
Abstract
Background
Numerous meta-analyses have explored the association between the triglyceride-glucose (TyG) index and diverse health outcomes, yet the comprehensive assessment of the scope, validity, and quality of this evidence remains incomplete. Our aim was to systematically review and synthesise existing meta-analyses of TyG index and health outcomes and to assess the quality of the evidence.
Methods
A thorough search of PubMed, EMBASE, and Web of Science databases was conducted from their inception through to 8 April 2024. We assessed the quality of reviews using A Measurement Tool to Assess Systematic Reviews (AMSTAR) and the certainty of the evidence using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system. This study was registered with PROSPERO (CRD: 42024518587).
Results
Overall, a total of 95 associations from 29 meta-analyses were included, investigating associations between TyG index and 30 health outcomes. Of these, 83 (87.4%) associations were statistically significant (P < 0.05) according to the random effects model. Based on the AMSTAR tool, 16 (55.2%) meta-analyses were high quality and none was low quality. The certainty of the evidence, assessed by the GRADE framework, showed that 6 (6.3%) associations were supported by moderate-quality evidence. When compared with the lowest category of the TyG index, the risk of contrast-induced nephropathy (CIN) [relative risk (RR) = 2.25, 95%CI 1.82, 2.77], the risk of stroke in patients with diabetes mellitus (RR = 1.26, 95%CI 1.18, 1.33) or with acute coronary syndrome disease (RR = 1.56, 95%CI 1.06, 2.28), the prognosis of coronary artery disease (CAD)-non-fatal MI (RR = 2.02, 95%CI 1.32, 3.10), and the severity of CAD including coronary artery stenosis (RR = 3.49, 95%CI 1.71, 7.12) and multi-vessel CAD (RR = 2.33, 95%CI 1.59, 3.42) increased with high TyG index.
Conclusion
We found that the TyG index was positively associated with many diseases including the risk of CIN and stroke, the prognosis of CAD, and the severity of CAD which were supported by moderate-quality evidence. TyG index might be useful to identify people at high-risk for developing these diseases.
Similar content being viewed by others

Introduction
Insulin resistance (IR) is a pathological state marked by diminished cellular response to insulin, resulting in metabolic dysregulation that contributes to the onset of multiple chronic diseases [1]. Although the hyperinsulinemic-euglycemic clamp test is regarded as the gold standard for evaluating IR, its extensive clinical application is limited due to its high cost, time-consuming nature, and complex procedural requirements [2]. Besides, despite the homeostasis model assessment of IR index being the most readily available marker for assessing IR in clinical settings, it lacks convenience and economic viability for widespread clinical application [3]. However, triglyceride-glucose (TyG) index which obtained as the product of fasting triglycerides and plasma glucose levels serves as an arithmetic expression of IR [4]. This index is considered a more practical and reliable predictor of IR compared to the two aforementioned measurement tools and has been extensively utilized in clinical settings [3, 5]. Moreover, prior research indicates that the TyG index exhibits high sensitivity and specificity in diagnosing IR, offering benefits such as cost-effectiveness, simplicity of measurement, and potential for positive societal impact [6].
Recently, numerous studies have been performed to evaluate the associations between TyG index and a range of health outcomes like arterial stiffnes [7], heart failure [8], cardiovascular disease [9], and cancer [10]. Additionally, the TyG index may provide information for the risk assessment of diseases such as type 2 diabetes mellitus (T2DM) [11], atherosclerosis [12], and critical delirium [13]. With the rapid increase in primary studies on TyG index, the number of systematic reviews and meta-analyses are also accumulating [14,15,16,17]. However, these evidences have covered a wide range of health outcomes, and have inconsistent endpoints, making it challenging for researchers and policymakers. Consequently, it is imperative to objectively and succinctly synthesize these findings to facilitate evidence-based decision-making.
The methods of the umbrella review (UR) are standardized tool to provide a relatively comprehensive understanding of published systematic reviews with meta-analyses on a specific topic recently [18,19,20]. A unique feature of the included studies is that they are systematic reviews and meta-analyses with the aim of describing their quality, summarising and comparing their results, and discussing the strength of these results [20, 21]. Herein, we conducted an UR of systematic reviews with meta-analyses of observational studies to evaluate the associations between TyG index and health outcomes, which thus provide important information to decision makers for facilitating their comprehension.
Methods
Protocol registration
The UR was developed in accordance with the reporting guidance in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline and the Reporting guideline for overviews of reviews of healthcare interventions (PRIOR statement) (Additional file 1: Tables S1–S2) [22, 23]. We have registered the protocol of this UR in PROSPERO (https://www.crd.york.ac.uk/ PROSPERO, CRD: 42024518587).
Literature search
We conducted a comprehensive literature search from inception to July 2023 by screening PubMed, EMBASE, and Web of Science of for systematic reviews with meta-analyses that investigated the association between TyG index and any human health outcome. Furthermore, one additional search was conducted on 8 April 2024 to ensure completeness. Our detailed search strategy was displayed in Additional file 1: Table S3. In addition, manual inspection of the bibliographies of the located systematic reviews and meta-analyses was conducted to uncover supplementary pertinent publications.
Eligibility criteria
Two trained reviewers (JY and J-LY) screened independently the titles and abstracts retrieved from the database and conducted full-text screening to meet the inclusion criteria. Any discrepancy in the literature screening was resolved by a third reviewer (Q-JW). Studies were included according to the PECOS (Population, Exposure, Comparison, Outcome, Study design) strategy:
-
(1)
Population: adults (participants ≥ 18 years of age);
-
(2)
Exposure: TyG index;
-
(3)
Comparison: The lowest category of the TyG index;
-
(4)
Outcomes: any health outcome such as T2DM, cardiovascular disease, and cancer;
-
(5)
Study design: systematic review with meta-analyses of observational studies including cohort, case–control, and cross-sectional studies.
Studies were excluded on the basis of the following criteria:
-
(1)
Narrative reviews or systematic reviews that did not contain a quantitative synthesis;
-
(2)
Letters, comments or conference abstracts;
-
(3)
Systematic review with meta-analyses that included less than two primary studies;
-
(4)
Systematic reviews with meta-analyses not reporting comprehensive data for re-analysis, such as effect sizes [hazard ratio (HR), relative risk (RR), or odds ratio (OR)], 95% confidence intervals (CIs), the number of cases, and total population;
-
(5)
Systematic reviews with meta-analyses of animal studies and/or in vitro studies.
Furthermore, when more than one meta-analysis presented overlapping datasets on the same outcome, we chose the meta-analysis with the largest dataset [24]. If more than one comparison form was analyzed for a given outcome (e.g., dose–response analysis; highest vs. lowest, etc.), all comparison forms were included in our study [25].
Data extraction
Two trained reviewers (JY and J-LY) collected the information from each eligible study independently. All disagreements were resolved by consultation with the senior reviewer (Q-JW). Extracted information from each eligible systematic review with meta-analysis were the first author, year of publication, journal, study design (such as cohort, case–control, and cross-sectional study), number of included studies, number of cases and participants, comparison, health outcomes type, meta-analysis metrics (HR, RR, or OR), and pooled effect. From each study included in the systematic review with meta-analysis, we also extracted the first author, publication year, number of cases and participants, comparison form (dose–response analysis; highest vs. lowest), specific risk estimates, and corresponding 95% CIs.
Data analysis
For each association from eligible meta-analysis, we extracted the data from the original studies and recalculated the adjusted summary effect sizes and corresponding 95% CIs using random effects models [20, 26]. In each meta-analysis, we evaluated heterogeneity by using the I2 statistic, which ranges from 0 to 100% and represents the percentage of the total variation across studies that can be explained by heterogeneity. An I2 value exceeded 50% or 75% indicated significant or considerable heterogeneity, respectively [27].
In addition, to verify the robust of our results, a sensitivity analysis was conducted. If meta-analyses were excluded due to overlap, we did a re-analysis to verify whether their results were consistent with the main analysis [28]. All statistical analyses were conducted in STATA version 16.
Quality assessment of evidence and methods
According to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE), the evidence was graded as high, moderate, low, or very low quality to draw conclusions [29]. Observational studies initiating with low-quality evidence can be subjected to downgrades due to factors like risk of bias, inconsistency among results, indirect evidence, imprecision, and publication bias. We assigned risk of bias when the weight of studies less than 6 points assessed by Newcastle–Ottawa score exceed 50%. Imprecision was determined when the sample size was insufficient, and we judged imprecision when the events size less than 300. Indirectness reflects differences in study populations. We assigned inconsistency when heterogeneity measured by the I2 statistic was greater than 50% for binary outcomes, and a revised cut-off of I2 > 75% for high heterogeneity. The publication bias study was determined to have publication bias when the funnel plot was asymmetrical and the P values for Egger’s test was 0.10 [30]. Conversely, they may be upgraded in quality for reasons including a substantial effect size, the presence of a dose–response relationship, or the existence of plausible confounding that would, in all likelihood, underestimate the true effect [30]. We determined the dose–response relationship if the effect size increased proportionally with TyG index. The large magnitude was determined when the effect size above 2 or 5, and the plausible residual confounding supporting inferences regarding conclusions [30, 31].
Besides, the methodological quality of included studies was assessed by A Measurement Tool to Assess Systematic Reviews (AMSTAR) [32]. As a valid and dependable measurement tool in assessing the quality of systematic reviews and meta-analyses, AMSTAR assesses quality based on 11 aspects including a literature search, literature inclusion, data extraction, statistical analysis, and bias evaluation [33]. Two trained reviewers (JY and J-LY) completed the quality assessment of evidence and methods independently. Discrepancies were resolved through discussion with a senior reviewer (Q-JW).
Results
Literature review
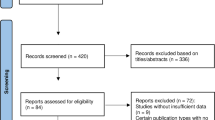
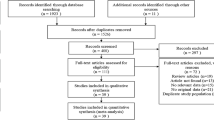
Overall, the search retrieved 1362 records from PubMed, Web of Science, and Embase databases (Fig. 1). After removal of duplicates, 842 records were identified. After screening the titles and abstracts, 805 records were excluded. Eight records were further excluded based on full-text assessment (Additional file 1: Table S4). Ultimately, 29 [14,15,16,17, 34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58] articles were eligible to be included in the present UR (Fig. 1).

Flow diagram of the study selection process
Characteristics of the included meta-analyses
The eligible 29 articles described 95 associations published from 2020 to 2024, which estimated TyG index with four types of health outcomes, including disease risk (n = 59) (Table 1), prognosis (n = 31) (Table 2), severity (n = 3) (Table 3), and mortality (n = 2) (Table 4). We included 30 different health outcomes, such as cardiovascular disease, cancer, and so on (Additional file 1: Table S5). The majority of pooled analyses concerning the correlation between TyG index and coronary artery disease (CAD) (n = 26), followed by stroke (n = 7). We observed that the median number of primary studies was 4 (range 2–22), and the median number of participants was 11,615 (range 437–11,644,261) (Additional file 1: Table S5).
Methodological quality of included meta-analyses
The AMSTAR scores of these articles ranged from 5 to 10, with a median score of 8. Among them, 16 (55.2%) and 13 articles (44.8%) were designated as high and moderate quality, respectively (Fig. 2). AMSTAR, assessment of multiple systematic reviews.

Methodological quality assessment of the included articles with AMSTAR
Summary findings and heterogeneity of the included meta-analyses
Among the 95 associations, the magnitude of the observed summary random-effects estimates ranged from 0.80 to 7.52 (Tables 1, 2, 3, 4). A total of 83 associations (87.4%) showed statistical significance at the P < 0.05 level based on random effects model (Additional file 1: Table S5). Out of the 95 associations, 33 (34.7%) displayed low heterogeneity (I2 < 50%), 18 (19.0%) exhibited high heterogeneity (I2 = 50–75%), and 44 (46.3%) presented very high heterogeneity (I2 > 75%) (Tables 1, 2, 3, 4).
Certainty of evidence
The certainty of the evidence assessed using the GRADE framework revealed that 6 (6.3%) associations were supported by moderate-quality evidence. These associations included the risk of contrast-induced nephropathy (CIN) in non-diabetes mellitus patients with non-ST-segment elevation myocardial infarction (MI) after percutaneous coronary intervention (PCI) (high vs. low, RR = 2.25, 95%CI 1.82, 2.77), the risk of stroke in patients with diabetes mellitus (highest vs. lowest, RR = 1.26, 95%CI 1.18, 1.33), and the risk of stroke in patients with acute coronary syndrome (ACS) disease (highest vs. lowest, RR = 1.56, 95%CI 1.06, 2.28), the prognosis of CAD—non-fatal MI after PCI (highest vs. lowest, RR = 2.02, 95%CI 1.32, 3.10), the severity of CAD—Coronary artery stenosis (high vs. low, RR = 3.49, 95%CI 1.71, 7.12), the severity of CAD—Multi-vessel CAD (high vs. low, RR = 2.33, 95%CI 1.59, 3.42) (Tables 1, 2, 3, 4 and Additional file 1: Table S5). The remaining associations were categorized as low-quality evidence (n = 18, 19.0%) and very low-quality evidence (n = 71, 74.7%). The most common reason for downgrading was inconsistency (68 associations), followed by publication bias (25 associations) and risk of bias (4 associations) (Additional file 1: Table S6).
Sensitivity analyses
Sensitivity analysis was conducted for meta-analyses excluded due to overlap, with 15 associations qualifying for this analysis (Additional file 1: Table S7). The outcomes evaluated in these meta-analyses included eight outcomes [arterial stiffness, CAD, hypertension, gestational diabetes mellitus, major adverse cardiovascular events (MACEs), nonalcoholic fatty liver disease, stroke, and T2DM]. The two meta-analyses that elevated the level of evidence from very low to low pertained to the association between the TyG index and the risk of hypertension in females, as well as the association between the TyG index and the risk of MACE in patients with ACS. Besides, the evidence of a meta-analysis increased from low to moderate with regard to the association between TyG index and risk of stroke. However, the evidence provided by one meta-analyse decreased to very low from low, and 11 meta-analyses remained unchanged (Additional file 1: Table S7).
Discussion
Main findings
This UR first summarized and evaluated the evidence of TyG index with diverse health outcomes. According to the criteria of GRADE, six associations consisting of the risk of CIN in non-diabetic patients with non-ST-elevation MI after PCI (high vs. low), the risk of stroke in patients with diabetes mellitus (highest vs. lowest), the risk of stroke in patients with ACS disease (highest vs. lowest), the prognosis of CAD—non-fatal MI after PCI (highest vs. lowest), the the severity of CAD—Coronary artery stenosis (high vs. low), the severity of CAD—Multi-vessel CAD (high vs. low) were graded as moderate-quality level.
We found that a high TyG index was associated with an increased risk of CIN in non-diabetic patients with non-ST-segment elevation MI after PCI with moderate-quality evidence. However, the diagnostic accuracy of the TyG index for CIN after PCI is moderate and the TyG index should not be used alone for CIN screening [53]. Contrast-induced acute kidney injury (CI-AKI), also known as CIN, is an acute kidney injury caused by the use of iodinated contrast media and has emerged as one of the major complications associated with coronary angiography and interventional cardiology [59]. A high TyG index is significantly and independently associated with the incidence of CIN in patients with non-ST-elevation ACS undergoing initial drug-eluting stent (DES) implantation [60]. Routine preoperative assessment of the TyG index may alleviate CIN and the TyG index is a potential target for intervention to prevent CIN [60]. In addition, a study of patients with suspected CAD undergoing coronary angiography or PCI found that the incidence of CI-AKI increased sharply with increasing TyG [61]. Univariate and multivariate analysis identified TyG as an independent risk factor for CI-AKI [61]. Furthermore, a higher TyG index was found to increase the incidence of CIN in non-diabetic, non-ST-elevation acute MI patients undergoing coronary angiography and is an independent risk factor for the development of CIN [62]. The results of these studies have been consistent with our findings.
Stroke was the outcome for two other associations that were supported by moderate-quality evidence. Subgroup analyses showed that the baseline TyG index was positively associated with the risk of stroke, regardless of whether comorbidity with diabetes or not. There was a linear trend between the TyG index and the risk of stroke in diabetic patients, but there was insufficient data to perform a dose–response analysis in non-diabetic patients [45]. Findings from a cohort study of 5014 seemingly healthy individuals found that high TyG index was associated with an increased risk of cardiovascular disease, including stroke, irrespective of diabetic status [63]. Nested case–control study of 1282 patients with T2DM and stable CAD found positive association between TyG index and future cardiovascular events, including stroke [64]. Liu et al. [65] demonstrated that the TyG index could predict the risk of stroke in non-diabetic populations. Additionally, alterations in the TyG index exhibited a more robust correlation with stroke events in non-diabetic individuals, possibly attributable to the application of glucose-lowering medications mitigating stroke risk [66]. Meanwhile, elevated TyG index related to the increased risk of stroke in ACS patients has been confirmed by many studies [67,68,69]. Of note, the TyG index was positively associated with an increased risk of MACE including stroke in a cohort study of 2531 consecutive diabetic patients [67]. The researchers concluded that the TyG index serves as an independent predictor for the manifestation of MACE in individuals with diabetes and ACS [67]. Besides, Ma et al. demonstrated that, following adjustment for confounding variables, the TyG index was significantly associated with a heightened risk of cardiovascular events in patients with T2DM and ACS who underwent PCI [68]. A retrospective study of 1158 patients with ACS who had previously undergone coronary artery bypass grafting and were undergoing PCI found that those with a higher TyG index had a significantly higher incidence of stroke than those with a lower TyG index [69].
Our research showed that those with the highest TyG index had a significantly higher risk of non-fatal MI after PCI than those with the lowest TyG index, supported by moderate-quality evidence. This result is in line with several previous surveys [70,71,72]. The study by Sun et al. [70] investigating the impact of the TyG index on the prognosis of patients with ischemic heart failure undergoing PCI showed that the incidence of non-fatal MI increased significantly with increasing TyG quartiles. The independent association between TyG index and increased risk of non-fatal MI was confirmed [70]. Besides, a retrospective study showed that in patients with T2DM and non-ST-segment elevation ACS treated with PCI, the incidence of non-fatal MI was significantly increased in patients with a higher TyG index [71]. In addition, a study of ACS patients without diabetes mellitus who underwent emergency PCI with DES found that the TyG index may be an independent predictor of major adverse cardiovascular and cerebrovascular event (MACCE). This study had a median follow-up of 47 months and selected MACCE as the observed endpoint [72]. However, there was no significant difference in the incidence of non-fatal MI in patients with high TyG compared with the low group [72]. This may be due to the insufficient sample size of this study (only 10 for non-fatal MI).
Our UR provided moderate-quality evidence supporting the positive association between TyG index and the severity of coronary artery stenosis in CAD patients, aligning with the findings of several preceding studies [73,74,75]. For example, a retrospective study conducted by Xu et al. [73] showed a significant positive correlation between the TyG index and severe coronary artery stenosis in patients with hypertension and CAD. Additionally, the TyG index has been identified as an independent risk factor for the severity of coronary artery stenosis [73]. Besides, a cross-sectional study demonstrated that the TyG index might serve as a marker for IR [74]. An elevated TyG index may be indicative of patients at heightened risk for coronary artery stenosis and is linked to the extent of arterial stenoses [74]. In addition, a retrospective analysis involving 2,952 patients revealed that the TyG index serves as a predictor for the severity of coronary artery stenosis in individuals with premature cardiovascular artery disease (PCAD), thus establishing its utility as both a diagnostic and risk marker for coronary artery stenosis in PCAD patients [75].
Our results showed that the TyG index in CAD patients is positively correlated with CAD severity-Multi-vessle CAD severity, which is supported by moderate-quality evidence. This finding was consisted with results of several previous studies [76,77,78]. For instance, a retrospective analysis revealed that patients with multivessel CAD exhibited a significantly increased TyG index compared to individuals with single-vessel CAD, suggesting that the TyG index is associated with the severity of CAD and also constitutes an independent risk factor for multivessel CAD [76]. Furthermore, an increased TyG index was associated with an increased risk of multivessel CAD in a study of patients with CAD [77]. What is more, a multicentre retrospective study of patients with CAD showed that an elevated TyG index was associated with an increased risk of multiple coronary atherosclerosis [78].
Our study confirms the association between TyG and a range of health outcomes. The cost-effective measurement of TyG indices has important clinical implications for the early identification of individuals at risk for these diseases and for improving risk stratification and treatment management [79]. Based on the dynamic nature of disease progression and the TyG index, it is suggested that clinical assessment of the TyG index at a single time point has limitations [80]. Primary care physicians additionally need to be aware of this when making judgements using the TyG index.
Strengths and limitations
This study constitutes the first systematic appraisal of the association between the TyG index and diverse health outcomes, integrating findings from meta-analyses of extant observational studies and utilizing the well-recognized GRADE criteria for the assessment of evidence quality. Furthermore, to facilitate enhanced comparability of outcome associations, each correlation was recalibrated utilizing a random-effects model. We assessed the methodological quality of the included meta-analyses using a standard method (AMSTAR), and all the articles were of moderate or higher quality, with 55.2% being of high quality. However, a recent study in the cardiovascular field reported that the majority of systematic reviews were of "Critically low" (53%) or "Low" (18.7%) quality [81], which was contrast starkly with our findings. The reason for this inconsistent is that we use different tools for assessing the methodological quality of the included meta-analyses, and the quality assessments in the our study were relatively lenient (AMSTAR). To further improve the reliability of the results, we performed sensitivity analyses on meta-analyses that were excluded due to overlap and found that the certainty of most evidence remained unchanged. Moreover, our study included a large sample size with a comprehensive range of outcomes, and we presented them separately for different subgroups of the same outcome.
Potential limitations should be considered in our study. Firstly, the UR consisted entirely of meta-analyses of observational studies, which are subject to inherent limitations such as selection and confounding biases in the original articles. This may also be the reason for the low certainty of evidence. However, limited randomized controlled trials have examined the association between the TyG index and health outcomes. For example, one randomized controlled trial examined whether there were sex differences in the relationship between IR (evaluated by TyG index) and MACEs in hypertensive patients without diabetes [82]. The findings indicated an association between the TyG index and MACEs among hypertensive patients, with no observed differences in this association with respect to gender [82]. Nonetheless, a short follow-up time may limit the application of the results of this study. Hence, observational studies become more pertinent to our subject matter due to their advantages, such as larger sample sizes, a sufficient quantity of studies, and extended follow-up durations [83]. Secondly, the UR relied on previously published systematic reviews with meta-analyses. Although it is possible that some individual studies were missed, the use of a comprehensive search strategy and MeSH terms likely mitigated this risk. Thirdly, systematic reviews with only qualitative analyses and meta-analyses without study-specific data were excluded. Consequently, there is a potential for misestimation of these findings. Nevertheless, we summarized findings from these studies to ensure that we considered all relevant research. The majority (77.8%) of qualitative studies showed that increased TyG index raised the risk of atherosclerosis, MACE, and cerebrovascular disease, which was in line with our findings. (Additional file 1: Table S8). Moreover, several meta-analyses in our UR included fewer than 10 original studies. This may reduce the statistical power of Egger’s regression test [84] and make it difficult to assess the risk of publication bias.
Conclusion
Although the TyG index is associated with many health outcomes, the high certainty evidence has been only observed for six associations, in which the TyG index is positively associated with the risk of CIN in non-diabetic patients with non-ST-segment elevation MI after PCI, the risk of stroke in patients with diabetes or ACS patients, the prognosis of CAD (non-fatal MI after PCI) and the severity of CAD (coronary artery stenosis and multivessel CAD). Therefore, there is a critical need for high quality meta-analyses of the association of TyG index with a wider range of health outcomes in the future.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACS:
-
Acute coronary syndrome
- AMSTAR:
-
A Measurement Tool to Assess Systematic Reviews
- CAD:
-
Coronary artery disease
- CI:
-
Confidence intervals
- CI-AKI:
-
Contrast-induced acute kidney injury
- CIN:
-
Contrast-induced nephropathy
- GRADE:
-
Grading of Recommendations, Assessment, Development and Evaluation
- HR:
-
Hazard ratio
- IR:
-
Insulin resistance
- MACE:
-
Major adverse cardiovascular event
- MI:
-
Myocardial infarction
- MOOSE:
-
Meta-analyses of observational studies in epidemiology
- OR:
-
Odds ratio
- PCAD:
-
Premature cardiovascular artery disease
- PCI:
-
Percutaneous coronary intervention
- PECOS:
-
Population, Exposure, Comparison, Outcome, Study design
- PRIOR:
-
Reporting guideline for overviews of reviews of healthcare interventions
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- RR:
-
Relative risk
- TyG:
-
Triglyceride glucose
- T2DM:
-
Type 2 diabetes mellitus
- UR:
-
Umbrella review
References
Adeva-Andany MM, Martínez-Rodríguez J, González-Lucán M, Fernández-Fernández C, Castro-Quintela E. Insulin resistance is a cardiovascular risk factor in humans. Diabetes Metab Syndr. 2019;13(2):1449–55.
Cersosimo E, Solis-Herrera C, Trautmann ME, Malloy J, Triplitt CL. Assessment of pancreatic β-cell function: review of methods and clinical applications. Curr Diabetes Rev. 2014;10(1):2–42.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–9.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304.
Muniyappa R, Lee S, Chen H, Quon MJ. Current approaches for assessing insulin sensitivity and resistance in vivo: advantages, limitations, and appropriate usage. Am J Physiol Endocrinol Metab. 2008;294(1):E15-26.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity: comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010. https://doi.org/10.1210/jc.2010-0288.
Yan Y, Wang D, Sun Y, Ma Q, Wang K, Liao Y, et al. Triglyceride-glucose index trajectory and arterial stiffness: results from Hanzhong Adolescent Hypertension Cohort Study. Cardiovasc Diabetol. 2022;21(1):33.
Xu L, Wu M, Chen S, Yang Y, Wang Y, Wu S, et al. Triglyceride-glucose index associates with incident heart failure: a cohort study. Diabetes Metab. 2022;48(6):101365.
Alizargar J, Bai CH, Hsieh NC, Wu SV. Use of the triglyceride-glucose index (TyG) in cardiovascular disease patients. Cardiovasc Diabetol. 2020;19(1):8.
Fritz J, Bjørge T, Nagel G, Manjer J, Engeland A, Häggström C, et al. The triglyceride-glucose index as a measure of insulin resistance and risk of obesity-related cancers. Int J Epidemiol. 2020;49(1):193–204.
Deng H, Hu P, Li H, Zhou H, Wu X, Yuan M, et al. Novel lipid indicators and the risk of type 2 diabetes mellitus among Chinese hypertensive patients: findings from the Guangzhou Heart Study. Cardiovasc Diabetol. 2022;21(1):212.
Li M, Zhan A, Huang X, Hu L, Zhou W, Wang T, et al. Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients: the China H-type Hypertension Registry Study. Cardiovasc Diabetol. 2020;19(1):139.
Huang X, Cheng H, Yuan S, Ling Y, Tan S, Tang Y, et al. Triglyceride-glucose index as a valuable predictor for aged 65-years and above in critical delirium patients: evidence from a multi-center study. BMC Geriatr. 2023;23(1):701.
Pranata R, Huang I, Irvan LMA, Vania R. The association between triglyceride-glucose index and the incidence of type 2 diabetes mellitus-a systematic review and dose-response meta-analysis of cohort studies. Endocrine. 2021. https://doi.org/10.1007/s12020-021-02780-4.
Liao C, Xu H, Jin T, Xu K, Xu Z, Zhu L, et al. Triglyceride-glucose index and the incidence of stroke: a meta-analysis of cohort studies. Front Neurol. 2022;13:1033385.
Luo JW, Duan WH, Yu YQ, Song L, Shi DZ. Prognostic significance of triglyceride-glucose index for adverse cardiovascular events in patients with coronary artery disease: a systematic review and meta-analysis. Front Cardiovasc Med. 2021;8:774781.
Wang H, Yan F, Cui Y, Chen F, Wang G, Cui W. Association between triglyceride glucose index and risk of cancer: a meta-analysis. Front Endocrinol. 2023;13:1098492.
Brabaharan S, Veettil SK, Kaiser JE, Raja Rao VR, Wattanayingcharoenchai R, Maharajan M, et al. Association of hormonal contraceptive use with adverse health outcomes: an umbrella review of meta-analyses of randomized clinical trials and cohort studies. JAMA Netw Open. 2022;5(1): e2143730.
Okoth K, Chandan JS, Marshall T, Thangaratinam S, Thomas GN, Nirantharakumar K, et al. Association between the reproductive health of young women and cardiovascular disease in later life: umbrella review. BMJ. 2020;371: m3502.
Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. Int J Evid Based Healthc. 2015;13(3):132–40.
Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. 2011;11(1):15.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350: g7647.
Gates M, Gates A, Pieper D, Fernandes RM, Tricco AC, Moher D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378: e070849.
Neuenschwander M, Ballon A, Weber KS, Norat T, Aune D, Schwingshackl L, et al. Role of diet in type 2 diabetes incidence: umbrella review of meta-analyses of prospective observational studies. BMJ. 2019;366: l2368.
Li YZ, Yang ZY, Gong TT, Liu YS, Liu FH, Wen ZY, et al. Cruciferous vegetable consumption and multiple health outcomes: an umbrella review of 41 systematic reviews and meta-analyses of 303 observational studies. Food Funct. 2022;13(8):4247–59.
Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Intern Med. 1997;127(9):820–6.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Dragioti E, Solmi M, Favaro A, Fusar-Poli P, Dazzan P, Thompson T, et al. Association of antidepressant use with adverse health outcomes: a systematic umbrella review. JAMA Psychiat. 2019;76(12):1241–55.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011. https://doi.org/10.1016/j.jclinepi.2010.04.026.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6.
Lee JS, Lee YA, Shin CH, Suh DI, Lee YJ, Yon DK. Long-term health outcomes of early menarche in women: an umbrella review. QJM Mon J Assoc Phys. 2022;115(12):837–47.
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10.
Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E, Grimshaw J, et al. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol. 2009;62(10):1013–20.
Sajdeya O, Beran A, Mhanna M, Alharbi A, Burmeister C, Abuhelwa Z, et al. Triglyceride glucose index for the prediction of subclinical atherosclerosis and arterial stiffness: a meta-analysis of 37,780 individuals. Curr Probl Cardiol. 2022;47(12):101390.
Liu F, Ling Q, Xie S, Xu Y, Liu M, Hu Q, et al. Association between triglyceride glucose index and arterial stiffness and coronary artery calcification: a systematic review and exposure-effect meta-analysis. Cardiovasc Diabetol. 2023;22(1):111.
Ding X, Wang X, Wu J, Zhang M, Cui M. Triglyceride-glucose index and the incidence of atherosclerotic cardiovascular diseases: a meta-analysis of cohort studies. Cardiovasc Diabetol. 2021;20(1):76.
Liu X, Tan Z, Huang Y, Zhao H, Liu M, Yu P, et al. Relationship between the triglyceride-glucose index and risk of cardiovascular diseases and mortality in the general population: a systematic review and meta-analysis. Cardiovasc Diabetol. 2022;21(1):124.
Yan F, Yan S, Wang J, Cui Y, Chen F, Fang F, et al. Association between triglyceride glucose index and risk of cerebrovascular disease: systematic review and meta-analysis. Cardiovasc Diabetol. 2022;21(1):226.
Ren X, Jiang M, Han L, Zheng X. Association between triglyceride-glucose index and chronic kidney disease: a cohort study and meta-analysis. Nutr Metab Cardiovasc Dis. 2023;33(6):1121–8.
Liang S, Wang C, Zhang J, Liu Z, Bai Y, Chen Z, et al. Triglyceride-glucose index and coronary artery disease: a systematic review and meta-analysis of risk, severity, and prognosis. Cardiovasc Diabetol. 2023;22(1):170.
Song T, Su G, Chi Y, Wu T, Xu Y, Chen C. Triglyceride-glucose index predicts the risk of gestational diabetes mellitus: a systematic review and meta-analysis. Gynecol Endocrinol. 2022;38(1):10–5.
Yang Y, Huang X, Wang Y, Leng L, Xu J, Feng L, et al. The impact of triglyceride-glucose index on ischemic stroke: a systematic review and meta-analysis. Cardiovasc Diabetol. 2023;22(1):2.
Ling Q, Chen J, Liu X, Xu Y, Ma J, Yu P, et al. The triglyceride and glucose index and risk of nonalcoholic fatty liver disease: a dose-response meta-analysis. Front Endocrinol. 2022;13:1043169.
Beran A, Ayesh H, Mhanna M, Wahood W, Ghazaleh S, Abuhelwa Z, et al. Triglyceride-glucose index for early prediction of nonalcoholic fatty liver disease: a meta-analysis of 121,975 individuals. J Clin Med. 2022. https://doi.org/10.3390/jcm11092666.
Feng X, Yao Y, Wu L, Cheng C, Tang Q, Xu S. Triglyceride-glucose index and the risk of stroke: a systematic review and dose-response meta-analysis. Horm Metab Res. 2022;54(3):175–86.
da Silva A, Caldas APS, Rocha D, Bressan J. Triglyceride-glucose index predicts independently type 2 diabetes mellitus risk: a systematic review and meta-analysis of cohort studies. Prim Care Diabetes. 2020;14(6):584–93.
Li J, Ren L, Chang C, Luo L. Triglyceride-glukose index predicts adverse events in patients with acute coronary syndrome: a meta-analysis of cohort studies. Horm Metab Res. 2021;53(9):594–601.
Ma X, Han Y, Jiang L, Li M. Triglyceride-glucose index and the prognosis of patients with acute ischemic stroke: a meta-analysis. Horm Metab Res. 2022;54(6):361–70.
Sun C, Hu L, Li X, Zhang X, Chen J, Li D, et al. Triglyceride-glucose index’s link to cardiovascular outcomes post-percutaneous coronary intervention in China: a meta-analysis. ESC Heart Fail. 2024. https://doi.org/10.1002/ehf2.14679.
Xu AR, Jin Q, Shen Z, Zhang J, Fu Q. Association between the risk of hypertension and triglyceride glucose index in Chinese regions: a systematic review and dose-response meta-analysis of a regional update. Front Cardiovasc Med. 2023;10:1242035.
Khalaji A, Behnoush AH, Khanmohammadi S, Ghanbari Mardasi K, Sharifkashani S, Sahebkar A, et al. Triglyceride-glucose index and heart failure: a systematic review and meta-analysis. Cardiovasc Diabetol. 2023;22(1):244.
Azarboo A, Behnoush AH, Vaziri Z, Daneshvar MS, Taghvaei A, Jalali A, et al. Assessing the association between triglyceride-glucose index and atrial fibrillation: a systematic review and meta-analysis. Eur J Med Res. 2024;29(1):118.
Chang WT, Liu CC, Huang YT, Wu JY, Tsai WW, Hung KC, et al. Diagnostic efficacy of the triglyceride-glucose index in the prediction of contrast-induced nephropathy following percutaneous coronary intervention. Front Endocrinol. 2023;14:1282675.
Zhou J, Zhu L, Li Y. Association between the triglyceride glucose index and diabetic retinopathy in type 2 diabetes: a meta-analysis. Front Endocrinol. 2023;14:1302127.
Wang H, Ling Q, Wu Y, Zhang M. Association between the triglyceride glucose index and cognitive impairment and dementia: a meta-analysis. Front Aging Neurosci. 2023;15:1278730.
Behnoush AH, Khalaji A, Ghondaghsaz E, Masrour M, Shokri Varniab Z, Khalaji S, et al. Triglyceride-glucose index and obstructive sleep apnea: a systematic review and meta-analysis. Lipids Health Dis. 2024;23(1):4.
Wang J, Yan S, Cui Y, Chen F, Piao M, Cui W. The diagnostic and prognostic value of the triglyceride-glucose index in metabolic dysfunction-associated fatty liver disease (MAFLD): a systematic review and meta-analysis. Nutrients. 2022. https://doi.org/10.3390/nu14234969.
Nabipoorashrafi SA, Seyedi SA, Rabizadeh S, Ebrahimi M, Ranjbar SA, Reyhan SK, et al. The accuracy of triglyceride-glucose (TyG) index for the screening of metabolic syndrome in adults: a systematic review and meta-analysis. Nutr Metab Cardiovasc Dis. 2022;32(12):2677–88.
Yu R, Wu C, Xiao Y, Li Q, Chen J, Song J, et al. The clinical predictive value and regulation mechanism of microRNA-188-5p in contrast-induced acute kidney injury. Biochem Biophys Res Commun. 2023;679:215–23.
Li M, Li L, Qin Y, Luo E, Wang D, Qiao Y, et al. Elevated TyG index predicts incidence of contrast-induced nephropathy: a retrospective cohort study in NSTE-ACS patients implanted with DESs. Front Endocrinol. 2022;13:817176.
Qin Y, Tang H, Yan G, Wang D, Qiao Y, Luo E, et al. A high triglyceride-glucose index is associated with contrast-induced acute kidney injury in Chinese patients with type 2 diabetes mellitus. Front Endocrinol. 2020;11:522883.
Aktas H, Inci S, Gul M, Gencer S, Yildirim O. Increased triglyceride-glucose index predicts contrast-induced nephropathy in non-diabetic NSTEMI patients: a prospective study. J Investig Med. 2023;71(8):838–44.
Sánchez-Íñigo L, Navarro-González D, Fernández-Montero A, Pastrana-Delgado J, Martínez JA. The TyG index may predict the development of cardiovascular events. Eur J Clin Invest. 2016;46(2):189–97.
Jin JL, Sun D, Cao YX, Guo YL, Wu NQ, Zhu CG, et al. Triglyceride glucose and haemoglobin glycation index for predicting outcomes in diabetes patients with new-onset, stable coronary artery disease: a nested case-control study. Ann Med. 2018;50(7):576–86.
Liu L, Wu Z, Zhuang Y, Zhang Y, Cui H, Lu F, et al. Association of triglyceride-glucose index and traditional risk factors with cardiovascular disease among non-diabetic population: a 10-year prospective cohort study. Cardiovasc Diabetol. 2022;21(1):256.
Wu Y, Yang Y, Zhang J, Liu S, Zhuang W. The change of triglyceride-glucose index may predict incidence of stroke in the general population over 45 years old. Cardiovasc Diabetol. 2023;22(1):132.
Wang L, Cong HL, Zhang JX, Hu YC, Wei A, Zhang YY, et al. Triglyceride-glucose index predicts adverse cardiovascular events in patients with diabetes and acute coronary syndrome. Cardiovasc Diabetol. 2020;19(1):80.
Ma X, Dong L, Shao Q, Cheng Y, Lv S, Sun Y, et al. Triglyceride glucose index for predicting cardiovascular outcomes after percutaneous coronary intervention in patients with type 2 diabetes mellitus and acute coronary syndrome. Cardiovasc Diabetol. 2020;19(1):31.
Dong S, Zhao Z, Huang X, Ma M, Yang Z, Fan C, et al. Triglyceride-glucose index is associated with poor prognosis in acute coronary syndrome patients with prior coronary artery bypass grafting undergoing percutaneous coronary intervention. Cardiovasc Diabetol. 2023;22(1):286.
Sun T, Huang X, Zhang B, Ma M, Chen Z, Zhao Z, et al. Prognostic significance of the triglyceride-glucose index for patients with ischemic heart failure after percutaneous coronary intervention. Front Endocrinol. 2023;14:1100399.
Zhao Q, Zhang TY, Cheng YJ, Ma Y, Xu YK, Yang JQ, et al. Impacts of triglyceride-glucose index on prognosis of patients with type 2 diabetes mellitus and non-ST-segment elevation acute coronary syndrome: results from an observational cohort study in China. Cardiovasc Diabetol. 2020;19(1):108.
Zhang Y, Chu C, Zhong Z, Luo YB, Ning FF, Guo N. High triglyceride-glucose index is associated with poor cardiovascular outcomes in Chinese acute coronary syndrome patients without diabetes mellitus who underwent emergency percutaneous coronary intervention with drug-eluting stents. Front Endocrinol. 2023;14:1101952.
Xu Z, Chen P, Wang L, Yan J, Yan X, Li D. Relationship between TyG index and the degree of coronary artery lesions in patients with H-type hypertension. Cardiovasc Diabetol. 2024;23(1):23.
Thai PV, Tien HA, Van Minh H, Valensi P. Triglyceride glucose index for the detection of asymptomatic coronary artery stenosis in patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19(1):137.
Chen S, Li Z, Li H, Zeng X, Yuan H, Li Y. Novel lipid biomarkers and ratios as risk predictors for premature coronary artery disease: a retrospective analysis of 2952 patients. J Clin Hypertens. 2023;25(12):1172–84.
Zhang Y, Wang R, Fu X, Song H. Non-insulin-based insulin resistance indexes in predicting severity for coronary artery disease. Diabetol Metab Syndr. 2022;14(1):191.
Wang X, Xu W, Song Q, Zhao Z, Meng X, Xia C, et al. Association between the triglyceride-glucose index and severity of coronary artery disease. Cardiovasc Diabetol. 2022;21(1):168.
Su J, Li Z, Huang M, Wang Y, Yang T, Ma M, et al. Triglyceride glucose index for the detection of the severity of coronary artery disease in different glucose metabolic states in patients with coronary heart disease: a RCSCD-TCM study in China. Cardiovasc Diabetol. 2022;21(1):96.
Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68.
Zhou H, Ding X, Lan Y, Chen S, Wu S, Wu D. Multi-trajectories of triglyceride-glucose index and lifestyle with cardiovascular disease: a cohort study. Cardiovasc Diabetol. 2023;22(1):341.
Karakasis P, Bougioukas KI, Pamporis K, Fragakis N, Haidich AB. Appraisal methods and outcomes of AMSTAR 2 assessments in overviews of systematic reviews of interventions in the cardiovascular field: a methodological study. Res Synth Methods. 2024;15(2):213–26.
Yang K, Liu W. Triglyceride and glucose index and sex differences in relation to major adverse cardiovascular events in hypertensive patients without diabetes. Front Endocrinol. 2021;12:761397.
Papadimitriou N, Markozannes G, Kanellopoulou A, Critselis E, Alhardan S, Karafousia V, et al. An umbrella review of the evidence associating diet and cancer risk at 11 anatomical sites. Nat Commun. 2021;12(1):4579.
Bellou V, Belbasis L, Tzoulaki I, Evangelou E, Ioannidis JP. Environmental risk factors and Parkinson’s disease: an umbrella review of meta-analyses. Parkinsonism Relat Disord. 2016;23:1–9.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Key Research and Development Program of China (No. 2022YFC2704205 to Wu QJ), the Natural Science Foundation of China (No. 82073647 and No. 82373674 to Wu QJ and No.82103914 to Gong TT), Outstanding Scientific Fund of Shengjing Hospital (Q-JW), and 345 Talent Project of Shengjing Hospital of China Medical University (Gong TT).
Author information
Authors and Affiliations
Contributions
J-LY, JY, X-JS, XQ, TT, JD, T-TG, and Q-JW contributed to the study design. J-LY, JY, Y-JC, XC, and F-HL collection of data. J-LY, JY, Y-JC, XC, F-HL, Y-ZL, and H-LX analysis of data. J-LY, JY, X-JS, XQ, Y-FW, FC, X-LB, LW, TT, JD, T-TG, and Q-JW wrote the first draft of the manuscript and edited the manuscript. All authors read and approved the final manuscript. J-LY, JY, X-JS, and XQ contributed equally to this work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Table S1. PRISMA checklist of items to include when reporting a systematic review or meta-analysis. Table S2: PRIOR Checklist. Table S3. Search strategy. Table S4. The list of the excluded records during the process of full-text review. Table S5. Description of 95 meta-analyses investigating the associations between Triglyceride-glucose index and health outcomes. Table S6. GRADE classification of quality of evidence. Table S7. Sensitivity analysis results of excluded meta-analyses due to overlap. Table S8. The summary results of meta-analyses excluded due to lack of data for quantitative synthesis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yin, JL., Yang, J., Song, XJ. et al. Triglyceride-glucose index and health outcomes: an umbrella review of systematic reviews with meta-analyses of observational studies. Cardiovasc Diabetol 23, 177 (2024). https://doi.org/10.1186/s12933-024-02241-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02241-y