
Abstract
Background
Patients with critical illness due to COVID-19 exhibit increased coagulability associated with a high risk of venous thrombo-embolism (VTE). Data on prophylactic anticoagulation for these patients are limited and conflicting. The purpose of this study was to evaluate whether intermediate-dose prophylactic anticoagulation in patients with COVID-19 requiring ICU admission was associated with better outcomes compared to standard-dose prophylactic anticoagulation.
Methods
We retrospectively included adults admitted with severe COVID-19 to any of 15 ICUs, in 2020 or 2021. We compared the groups given intermediate-dose vs. standard-dose prophylactic anticoagulation. The primary outcome was all-cause day-90 mortality. Secondary outcomes were VTE (pulmonary embolism or deep vein thrombosis), ICU stay length, and adverse effects of anticoagulation.
Results
Of 1174 included patients (mean age, 63 years), 399 received standard-dose and 775 intermediate-dose prophylactic anticoagulation. Of the 211 patients who died within 90 days, 86 (21%) received intermediate and 125 (16%) standard doses. After adjustment on early corticosteroid therapy and critical illness severity, there were no significant between-group differences in day-90 mortality (hazard ratio [HR], 0.73; 95%CI, 0.52–1.04; p = 0.09) or ICU stay length (HR, 0.93; 95%CI, 0.79–1.10; p = 0.38). Intermediate-dose anticoagulation was significantly associated with fewer VTE events (HR, 0.55; 95%CI, 0.38–0.80; p < 0.001). Bleeding events occurred in similar proportions of patients in the two groups (odds ratio, 0.86; 95%CI, 0.50–1.47; p = 0.57).
Conclusions
Mortality on day 90 did not differ between the groups given standard-dose and intermediate-dose prophylactic anticoagulation, despite a higher incidence of VTE in the standard-dose group.
Similar content being viewed by others


Introduction
The inflammatory response to COVID-19 triggers coagulation disorders that can cause venous thrombo-embolism (VTE) [1,2,3,4,5]. Autopsy studies have evidenced high frequencies of both thrombotic microangiopathy, notably in the lungs, and macrovascular thrombotic events such as deep vein thrombosis (DVT) and pulmonary embolism (PE) [6, 7]. Moreover, a high incidence of clinical PE was reported early in the pandemic [8, 9]. In patients with acute respiratory distress syndrome (ARDS), the cumulative incidence of PE was 11.7% in patients with COVID-19 and 2.1% in those with other diagnoses [8, 10]. Interestingly, PE was not always associated with DVT, suggesting in situ thrombosis at sites of microangiopathy rather than migration of emboli [11]. The complex process of runaway inflammation that occurs during severe COVID-19 may contribute to vascular obstruction by inducing capillary damage, thrombosis, and even organ dysfunction [12, 13]. The high incidences of DVT and PE in patients with COVID-19 have prompted some experts to advocate higher-than-standard prophylactic anticoagulation dosages in patients with risk factors [14]. Others, however, continue to recommend standard dosages [15]. These differences of opinion may be ascribable to the lack of convincing evidence that intensified anticoagulation improves survival or decreases the duration of invasive mechanical ventilation [16]. Several observational studies in small populations demonstrated a significant reduction in VTE with intermediate- or therapeutic-dose anticoagulant regimens used for prevention [7, 13,14,15, 17], although mortality was unchanged. The REMAP-CAP randomised controlled trial of therapeutic-dose versus standard-dose prophylactic anticoagulation in patients admitted to the intensive care unit (ICU) for severe COVID-19 was stopped early because the therapeutic dosage failed to decrease the number of days without organ failures [18]. This result would not seem to support routine therapeutic-dose anticoagulation in ICU patients with COVID-19. However, D-dimer elevation at admission has been reported to be associated with greater severity and higher mortality in patients with COVID-19 [19]. Consequently, higher anticoagulant doses might be warranted in patients with early D-dimer elevation. Thus, the current evidence fails to conclusively indicate whether and when standard- or intermediate-dose prophylactic anticoagulation is optimal.
The aim of this retrospective multicentre study was to compare standard-dose vs. intermediate-dose anticoagulation used to prevent VTE in ICU patients with COVID-19-related acute respiratory failure. The primary outcome was mortality 90 days after ICU admission. Given the non-randomised design of our study, we adjusted the statistical analyses on the main known determinant of ICU mortality, namely, the SAPS II score [20], and on early corticosteroid therapy defined as started before or within 24 h after ICU admission [21].
Methods
Study design and participants
We retrospectively collected data for patients admitted to any of 15 ICUs in western France between 1 and 2020 and 31 December 2021. The data for each patient were entered into an electronic case-report form (Castor EDC, Amsterdam, The Netherlands) by the investigators in each participating centre.
Patients older than 18 years were eligible for inclusion if they required ICU admission due to severe lung disease with a positive reverse transcriptase-polymerase chain reaction test for SARS-CoV-2 in one or more upper and/or lower respiratory tract samples. Non-inclusion criteria were pregnancy, guardianship, therapeutic-dose anticoagulation for comorbidities or prevention of COVID-19-related VTE, and PE diagnosed by computed tomography pulmonary angiography (CTPA) before or within 24 h after ICU admission.
Definitions
We defined standard-dose prophylactic anticoagulation as subcutaneous low-molecular-weight heparin (usually enoxaparin in a dosage of 4000 IU/day or low-dose unfractionated heparin, usually calciparine, in a dosage of 500 IU/kg/day in two or three injections depending on body weight) [22]. We defined intermediate-dose prophylactic anticoagulation as subcutaneous low-molecular-weight heparin in a dosage of about 1 mg/kg/day [23], e.g., 6000 IU/24 h for patients with a body mass index (BMI) below < 30 kg/m2 or 4000 IU/12 hours for those with a BMI > 30 kg/m2.
The anticoagulation regimen prescribed at ICU admission followed the local protocol in each participating ICU. This regimen was kept unchanged unless thrombosis occurred. No changes in local protocols occurred during the study enrolment period.
In patients who had acute or chronic renal failure with a creatinine clearance below 30 mL/min/1.73 m2, intermediate-dose prophylactic anticoagulation was defined as unfractionated heparin with an anti-factor Xa assay target of 0.2 to 0.3 IU/mL [24].
DVT was defined as complete obstruction of a deep vein in an upper or lower limb by a thrombus formed in situ, confirmed by Doppler ultrasound [25]. Doppler ultrasound was performed when DVT was suspected during daily clinical screening by the bedside intensivist. PE was defined as complete or partial obstruction of a pulmonary main artery or branch, confirmed by CTPA. CTPA was performed routinely before or within 24 h after ICU admission.
Major bleeding was defined as type ≥ 3 bleeding according to the Bleeding Academic Research Consortium (BARC) scale [26]. Type 3 bleeding includes (a) overt bleeding responsible for a haemoglobin drop of 3–5 g/dL or leading to blood transfusion; (b) overt bleeding responsible for a haemoglobin drop of 5 g/dL or cardiac tamponade or need for surgical haemostasis or need for intravenous vasoactive drugs; and (c) intracranial or intraspinal bleeding or intraocular bleeding compromising vision. Type 4 is coronary-artery bypass grafting-related bleeding or perioperative intracranial bleeding within 48 h or need for surgical haemostasis after sternotomy closure or transfusion of 5 units of whole blood or packed red blood cells within a 48-hour period or chest-tube output of at least 2 L within a 24-hour period. Finally, type 5 includes (a) death probably due to bleeding but without imaging or autopsy confirmation and (b) fatal bleeding, either overt or confirmed by imaging or autopsy.
Outcomes
The primary outcome was mortality on day 90. We compared the primary outcome in the groups with intermediate-dose vs. standard-dose prophylactic anticoagulation. Secondary outcomes were ICU stay length, proportion of patients with VTE, and proportions of patients with major bleeding and with blood transfusion.
Data collection
At each centre, the study investigator used standardised forms to collect the data listed in Table 1; presence of co-infection; and use of antiviral agents, immunomodulatory drugs, and/or initial antibiotics.
Statistical analysis
Categorical variables were described as count (percentage) and continuous variables as mean ± SD if normally distributed and as median [interquartile range] otherwise. Normality was assessed by visual inspection of the distribution curve. For comparisons of the intermediate-dose and standard-dose groups, we applied the chi-square test or Fisher’s exact test for categorical variables and Student’s t-test or the Mann-Whitney U test for quantitative variables, as appropriate.
Day-90 mortality was compared between groups by building a Cox model adjusted for the SAPS II score [21] for early corticosteroid therapy defined as started before or within 24 h after ICU admission [27]. Centre was included as a random effect. A Kaplan-Meier plot was also produced. ICU stay length and the proportion of patients with VTE were compared between groups using a Fine-and-Gray competitive-risk model with death as the competing event and adjustment for the SAPS II score and early corticosteroid therapy [28]. Finally, we compared the sub-groups of patients with D-dimer levels no higher than 1000 ng/mL vs. higher than 1000 ng/mL at ICU admission; when the D-dimer level was unavailable, the dichotomising criterion was a fibrinogen level no higher than vs. higher than 4 g/L [20, 29].
The statistical analysis was performed using SAS software version 9.4 (SAS Institute, Cary, NC). All tests were two-sided, and p values smaller than 0.05 were considered significant.
Results
Patient characteristics
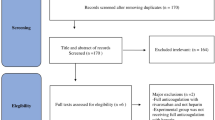
Between 1 and 2020 and 31 December 2021, 1449 patients with COVID-19 were admitted to the 15 participating ICUs. After exclusion of the 275 patients who received therapeutic-dose anticoagulation (for VTE or as required per prophylaxis by local protocol), 1174 patients were left for the analysis, including 775 in the intermediate group and 399 in the standard group (eFigure 1).
Table 1 reports the main characteristics of the patients. Disease severity assessed using the SOFA score and SAPS II was greater in the standard group. Both early corticosteroid therapy and interleukin-6-antagonist therapy were used significantly more often in the intermediate than in the standard patients. In the standard group, median time to corticosteroid initiation was 0 [-1 to 0] days, mean duration was 9.0 ± 4.5 days, and mean dosage was 80 ± 156 mg/day prednisone-equivalent, with dexamethasone used in 75% of patients; corresponding values in the intermediate group were 0 [-2 to 0] days, 9 ± 14 days, and 48 ± 31 mg/day prednisone-equivalent, with dexamethasone used in 95% of patients.
Day-90 mortality (primary outcome measure)
Table 2 reports the main outcomes of the patients. Of the 1174 patients, 211 died within 90 days, 86 (21%) in the standard group and 125 (16%) in the intermediate group (-5.4; 95% confidence interval [95%CI], -10.2 to -0.6). The Cox model comparing day-90 survival after adjustment for the SAPS II score and early corticosteroid therapy showed no significant difference between the intermediate and standard groups (hazard ratio [HR], 0.73; 95%CI, 0.52–1.04; p = 0.09) (Fig. 1).
When we compared patients with D-dimer levels no greater than vs. greater than 1000 ng/mL (or fibrinogen no greater than vs. greater than 4 g/L), we also found no significant difference in day-90 mortality (HR, 0.80; 95%CI, 0.55–1.17; p = 0.25) (eFigure 2).

Kaplan-Meier plot of day-90 survival
ICU stay length
Overall, length of stay in the ICU was 10 [4.00–22.00] days. The Fine-and-Gray competitive risk model, with death as a competing event and adjustment for the SAPS II score and early corticosteroid therapy, showed no significant difference between the two groups regarding ICU stay length (HR, 0.93; 95%CI, 0.79–1.10; p = 0.38) (eFigure 3).
Frequency of venous thrombo-embolism
Of the 1174 patients, 186 (16%) experienced at least one VTE event. Details are given in eTable1. Mean time from ICU admission to VTE diagnosis was 11 ± 9 days.
PE was diagnosed in 111 (9%) patients overall, 58 (7%) in the intermediate group and 53 (13%) in the standard group. Segmental arteries were predominantly involved (n = 60, 54%), followed by sub-segmental arteries (n = 31, 28%) then proximal arteries (n = 19, 17%). Mean time from ICU admission to PE diagnosis was 9 ± 7 days overall. PE was significantly more common in the standard than in the intermediate patients (p = 0.0005).
DVT was diagnosed in 107 (9%) patients overall, 54 (7%) in the intermediate group and 48 (12%) in the standard group. Mean time from ICU admission to DVT diagnosis was 16 ± 14 days in the intermediate and 14 ± 8 days in the standard patients. DVT was significantly more common in the standard than in the intermediate patients (p = 0.013).
In the multivariable analysis adjusted for the SAPS II score and early corticosteroid therapy, intermediate-dose prophylactic anticoagulation was significantly associated with a lower frequency of VTE (HR, 0.55; 95%CI, 0.38–0.80; p = 0.0018) (Fig. 2).

Cumulative incidence of venous thromboembolism with death as a competing event
Adverse events
Major bleeding occurred in 95 (8%) patients and blood transfusion was required in 163 (14%) patients (Table 3). By logistic regression adjusted for the SAPS II score and early corticosteroid therapy, the frequency of major bleeding and/or blood transfusion was not significantly different between the two groups (odds ratio, 0.86; 95%CI, 0.50–1.47; p = 0.57).
Discussion
In this large retrospective multicentre study, day-90 mortality was not different between groups given standard-dose vs. intermediate-dose prophylactic anticoagulation. PE and DVT each occurred in 9% of the patients overall, and both were significantly more common with the standard dose; 29 patients (2.5%) with DVT also had PE. Major bleeding was experienced by similar proportions of patients in the two groups.
VTE occurred in 16% of our patients. In a retrospective study of 184 ICU patients given at least standard-dose prophylactic anticoagulation, PE was the predominant thrombo-embolic event and was more common than in our study (14% vs. 9% overall), whereas DVT was less common (1.6% vs. 9%) [30]. In a far larger study of 3334 hospitalised patients, most of whom received standard-dose prophylactic anticoagulation, the incidences were only 3.2% for PE and 3.9% for DVT [31]. However, only a fourth of the patients required ICU admission, and in this sub-group the incidence of PE and/or DVT was 13.6%. Heterogeneity in healthcare systems, notably in the algorithms used to diagnose PE and DVT, may affect the anticoagulation strategy at the centre level [32].
In a meta-analysis with over 18 000 patients admitted to a ward or ICU for COVID-19, any anticoagulation (therapeutic, intermediate, or prophylactic) was associated with a 50% reduction in all-cause hospital mortality (relative risk, 0.50; 95% confidence interval, 0.40–0.62) [33]. The decrease in mortality was even higher in patients who required ICU admission and received therapeutic-dose anticoagulation (0.30; 0.15–0.60). However, therapeutic doses were associated with a higher risk of bleeding. Another meta-analysis, however, which had data for 5700 patients, compared standard-dose to either intermediate- or therapeutic-dose prophylactic anticoagulation and found no significant difference in hospital mortality; with the higher doses, thrombo-embolic events were less common and bleeding more common [34]. Moreover, large, well-done, randomised, controlled trials (ATTACC, ACTIV-4a, and REMAP-CAP [19]) failed to demonstrate any benefits of therapeutic-dose anticoagulation on mortality or organ dysfunction. Thus, the evidence does not support therapeutic-dose anticoagulation for prophylactic purposes in patients with critical illness due to COVID-19. The randomised controlled trial INSPIRATION in 562 ICU patients focussed on intermediate-dose prophylactic anticoagulation [35]. Compared to standard-dose prophylactic anticoagulation, the frequency of the composite primary outcome comprising 30-day mortality, venous and arterial thrombosis, and extracorporeal membrane oxygenation was not significantly different, and neither did bleeding differ in frequency, although severe thrombocytopenia occurred only in the intermediate-dose group [35]. This study cannot be readily compared to ours, however, given the difference in the primary outcome. A smaller randomised controlled trial of intermediate- vs. standard-dose prophylactic anticoagulation included 176 patients who either required ICU admission or had coagulopathy [36]. There were no differences in the primary outcome of 30-day mortality or the secondary outcomes of arteriovenous thrombosis and bleeding. A retrospective observational study compared standard thromboprophylaxis to enhanced thromboprophylaxis, which usually consisted in a higher-than-intermediate dose of 100 to 200 IU/kg/day of enoxaparin [37]. By propensity-matched analysis, ICU mortality was significantly lower with the enhanced regimen. However, the absence of a between-group difference in the frequency of thrombo-embolic events suggests potential unrecognised selection bias in this non-randomised study [37]. Finally, a retrospective review of 565 ICU patients with propensity-score matching compared standard- to intermediate-dose enoxaparin for prophylaxis [38]. The two groups were not significantly different for 30-day mortality, hospital mortality, VTE, or any thrombo-embolism. Thus, the overall body of data would not seem to support higher-than-standard doses of prophylactic anticoagulation in critically ill COVID-19 patients.
The effect of anticoagulation may vary with time of initiation, degree of coagulation activation, and severity of inflammation [39,40,41]. D-dimer elevation was associated with severe disease and death among patients with COVID-19 [42, 43]. In a meta-analysis, D-dimer levels above the upper limit of normal were significantly associated with both severe disease (relative risk [RR], 1.58; 95%CI, 1.25–2.00; p < 0.0001) and mortality (RR, 1.82; 95%CI, 1.40–2.37; p < 0.0001) [44]. In our overall population, two-thirds of patients had high D-dimer or fibrinogen levels. Despite this high prevalence, VTE occurred in only 16% of patients. Thus, the clinical relevance of high D-dimer and fibrinogen levels is unclear [45], perhaps due in part to variations in assays and in the cut-offs used to define normal ranges [46]. Importantly, day-90 mortality was not higher in patients with D-dimer or fibrinogen elevation compared to those with normal values for these parameters.
CTPA is now widely performed to detect PE in patients admitted for severe COVID-19. Data suggesting that CTPA may lead to PE overdiagnosis were reported several years before the COVID-19 pandemic [47]. In our cohort, 28% of PE cases involved sub-segmental arteries. Recent guidelines suggest withholding anticoagulation in patients with sub-segmental PE who have no risk factors for thrombosis recurrence, no evidence of DVT on serial imaging, and good cardiorespiratory reserve [48]. However, these criteria are unlikely to be met by patients with critical illness due to COVID-19. More research is needed to determine the optimal anticoagulation strategies for preventing and treating PE in patients with COVID-19.
The retrospective design is a major limitation of our study. Another is that our patients were managed over the first two years of the pandemic, during which the treatment of severe COVID-19 underwent considerable changes driven by robust scientific evidence. In particular, routine dexamethasone was introduced in July 2020 [41]. Disease severity was greater in our standard group, which received a higher mean corticosteroid dose. Dexamethasone decreases lung inflammation, thereby potentially diminishing the risk of PE. We adjusted our analysis for the use of early corticosteroid therapy but not for corticosteroid dose, which may have resulted in bias. Third, CTPA was performed routinely at or within 24 h after ICU admission, whereas Doppler ultrasonography to detect DVT was done only when DVT was suspected clinically. Moreover, repeat CTPA to diagnose PE occurring during the ICU stay was also performed only based on a clinical suspicion. Thus, PE at ICU admission may have been overdiagnosed, while DVT and PE during the ICU stay may have been underdiagnosed. Finally, mortality was lower in our study than in earlier reports [49]. One possible explanation is the younger age of our patients (62 ± 13 years). Moreover, the inclusion period extended well into the pandemic, until the end of 2021, when the management of severe COVID-19 had improved [50]. Finally, all participating ICUs were in western France, where COVID-19 had a lower incidence than in other parts of the country and, therefore, put less strain on the healthcare system. This fairly low mortality may have limited our ability to detect a difference in mortality between our two study groups.
Conclusion
Day-90 mortality did not differ between the groups given standard-dose vs. intermediate-dose prophylactic anticoagulation in the analysis adjusted for critical-illness severity and early corticosteroid therapy. However, VTE was more common in the standard-dose group. Our findings suggest that either standard-dose or intermediate-dose prophylactic anticoagulation can be used in patients with critical COVID-19 illness. Local practices might deserve to be adapted for specific sub-groups, which remain to be identified. The World Health Organisation is planning a meta-analysis that may provide information of relevance to clinical practice.
Data Availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 95%CI:
-
95% confidence interval
- ARDS:
-
acute respiratory distress syndrome
- COVID-19:
-
coronavirus disease
- CTPA:
-
computed tomography pulmonary angiography
- DVT:
-
deep vein thrombosis
- OR:
-
odds ratio
- PE:
-
pulmonary embolism
- SAPS II:
-
Simplified Acute Physiology Score version II
- SARS-CoV-2:
-
severe acute respiratory syndrome coronavirus type 2
- VTE:
-
venous thromboembolism
References
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet Lond Engl 15 févr. 2020;395(10223):507–13.
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet Lond Engl 15 févr. 2020;395(10223):497–506.
Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost JTH avr. 2020;18(4):844–7.
Llitjos JF, Leclerc M, Chochois C, Monsallier JM, Ramakers M, Auvray M, et al. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J Thromb Haemost. 2020;18(7):1743–6.
Stattin K, Lipcsey M, Andersson H, Pontén E, Bülow Anderberg S, Gradin A, et al. Inadequate prophylactic effect of low-molecular weight heparin in critically ill COVID-19 patients. J Crit Care 1 déc. 2020;60:249–52.
Ackermann M, Verleden SE, Kuehnel M, Haverich A, Welte T, Laenger F et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N Engl J Med. 9 juill 2020;383(2):120–8.
Wichmann D, Sperhake JP, Lütgehetmann M, Steurer S, Edler C, Heinemann A et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann Intern Med. 18 août 2020;173(4):268–77.
Soumagne T, Lascarrou JB, Hraiech S, Horlait G, Higny J, d’Hondt A, et al. Factors Associated with Pulmonary Embolism among Coronavirus Disease 2019 Acute Respiratory Distress Syndrome: a Multicenter Study among 375 patients. Crit Care Explor. 2020;2(7):e0166.
Boonyawat K, Chantrathammachart P, Numthavaj P, Nanthatanti N, Phusanti S, Phuphuakrat A, et al. Incidence of thromboembolism in patients with COVID-19: a systematic review and meta-analysis. Thromb J 23 nov. 2020;18(1):34.
Gong X, Yuan B, Yuan Y. Incidence and prognostic value of pulmonary embolism in COVID-19: A systematic review and meta-analysis. PLoS ONE. 14 mars 2022;17(3):e0263580.
Lax SF, Skok K, Zechner P, Kessler HH, Kaufmann N, Koelblinger C et al. Pulmonary Arterial Thrombosis in COVID-19 With Fatal Outcome: Results From a Prospective, Single-Center, Clinicopathologic Case Series.Ann Intern Med.14 mai 2020;M20-2566.
Voicu S, Ketfi C, Stépanian A, Chousterman BG, Mohamedi N, Siguret V, et al. Pathophysiological processes underlying the high prevalence of deep vein thrombosis in critically ill COVID-19 patients. Front Physiol. 2020;11:608788.
Kox M, Waalders NJB, Kooistra EJ, Gerretsen J, Pickkers P. Cytokine levels in critically ill patients with COVID-19 and other conditions. JAMA. sept 2020;3(15):1565–7.
Susen S, Tacquard CA, Godon A, Mansour A, Garrigue D, Nguyen P, et al. Prevention of thrombotic risk in hospitalized patients with COVID-19 and hemostasis monitoring. Crit Care 19 juin. 2020;24(1):364.
Cuker A, Tseng EK, Nieuwlaat R, Angchaisuksiri P, Blair C, Dane K, et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv 9 févr. 2021;5(3):872–88.
Bais B, Sozio E, De Silvestri D, Volpetti S, Zannier ME, Filì C et al. Effect of heparin treatment on pulmonary embolism and in-hospital death in unvaccinated COVID-19 patients without overt deep vein thrombosis. Thromb J. 20 juin 2022;20(1):34.
Helms J, Severac F, Merdji H, Schenck M, Clere-Jehl R, Baldacini M et al. Higher anticoagulation targets and risk of thrombotic events in severe COVID-19 patients: bi-center cohort study. Ann Intensive Care. 25 janv 2021;11(1):14.
Investigators REMAP-CAP, ACTIV-4a Investigators, Investigators ATTACC, Goligher EC, Bradbury CA, McVerry BJ et al. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N Engl J Med. 26 août 2021;385(9):777–89.
Gungor B, Atici A, Baycan OF, Alici G, Ozturk F, Tugrul S, et al. Elevated D-dimer levels on admission are associated with severity and increased risk of mortality in COVID-19: a systematic review and meta-analysis. Am J Emerg Med janv. 2021;39:173–9.
Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA. 22 déc 1993;270(24):2957–63.
The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association between Administration of systemic Corticosteroids and Mortality among critically ill patients with COVID-19: a Meta-analysis. JAMA. oct 2020;6(13):1330–41.
Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and Prevention of thrombosis, 9th ed: american college of chest Physicians evidence-based clinical practice guidelines. Chest févr. 2012;141(2 Suppl):e195S–e226S.
Antithrombotic Therapy [Internet]. COVID-19 Treatment Guidelines. [cité 7 août 2022]. Disponible sur: https://www.covid19treatmentguidelines.nih.gov/therapies/antithrombotic-therapy/
Helms J, Tacquard C, Severac F, Leonard-Lorant I, Ohana M, Delabranche X et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 4 mai 2020;1–10.
Sanchez O, Benhamou Y, Bertoletti L, Constant J, Couturaud F, Delluc A, et al. Recommandations de bonne pratique pour la prise en charge de la maladie veineuse thromboembolique chez l’adulte. Version courte. Rev Mal Respir 1 févr. 2019;36(2):249–83.
Hicks KA, Stockbridge NL, Targum SL, Temple RJ. Bleeding Academic Research Consortium consensus report: the Food and Drug Administration perspective. Circulation 14 juin. 2011;123(23):2664–5.
Lamouche-Wilquin P, Souchard J, Pere M, Raymond M, Asfar P, Darreau C, et al. Early steroids and ventilator-associated pneumonia in COVID-19-related ARDS. Crit Care Lond Engl 2 août. 2022;26(1):233.
Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 30 mars 1999;18(6):695–706.
Moores LK, Tritschler T, Brosnahan S, Carrier M, Collen JF, Doerschug K, et al. Thromboprophylaxis in patients with COVID-19: a brief update to the CHEST Guideline and Expert Panel Report. Chest juill. 2022;162(1):213–25.
Klok FA, Kruip MJHA, van der Meer NJM, Arbous MS, Gommers DAMPJ, Kant KM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res 1 juill. 2020;191:145–7.
Bilaloglu S, Aphinyanaphongs Y, Jones S, Iturrate E, Hochman J, Berger JS. Thrombosis in Hospitalized Patients With COVID-19 in a New York City Health System. JAMA. 25 août 2020;324(8):799–801.
Mesotten D, Meijs DAM, van Bussel BCT, Stessel B, Mehagnoul-Schipper J, Hana A et al. Differences and Similarities Among COVID-19 Patients Treated in Seven ICUs in Three Countries Within One Region: An Observational Cohort Study. Crit Care Med. 1 avr 2022;50(4):595–606.
Parisi R, Costanzo S, Di Castelnuovo A, de Gaetano G, Donati MB, Iacoviello L. Different anticoagulant regimens, mortality, and bleeding in hospitalized patients with COVID-19: a systematic review and an updated Meta-analysis. Semin Thromb Hemost juin. 2021;47(4):372–91.
Jorda A, Siller-Matula JM, Zeitlinger M, Jilma B, Gelbenegger G. Anticoagulant treatment regimens in patients with Covid-19: a Meta-analysis. Clin Pharmacol Ther. 2022;111(3):614–23.
Investigators INSPIRATION, Sadeghipour P, Talasaz AH, Rashidi F, Sharif-Kashani B, Beigmohammadi MT et al. Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA. 27 avr 2021;325(16):1620–30.
Perepu US, Chambers I, Wahab A, Ten Eyck P, Wu C, Dayal S, et al. Standard prophylactic versus intermediate dose enoxaparin in adults with severe COVID-19: a multi-center, open-label, randomized controlled trial. J Thromb Haemost JTH sept. 2021;19(9):2225–34.
Lavinio A, Ercole A, Battaglini D, Magnoni S, Badenes R, Taccone FS et al. Safety profile of enhanced thromboprophylaxis strategies for critically ill COVID-19 patients during the first wave of the pandemic: observational report from 28 European intensive care units. Crit Care Lond Engl. 22 avr 2021;25(1):155.
Aljuhani O, Al Sulaiman K, Hafiz A, Eljaaly K, Alharbi A, Algarni R, et al. Comparison between standard Vs. escalated dose venous thromboembolism (VTE) prophylaxis in critically ill patients with COVID-19: a two centers, observational study. Saudi Pharm J SPJ Off Publ Saudi Pharm Soc avr. 2022;30(4):398–406.
Libster R, Pérez Marc G, Wappner D, Coviello S, Bianchi A, Braem V et al. Early High-Titer Plasma Therapy to Prevent Severe Covid-19 in Older Adults. N Engl J Med. 18 févr 2021;384(7):610–8.
Salama C, Han J, Yau L, Reiss WG, Kramer B, Neidhart JD et al. Tocilizumab in Patients Hospitalized with Covid-19 Pneumonia. N Engl J Med. 7 janv 2021;384(1):20–30.
RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL et al. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med. 25 févr 2021;384(8):693–704.
Zhang L, Yan X, Fan Q, Liu H, Liu X, Liu Z, et al. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J Thromb Haemost JTH juin. 2020;18(6):1324–9.
Lippi G, Favaloro EJ. D-dimer is Associated with Severity of Coronavirus Disease 2019: a pooled analysis. Thromb Haemost mai. 2020;120(5):876–8.
Gungor B, Atici A, Baycan OF, Alici G, Ozturk F, Tugrul S, et al. Elevated D-dimer levels on admission are associated with severity and increased risk of mortality in COVID-19: a systematic review and meta-analysis. Am J Emerg Med janv. 2021;39:173–9.
Poyiadji N, Cormier P, Patel PY, Hadied MO, Bhargava P, Khanna K, et al. Acute Pulmonary Embolism and COVID-19. Radiol déc. 2020;297(3):E335–8.
Thachil J, Longstaff C, Favaloro EJ, Lippi G, Urano T, Kim PY. The need for accurate D-dimer reporting in COVID‐19: communication from the ISTH SSC on fibrinolysis. J Thromb Haemost sept. 2020;18(9):2408–11.
Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 9 mai 2011;171(9):831–7.
Carrier M, Klok FA. Symptomatic subsegmental pulmonary embolism: to treat or not to treat? Hematol Am Soc Hematol Educ Program 8 déc. 2017;2017(1):237–41.
Kloka JA, Blum LV, Old O, Zacharowski K, Friedrichson B. Characteristics and mortality of 561,379 hospitalized COVID-19 patients in Germany until December 2021 based on real-life data. Sci Rep 1 juill. 2022;12(1):11116.
COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study. Intensive Care Med janv. 2021;47(1):60–73.
Acknowledgements
We are indebted to A. Wolfe, MD, who helped to prepare and review the manuscript. We thank Mariana Ismael from Castor EDC (Amsterdam, The Netherlands) for technical support in designing the electronic case-report form.
Funding
Partially funded by Centre Hospitalier Bretagne Atlantique, Vannes, France.
Author information
Authors and Affiliations
Contributions
PLW, LP, and JBL designed and set up the study.PLW, MR, EC, and JBL enrolled the patients, collected the data, and supervised the study.MP performed the statistical analysis. PLW, LP, and JBL wrote the initial draft of the manuscript. All authors revised the manuscript several times for important intellectual content.All authors vouch for the accuracy and completeness of the data and analyses, and for the fidelity of the trial to the protocol.
Corresponding author
Ethics declarations
Competing interests
None
Ethics approval and consent to participate
This study was approved by the appropriate French ethics committee (Rennes Hospital N°20.182), which waived the need for informed consent in keeping with French legislation on retrospective healthcare studies of anonymised data. The study database was reported to the French data privacy protection authority (CNIL 22.17.312).
Consent for publication
Not applicable; however, each patient, or next of kin of incompetent patients, was informed about the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lamouche-Wilquin, P., Perrin, L., Pere, M. et al. Anticoagulation strategy and safety in critically ill COVID-19 patients: a French retrospective multicentre study. Thrombosis J 21, 42 (2023). https://doi.org/10.1186/s12959-023-00491-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12959-023-00491-6