
Abstract
Introduction
Economic evaluation studies demonstrate the value of money in health interventions and enhance the efficiency of the healthcare system. Therefore, this study reviews published economic evaluation studies of public health interventions from 26 Middle East and North Africa (MENA) countries and examines whether they addressed the region's major health problems.
Methods
PubMed and Scopus were utilized to search for relevant articles published up to June 26, 2021. The reviewers independently selected studies, extracted data, and assessed the quality of studies using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist.
Results
The search identified 61 studies. Approximately half (28 studies; 46%) were conducted in Israel and Iran. The main areas of interest for economic evaluation studies were infectious diseases (21 studies; 34%), cancers (13 studies; 21%), and genetic disorders (nine studies; 15%). Five (8%), 39 (64%), 16 (26%), and one (2%) studies were classified as excellent, high, average, and poor quality, respectively. The mean of CHEERS checklist items reported was 80.8% (SD 14%). Reporting the structure and justification of the selected model was missed in 21 studies (37%), while price and conversion rates and the analytical methods were missed in 21 studies (34%).
Conclusions
The quantity of economic evaluation studies on public health interventions in the MENA region remains low; however, the overall quality is high to excellent. There were obvious geographic gaps across countries regarding the number and quality of studies and gaps within countries concerning disease prioritization. The observed research output, however, did not reflect current and upcoming disease burden and risk factors trends in the MENA region.
Similar content being viewed by others
Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
The purposes of health interventions are not only to diagnose, treat, or relieve diseases but also to prevent and protect against illnesses [1]. Interventions to provide safe drinking water, healthy food, and clean air, along with interventions to control vectors, control tobacco and alcohol, detect diseases, promote regular exercise and a healthy lifestyle, prevent injury and avoid risky behaviors, are deemed health interventions that could improve overall health, longevity, and productivity of communities [2, 3]. Despite their effectiveness in most cases, these public health interventions always need resources. With a limited health care budget, implementing such interventions must compete with other interventions for the same resources. Thus, to maximize health outcomes within a limited budget, health technology assessment (HTA), particularly health economics (HE) or economic evaluation studies which provide value for money derived from the investment, plays an important role in informing healthcare resource allocation decisions [4, 5]. However, compared to other health interventions, there is limited evidence in economic evaluation studies on public health intervention [4].
Despite its current limited role in policy decision-making, the number of HE articles published in the Middle East and North Africa (MENA) countries has recently increased and begun to attract the interest of policy-makers to inform priority-setting toward achieving universal health coverage (UHC) in many countries [6]. Similar to other regions, the growing demand for such kind of evidence in MENA is mainly driven by several factors, including rising healthcare costs as a result of remarkable advances and high costs of healthcare technologies, the World Health Organization (WHO)’s recommendations on the use of HTA, and the movement towards evidence-based healthcare system [5, 7]. Hence, in the face of the inevitable pressures from competing for alternative interventions, countries should direct their finite health budgets to meet the priority health needs of their populations to reach fair and efficient outcomes [8].
Furthermore, the burden of diseases and their background risk factors in the MENA region have shifted dramatically in the past decades, with wide variation across countries [9,10,11]. The region is also dealing with an epidemiological shift in burden from infectious to chronic diseases. In addition, some communicable diseases have recently re-emerged [12]. In the meantime, cardiovascular diseases (CVDs), cancers, diabetes mellitus, chronic kidney diseases, and chronic lung diseases represent a significant disease burden in the MENA region and pose a growing threat to public health [13]. These diseases impose enormous pressures on the health system and resources. Moreover, this burden increases with alarming future prevalence projections of up to 2.4 million deaths from the diseases mentioned earlier in the region in 2025 [14]. Coupled with ongoing wars and turmoil, several risk factors affect the people’s health in this region [9]. In this regard, MENA has some of the highest rates of non-communicable diseases (NCDs)-risk factors, such as high blood pressure, obesity, physical inactivity, tobacco use, and high intake of salt, sugar and fats, along with the absence of an efficient surveillance system for early-stage disease detection in most countries [15]. Therefore, MENA countries need integral strategies built on existing expertise and projects to handle the existing health challenges and the ones that may occur in the future.
Based on this background, this study aims to systematically review the characteristics and critically assess the quality of economic evaluation studies on public health interventions in MENA countries. It also aims to examine whether the economic evaluation studies have addressed the major health problems and are suitable for policy decision-making in the region. The findings of this study may support existing evidence for better allocating healthcare and research resources in the region.
Methods
This review was reported following the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) statement [16].
Data sources and search strategy
The researchers searched the literature in PubMed and Scopus for relevant articles published since databases inception up to June 26, 2021. The search strategy involved combining terms for public health interventions and economic evaluations using the Boolean ‘AND’, ‘OR’, and ‘NOT’ operators. The term "public health" was purposefully broad, and the authors expected that it would incorporate a wide array of interventions in the field. Search terms used involved the combination of the following Medical Subject Heading (MeSH) terms and keywords: (health promotion [MeSH]) OR (public health intervention [Title/Abstract]) OR (Exercise [MeSH]) OR (smoking cessation [MeSH]) OR (Mass Screening [MeSH]) OR (prevention [Title/Abstract]) OR (tobacco control [Title/Abstract]) OR (Public Policy [MeSH]) AND (cost [MeSH]) OR (Cost–Benefit Analysis [MeSH]) OR (economic evaluation [Title/Abstract]) AND (Middle East [MeSH]) OR (North Africa [MeSH]) OR (Djibouti [Title/Abstract]) OR (Mauritania [Title/Abstract]) OR (Pakistan [Title/Abstract]) OR (Palestine [Title/Abstract]) OR (Sudan [Title/Abstract]) OR (Somalia [Title/Abstract]) NOT (vaccine [MeSH]) OR (vaccination [MeSH]) OR (immunization [MeSH]) OR (immunization program [Title/Abstract]) OR (immunoprophylaxis [Title/Abstract]). The search was restricted to journal articles, studies of human subjects, and studies written in the English language.
Eligibility criteria
Economic evaluation studies (cost–benefit analyses, cost-effectiveness analyses, cost-minimization analyses, and cost-utility analyses) of public health interventions available in full text, published in English, and about at least one country in the MENA region were included in this review. In this study, the researchers adopted the comprehensive definition of the MENA region [17], which included 24 countries (i.e., Afghanistan, Algeria, Bahrain, Djibouti, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, United Arab Emirates, and Yemen). Besides, Turkey and Israel were added to the analysis as they were involved in PubMed (MeSH) definition of the Middle East region. Meanwhile, cost of illness studies and other partial economic evaluation studies were excluded. The researchers also excluded the full economic evaluation studies on vaccines (unless screening was one of the comparators) and diagnostic and therapeutic interventions. These interventions were reviewed separately in other manuscripts to ensure harmony and consistency of compared studies, thus, gaining more insight into the specific characteristics of each group of interventions [18, 19].
Study selection and data extraction
Study selection was performed independently by two reviewers (MAN and SS) according to the exclusion and inclusion criteria; first by title, followed by abstract, and finally by full-text screening. Discrepancies were resolved by discussion and consensus with another reviewer (MT). Then, identified studies were screened independently by two reviewers (MAN and MAAR) to extract (1) general information (e.g., year and country of publication, author’s affiliation, disease/risk factor domain, type of analysis, the model used, and interventions and comparators assessed); (2) methodological characteristics (e.g., the year of estimation, study population, perspective, time horizon, the discount rate, model’s internal validity, double-counting, and the type of sensitivity analysis performed); (3) source of input parameters (e.g., epidemiology, effectiveness, utility, and cost data). In addition, the source of funding, result and conclusion, cost-effectiveness threshold, and types of included costs were also extracted. Any disagreements were resolved in discussion with another reviewer (MT).
Quality assessment and appraisal
The methodological and reporting quality of each included economic evaluation study was assessed by two independent reviewers (MAN, PEND). Disagreement was resolved by discussion and consensus with the third reviewer (MT). Studies were assessed for their quality of reporting by their compliance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement [20]. Studies were then scored against each of the applicable 24 checklist items according to whether reporting was fully satisfied or did not satisfy the item requirements. Each reporting quality criterion was rated as reported (score = +), not reported if the item was missing when expected to be reported (score = −) or not applicable (NA). Subsequently, studies were classified by their percentage of applicable items as "excellent", "high", "average", or "poor" quality when they fulfilled 100%, 76–99%, 50–75%, or less than 50% of the CHEERS checklist items, respectively [18]. The overall quality of reporting was presented as a percentage score of applicable items. Studies scoring above 75% were considered of higher reporting quality.
Data management and analysis
EndNote X8 software was utilized for duplicate removal. All data extracted from the final list of included studies were entered into a pre-designed data extraction form in Microsoft Excel 2013 spreadsheet. Data synthesis involved stratifying and summarizing the evidence by intervention type, appraising the economic evaluation methods used to assess interventions, and presenting the cost-effectiveness outcomes. Then, descriptive statistics were used with percentages, mean, standard deviation (SD), and median to display the results of extracted data and evaluated items obtained in this review.
Results
Search results
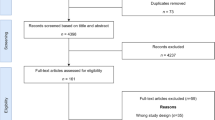
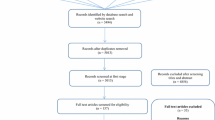
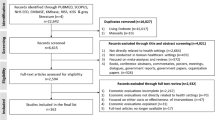
In total, 849 studies were identified following the initial search (i.e., 388 from PubMed and 461 from Scopus). The removal of 69 duplicates resulted in 780 remaining articles. Title and abstract screening resulted in the removal of 623 papers and left 157 potentially relevant studies for full article text screening. Finally, 61 studies [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81] were included in this review. The reasons for exclusion in each step are provided in the PRISMA flowchart in Fig. 1.

PRISMA flow chart of search procedure
General and methodological characteristics
This review identified economic evaluation studies on screening programs (36 studies; 59%) [21, 22, 24, 26, 28,29,30,31, 33,34,35,36,37, 39, 41, 45, 48,49,50,51,52, 54,55,56, 58, 60, 63,64,65, 70, 71, 73, 74, 79,80,81] and health promotion campaigns (four studies; 7%) [40, 46, 59, 78]. In addition, two studies concerned vector control programs [43, 68] and two studies for smoking cessation interventions [57, 66] (3% each), while the remaining 17 studies (28%) focused on other different interventions, as shown in Table 1. The main areas of interest for economic evaluation studies identified in this review were infectious diseases (21 studies; 34%) [21, 22, 25, 28,29,30,31, 33, 38, 39, 43, 44, 50, 55, 61, 62, 67, 68, 72, 75, 76], cancers (13 studies; 21%) [26, 34, 35, 37, 41, 45, 51, 54, 60, 63, 69, 71, 73], genetic disorders (nine studies; 15%) [36, 48, 49, 52, 64, 65, 70, 74, 79], CVDs (seven studies; 12%) [24, 40, 46, 59, 78, 80, 81], gestational diabetes mellitus (two studies; 3.3%) [56, 58], maternal issues (two studies; 3.3%) [27, 77], tobacco control (two studies; 3.3%) [57, 66], and other domains (five studies; 8%) [23, 32, 42, 47, 53]. Regionally, all disease domains that accounted for the highest burden (i.e., CVDs, cancers, diabetes, chronic kidney and lung diseases, and nutritional diseases and injuries) had not been adequately studied or even not studied at all in some MENA countries. Similarly, the most prevalent risk factors (smoking, physical inactivity, obesity, high blood pressure, and high intake of salt, sugar and fats) were not studied in almost all MENA countries.
Geographically, this review identified 18 studies (30%) from Israel [25, 28,29,30, 36,37,38,39,40, 52, 54, 56, 58, 65, 72, 73, 80, 81], ten studies (16%) from Iran [21, 26, 41, 45, 46, 63, 67, 68, 70, 79], and five studies from Egypt [33, 34, 50, 61, 62] and Pakistan [42,43,44, 47, 55] (8% each). Further, the researchers obtained three studies from Afghanistan [27, 31, 76], Jordan [23, 32, 57] and Lebanon [48, 49, 71] (5% each) and two studies (3%) from Turkey [64, 69]. Only one study was identified from Algeria [24], Libya [74], Morocco [60], Oman [22], Somalia [77], Syria [78] and Tunisia [35] (12% all). Additionally, five studies (8%) were conducted in more than one MENA country [51, 53, 59, 66, 75], as shown in Table 1. In this review, 57 studies (93.4%) found public health interventions to be cost-effective or even cost-saving while only four studies (6.6%) reported non-cost-effective outcomes. The general and methodological characterestics along with the data extracted from the included studies are presented in Tables 1, 2 and 3.
Quality assessment
Table 4 presents the quality assessment results using the CHEERS checklist. Overall, study quality was good, with a median of 82.6% of applicable items being met (SD 14%). Forty-four studies (72%) achieved scores above an arbitrary threshold of 75%; therefore, they were considered high quality and potentially useful in policy decision-making [18, 19, 82]. The mean (SD) of items reported was 80.8% (14%). The evaluation of reporting adequacy guided by the CHEERS checklist resulted in scores ranging from 8 (35%) to 24 (100%), as shown in Table 4. Of the 61 studies included in this review, five studies (8%) [21, 41, 44, 51, 60] were deemed to be of excellent quality and 39 studies (64%) [22,23,24, 26,27,28,29,30,31, 36,37,38,39,40, 42, 43, 45,46,47, 50, 53,54,55, 57,58,59, 61,62,63, 66, 67, 70,71,72,73,74, 76,77,78] of high quality. However, 16 studies (26%) [25, 32, 34, 35, 48, 49, 52, 56, 64, 65, 68, 69, 75, 79,80,81] and one study (2%) [33] were incomplete with respect to important methodological details and were considered to be of average and poor quality, respectively.
Against applicable CHEERS items of each study, 21 studies (37%) did not explicitly mention the modeling approach and did not provide the model structure (item 15). Data on the quantities and unit costs of the resources used, the methods of currency conversion and the exchange rates (item 14), the description of the analytical methods supporting the evaluation (item 17), and the perspective (item 6) were missed in 21 studies (34%). Similarly, 21 studies (64%) did not specify whether they dealt with heterogeneity (item 21), as shown in Table 4.
Discussion
This review identified a heterogeneous body of literature on economic evaluations of different public health interventions in MENA countries, dominated by several screening programs (n = 36; 59%). In addition, the number of published studies has been growing over time, particularly after 2013, and appears to be generated only in a few countries: Israel, Iran, Egypt, and Pakistan, contributing to 38 studies or 62% of the economic evaluation studies across all MENA countries. However, the number of published economic evaluation studies identified in this review remains very low and might not truly reflect the research efforts in the region. In this case, the actual number of economic evaluation studies on public health interventions might be higher in this region as studies are more likely to be written in local languages for submission to local authorities. Also, unlike economic evaluations of pharmaceutical products and vaccines, economic evaluation studies on public health interventions do not attract industry sponsorship; therefore, the chance of their publication is limited.
Consequently, this review found that the number of economic evaluation studies on public health interventions was lower than economic evaluation studies on diagnostic and therapeutic interventions (69 studies) [19] but higher than those on vaccines (46 studies) [18] in the MENA region. Besides, the low number of studies on public health intervention might be partly related to low public investment in public health interventions coupled with an industry-low interest in such interventions, considering that industry has contributed a large portion (32%) of the funding for economic evaluation studies in other regions [83]. The low number of innovative interventions in public health areas might also play a role. In addition, it could be explained by the fact that public health policy decision-making in many countries in the MENA region is not currently guided by the economic evaluation evidence and that there is a lack of region-specific data on important parameters such as epidemiological data and public health program effectiveness that could facilitate the conduct of economic evaluation studies. Furthermore, barriers to conducting economic evaluations still exist in this region. These barriers have been discussed elsewhere in previous studies [6, 18, 19, 84,85,86].
Moreover, several gaps were identified in this review. First is a geographical gap; there was a complete absence of economic evaluation studies from several high-income countries (i.e., Bahrain, Kuwait, Qatar, Saudi Arabia and UAE), middle-income countries (i.e., Djibouti, Iraq, Mauritania and Palestine), and low-income countries (Sudan and Yemen). In these countries, HE and HTA studies are not mandatory in decision-making [6, 18, 19, 84, 85]. Meanwhile, these countries share some common features: the lack of HTA institutionalization, the absence of national HE guidelines, the lack of HE and HTA graduate and post-graduate academic programs, the limited technical capacity to conduct economic evaluation studies, and the fragility of UHC programs [6, 18, 19, 84, 85]. Another possible explanation for the low number of economic evaluation studies in high-income and low-income countries in MENA is that high-income countries (Gulf States) have sufficient financial resources to adopt expensive interventions, while public health interventions in low-income countries are mainly funded by donors and international agencies. Based on the results of this study, 19 studies (31%) and 11 studies (18%) were conducted in high- and low-income countries, respectively. On the other hand, 29 studies (48%) were conducted in middle-income countries. These middle-income countries have faced many challenges in adopting new public health interventions under finite resources; hence, HE and HTA evidence are greatly needed to support policy decision-making. As such, an increase in the number of economic evaluation studies from these countries shortly can be expected.
While this review found that most of the identified studies were of good quality, other factors influenced the transferability or generalizability of economic evaluation results across jurisdictions. These included epidemiological data, resource use, unit costs, utility value, health care delivery pattern, and effectiveness of public health interventions. As the MENA region comprises different countries in different geographies and income levels, these parameters might not be similar across all countries. For high-income countries in the region, this review identified 19 studies. Of which, 18 were from Israel, which might limit the generalizability or transferability to other high-income countries in the region (Gulf States) due to differences in the above factors. The researchers also identified 29 studies from middle-income countries, out of which 20 studies came from Egypt, Iran, and Pakistan. In this case, the studies identified in these middle-income countries can be generalized to other countries within the same income group in the region.
Furthermore, 11 studies from low-income countries were identified. Many of them were conducted as multi-country studies, indicating the possibility of transferring their results across low-income countries. Also, it is important to note that the transferability of such findings could not be applied solely to all countries in the region. Even within the same income group in the MENA region, similarities in terms of epidemiology data, disease burden, and patterns of health care delivery should be considered when transferring economic evaluation evidence. Generally, they can be transferred to close similar countries. For example, the findings of high-quality studies conducted in Pakistan can be transferred to Afghanistan and vice versa.
Similarly, high-quality studies conducted in Algeria, Morocco, and Tunisia can be generalized among these countries. The same can be applied to Iran, Iraq, Jordan, Lebanon, and Turkey. Although there was a limited number of economic evaluation studies in the region, the authors believe that transferability could be generally made across the middle- and low-income countries in the region, as they are less heterogeneous in terms of epidemiological parameters, patterns of healthcare delivery, unit cost, and utility values. Therefore, economic evaluation evidence is suitable to inform policy decision-making in similar settings but not in the wider range of the region. However, for decision-makers, careful consideration is required when transferring and adopting economic evaluation results from studies conducted outside their countries, and more economic evaluation studies are warranted to support evidence-based policy decision-making.
Second, there is also a gap in research quality: although the quality of the included studies was generally good [44 studies (72%) achieved scores of 75% or over], there is room to improve the overall quality of HE studies in this region. Utilizing locally-generated epidemiological data, unit cost of health service, effectiveness and utility data, model calibration and validation, dealing with skewed and missing data, and testing the robustness of results are all warranted. It is also required to explicitly describe the modeling approach and provide the model structure, mention the currency conversion methods and the exchange rates, report the perspective, and deal with heterogeneity. It is noteworthy that the number and quality of economic evaluation studies conducted in countries where HE academic programs, national HE guidelines, and HTA agencies exist (i.e., Egypt, Iran, Israel, Turkey, and Tunisia) tend to be much better than studies performed in countries where HE academic programs and guidelines are still inexistent.
As revealed by this study’s results, more than half of the studies conducted in the region (33 studies; 54%) were performed in 3 countries (i.e., Israel, Iran, and Egypt), where HTA and HE had formal roles in the decision-making process [18, 19]. Besides, the researchers observed that studies performed by health economists and public health professionals tended to be of better quality than studies performed by clinicians. Furthermore, the researchers noticed the relationship between the year of publication and the overall quality of the study. Studies published since 2015 tended to be of better quality than the previous studies. It may be due to the development of standards and guidelines aimed to ensure the quality of reporting in the HE field.
This study’s results showed that the economic evaluation studies were conducted for the following diseases: infectious diseases (21 studies; 34%), cancers (13 studies; 21%), genetic disorders (nine studies; 15%), CVDs (seven studies; 12%), and other disease domains including maternal diseases, back pain, malnutrition, gestational diabetes mellitus, and mental diseases (11 studies; 18%). The observed research output did not adequately reflect the current and upcoming disease burden and risk factors trends in the MENA region. Currently, several MENA countries have some of the highest rates of NCD-risk factors, such as high blood pressure, obesity, physical inactivity, tobacco use, and high intake of salt, sugar and fats [15, 87]. Likewise, many diseases, such as CVDs, cancers, diabetes, and chronic lung and kidney diseases, are serious public health issues representing a significant disease burden in the MENA region. These risk factors and diseases place enormous pressures on the health system and resources; therefore, they require significant policy attention. For example, the MENA region experienced the highest global increase in the prevalence of diabetes mellitus in 2019 (12.2% of the adult population aged 20–79 years) and is expected to witness the second-highest increase (96%) in this prevalence between 2019 and 2045 compared to other parts of the world [88]. Similarly, a recently published review article indicated that the overall estimated pooled prevalence of hypertension in MENA was 26% and is estimated to double by 2025 [89]. Another recent study indicated that smoking prevalence was 62.7% and 27.5% among adult men and women in some MENA countries, respectively. These rates ranked among the highest worldwide [90].
On the other hand, MENA countries have witnessed many infectious disease outbreaks, such as polio outbreaks (Afghanistan, Pakistan, and Syria) and cholera outbreaks (Iraq and Yemen). Highly pathogenic and serious viral infections like hepatitis B and hepatitis C are also still an important risk of morbidity and mortality and pose a real threat to some MENA countries like Egypt. Similarly, malaria, hepatitis A virus, Chikungunya, dengue fever, cholera, diphtheria, Leishmaniasis, measles, and Rift Valley fever constitute major health, social, and economic challenges for several MENA countries [12, 91].
By the end of the study identification process, the researchers could find only one economic evaluation study on public health interventions to control and prevent COVID-19 [72]. Given the growing concern about the economic impact and value of such interventions (lockdowns, border closures, screening of suspected cases, tracing and isolating symptomatic individuals and their contacts, quarantine, personal protective equipment, and social distancing), the researchers may expect that the number of economic evaluation studies on COVID-19 interventions will increase globally, including the MENA region as these interventions have substantial economic and social consequences. In addition, a recent systematic review of these interventions suggested that screening and social distancing have been cost-effective in preventing and controlling COVID-19 over a long-time horizon. However, the evidence remains inconclusive and too heterogeneous to provide firm conclusions regarding the costs of the interventions [92]. In emergencies or epidemics such as COVID-19, it is not justified to delay policy decisions in priority areas due to the immaturity of scientific evidence (e.g., economic evaluation studies). Waiting for a better evidence base to judge the true value of potentially beneficial interventions increases the risk of infection spreading, which could have huge social and economic implications. However, decisions have to comply with the basic principles of what is considered good evidence-based decision-making practices as much as possible, while at the same time, additional data must be collected, generated, and evaluated; this strategy is called "coverage with evidence development". These decisions should be reviewed regularly as new evidence emerges [93].
Notably, there was a complete absence of economic evaluation studies on interventions targeting specific realms, such as physical inactivity, alcohol drinking, occupational health, and mental health. Previous global systematic reviews on economic evaluations of occupational health interventions also revealed no single study from the MENA region and a very limited number from other regions, indicating a great need for further research in these domains [94, 95]. Another study covering some MENA countries indicated that occupational health research is neglected, although occupational injuries have been reported to be high in these countries [91]. One potential reason for this negligence of occupational health research in MENA countries is the lack of experts or awareness about the importance of this discipline. Likewise, the lack of economic evaluation studies on mental health may result from the absence of governments’ spending on mental health, insufficient capacity, and the absence of public health interventions in this field. Following the same pattern, the lack of economic evaluation studies on interventions targeting alcohol drinking may be caused by the fact that almost all MENA countries are dominated by Muslim populations, where drinking alcohol is religiously forbidden; therefore, these countries may not bear the same burden experienced in other regions. Meanwhile, the lack of economic evaluation studies on interventions promoting physical activity despite the region's high prevalence of diabetes, obesity, and NCDs cannot be justified.
Moreover, it is noteworthy that the researchers observed that most public health interventions were significantly cost-effective or even cost-saving. Even low-intensity public health interventions can have strong positive effects on the population’s health in less developed countries and may positively impact the possibility of reducing poverty and boosting economic indicators and living standards. In this sense, a public health system that responds to the health need is a facilitator of human development since components of human capital, such as health and education, are positively correlated with the quality of the public health system [96]. It is also evident that healthier countries tend to be wealthier than countries with lower health status, a relationship known as the “Preston curve” [97]. In addition, public health interventions may generate wider economic consequences than those related to the healthcare sector alone. Investing in public health interventions, therefore, extends to many other sectors, such as education, manufacturing, commerce, tourism, and transportation [98]. Paradoxically, despite proven benefits and long-term returns on investment, public health is frequently considered a politically easy target for budget cuts, as reported in some MENA countries and elsewhere [98].
Further, the findings of this review reflect a misperception of the role of public health in communities. In this region, as in other parts of the world, the political nature of policy-making processes is apparent where policy-makers tend to advocate for curative interventions and invest in building large hospitals and medical cities as they perceive it as the best way to foster health and well‑being. However, the healthcare system has other tasks with prevention, health promotion, health education, and early disease detection even before one becomes ill and requires a hospital visit [99]. Thus, the focus must shift to upgrading the healthcare system to become more proactive, comprehensive, and integrated. As such, health issues can be addressed earlier, and quality healthcare services can be accessed once needed [100]. Guided by the WHO resolution on HTA in support of UHC [101] and motivated by the challenges of rising and escalating healthcare costs under the economic pressure these countries are suffering from, more serious local initiatives are required to establish a healthcare prioritization system (including HTA) transparently and legitimately, to ensure the sustainability of healthcare systems and to promote equitable, efficient, and high-quality healthcare services. In addition, worth mentioning that MENA countries began to implement effective interventions and policies to curb NCDs risk factors [13], yet these responses have been slow and appear not to be fully aligned with each country's social, economic, and health situations [11]. Further, these policies have largely focused on clinical and curative activities rather than preventive, educative, and promotive services.
On the other side, disease burden is commonly seen as an important criterion for low- and middle-income countries (LMICs) in national decision-making to prioritize research directions [102,103,104]. While it is indicative of the potential scale of the population that would benefit from a healthcare intervention, understanding the value of interventions that target high disease burdens requires information about the cost of those interventions and the opportunity cost of funding them. It can be operationalized using a threshold reflecting health opportunity cost. Country-specific thresholds reflecting the healthcare system, local priorities, local preferences, and ability to pay are also needed in the MENA region (see Table 3). More details and discussions were also provided in previous reviews [6, 18, 19, 84,85,86].
This study is the first systematic review of economic evaluations of public health intervention in the MENA region, highlighting under-studied disease areas to fill these clear gaps. Although the strengths of this study lie in its rigorous and systematic search strategy, broad time horizon (database inception onwards), geographic coverage of all 26-MENA countries, and the quality assessment of included studies, this study has some limitations. First, it has been difficult to include all that constitutes a ‘public health intervention’ due to terminology diffusion. As such, the researchers had limited the search to the abovementioned terms. Second, the search was limited to studies published in English identified from the two main databases: PubMed and Scopus. Hence, this review did not include technical reports, HE, HTA, and other grey literature written in local languages. Concerning this, it can be argued that government institutions may perform more economic evaluation studies, but as in some other regions, they may not choose to publish their results due to the political environment in which the decision-making process remains largely secretive with limited transparency [105]. However, the full impact of such exclusions on this study’s results still requires further identification. Therefore, further studies covering more databases (Embase, Cochrane, and Cost-Effectiveness Analysis Registry, and others), unpublished studies, and studies published in local languages are warranted. Third, this review did not include HE studies that evaluated vaccines, diagnostic tools, pharmaceutical products, or other therapeutic interventions. These studies were evaluated separately to ensure harmony and consistency of compared studies, thus, gaining more insight into the specific characteristics of each group of interventions [18, 19]. Lastly, focusing on full HE studies, partial economic evaluations such as cost-of-illness studies were excluded from this review.
Conclusions
The number of economic evaluation studies on public health interventions conducted in MENA countries has increased in the past years; however, this number was still very limited, indicating that economic evaluation evidence is not widely used to guide public health decisions in the MENA region. Geographic gaps across countries in the region were also identified concerning the number of economic evaluation studies. In addition, this review found that the number of economic evaluation studies did not align with disease domains with the highest burden and the most prevalent risk factors in some countries. It suggested that MENA governments should prioritize the disease domains and innovative interventions when funding economic evaluation studies to reflect the health burden in the region better. Although the overall quality of the reviewed studies was good—more than two-thirds of them were of high to excellent quality—and were potentially useful for policy decision-making, the limited number of studies in high- and low-income countries and the transferability issues across jurisdictions since MENA region consisted of heterogeneous countries suggested that the existing economic evaluation evidence might not be sufficient to informed policy decision-making in the wider range of the region. The commitment to adopting economic evaluation evidence for public health policy decision-making and developing economic evaluation evidence on major disease burdens are also clearly warranted for efficient public health resource allocation in the MENA region. To facilitate this, national HE guidelines and institutionalizing HTA policy should be established in all countries.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
References
World Health Organization. Continuity and coordination of care: a practice brief to support implementation of the WHO Framework on integrated people-centred health services. 2018. https://apps.who.int/iris/bitstream/handle/10665/274628/9789241514033-eng.pdf. Accessed 19 Oct 2021.
Alderwick H, Hutchings A, Briggs A, Mays N. The impacts of collaboration between local health care and non-health care organizations and factors shaping how they work: a systematic review of reviews. BMC Public Health. 2021;21(1):753.
Budreviciute A, Damiati S, Sabir DK, Onder K, Schuller-Goetzburg P, Plakys G, et al. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Public Health. 2020;8:788.
Reeves P, Edmunds K, Searles A, Wiggers J. Economic evaluations of public health implementation-interventions: a systematic review and guideline for practice. Public Health. 2019;169:101–13.
Mueller D, Tivey D, Croce D. Health-technology assessment: its role in strengthening health systems in developing countries. South Afr J Pub Health. 2017;2(1):6–11.
Fasseeh A, Karam R, Jameleddine M, George M, Kristensen FB, Al-Rabayah AA, et al. Implementation of Health Technology Assessment in the Middle East and North Africa: comparison between the current and preferred status. Front Pharmacol. 2020;11:15.
World Health Organization. A vision for primary health care in the 21st century: towards universal health coverage and the Sustainable Development Goals. Geneva: World Health Organization and the United Nations Children’s Fund (UNICEF): World Health Organization. 2018. https://apps.who.int/iris/bitstream/handle/10665/328065/WHO-HIS-SDS-2018.15-eng.pdf. Accessed 19 Oct 2021.
Wang DWL. Priority-setting and the right to health: synergies and tensions on the path to universal health coverage. Hum Rights Law Rev. 2020;20(4):704–24.
Bcheraoui CE, Charara R, Khalil I, Moradi-Lakeh M, Afshin A, Collison M, et al. Danger ahead: the burden of diseases, injuries, and risk factors in the Eastern Mediterranean Region, 1990–2015. Int J Public Health. 2018;63(1):11–23.
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22.
Aggarwal A, Patel P, Lewison G, Ekzayez A, Coutts A, Fouad FM, et al. The profile of non-communicable disease (NCD) research in the Middle East and North Africa (MENA) region: analyzing the NCD burden, research outputs and international research collaboration. PLoS ONE. 2020;15(4):e0232077.
Mostafavi E, Ghasemian A, Abdinasir A, Nematollahi Mahani SA, Rawaf S, Salehi Vaziri M, et al. Emerging and re-emerging infectious diseases in the WHO Eastern Mediterranean Region, 2001–2018. Int J Health Policy Manag. 2021.
El-Saharty S, Kaneda T, Liu AC. Tackling noncommunicable diseases in the Arab Region. Laher I, editor. Springer, Cham; 2021. p. 789–836.
World Health Organization. Burden of noncommunicable diseases in the Eastern Mediterranean Region. WHO Regional Office for Eastern Mediterranean Region; Cairo. 2015. http://www.emro.who.int/noncommunicable-diseases/publications/burden-of-noncommunicable-diseases-in-the-eastern-mediterranean-region.html. Accessed 30 April 2022.
Fikri M, Hammerich A. Scaling up action on the prevention and control of noncommunicable diseases in the WHO Eastern Mediterranean Region. East Mediterr Health J. 2018;24(1):3–4.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Abed GT, Davoodi HR. Challenges of growth and globalization in the Middle East and North Africa. International Monetary Fund; 2003.
Nagi MA, Luangsinsiri C, Thavorncharoensap M. A systematic review of economic evaluations of vaccines in Middle East and North Africa countries: is existing evidence good enough to support policy decision-making? Expert Rev Pharmacoecon Outcomes Res. 2021;21:1–20.
Nagi MA, Dewi PEN, Thavorncharoensap M, Sangroongruangsri S. A systematic review on economic evaluation studies of diagnostic and therapeutic interventions in the Middle East and North Africa. Appl Health Econ Health Policy. 2021.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. Consolidated health economic evaluation reporting standards (CHEERS)—explanation and elaboration: a report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health. 2013;16(2):231–50.
Adibi P, Rezailashkajani M, Roshandel D, Behrouz N, Ansari S, Somi MH, et al. An economic analysis of premarriage prevention of hepatitis B transmission in Iran. BMC Infect Dis. 2004;4:31.
Al Abri S, Kowada A, Yaqoubi F, Al Khalili S, Ndunda N, Petersen E. Cost-effectiveness of IGRA/QFT-Plus for TB screening of migrants in Oman. Int J Infect Dis. 2020;92:S72–7.
Al-Qudah RA, Al-Badriyeh D, Al-Ali FM, Altawalbeh SM, Basheti IA. Cost-benefit analysis of clinical pharmacist intervention in preventing adverse drug events in the general chronic diseases outpatients. J Eval Clin Pract. 2020;26(1):115–24.
Assanelli D, Levaggi R, Carré F, Sharma S, Deligiannis A, Mellwig KP, et al. Cost-effectiveness of pre-participation screening of athletes with ECG in Europe and Algeria. Intern Emerg Med. 2015;10(2):143–50.
Balicer RD, Huerta M, Davidovitch N, Grotto I. Cost-benefit of stockpiling drugs for influenza pandemic. Emerg Infect Dis. 2005;11(8):1280–2.
Barfar E, Rashidian A, Hosseini H, Nosratnejad S, Barooti E, Zendehdel K. Cost-effectiveness of mammography screening for breast cancer in a low socioeconomic group of Iranian women. Arch Iran Med. 2014;17(4):241–5.
Carvalho N, Salehi AS, Goldie SJ. National and sub-national analysis of the health benefits and cost-effectiveness of strategies to reduce maternal mortality in Afghanistan. Health Policy Plan. 2013;28(1):62–74.
Chodick G, Ashkenazi S, Livni G, Lerman Y. Cost-effectiveness of varicella vaccination of healthcare workers. Vaccine. 2005;23(43):5064–72.
Chodick G, Lerman Y, Wood F, Aloni H, Peled T, Ashkenazi S. Cost-utility analysis of hepatitis A prevention among health-care workers in Israel. J Occup Environ Med. 2002;44(2):109–15.
Chowers M, Shavit O. Economic evaluation of universal prenatal HIV screening compared with current “at risk” policy in a very low prevalence country. Sex Transm Infect. 2017;93(2):112–7.
Devine A, Howes RE, Price DJ, Moore KA, Ley B, Simpson JA, et al. Cost-effectiveness analysis of sex-stratified plasmodium vivax treatment strategies using available G6PD diagnostics to accelerate access to radical cure. Am J Trop Med Hyg. 2020;103(1):394–403.
El-Dahiyat F. Pharmacoeconomic evidence and policies to promote use of generic medicines in Jordan. Pharm Policy Law. 2017;19(1–2):71–86.
El-Ghitany EM. Cost-effectiveness of EGCRISC application versus hepatitis C virus mass screening in Egypt. J Infect Public Health. 2019;12(3):442–4.
Eltabbakh M, Zaghla H, Abdel-Razek W, Elshinnawy H, Ezzat S, Gomaa A, et al. Utility and cost-effectiveness of screening for hepatocellular carcinoma in a resource-limited setting. Med Oncol. 2015;32(1):432.
Gamaoun R. National cervical cancer prevention program in the Arab States: strategies and cost-minimization study of the Tunisian case. Vaccine. 2018;36(33):5091–6.
Ginsberg G, Tulchinsky T, Filon D, Goldfarb A, Abramov L, Rachmilevitz EA. Cost-benefit analysis of a national thalassaemia prevention programme in Israel. J Med Screen. 1998;5(3):120–6.
Ginsberg GM. Cost-utility analysis of interventions to reduce the burden of cervical cancer in Israel. Vaccine. 2013;31(Suppl 8):I46-52.
Ginsberg GM, Chemtob D. Cost utility analysis of HIV pre exposure prophylaxis among men who have sex with men in Israel. BMC Public Health. 2020;20(1):271.
Ginsberg GM, Fisher M, Ben-Shahar I, Bornstein J. Cost-utility analysis of vaccination against HPV in Israel. Vaccine. 2007;25(37–38):6677–91.
Ginsberg GM, Rosenberg E. Economic effects of interventions to reduce obesity in Israel. Isr J Health Policy Res. 2012;1(1):1–9.
Haghighat S, Akbari ME, Yavari P, Javanbakht M, Ghaffari S. Cost-effectiveness of three rounds of mammography breast cancer screening in Iranian Women. Iran J Cancer Prev. 2016;9(1):e5443.
Hamdani SU, Huma ZE, Rahman A, Wang D, Chen T, van Ommeren M, et al. Cost-effectiveness of WHO Problem Management Plus for adults with mood and anxiety disorders in a post-conflict area of Pakistan: randomised controlled trial. Br J Psychiatry. 2020;217(5):623–9.
Howard N, Guinness L, Rowland M, Durrani N, Hansen KS. Cost-effectiveness of adding indoor residual spraying to case management in Afghan refugee settlements in Northwest Pakistan during a prolonged malaria epidemic. PLoS Negl Trop Dis. 2017;11(10):e0005935.
Hussain H, Mori AT, Khan AJ, Khowaja S, Creswell J, Tylleskar T, et al. The cost-effectiveness of incentive-based active case finding for tuberculosis (TB) control in the private sector Karachi, Pakistan. BMC Health Serv Res. 2019;19(1):690.
Javadinasab H, Daroudi R, Salimzadeh H, Delavari A, Vezvaie P, Malekzadeh R. Cost-effectiveness of screening colonoscopy in Iranian high risk population. Arch Iran Med. 2017;20(9):564–71.
Javanbakht M, Jamshidi AR, Baradaran HR, Mohammadi Z, Mashayekhi A, Shokraneh F, et al. Estimation and prediction of avoidable health care costs of cardiovascular diseases and type 2 diabetes through adequate dairy food consumption: a systematic review and micro simulation modeling study. Arch Iran Med. 2018;21(5):213–22.
Kashi B, Godin CM, Kurzawa ZA, Verney AMJ, Busch-Hallen JF, De-Regil LM. Multiple micronutrient supplements are more cost-effective than iron and folic acid: modeling results from 3 high-burden Asian countries. J Nutr. 2019;149(7):1222–9.
Khneisser I, Adib S, Assaad S, Megarbane A, Karam P. Cost-benefit analysis: newborn screening for inborn errors of metabolism in Lebanon. J Med Screen. 2015;22(4):182–6.
Khneisser I, Adib SM, Loiselet J, Megarbane A. Cost-benefit analysis of G6PD screening in Lebanese newborn males. J Med Liban. 2007;55(3):129–32.
Kim DD, Hutton DW, Raouf AA, Salama M, Hablas A, Seifeldin IA, et al. Cost-effectiveness model for hepatitis C screening and treatment: implications for Egypt and other countries with high prevalence. Glob Public Health. 2015;10(3):296–317.
Kim JJ, Sharma M, O’Shea M, Sweet S, Diaz M, Sancho-Garnier H, et al. Model-based impact and cost-effectiveness of cervical cancer prevention in the Extended Middle East and North Africa (EMENA). Vaccine. 2013;31(Suppl 6):G65-77.
Koren A, Profeta L, Zalman L, Palmor H, Levin C, Zamir RB, et al. Prevention of β Thalassemia in Northern Israel—a cost-benefit analysis. Mediterr J Hematol Infect Dis. 2014;6(1):e2014012.
Lahiri S, Markkanen P, Levenstein C. The cost effectiveness of occupational health interventions: preventing occupational back pain. Am J Ind Med. 2005;48(6):515–29.
Leshno M, Halpern Z, Arber N. Cost-effectiveness of colorectal cancer screening in the average risk population. Health Care Manag Sci. 2003;6(3):165–74.
Lim AG, Walker JG, Mafirakureva N, Khalid GG, Qureshi H, Mahmood H, et al. Effects and cost of different strategies to eliminate hepatitis C virus transmission in Pakistan: a modelling analysis. Lancet Glob Health. 2020;8(3):e440–50.
Lohse N, Marseille E, Kahn JG. Development of a model to assess the cost-effectiveness of gestational diabetes mellitus screening and lifestyle change for the prevention of type 2 diabetes mellitus. Int J Gynaecol Obstet. 2011;115(Suppl 1):S20–5.
Madae’en S, Obeidat N, Adeinat M. Using cost-effectiveness analysis to support policy change: varenicline and nicotine replacement therapy for smoking cessation in Jordan. J Pharm Policy Pract. 2020;13:65.
Marseille E, Lohse N, Jiwani A, Hod M, Seshiah V, Yajnik CS, et al. The cost-effectiveness of gestational diabetes screening including prevention of type 2 diabetes: application of a new model in India and Israel. J Matern Fetal Neonatal Med. 2013;26(8):802–10.
Mason H, Shoaibi A, Ghandour R, O’Flaherty M, Capewell S, Khatib R, et al. A cost effectiveness analysis of salt reduction policies to reduce coronary heart disease in four Eastern Mediterranean countries. PLoS ONE. 2014;9(1):e84445.
Messoudi W, Elmahi T, Nejjari C, Tachfouti N, Zidouh A, Saadani G, et al. Cervical cancer prevention in Morocco: a model-based cost-effectiveness analysis. J Med Econ. 2019;22(11):1153–9.
Mostafa A, El-Sayed MH, El Kassas M, Elhamamsy M, Elsisi GH. Safety-engineered syringes: an intervention to decrease hepatitis C burden in developing countries—a cost-effectiveness analysis from Egypt. Value Health Reg Issues. 2019;19:51–8.
Mostafa A, Elsisi GH. A cost-effectiveness analysis of the use of safety-engineered syringes in reducing HBV, HCV, and HIV burden in Egypt. Expert Rev Med Devices. 2019;16(2):155–63.
Nahvijou A, Daroudi R, Tahmasebi M, Amouzegar Hashemi F, Rezaei Hemami M, Akbari Sari A, et al. Cost-effectiveness of different cervical screening strategies in Islamic Republic of Iran: a middle-income country with a low incidence rate of cervical cancer. PLoS ONE. 2016;11(6):e0156705.
Ökem ZG, Örgül G, Kasnakoglu BT, Çakar M, Beksaç MS. Economic analysis of prenatal screening strategies for Down syndrome in singleton pregnancies in Turkey. Eur J Obstet Gynecol Reprod Biol. 2017;219:40–4.
Ornoy A, Spivak A. Cost effectiveness of optimal treatment of ADHD in Israel: a suggestion for national policy. Health Econ Rev. 2019;9(1):24.
Ranson MK, Jha P, Chaloupka FJ, Nguyen SN. Global and regional estimates of the effectiveness and cost-effectiveness of price increases and other tobacco control policies. Nicotine Tob Res. 2002;4(3):311–9.
Rashidian A, Alinia C, Majdzadeh R. Cost-effectiveness analysis of health care waste treatment facilities in iran hospitals; a provider perspective. Iran J Public Health. 2015;44(3):352–60.
Rezaei-Hemami M, Akbari-Sari A, Raiesi A, Vatandoost H, Majdzadeh R. Cost effectiveness of malaria interventions from preelimination through elimination: a study in Iran. J Arthropod Borne Dis. 2014;8(1):43–52.
Saygili M, Çelik Y. An evaluation of the cost-effectiveness of the different palliative care models available to cancer patients in Turkey. Eur J Cancer Care (Engl). 2019;28(5):e13110.
Shamshiri AR, Yarahmadi S, Forouzanfar MH, Haghdoost AA, Hamzehloo G, Holakouie NK. Evaluation of current guthrie TSH cut-off point in Iran congenital hypothyroidism screening program: a cost-effectiveness analysis. Arch Iran Med. 2012;15(3):136–41.
Sharma M, Seoud M, Kim JJ. Cost-effectiveness of increasing cervical cancer screening coverage in the Middle East: an example from Lebanon. Vaccine. 2017;35(4):564–9.
Shlomai A, Leshno A, Sklan EH, Leshno M. Modeling social distancing strategies to prevent SARS-CoV-2 spread in Israel: a cost-effectiveness analysis. Value Health. 2020.
Shmueli A, Fraifeld S, Peretz T, Gutfeld O, Gips M, Sosna J, et al. Cost-effectiveness of baseline low-dose computed tomography screening for lung cancer: the Israeli experience. Value Health. 2013;16(6):922–31.
Sladkevicius E, Pollitt RJ, Mgadmi A, Guest JF. Cost effectiveness of establishing a neonatal screening programme for phenylketonuria in Libya. Appl Health Econ Health Policy. 2010;8(6):407–20.
Verguet S, Stalcup M, Walsh JA. Where to deploy pre-exposure prophylaxis (PrEP) in sub-Saharan Africa? Sex Transm Infect. 2013;89(8):628–34.
Vijayaraghavan M, Lievano F, Cairns L, Wolfson L, Nandy R, Ansari A, et al. Economic evaluation of measles catch-up and follow-up campaigns in Afghanistan in 2002 and 2003. Disasters. 2006;30(2):256–69.
Vijayaraghavan M, Wallace A, Mirza IR, Kamadjeu R, Nandy R, Durry E, et al. Economic evaluation of a Child Health Days strategy to deliver multiple maternal and child health interventions in Somalia. J Infect Dis. 2012;205(Suppl 1):S134–40.
Wilcox ML, Mason H, Fouad FM, Rastam S, al Ali R, Page TF, et al. Cost-effectiveness analysis of salt reduction policies to reduce coronary heart disease in Syria, 2010–2020. Int J Public Health. 2015;60(Suppl 1):S23-30.
Yarahmadi S, Tabibi S, Alimohammadzadeh K, Ainy E, Gooya MM, Mojarrad M, et al. Cost-benefit and effectiveness of newborn screening of congenital hypothyroidism: findings from a national program in Iran. Int J Endocrinol Metab. 2010;8:1–6.
Yosefy C, Ginsberg G, Viskoper R, Dicker D, Gavish D. Cost-utility analysis of a national project to reduce hypertension in Israel. Cost Eff Resour Alloc. 2007;5:16.
Yosefy C, Ginsberg GM, Dicker D, Viskoper JR, Tulchinsky TH, Leibovitz E, et al. Risk factor profile and achievement of treatment goals among hypertensive patients from the Israeli Blood Pressure Control (IBPC) program–initial cost utility analysis. Blood Press. 2003;12(4):225–31.
Geng J, Yu H, Mao Y, Zhang P, Chen Y. Cost effectiveness of dipeptidyl peptidase-4 inhibitors for type 2 diabetes. Pharmacoeconomics. 2015;33(6):581–97.
Decimoni TC, Leandro R, Rozman LM, Craig D, Iglesias CP, Novaes HMD, et al. Systematic review of health economic evaluation studies developed in Brazil from 1980 to 2013. Front Public Health. 2018;6:52-.
Almazrou SH, Alaujan SS, Al-Aqeel SA. Barriers and facilitators to conducting economic evaluation studies of Gulf Cooperation Council (GCC) countries: a survey of researchers. Health Res Policy Syst. 2021;19(1):71.
Zrubka Z, Rashdan O, Gulácsi L. Health economic publications from the Middle East and North Africa Region: a scoping review of the volume and methods of research. JQSH. 2020;3(2):44–54.
Kim T, Sharma M, Teerawattananon Y, Oh C, Ong L, Hangoma P, et al. Addressing challenges in health technology assessment institutionalization for furtherance of universal health coverage through south-south knowledge exchange: lessons from Bhutan, Kenya, Thailand, and Zambia. Value Health Reg Issues. 2021;24:187–92.
Fouad H, Latif N, Ingram R, Hammerich A. Scaling up prevention and control of noncommunicable diseases in the WHO Eastern Mediterranean Region. East Mediterr Health J. 2018;24:52–62.
El-Kebbi IM, Bidikian NH, Hneiny L, Nasrallah MP. Epidemiology of type 2 diabetes in the Middle East and North Africa: Challenges and call for action. World J Diabetes. 2021;12(9):1401–25.
Khonsari NM, Shahrestanaki E, Ejtahed H-S, Djalalinia S, Sheidaei A, Hakak-Zargar B, et al. Long-term trends in hypertension prevalence, awareness, treatment, and control rate in the Middle East and North Africa: a systematic review and meta-analysis of 178 population-based studies. Curr Hypertens Rep. 2021;23(9):41.
Nagi M, Riewpaiboon A, Thavorncharoensap M. Cost of premature mortality attributable to smoking in the Middle East and North Africa. East Mediterr Health J. 2021.
Sweileh WM, Zyoud SEH, Al-Jabi SW, Sawalha AF. Public, environmental, and occupational health research activity in Arab countries: bibliometric, citation, and collaboration analysis. Arch Public Health. 2015;73(1):1.
Rezapour A, Souresrafil A, Peighambari MM, Heidarali M, Tashakori-Miyanroudi M. Economic evaluation of programs against COVID-19: a systematic review. Int J Surg (Lond Engl). 2021;85:10–8.
Kaló Z, Németh B, Zemplényi A. Can cost-effectiveness principles be ignored in urgent times? J Comp Effect Res. 2021. https://doi.org/10.2217/cer-021-0211.
Grimani K, Bergström G, Riaño-Casallas M, Aboagye E, Jensen I, Lohela-Karlsson M. Economic evaluation of occupational safety and health interventions from the employer perspective: a systematic review. J Occup Environ Med. 2017;60:1.
Do LA, Synnott PG, Ma S, Ollendorf DA. Bridging the gap: aligning economic research with disease burden. BMJ Glob Health. 2021;6(6):e005673.
Sharma R. Health and economic growth: evidence from dynamic panel data of 143 years. PLoS ONE. 2018;13(10):e0204940.
Ghimire U. The impact of health on wealth: empirical evidence. Storrs: University of Connecticut; 2020.
Masters R, Anwar E, Collins B, Cookson R, Capewell S. Return on investment of public health interventions: a systematic review. J Epidemiol Community Health. 2017;71(8):827–34.
Ross AM, de Saxe ZL. Prevention, health promotion, and social work: aligning health and human service systems through a workforce for health. Am J Public Health. 2020;110(S2):S186–90.
Islam QM. Innovation in primary healthcare in the twenty-first century. J Health Manag. 2021;23(1):129–42.
World Health Organization. World Health Assembly, 67. (2014). Health intervention and technology assessment in support of universal health coverage. 2014. https://apps.who.int/iris/handle/10665/162870. Accessed 29 Oct 2021.
van der Putten IM, Evers SM, Deogaonkar R, Jit M, Hutubessy RC. Stakeholders’ perception on including broader economic impact of vaccines in economic evaluations in low and middle income countries: a mixed methods study. BMC Public Health. 2015;15:356.
Youngkong S, Kapiriri L, Baltussen R. Setting priorities for health interventions in developing countries: a review of empirical studies. Trop Med Int Health. 2009;14(8):930–9.
Haider MS, Youngkong S, Thavorncharoensap M, Thokala P. Priority setting of vaccine introduction in Bangladesh: a multicriteria decision analysis study. BMJ Open. 2022;12(2):e054219.
Butt T, Liu GG, Kim DD, Neumann PJ. Taking stock of cost-effectiveness analysis of healthcare in China. BMJ Glob Health. 2019;4(3):e001418.
Acknowledgements
The authors would like to gratefully acknowledge Health Technology Assessment international (HTAi), Alberta—Canada and Mahidol University, Bangkok—Thailand. The findings, interpretations, and conclusions expressed in this article do not necessarily reflect the agencies' views mentioned above.
Funding
This research did not receive any specific grant from the public, commercial, or not-for-profit funding agencies.
Author information
Authors and Affiliations
Contributions
All authors attest that they met the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. All authors contributed to the study's conception and design. Material preparation, data collection, and analysis were performed by [Mouaddh Abdulmalik Nagi], [Mustafa Ali Ali Rezq], [Sermsiri Sangroongruangsri], [Montarat Thavorncharoensap], and [Pramitha Esha Nirmala Dewi]. The first draft of the manuscript was written by [Mouaddh Abdulmalik Nagi]. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was not required for this study since it did not include human subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. It includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants, patents received or pending, or royalties.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nagi, M.A., Rezq, M.A.A., Sangroongruangsri, S. et al. Does health economics research align with the disease burden in the Middle East and North Africa region? A systematic review of economic evaluation studies on public health interventions. glob health res policy 7, 25 (2022). https://doi.org/10.1186/s41256-022-00258-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41256-022-00258-y