
Abstract
Background
Humans are widely exposed to perfluoroalkyl substances (PFAS), which have been found to be associated with various adverse birth outcomes. As blood pressure (BP) is an important parameter reflecting cardiovascular health in early life, it is necessary to investigate the association of PFAS exposure during early lifetime and BP in childhood. Therefore, we investigated the potential association between PFAS levels in umbilical cord blood and BP of the offspring at 4 years of age in a prospective cohort study.
Methods
PFAS in umbilical cord blood samples after birth were measured with high-performance liquid chromatography/tandem mass spectrometry in the Shanghai Birth Cohort. BP was measured at 4 years of age in the offspring. Multiple linear regression model was used to investigate the association between individual PFAS level and BP of the offspring. Bayesian kernel machine regression (BKMR) was used to analyze the relationship between the PFAS mixture and BP of the offspring, while weighted quantile sum (WQS) regression was utilized for sensitivity analysis.
Results
A total of 129 mother-child pairs were included in our analysis. In multiple linear regressions, we observed that long-chain PFAS, mainly including perfluorooctane sulfonate (PFOS), perfluorodecanoic acid (PFDA) and perfluoroundecanoic acid (PFUA), was negatively associated with systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial blood pressure (MAP). BKMR showed that an increase in umbilical cord blood PFAS mixture levels was significantly associated with a decrease in SBP, DBP and MAP [Estimated differences (SD): -0.433 (0.161); -0.437 (0.176); -0.382 (0.179), respectively]. The most important component in the association with SBP, DBP, and MAP was PFUA. PFDoA was found to be positively associated with SBP, DBP and MAP in both models. Sensitivity analysis with WQS regression showed consistent results.
Conclusion
Our findings suggested that umbilical blood PFAS exposure was negatively associated with BP in offspring at 4 years of age, including SBP, DBP, and MAP.
Similar content being viewed by others


Background
Perfluoroalkyl substances (PFAS) are a series of organic fluoride compounds, which contain one or more carbon with fluorine in place of hydrogen atoms [1]. Because of their chemical and thermal stability, they are widely used in industrial processes and the production of consumer goods. Humans can be exposed through the air, food, and water [2]. Meanwhile, these physicochemical properties resulted in a long half-life and bioaccumulation in human bodies and the environment [3]. PFAS could cross the placenta and be detected in umbilical cord blood, which might harm fetal development [4].
According to the developmental origins of health and disease (DOHaD) hypothesis, the abnormal intrauterine environment and prenatal exposure can lead to abnormal offspring development and an increased risk of diseases during adulthood [5]. As a widely existing organic compound, PFAS exposure has been found to be associated with a lot of adverse birth outcomes, including low birth weight, preterm birth, intrauterine growth restriction [3, 6], thyroid dysfunction [7], and nervous dysplasia [8]. As blood pressure (BP) is an important parameter of early life cardiovascular health, it is important to investigate the association between PFAS exposure and BP. However, in terms of the correlation between PFAS exposure and children’s BP, current evidences remain controversial. Two studies have found serum PFAS levels in children were positively associated with their BP [9, 10], while four other studies have showed that neither prenatal nor postnatal PFAS exposure was associated with BP of the offspring [11,12,13,14]. Furthermore, the concentrations of PFAS in umbilical cord blood reflects the exposure level of the fetus after filtration through the placental barrier [15,16,17], which might provide additional evidence for early life time PFAS exposure, and there has been no evidence about the association between PFAS levels in umbilical cord blood and offspring BP. Therefore, since these inconsistent and relative deficient evidences, further investigations between umbilical cord blood PFAS exposure and offspring BP levels are in need.
This study aimed to explore the association between individual and mixture PFAS exposure in umbilical cord blood with offspring’s BP in early childhood.
Materials and methods
Study design and participants
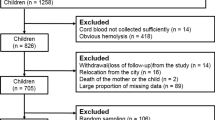
The present analysis was based on the Shanghai Birth Cohort (SBC). A detailed description of the cohort was previously published [18]. In brief, 255 mother-child pairs with data of PFAS levels in umbilical cord blood were recruited between 2013 and 2016 at 6 SBC participating hospitals [19]. At admission to the study, structured questionnaires were filled in with participants’ basic characteristics, medical records, lifestyle with the assist of well-trained staff. Regular follow-ups were carried out for anthropometric indicators of children including weight, height, and body mass index (BMI) from birth to 4 years of age. The 4-year -old follow-up was conducted from 2018 to 2021. Cord blood samples were collected after birth. Among the 255 mother-child pairs, after exclusion of participants with loss-to-follow-up, miscarriages, stillbirths, and lack of BP data at 4 years old, 129 offspring accomplished BP measurements at 4 years old. This research was approved by the Research Ethics Committees from Xinhua Hospital affiliated to Shanghai Jiao Tong University School of Medicine (XHEC-C-3-001-3). Written informed consents were acquired from all parents or guardians of participants before enrollment.
PFAS Concentration Measurement
Cord blood samples were collected after birth and immediately centrifuged and frozen at − 80 °C. A detailed description of the collective and analytical method was published elsewhere [20]. In brief, a total of 10 targeted PFAS, including perfluorooctanate (PFOA), perfluorodecanoic acid (PFDA), perfluorooctane sulfonate (PFOS), perfluorohexanesulfonate (PFHxS), perfluorononanoic acid (PFNA), perfluoroundecanoic acid (PFUA), perfluorobutane sulfonate (PFBS), perfluoroheptanoic acid (PFHpA), perfluorododecanoic acid (PFDoA) and perfluorooctane sulfonamide (PFOSA) were quantified in 100 µl plasma using high-performance liquid chromatography/tandem mass spectrometry (HPLC/MS-MS; Agilent1290–6490, Agilent Technologies Inc., USA). PFOSA was not included in the further analysis as it was detected in only 52.7% of samples while other PFAS substances were detected in all samples. The intra-assay coefficients of variation (CV) were between 0.8 and 8.5% and the inter-assay CV were between 1.7 and 8.4% [21].
BP measurements
Systolic BP (SBP) and diastolic BP (DBP) of the children were assessed in the supine position by trained staff members on the left arm at heart level with the appropriate cuff size for arm circumference by the OMRAN HBP-1300 automatic BP device (Omron Healthcare, Guangzhou, China) [22, 23]. After the child relaxed, three measurements were taken at 5-min intervals. The mean of the last 2 measurements was used in all analyses. The mean arterial BP (MAP) was calculated by the formula [MAP=(SBP + DBP×2)/3]. Pulse pressure (PP) was calculated as SBP - DBP.
Statistics analysis
In order to increase the normality of the data, ln-transformation of PFAS concentrations was conducted. The assessment of the bivariate correlation among the different PFAS substances was carried out by Spearman correlation and cluster analysis (Figure S1).
The assessment of the relationship between individual PFAS chemical and BP was applied by a multiple linear regression model. Model 1 was adjusted for household income, educational levels, hypertensive disorder complicating pregnancy (HDP), gestational diabetes mellitus (GDM), drinking history, passive smoking history, and maternal age. Model 2 was adjusted for birthweight, sex, BMI at 4 year of age, and confounder adjusted in Model 1 [24,25,26,27].
The assessment of the combined effects of the PFAS mixture and BP was conducted by the nonparametric Bayesian kernel machine regression (BKMR) with the R packages of “bkmr”. The BKMR flexibly models the exposure-response relationship with a Gaussian kernel function [28]. The differences between all PFAS levels fixed at a specific quartile compared to their 50th percentile after a total of 20,000 iterations indicated the combined effects of PFAS mixture in umbilical cord blood on BP, which was presented as estimated differences and standard deviation (SD). The weights of the effect on the outcome were represented by estimated conditional posterior inclusion probabilities (condPIPs) of different PFAS substances. The model was adjusted for household income, educational levels, GDM, HDP, drinking history, passive smoking history, maternal age, birthweight, sex and BMI of children.
Weighted quantile sum (WQS) regression was conducted using the ‘gWQS’ packages [29]. A total of 10,000 bootstrap samples were generated from the full data set and used to estimate weights for each PFAS. The WQS index was used to estimate the combined effect of the PFAS mixture on BP. The corresponding average weight of each PFAS was calculated to identify the important component.
Nonlinear association was investigated with restricted cubic spline (RCS) based on four knots of PFAS levels using ‘ggrcs’ R packages. RCS models were adjusted for household income, educational levels, GDM, HDP, drinking history, passive smoking history, maternal age, birthweight, sex and BMI of children. Tests for non-linearity were conducted by using analysis of variance tests. Sex-subgroup analysis was performed with multiple linear regression models and adjusted for the same covariates. An interactive effect analysis of individual PFAS level and sex was also conducted in subgroup analysis.
All the analyses were performed using the STATA software, version 15.0 (Stata Corporation, College Station, TX, USA) and R version 4.0.4 (R Foundation for Statistical Computing) with p < 0.05 were considered statistically significant.
Results
The general characteristics of the study population are presented in Table 1. The mean (SD) maternal age was 31.2 (3.1) years old. Most mothers had a bachelor’s degree and nearly half had a household income ≥ 100,000 RMB/year. There are 5 (3.9%) mothers who had HDP and 12 (9.3%) mothers who had GDM during pregnancy. The mean gestational age, birth weight, birth height and BMI of the offspring at 4 years old was 38.9 (1.3) weeks, 3.4 (0.4) kg, 50.0 (1.0) cm and 15.0 (1.5) kg/m2, respectively. The mean SBP, DBP, MAP, and PP were 98.4 (7.9), 57.5 (6.2), 71.2 (5.8), and 41.2 (6.3), respectively.
The distribution of PFAS detected in umbilical cord blood was described with median and inter-quartile range. The limit of detection (LOD) and the detected rate of each PFAS were shown in Table 2. The highest median concentration of PFAS in umbilical blood was PFOA (7.29ng/ml), followed by PFOS (3.14ng/ml), PFNA (0.63ng/ml), PFHxS(0.46ng/ml), PFDA (0.39ng/ml), PFUA (0.37ng/ml), PFOSA (0.17ng/ml), PFBS (0.13ng/ml), PFHpA (0.12ng/ml), PFDoA (0.09ng/ml). Nine PFAS had detection rates of 100%, except for PFOSA, which was excluded from the further analyses. The PFAS concentrations were highly correlated (Figure S1).
Multiple linear regression models were used to investigate the association between individual umbilical PFAS concentration and BP of the offspring. PFOS had a negative correlation with SBP after confounders adjustment (PFOS: β=-3.10, 95%CI: -5.20, -0.89). In terms of DBP, we found that PFDA, PFOS, and PFUA were inversely associated with DBP (PFDA: β=-2.31, 95%CI: -4.56, -0.06; PFOS: β=-2.15, 95%CI: -4.04, -0.33; PFUA: β=-2.48, 95%CI: -4.91, -0.11). Besides, PFDA and PFOS were also negatively correlated with MAP (PFDA: β=-2.30, 95%CI: -4.42, -0.22; PFOS: β=-1.96, 95%CI: -3.72, -0.24). Meanwhile, we also found that PFDoA and PFHpA showed a positive trend with BP of offspring (Table 3).
As there might be a sex disparity of the influence of PFAS [30], we further conducted a sex subgroup analysis and an interactive effect analysis of PFAS and sex with multiple linear regression models. It indicated that the negative association of PFDA, PFOS and PFUA with BP was mainly showed in boys, while the positive association of PFDoA and PFHpA with BP was mainly showed in girls (Table S3). Besides, we found that in terms of SBP, DBP and MAP, the interactive effect was generally not significant, only PFDoA and sex showed a significant interactive effect in the association between PFDoA and SBP. Moreover, long-chain PFAS showed a significant interactive effect with sex in the association between them and PP (Table S3).
The PFAS mixture in cord blood was significantly associated with lower SBP, DBP and MAP, but not with PP. When all PFAS mixture were fixed at the 75th percentile, in comparison to at their 50th percentile, SBP, DBP and MAP significantly decreased [Estimated differences (SD): -0.433 (0.161); -0.437 (0.176); -0.382 (0.179) respectively) (Fig. 1, Table S1). To characterize the contribution of individual PFAS chemical to the overall effect, we further estimated the association of an inter-quartile range increase of each PFAS on BP when others were set at different percentile levels [29]. Generally, all the PFAS substances showed a negative correlation with SBP, DBP and PP, except that PFDoA showed a positive association with them (Figure S2). The main contribution of the effect of PFAS on SBP, DBP, and MAP was PFUA (condPIP = 0.871, condPIP = 0.753, condPIP = 0.684, respectively) (Table 4), with an inversed relationship (Figure S2). Among all the PFAS substances in umbilical blood, the effect of PFUA on SBP and DBP was significant when all of the other PFAS were fixed at 25th and 50th percentile levels, except that when all of the other PFAS were fixed at 75th, the correlation became not significant. (Figure S3). In general, the univariate exposure-response relationship analysis in BKMR showed the consistent results with multiple linear regression models.

Joint associations of umbilical cord blood PFAS mixture (ln-transformed) with children BP (A. SBP, B. DBP, C. MAP, D. PP) estimated by Bayesian kernel machine regression (BKMR) (N = 129). The figure plotted the estimated differences and 95% CIs in the BP when all the PFAS were fixed at a specific quantile (from 0.25 to 0.75) compared to all the PFAS at their 50th percentile. The results were adjusted for household income, educational levels, GDM, HDP, drink history, passive smoke history, age of mom, birthweight, sex and BMI of children. SBP: systolic blood pressure, DBP: diastolic blood pressure, MAP: mean artery pressure, PP: pulse pressure, BMI: body mass index, HDP: hypertensive disorders in pregnancy, GDM: gestational diabetes mellitus
In WQS regression models, the WQS index was negatively associated with BP in general (Table S2), which was similar to the results of BKMR. Likewise, the directions of the contribution of PFUA were consistent with BKMR (Figure S4).
In terms of nonlinearity, most PFAS substances didn’t show a nonlinear association with children’s BP. Only PFBS showed an inverse U-shape curve with DBP (P for nonlinearity = 0.008) and MAP (P for nonlinearity = 0.017) (Figure S5-S8).
Discussion
This study aimed to investigate the individual and combined effects of multiple PFAS in umbilical cord blood and BP in offspring. In individual models, PFOS showed a negative correlation with SBP. PFDA, PFOS and PFUA were inversely associated with DBP. PFDA and PFOS were also negatively correlated with MAP. In mixture analysis, a significantly inverse association of PFAS mixture in umbilical cord blood with SBP, DBP and MAP of offspring was found, using both BKMR and WQS regression. PFDoA showed a positive association with SBP, DBP and MAP in both multiple linear regression models and BKMR.
To our knowledge, this was the first prospective cohort study that reported the negative association between multiple PFAS in umbilical cord blood and BP in offspring. Currently, there have been a series of studies on the impact of individual PFAS exposure on gestational age, fetal development [31], neurodevelopment [32], behavioral problem [33], endocrine function [34, 35], and immune function [36]. But the relationship between PFAS and BP is inconsistent. Two prospective cohort studies have found no significant association between individual PFAS exposure and BP of offspring [11, 12]. Furthermore, cross-sectional studies also had also found no association between children’s serum PFAS concentration and their own BP level [13, 14]. However, two studies had found that children’s serum PFAS concentration was positively correlated with elevated BP [9, 10]. For adults, one study has found a significantly positive association between early pregnancy plasma PFAS levels and gestational hypertension [37], while another study has found a positive but not significant trend [38]. In the pre-diabetic population, a small but significant positive association of PFOA and N-methyl-perfluorooctane sulfonamido acetic acid (MeFOSAA) with BP has been found [39].
Furthermore, most current studies focused on individual PFAS substances and BP of children, mainly focused on long-chain PFAS including PFOS, PFOA, PFNA, PFDA and PFUA [9,10,11,12,13,14], which lack studies on mixture PFAS exposure during pregnancy. Our study revealed that PFAS mixture exposure in umbilical cord blood was negatively associated with SBP, DBP and MAP in 4-year-old young children, while the most important contributor to the combined effect was PFUA. As far as we know, there has been no evidence on the association between PFUA and BP of the offspring. Besides, our study also found the sex disparity of the effect of umbilical PFAS levels and offspring BP, which has not been explored in previous studies [9, 10]. Negative association between PFDA, PFOS and PFUA with BP was mainly showed in boys, while the positive association of PFDoA and PFHpA with BP was mainly showed in girls.
PFAS, as a kind of organic chemical pollutant with diverse and complicated structures, have different permeability and toxicity for humans [40,41,42,43]. The length of the carbon chain of PFAS can strongly affect their toxicity. As such, long-chain PFAS is more toxic than short-chain PFAS [41]. Our results demonstrated that the inverse association between PFAS and BP of the offspring mainly resulted from long-chain PFAS. Long-chain PFAS exposure, especially PFDA, PFOS, and PFUA were significantly negatively associated with BP of the offspring, among which PFUA contributed mainly to the impact of the mixed PFAS exposure. However, the short-chain PFAS showed no significant association with BP of the offspring. Moreover, we also found that there was a positive trend between PFDoA and BP of the offspring with both multiple linear regression and BKMR. Only one cohort study has investigated the association between individual PFDoA levels in maternal serum and the risk of gestational hypertension, and demonstrated an inverse relationship, which is inconsistent with our results [44]. Thus, further studies with larger sample size, multiple regions and detailed evaluation of BP are in need.
As BP is affected by cardiac output, cardiac function, and peripheral vascular resistance. SBP, DBP, and MAP are influenced by cardiac output and function, while PP reflects the stiffness of the peripheral blood vessels. Our previous study found that prenatal PFAS exposure might be associated with a decrease in left ventricular wall thickness, intraventricular septum thickness [45]. Therefore, we speculated that PFAS might influence BP by reducing cardiac output or function but not by vascular resistance [46]. To further investigate the potential mechanism behind the negative association between PFAS exposure and BP in offspring, a group of animal experiments were conducted. One study using zebrafish as a study model has shown that PFOA exposure during the embryonic development might result in low heart rate and affect the contraction of the myocardial cell (MC) by increasing the apoptosis of MC [47]. Another study using mouse model to investigate PFOA exposure during pregnancy has shown that PFOA exposure may cause microcardia probably through mitochondrial dysfunction induced by reactive oxygen species (ROS) release [48]. Low heart rate, reduction of the cardiac chambers, and impairment of the contraction of MC might affect the contraction of the heart and lead to reduced BP as follow. Moreover, as one kind of endocrine disruptor chemical (EDCs), PFAScna affect BP through disrupted endocrine function. A cross-species with molecular dynamics has suggested that the binding affinity of PFOS and estrogen receptor-α(ER-α) is much stronger in human beings, which signified that PFAS might combine with ER-α [49]. A series of studies have demonstrated that PFAS could mimic the function of estrogen and activate the estrogen-responsive gene expression [50, 51], while estrogen could serve as a vasodilator and lower BP [52].
Our study was the first to evaluate the association between PFAS concentrations in umbilical cord blood and blood pressure in the offspring. Most of researches focused on the hypertension but studies with results of low blood pressure rarely reported. That might be the reason that exploration on PFAS and blood pressure was so few. Besides, we used multiple PFAS levels as exposure and evaluated both mixed exposure and individual exposure. We chose PFAS levels in umbilical cord blood, which eliminated the impact of the placental barrier and were representative of the real exposed situation in utero.
Nevertheless, we still had several limitations in our study. First, we only investigated the relationship between umbilical cord blood PFAS levels and the BP in offspring. As a prospective cohort study conducted in Shanghai, China, the volunteers were mainly focused on the long-term residents in Shanghai, which might lead to a selection bias of the regions, occupations, and nations. Besides, the lack of postnatal PFAS exposure of the offspring was a potential study limitation. One study found that postnatal PFAS exposure through lactation accounted for a proportion of the total perinatal PFAS exposure, which revealed that postnatal PFAS exposure should be taken into concern [53]. Further research, with detailed pediatric echocardiography, a larger sample, and multiple regions included, would be helpful to validate our findings.
Conclusions
Our prospective cohort study demonstrated that in individual analysis, long-chain PFAS showed an inverse association with BP of the offspring, which was mainly found in boys, while PFDoA showed a positive correlation, while was mainly found in girls. In mixture analysis, higher umbilical cord PFAS levels were associated with decreased BP of the offspring. Similarly, long-chain PFAS, especially PFUA, played a dominant role in this negative effect. These findings may have essential public health implications for the management of BP of 4-year-old children. Therefore, it might be important to inspect PFAS exposure during early life time, which has an association with cardiovascular health later in life.
Data Availability
Deidentified individual participant data (including data dictionaries) will be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. Proposals should be submitted to wangjian@xinhuamed.com.cn.
Abbreviations
- PFAS:
-
Perfluoroalkyl substances
- DOHaD:
-
developmental origins of health and disease
- BP:
-
blood pressure
- SBC:
-
Shanghai Birth Cohort
- BMI:
-
body mass index
- PFOA:
-
perfluorooctanate
- PFOS:
-
perfluorooctane sulfonate
- PFNA:
-
perfluorononanoic acid
- PFDA:
-
perfluorodecanoic acid
- PFUA:
-
perfluoroundecanoic acid
- PFHxS:
-
perfluorohexanesulfonate
- PFOSA:
-
perfluorooctane sulfonamide
- PFBS:
-
perfluorobutane sulfonate
- PFDoA:
-
perfluorododecanoic acid
- PFHpA:
-
perfluoroheptanoic acid
- CV:
-
coefficients of variation
- SBP:
-
systolic blood pressure
- DBP:
-
diastolic blood pressure
- MAP:
-
mean arterial pressure
- PP:
-
pulse pressure
- GDM:
-
gestational diabetes mellitus
- HDP:
-
hypertensive disorder complicating pregnancy
- BKMR:
-
Bayesian kernel machine regression
- CI:
-
confidential intervals
- condPIPs:
-
conditional posterior inclusion probabilities
- WQS:
-
weighted quantile sum
- GH:
-
gestational hypertension
- MeFOSAA:
-
N-methyl-perfluorooctane sulfonamido acetic acid
- MC:
-
myocardial cell
- ROS:
-
reactive oxygen species
- EDCs:
-
endocrine disruptor chemical
- ER-α:
-
estrogen receptor-α
References
Blake BE, Fenton SE. Early life exposure to per- and polyfluoroalkyl substances (PFAS) and latent health outcomes: a review including the placenta as a target tissue and possible driver of peri- and postnatal effects. Toxicology. 2020;443:152565.
De Silva AO, Armitage JM, Bruton TA, Dassuncao C, Heiger-Bernays W, Hu XC, et al. PFAS exposure pathways for humans and Wildlife: a synthesis of current knowledge and key gaps in understanding. Environ Toxicol Chem. 2021;40(3):631–57.
Lee YJ, Jung HW, Kim HY, Choi YJ, Lee YA. Early-life exposure to Per- and poly-fluorinated Alkyl Substances and Growth, Adiposity, and puberty in children: a systematic review. Front Endocrinol (Lausanne). 2021;12:683297.
Cao W, Liu X, Liu X, Zhou Y, Zhang X, Tian H, et al. Perfluoroalkyl substances in umbilical cord serum and gestational and postnatal growth in a chinese birth cohort. Environ Int. 2018;116:197–205.
Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412–7.
Negri E, Metruccio F, Guercio V, Tosti L, Benfenati E, Bonzi R, et al. Exposure to PFOA and PFOS and fetal growth: a critical merging of toxicological and epidemiological data. Crit Rev Toxicol. 2017;47(6):482–508.
Ballesteros V, Costa O, Iniguez C, Fletcher T, Ballester F, Lopez-Espinosa MJ. Exposure to perfluoroalkyl substances and thyroid function in pregnant women and children: a systematic review of epidemiologic studies. Environ Int. 2017;99:15–28.
Liew Z, Goudarzi H, Oulhote Y. Developmental Exposures to Perfluoroalkyl substances (PFASs): an update of Associated Health Outcomes. Curr Environ Health Rep. 2018;5(1):1–19.
Averina M, Brox J, Huber S, Furberg A-S. Exposure to perfluoroalkyl substances (PFAS) and dyslipidemia, hypertension and obesity in adolescents. The Fit Futures study. Environmental Research. 2021;195.
Khalil N, Ebert JR, Honda M, Lee M, Nahhas RW, Koskela A, et al. Perfluoroalkyl substances, bone density, and cardio-metabolic risk factors in obese 8–12 year old children: a pilot study. Environ Res. 2018;160:314–21.
Warembourg C, Maitre L, Tamayo-Uria I, Fossati S, Roumeliotaki T, Aasvang GM, et al. Early-Life Environmental Exposures and blood pressure in children. J Am Coll Cardiol. 2019;74(10):1317–28.
Manzano-Salgado CB, Casas M, Lopez-Espinosa MJ, Ballester F, Iñiguez C, Martinez D, et al. Prenatal exposure to Perfluoroalkyl Substances and Cardiometabolic Risk in Children from the spanish INMA birth cohort study. Environ Health Perspect. 2017;125(9):097018.
Canova C, Di Nisio A, Barbieri G, Russo F, Fletcher T, Batzella E et al. PFAS concentrations and cardiometabolic traits in highly exposed children and adolescents. Int J Environ Res Public Health. 2021;18(24).
Geiger SD, Xiao J, Shankar A. No association between perfluoroalkyl chemicals and hypertension in children. Integr Blood Press Control. 2014;7:1–7.
Kang H, Kim HS, Yoon YS, Lee J, Kho Y, Lee J et al. Placental transfer and composition of Perfluoroalkyl substances (PFASs): a korean birth panel of parent-infant triads. Toxics. 2021;9(7).
Bao J, Shao LX, Liu Y, Cui SW, Wang X, Lu GL, et al. Target analysis and suspect screening of per- and polyfluoroalkyl substances in paired samples of maternal serum, umbilical cord serum, and placenta near fluorochemical plants in Fuxin, China. Chemosphere. 2022;307(Pt 1):135731.
Manzano-Salgado CB, Casas M, Lopez-Espinosa MJ, Ballester F, Basterrechea M, Grimalt JO, et al. Transfer of perfluoroalkyl substances from mother to fetus in a spanish birth cohort. Environ Res. 2015;142:471–8.
Zhang J, Tian Y, Wang W, Ouyang F, Xu J, Yu X, et al. Cohort profile: the Shanghai Birth Cohort. Int J Epidemiol. 2019;48(1):21–g.
Chen L, Tong C, Huo X, Zhang J, Tian Y, Shanghai Birth C. Prenatal exposure to perfluoroalkyl and polyfluoroalkyl substances and birth outcomes: a longitudinal cohort with repeated measurements. Chemosphere. 2021;267:128899.
Zhou W, Zhang L, Tong C, Fang F, Zhao S, Tian Y, et al. Plasma perfluoroalkyl and polyfluoroalkyl substances concentration and menstrual cycle characteristics in Preconception Women. Environ Health Perspect. 2017;125(6):067012.
Huang R, Chen Q, Zhang L, Luo K, Chen L, Zhao S, et al. Prenatal exposure to perfluoroalkyl and polyfluoroalkyl substances and the risk of hypertensive disorders of pregnancy. Environ Health. 2019;18(1):5.
Wang J, Wu Y, Du B, Li Z, Ye Y, Wang H et al. Growth patterns in early childhood and cardiovascular structure and function at 4 years old: a prospective cohort study. 2021;31(12):3492–501.
Wang J, Du B, Wu Y, Li Z, Chen Q, Zhang X, et al. Association of maternal Gestational Weight Gain with Left Ventricle geometry and function in offspring at 4 years of age: a prospective birth Cohort Study. Front Pead. 2021;9:722385.
Wang Y, Min C, Song X, Zhang H, Yuan C, Chen L, et al. The dose-response relationship between BMI and hypertension based on restricted cubic spline functions in children and adolescents: a cross-sectional study. Front Public Health. 2022;10:870568.
Geelhoed JJ, Fraser A, Tilling K, Benfield L, Davey Smith G, Sattar N, et al. Preeclampsia and gestational hypertension are associated with childhood blood pressure independently of family adiposity measures: the Avon Longitudinal Study of parents and children. Circulation. 2010;122(12):1192–9.
Zhang X, Wang Y, Xiao W, Jiang D, Zhou J, Ye X, et al. Hyperglycaemia in pregnancy and offspring blood pressure: a systematic review and meta-analysis. Diabetol Metab Syndr. 2023;15(1):10.
Du B, Wang H, Wu Y, Li Z, Niu Y, Wang Q, et al. The association of gestational age and birthweight with blood pressure, cardiac structure, and function in 4 years old: a prospective birth cohort study. BMC Med. 2023;21(1):103.
Bobb JF, Claus Henn B, Valeri L, Coull BA. Statistical software for analyzing the health effects of multiple concurrent exposures via bayesian kernel machine regression. Environ Health. 2018;17(1):67.
Carrico C, Gennings C, Wheeler DC, Factor-Litvak P. Characterization of Weighted Quantile Sum Regression for highly correlated data in a risk analysis setting. J Agricultural Biol Environ Stat. 2015;20(1):100–20.
Lopez-Espinosa MJ, Mondal D, Armstrong BG, Eskenazi B, Fletcher T. Perfluoroalkyl Substances, Sex Hormones, and insulin-like growth Factor-1 at 6–9 years of age: a cross-sectional analysis within the C8 Health Project. Environ Health Perspect. 2016;124(8):1269–75.
Chen MH, Ha EH, Wen TW, Su YN, Lien GW, Chen CY, et al. Perfluorinated compounds in umbilical cord blood and adverse birth outcomes. PLoS ONE. 2012;7(8):e42474.
Chen MHHE, Liao HF, Jeng SF, Su YN, Wen TW, Lien GW, Chen CY, Hsieh WS, Chen PC. Perfluorinated compound levels in cord blood and neurodevelopment at 2 years of age. Epidemiology. 2013;24(6):800–8.
Lien GW, Huang CC, Shiu JS, Chen MH, Hsieh WS, Guo YL, et al. Perfluoroalkyl substances in cord blood and attention deficit/hyperactivity disorder symptoms in seven-year-old children. Chemosphere. 2016;156:118–27.
Shah-Kulkarni S, Kim BM, Hong YC, Kim HS, Kwon EJ, Park H, et al. Prenatal exposure to perfluorinated compounds affects thyroid hormone levels in newborn girls. Environ Int. 2016;94:607–13.
Tsai MS, Lin CC, Chen MH, Hsieh WS, Chen PC. Perfluoroalkyl substances and thyroid hormones in cord blood. Environ Pollut. 2017;222:543–8.
Wang IJ, Hsieh WS, Chen CY, Fletcher T, Lien GW, Chiang HL, et al. The effect of prenatal perfluorinated chemicals exposures on pediatric atopy. Environ Res. 2011;111(6):785–91.
Preston EV, Hivert MF, Fleisch AF, Calafat AM, Sagiv SK, Perng W, et al. Early-pregnancy plasma per- and polyfluoroalkyl substance (PFAS) concentrations and hypertensive disorders of pregnancy in the project viva cohort. Environ Int. 2022;165:107335.
Birukov A, Andersen LB, Andersen MS, Nielsen JH, Nielsen F, Kyhl HB, et al. Exposure to perfluoroalkyl substances and blood pressure in pregnancy among 1436 women from the Odense Child Cohort. Environ Int. 2021;151:106442.
Lin PD, Cardenas A, Hauser R, Gold DR, Kleinman KP, Hivert MF, et al. Per- and polyfluoroalkyl substances and blood pressure in pre-diabetic adults-cross-sectional and longitudinal analyses of the diabetes prevention program outcomes study. Environ Int. 2020;137:105573.
Appel M, Forsthuber M, Ramos R, Widhalm R, Granitzer S, Uhl M, et al. The transplacental transfer efficiency of per- and polyfluoroalkyl substances (PFAS): a first meta-analysis. J Toxicol Environ Health B Crit Rev. 2022;25(1):23–42.
Gaballah S, Swank A, Sobus JR, Howey XM, Schmid J, Catron T, et al. Evaluation of Developmental Toxicity, Developmental Neurotoxicity, and tissue dose in zebrafish exposed to GenX and other PFAS. Environ Health Perspect. 2020;128(4):47005.
Sprengel J, Behnisch PA, Besselink H, Brouwer A, Vetter W. In vitro human cell-based TTR-TRβ CALUX assay indicates thyroid hormone transport disruption of short-chain, medium-chain, and long-chain chlorinated paraffins. Arch Toxicol. 2021;95(4):1391–6.
Palazzolo S, Caligiuri I, Sfriso AA, Mauceri M, Rotondo R, Campagnol D et al. Early warnings by liver organoids on short- and long-chain PFAS toxicity. Toxics. 2022;10(2).
Yang L, Ji H, Liang H, Yuan W, Song X, Li X, et al. Associations of perfluoroalkyl and polyfluoroalkyl substances with gestational hypertension and blood pressure during pregnancy: a cohort study. Environ Res. 2022;215(Pt 2):114284.
Wang J, Du B, Wu Y, Li Z, Wang H, Niu Y, et al. Maternal plasma perfluoroalkyl substances concentrations in early pregnancy and cardiovascular development in offspring: a prospective cohort study. Environ Int. 2023;173:107748.
Vennin S, Li Y, Willemet M, Fok H, Gu H, Charlton P, et al. Identifying hemodynamic determinants of pulse pressure: a Combined Numerical and physiological Approach. Hypertension. 2017;70(6):1176–82.
Yu J, Cheng W, Jia M, Chen L, Gu C, Ren HQ, et al. Toxicity of perfluorooctanoic acid on zebrafish early embryonic development determined by single-cell RNA sequencing. J Hazard Mater. 2022;427:127888.
Salimi A, Nikoosiar Jahromi M, Pourahmad J. Maternal exposure causes mitochondrial dysfunction in brain, liver, and heart of mouse fetus: an explanation for perfluorooctanoic acid induced abortion and developmental toxicity. Environ Toxicol. 2019;34(7):878–85.
Qu K, Song J, Zhu Y, Liu Y, Zhao C. Perfluorinated compounds binding to estrogen receptor of different species: a molecular dynamic modeling. J Mol Model. 2018;25(1):1.
Benninghoff AD, Bisson WH, Koch DC, Ehresman DJ, Kolluri SK, Williams DE. Estrogen-like activity of perfluoroalkyl acids in vivo and interaction with human and rainbow trout estrogen receptors in vitro. Toxicol Sci. 2011;120(1):42–58.
Wei Y, Dai J, Liu M, Wang J, Xu M, Zha J, et al. Estrogen-like properties of perfluorooctanoic acid as revealed by expressing hepatic estrogen-responsive genes in rare minnows (Gobiocypris rarus). Environ Toxicol Chem. 2007;26(11):2440–7.
Maranon R, Reckelhoff JF. Sex and gender differences in control of blood pressure. Clin Sci (Lond). 2013;125(7):311–8.
Zheng P, Liu Y, An Q, Yang X, Yin S, Ma LQ, et al. Prenatal and postnatal exposure to emerging and legacy per-/polyfluoroalkyl substances: levels and transfer in maternal serum, cord serum, and breast milk. Sci Total Environ. 2022;812:152446.
Acknowledgements
We thank all children and their families who were involved in this study. We thank the support of the Shanghai Municipal Health Commission (GWIII-26, GWIV-26, 2020CXJQ01) and the Shanghai Jiao Tong University School of Medicine, Xinhua Hospital and the National Human Genetic Resources Sharing Service Platform (2005DKA21300).
Funding
This work was supported by Natural Science Foundation of China (grant numbers: 82130015 and 82100320), Collaborative Innovation Program of Shanghai Municipal Health Commission (grant number: 2020CXJQ01).
Author information
Authors and Affiliations
Contributions
Zhikang Xu and Bowen Du:Conceptualization; Data curation; Formal analysis;Investigation; Methodology; Project administration; Writing - original draft; Writing - review & editing. Hualin Wang, Zhuoyan Li, Yujian Wu, Qianchuo Wang, Yiwei Niu and Qianlong Zhang: Data curation; Methodology;Project administration;Writing - review & editing. Kun Sun: Writing - review & editing, Funding acquisition; Investigation;Methodology. Jian Wang and Sun Chen:Conceptualization; Funding acquisition; Investigation; Methodology;Resources;Supervision; Writing - review & editing.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This research was approved by the Research Ethics Committees from Xinhua Hospital affiliated to Shanghai Jiao Tong University School of Medicine (XHEC-C-3-001-3).
Consent for publication
All parents or guardians of participants signed the written informed consent before enrollment.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, Z., Du, B., Wang, H. et al. Perfluoroalkyl substances in umbilical cord blood and blood pressure in offspring: a prospective cohort study. Environ Health 22, 72 (2023). https://doi.org/10.1186/s12940-023-01023-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-023-01023-5