
Abstract
Background
According to the EU-MIDIS report on discrimination, Roma are the most discriminated against group in Europe. Research suggests that experiencing discrimination may itself be detrimental to health. The aim of this paper is to investigate whether discrimination, hopelessness and social support mediate differences in self-rated health (SRH) between Roma and non-Roma adolescents.
Methods
We conducted a cross-sectional study among Roma from separated and segregated settlements in the eastern part of Slovakia (N = 330; mean age = 14.50; interview) and non-Roma adolescents (N = 722; mean age = 14.86; questionnaire); only non-missing data were used for analyses (n = 759). The effect of perceived discrimination, mother and father social support, and hopelessness on SRH was analysed as crude and adjusted for ethnicity, age, gender, parental education and social desirability. Mediating effects were separately assessed using the Sobel test and structural equation modelling.
Results
Roma adolescents reported poorer SRH and more discrimination, mother and father social support, hopelessness and social desirability. Roma ethnicity (Odds ratio/95 %-Confidence interval 3.27/2.40–4.47), discrimination (2.66/1.82–3.88), hopelessness (1.35/1.20–1.51) and mother (0.92/0.88–0.97) and father social support (0.96/0.93 – 0.997) were statistically significant predictors of poor SRH. Perceived discrimination, social support and hopelessness mediated the ethnicity-health association, with adjustment for social support increasing its strength and the other two variables decreasing it.
Conclusions
Perceived discrimination, social support and hopelessness mediate a part of the association between Roma ethnicity and poor SRH, with discrimination and hopelessness being risk factors and social support a protective factor.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
According to the EU-MIDIS report on discrimination, Roma are the most discriminated group in Europe, and this may still be an underestimation, as under-reporting of discrimination is generally high among Roma [1]. Stereotypes about and prejudices against Roma highly influence their status in society and lead to open and covert discrimination by the non-Roma population [2–4]. Physical attacks by right-wing extremists occur regularly and occasionally result in the death of the victim [5]. Discrimination against Roma also occurs in institutions [2]. A high percentage of Roma reports being discriminated against in health facilities, and research conducted among medical providers confirms that many of them hold prejudicial beliefs about Roma. The most frequently reported manifestations of discrimination include: general practitioners refusing to register Roma clients on their rosters, emergency services not responding to calls from Roma communities, health service providers refusing to treat them, as well as verbal abuse, denial of access to medical records and segregation into maternity wards of inferior quality [6].
Roma are a rather large minority in many Central European countries and generally report poorer health than the non-Roma population. Estimates on their numbers vary; e.g. for Slovakia, they vary from 105,738 (2.0 %) to 750,000 (13.8 %), with 380,000 (7.2 %) probably being the best estimate (2011 census) [7]. Roma adolescents have been shown to perceive their health as poorer than non-Roma adolescents [8], but the mechanisms explaining this finding have not yet been established. One explanation is that their poorer perceived health is simply due to their socioeconomic deprivation and discrimination [6, 8, 9].
Research suggests that experiencing discrimination is itself detrimental to health [10]. This concerns not just exposure but in particular some types of responses to the exposure seem to have health consequences [10]. The association between discrimination and health may occur through the mechanisms of stress responses and health behaviours. The perception of discrimination is related to increased physiological stress responses, more negative psychological stress responses and increased participation in unhealthy behaviours [11]. The negative association between discrimination and health was shown in several studies [12–15].
The poor health of Roma might also be due to factors other than discrimination, such as their on average lower socioeconomic status (SES) compared to the non-Roma population [7]. People with low SES in general perceive their health as poorer, and this association has been shown to be mediated by a number of psychosocial factors such as social support, depression, hopelessness and life satisfaction [16–20]. Self-rated Health (SRH) is a valid indicator of current health status and of future morbidity and mortality [21]. Smith et al. showed that lower SES groups have a higher prevalence of poorer SRH and a higher incidence of many predictors of poor SRH such as physical health problems, mental health problems, health care utilization, and unhealthy behaviours [22]. Another study shows that the probability of reporting poor SRH generally increased when SES became lower or neighbourhoods became more disadvantaged. This finding clearly suggests that the more life resources an individual has, the lower the risk is of reporting poor/very poor health [23]. Given the mostly low SES of Roma, this offers a rather likely explanation for their poor health as well.
In contrast to low SES, social support has a positive relation to health, but it is unknown how this association operates in Roma [24]. Among both adults and adolescents, social support – i.e. resources provided by other people, such as various social networks and relationships – is associated with positive health outcomes and the avoidance of risk-taking behaviour [24]. Klineberg et al. report ethnic differences in social support, with associations between social support and health characteristics being similar across different ethnic groups [24, 25]. Evidence on Roma is completely lacking, but social structures among them are generally strong [26].
Another factor affecting the health of Roma might be hopelessness. In general, disadvantaged people are more likely to perceive themselves as hopeless to change their situation and to improve their quality of life and well-being [27]. Such beliefs have a negative effect on health. Hopelessness correlates positively with depression, predicts suicidal ideation and attempts and psychopathology in general, and is negatively correlated with self-esteem and social skills [28]. Banks et al. found that increased levels of hope were strongly related to reporting fewer depressive symptoms when respondents reported discrimination than among those with lower levels of hope [29]. All in all, perceived discrimination obviously acts as a health-risk factor, and its negative effect might be buffered by a potential health-protective factor such as social support or magnified by the negative health effect of hopelessness.
When a sensitive topic is surveyed, and perceived discrimination might be considered as such a topic, results may be confounded by a respondent’s tendency to answer in a socially desirable way [30]. Social desirability reflects the tendency on behalf of the subjects to deny socially undesirable traits and to claim socially desirable ones, and the tendency to say things which place the speaker in a favourable light [31]. Bardwell and Dimsdale have summarised several studies that reported ethnic differences in response bias [32]. Therefore, such bias should be considered when assessing psychosocial variables by self-report.
The findings about the negative association between Roma ethnicity and their health are widely acknowledged and accepted, but further insight into the pathways leading to this association is lacking. It is also known that Roma face discrimination in everyday life, have higher levels of hopelessness, but receive more social support. All those variables are also known as significant predictors of health. Thus the aim of our study is to test the possible mediating role of those three variables on the ethnicity-health pathway and how those variables contribute to differences in self-rated health between Roma and non-Roma adolescents.
Methods
Sample and procedure
We obtained information on perceived discrimination, self-rated health, hopelessness, parental social support, social desirability and demographic characteristics among Roma and non-Roma adolescents. The Roma sample was recruited via elementary schools in small towns and villages in the eastern part of Slovakia which met the following criteria: the number of children aged 13 years or older living in Roma settlements (segregated and separated type) was at least 30; the school was able to provide 3 or 4 separate rooms where interviews could be conducted without disruption; and the school made an internal list of children suitable for our study, who could then be randomly chosen and asked to participate in the interview. We contacted 22 elementary schools in municipalities in the study area that had separated or segregated communities of Roma whose children could potentially attend the schools. Out of these, 15 met our criteria, though one was not willing to participate. From the lists of pupils living in Roma settlements prepared by the remaining 14 schools, we randomly chose respondents while trying to include a similar proportion of boys and girls. Respondents were interviewed individually during regular class time by community workers who had ample experience in working with Roma and were trained for our study. One hour was scheduled for each interview; they lasted between 30 and 65 minutes.
Because non-Roma pupils in schools with higher proportions of pupils from Roma settlements might not be representative of all non-Roma adolescents, we decided to recruit a non-Roma sample from elementary schools in the same geographical area without an evident Roma community in the neighbourhood. We identified 25 such schools in the Košice and Prešov regions of eastern Slovakia and contacted a random sample of 15 of them. Of these, 11 schools were willing to participate, but two were excluded because they did not have at least one class of 8th and 9th grade that had not been previously included in a research project of our department. The questionnaires were administered during regular class time (45 minutes) by our research assistants, who had training and experience. The questionnaire asked the same questions as the structured interview in the Roma sample.
The study was approved by the Ethics Committee of the Faculty of Science at P.J. Safarik University in Košice. Data were collected in May-June 2007. Parents were informed of the study via the school administration and could opt out if they disagreed. Participation in the study was fully voluntary and anonymous, with no explicit incentives provided for participation.
The sample of Roma adolescents consisted of 330 Roma elementary school pupils, all living in Roma settlements (the segregated and separated types) in the eastern part of Slovakia, in or near small towns and villages (response: 99.7 %). It comprised 160 boys (48.5 %) and 170 girls (51.5 %), with ages ranging from 12 to 17 years (mean 14.50; SD = 1.03). The sample of non-Roma adolescents consisted of 722 elementary school pupils attending the 8th and 9th grades (response 95.9 %). It comprised 354 boys (53.2 %) and 312 (46.8 %) girls. Ages ranged from 14 to 17 years (mean 14.86; SD = 0.63). High response rates were achieved due to the way of acquiring parental consent with the study, using elementary school administration.
Measures
Questionnaires covered demographic (age, gender) and socioeconomic characteristics (father’s and mother’s highest completed education; four levels of education were distinguished: elementary education, apprenticeship, secondary education (with leaving certificate) and university education), one item assessing self-rated health, and scales for social desirability, perceived social support from mother and father, hopelessness and one item for perceived discrimination. All scales and items were translated from the English original to Slovak by means of a forward-backward procedure. An expert panel solved the translation issues that came out of the forward and backward translation. We did not pilot the translated scales.
Perceived discrimination was measured using an item adopted from the ISRD questionnaire [33]: “Have people ever treated you badly because of your religion or the language you speak, or the colour of your skin?” with a four-point scale ((1) No, never, (2) Once, (3) Sometimes, (4) Often). For the purposes of the analyses the four response categories were dichotomized into: No, Never (0) and at least once (1).
Self-rated health (SRH) was measured with one item from the SF-36 questionnaire [34]. Respondents were asked to assess their health (In general, would you say your health is:) as (1) excellent, (2) very good, (3) good, (4) fairly good or (5) bad. First two (1-2) and the last three (3-5) responses were merged into two resulting categories, similarly as was it was performed by Geckova et al., because the standard dichotomisation resulted in unbalanced categories [35]. The use of a different cut-off led to very similar results. This measure is widely used in health studies as an indicator of general health status, because it is a good predictor of mortality and morbidity [36, 37].
Perceived social support from the mother, father and significant others was measured using adapted items from the ‘Spouse/partner perceived social support’ subscale [38]. Items focused on aspects like closeness with the respondent, availability for chatting with the respondent, expressing worth to the respondent, feeling relaxed when together, being available when needed and confidence in the respondent. Mother’s and father’s social support subscales had 6 items, each with the following response categories (values): fully agree (4), agree (3), disagree (2), fully disagree (1). A higher total score indicates a higher level of perceived social support from the person concerned. The internal consistencies of the scales were satisfactory: mother (Cronbach’s alpha: 0.83), father (0.91).
Hopelessness was measured by the brief Hopelessness Scale for Children [39], which contains 5 items from the longer version of Kazdin et al. [40]. The items were: “All I see ahead of me are bad things, not good things; There’s no use in really trying to get something I want because I probably won’t get it; I might as well give up because I can’t make things better for myself; I don’t have good luck now and there’s no reason to think I will when I get older; I never get what I want, so it’s dumb to want anything.” Answers were dichotomous (values): agree (1), disagree (0), with a higher total score indicating a higher level of hopelessness. The internal consistency of the scale was satisfactory (Cronbach’s alpha: 0.70).
Social desirability is the tendency of respondents to reply in a manner that will be viewed favourably by others. Higher social desirability thus can affect the validity of results. It was measured using the Social Desirability Response Set (SDRS-5) [41]. The scale inquires about common situations in which people are prone to respond favourably (e.g.: “No matter who I’m talking to, I’m always a good listener“). The five items are then rated with a five-point Likert scale (definitely true, mostly true, don’t know, mostly false, definitely false). The total score is counted only from the extreme answers of each item (scored 1 point), with a higher total score indicating a higher level of socially desirable responses. Cronbach’s α for the current sample was 0.53, but the mean inter-item correlation was 0.19. According to Clark & Watson [42] and Parker, Taylor, & Bagby [43], consistency is acceptable if the MIIC is above 0.15.
Statistical analysis
From the total number of 1052 respondents we excluded respondents who had missing answers for at least one of the assessed variables (ethnicity, age, gender, mother and father social support, hopelessness, discrimination, social desirability), leaving 759 for analysis. First, we described the samples. Then, the association of ethnicity with (poor) SRH and the way in which discrimination, social support, hopelessness, SES (highest parental education) and social desirability affected this association’, were assessed using multilevel logistic regression in order to take into account the hierarchical nature of sampling (random sample of locality at first level and then random sample of student at second level) (Table 2). As a first step, the crude associations of ethnicity, discrimination, social support, hopelessness and confounding variables (age, gender, parental education, social desirability) with SRH were assessed (Model 1, bivariate model), to see individual associations of independent variables with the dependent one. Next, we adjusted the ethnicity effect separately for perceived discrimination (Model 2), for social support (Model 3) and for hopelessness (Model 4), to see changes in the odds ratios of ethnicity regarding health outcomes after introducing these variables. Similarly, Model 5 tested the ethnicity effect adjusted for discrimination, social support, and hopelessness combined. The last model (Model 6) repeated Model 5 with adjustment for confounders: age, gender, parental education and social desirability, to consider their combined influence on the ethnicity-health association. Possible mediating effects of discrimination, hopelessness and social support on the association between ethnicity and SRH were separately assessed using the Sobel test [44]. The final mediating model was assessed using structural equation modelling. Analyses were performed using IBM SPSS 22.0 and SPSS AMOS 22.0.
Results
The final sample is made up of 759 adolescents, of which non-Roma N = 459 (60.5 %; 234 boys = 51.0 % and 225 girls = 49.0 %) and Roma N = 300 (39.5 %; 147 boys = 49.0 %, 153 and girls = 51.0 %). Basic descriptive statistics of the sample are presented and compared in Table 1.
Roma adolescents reported more perceived discrimination, poorer SRH as well as more mother’s and father’s social support, more hopelessness and more social desirability (Table 1). Roma came from families with parents mostly with elementary education, which reflects the poor educational level among this minority and their lower socioeconomic status.
Logistic regression showed that Roma ethnicity was a significant predictor of poor SRH. Statistically significant crude associations with SRH were also found for discrimination, hopelessness and mother’s and father’s social support. Respondents who reported being discriminated against, lower social support and higher hopelessness were more likely to report poor SRH.
The adjustment for discrimination (Model 2) and hopelessness (Model 4) led to a decrease of the ethnicity effect on SRH of about one-fifth. Adding social support (Model 3) led to an increase of the ethnicity effect on SRH of about 42 %. The adjustment for the discrimination, social support and hopelessness combined (Model 5) decreased the ethnicity effect to a smaller extent than did discrimination and hopelessness separately. Additional adjustment for the confounders (age, gender, parental education, social desirability) led to a decrease of the ethnicity-SRH effect of about one-third (Table 2).
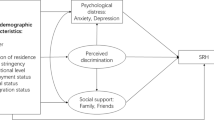
We assessed possible mediation of the above mentioned variables on the ethnicity-SRH effect by using the Sobel test. The Sobel test confirmed that discrimination, hopelessness and mother’s and father social support all were significant mediators of the ethnicity-SRH association (Sobel test values were 4.38***; 4.57***, -2.55** and -2.15*, respectively). Structural equation modelling also confirmed mediation and showed it in a more sophisticated way than simple Sobel tests. A part of the ethnicity effect on SRH was occurring via discrimination, mother’s and father’s social support, and hopelessness with a relatively small effect on SRH although SRH was more strongly influenced by the direct effect of ethnicity as shown in Fig. 1. Thus being Roma implies to have a worse SRH, but with higher perceived social support from mother and father the SRH might slightly improve. More hopelessness and discrimination on the other hand might slightly contribute to a worse SRH. The model also shows the effect of discrimination to be mediated through hopelessness on mother’s and father’s social support but the effect is rather small and almost trivial. The structural equation model yielded good fit as indicated by the goodness-of-fit indices (Chi-square = 4.062, p = 0.131; CMIN/DF = 2.031; CFI = 0.996; RMSEA = 0.033) (Fig. 1).

Structural model of the ethnicity effect on SRH mediated by discrimination, mother’s and father’s social support and hopelessness with indication of the association among variables using standardized coefficients. Note: e – represents residual variance
Discussion
Our aim was to assess the possible mediating role of discrimination, mother’s and father’s social support and hopelessness in the ethnicity-SRH pathway and their contribution to differences in self-rated health between Roma and non-Roma adolescents. Further analysis revealed that discrimination, social support and hopelessness significantly mediated the ethnicity effect on SRH. Being discriminated against and having higher hopelessness consist a relatively great part of negative effect of ethnicity on SRH. Mother’s and father’s social support were also a part of the mediating pathway between ethnicity and SRH and constituted also a part of the pathway but in the opposite direction and social support can diminish the negative effect of discrimination and hopelessness.
Our results support previous findings that perceived discrimination is associated with poorer SRH [12–15]. However, from the simple association of discrimination with SRH we have also shown a more detailed picture enriched by the role of hopelessness and social support controlled for demographics and SES in the pathway between Roma ethnicity and SRH by testing of possible mediators. The mediating role of social support was already reported e.g. by Salonna et al. [45]. Hopelessness was not earlier tested before as a mediating variable in health studies.
Being Roma in our sample implies worse SRH, but this SRH is even worse when the Roma respondent reported being discriminated against. Similarly, feeling hopeless aggravated worse SRH even further. On the other hand, mother’s social support can compensate for the negative effect of ethnicity on health mediated by discrimination and hopelessness. The role of mother’s social support suggests that even the difficult living conditions represented by being Roma, living in a Roma settlement, being discriminated against and feeling hopeless, might by compensated for by a warm relationship with the mother [46]. The buffer effect of social support against the negative effect of perceived discrimination was reported by Ajrouch et al. [47]. What is interesting is that mother’s social support seems to be a more important factor than father’s social support in promoting better SRH.
Hopelessness, after discrimination, appeared to be a very influential factor related to adolescents’ SRH. The higher the hopelessness, the worse the SRH of the adolescent is. The connection of hopelessness with worse well-being and depression is already known [27, 29], and our study expands on the detrimental effect of hopelessness on SRH among adolescents who perceive discrimination, especially Roma adolescents, in whom the level of hopelessness and discrimination is much higher compared with non-Roma counterparts.
The worse SRH of Roma adolescents compared with their non-Roma counterparts might be partially attributed to their perceived discrimination and higher hopelessness, but these two factors do not explain the entire variability of their health. Another very important factor which affects their SRH might be the low education attainment of Roma parents and low SES widely prevalent among Roma living in settlements [8]. When evaluating the effect of several factors relevant for SRH, like discrimination, hopelessness and social support, parental education or other indicators of SES have to be taken into account, because, as our study has shown, every one of them plays an important role in the ethnicity–health relation. Also, there might be other factors related to Roma ethnicity, or their culture and habits, which might impact their health and which were not measured in our study and might confound associations, as parental education did.
Strengths and limitations
Our study was conducted on a Roma sample, which is a hard-to-reach population. We succeeded in recruiting a considerable number of Roma adolescents. In addition, we achieved relatively high response rates in both samples of Roma and non-Roma. Due to the selection of participants with non-missing variables, the sample size was reduced, but the size was still large enough to perform all analyses with no impact on validity.
Besides these strengths, our study also has some limitations. A major limitation of our study may be the different methods of data collection among the Roma and non-Roma samples (interviews vs. questionnaires). We chose these different methods of data collection because in research comparing hard-to-reach groups with other groups, the use of different methodological approaches is sometimes unavoidable; see e.g. a recent study of Crone et al. [48] among ethnic minorities in The Netherlands. Furthermore, feasibility played a role, i.e. the acceptability for the target group and the available resources. It is likely that differences occurred in responses due to different methods of data collection, but Brittingham et al. [49] concluded that such differences tend to be small. The different approach to collect data from Roma than from non-Roma adolescents could have led to higher levels of social desirability among Roma, as disclosure may be lower in an interview [50–52]. Fortunately, we were able to adjust for this, but we cannot exclude some remaining information bias. Another limitation might be the use of a single item measure of perceived discrimination, which may have increased measurement error. However, previous research has shown this to be a valid measure of discrimination [53]. Moreover, its brevity led to a very small item-nonresponse, also increasing the validity of our approach. Finally, the low internal consistency of the social desirability scale (SDRS-5) might be considered as a limitation. The consequences of the low internal consistency of this scale are larger measurement errors and underestimation of its confounding effect.
Discrimination among Roma is a frequently discussed topic without objective and valid data. Our study brings fresh insights and an assessment of perceived discrimination among Roma adolescents compared with non-Roma adolescents.
Implications
Since we found the worse self-rated health among Roma adolescents in comparison with the non-Roma population might be partially explained by higher exposure to perceived discrimination and hopelessness, interventions aiming to counteract such discrimination are justified. One place to start could be balancing the negative image of Roma in media with more positive ones and with education of the non-Roma population about the Roma with intention of replacing various stereotypes, superstitions and myths. Roma adolescents also reported having strong parental support with a protective effect on their self-rated health. This should be maintained and developed in cultural frameworks of this ethnic minority group.
Roma may avoid health services because they have experienced or heard about discrimination in health care settings [54]. A few negative interactions can be amplified in the community, as experiences are told and retold to others [6]. Wider utilisation of the existing Roma health assistants’ (or mediators’) program may be an effective route to prevent this but the project has been established in 2002 but have been used very scarcely until now [55]. E.g. in Slovakia only 0.6 Roma health assistants per 10,000 Roma are employed [56]. Further research on the effectiveness of the application of Roma health assistants’ program is urgently needed. Their work may also provide a means to realise a more positive image of Roma to counteract discrimination and improve the self-rated health of the Roma.
Conclusions
Roma ethnicity, perceived discrimination, social support and hopelessness were the main predictors of poor self-rated health even after controlling for parental education and social desirability. As anticipated, perceived discrimination, like hopelessness, is a contributing factor for poor self-rated health. Parental social support also partially contributes to the effect on SRH, but in the opposite direction than discrimination and hopelessness, and thus protects against poor SRH. Perceived discrimination, hopelessness and mother’s and father’s social support are mediators of the ethnicity-health association. Our study presents one of the first findings about discrimination and health among Roma adolescents and explores potential protective and risk factors in such an association, providing important clues to improving their health.
Abbreviations
- EU-MIDIS:
-
European Union minorities and discrimination survey
- SES:
-
Socioeconomic status
- SRH:
-
Self-rated health
- ISRD:
-
International Self-Report Delinquency Study
- SDRS-5:
-
Social Desirability Response Set
- OR:
-
Odds ratio
- CI:
-
Confidence interval
References
European Union Agency for Fundamental Rights. Housing conditions of Roma and Travellers in the European Unioin. Comparative report. Wien: European Union Agency for Fundamental Rights; 2009.
Fundación Secretariado Gitano. Health and the Roma community, analysis of the situation in Europe. Bulgaria, Czech Republic, Greece, Portugal, Romania, Slovakia, Spain. Madrid: Fundación Secretariado Gitano; 2009.
Mudde C. Racist Extremism in Central and Eastern Europe. London: Routledge; 2005.
Council of Europe. Human Rights of Roma and Travellers in Europe. Strasbourg: Council of Europe Publishing; 2012.
European Roma Rights Centre. Attacks against Roma in Slovakia: January 2008-July 2012. Budapest: European Roma Rights Centre; 2012.
Schaaf M. Roma health. In: Koller T, editor. Poverty and social exclusion in the WHO European Region: health systems respond. Copenhagen: WHO Regional Office for Europe; 2010. p. 226–56.
Filadelfiová J, Gerbery D, Škobla D. Report on the living conditions of Roma in Slovakia. Bratislava: United Nations Development Programme Regional Bureau for Europe; 2007.
Kolarcik P, Geckova AM, Orosova O, van Dijk J, Reijneveld SA. To what extent does socioeconomic status explain differences in health between Roma and non-Roma adolescents in Slovakia? Soc Sci Med. 2009;68(7):1279–84.
Reijneveld SA. Ethnic differences in health and use of health care: the questions to be answered. Int J Public Health. 2010;55(5):353–5.
Richardson LD, Norris M. Access to Health and Health Care: How Race and Ethnicity Matter. Mount Sinai J Med. 2010;77(2):166–77.
Pascoe EA, Richman LS. Perceived Discrimination and Health: A Meta-Analytic Review. Psychol Bull. 2009;135(4):531–54.
D'Anna LH, Ponce NA, Siegel JM. Racial and ethnic health disparities: evidence of discrimination's effects across the SEP spectrum. Ethn Health. 2010;15(2):121–43.
Williams DR, Neighbors HW, Jackson JS. Racial/Ethnic Discrimination and Health: Findings From Community Studies. Am J Public Health. 2008;98:S29–37.
Todorova ILG, Falcón LM, Lincoln AK, Price LL. Perceived discrimination, psychological distress and health. Sociol Health Illn. 2010;32(6):843–61.
Schulz AJ, Israel BA, Gravlee CC, Mentz G, Williams DR, Rowe Z. Discrimination, Symptoms of Depression, and Self-Rated Health Among African American Women in Detroit: Results From a Longitudinal Analysis. Am J Public Health. 2006;96(7):1265–70.
Huurre T, Aro H, Rahkonen O. Well-being and health behaviour by parental socioeconomic status: A follow-up study of adolescents aged 16 until age 32 years. Social Psych Psych Epid. 2003;38(5):249–55.
Panzarella C, Alloy LB, Whitehouse WG. Expanded Hopelessness Theory of Depression: On the Mechanisms by which Social Support Protects Against Depression. Cognit Ther Res. 2006;30(3):307–33.
Proctor C, Linley P, Maltby J. Youth Life Satisfaction: A Review of the Literature. J Happiness Stud. 2009;10(5):583–630.
Roxburgh S. Untangling Inequalities: Gender, Race, and Socioeconomic Differences in Depression. Sociol Forum. 2009;24(2):357–81.
Stansfeld SA, Head J, Marmot MG. Explaining social class differences in depression and well-being. Soc Psych Psych Epid. 1998;33(1):1–9.
Idler EL, Benyamini Y. Self-Rated Health and Mortality: A Review of Twenty-Seven Community Studies. J Health Soc Behav. 1997;38(1):21–37.
Smith PM, Glazier RH, Sibley LM. The predictors of self-rated health and the relationship between self-rated health and health service needs are similar across socioeconomic groups in Canada. J Clin Epidemiol. 2010;63(4):412–21.
Bak CK, Andersen PT, Dokkedal U. The association between social position and self-rated health in 10 deprived neighbourhoods. BMC Public Health. 2015;15(1):512–27.
Klineberg E, Clark C, Bhui KS, Haines MM, Viner RM, Head J, et al. Social support, ethnicity and mental health in adolescents. Soc Psych Psych Epid. 2006;41(9):755–60.
Whitfield KE, Weidner G, Clark R, Anderson NB. Cultural aspects of health psychology. In: Nezu AM, Nezu CM, Geller PA, editors. Handbook of psychology: Volume 9, Health psychology. New Jersey: John Wiley & Sons, Inc; 2003. p. 545–68.
Goward P, Repper J, Appleton L, Hagan T. Crossing boundaries. Identifying and meeting the mental health needs of Gypsies and Travellers. J Ment Health. 2006;15(3):315–27.
Farquharson AB. The effect of hopelessness on students engaged in pattern misbehavior: a replication. In: MSc. Menomonie: The Graduate College University of Wisconsin-Stout; 2002.
Kashani JH, Reid JC, Rosenberg TK. Levels of hopelessness in children and adolescents: A developmental perspective. J Consult Clin Psychol. 1989;57(4):496–9.
Banks KH, Singleton JL, Kohn-Wood L. The Influence of Hope on the Relationship Between Racial Discrimination and Depressive Symptoms. J Multicult Couns D. 2008;36(4):231–44.
van deMortel TF. Faking it: social desirability response bias in self-report research. Aust J Adv Nurs. 2008;25(4):40–8.
Nederhof AJ. Methods of coping with social desirability bias: a review. Eur J Soc Psychol. 1985;15(3):263–80.
Bardwell WA, Dimsdale JE. The impact of ethnicity and response bias on the self-report of negative affect. J Appl Biobehav Res. 2001;6(1):27–38.
Zhang S, Benson T, Deng X. A test-retest reliability assessment of the international self-report delinquency instrument. J Crim Just. 2000;28(4):283–95.
Ware JEJ, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–83.
Geckova AM, van Dijk JP, Zezula I, Tuinstra J, Groothoff JW, Post D. Socio-economic differences in health among Slovak adolescents. Soz Praventivmed. 2004;49(1):26–35.
Matthews S, Manor O, Power C. Social inequalities in health: are there gender differences? Soc Sci Med. 1999;48(1):49–60.
Sadava SW, O'Connor R, McCreary DR. Employment status and health in young adults: Economic and behavioural mediators? J Health Psychol. 2000;5(4):549–60.
Turner RJ, Marino F. Social Support and Social Structure: A Descriptive Epidemiology. J Health Soc Behav. 1994;35(3):193–212.
Bolland JM. Hopelessness and risk behaviour among adolescents living in high-poverty inner-city neighbourhoods. J Adolesc. 2003;26(2):145–58.
Kazdin AE, French NH, Unis AS, Esveldt-Dawson K, Sherick RB. Hopelessness, depression, and suicidal intent among psychiatrically disturbed inpatient children. J Consult Clin Psychol. 1983;51(4):504–10.
Hays RD, Hayashi T, Stewart AL. A five-item measure of socially desirable response set. Educ Psychol Meas. 1989;49(3):629–36.
Clark LA, Watson D. Constructing validity: Basic issues in objective scale development. Psychol Assess. 1995;7(3):309–19.
Parker JDA, Taylor GJ, Bagby RM. The 20-Item Toronto Alexithymia Scale: III. Reliability and factorial validity in a community population. J Psychosom Res. 2003;55(3):269–75.
Soper DS. Sobel Test Calculator for the Significance of Mediation [Software]. http://danielsoper.com/statcalc3/calc.aspx?id=31 (2014). Accessed 16 Sep 2014.
Salonna F, Geckova AM, Zezula I, Sleskova M, Groothoff JW, Reijneveld SA, et al. Does social support mediate or moderate socioeconomic differences in self-rated health among adolescents? Int J Public Health. 2012;57:609–17.
Cederblad M, Dahlin L, Hagnell O, Hansson K. Salutogenic childhood factors reported by middle-aged individuals: Follow-up of the children from the Lundby Study grown up in families experiencing three or more childhood psychiatric risk factors. Eur Arch Psychiatry Clin Neurosci. 1994;244(1):1–11.
Ajrouch KJ, Reisine S, Lim S, Sohn W, Ismail A. Perceived everyday discrimination and psychological distress: does social support matter? Ethn Health. 2010;15(4):417–34.
Crone MR, Bekkema N, Wiefferink CH, Reijneveld SA. Professional identification of psychosocial problems among children from ethnic minority groups: Room for improvement. J Pediatr. 2010;156(2):277–84.
Brittingham A, Tourangeau R, Kay W. Reports of smoking in a National survey: data from screening and detailed interviews, and from self- and interviewer-administered questions. Ann Epidemiol. 1998;8(6):393–401.
Bowling A. Mode of questionnaire administration can have serious effects on data quality. J Public Health. 2005;27(3):281–91.
Brener ND, Billy J, Grady WR. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: evidence from the scientific literature. J Adolesc Health. 2003;33(6):436–57.
Tourangeau R, Yan T. Sensitive questions in surveys. Psychol Bull. 2007;133(5):859–83.
Paradies Y. A systematic review of empirical research on self-reported racism and health. Int J Epidemiol. 2006;35(4):888–901.
Belák A. Health-system limitations of Roma health in Slovakia: A qualitative study. Bratislava: WHO Country Office in Slovakia; 2013.
Belák A. Responding to health literacy needs of the Roma in Slovakia. In: Dodson S, Good S, Osborne RH, editors. Health literacy toolkit for lowand middle-income countries: a series of information sheets to empower communities and strengthen health systems. New Delhi: World Health Organization, Regional Office for South-East Asia; 2015. p. 141–4.
Open Society Institute. Roma Health Mediators: Successes and Challenges. New York: Open Society Foundations; 2011.
Acknowledgements
This work was partially supported by the Research and Development Support Agency under Contract No. APVV-0032-11, by the Agency of the Slovak Ministry of Education for the Structural Funds of the EU (ITMS: 26220120058 (30 %)) and was also partially funded within the framework of the project “Social determinants of health in socially and physically disadvantaged and other groups of population” of The Ministry of Education, Youth and Sports in Czech Republic CZ.1.07/2.3.00/20.0063.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None of the authors declare any competing interests.
Authors' contributions
The authors are justifiably credited with authorship, according to the authorship criteria. PK: data collection, conception of the paper, design, analysis and interpretation of the data, writing the article; AMG: data collection, conception, design, analysis and interpretation of the data, critical revision of the article, statistical expertise, obtaining funding; SAR: conception, design, analysis and interpretation of the data, writing and critical revision of the article, supervision; JPvD: conception, design, analysis and interpretation of the data, critical revision of the article, supervision. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kolarcik, P., Geckova, A.M., Reijneveld, S.A. et al. The mediating effect of discrimination, social support and hopelessness on self-rated health of Roma adolescents in Slovakia. Int J Equity Health 14, 137 (2015). https://doi.org/10.1186/s12939-015-0270-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-015-0270-z