
Abstract
Background
Per- and polyfluoroalkyl substances (PFAS) are known environmental contaminants with immunosuppressive properties. Their connection to rheumatoid arthritis (RA), a condition influenced by the immune system, is not well studied. This research explores the association between PFAS exposure and RA prevalence.
Methods
This research utilized data from the NHANES, encompassing a sample of 10,496 adults from the 2003–2018 cycles, focusing on serum levels of several PFAS. The presence of RA was determined based on self-reports. This study used multivariable logistic regression to assess the relationship between individual PFAS and RA risk, adjusting for covariates to calculate odds ratios (ORs). The combined effects of PFAS mixtures were evaluated using BKMR, WQS regression, and quantile g-computation. Additionally, sex-specific associations were explored through stratified analysis.
Results
Higher serum PFOA (OR = 0.88, 95% CI: 0.79, 0.98), PFHxS (OR = 0.91, 95% CI: 0.83, 1.00), PFNA (OR = 0.87, 95% CI: 0.77, 0.98), and PFDA (OR = 0.89, 95% CI: 0.81, 0.99) concentration was related to lower odds of RA. Sex-specific analysis in single chemical models indicated the significant inverse associations were only evident in females. BKMR did not show an obvious pattern of RA estimates across PFAS mixture. The outcomes of sex-stratified quantile g-computation demonstrated that an increase in PFAS mixture was associated with a decreased odds of RA in females (OR: 0.76, 95% CI: 0.62, 0.92). We identified a significant interaction term of the WQS*sex in the 100 repeated hold out WQS analysis. Notably, a higher concentration of the PFAS mixture was significantly associated with reduced odds of RA in females (mean OR = 0.93, 95% CI: 0.88, 0.98).
Conclusions
This study indicates potential sex-specific associations of exposure to various individual PFAS and their mixtures with RA. Notably, the observed inverse relationships were statistically significant in females but not in males. These findings contribute to the growing body of evidence indicating that PFAS may have immunosuppressive effects.
Similar content being viewed by others

Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disorder characterized by inflammatory polyarthritis, predominantly affecting the smaller joints. It is estimated to affect between 0.24 and 1% of the global population, exhibiting a prevalence approximately twice as high in women compared to men [1]. The articular and systemic manifestations of RA have the potential to culminate in severe long-term consequences, including disability and mortality [2]. The etiology of RA is multifactorial, likely stemming from an intricate interplay between genetic susceptibilities and diverse lifestyle determinants [3,4,5]. Previous scientific investigations suggest a potential link between RA and exposure to environmental contaminants [6,7,8,9]. Notably, the influence of per- and polyfluoroalkyl substances (PFAS) in this context appears to be an underexplored avenue.
PFAS are a group of synthetic fluorinated organic compounds widely used in various consumer and commercial products, encompassing items such as upholstery, carpeting, clothing, nonstick kitchenware, firefighting foams, and specialized food packaging [10]. The recent meta-analysis that estimated the half-lives of PFAS in human studies found that the mean half-life ranged from 3.4 to 5.7 years for total perfluorooctanesulfonic acid (PFOS), from 1.48 to 5.1 years for perfluorooctanoic acid (PFOA), and from 2.84 to 8.5 years for perfluorohexanesulfonic acid (PFHxS) [11]. Due to their pervasive application and remarkable environmental persistence, human exposure to PFAS is virtually inescapable, predominantly stemming from dietary sources, potable water, and a mix of indoor and outdoor environments [10, 12, 13].
Previous research has consistently demonstrated an association between PFAS exposure and a wide array of adverse health outcomes. These include, but are not limited to, dyslipidemia, hypertension, diabetes, metabolic syndrome, various cancers, and negative pregnancy outcomes [14,15,16,17,18,19]. The existing evidence from animal studies indicates potential disruptions in immune functions as a consequence of exposure to PFAS [20,21,22]. In addition, human epidemiological studies have further explored the potential associations of PFAS exposure with various immunological outcomes [23,24,25,26,27,28], encompassing asthma, allergic manifestations, susceptibility to infectious agents, and serological responses after vaccination. Cumulatively, the existing body of evidence suggests that PFAS exposure might exert effects similar to the onset and persistence of RA, which is an immune-related disease.
In the existing literature, investigations into the relationships between PFAS exposure and RA are notably limited. Two previous studies [29, 30] have assessed the association of RA with PFAS exposure among population exposed to extremely high environmental concentrations, and one [29] of them reported that RA was positively linked to PFOA exposure among workers. One recent study from China among the general population suggested that specific PFAS exposure is associated with alterations in defined immune markers of RA [31]. In addition, results from two other studies conducted in China indicated that certain types of PFAS exposure may either be associated with an increased risk of RA or enhance the disease activity of RA [32, 33]. While comprehensive data clarifying the association between PFAS exposure and RA risk remains scarce, various studies have underscored a potential association between RA risk and exposure to environmental contaminants, including but not limited to heavy metals [9], phthalates [7], and airborne pollutants [34]. Given the hypothesized shared pathogenic mechanisms, it becomes imperative to systematically assess the association of PFAS exposure with the risk of RA. Based on a comprehensive consideration of multiple factors, an initial hypothesis was formulated that elevated PFAS exposure correlates with an increasing risk of RA. In light of this, our study aims to clarify the association of serum PFAS concentrations, both as individual and mixtures, with RA risk, leveraging a robust cross-sectional study design and, explore if these associations differed by sex.
Methods
Study population and design
The National Health and Nutrition Examination Survey (NHANES) is an ongoing, nationally representative survey that utilizes a complex multi-stage sampling methodology. This open-access initiative, carried out across the United States, aims to capture the nutritional and health profiles of the non-institutionalized U.S. population (National Center for Health Statistics). The survey is conducted biennially.
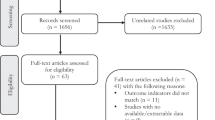
Between 2003 and 2018, NHANES registered a total of 76,848 participants. However, 58,612 of these participants were excluded as they did not provide biospecimens for PFAS measurements. Furthermore, 1909 participants were excluded due to unqualified biospecimens, which led to missing PFAS concentration data, often resulting from the provision of insufficient or substandard plasma samples. Another 3392 participants without RA data were also excluded. Figure 1 shows the detailed participant selection process. Every participant submitted written consent, and the data gathering approach, along with the research protocol, received approval from the National Center for Health Statistics (NCHS) Research Ethics Review Board (protocol number: #98-12, #2005-06, #2011-17, #2018-01) [35]. To maintain analytical consistency, we excluded participants lacking available covariate data (N = 2439). Finally, this study comprised 10,496 individuals, consisting of 9924 without RA and 572 with RA.

Flowchart of participants selection from the NHANES 2003–2018
Exposure assessment: serum PFAS concentrations
Serum samples collected from participants were processed and stored at − 80 °C in specialized containers and subsequently transported to a CDC (Centers for Disease Control and Prevention) designated laboratory for analysis. Detailed procedures for specimen collection and processing are outlined in the NHANES laboratory/medical technician procedure manual [36, 37]. For the quantitative detection of PFOA, PFOS, pefluorodecanoic acid (PFDA), PFHxS, perfluorononanoic acid (PFNA), perfluoroundecanoic acid (PFUnDA), 2-N-methyl-perfluorooctane sulfonamido acetic acid (Me-PFOSA-AcOH), online solid phase extraction coupled with High Performance Liquid Chromatography-Turbo Ion Spray-Tandem Mass Spectrometry (online SPE-HPLC-TIS-MS/MS) was employed. The limit of detection (LOD) for each PFAS was set at three times the standard deviation (SD) of the blank concentration [38]. In instances where the concentration was below the LOD, the machine-read value obtained through machine reading from the instrumental analysis was utilized if detectable. In cases where no machine-read value was available, the values were imputed using LOD/\(\sqrt{2}\) [39].
Outcome assessment: rheumatoid arthritis
The determination of participants’ RA status or non-RA status was achieved through a structured questionnaire. Initially, participants were posed the question, “Has a doctor or another medical professional ever diagnosed you with arthritis?” In cases where the response was affirmative, a subsequent question was raised: “Which specific type of arthritis were you diagnosed with?” Based on the responses to these two queries, participants were classified into either the RA or non-RA categories. Those who responded negatively to the primary question were allocated to the non-arthritis group, whereas individuals who answered positively to the first and identified “RA” for the second were categorized under the RA group.
Covariate assessment
In our analysis, the selection of covariates was informed according to previous studies on the association of PFAS with RA [31, 32] and the using of a directed acyclic graph (DAG) (Supplemental Fig. S1). The categorical covariates encompassed sex (male, female), ethnicity (Mexican-American, non-Hispanic white, non-Hispanic black, other Hispanic, or other/multiracial), educational attainment (lower than high school, greater than or equal to high school), family poverty-income ratio (PIR) (≤ 1.30, 1.31–3.50, > 3.50), alcohol consumption (never, former, mild, moderate, heavy), and physical activity (yes, no). Age and body mass index (BMI) were used as continuous covariates for the comparation between the RA and no RA groups. In addition, age (young: 20–39, middle-aged: 40–59, old: ≥ 60 years) [7, 33] and BMI (< 25, 25–29.90, ≥ 30 kg/m2) [40, 41] were categorized for detailed characterization of the study population and to support subsequent subgroup analyses.
Statistical methods
Individual pollutant analysis
We employed descriptive statistics to analyze the distribution of demographic characteristics, presenting the results as mean (± SD) or frequency (%) for the two groups (RA and non-RA). For variables that followed a normal distribution, we used the Student’s t test to compare between groups. In contrast, for variables with skewed distributions, the Wilcoxon rank-sum test was employed. Additionally, the chi-square test was used to assess differences in categorical variables across groups. To account for the skewed distributions of PFAS, we log2-transformed PFAS concentrations in subsequent analyses [42]. Pearson correlation coefficients among the PFAS biomarkers were calculated using log2-transformed concentrations. Our primary analysis involved multivariable logistic regression models to clarify the associations between PFAS concentrations and the odds of RA. These models were adjusted for a range of covariates: age, sex, ethnicity, educational attainment, BMI, PIR, alcohol consumption, and physical activity. Depending on the number of covariates, we employed three different models: unadjusted model was not adjusted for covariates; model 1 was adjusted for age and sex; model 2 was adjusted for all the covariates mentioned above. To address potential non-linear relationships, PFAS concentrations were modeled both continuously (as log2-transformed values) and categorically (in quartiles). In models where PFAS levels were treated continuously, the estimates reflected the change in odds of RA per doubling of PFAS concentrations. False Discovery Rate (FDR) correction using the Benjamini-Hochberg (BH) procedure was used to address the issue of multiple comparisons [43]. Statistical significance was determined with an FDR adjusted p-value (also called q-value) < 0.05, while results displaying an unadjusted p-value < 0.05 but an adjusted p-value > 0.05 were also discussed as marginal. All analyses were conducted using NHANES recommended sampling weights, which compensate for the survey’s stratified sampling design and non-response factors [44]. Subgroup analysis was also performed to evaluate the relationship between RA and PFAS in diverse populations by stratifying age, sex, ethnicity, educational attainment, BMI, PIR, alcohol consumption, and physical activity.
Mixture analysis
We examined the joint effects of seven PFAS on rheumatoid arthritis (RA) using three distinct approaches to model and parameterize exposure mixtures: quantile g-computation, Bayesian kernel machine regression (BKMR), and repeated hold out weighted quantile sum (WQS) regression. These models provide insights into both partial and cumulative dose-response relationships between environmental chemical mixtures and health outcomes, often obscured in single pollutant models. They also account for co-exposures that are highly correlated. All models were adjusted for age, sex, ethnicity, educational attainment, BMI, PIR, alcohol consumption, and physical activity. We also performed sex-stratified analyses for the mixture effect.
Our first approach, quantile g-computation, is a parametric, generalized linear model-based implementation of g-computation [45]. Quantile g-computation yields an estimate of the cumulative impact of the exposure mixture on the specified outcome, along with weights for each component within the mixture. These weights signify the proportional contribution of each element to the collective effect of the mixture. In this study, we specified quartiles as the quantile unit for PFAS concentrations. Thus, the mixture effect estimate denotes the OR of RA associated with a concurrent increase across quartiles in all six PFAS components. This method allows for both positive and negative effects of each exposure in the mixture, represented by relative weights summing to 1.0 [45].
The second approach, BKMR, uses a kernel function to flexibly model both the overall joint effect of an exposure mixture and to estimate individual exposure-outcome associations [46]. We conducted BKMR with 10,000 iterations, assessing convergence using the Markov chain Monte Carlo procedure. Univariate exposure-response functions evaluated the relationship between single PFAS levels and RA odds, while bivariate functions assessed interactions. We used posterior inclusion probabilities (PIPs) to determine the importance of each PFAS exposure [47]. The overall effect of the PFAS mixture was estimated by comparing the odds of RA when all PFAS exposures were set at the first and third quartiles versus the median value. We standardized all log2-transformed PFAS concentrations and excluded outliers exceeding 5 SDs from the mean (N = 8) [48].
The third approach, WQS regression, constructs a unidirectional weighted index from quantiled chemical exposures, addressing dimensionality and multi-collinearity issues in co-exposures [49], has been previously applied in several environmental epidemiologic studies [50,51,52]. We binned the chemicals into deciles, using negative weights from 100 bootstrap samples based on preliminary analysis suggesting PFAS were associated with lower RA odds. Significant chemicals of concern were determined as PFAS biomarkers with weights greater than a concern threshold of 1/c (14.3%), where c is the number of chemicals in the mixture as recommended by previous studies [49, 53]. We applied 100 repeated holdout validation to assess stability and potential generalizability [54]. WQS regression models with a WQS*sex interaction term and stratified sex-specific weights were also performed, allowing the WQS index effect to differ by sex [55]. Relative weights were calculated within each stratum, with chemicals exceeding 14.3% in at least 50% of the holdouts identified as chemicals of concern [56].
Sensitivity analyses in the individual pollutant model included adjusting for the NHANES calendar cycle. Multi-cycle analyses were also conducted to evaluate result stability. All statistical analyses were performed using R version 4.1.0 (R Core Team), with mixture analyses using the “bkmr”, “qgcomp”, and “gWQS” packages.
Results
A total of 10,496 adults were included in the study, consisting of 5138 males and 5358 females. Among them, 572 participants had self-reported diagnoses of RA, resulting in a prevalence of 5.4%. The characteristics of the population, both with and without RA, are presented in Table 1. Noteworthy variations were observed in age, BMI, sex, ethnicity, educational attainment, PIR, alcohol consumption and physical activity.
Table 2 presents the serum concentration distributions and detection frequencies of the seven PFAS analyzed in our study. PFUnDA, Me-PFOSA-AcOH, and PFDA were detected in 46.70%, 57.01%, and 74.91% of participant samples, respectively, while the detection rates for the remaining PFAS exceeded 98%. PFOS exhibited the highest median concentration at 9.70 ng/mL, followed by PFOA at 2.63 ng/mL. The strongest correlation was observed between PFDA and PFUnDA (r = 0.77, P < 0.001). Correlation coefficients among other PFAS pairs varied, ranging from 0.04 (between PFUnDA and Me-PFOSA-AcOH) to 0.47 (between PFOS and PFUnDA) (Fig. 2).

Pearson correlation between serum per- and polyfluoroalkyl substances (PFAS) after Iog2 transformed
Associations of individual PFAS with RA
The study predominantly found no significant association between the doubling of PFAS concentrations and the risk of RA, with occasional inverse associations observed (Table 3). Specifically, a doubling in PFOA concentration was associated with a 12% reduction in RA odds (OR = 0.88, 95% CI: 0.79, 0.98) and similar result was observed for a doubling in PFDA and PFNA concentration (OR = 0.89, 95% CI: 0.81, 0.99 and OR = 0.87, 95% CI: 0.77, 0.98, respectively). PFUnDA also exhibited associations with lower RA odds in the partially adjusted model, although these associations were not statistically significant in the fully adjusted models. Conversely, Me-PFOSA-AcOH was linked to increased RA odds in the unadjusted model (OR = 1.13, 95%CI: 1.05, 1.22). The estimates for other PFAS compounds generally showed a consistent direction of effect, but were not statistically significant.
When PFAS levels were categorized into quartiles, similar patterns emerged. For instance, the highest quartile of PFDA exposure was associated with lower RA odds [Q4 vs. Q1: OR = 0.72 (95% CI: 0.52, 1.00)]. PFOA showed a similar association with lower RA odds, with the relationship not being monotonic [Q2 vs. Q1: OR = 0.67 (95% CI: 0.46, 0.98); Q3 vs. Q1: OR = 0.87 (95% CI: 0.62, 1.22); Q4 vs. Q1: OR = 0.60 (95% CI: 0.42, 0.86)]. Assessments of other PFAS exposures in quartiles mostly yielded null results, except for Me-PFOSA-AcOH, which was associated with increased odds of RA in the unadjusted model. After correcting for multiple comparisons in the main analyses, significant p-values from the primary analysis only remained in small number of the analyses.
In subgroup analyses stratified by general characteristics of participants for each PFAS, we found that PFOA, PFDA, PFUnDA, and PFHxS was associated with lower odds of RA in female for both continuous and categorical exposure, and most significantly associations were only existed in some subgroups (Supplemental Table S1–S7). For the remained PFAS, we also found that there are some significant associations in some subgroups for specific exposure pattern.
Associations of the PFAS mixture with RA
Univariate exposure-response functions for seven PFAS in relation to RA risk, showing no apparent increasing or decreasing trends (Supplemental Fig. S2). BKMR analysis for the overall effect of the PFAS mixture on RA odds indicates that there is not significant association between serum PFAS mixture concentrations and RA odds (Supplemental Fig. S3). When examining the associations between individual PFAS and RA while controlling for other PFAS at the 25th, 50th, and 75th percentiles, no significant associations were found (Supplemental Fig. S4). The PIPs for each PFAS exposure are specified as follows: PFOA, 0.444; PFOS, 0.298; PFHxS, 0.368; PFDA, 0.058; PFNA, 0.052; PFUnDA, 0.242, and Me-PFOSA-AcOH, 0.276. BKMR analyses stratified by sex showed similar results (Supplemental Figs. S5 and S6). However, significant associations of Me-PFOSA-AcOH and PFUnDA with RA were found while controlling for other PFAS at the 50th percentile among males (Fig. 3). In addition, PFOA was found to be associated with lower odds of RA while controlling for other PFAS at the 50th and 75th percentiles among females (Fig. 3).

Associations of each individual PFAS with RA status in BKMR model stratified by sex. This plot describes the estimated RA status associated with a change in each individual PFAS from its 25th to 75th percentile, when all the other PFAS are fixed at either the 25th (red line), 50th (green line), or 75th percentile (blue line). Dots indicate the estimate, and horizontal lines indicate the 95% credible intervals. All models were adjusted for age, sex, ethnicity, educational attainment, body mass index, poverty income ratio, alcohol consumption and physical activity
Quantile g-computation model analysis demonstrated that an increase in PFAS mixture quartile was not linked to higher RA odds (OR = 0.88, 95% CI: 0.76, 1.02). However, a sex-stratified analysis revealed a significant decrease in RA odds among females with a quartile increase in PFAS mixture (OR = 0.76, 95% CI: 0.62, 0.92), but not in males (OR = 1.07, 95% CI: 0.88, 1.29). For females, five serum PFAS were negatively associated with RA risk, while two showed a positive association (Fig. 4). PFOS had the most substantial positive relationship with RA, followed by PFNA. Conversely, PFUnDA led the negative association, followed by PFOA, PFHxS, PFDA, and Me-PFOSA-AcOH.

The directions and magnitude of the assigned weights for each log2-transformed PFAS in relation to RA status in quantile g-computation for (A) overall population, (B) male, and (C) female. Each weight represents the proportion of the positive or negative partial impact per individual PFAS. The length of each bars indicates the effect size of each exposure in the same direction. All models were adjusted for age, sex, ethnicity, educational attainment, BMI, poverty income ratio, alcohol consumption and physical activity
We also analyzed the chemical mixture’s associations with RA risk in both positive and negative directions using WQS. While the WQS indices in the positive and negative directions were not significantly associated with RA risk. In the fully adjusted models, a quartile increase in the WQS index was linked to a 5% decrease in RA odds (OR = 0.95, 95%CI: 0.89, 1.02) in the negative direction, with PFUnDA contributing the most, followed by PFHxS, PFDA, PFNA and PFOA; however, the effect estimate was not statistically significant. Similar result was also observed in the positive direction (OR = 0.99, 95% CI: 0.94, 1.05), with Me-PFOSA-AcOH contributing the most, followed by PFOS and PFDA. Detailed chemical weight estimates for each WQS index are presented in Supplemental Fig. S7.
Further, sex-specific associations and chemical weight distributions were observed in the repeated hold out WQS analysis with an interaction term (Supplemental Fig. S8A, B). The WQS*sex interaction term was significant (mean OR = 0.91, 95%CI: 0.84, 0.96), with differing slopes for males and females. Females showed a reduced odds of RA (mean OR = 0.93, 95%CI: 0.88, 0.98). Conversely, males demonstrated a marginally increased odds of RA (mean OR = 1.03, 95%CI: 0.98, 1.10); however, this increase was not statistically significant. The distribution of the ORs was opposite for males and females, with 75 out of 100 betas positive for males and 100 out of 100 negative for females. However, significance was only reached for females. These findings are elaborated in Table 4. Notable chemicals of concern differed by sex, with PFUnDA, PFOA, PFHxS, and PFDA for females and PFNA and PFHxS for males (Supplemental Fig. S8B).
Sensitivity analysis
Sensitivity analyses was performed by additionally adjusting the NHANES calendar cycle. There were significantly associations of PFAS exposure with lower odds of RA for both continuous [PFOA: OR = 0.85 (95% CI: 0.76, 0.95); PFHxS: OR = 0.90 (95% CI: 0.82, 0.99); PFDA: OR = 0.88 (95% CI: 0.79, 0.99); PFNA: OR = 0.86 (95% CI: 0.76, 0.97); PFUnDA: OR = 0.88 (95% CI: 0.80, 0.97)] and categorical exposure [PFOA, Q4 vs. Q1: OR = 0.52 (95% CI: 0.37, 0.75); PFHxS, Q4 vs. Q1: OR = 0.68 (95% CI: 0.48, 0.98); PFDA, Q4 vs. Q1: OR = 0.70 (95% CI: 0.50, 0.97); PFUnDA, Q4 vs. Q1: OR = 0.68 (95% CI: 0.48, 0.94)] (Supplemental Table S8). Additionally, the multi-cycle sensitivity analysis revealed significant associations with RA odds for PFOA, PFOS, PFHxS, PFNA, and me-PFOSA-AcOH in at least one cycle (Supplemental Table S9).
Discussion
Summary of main results
To the best of our knowledge, this is the first cross-sectional study to assess the association between serum PFAS concentration and RA. In this extensive cross-sectional analysis, we observed a RA prevalence of 5.4%, which is higher than the 0.5 to 1% typically reported in prior research [57, 58]. The discrepancy could be attributed to the exclusion of certain data in our study, implemented to ensure a complete and thorough data analysis. We also identified significant inverse associations of serum PFOA, PFHxS, PFDA, and PFNA levels with the odds of RA. Further, sex-specific analyses within the individual pollutant models indicated that these associations were more marked among females, whereas they were not observed in males. In addition, a stratified analysis of the quantile g-computation by sex revealed a significant association in females. Notably, PFOS demonstrated the most substantial positive influence, whereas PFUnDA showed the most significant negative impact. In the case of WQS regression, we identified a significant WQS*sex interaction term, indicating the presence of sex-specific differences. The results suggest that PFAS, when considered as a mixture, is associated with a reduced odds of RA in females. PFUnDA, PFOA, PFHxS, and PFDA emerged as the primary contributors to this mixed effect. Conversely, WQS analysis did not reveal significant association of the PFAS mixture with RA in males. The BKMR analysis suggests that PFUnDA and Me-PFOSA-AcOH were associated with increased risk of RA in males, while PFOA was associated with lower odds of RA in females.
Comparison with previous studies and potential biological mechanisms
To our knowledge, only three prior epidemiological studies [31,32,33] have explored the relationship between PFAS exposure and immune markers relating to RA, disease activity of RA and risk of RA, respectively. One study in China by Zhao et al. [31] analyzed serum from 280 healthy individuals and 294 RA patients, finding several PFAS were associated with elevated immune-related parameters, such as C-reactive protein and IgA. They further reported that PFAS may prompt the disease activity of RA [32]. Qu et al. [33] investigated the association of PFAS with RA in a case-control study, and identified a significant association between PFOA exposure and increased risk of RA [33]. However, these three studies were based on case-control design with small sample size. Our study, using the latest NHANES data from 2003 to 2018, presents a contrasting view. We noted inverse associations of various PFAS, particularly PFOA, PFHxS, PFDA and PFNA, and PFAS mixture with RA in females. These differences may stem from variations in study design, exposure levels, or demographic characteristics. Additionally, our study accounted for numerous covariates such as physical activity and alcohol consumption, which previous studies overlooked.
Despite the scarcity of research on PFAS exposure and RA, there is evidence linking PFAS to suppressed antibody responses after vaccination [59,60,61], increased risk of infectious diseases [62,63,64,65] and allergic outcomes [24], though with both positive and negative associations. Our research identified a significant trend: both individual and mixed PFAS exposures were inversely associated with the odds of RA. However, the cross-sectional nature of our study necessitates a cautious interpretation of these associations. At this stage, it is premature to conclude that PFAS exposure acts as a protective factor against RA. The potential immunosuppressive mechanisms of PFAS, as reviewed in previous literature [66], may explain these findings. In detail, RA is a chronic inflammatory disease characterized by significant immune activation within the synovial compartment of joints and numerous systemic effects [67]. The pathophysiology of RA, although not fully understood, is marked by the dominance of T cells and T cell-derived cytokines in the synovial membrane’s mononuclear infiltrates, highlighting their critical role in the disease’s autoimmune response [68]. Furthermore, the observed upregulation of the Th1 response within the synovial compartment suggests that a Th1/Th2 imbalance is crucial in the pathogenesis of RA [69]. Epidemiological studies have demonstrated a PFAS-induced disruption in this balance, characterized by increased Th2 [70] and decreased Th1 cytokine production [59, 70]. This shift towards a Th2-dominant response has been corroborated in both in vitro [71] and in vivo studies [72, 73]. Additionally, He et al. (2017) found that RA patients typically exhibit a Th1/Th2 balance skewed towards Th1 [74]. These evidence, taken together with our findings, suggests that PFAS exposure may mitigate RA risk by inducing an opposing effect on the Th1/Th2 balance. In summary, mechanistic studies indicate that PFAS exposure can influence Th1/Th2 balance and downstream signaling. However, the mechanism likely extends beyond Th1/Th2 imbalance, possibly involving more specific immune processes, such as calcium signaling, and broader systemic mechanisms like lipid metabolism and oxidative stress, contributing to the immunotoxicity of PFAS [20].
In our study, we specifically investigated how sex modifies the relationship between PFAS exposure and RA. Our findings revealed a striking sex-specific disparity: while PFAS exposure was inversely associated with RA in females, such an association was not evident in males [64, 75]. The literature frequently reports sex-specific differences in the health effects of PFAS [36, 76, 77], but the precise mechanisms underlying these differences remain elusive. One possible factor is the observed variance in PFAS blood concentrations between men and women [78]. Additionally, interactions between PFAS and sex hormones [79,80,81], particularly estradiol, may play a significant role, as available data support hypoandrogenicity in RA patients [73, 82]. Additionally, sex-specific differences in metabolic and detoxification processes could also modulate the effects of PFAS exposure [83, 84]. To comprehensively understand these contradictory associations, detailed mechanistic studies focusing on individual PFAS chemicals are essential.
Strengths and limitations
Our study demonstrates several strengths. Firstly, it capitalizes on data from the NHANES, noted for its representative sampling of the U.S. general population. NHANES employs rigorous and standardized methods for data collection via questionnaires and biological sample analysis, also providing sample weights. These methodologies significantly bolster the robustness and reliability of our findings. Secondly, the innovative use of a repeated holdout WQS regression model in our study enhances the stability of the WQS estimates. This model is particularly adept at identifying chemicals of concern and observing sex-specific effects, which are critical aspects of our research.
However, certain limitations warrant consideration. The cross-sectional nature of our study, inherent in its observational design, provides foundational insights into potential associations but falls short in definitively establishing temporal sequences or causality. This necessitates the replication of our results and encourages future longitudinal studies for a more robust validation of the observed associations. Additionally, the reliance on a single time points serum sample assessment to infer long-term PFAS exposure status could potentially limit its scope. Given that one measurement of PFAS in blood is indicative of cumulative exposure spanning 5–10 years [85], and considering the prolonged development period of RA, this approach may overlook crucial long-term chemical influences, thereby introducing potential confounding variables. This study conducted numerous subgroup analyses to uncover associations within particular subgroups. While we did identify some significant associations in certain subgroups, it is important to note the potential risk of false positives arising from multiple comparisons. Therefore, these findings should be interpreted with caution. Finally, the exclusive inclusion of adult participants from the United States in this study constrains the generalizability of our conclusions to other geographic contexts.
Conclusions
In conclusion, our findings indicate potential inverse associations at background exposure levels between several prominent PFAS and RA risk. It is imperative to conduct further longitudinal studies to explore the effects of PFAS and to elucidate the mechanisms by which PFAS exposure might influence the development of autoimmune diseases. Such research is crucial to both substantiate and elucidate the implications of the findings presented in this study.
Data availability
All data are open access and available for download at url: https://www.cdc.gov/nchs/nhanes/index.htm.
Change history
29 April 2024
The last paragraph of the Conclusions section should be Table 4 notes.
References
Gabriel SE, Crowson CS. Epidemiology of risk factors for, and possible causes of rheumatoid arthritis. Up Date 2018, 20181.
Black RJ, Cross M, Haile LM, Culbreth GT, Steinmetz JD, Hagins H, Kopec JA, Brooks PM, Woolf AD, Ong KL. Global, regional, and national burden of rheumatoid arthritis, 1990–2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(10):e594–610.
Dedmon LE. The genetics of rheumatoid arthritis. Rheumatology. 2020;59(10):2661–70.
Sugiyama D, Nishimura K, Tamaki K, Tsuji G, Nakazawa T, Morinobu A, Kumagai S. Impact of smoking as a risk factor for developing rheumatoid arthritis: a meta-analysis of observational studies. Ann Rheum Dis. 2010;69(01):70–81.
Maisha JA, El-Gabalawy HS, O’Neil LJ. Modifiable risk factors linked to the development of rheumatoid arthritis: evidence, immunological mechanisms and prevention. Front Immunol 2023, 14.
Sheng N, Wang J, Xing F, Duan X, Xiang Z. Associations between exposure to phthalates and rheumatoid arthritis risk among adults in NHANES, 2007–2016. Chemosphere. 2023;338:139472.
Chen Y, Shen J, Wu Y, Fang L, Xu S, Peng Y, Pan F. Associations between urinary phthalate metabolite concentrations and rheumatoid arthritis in the US adult population. Chemosphere. 2023;337:139382.
Essouma M, Noubiap JJN. Is air pollution a risk factor for rheumatoid arthritis? J Inflamm. 2015;12:1–7.
Chen L, Sun Q, Peng S, Tan T, Mei G, Chen H, Zhao Y, Yao P, Tang Y. Associations of blood and urinary heavy metals with rheumatoid arthritis risk among adults in NHANES, 1999–2018. Chemosphere. 2022;289:133147.
Sunderland EM, Hu XC, Dassuncao C, Tokranov AK, Wagner CC, Allen JG. A review of the pathways of human exposure to poly-and perfluoroalkyl substances (PFASs) and present understanding of health effects. J Expo Sci Environ Epidemiol. 2019;29(2):131–47.
Rosato I, Bonato T, Fletcher T, Batzella E, Canova C. Estimation of per- and polyfluoroalkyl substances (PFAS) half-lives in human studies: a systematic review and meta-analysis. Environ Res. 2024;242:117743.
Guelfo JL, Korzeniowski S, Mills MA, Anderson J, Anderson RH, Arblaster JA, Conder JM, Cousins IT, Dasu K, Henry BJ. Environmental sources, Chemistry, Fate, and transport of per-and polyfluoroalkyl substances: state of the Science, Key Knowledge gaps, and recommendations presented at the August 2019 SETAC Focus Topic Meeting. Environ Toxicol Chem. 2021;40(12):3234–60.
Kato K, Wong L-Y, Jia LT, Kuklenyik Z, Calafat AM. Trends in exposure to polyfluoroalkyl chemicals in the US population: 1999–2008. Environ Sci Technol. 2011;45(19):8037–45.
Fenton SE, Ducatman A, Boobis A, DeWitt JC, Lau C, Ng C, Smith JS, Roberts SM. Per-and polyfluoroalkyl substance toxicity and human health review: current state of knowledge and strategies for informing future research. Environ Toxicol Chem. 2021;40(3):606–30.
Averina M, Brox J, Huber S, Furberg A-S. Exposure to perfluoroalkyl substances (PFAS) and dyslipidemia, hypertension and obesity in adolescents. The Fit futures study. Environ Res. 2021;195:110740.
Gui S-Y, Qiao J-C, Xu K-X, Li Z-L, Chen Y-N, Wu K-J, Jiang Z-X, Hu C-Y. Association between per-and polyfluoroalkyl substances exposure and risk of diabetes: a systematic review and meta-analysis. J Expo Sci Environ Epidemiol. 2023;33(1):40–55.
Christensen KY, Raymond M, Meiman J. Perfluoroalkyl substances and metabolic syndrome. Int J Hyg Environ Health. 2019;222(1):147–53.
Steenland K, Winquist A. PFAS and cancer, a scoping review of the epidemiologic evidence. Environ Res. 2021;194:110690.
Gao X, Ni W, Zhu S, Wu Y, Cui Y, Ma J, Liu Y, Qiao J, Ye Y, Yang P. Per-and polyfluoroalkyl substances exposure during pregnancy and adverse pregnancy and birth outcomes: a systematic review and meta-analysis. Environ Res. 2021;201:111632.
Ehrlich V, Bil W, Vandebriel R, Granum B, Luijten M, Lindeman B, Grandjean P, Kaiser A-M, Hauzenberger I, Hartmann C. Consideration of pathways for immunotoxicity of per-and polyfluoroalkyl substances (PFAS). Environ Health. 2023;22(1):19.
Huang J, Wang Q, Liu S, Lai H, Tu W. Comparative chronic toxicities of PFOS and its novel alternatives on the immune system associated with intestinal microbiota dysbiosis in adult zebrafish. J Hazard Mater. 2022;425:127950.
Maddalon A, Pierzchalski A, Kretschmer T, Bauer M, Zenclussen AC, Marinovich M, Corsini E, Herberth G. Mixtures of per-and poly-fluoroalkyl substances (PFAS) reduce the in vitro activation of human T cells and basophils. Chemosphere 2023:139204.
Granum B, Haug LS, Namork E, Stølevik SB, Thomsen C, Aaberge IS, van Loveren H, Løvik M, Nygaard UC. Pre-natal exposure to perfluoroalkyl substances may be associated with altered vaccine antibody levels and immune-related health outcomes in early childhood. J Immunotoxicol. 2013;10(4):373–9.
Rudzanova B, Vlaanderen J, Kalina J, Piler P, Zvonar M, Klanova J, Blaha L, Adamovsky O. Impact of PFAS exposure on prevalence of immune-mediated diseases in adults in the Czech Republic. Environ Res. 2023;229:115969.
Van Larebeke N, Koppen G, De Craemer S, Colles A, Bruckers L, Den Hond E, Govarts E, Morrens B, Schettgen T, Remy S. Per-and polyfluoroalkyl substances (PFAS) and immune system-related diseases: results from the flemish environment and Health Study (FLEHS) 2008–2014. Environ Sci Europe. 2023;35(1):28.
von Holst H, Nayak P, Dembek Z, Buehler S, Echeverria D, Fallacara D, John L. Perfluoroalkyl substances exposure and immunity, allergic response, infection, and asthma in children: review of epidemiologic studies. Heliyon 2021, 7(10).
Zeng X-W, Bloom MS, Dharmage SC, Lodge CJ, Chen D, Li S, Guo Y, Roponen M, Jalava P, Hirvonen M-R. Prenatal exposure to perfluoroalkyl substances is associated with lower hand, foot and mouth disease viruses antibody response in infancy: findings from the Guangzhou Birth Cohort Study. Sci Total Environ. 2019;663:60–7.
Dalsager L, Christensen N, Halekoh U, Timmermann CAG, Nielsen F, Kyhl HB, Husby S, Grandjean P, Jensen TK, Andersen HR. Exposure to perfluoroalkyl substances during fetal life and hospitalization for infectious disease in childhood: a study among 1,503 children from the Odense Child Cohort. Environ Int. 2021;149:106395.
Steenland K, Zhao L, Winquist A. A cohort incidence study of workers exposed to perfluorooctanoic acid (PFOA). Occup Environ Med. 2015;72(5):373–80.
Steenland K, Zhao L, Winquist A, Parks C. Ulcerative colitis and perfluorooctanoic acid (PFOA) in a highly exposed population of community residents and workers in the Mid-ohio valley. Environ Health Perspect. 2013;121(8):900–5.
Zhao Y, Liu W, Qu J, Hu S, Zhang L, Zhao M, Wu P, Xue J, Hangbiao J. Per-/polyfluoroalkyl substance concentrations in human serum and their associations with immune markers of rheumatoid arthritis. Chemosphere. 2022;298:134338.
Zhao Y, Jin H, Qu J, Zhang S, Hu S, Xue J, Zhao M. The influences of perfluoroalkyl substances on the rheumatoid arthritis clinic. BMC Immunol. 2022;23(1):10.
Qu J, Zhao Y, Zhang L, Hu S, Liao K, Zhao M, Wu P, Jin H. Evaluated serum perfluoroalkyl acids and their relationships with the incidence of rheumatoid arthritis in the general population in Hangzhou, China. Environ Pollut. 2022;307:119505.
Jung C-R, Hsieh H-Y, Hwang B-F. Air pollution as a potential determinant of rheumatoid arthritis. Epidemiology. 2017;28:S54–9.
Yi W, Xuan L, Zakaly HM, Markovic V, Miszczyk J, Guan H, Zhou P-K, Huang R. Association between per-and polyfluoroalkyl substances (PFAS) and depression in US adults: a cross-sectional study of NHANES from 2005 to 2018. Environ Res. 2023;238:117188.
Wen X, Wang M, Xu X, Li T. Exposure to per-and polyfluoroalkyl substances and mortality in US adults: a population-based cohort study. Environ Health Perspect. 2022;130(6):067007.
Taibl KR, Schantz S, Aung MT, Padula A, Geiger S, Smith S, Park J-S, Milne GL, Robinson JF, Woodruff TJ. Associations of per-and polyfluoroalkyl substances (PFAS) and their mixture with oxidative stress biomarkers during pregnancy. Environ Int. 2022;169:107541.
Morello-Frosch R, Cushing LJ, Jesdale BM, Schwartz JM, Guo W, Guo T, Wang M, Harwani S, Petropoulou S-SE, Duong W. Environmental chemicals in an urban population of pregnant women and their newborns from San Francisco. Environ Sci Technol. 2016;50(22):12464–72.
Hornung RW, Reed LD. Estimation of average concentration in the presence of nondetectable values. Appl Occup Environ Hyg. 1990;5(1):46–51.
Liu B, Wang J, Li YY, Li KP, Zhang Q. The association between systemic immune-inflammation index and rheumatoid arthritis: evidence from NHANES 1999–2018. Arthritis Res Ther. 2023;25(1):34.
Wen X, Wang M, Xu X, Li T. Exposure to Per- and polyfluoroalkyl substances and mortality in U.S. adults: a Population-based Cohort Study. Environ Health Perspect. 2022;130(6):67007.
Choi G, Buckley JP, Kuiper JR, Keil AP. Log-transformation of independent variables. Must We? Epidemiol. 2022;33(6):843–53.
Iwata H, Kobayashi S, Itoh M, Itoh S, Mesfin Ketema R, Tamura N, Miyashita C, Yamaguchi T, Yamazaki K, Masuda H, et al. The association between prenatal per-and polyfluoroalkyl substance levels and Kawasaki disease among children of up to 4 years of age: a prospective birth cohort of the Japan Environment and Children’s study. Environ Int. 2024;183:108321.
Johnson CL, Paulose-Ram R, Ogden CL, Carroll MD, Kruszan-Moran D, Dohrmann SM, Curtin LR. National health and nutrition examination survey. Analytic guidelines; 2013. pp. 1999–2010.
Keil AP, Buckley JP, O’Brien KM, Ferguson KK, Zhao S, White AJ. A quantile-based g-computation approach to addressing the effects of exposure mixtures. Environ Health Perspect. 2020;128(4):047004.
Bobb JF, Valeri L, Claus Henn B, Christiani DC, Wright RO, Mazumdar M, Godleski JJ, Coull BA. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics. 2015;16(3):493–508.
Cathey AL, Eaton JL, Ashrap P, Watkins DJ, Rosario ZY, Vega CV, Alshawabkeh AN, Cordero JF, Mukherjee B, Meeker JD. Individual and joint effects of phthalate metabolites on biomarkers of oxidative stress among pregnant women in Puerto Rico. Environ Int. 2021;154:106565.
Preston EV, Hivert M-F, Fleisch AF, Calafat AM, Sagiv SK, Perng W, Rifas-Shiman SL, Chavarro JE, Oken E, Zota AR. Early-pregnancy plasma per-and polyfluoroalkyl substance (PFAS) concentrations and hypertensive disorders of pregnancy in the project viva cohort. Environ Int. 2022;165:107335.
Carrico C, Gennings C, Wheeler DC, Factor-Litvak P. Characterization of weighted quantile sum regression for highly correlated data in a risk analysis setting. J Agricultural Biol Environ Stat. 2015;20:100–20.
Yang X, Li Y, Li J, Bao S, Zhou A, Xu S, Xia W. Associations between exposure to metal mixtures and birth weight. Environ Pollut. 2020;263:114537.
Zhang Y, Dong T, Hu W, Wang X, Xu B, Lin Z, Hofer T, Stefanoff P, Chen Y, Wang X. Association between exposure to a mixture of phenols, pesticides, and phthalates and obesity: comparison of three statistical models. Environ Int. 2019;123:325–36.
Loftus CT, Bush NR, Day DB, Ni Y, Tylavsky FA, Karr CJ, Kannan K, Barrett ES, Szpiro AA, Sathyanarayana S. Exposure to prenatal phthalate mixtures and neurodevelopment in the conditions affecting Neurocognitive Development and Learning in early childhood (CANDLE) study. Environ Int. 2021;150:106409.
Kupsco A, Wu H, Calafat AM, Kioumourtzoglou M-A, Tamayo-Ortiz M, Pantic I, Cantoral A, Tolentino M, Oken E, Braun JM. Prenatal maternal phthalate exposures and child lipid and adipokine levels at age six: a study from the PROGRESS cohort of Mexico City. Environ Res. 2021;192:110341.
Tanner EM, Bornehag C-G, Gennings C. Repeated holdout validation for weighted quantile sum regression. MethodsX. 2019;6:2855–60.
Busgang SA, Spear EA, Andra SS, Narasimhan S, Bragg JB, Renzetti S, Curtin P, Bates M, Arora M, Gennings C. Application of growth modeling to assess the impact of hospital-based phthalate exposure on preterm infant growth parameters during the neonatal intensive care unit hospitalization. Sci Total Environ. 2022;850:157830.
Svensson K, Gennings C, Lindh C, Kiviranta H, Rantakokko P, Wikström S, Bornehag C-G. Prenatal exposures to mixtures of endocrine disrupting chemicals and sex-specific associations with children’s BMI and overweight at 5.5 years of age in the SELMA study. Environ Int. 2023;179:108176.
Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE. Is the incidence of rheumatoid arthritis rising? Results from Olmsted County, Minnesota, 1955–2007. Arthr Rhuem. 2010;62(6):1576–82.
Hunter TM, Boytsov NN, Zhang X, Schroeder K, Michaud K, Araujo AB. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol Int. 2017;37:1551–7.
Abraham K, Mielke H, Fromme H, Völkel W, Menzel J, Peiser M, Zepp F, Willich SN, Weikert C. Internal exposure to perfluoroalkyl substances (PFASs) and biological markers in 101 healthy 1-year-old children: associations between levels of perfluorooctanoic acid (PFOA) and vaccine response. Arch Toxicol. 2020;94(6):2131–47.
Grandjean P, Heilmann C, Weihe P, Nielsen F, Mogensen UB, Budtz-Jørgensen E. Serum vaccine antibody concentrations in adolescents exposed to perfluorinated compounds. Environ Health Perspect. 2017;125(7):077018.
Timmermann CAG, Jensen KJ, Nielsen F, Budtz-Jørgensen E, van der Klis F, Benn CS, Grandjean P, Fisker AB. Serum perfluoroalkyl substances, vaccine responses, and morbidity in a cohort of Guinea-Bissau children. Environ Health Perspect. 2020;128(8):087002.
Bamai YA, Goudarzi H, Araki A, Okada E, Kashino I, Miyashita C, Kishi R. Effect of prenatal exposure to per-and polyfluoroalkyl substances on childhood allergies and common infectious diseases in children up to age 7 years: the Hokkaido study on environment and children’s health. Environ Int. 2020;143:105979.
Averina M, Brox J, Huber S, Furberg A-S, Sørensen M. Serum perfluoroalkyl substances (PFAS) and risk of asthma and various allergies in adolescents. The Tromsø study Fit futures in Northern Norway. Environ Res. 2019;169:114–21.
Kvalem HE, Nygaard UC, Carlsen KL, Carlsen K-H, Haug LS, Granum B. Perfluoroalkyl substances, airways infections, allergy and asthma related health outcomes–implications of gender, exposure period and study design. Environ Int. 2020;134:105259.
Bulka CM, Avula V, Fry RC. Associations of exposure to perfluoroalkyl substances individually and in mixtures with persistent infections: recent findings from NHANES 1999–2016. Environ Pollut. 2021;275:116619.
DeWitt JC, Blossom SJ, Schaider LA. Exposure to per-fluoroalkyl and polyfluoroalkyl substances leads to immunotoxicity: epidemiological and toxicological evidence. J Expo Sci Environ Epidemiol. 2019;29(2):148–56.
Lina C, Conghua W, Nan L, Ping Z. Combined treatment of etanercept and MTX reverses Th1/Th2, Th17/Treg imbalance in patients with rheumatoid arthritis. J Clin Immunol. 2011;31:596–605.
Weyand CM, Goronzy JJ. Pathogenesis of rheumatoid arthritis. Med Clin. 1997;81(1):29–55.
Hirota K, Hashimoto M, Yoshitomi H, Tanaka S, Nomura T, Yamaguchi T, Iwakura Y, Sakaguchi N, Sakaguchi S. T cell self-reactivity forms a cytokine milieu for spontaneous development of IL-17 + th cells that cause autoimmune arthritis. J Exp Med. 2007;204(1):41–7.
Zhu Y, Qin X-D, Zeng X-W, Paul G, Morawska L, Su M-W, Tsai C-H, Wang S-Q, Lee YL, Dong G-H. Associations of serum perfluoroalkyl acid levels with T-helper cell-specific cytokines in children: by gender and asthma status. Sci Total Environ. 2016;559:166–73.
Li R, Guo C, Lin X, Chan TF, Lai KP, Chen J. Integrative omics analyses uncover the mechanism underlying the immunotoxicity of perfluorooctanesulfonate in human lymphocytes. Chemosphere. 2020;256:127062.
Zheng L, Dong G-H, Zhang Y-H, Liang Z-F, Jin Y-H, He Q-C. Type 1 and type 2 cytokines imbalance in adult male C57BL/6 mice following a 7-day oral exposure to perfluorooctanesulfonate (PFOS). J Immunotoxicol. 2011;8(1):30–8.
Zhong S-Q, Chen Z-X, Kong M-L, Xie Y-Q, Zhou Y, Qin X-D, Paul G, Zeng X-W, Dong G-H. Testosterone-mediated endocrine function and TH1/TH2 cytokine balance after prenatal exposure to perfluorooctane sulfonate: by sex status. Int J Mol Sci. 2016;17(9):1509.
He C, Feng P, Su H, Gu A, Yan Z, Zhu X. Disrupted Th1/Th2 balance in patients with rheumatoid arthritis (RA). Int J Clin Exp Pathol. 2017;10(2):1233–42.
Nyström J, Benskin JP, Plassmann M, Sandblom O, Glynn A, Lampa E, Gyllenhammar I, Moraeus L, Lignell S. Demographic, life-style and physiological determinants of serum per-and polyfluoroalkyl substance (PFAS) concentrations in a national cross-sectional survey of Swedish adolescents. Environ Res. 2022;208:112674.
Dunder L, Salihovic S, Elmståhl S, Lind PM, Lind L. Associations between per-and polyfluoroalkyl substances (PFAS) and diabetes in two population-based cohort studies from Sweden. J Expo Sci Environ Epidemiol 2023:1–9.
Hall SM, Zhang S, Hoffman K, Miranda ML, Stapleton HM. Concentrations of per-and polyfluoroalkyl substances (PFAS) in human placental tissues and associations with birth outcomes. Chemosphere. 2022;295:133873.
Rickard BP, Rizvi I, Fenton SE. Per-and poly-fluoroalkyl substances (PFAS) and female reproductive outcomes: PFAS elimination, endocrine-mediated effects, and disease. Toxicology. 2022;465:153031.
Xie X, Weng X, Liu S, Chen J, Guo X, Gao X, Fei Q, Hao G, Jing C, Feng L. Perfluoroalkyl and polyfluoroalkyl substance exposure and association with sex hormone concentrations: results from the NHANES 2015–2016. Environ Sci Europe. 2021;33(1):1–12.
Wang Y, Aimuzi R, Nian M, Zhang Y, Luo K, Zhang J. Perfluoroalkyl substances and sex hormones in postmenopausal women: NHANES 2013–2016. Environ Int. 2021;149:106408.
He Y, Hu C, Zhang Y, Fan X, Gao W, Fang J, Wang Y, Xu Y, Jin L. Association of perfluoroalkyl and polyfluoroalkyl substances with sex hormones in children and adolescents 6–19 years of age. Environ Pollut. 2023;329:121707.
Cutolo M, Villaggio B, Craviotto C, Pizzorni C, Seriolo B, Sulli A. Sex hormones and rheumatoid arthritis. Autoimmun rev. 2002;1(5):284–9.
Wahlang B. Sex differences in toxicant-associated fatty liver disease. J Endocrinol 2023, 258(1).
Roth K, Yang Z, Agarwal M, Liu W, Peng Z, Long Z, Birbeck J, Westrick J, Liu W, Petriello MC. Exposure to a mixture of legacy, alternative, and replacement per- and polyfluoroalkyl substances (PFAS) results in sex-dependent modulation of cholesterol metabolism and liver injury. Environ Int. 2021;157:106843.
Olsen GW, Burris JM, Ehresman DJ, Froehlich JW, Seacat AM, Butenhoff JL, Zobel LR. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ Health Perspect. 2007;115(9):1298–305.
Acknowledgements
We extend our special thanks to Drs. Stefano Renzetti and Katherine Svensson for their invaluable advice and guidance on the application of repeated holdout Weighted Quantile Sum methods in our study.
Funding
This study was supported the National Innovation and Entrepreneurship Training Program for College Students (grant number 202210366019), the Key Projects of Natural Science Research of Anhui Provincial Department of Education (grant number 2023AH050603), and the Excellence in Doctoral Education and Training Enhancement Program.
Author information
Authors and Affiliations
Contributions
Study concept and design: C-YH and X-JZ. Acquisition of data: J-CQ. Analysis of data: J-CQ, Z-HL, M-YZ, and Y-BM. Interpretation of data: All authors. Drafting of the manuscript: C-YH and J-CQ. Critical revision of the manuscript for important intellectual content: All authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qiao, JC., Li, ZH., Ma, YB. et al. Associations of per- and polyfluoroalkyl substances (PFAS) and their mixture with risk of rheumatoid arthritis in the U.S. adult population. Environ Health 23, 38 (2024). https://doi.org/10.1186/s12940-024-01073-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-024-01073-3