
Abstract
Background
Unilateral breast cancer (UBC) patients with germline pathogenic BRCA1/2 variants have a higher risk of developing contralateral breast cancer (CBC) and need contralateral risk-reducing local treatments, including contralateral risk-reducing mastectomy (CRRM) and prophylactic irradiation (CPI). The aim of our study was to systematically explore the efficacy of CRRM and CPI in reducing CBC risk and increasing survival.
Methods
A search was done, and eligible randomized trials and cohort studies should include and compare UBC patients with germline pathogenic BRCA1/2 variants who have and have not received contralateral risk-reducing local treatment. Random-effects meta-analysis was used in this study. Primary outcomes of the studies included overall survival (OS) and the incidence of contralateral breast cancer (CBC), and secondary outcomes included breast cancer-specific survival (BCSS).
Results
A total of five studies with 1769 UBC patients with germline pathogenic BRCA1/2 variants were enrolled in our meta-analysis. CRRM was correlated with a lower risk of CBC in UBC patients with germline pathogenic BRCA1/2 variants (summary RR = 0.07; 95%CI 0.03–0.13, I2 = 3%), a significantly increased OS (summary RR, 1.15; 95%CI 1.04–1.26, I2 = 26%) and a significantly increased BCSS (summary RR, 1.18; 95%CI 1.07–1.31, I2 = 64%) compared with surveillance. CPI also decreased the risk of CBC (RR 0.02; 95%CI 0.05–0.88) but did not significantly improve OS (RR 0.97; 95%CI 0.90–1.05) and BCSS (RR 0.97; 95%CI 0.90–1.05) compared with surveillance.
Conclusions
CRRM reduces CBC risk and increases OS and BCSS in UBC patients with germline pathogenic BRCA1/2 variants, and could be offered as a risk-reducing local treatment. For those who oppose CRRM, CPI could be offered for CBC-risk reduction, while its survival benefit is still uncertain.
Similar content being viewed by others

Background
Breast cancer has become the most commonly diagnosed cancer since 2020 [1], 0.85–3.0% of whom carry a germline pathogenic BRCA1/2 variation [2,3,4,5]. Unilateral breast cancer (UBC) patients harboring BRCA1/2 mutations have higher risks of developing contralateral breast cancer (CBC) after the diagnosis of the first breast cancer (1st BC) than those who do not. The 10-year CBC risk after the diagnosis of the 1st BC was reported as 18–25%, 32–42%, and 15.5–23.8% in non-Jewish Caucasian, Jewish, and Asian women, respectively, as compared to only 3–7% in non-carriers [6,7,8]. Contralateral risk-reducing mastectomy (CRRM) was offered to UBC patients with BRCA1/2 mutations historically to reduce CBC risk. In the pathological review of CRRM surgical specimens of BRCA1/2 mutation carriers, the risk of CBC lifted even higher because about 11% of occult cancer was observed despite the negative pre-surgical imaging findings [9]. A gradually increasing number of UBC patients carrying BRCA1/2 mutations are adopting CRRM, especially in those under the age of 45 considering these patients have more a more aggressive tumor biology and higher expectations for a longer survival [10,11,12]. However, the efficacy of CRRM needed evaluation.
Previous meta-analysis studies agreed that CRRM reduced the risk of CBC in UBC patients with high familial/genetic risk (RR 0.04; 95%CI 0.02–0.09; P < 0.001) [13], especially those harboring a BRCA1/2 mutation (reduced by 91–93%; RR 0.07; 95%CI 0.04–0.15; P = 0.34) [14, 15]. However, there has been conflicting evidence on whether CRRM improves overall survival (OS) and breast cancer-specific survival (BCSS) in UBC patients harboring BRCA1/2 mutations [10, 16,17,18,19,20]. Meta-analyses focusing on the survival benefit of CRRM revealed no significant difference in BCSS (HR 0.78; 95% CI 0.44–1.39; P = 0.40) by Valachis et al., and a significantly decreased all-cause mortality rate (HR 0.51; 95% CI 0.368–0.714) by Li et al. [14, 15]. Based on the current evidence of reduction in CBC risk and all-cause mortality, recent guidelines from National Comprehensive Cancer Network (NCCN) recommended that CRRM should be offered as a choice to patients with a BRCA1/2 mutation and diagnosed with UBC according to formal consensus [21].
Under the overall trend towards less invasive oncologic care, the de-escalation of CRRM and non-invasive substitute of CRRM have been explored. Nevertheless, risk-reducing local treatment is still needed because systemic treatments such as risk-reducing bilateral salpingo-oophorectomy (BSO), although effective (HR, 0.44; 95% CI 0.21–0.91; P = 0.03), may not be considered by women who have not yet given birth, and adjuvant chemotherapy (HR 1.03; 95%CI 0.68–1.55; P = 0.90), or tamoxifen (HR, 0.59; 95% CI 0.35–1.01; P = 0.05), cannot significantly reduce metachronous CBC risk [7, 22]. Contralateral prophylactic irradiation (CPI) has recently been proposed as a potential alternative to CRRM with advantages such as being non-disfiguring and less invasive [23]. Recently, Evron et al. reported the beneficial results of a phase-II clinical trial of CPI in early-stage UBC patients with BRCA1/2 mutations [24].
Here, we performed a systemic review and meta-analysis of the contralateral risk-reducing local treatments, including CRRM and CPI, in female UBC patients harboring BRCA1/2 mutations. We aimed to update the summarized efficacy of CRRM on CBC risk reduction and survival improvement, while compare the efficacy of CPI with CRRM, in order to provide further preventive oncological care suggestions for BRCA1/2 carriers.
Methods
Protocol and registration
This systemic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [25]. The protocol for this systematic review was registered on PROSPERO (CRD42020199036) and is available in full from: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=199036. since Aug 5, 2020 [26].
Eligibility criteria
Eligible studies were those that included and compared UBC patients harboring BRCA1/2 mutation who had received and had not received contralateral risk-reducing local treatment. Primary surgery of UBC include breast-conserving surgery and mastectomy. Contralateral risk-reducing local treatment is defined as modified radical or radical mastectomy or irradiation on the contralateral breast. The outcomes of the studies include CBC and OS, and secondary outcome include BCSS. Follow-up time was not an exclusion criteria and comprehensive search including randomized controlled trials and observational studies was performed. Exclusion criteria include: (1) patients for whom contralateral breast cancer incidence in terms of hazard ratio or risk ratio is not available will be excluded; (2) patients with BRCA1/2 mutation having any other type of cancer (except breast cancer); (3) reviews and clinical studies with designs other than retrospective observational, prospective observational cohort studies, and interventional studies were excluded from the analysis. Conference abstracts were included in the qualitative systemic review but not the quantitative synthesis because they were not peer-reviewed and may include unreported bias.
Information source and search strategy
A search was done on Aug 14, 2020 in the following databases: MEDLINE via PubMed, Web of Science, EMBASE, Scopus, Cochrane Central Register of Controlled Trials, Cochrane Database of Systemic Reviews, and ClinicalTrials.gov. Search terms included the keywords: breast neoplasms, BRCA, contralateral AND mastectomy, contralateral AND radiotherapy, survival, contralateral breast cancer and their synonyms and Medical Subject Headings (MeSHs). The complete searching strategy is shown in Additional file 1: Methods S1, S2. We also hand-searched references cited by the included research articles and found five studies that met the inclusion criteria.
Study selection, data items and collection process
Titles and keywords were assessed after deduplication, and abstracts and full-texts were obtained and evaluated to determine whether the study met the eligibility criteria. Eligibility assessment and data extraction were completed independently by two researchers and disagreements were resolved through discussion with a third researcher. Effect measures were extracted as component values (i.e., incidence in both groups) for the local treatment and control groups. When such data was not accessable, researchers were contacted for additional unreported data. For each outcome, study-specific risk ratios (RRs), or hazard ratios (HRs), and 95% confidence intervals (CIs) were collected for CBC risk and survival for patients receiving CRRM or CPI versus surveillance. When necessary, HRs were calculated using data extracted from graphical format (e.g. Kaplan–Meier curve).
Quality assessment
Cochrane risk-of-bias tool for randomized trials should be used for included randomized trials. And ROBINS-I [27], a tool to assess the risks of bias of non-randomized studies recommended by Cochrane Handbook for Systemic Reviews of Intervenions, was used if cohort studies were included [28]. This tool required the review authors to describe a ‘target trial’, which is a hypothetical pragmatic randomized trial of the interventions compared in the study, conducted on the same participant group without features putting it at risk of bias and need not to be feasible or ethical. Signaling questions were structured according to a fixed set of domains of bias, including confounding, selection bias, information bias, reporting bias, etc. Based on answers to the signaling questions, judgements for each bias domain, and for overall risk of bias, can be ‘Low’, ‘Moderate’, ‘Serious’ or ‘Critical’ risk of bias. No conflict of interests that might influence author judgements were involved. A study can be assessed at low, moderate, serious, and critical risk of bias.
Summary measures and synthesis of results
We performed an updated meta-analysis of CRRM in UBC patients carrying BRCA1/2 mutations. Basic demographic and clinical characteristics were summarized and compared between CRRM and CPI studies. Pooled rates along with 95% CIs for CBC risk, OS, and BCSS were calculated as dichotomous data. RR was selected as the primary meta-analytic measure of association due to the lack of time-to-event data in certain individual studies. Because HR and 95% CIs for BCSS were not reported in a study [17], estimates were obtained from the Kaplan-Meier curve with data extracted by Engauge-Digitizer software [29].
Statistical heterogeneity was tested across trials by the Cochran’s Q test. A two-sided α value of less than 0.1 was taken to indicate between-trial heterogeneity, with is represented by I2 values (25%-low, 50%-moderate, 75%-high level of heterogeneity) [30]. Random-effects meta-analysis (the DerSimonian and Laird method) of RR was used. Two-sided P< 0.05 was considered statistically significant for the synthesis of the primary and secondary outcomes. All statistical analyses were conducted using Stata version MP 16.0 (StataCorp, TX) and forrest plots and included data were generated using Review Manager 5.4 (The Nordic Cochrane Centre) [31].
Results
Study selection
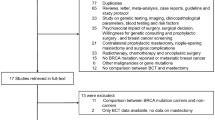
The initial literature search yielded 6529 records (Fig. 1). A non-randomized clinical trial, which studied the efficacy of CRRM in Japanese UBC patients carrying BRCA1/2 mutations, was still recruiting and thus excluded from this study [32]. Of the 14 studies with full texts after selection and deduplication, six were excluded according to the eligibility criteria described in the meta-analysis protocol: inappropriate study design, intervention, population, or outcomes [33]. Two of the studies were conducted on the same population [7, 18], and the most recently published one was included [18]. Two studies were not designed to study CRRM efficacy in BRCA carriers, but included patients who underwent CRRM and were harboring BRCA1/2[16, 34]. In total, seven articles [10, 11, 17,18,−19, 35, 36] were included in the qualitative analysis and the results of five studies [10, 11, 17,18,−19, 36] were pooled in a meta-analysis.

PRISMA flowchart of literature search for contralateral local therapy in unilateral breast cancer patients with germline pathogenic BRCA1/2 mutations. CBC contralateral breast cancer, CRRM contralateral risk-reducing mastectomy
Study characteristics
The characteristics of included studies for quality assessment are presented in Table 1. Four of the studies were observational retrospective cohort studies and the other three were prospective cohort studies. A total of 3087 UBC patients carrying BRCA1/2 mutations were included in this systemic review, with 1706 included in the meta-analysis. Characteristics of patients of the individual studies included in the qualitative systemic review are shown in Table 2. Six of the studies [10, 11, 17,18,−19, 35] focused on the efficacy of CRRM and the remaining study [36] focused on CPI. Sample sizes of the included studies ranged from 88 to 1018 participants. Follow-up years of individual studies ranged from 3.5 to 14.3 years. Six of the seven studies were multicenter studies [10, 11, 16,17,18,−19, 36]. One study has been reported as a conference abstract because not all observational endpoints have been achieved and thus, was excluded from quantitative analysis [35]. Among the included studies, five studies reported CBC as primary of secondary outcome measure. OS is reported as a hazard ratio in four studies [10, 17,18,−19] and as a risk ratio in three studies [11, 35, 36] .
Risk of bias within studies and confounding factors
Due to ethical and operational reasons, none of the eligible studies were randomized [10, 11, 17,18,−19, 35, 36]. Risk of bias within studies was assessed by the ROBINS-I tool [27] (Table 1). Confounding factors should be carefully discussed and considered in the analysis. It was reported that the 5-year cumulative risk of CBC is 13% in UBC patients harboring BRCA1 mutation and 8% in those with BRCA2 mutation. And the cumulative risk of CBC at 10-years is 40 and 26%, respectively [37]. Thus, the mutated gene should be considered as a confounding factor, and subgroup analysis should as well be performed. Younger age at 1st BC diagnosis, higher Body Mass Index (BMI), lobular histology, greater histological grade and size of the tumor, ER/PR-negative status, and higher breast density are all variables that raise CBC risk to a lesser extent. Furthermore, these variables were also less favorable to a longer OS and BCSS. A combination of these characteristics might be associated with an even further increase in risk [33, 38, 39]. Individual inclination was also observed in relationship with younger age at diagnosis, lobular histology, ER/PR-positive pathological status, and Caucasian race, which might act as confounding factors as well [40]. However, the meta-analysis-included studies did not provide according subgroup analysis in how CRRM or CPI reduces the risk of CBC and prolongs OS or BCSS in these subgroups. Three of the studies are prospective cohort studies that had moderate risk of bias and can be considered as a sound non-randomized study. The other four studies were retrospective cohort studies in which two were of moderate risk of bias, one was of serious risk of bias, and one was of no information of bias.
Contralateral breast cancer risk
For CRRM, four non-overlapping studies of low to moderate risk of bias investigated the CBC risk in UBC patients carrying BRCA1/2 mutations who were treated with CRRM relative to those who did not receive CRRM [10, 17,18,−19]. In total, 1607 UBC patients carrying BRCA1/2 mutations were included in the meta-analysis. Results showed that CRRM was correlated with a lower risk of CBC in UBC patients carrying BRCA1/2 mutations (summary RR, 0.07; 95%CI 0.03–0.13; Fig. 2A). As reported by Heemskerk-Gerritsen et al., most metachronous CBCs in BRCA1/2 carriers had a favorable tumour stage, with 87% having a Tis/T1 classification, and 79% having a node-negative disease. Nevertheless, the HR/HER2 status of CBC is similar to the 1st BC, with 73% being triple-negative. The risk of CBC is slightly different between BRCA1 and BRCA2, being 13 and 8%, respectively (P = 0.122). For CPI, Evron et al. reported two cases (2.5%) of CBC among 81 patients who received CPI and 10 cases (12.4%) of CBC among 81 patients who did not receive CPI and underwent surveillance (RR 0.20; 95%CI 0.05–0.88; Fig. 2A) [36]. No study has looked at the risk decrease related with CPM in BRCA1 and BRCA2 mutation carriers individually.

Contralateral breast cancer: relative risk. A CRRM, CPI, and Contralateral breast cancer risk in unilateral breast cancer patients carrying BRCA1/2 mutation. B CRRM, CPI, and overall survival in unilateral breast cancer patients carrying BRCA1/2 mutation. C CRRM, CPI, and breast cancer-specific survival in unilateral breast cancer patients carrying BRCA1/2 mutation. The width of the horizontal line represents the 95% CI of the individual study, and the square proportional represents the weight of each study. The weight was calculated by the sample size of each individual study, and was presented by the percentage of total. The diamond represents the pooled RR and 95% CI. CBC contralateral breast cancer, CRRM contralateral risk-reducing mastectomy, CPI contralateral prophylactic irradiation
Overall survival
For CRRM, four non-overlapping studies of low to moderate risk of bias investigated OS in UBC patients carrying BRCA1/2 mutations who were treated with CRRM relative to those who did not receive CRRM [10, 17,18,−19]. In total, 724 UBC patients carrying BRCA1/2 mutations were included in the meta-analysis. Results show that CRRM was associated with a significantly increased OS in UBC patients carrying BRCA1/2 mutations (summary RR, 1.15; 95%CI 1.04–1.26; Fig. 2B). Four of the aforementioned studies analyzed OS as time-to-event data and also reported HR as an effect measure. When assessed according to HR, CRRM was also associated with a significantly increased OS in UBC patients carrying BRCA1/2 mutations (summary HR, 0.53; 95%CI 0.38–0.74; Additional file 1: Figure S1). To circumvent confounding factors, Evans et al. reported a significanly improved OS (HR 0.37, 95%CI 0.17–0.8) in 105 unilateral breast cancer patients with germline BRCA1/2 mutations who underwent CRRM were compared to 105 specifically matched controls, the OS improvement is still significant after adjusted for risk-reduction bilateral salpingo-oophorectomy (HR 0.43, 95%CI 0.2–0.95).
For CPI, Evron et al. reported 6 cases (7.4%) of death among 81 patients who received CPI and 4 cases (4.9%) of CBC among 81 patients who did not receive CPI and underwent surveillance (RR 0.97; 95%CI 0.90–1.05; Fig. 2B) [36].
Breast cancer-specific survival
For CRRM, three non-overlapping studies investigated BCSS in UBC patients carrying BRCA1/2 mutations who were treated with CRRM relative to those who did not receive CRRM [10, 17, 18]. In total, 383 UBC patients carrying BRCA1/2 mutations were included in the meta-analysis. CRRM was associated with a significantly increased BCSS in UBC patients carrying BRCA1/2 mutations (summary RR, 1.18; 95%CI 1.07–1.31; Fig. 2 C). Metcalfe et al. explored extensively on BCSS according to the length of follow-up. They reported a hazard ratio for the women treated with CRRM compared with control group of 0.52 (0.29 to 0.93; P = 0.03) for 20-year of follow-up and 0.20 (0.05 to 0.89; P = 0.03) for the second decade of follow-up, adjusted for BRCA mutation, tumour size, nodal status, age at diagnosis, year of diagnosis, chemotherapy, radiotherapy, and oophorectomy.
For CPI, all of the above-mentioned deaths were caused by breast cancer. Thus, for BCSS, RR is also reported as 0.97 (95%CI 0.90–1.05; Fig. 2C) [36].
Toxicity and side-effects
CRRM has twice the complication rate when compared to unilateral mastectomy, and is also associated with longer surgery time, higher cost, and longer hospital stays, regardless of whether or not reconstruction is done [41,42,43,44,45]. The risk of complication is approximately the same in the index or the contralateral breast. Such complications are classified into surgical, oncologic, and aesthetic/reconstruction according to the etiology. Surgical complications including bleeding, infection, skin/tissue flap necrosis/loss, anesthesia complications, and thrombosis often have an early onset. Taking mastectomy and reconstructive complications into account, the incidence of complication is about 40–64%, and about 52% of patients undergo at least one unanticipated surgery [46]. The risk of surgical complication cannot be emphasized enough in patients who smoke or with potential comorbidities, such as obesity, diabetes, or cardiac/pulmonary comorbidities. Oncologic side-effects refer to the likelihood of worse prognosis, as patients who receive CRRM may delay adjuvant therapy or refuse further radiotherapy [47]. From the aesthetic/reconstruction aspect, 20–30% of patients who received CRRM reported worse outcomes regarding appearance, pain, and sexuality than expected [48, 49]. Although symmetry is one of the critical motivations of CRRM, especially in patients with large or ptotic breast, they should be advised for other available symmetry procedures, especially when breast conservation is advocated for all eligible patients with or without neoadjuvant systemic treatments.
For patients who opted for CPI, the major concern was radiation-induced malignancy [50, 51]. In Evron et al.’s study, one case of pleomorphic sarcoma was reported and grade I–II acute irradiation toxicity was observed in most patients [36] (Fig. 3).

Summarizing figure of the meta-analysis comparing CRRM and CPI in BRCA1/2 carriers. CBC, contralateral breast cancer; OS, overall survival; BCSS, breast-cancer specific survival; RR, risk ratio; gBRCA1/2m, germline BRCA1/2 mutation
Discussion
To the best of our knowledge, this is the first study that systemically reviews and compares contralateral risk-reducing local treatments, including CRRM and CPI, in BRCA1/2 mutated UBC patients. We meta-analyzed the data for CRRM in CBC risk and mortality rates in UBC patients harboring BRCA1/2 mutation, and compared it to the efficacy data of CPI (Fig. 3). Adverse events were also summarized and reported for these studies.
The results of the meta-analysis for CRRM suggested a 93% (95% CI 96–87%) reduction in CBC risk in UBC patients harboring BRCA1/2 mutations who received CRRM. However, CRRM did not eliminate the risk of developing a secondary breast cancer in the residual contralateral breast. Additionally, our meta-analysis suggested an 18% increase in OS rate and an 18% increase in BCSS rate of UBC patients harboring BRCA1/2 mutations who received CRRM. Although CRRM did not improve OS in UBC patients at average genetic risk [13], our study accorded with previous meta-analysis that CRRM can improve OS in UBC patients at elevated familial risk [13].
Based on the individual studies, guidelines from NCCN and European countries stated that CRRM should be offered as an option to UBC patients carrying BRCA1/2 mutations [21, 52,53,54]. No directly-relevant guidelines were published in Asian countries, likely due to the fact that no relevant data of Asian patients have been published. A non-randomized Japanese clinical trial is now under recruitment and may reveal the efficacy of CRRM in Asian population in the future [32]. However, the decision for CRRM is a personal decision affected by patients’ weigh on symmetry, anxiety during surveillance, and acceptance of removing a normal breast. Although post-surgical satisfaction is reported by most patients who received CRRM, 57.7% of BRCA1/2 carriers forego the choice of CRRM before or after the surgery for primary breast cancer [55]. These BRCA1/2 carriers, who refused CRRM, made this decision because their reluctance to remove a normal breast [56], but the risk of CBC is still worrying nonetheless.
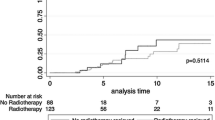
CPI is a novel risk-reducing local intervention on the contralateral breast. Clinicians need to consider both the therapeutic effect of radiation to kill malignant and premalignant cells and the adverse effect of radiation to cause cancer [57]. Based on the fact that the genetic background is the same in both breasts, the risk reduction observed in the ipsilateral residual breast after adjuvant radiation results from radiation therapy [23]. This hypothesis was validated by an experimental breast cancer mouse model [58]. A phase II non-randomized clinical trial [36]and a study focusing on MRI images of breast cancer patients [59] were later published on the application of CPI in breast cancer patients. CPI is proposed as an alternative to UBC patients harboring BRCA1/2 mutations who underwent standard loco-regional treatment for the primary breast cancer and declined CRRM. However, it is critical to understand the risk reduction efficacy of CRRM and CPI before further application. Compared to the summary efficacy of CRRM (summary RR, 0.07; 95%CI), CPI has a lower efficacy in CBC risk reduction (RR 0.20; 95%CI 0.05–0.13). In terms of OS and BCSS, the efficacy of CPI is less than CRRM, because CRRM significantly improved survival of UBC patients harboring BRCA1/2 mutations while CPI did not. This conclusion might result from the relatively short follow-up period in the study of CPI. Heemskerk-Gerritson et al. reported that survival curves diverge between CRRM group and surveillance group after 10–11 years of follow-up [19], which is longer than the follow-up period of the CPI study (58 months). The reported average time from the diagnosis of the primary breast cancer to secondary primary breast cancer is 5.7 years [6]. However, a significant reduction in CBC risk is observed in the CPI study. We optimistically expect to see a more significant difference in CBC risk and a significant improvement in survival rate between patients who underwent CPI and surveillance in an updated report, as the reported trend in CRRM studies.
The study of CPI gathered patients who declined CRRM. The decision of using CRRM is influenced by many factors including age, family history, loco-regional surgery for 1st BC, etc [11]. Many of these factors are potential confounding factors in the survival analysis. Thus, comparison is made between the baseline demographic and clinical characteristics of the patients across the included studies. It is observed that patients who declined CRRM and opted for CPI are significantly older. This could also account for the insignificant result on OS and BCSS in the CPI study.
Nevertheless, our meta-analysis had several limitations. First, the study design of the included studies were not entirely accordant. Because of the invasive and irreversible nature of CRRM, it is infeasible to design a randomized controlled clinical trial. It is also not possible to randomize CPI either because of limited clinical study and untestified efficacy. To conduct a high-quality meta-analysis, studies that are well-designed and well-performed are needed. Therefore, we provide a proposed design for a non-randomized trial that is comparable to a well-performed randomized clinical trial on this topic (Additional file 1: Figure S1). This design considered the following domain as possible confounders: age at 1st BC diagnosis, year of 1st BC diagnosis, surgery for 1st BC, T stage, nodal involvement, grade, family history, involved gene: BRCA1/BRCA2. We also considered co-intervention as an important potential bias including: BSO, chemotherapy and endocrine therapy per standard guidelines, radiotherapy on the ipsilateral side. Also, our study could not perform subgroup analysis regarding BRCA1/2 genes, age/ menopause status, ER/PR/HER2 status, or BMI, because the included studies did not report some of the clinical characteristics of their cohort, nor performed subgroup analyses. Our study referenced a limited number of studies; the referenced studies require long terms of follow-up and more studies are needed to be planned and conducted.
Breast cancer incidence is predicted to grow in the coming future, as global awareness of breast cancer screening is increasing and women lifestyle is shifting towards higher breast cancer risk [60, 61]. At the same time, the treatment regimen of breast cancer has significantly improved in the past few decades, resulting in lower mortality rates and a trend toward less invasive oncological care [62]. To facilitate such trend, a predictive risk score regarding the risk of CBC in hereditarily/genetically high risk patients is needed in the future to guide precision medicine tailored for individual patients.
Conclusions
In conclusion, CPM and CPI are both available to be offered as an option to reduce CBC risk for UBC patients harboring BRCA1/2 mutations. While, CPM is the only effective treatment with enough retrospective evidence to improve survival in this cohort until now. Under the trend toward less invasive oncological care, this systemic review and meta-analysis could provide helpful evidence-based guidance for clinicians when offering prophylactic treatment options to patients with BRCA1/2 mutations. However, longer follow-up, larger sample size, and delicate pre-study protocols are still needed for both interventions, especially for CPI.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its additional information files.
Abbreviations
- UBC:
-
Unilateral breast cancer
- CBC:
-
Contralateral breast cancer
- CPM:
-
Contralateral prophylactic mastectomy
- CPI:
-
Contralateral prophylactic irradiation
- OS:
-
Overall survival
- CBC:
-
Contralateral breast cancer
- BCSS:
-
Breast cancer-specific survival
- 1st BC:
-
First breast cancer
- NCCN:
-
National Comprehensive Cancer Network
- BSO:
-
Bilateral salpingo-oophorectomy
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- MeSHs:
-
Medical Subject Headings
- RR:
-
Risk ratio
- HR:
-
Hazard ratios
- CI:
-
Confidence interval
References
International Agency for Research on Cancer. Latest global cancer data: cancer burden rises to 19.3 million new cases and 10.0 million cancer deaths in 2020. International Agency for Research on Cancer. https://www.iarc.who.int/wp-content/uploads/2020/12/pr292_E.pdf. Accessed 11 Jan 2021.
Li G, Guo X, Tang L, et al. Analysis of BRCA1/2 mutation spectrum and prevalence in unselected Chinese breast cancer patients by next-generation sequencing. J Cancer Res Clin Oncol. 2017;143(10):2011–24. doi:https://doi.org/10.1007/s00432-017-2465-8.
Dorling L, Carvalho S, Allen J, et al. Breast cancer risk genes—association analysis in more than 113,000 women. N Engl J Med. 2021. https://doi.org/10.1056/nejmoa1913948.
Hu C, Hart SN, Gnanaolivu R, et al. A population-based study of genes previously implicated in breast cancer. N Engl J Med. 2021. https://doi.org/10.1056/nejmoa2005936.
Armstrong N, Ryder S, Forbes C, Ross J, Quek RG. A systematic review of the international prevalence of BRCA mutation in breast cancer. Clin Epidemiol. 2019;11:543–61. https://doi.org/10.2147/CLEP.S206949.
Metcalfe K, Gershman S, Lynch HT, et al. Predictors of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. Br J Cancer. 2011;104(9):1384–92. https://doi.org/10.1038/bjc.2011.120.
Metcalfe K, Lynch HT, Chadirian P, et al. Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2004;15(12):2328–35. https://doi.org/10.1200/jco.2004.04.033.
Verhoog LC, Brekelmans CTM, Seynaeve C, Meijers-Heijboer EJ, Klijn JGM. Contralateral breast cancer risk is influenced by the age at onset in BRCA1-associated breast cancer. Br J Cancer. 2000;83(3):384–6. https://doi.org/10.1054/bjoc.2000.1239.
Yamauchi H, Okawa M, Yokoyama S, et al. High rate of occult cancer found in prophylactic mastectomy specimens despite thorough presurgical assessment with MRI and ultrasound: findings from the Hereditary Breast and Ovarian Cancer Registration 2016 in Japan. Breast Cancer Res Treat. 2018;172(3):679–87. https://doi.org/10.1007/s10549-018-4953-1.
Evans DG, Ingham SL, Baildam A, et al. Contralateral mastectomy improves survival in women with BRCA1/2-associated breast cancer. Breast Cancer Res Treat. 2013;140(1):135–42.
Kiely BE, Jenkins MA, McKinley JM, et al. Contralateral risk-reducing mastectomy in BRCA1 and BRCA2 mutation carriers and other high-risk women in the Kathleen Cuningham Foundation Consortium for Research into Familial Breast Cancer (kConFab). Breast Cancer Res Treat. 2010;120(3):715–23. https://doi.org/10.1007/s10549-009-0497-8.
Pesce CE, Liederbach E, Czechura T, Winchester DJ, Yao K. Changing surgical trends in young patients with early stage breast cancer, 2003 to 2010: a report from the national cancer data base. J Am Coll Surg. 2014;219(1):19–28. https://doi.org/10.1016/j.jamcollsurg.2014.03.043.
Fayanju OM, Stoll CRT, Fowler S, Colditz GA, Margenthaler JA. Contralateral prophylactic mastectomy after unilateral breast cancer: a systematic review and meta-analysis. Ann Surg. 2014;260(6):1000–10. https://doi.org/10.1097/SLA.0000000000000769.
Li X, You R, Wang X, et al. Effectiveness of prophylactic surgeries in BRCA1 or BRCA2 mutation carriers: a meta-analysis and systematic review. Clin Cancer Res. 2016;22(15):3971–81. https://doi.org/10.1158/1078-0432.CCR-15-1465.
Valachis A, Nearchou AD, Lind P. Surgical management of breast cancer in BRCA-mutation carriers: a systematic review and meta-analysis. Breast Cancer Res Treat. 2014;144(3):443–55. https://doi.org/10.1007/s10549-014-2890-1.
Brekelmans CTM, Tilanus-Linthorst MMA, Seynaeve C, et al. Tumour characteristics, survival and prognostic factors of hereditary breast cancer from BRCA2-, BRCA1- and non-BRCA1/2 families as compared to sporadic breast cancer cases. Eur J Cancer. 2007;43(5):867–76. doi:https://doi.org/10.1016/j.ejca.2006.12.009.
van Sprundel TC, Schmidt MK, Rookus MA, Brohet R, van Asperen CJ, Rutgers EJ. Risk reduction of contralateral breast cancer and survival after contralateral prophylactic mastectomy in BRCA1 or BRCA2 mutation carriers. Br J Cancer. 2005;93(3):287–92.
Metcalfe K, Gershman S, Ghadirian P, et al. Contralateral mastectomy and survival after breast cancer in carriers of BRCA1 and BRCA2 mutations: retrospective analysis. BMJ. 2014;348:g226.
Heemskerk-Gerritsen BA, Rookus MA, Aalfs CM, et al. Improved overall survival after contralateral risk-reducing mastectomy in BRCA1/2 mutation carriers with a history of unilateral breast cancer: a prospective analysis. Int J Cancer. 2015;136(3):668–77.
Kiely B, Jenkins M, McKinley J, et al. Contralateral risk reducing mastectomy in BRCA1 and BRCA2 mutation carriers and other high risk women in the kathleen cuningham foundation consortium for research into familial breast cancer (KCONFAB). Conference Abstract. Asia Pac J Clin Oncol. 2009;5:715–23.https://doi.org/10.1111/j.1743-7563.2009.01222.x
National Comprehensive Cancer Network. Breast cancer risk reduction (Version 1.2020). National Comprehensive Cancer Network. https://www.nccn.org/professionals/physician_gls/pdf/breast_risk.pdf. Accessed 14 Oct 2020.
Pierce LJ, Levin AM, Rebbeck TR, et al. Ten-year multi-institutional results of breast-conserving surgery and radiotherapy in BRCA1/2-associated stage I/II breast cancer. J Clin Oncol. 2006;24(16):2437–43. https://doi.org/10.1200/jco.2005.02.7888.
Brenner DJ, Shuryak I, Russo S, Sachs RK. Reducing second breast cancers: a potential role for prophylactic mammary irradiation. J Clin Oncol. 2007;25(31):4868–72. https://doi.org/10.1200/jco.2007.11.0379.
Evron E, Ben-David AM, Goldberg H, et al. Prophylactic irradiation to the contralateral breast for BRCA mutation carriers with early-stage breast cancer. Ann Oncol. 2019;1(3):412–7. https://doi.org/10.1093/annonc/mdy515.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;18(4):W65-94. https://doi.org/10.7326/0003-4819-151-4-200908180-00136.
Jia Z, Li J, Liu J, Wang X. The efficacy of prophylactic contralateral mastectomy and contralateral irradiation BRCA carriers diagnosed with unilateral breast cancer. PROSPERO: International prospective register of systematic reviews. 2020. CRD42020199036. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=199036.
Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016. https://doi.org/10.1136/bmj.i4919.
National Institutes of Health. Quality assessment tool for observational cohort and cross-sectional studies. National Institutes of Health. https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort. Accessed 8 Oct 2020.
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007/06/07 2007;8(1):16. doi:https://doi.org/10.1186/1745-6215-8-16.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Review Manager (RevMan) [Computer program]. Version 5.4, The Cochrane Collaboration, 2020.
Study of risk reducing contralateral mastectomy (RRM) for Japanese BRCA1/2 mutation carriers. Japan; 2018. (JPRN-UMIN000031603). The National Institute of Public Health: NIPH Clinical Trials Search. https://rctportal.niph.go.jp/en/detail?trial_id=UMIN000031603. Accessed 10 Sept 2021.
Akdeniz D, Schmidt MK, McCool D, et al. Risk of metachronous contralateral breast cancer: Systematic review and meta-analysis. Conference Abstract. Cancer Res. 2017. https://doi.org/10.1158/1538-7445.SABCS16-P2-07-05.
Murphy B, Hoskin T, Boughey J, Degnim A, Glazebrook K, Hieken T. Contralateral prophylactic mastectomy in women with T4 locally advanced breast cancer. Conference Abstract. Ann Surg Oncol. 2016;23(3):406–8.
Fachinetti A, Chiappa C, Vischi S, et al. Surgical management of breast cancer in BRCA mutation carriers: a single centre experience. Conference Abstract. Ann Oncol. 2019;30:42. https://doi.org/10.1093/annonc/mdz098.009.
Evron E, Ben-David AM, Goldberg H, et al. Prophylactic irradiation to the contralateral breast for BRCA mutation carriers with early-stage breast cancer. Ann Oncol. 2019;30(3):412–7. https://doi.org/10.1093/annonc/mdy515.
Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. Jama. 2017;20(23):2402–16. https://doi.org/10.1001/jama.2017.7112.
Kurian AW, Canchola AJ, Ma CS, Clarke CA, Gomez SL. Magnitude of reduction in risk of second contralateral breast cancer with bilateral mastectomy in patients with breast cancer: Data from California, 1998 through 2015. Cancer. 2020;1(5):958–70. https://doi.org/10.1002/cncr.32618.
Reiner AS, Lynch CF, Sisti JS, et al. Hormone receptor status of a first primary breast cancer predicts contralateral breast cancer risk in the WECARE study population. Breast Cancer Res. 2017;19(1):83. https://doi.org/10.1186/s13058-017-0874-x.
Brown D, Shao S, Jatoi I, Shriver CD, Zhu K. Trends in use of contralateral prophylactic mastectomy by racial/ethnic group andï ER/PR status among patients with breast cancer: a SEER population-based study. Cancer Epidemiol. 2016;42:24–31. https://doi.org/10.1016/j.canep.2016.02.011.
Miller ME, Czechura T, Martz B, et al. Operative risks associated with contralateral prophylactic mastectomy: a single institution experience. Ann Surg Oncol. 2013;20(13):4113–20. https://doi.org/10.1245/s10434-013-3108-1.
Crosby MA, Garvey PB, Selber JC, et al. Reconstructive outcomes in patients undergoing contralateral prophylactic mastectomy. Plast Reconstr Surg. 2011;128(5):1025–33. https://doi.org/10.1097/PRS.0b013e31822b6682.
Silva AK, Lapin B, Yao KA, Song DH, Sisco M. The effect of contralateral prophylactic mastectomy on perioperative complications in women undergoing immediate breast reconstruction: a NSQIP analysis. Ann Surg Oncol. 2015;22(11):3474–80. https://doi.org/10.1245/s10434-015-4628-7.
Osman F, Saleh F, Jackson TD, Corrigan MA, Cil T. Increased postoperative complications in bilateral mastectomy patients compared to unilateral mastectomy: an analysis of the NSQIP database. Ann Surg Oncol. 2013;20(10):3212–7. https://doi.org/10.1245/s10434-013-3116-1.
Elmi M, Carpenter K, Azin A, Azouz V, McCready D, Cil T. Contralateral prophylactic mastectomies lead to increased surgical complications: a coarsened exact matching analysis of the national surgical quality improvement program (NSQIP) database. Conference Abstract. Ann Surg Oncol. 2019;26(2):202. https://doi.org/10.1245/s10434-019-07407-7.
Zion SM, Slezak JM, Sellers TA, et al. Reoperations after prophylactic mastectomy with or without implant reconstruction. Cancer. 2003;15(10):2152–60. https://doi.org/10.1002/cncr.11757.
Sharpe SM, Liederbach E, Czechura T, Pesce C, Winchester DJ, Yao K. Impact of bilateral versus unilateral mastectomy on short term outcomes and adjuvant therapy, 2003–2010: a report from the National Cancer Data Base. Ann Surg Oncol. 2014;21(9):2920–7. https://doi.org/10.1245/s10434-014-3687-5.
Rosenberg SM, Tracy MS, Meyer ME, et al. Perceptions, knowledge, and satisfaction with contralateral prophylactic mastectomy among young women with breast cancer: a cross-sectional survey. Ann Intern Med. 2013;159(6):373–81. https://doi.org/10.7326/0003-4819-159-6-201309170-00003.
Altschuler A, Nekhlyudov L, Rolnick SJ, et al. Positive, negative, and disparate–women’s differing long-term psychosocial experiences of bilateral or contralateral prophylactic mastectomy. Breast J. 2008;14(1):25–32. https://doi.org/10.1111/j.1524-4741.2007.00521.x.
Grantzau T, Overgaard J. Risk of second non-breast cancer after radiotherapy for breast cancer: a systematic review and meta-analysis of 762,468 patients. Radiother Oncol. 2015;114(1):56–65. https://doi.org/10.1016/j.radonc.2014.10.004.
Kirova YM, Vilcoq JR, Asselain B, Sastre-Garau X, Fourquet A. Radiation-induced sarcomas after radiotherapy for breast carcinoma: a large-scale single-institution review. Cancer. 2005;15(4):856–63. https://doi.org/10.1002/cncr.21223.
Tung NM, Boughey JC, Pierce LJ, et al. Management of hereditary breast cancer: American society of clinical oncology, American society for radiation oncology, and society of surgical oncology guideline. J Clin Oncol. 2020;38(18):2080–106. https://doi.org/10.1200/JCO.20.00299.
Paluch-Shimon S, Cardoso F, Sessa C, et al. Prevention and screening in BRCA mutation carriers and other breast/ovarian hereditary cancer syndromes: ESMO Clinical Practice Guidelines for cancer prevention and screening. Ann Oncol. 2016;27:v103–10. doi:https://doi.org/10.1093/annonc/mdw327.
Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer. 20 Oct 2020, Updated 20 Nov 2019.
Elsayegh N, Webster RD, Barrera AMG, et al. Contralateral prophylactic mastectomy rate and predictive factors among patients with breast cancer who underwent multigene panel testing for hereditary cancer. Cancer Med. 2018;7(6):2718–26. https://doi.org/10.1002/cam4.1519.
Huang J, Chagpar A. Factors associated with decision to undergo contralateral prophylactic mastectomy versus unilateral mastectomy. Am J Surg. 2019;218(1):170–4. https://doi.org/10.1016/j.amjsurg.2018.11.040.
Andrieu N, Easton DF, Chang-Claude J, et al. Effect of chest X-rays on the risk of breast cancer among BRCA1/2 mutation carriers in the international BRCA1/2 carrier cohort study: a report from the EMBRACE, GENEPSO, GEO-HEBON, and IBCCS Collaborators’ Group. J Clin Oncol. 2006;20(21):3361–6. https://doi.org/10.1200/jco.2005.03.3126.
Shuryak I, Smilenov LB, Kleiman NJ, Brenner DJ. Potential reduction of contralateral second breast-cancer risks by prophylactic mammary irradiation: Validation in a breast-cancer-prone mouse model. PLoS ONE. 2013. https://doi.org/10.1371/journal.pone.0085795.
Ben-David MA, Corn BW, Evron E, et al. Prophylactic breast irradiation reduces background parenchymal enhancement (BPE) on MRI: a secondary analysis. Breast. 2020;49:70–3. https://doi.org/10.1016/j.breast.2019.10.011.
Omotoso OE, Matariek G, Omotoso EF, et al. Practice of breast self-examination and knowledge of breast and cervical cancer screening. SciMed J. 2021;3(3):219–29. https://doi.org/10.28991/scimedj-2021-0303-3.
Ronco AL, Martínez-López W, Mendoza B, Calderón JM. Epidemiologic evidence for association between a high dietary acid load and the breast cancer risk. SciMed J. 2021;3(2):166–76. https://doi.org/10.28991/scimedj-2021-0302-8.
Wrubel E, Natwick R, Wright GP. Breast-conserving therapy is associated with improved survival compared with mastectomy for early-stage breast cancer: a propensity score matched comparison using the national cancer database. Ann Surg Oncol. 2020. https://doi.org/10.1245/s10434-020-08829-4.
Acknowledgements
We thank all the researchers and authors of the previous studies which were enrolled in this meta-analysis, especially Dr. Evron for providing unpublished data. We thank Prof. Xiaoqing Liu from Peking Union Medical College Hospital for her help in statistical methods. We thank Prof. Dr. Gwendolyn Zahner for her advice on the methodology of meta-analysis. We thank Samson Qian for his assistance on editing the manuscript. We thank the National Natural Science Foundation of China (81802669 to J.L.), CAMS Initiative Fund for Medical Sciences (2016-I2M-1-001 to X.W.), and the CAMS Innovation Fund for Medical Sciences (2020-I2M-C&T-B-068 to J.L.) for the grant support for this study. And this study is preregistered in PROSPERO as CRD42020199036 with an analysis plan.
Material support
We thank all the researchers and authors of the previous studies which were enrolled in this meta-analysis, especially Dr. Evron for providing unpublished data.
Funding
This research was funded in part by the National Natural Science Foundation of China (81802669 to J.L.), CAMS Initiative Fund for Medical Sciences (2016-I2M-1-001 to X.W.), and the CAMS Innovation Fund for Medical Sciences (2020-I2M-C&T-B-068 to J.L.).
Author information
Authors and Affiliations
Contributions
ZJ, JQL, Xiang.W conceptualized the study. ZJ, JXL, YZ, Xin.W, JX extracted and curated the data, conducted the statistical analysis and interpreted the results. ZJ wrote the first draft. XH, GL, MZ, KF, JW, WW, JW critically revised the manuscript. All authors have commented on the different versions of the manuscript and approved the final version. ZJ, JL, and YZ contributed equally to this article. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declared no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Searching strategy, quality assessment tool, and proposed design for a non-randomized trialSearching strategy, quality assessment tool, and proposed design for a non-randomized trial
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jia, Z., Li, J., Zhang, Y. et al. Contralateral risk-reducing local therapy in breast cancer patients with BRCA1/2 mutations: systemic review and meta-analysis. Cancer Cell Int 21, 512 (2021). https://doi.org/10.1186/s12935-021-02194-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12935-021-02194-2