treatment of type 2 diabetes in low-income and middle-income countries: a modelling analysis. Lancet Diabetes Endocrinol. 2016;4:922–32.
Basu S, Wagner RG, Sewpaul R, Reddy P, Davies J. Implications of scaling up cardiovascular disease treatment in South Africa: a microsimulation and cost-effectiveness analysis. Lancet Glob Health. 2019;7:e270–80.
Bekele M, Norheim OF, Hailu A. Cost-effectiveness of Saxagliptin compared with glibenclamide as a second-line therapy added to Metformin for type 2 diabetes Mellitus in Ethiopia. MDM Policy Pract. 2021;6:23814683211005771.
Bertram MY, Chisholm D, Watts R, Waqanivalu T, Prasad V, Varghese C. Cost-effectiveness of Population Level and Individual Level Interventions to combat non-communicable disease in Eastern Sub-Saharan Africa and South East Asia: a WHO-CHOICE analysis. Int J Health Policy Manag. 2021;10:724–33.
Biccard BM, Sear JW, Foex P. The pharmaco-economics of peri-operative beta-blocker and statin therapy in South Africa. S Afr Med J. 2006;96:1199–202.
Coates MM, Sliwa K, Watkins DA, Zuhlke L, Perel P, Berteletti F, Eisele JL, Klassen SL, Kwan GF, Mocumbi AO, et al. An investment case for the prevention and management of rheumatic heart disease in the African Union 2021-30: a modelling study. Lancet Glob Health. 2021;9:e957–66.
Ekwunife OI, Okafor CE, Ezenduka CC, Udeogaranya PO. Cost-utility analysis of antihypertensive medications in Nigeria: a decision analysis. Cost Eff Resour Alloc. 2013;11:2.
Eregata GT, Hailu A, Stenberg K, Johansson KA, Norheim OF, Bertram MY. Generalised cost-effectiveness analysis of 159 health interventions for the Ethiopian essential health service package. Cost Eff Resour Alloc. 2021;19:2.
Gad M, Lord J, Chalkidou K, Asare B, Lutterodt MG, Ruiz F. Supporting the development of evidence-informed Policy Options: an economic evaluation of Hypertension Management in Ghana. Value Health. 2020;23:171–9.
Gaziano TA, Opie LH, Weinstein MC. Cardiovascular disease prevention with a multidrug regimen in the developing world: a cost-effectiveness analysis. Lancet. 2006;368:679–86.
Gaziano TA, Steyn K, Cohen DJ, Weinstein MC, Opie LH. Cost-effectiveness analysis of hypertension guidelines in South Africa: absolute risk versus blood pressure level. Circulation. 2005;112:3569–76.
Gregory GA, Guo J, Klatman EL, Ahmadov GA, Besancon S, Gomez ED, Fawwad A, Ramaiya K, Wijesuriya MA, Orchard TJ, Ogle GD. Costs and outcomes of intermediate vs minimal care for youth-onset type 1 diabetes in six countries. Pediatr Diabetes. 2020;21:628–36.
Hangoma P, Bulawayo M, Chewe M, Stacey N, Downey L, Chalkidou K, Hofman K, Kamanga M, Kaluba A, Surgey G. The potential health and revenue effects of a tax on sugar sweetened beverages in Zambia. BMJ Glob Health 2020, 5.
Lin JK, Moran AE, Bibbins-Domingo K, Falase B, Pedroza Tobias A, Mandke CN, Kazi DS. Cost-effectiveness of a fixed-dose combination pill for secondary prevention of cardiovascular disease in China, India, Mexico, Nigeria, and South Africa: a modelling study. Lancet Glob Health. 2019;7:e1346–58.
Louw Q, Twizeyemariya A, Grimmer K, Leibbrandt D. Estimating the costs and benefits of stroke rehabilitation in South Africa. J Eval Clin Pract. 2020;26:1181–7.
Manyema M, Veerman LJ, Tugendhaft A, Labadarios D, Hofman KJ. Modelling the potential impact of a sugar-sweetened beverage tax on stroke mortality, costs and health-adjusted life years in South Africa. BMC Public Health. 2016;16:405.
Mash R, Kroukamp R, Gaziano T, Levitt N. Cost-effectiveness of a diabetes group education program delivered by health promoters with a guiding style in underserved communities in Cape Town, South Africa. Patient Educ Couns. 2015;98:622–6.
Ngalesoni F, Ruhago G, Mayige M, Oliveira TC, Robberstad B, Norheim OF, Higashi H. Cost-effectiveness analysis of population-based tobacco control strategies in the prevention of cardiovascular diseases in Tanzania. PLoS ONE. 2017;12:e0182113.
Ngalesoni FN, Ruhago GM, Mori AT, Robberstad B, Norheim OF. Cost-effectiveness of medical primary prevention strategies to reduce absolute risk of cardiovascular disease in Tanzania: a Markov modelling study. BMC Health Serv Res. 2016;16:185.
Ortegon M, Lim S, Chisholm D, Mendis S. Cost effectiveness of strategies to combat cardiovascular disease, diabetes, and tobacco use in sub-saharan Africa and South East Asia: mathematical modelling study. BMJ. 2012;344:e607.
Oti SO, van de Vijver S, Gomez GB, Agyemang C, Egondi T, Kyobutungi C, Stronks K. Outcomes and costs of implementing a community-based intervention for hypertension in an urban slum in Kenya. Bull World Health Organ. 2016;94:501–9.
Robberstad B, Hemed Y, Norheim OF. Cost-effectiveness of medical interventions to prevent cardiovascular disease in a sub-saharan african country–the case of Tanzania. Cost Eff Resour Alloc. 2007;5:3.
Rosendaal NT, Hendriks ME, Verhagen MD, Bolarinwa OA, Sanya EO, Kolo PM, Adenusi P, Agbede K, van Eck D, Tan SS, et al. Costs and cost-effectiveness of hypertension screening and treatment in adults with hypertension in Rural Nigeria in the context of a Health Insurance Program. PLoS ONE. 2016;11:e0157925.
Sando D, Kintu A, Okello S, Kawungezi PC, Guwatudde D, Mutungi G, Muyindike W, Menzies NA, Danaei G, Verguet S. Cost-effectiveness analysis of integrating screening and treatment of selected non-communicable diseases into HIV/AIDS treatment in Uganda. J Int AIDS Soc. 2020;23(Suppl 1):e25507.
Schouw DD, Mash R. Cost and consequence analysis of the healthy choices at work programme to prevent non-communicable diseases in a commercial power plant, South Africa. Afr J Prim Health Care Fam Med. 2020;12:e1–e8.
Stephens JH, Addepalli A, Chaudhuri S, Niyonzima A, Musominali S, Uwamungu JC, Paccione GA. Chronic disease in the community (CDCom) program: hypertension and non-communicable disease care by village health workers in rural Uganda. PLoS ONE. 2021;16:e0247464.
Subramanian S, Gakunga R, Kibachio J, Gathecha G, Edwards P, Ogola E, Yonga G, Busakhala N, Munyoro E, Chakaya J, et al. Cost and affordability of non-communicable disease screening, diagnosis and treatment in Kenya: patient payments in the private and public sectors. PLoS ONE. 2018;13:e0190113.
Tolla MT, Norheim OF, Memirie ST, Abdisa SG, Ababulgu A, Jerene D, Bertram M, Strand K, Verguet S, Johansson KA. Prevention and treatment of cardiovascular disease in Ethiopia: a cost-effectiveness analysis. Cost Eff Resour Alloc. 2016;14:10.
Verguet S, Pecenka C, Johansson KA, Memirie ST, Friberg IK, Driessen JR, Jamison DT. Health Gains and Financial Risk Protection Afforded by Treatment and Prevention of Diarrhea and Pneumonia in Ethiopia: An Extended Cost-Effectiveness Analysis. In Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2) Edited by Black RE, Laxminarayan R, Temmerman M, Walker N. Washington (DC); 2016.
Volmink HC, Bertram MY, Jina R, Wade AN, Hofman KJ. Applying a private sector capitation model to the management of type 2 diabetes in the south african public sector: a cost-effectiveness analysis. BMC Health Serv Res. 2014;14:444.
Wessels F. Is fenofibrate a cost-saving treatment for middle-aged individuals with type 2 diabetes? A south african private-sector perspective. Cardiovasc J Afr. 2010;21:43–6.
Manyema M, Veerman JL, Chola L, Tugendhaft A, Labadarios D, Hofman K. Decreasing the Burden of type 2 diabetes in South Africa: the impact of taxing Sugar-Sweetened Beverages. PLoS ONE. 2015;10:e0143050.
Kowal P, Chatterji S, Naidoo N, Biritwum R, Fan W, Lopez Ridaura R, Maximova T, Arokiasamy P, Phaswana-Mafuya N, Williams S, et al. Data resource profile: the world health organization study on global AGEing and adult health (SAGE). Int J Epidemiol. 2012;41:1631–49.
Haacker M, Hallett TB, Atun R. On discount rates for economic evaluations in global health. Health Policy Plan. 2020;35:107–14.
Briggs ADM, Wolstenholme J, Blakely T, Scarborough P. Choosing an epidemiological model structure for the economic evaluation of non-communicable disease public health interventions. Popul Health Metrics 2016, 14.
Petrou S, Gray A. Economic evaluation alongside randomised controlled trials: design, conduct, analysis, and reporting. BMJ. 2011;342:d1548–8.
Claxton K. Exploring uncertainty in cost-effectiveness analysis. PharmacoEconomics. 2008;26:781–98.
Briggs AD, Wolstenholme J, Blakely T, Scarborough P. Choosing an epidemiological model structure for the economic evaluation of non-communicable disease public health interventions. Popul Health Metr. 2016;14:17.
Mulligan J-A, Walker D, Fox-Rushby J. Economic evaluations of non-communicable disease interventions in developing countries: a critical review of the evidence base. Cost Eff Resource Allocation 2006, 4.
Welie AG, Gebretekle GB, Stolk E, Mukuria C, Krahn MD, Enquoselassie F, Fenta TG. Valuing Health State: an EQ-5D-5L value set for Ethiopians. Value Health Reg Issues. 2020;22:7–14.
Welie AG, Stolk E, Mukuria C, Belay YB, Krahn MD, Sander B, Gebretekle GB. Reliability and validity of using EQ-5D-5L among healthy and adolescents with major mental health disorders in Ethiopia. Eur J Health Econ. 2022;23:1105–19.
Yang F, Katumba KR, Roudijk B, Yang Z, Revill P, Griffin S, Ochanda PN, Lamorde M, Greco G, Seeley J, Sculpher M. Developing the EQ-5D-5L value set for Uganda using the ‘Lite’ protocol. PharmacoEconomics. 2022;40:309–21.
Thiboonboon K, Santatiwongchai B, Chantarastapornchit V, Rattanavipapong W, Teerawattananon Y. A systematic review of economic evaluation methodologies between resource-limited and resource-rich countries: a case of rotavirus vaccines. Appl Health Econ Health Policy. 2016;14:659–72.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, Augustovski F, Briggs AH, Mauskopf J, Loder E, Force CT. Consolidated Health Economic evaluation reporting Standards (CHEERS) statement. BMJ. 2013;346:f1049.
Drummond M, Tarricone R, Torbica A. Assessing the added value of health technologies: reconciling different perpsectives Value in Health 2013, 16.
Heupink LF, Peacocke EF, Saeterdal I, Chola L, Fronsdal K. Considerations for transferability of health technology assessments: a scoping review of tools, methods, and practices. Int J Technol Assess Health Care. 2022;38:e78.
Teerawattananon Y, Russel S, Mugford M. A systematic review of economic evaluation literature in Thailand- are the data good enough to be used by policy-makers? Pharmacoeconomics Pharmacoeconomics. 2007;25:467–79.
Prinja S, Nandi A, Horton S, Levin C, Laxminarayan R. Costs, Effectiveness, and Cost-Effectiveness of Selected Surgical Procedures and Platforms. In Essential Surgery: Disease Control Priorities (3rd Edition, Volume 1) Edited by Debas H, Donkor P, Gawande A, Jamison D, Kruk M, Mock C. Washington DC: The International Bank for Reconstruction and Development / The World Bank; 2015.
Chinganya O, Mansour N, Perini. Fernando, Jellema, Anne: The Africa data revolution report United Nations, Economics Committee 2015.
Karthikeyan N, Sukanesh R. Cloud based emergency health care information in India. J Med Syst. 2012;36:4031–6.
Medhanyie AA, Spigt M, Yebyo H, Little A, Tadesse K, Dinant GJ, Blanco R. Quality of routine health data collected by health workers using smartphone at primary health care in Ethiopia. Int J Med Inform. 2017;101:9–14.
Storisteanu DM, Norman TL, Grigore A, Norman TL. Biometric fingerprint system to enable rapid and accurate identification of beneficiaries. Glob Health Sci Pract. 2015;3:135–7.
Vellekoop H, Odame E, Ochalek J. Supporting a review of the benefits package of the National Health Insurance Scheme in Ghana. Cost Eff Resour Alloc. 2022;20:32.
Hollingworth SA, Downey L, Ruiz FJ, Odame E, Dsane-Selby L, Gyansa-Lutterodt M, Nonvignon J, Chalkidou K. What do we need to know? Data sources to support evidence-based decisions using health technology assessment in Ghana. Health Res Policy Syst. 2020;18:41.
Lou J, Kc S, Toh KY, Dabak S, Adler A, Ahn J, Bayani DBS, Chan K, Choiphel D, Chua B, et al. Real-world data for health technology assessment for reimbursement decisions in Asia: current landscape and a way forward. Int J Technol Assess Health Care. 2020;36:474–80.
Alshreef A, MacQuilkan K, Dawkins B, Riddin J, Ward S, Meads D, Taylor M, Dixon S, Culyer A, Ruiz F et al. Cost-effectiveness of docetaxel and paclitaxel for adjuvant treatment of early breast cancer: adaptation of a model-based economic evaluation from the United Kingdom to South Africa. Value in Health Regional Issues 2019 19 65–74.
Goeree R, He J, O’Reilly D, Tarride JE, Xie F, Lim M, Burke N. Transferability of health technology assessments and economic evaluations: a systematic review of approaches for assessment and application. Clinicoecon Outcomes Res. 2011;3:89–104.
Drummond M, Barbieri M, Cook J, Glick H, Lis J, Malik F, Reed S, Rutten F, Sculpher M, Severens J. Transferability of economic evaluations across jurisdictions: ISPOR good gesearch practices task force report. Value in Health 2009, 12.
Kim DD, Do LA, Synnott PG, Lavelle TA, Prosser LA, Wong JB, Neumann PJ. Developing Criteria for Health Economic Quality evaluation Tool. Value Health 2023.
Acknowledgements
The authors are grateful to Ms Christine Dalais from the University of Queensland Library for assistance with literature searching. We appreciate the guidance provided by Prof Stephen Birch at the University of Queensland.
Funding
This work was produced under the International Decision Support Initiative (https://idsihealth.org/), a global initiative to support decision makers in priority setting for universal health coverage. This work was funded, in part, by the Bill & Melinda Gates Foundation [OPP1202541]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission.
Author information
Authors and Affiliations
Contributions
SH instigated the study. GL and SH searched the literature. SH and GL reviewed the search results and selected the papers. GL and SH extracted the data from the studies. GL did the first draft of the manuscript with help from SH. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hollingworth, S.A., Leaupepe, GA., Nonvignon, J. et al. Economic evaluations of non-communicable diseases conducted in Sub-Saharan Africa: a critical review of data sources. Cost Eff Resour Alloc 21, 57 (2023). https://doi.org/10.1186/s12962-023-00471-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12962-023-00471-7