
Abstract
Background
Guidelines on coronary intermediate lesions strongly recommend deferred revascularization after detecting a normal fractional flow reserve (FFR). Researches about triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) on cardiovascular diseases has also been well conducted. However, the association of TG/HDL-C and long-term adverse clinical outcomes remains unknown for patients deferred revascularization following FFR.
Methods
This study retrospectively included 374 coronary artery disease (CAD) patients with non-significant coronary lesions diagnosed by coronary angiography (CAG) and FFR. The main outcome measure was the combination of major adverse cardiovascular and cerebrovascular events (MACCEs). All patients were categorized into three subgroups in terms of TG/HDL-C tertiles (T1 < 0.96, 0.96 ≤ T2 < 1.58, T3 ≥ 1.58). Three different Cox regression models were utilized to reveal the association between TG/HDL-C and prevalence of MACCEs.
Results
47 MACCEs were recorded throughout a median monitoring period of 6.6 years. The Kaplan-Meier survival curves showed a higher MACCEs rate occurred in the higher TG/HDL-C group (5.6% vs. 12.9% vs. 19.4%, log-rank P < 0.01). After adjustment, patients in T3 suffered a 2.6-fold risk compared to the T1 group (T3 vs. T1: HR 2.55, 95% CI 1.05–6.21, P = 0.038; T2 vs. T1: HR 1.71, 95% CI 0.65–4.49, P = 0.075; P for trend = 0.001). The restricted cubic spline (RCS) analysis demonstrated that the HR for MACCEs rose as TG/HDL-C increased. Both the receiver operating characteristic (ROC) and time-dependent ROC proved the excellent predictive ability of TG/HDL-C.
Conclusion
The study illustrates that TG/HDL-C correlates with the risk of MACCEs in CAD patients deferred revascularization following FFR. TG/HDL-C could serve as a dependable predictor of cardiovascular events over the long term in this population.
Similar content being viewed by others
Introduction
Determining whether revascularization for coronary intermediate stenosis presents a significant challenge for cardiovascular interventionalists, defined as having a 40–70% obstruction as visually estimated [1]. FFR, which is calculated based on the mean distal stenosis pressure and aortic pressure, is strongly advocated for assessing these intermediate lesions for its physiologic function detection ability [1, 2]. FFR > 0.8 indicates that the lesion is non-significant coronary stenosis and deferred revascularization is recommended. With evidence accumulation, other determinants on prognosis emerged, including the plaque vulnerability and progression [3], the interference of microvascular dysfunction on FFR [4], and other non-coronary factors. A recent meta-analysis containing 4275 patients deferred revascularization following a negative FFR concluded that the cardiovascular events of diabetic patients was 2.08 folds greater than non-diabetic [5]. Hence, it is crucial to screen high-risk populations for patients deferred revascularization and administer more comprehensive treatment, even if with a normal FFR, in order to decrease the occurrence of MACCEs.
Dyslipidemia, identified as a conventional risk factor for CAD, includes a range of lipid particle disorders, such as low-density lipoprotein cholesterol (LDL-C), HDL-C, total cholesterol, and TG, with the recent addition of lipoprotein (a) to this list. LDL-C has been the subject of extensive researches and lowering LDL-C level has been confirmed an effective therapeutic option by clinical practice. Recently, enormous studies have proved the relationship between components of lipids and CAD, besides LDL-C. Among these factors, TG/HDL-C is closely linked to cardiovascular metabolic diseases [6]. Nonetheless, the effect of this ratio still unknown among patients deferred revascularization following FFR. Thus, the study intended to explore association of TG/HDL-C with long-term cardiovascular events in this group.
Methods
Study population
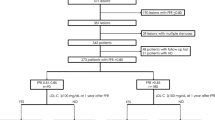
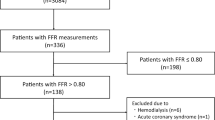
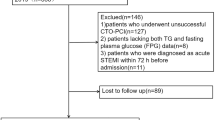
This study retrospectively included 1500 consecutive participants who received FFR and CAG for coronary intermediate lesions from February 2013 to October 2021, the same as the previous study population [7]. The study design was approved and performed in Beijing Anzhen Hospital, which is a major referral center dedicated to cardiovascular disease. The exclusion criteria were also similar to our previous work and are illustrated in Fig. 1. The main difference in this study is that only FFR > 0.8 out of the 1500 consecutive patients were included for analysis. Ultimately, 374 patients participated in this study. This study design was approved by The Second Xiangya Hospital of Central South University and Beijing Anzhen Hospital.

Population flow chart of enrolled patients. CAG, coronary angiography; FFR, fractional flow reserve; PCI, percutaneous coronary intervention
Interventional procedures
FFR and CAG procedures were performed by skilled operators in strict compliance with protocols. Should the CAG reveal intermediate stenosis, as determined by at least two seasoned interventionalists, an FFR evaluation is scheduled to be proceed, contingent upon patient and family consent. FFR findings informed decisions about whether PCI. Patients with a positive FFR results that indicated PCI but family members refused were excluded. The selection of specific stent size and perioperative drugs was at the discretion of the physician. No major complications occurred during interventional operation in all patients.
Baseline information collection and definition
Baseline information was acquired from electronic medical records system after approval by the ethics review committee. On the morning after admission, a fasting venous blood sample was collected then examined in Department of Laboratory Medicine. Monitoring information was gathered via electronic medical records system and through phone calls until October 2023. Diabetes mellitus and hypertension were diagnosed following globally recognized standards. Smoking status was identified if the individual had smoked within the six months leading up to the follow-up. FFR represents the ratio of the average pressure in distal stenosis to the aortic pressure at maximal myocardial perfusion.
Primary endpoints
The median follow-up period in this study up to 79 months. The primary outcome measured was the composite of MACCEs, encompassing nonfatal stroke, repeat revascularization, all-cause death, and nonfatal myocardial infarction. Nonfatal stroke was characterized by the rapid onset of clinical symptoms indicating cerebral dysfunction persisting for over 24 h, supported by neuroimaging evidence [8]. The other three diagnoses were also made according to official guidelines. All MACCEs occurrence events were recorded and compared in the three groups stratified by TG/HDL-C tertiles.
Statistical analysis
Continuous variables were commonly showed as either the mean ± SD or the median (P25, P75), on the basis of their distribution normality. One-way ANOVA was utilized for comparing normally distributed data, while the Kruskal-Wallis test was calculated for non-normally distributed data. Categorical variables were depicted as counts and percentages, with chi-square or Fisher’s exact test employed for statistical analysis. Patients were stratified into three subgroups according to TG/HDL-C tertiles. The incidence of MACCEs was recorded using Kaplan-Meier curves, and differences among the sets were calculated with the log-rank test. Three different Cox regression models were constructed to explore the relationship between graded TG/HDL-C tertiles and MACCEs risk. Model 1 adjusted for sex and age; Model 2 adjusted for sex, age, diabetes mellitus, BMI, smoking, and hypertension; Model 3 adjusted for sex, age, diabetes mellitus, BMI, smoking, hypertension, EF, CRP, LDL-C, uric acid, and FFR. An RCS analysis using 4 knots was plotted to explore relationship between TG/HDL-C (as continuous variable) and MACCEs risk. TG/HDL-C and FFR were incorporated in logistic regression to generate a new “predict” variable, which was intended to plot receiver operating characteristic (ROC) curve. ROC curves were utilized to compare the predictive capacity of different markers, and time-dependent ROC analysis examined the predictive power of TG/HDL-C at different time points. Differences in AUCs compared to TG/HDL-C were assessed using the Delong test. Data analysis was performed with SPSS 26.0, and visualization was done with GraphPad Prism 9.5.0 and R language software (R 4.1.3). For all calculations, a significance level of P < 0.05 was employed.
Results
Ultimately, this study enrolled a total of 374 patients, and Fig. 1 displays the selection process flow chart. The average age was 58.63 ± 9.05 years, and 252 (67.4%) individuals were men. The mean value of TG/HDL-C was 1.49 ± 1.04, and tertiles were T1 < 0.96, 0.96 ≤ T2 < 1.58, T3 ≥ 1.58. Throughout a median follow-up duration up to 79 months, 47 cases of MACCEs were documented, accounting for 12.6%.
Baseline characteristics
The baseline information stratified by the TG/HDL-C tertiles were exhibited in Table 1. Patients in T3 group are more likely to have dyslipidemia, higher BMI, LDL-C, TG, TC, TG/HDL-C, Glu, UA, CRP, and lower HDL-C compared to the low TG/HDL-C group (P < 0.05).
Association between TG/HDL-C and MACCEs
Kaplan-Meier curves were utilized to depict the cumulative risk of adverse clinical outcomes across the three groups (Fig. 2). Over the duration of the follow-up, there were 7, 16, and 24 MACCEs occurred in the T1, T2, and T3 groups, respectively. As the tertiles of TG/HDL-C increased, significant escalation happened in the cumulative risk of MACCEs (log-rank P = 0.0026).

Kaplan-Meier curves for the incidence of MACCEs among the three groups of TG/HDL-C. T1 < 0.96; 0.96 ≤ T2 < 1.58; T3 ≥ 1.58
Three different regression models were constructed to analyze the HR of MACCEs for TG/HDL-C. (Table 2). When fully adjusted, the patients in T2 and T3 group encountered a greater risk of MACCEs compared to those in T1 group (Model 3, T2 vs. T1: HR 1.71, 95% CI 0.65–4.49; T3 vs. T1: HR 2.55, 95% CI 1.05–6.21, P for trend = 0.001).
To further investigate the possible nonlinear relationship, an RCS curve was conducted (Fig. 3). The likelihood of MACCE events will significantly rise when TG/HDL-C over 1.28, and HR escalated as the ratio TG/HDL-C increasing.

The restricted cubic spline of HR for MACCEs and TG/HDL-C. TG/HDL-C, triglyceride to high-density lipoprotein cholesterol; CI, confidence interval; HR, hazard ratio
ROC and time-dependent ROC were utilized to detect the predictive capacity of the ratio TG/HDL-C. The findings indicated that TD/HDL-C exhibited a larger AUC compared to BMI, LDL-C, TG, and HDL-C (Fig. 4). The statistical difference of AUCs and the specific AUC values of each indicator were clearly displayed in Table 3. Time-dependent ROC curves also exhibited satisfactory predictive value at different times (Fig. 5). For patients with deferred revascularization, the baseline FFR value also has important predictive value for their long-term prognosis. The combination of TG/HDL-C with FFR exhibited better diagnostic efficacy than either one alone (Fig. 6; Table 3).

ROC curves of TG/HDL-C and other markers for the incidence of MACCEs. TG/HDL-C, triglyceride to high-density lipoprotein cholesterol; BMI, body mass index; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol

Time-dependent ROC curves of TG/HDL-C for the incidence of MACCEs.

ROC curves of TG/HDL-C, FFR and combination of TG/HDL with FFR for the incidence of MACCEs. TG/HDL-C, triglyceride to high-density lipoprotein cholesterol; FFR, fractional flow reserve
Discussion
This study revealed long-term prognostic value of TG/HDL-C in CAD patients who deferred revascularization following a normal FFR assessment for the first time. First, the research findings indicated that patients with elevated TG/HDL-C were at a greater risk of cardiac events than those with lower ratio. Second, the detrimental effects of TG/HDL-C will be significant and aggravated as the ratio increase. Third, TG/HDL-C could act as a dependable predictive factor to predict MACCEs in patients deferred revascularization following FFR.
Revascularization in CAD patients should follow strict criteria, including those on optimal drug treatment still experiencing angina, and those diagnosed with severe stenosis through coronary angiography (CAG). Nevertheless, the decision of whether perform revascularization for patients with intermediate stenosis cloud be ambiguous when based exclusively on CAG. Several strategies are used in current practice to assess the functional significance of coronary lesions and further guide coronary interventional therapy [8]. Among them, FFR has emerged as the “gold standard” in detecting functional ischemia, supported by a wealth of accumulated evidence. FFR-guided PCI has been proved to yield greater benefits than angiography-guided [9, 10]. As evidence continues to grow, authoritative guidelines have classified FFR as IA recommendation for intermediate stenosis [11]. FFR > 0.8 indicates that the lesion is non-significant coronary stenosis and deferred revascularization is recommended. However, it has become evident that the outcomes of deferred revascularization may not be uniform across all patient subgroups, as the utilization of physiology-guided revascularization increases. A recent meta-analysis containing 4275 patients deferred revascularization following negative FFR concluded that the cardiovascular events of diabetic patients was 2.08 folds greater than non-diabetic [5]. A large multinational study demonstrated that sex differences existed in the prognosis among patients with negative FFR and the HR of males for patient-oriented composite outcome (including revascularization, myocardial infarction, and death) was 2.07 [12]. On the other hand, the pathophysiologic mechanisms underlying CAD are also worth considering. First, plaque vulnerability and progression are major contributors to MACCEs, which can’t be well detected by FFR [13]. The COMBINE OCT-FFR trial revealed that thin-cap fibroatheroma positive patients suffered a five-fold higher risk of MACE despite this patients with a negative FFR [14]. Second, the evaluation of coronary stenosis severity using FFR cloud be partially confounded by microvascular dysfunction [15]. More importantly, both atherosclerotic plaque vulnerability and microvascular dysfunction are associated with dyslipidemia [16]. This study findings uncovered the association between TG/HDL-C ratio, two important particles of dyslipidemia, and long-term adverse clinical outcomes among CAD patients who have a normal FFR.
The influence of TG and HDL-C on cardiovascular disease development remains a subject of heated debate, given the unclear effects and contradictory findings from clinical research. Triglycerides are fat molecules formed from 3 molecules of long chain fatty acids and glycerol. HDL-C is a lipoprotein that transports cholesterol from body tissues to the liver. Adequate research confirms the relationship between TG and cardiovascular disease; however, more importantly, there are conflicting conclusions about the ability of this intervention to achieve significant clinical benefit in randomized controlled studies [17]. The fibrates and omega-3 fatty acids, two classic types of TG-lowering drugs, exerted variable clinical results [18,19,20]. Similarly, the same phenomenon occurred in HDL-C [21]. With the birth of PCSK9 and clinical practice, more and more studies are focusing on patients achieving optimal LDL-C levels and finding that residual cardiovascular risk will be increased if these patients have combined dyslipidemia, particularly for low HDL-C concentrations and high TG levels [22]. However, it is evident that the ratio of TG to HDL-C is linked with cardiovascular events. For example, the widely studied and hot metric: atherogenic index of plasm, is calculated from TG and HDL-C. This study findings similarly suggest that TG/HDL-C possesses superior predictive capacity than TG and HDL alone. Ample studies have been conducted concerning the connection between TG/HDL-C ratio and severity of CAD, covering aspects including metabolic syndrome, insulin resistance, and the existence of high-risk coronary plaques [23,24,25]. Besides, TG/HDL-C also linked to adverse cardiovascular outcomes for CAD patients [26, 27]. As previously mentioned, as the shortcomings of FFR in identifying unstable plaques and vulnerability to other factors, this close connection of TG/HDL-C and CAD may play a greater role in patients with immediate lesion to assist in screening high-risk patients. Similar to these studies, this research proved that higher level of TG/HDL-C increased risk of MACCEs in patients deferred revascularization following FFR.
FFR related indicators, such as iFR, post-PCI FFR, CT-FFR, are strongly associated with prognosis. The reason why FFR is inferior to TG/HDL-C may be related to the following two points in current study. First, we all know that the cutoff value of FFR is controversial, and even the concept of “gray zone”. Second, this research design only included patients with FFR > 0.8. The range of FFR changed from 0 to 1 to 0.8-1, which may diminish the predict power of FFR. Furthermore, integrating FFR with the TG/HDL-C ratio demonstrated the highest predictive capability, indicating that a predictive model that combines interventional assessment and laboratory results could have a more significant impact on clinical treatments.
Study strengths and limitations
This study has several strengths. First, it enriches prognosis information of the population with deferred revascularization following FFR, which has rarely been studied. Second, the prognostic value of TG/HDL-C on long-term incidence of MACCEs were investigated in CAD patients who deferred revascularization following a normal FFR assessment for the first time. Third, attention should be paid to the management of the levels of lipid components in patients, not only LDL-C. On the other hand, several limitations also exist. First, the study was conducted at a single-center and was retrospective in nature, which may introduce selection bias or potential confounding variables. Second, TG and HDL-C were only assessed upon admission, with no record of their dynamic changes throughout the follow-up period.
Conclusion
The study illustrates that TG/HDL-C correlates with the risk of MACCEs in CAD patients deferred revascularization following FFR. TG/HDL-C could serve as a dependable predictor of long term cardiovascular events in this population.
Data availability
No datasets were generated or analysed during the current study.
References
Patel MR, Calhoon JH, Dehmer GJ, Grantham JA, Maddox TM, Maron DJ, Smith PK, ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS. 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J Am Coll Cardiol 2017, 69:2212–2241.
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165.
Kedhi E, Berta B, Roleder T, Hermanides RS, Fabris E, AJJ IJ, Kauer F, Alfonso F, von Birgelen C, Escaned J, et al. Thin-cap fibroatheroma predicts clinical events in diabetic patients with normal fractional flow reserve: the COMBINE OCT-FFR trial. Eur Heart J. 2021;42:4671–9.
Kovarnik T, Hitoshi M, Kral A, Jerabek S, Zemanek D, Kawase Y, Omori H, Tanigaki T, Pudil J, Vodzinska A, et al. Fractional Flow Reserve Versus Instantaneous Wave-Free ratio in Assessment of Lesion hemodynamic significance and explanation of their discrepancies. International, Multicenter and prospective trial: the FiGARO Study. J Am Heart Assoc. 2022;11:e021490.
Ekmejian A, Sritharan H, Selvakumar D, Venkateshka V, Allahwala U, Ward M, Bhindi R. Outcomes of deferred revascularisation following negative fractional flow reserve in diabetic and non-diabetic patients: a meta-analysis. Cardiovasc Diabetol. 2023;22:22.
Yang T, Liu Y, Li L, Zheng Y, Wang Y, Su J, Yang R, Luo M, Yu C. Correlation between the triglyceride-to-high-density lipoprotein cholesterol ratio and other unconventional lipid parameters with the risk of prediabetes and type 2 diabetes in patients with coronary heart disease: a RCSCD-TCM study in China. Cardiovasc Diabetol. 2022;21:93.
Li F, Zhao D, Li Q, Lin X, Sun H, Fan Q, De Rosa S. Uric acid to High-Density Lipoprotein Cholesterol Ratio is a novel marker to Predict functionally significant coronary artery stenosis. J Interv Cardiol. 2022;2022:1–8.
Moscarella E, Gragnano F, Cesaro A, Ielasi A, Diana V, Conte M, Schiavo A, Coletta S, Di Maio D, Fimiani F, Calabrò P. Coronary physiology Assessment for the diagnosis and treatment of coronary artery disease. Cardiol Clin. 2020;38:575–88.
Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–24.
Zhang D, Lv S, Song X, Yuan F, Xu F, Zhang M, Yan S, Cao X. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention: a meta-analysis. Heart. 2015;101:455–62.
Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, Garg S, Huber K, James S, Knuuti J, et al. Guidelines on myocardial revascularization. Eur Heart J. 2010;31:2501–55.
Hoshino M, Hamaya R, Kanaji Y, Kanno Y, Hada M, Yamaguchi M, Sumino Y, Hirano H, Horie T, Usui E et al. Sex differences in long-term outcomes in patients with deferred revascularization following fractional Flow Reserve Assessment: international collaboration Registry of Comprehensive physiologic evaluation. J Am Heart Association 2020, 9.
Nogic J, Prosser H, O’Brien J, Thakur U, Soon K, Proimos G, Brown AJ. The assessment of intermediate coronary lesions using intracoronary imaging. Cardiovasc Diagnosis Therapy. 2020;10:1445–60.
Kedhi E, Berta B, Roleder T, Hermanides RS, Fabris E, Ijsselmuiden AJJ, Kauer F, Alfonso F, von Birgelen C, Escaned J, et al. Thin-cap fibroatheroma predicts clinical events in diabetic patients with normal fractional flow reserve: the COMBINE OCT–FFR trial. Eur Heart J. 2021;42:4671–9.
van de Hoef TP, Nolte F, EchavarrÍa-Pinto M, van Lavieren MA, Damman P, Chamuleau SA, Voskuil M, Verberne HJ, Henriques JP, van Eck-Smit BL, et al. Impact of hyperaemic microvascular resistance on fractional flow reserve measurements in patients with stable coronary artery disease: insights from combined stenosis and microvascular resistance assessment. Heart. 2014;100:951–9.
Arvanitis M, Lowenstein CJ. Dyslipidemia. Ann Intern Med. 2023;176:ITC81–96.
Malick WA, Waksman O, Do R, Koenig W, Pradhan AD, Stroes ESG, Rosenson RS. Clinical Trial Design for triglyceride-rich lipoprotein-lowering therapies. J Am Coll Cardiol. 2023;81:1646–58.
Rubins HB, Robins SJ, Collins D, Fye CL, Anderson JW, Elam MB, Faas FH, Linares E, Schaefer EJ, Schectman G, et al. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. N Engl J Med. 1999;341:410–8.
Das Pradhan A, Glynn RJ, Fruchart JC, MacFadyen JG, Zaharris ES, Everett BM, Campbell SE, Oshima R, Amarenco P, Blom DJ, et al. Triglyceride lowering with Pemafibrate to Reduce Cardiovascular Risk. N Engl J Med. 2022;387:1923–34.
Nicholls SJ, Lincoff AM, Garcia M, Bash D, Ballantyne CM, Barter PJ, Davidson MH, Kastelein JJP, Koenig W, McGuire DK, et al. Effect of high-dose Omega-3 fatty acids vs corn oil on major adverse Cardiovascular events in patients at High Cardiovascular Risk: the STRENGTH Randomized Clinical Trial. JAMA. 2020;324:2268–80.
Endo Y, Fujita M, Ikewaki K. HDL functions-current status and future perspectives. Biomolecules 2023, 13.
Reiner Z. Managing the residual cardiovascular disease risk associated with HDL-cholesterol and triglycerides in statin-treated patients: a clinical update. Nutr Metab Cardiovasc Dis. 2013;23:799–807.
da Luz PL, Favarato D, Faria-Neto JR Jr., Lemos P, Chagas AC. High ratio of triglycerides to HDL-cholesterol predicts extensive coronary disease. Clin (Sao Paulo). 2008;63:427–32.
Lelis DF, Calzavara JVS, Santos RD, Sposito AC, Griep RH, Barreto SM, Molina M, Schmidt MI, Duncan BB, Bensenor I, et al. Reference values for the triglyceride to high-density lipoprotein ratio and its association with cardiometabolic diseases in a mixed adult population: the ELSA-Brasil study. J Clin Lipidol. 2021;15:699–711.
Miki T, Miyoshi T, Suruga K, Ichikawa K, Otsuka H, Toda H, Yoshida M, Nakamura K, Morita H, Ito H. Triglyceride to HDL-cholesterol ratio is a predictor of future coronary events: a possible role of high-risk coronary plaques detected by coronary CT angiography. Eur Heart J 2020, 41.
Sultani R, Tong DC, Peverelle M, Lee YS, Baradi A, Wilson AM. Elevated triglycerides to High-Density Lipoprotein Cholesterol (TG/HDL-C) ratio predicts long-term mortality in high-risk patients. Heart Lung Circ. 2020;29:414–21.
Zhan X, Yang M, Zhou R, Wei X, Chen Y, Chen Q. Triglyceride to high-density lipoprotein cholesterol ratio is associated with increased mortality in older patients on peritoneal dialysis. Lipids Health Dis. 2019;18:199.
Acknowledgements
Not applicable.
Funding
This study was funded by the National Natural Science Foundation of China (Grant No. 82270337, 82070356), the Hunan Provincial Natural Science Foundation of China (Grant No. 2021JJ30033), and the Key Project of Hunan Provincial Science and Technology Innovation (Grant No. 2020SK1013).
Author information
Authors and Affiliations
Contributions
Fanqi Li and Xiaofang Li did statistical analysis and wrote the manuscript draft. Fanqi Li, Qiuyu Li, and Donghui Zhao collected the raw data. Fanqi Li, Jiabao Zhou, and Jiayi Zhu followed up the patients. Qiming Liu and Haixiong Wang made substantial revisions to the content of the manuscript. Qiuzhen Lin, Yong Zhou, and Keke Wu searched the literatures. All authors read and approved this version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study design was approved by The Second Xiangya Hospital of Central South University and The Beijing Anzhen Hospital.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.

Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Li, F., Li, X., Zhou, J. et al. Triglyceride to high-density lipoprotein cholesterol ratio associated with long-term adverse clinical outcomes in patients deferred revascularization following fractional flow reserve. Lipids Health Dis 23, 96 (2024). https://doi.org/10.1186/s12944-024-02093-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02093-1