
Abstract
Background
The triglyceride-glucose index (TyG), an established indicator of insulin resistance, is closely correlated with the prognosis of several metabolic disorders. This study aims to investigate the association between the TyG index and the incidence of critical delirium in patients aged 65 years and older.
Methods
We focused on evaluating patients aged 65 years and older diagnosed with critical delirium. Data were obtained from the Medical Information Database for Intensive Care (MIMIC-IV) and the eICU Collaborative Research Database (eICU-CRD). Multivariate logistic regression and restricted cubic spline (RCS) regression were used to determine the relationship between the TyG index and the risk of delirium.
Results
Participants aged 65 years and older were identified from the MIMIC-IV (n = 4,649) and eICU-CRD (n = 1,844) databases. Based on optimal thresholds derived from RCS regression, participants were divided into two cohorts: Q1 (< 8.912), Q2 (≥ 8.912). The logistic regression analysis showed a direct correlation between the TyG index and an increased risk of critical delirium among ICU patients aged 65 and older. These findings were validated in the eICU-CRD dataset, and sensitivity analysis further strengthened our conclusions. In addition, the subgroup analysis revealed certain differences.
Conclusion
This study highlights a clear, independent relationship between the TyG index and the risk of critical delirium in individuals aged 65 years and older, suggesting the importance of the TyG index as a reliable cardio-cerebrovascular metabolic marker for risk assessment and intervention.
Similar content being viewed by others


Introduction
Delirium, an acute neuropsychiatric syndrome characterized by altered consciousness and cognitive impairment, is a frequently overlooked manifestation of organ dysfunction in older adults with acute medical illness [1,2,3]. It is associated with an increased risk of adverse clinical outcomes in the short or long term and is most common in intensive care unit (ICU) [4, 5]. The underlying pathophysiology of delirium remains complex and speculative, involving various mechanisms contributing to nerve conduction disorders, neuroinflammation, inadequate brain metabolism, and neurotransmitter imbalances [6, 7]. Delirium in elderly patients typically results from a complex interplay of factors, leading to exacerbated challenges in the ICU setting, such as prolonged hospitalization, increased mortality, and impaired quality of life [8,9,10]. Therefore, prospective biomarkers associated with delirium need to be explored to help reduce its risk.
Emerging evidence suggests that insulin resistance (IR) is strongly associated with several cerebrovascular diseases and cognitive decline. IR is a metabolic condition characterized by an impaired response of target tissues to insulin, resulting in abnormal glucose and lipid metabolism [11,12,13]. To assess IR, an index derived from fasting triglyceride and glucose levels, known as the TyG index, has been proposed as a simpler and more stable surrogate measure [14]. Significantly, the TyG index has demonstrated stand-alone predictive ability for conditions such as coronary heart disease, chronic kidney disease, stroke, and carotid atherosclerosis, fueling interest in its possible link to cognitive decline [15,16,17,18]. However, the TyG index has not confirmed a definitive association with the onset of ICU delirium in elderly patients, which requires further investigation.
The aim of this study was to investigate the relationship between the risk of delirium in elderly ICU patients and the TyG index and to elucidate the underlying mechanisms, based on a multicenter retrospective design with a large sample size. In addition, we hypothesized that elderly patients with higher TyG index would be at increased risk for adverse outcomes following delirium in ICU.
Methods
Data sources
All study data in this study were obtained from and the Medical Information Mart for Intensive Care (MIMIC-IV version 2.0) database [19, 20] and the eICU Collaborative Research Database (eICU-CRD) [21]. The MIMIC-IV database included data from tens of thousands of patients admitted to the ICU at Beth Israel Deakin Medical Center between 2008 and 2019. In contrast, the eICU-CRD included electronic medical records for more than 200,000 patients admitted to ICUs at more than 200 medical centers in 2014 and 2015. Institutional review boards at the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center approved the study. As such, patient informed consent and ethics approval were waived for this study.
Cohort selection
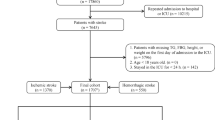
As shown in Fig. 1, we carefully selected our study cohort using strict inclusion and exclusion criteria. Initially, the cohort consisted of patients who had a documented TyG index and underwent delirium assessment during their initial ICU admission. We then excluded patients with an ICU stay of less than 24 h, those under 65 years of age, and those with a diagnosis of dementia, which can easily be confused with delirium. As a result, our study cohort included 4,649 patients, while the external validation cohort included 1,844 patients. We also stratified the study participants into two groups based on delirium status.

Flowchart illustrating the selection of patients from the MIMIC-IV database and eICU-CRD database Collaborative. Abbreviations: MIMIC-IV, Medical Information Mart for Intensive Care IV; eICU-CRD, eICU Collaborative Research Database; TyG, Triglyceride-glucose
Data collection
In this study, all data was extracted using a structured query language (SQL) server. The data extracted included various demographic characteristics including gender, age, ethnicity. In addition, vital signs such as temperature, heart rate, mean blood pressure, and respiratory rate were documented. Laboratory variables within the first 24 h of ICU admission, including white blood cell (WBC), red blood cell (RBC), platelet count, albumin, blood urea nitrogen (BUN), creatinine, serum sodium, serum potassium, international normalized ratio (INR), triglycerides, and glucose, were also collected. Comorbidities such as sepsis, myocardial infarction, cerebrovascular disease, chronic pulmonary disease, congestive heart failure, diabetes mellitus, renal disease, and malignant cancer were included in the analysis using International Classification of Diseases Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes. Data on post-admission procedures, including renal replacement therapy (RRT) and mechanical ventilation (MV), as well as length of stay and ICU stay, were also included. The TyG index was calculated from fasting glucose and triglyceride measurements obtained after ICU admission using the formula In[fasting triglycerides(mg/dl) × fasting blood glucose(mg/dl)/2] [22, 23].
Outcomes
The outcome variable of interest in this study was delirium, and the diagnosis of delirium relies on two main assessment tools, the Confusion Assessment Method for the ICU (CAM-ICU) [24] and the Intensive Care Delirium Screening Checklist (ICDSC) [25]. To the best of our knowledge, a bivariate meta-analysis demonstrated that both CAM-ICU and ICDSC had high sensitivity and specificity. The sensitivity for CAM-ICU was 0.84, and the pooled specificity was 0.95. For ICDSC, the pooled sensitivity was 0.83, and the pooled specificity was 0.87 [26]. Although in the MIMIC-IV database, only CAM-ICU assessment results were recorded, both assessment tools are available in the open eICU-CRD database. In addition, it should be noted that a small proportion of delirium patients in the MIMIC-IV database were diagnosed based on the care text diagnostic markers found in the “chartevents” table (itemid = 220,001). The key words for delirium diagnosis included “delirium”, “confusion”, “agitation” and “altered mental status”.
Statistical analysis
In this study, patients were divided into two groups according to whether they developed delirium while in the ICU. Differences were compared using chi-squared tests for categorical variables and Student’s t-test for continuous variables, with non-normal continuous variables expressed as medians over interquartile ranges.
To assess the association between the TyG index and the risk of ICU delirium, we used univariate and multivariate restricted cubic spline (RCS) regression to evaluate a possible nonlinear association between the TyG index and the risk of delirium in patients aged 65 years and older. We grouped the TyG index based on the cut points obtained from the RCS regression, using the lowest TyG index value as the reference group, and we used logistic regression to assess the risk ratios (ORs) and 95% confidence intervals (CIs) between the continuous variable per 1 unit and the grouped TyG indices on the primary outcome. Given the considerations of multicollinearity and clinical experience, we built three models, of which, model 1 was not adjusted for covariates; in model 2, adjusted for sex, age, laboratory parameters (albumin, serum potassium, serum sodium, creatinine, WBC, RBC, platelet); model 3 was fully adjusted for comorbidities (congestive heart failure, chronic pulmonary disease, myocardial infarction, liver disease, cerebrovascular disease, diabetes, renal disease, hypertension, malignant cancer) based on model 2. To avoid model overflow due to multicollinearity among variables, we also calculated variance inflation factors and excluded variables with variance input factors ≥ 2 (Supplementary Table 1).
To ensure the robustness of our findings, sensitivity analyses were performed in three scenarios. Firstly, patients with an ICU mortality outcome were excluded to minimize the influence of competing death outcomes on the risk of delirium. Secondly, patients with pre-existing diabetes were excluded to specifically examine the risk of delirium in patients without diabetes that is not strongly associated with the TyG index. Sepsis is known to be a major cause of delirium in the elderly, and we further excluded patients with sepsis to reduce the drawback of confounding factors. Lastly, propensity score matching (PSM) [27] was utilized to address any baseline imbalances between both groups of TyG patients and to reduce the potential impact of between-group differences on the models.
In addition, we performed stratified analyses based on several factors, including sex, age (≤ 80 and > 80 years), ethnicity (White and other), sepsis, chronic pulmonary disease, diabetes, congestive heart failure, and hypertension. The consistency of TyG index in predicting delirium was evaluated among subgroups.
Data analysis was performed using R software (version 4.1.3). A two-sided P value of < 0.05 was considered statistically significant.
Results
Baseline characteristics
After retrieving data from the MIMIC-IV database and the eICU database, a total of 4,649 patients from MIMIC-IV and 1,844 patients from the eICU were included in this study, following the specified inclusion and exclusion criteria. Among the enrolled patients, the median age was 76 years for the MIMIC-IV database and 75 years for the eICU database. The female population accounted for 46.1% (2,143 patients) in the MIMIC-IV database and 49.2% (907 patients) in the eICU database. The median TyG index were 8.9 (8.5, 9.4) and 8.9 (8.4, 9.3) for the MIMIC-IV and eICU databases, respectively. A total of 2,165 patients with delirium were included in the MIMIC-IV database and a total of 555 patients with delirium were included in the eICU database, as shown in Table 1. Especially in the MIMIC database, patients with delirium had higher WBC, RBC, BUN, creatinine, glucose, and triglyceride levels, and were more likely to have cerebrovascular disease, sepsis, and adverse outcomes (P < 0.001).
Association of TyG index with risk of delirium
We utilized restricted cubic splines to analyze the continuous relationship between the TyG index and the incidence of delirium in ICU. In the fully adjusted multivariate RCS model, our findings indicated a non-linear association between the TyG index and the risk of ICU delirium (P-nonlinear < 0.001, P-overall = 0.013). We observed that the risk of ICU delirium increased when the TyG index larger than 8.912 (Fig. 2). Based on the restricted cubic spline analysis, we defined two categories of patients: Q1 (< 8.912) and Q2 (≥ 8.912). Multivariate logistic regression analysis, with Q1 (< 8.912) as the reference group, showed that an elevated TyG index was associated with a higher risk of delirium (OR = 1.312, 95% CI: 1.157–1.488, P < 0.001). These findings were validated in the eICU-CRD dataset, consistently indicating that among ICU patients aged 65 and older, an elevated TyG index was positively correlated with increased delirium risk (OR = 1.259, 95% CI: 1.009–1.570, P = 0.041), especially in those with a TyG index of ≥ 8.912 (Table 2).

The potential nonlinear relationship between TyG index level and the risk of delirium in elderly ICU patients by restricted cubic spline regression. The red and dashed lines represent the estimated OR and 95% CIs, respectively. (A) Model 1 was an unadjusted model; (B) Model 2 was adjusted for sex, age, laboratory parameters (albumin, serum potassium, serum sodium, creatinine, WBC, RBC, platelet); (C) Model 3 was adjusted for comorbidities (congestive heart failure, sepsis, chronic pulmonary disease, myocardial infarction, liver disease, cerebrovascular disease, diabetes, renal disease, hypertension, malignant cancer) on the basis of Model 2. The final fully adjusted restricted cubic spline regression showed that the cut value of TyG index was 8.912. Abbreviations: TyG, Triglyceride-glucose
Sensitivity analysis of TyG index and the risk of delirium
The sensitivity analyses conducted in this study corroborated the robustness of the primary findings. Firstly, the exclusion of patients who died in the ICU did not significantly attenuate the statistical association between the TyG index and delirium. Secondly, even after excluding patients with sepsis, the relationship between the TyG index and the risk of delirium remained robust. Moreover, even after excluding patients with diabetes, which correlates with the TyG index, a significant association between the TyG index and the risk of delirium remained in patients without a history of the condition (Supplementary Tables 2–4). Lastly, PSM was employed to minimize discrepancies between the groups, The observed results were consistent with the primary analysis, indicating that in ICU patients aged 65 and above, a higher TyG index is associated with an increased risk of delirium (Supplementary Tables 5–6).
Subgroup analysis
Evaluating the association between the TyG index and the risk of delirium amongst geriatric patients in critical care, while taking into account variances such as sex, age, ethnicity, along with comorbidities like congestive heart failure, chronic pulmonary disease, hypertension, sepsis and renal disease, revealed intriguing outcomes. We observed significant differences in the subgroups of white males aged over 80 with comorbidities of congestive heart failure, chronic pulmonary disease, and sepsis. Within these subgroups, a substantial increase in the risk of delirium was evident, when the TyG index values larger than 8.912 (Fig. 3, Supplementary Table 7).

Subgroup analysis for the association of TyG index with the risk of delirium. Abbreviations: TyG, Triglyceride-glucose; OR, odds ratio; CI, confidence interval
Further analysis
Our study also found that individuals who succumbed to delirium had a propensity for adverse prognostic outcomes as determined by Kaplan-Meier survival analyses at various follow-up periods including 30 days, 90 days, and 360 days. There was a statistically significant difference in mortality between the two groups (log-rank test: all P < 0.05). It’s worth noting that these results were even more pronounced at the shorter, 30 days follow-up (HR = 2.134, Supplementary Fig. 1).
Discussion
This study demonstrated a definitive association between the TyG index and the risk of delirium in geriatric critically ill patients. Drawing from the MIMIC-IV and eICU-CRD databases, the study’s conclusions were strengthened by its large sample size and diverse representation. Notably, this was the first multicenter study to correlate the TyG index with delirium susceptibility in elderly ICU patients. It posited that an elevated TyG index correlates with an increased risk of delirium within a certain range for ICU patients aged 65 years and older.
As far as we know, insulin is a peptide hormone mainly secreted by beta cells of the pancreas, which is essential for the regulation of glucose metabolism in peripheral tissues. This hormone plays a special role in the central nervous system (CNS), where each cell type expresses insulin receptors [28]. These receptors are diffusely distributed throughout the brain, establishing insulin signaling pathways that influence brain plasticity and contribute to neurodegenerative processes. It’s noteworthy that insulin’s central influence extends to the hippocampus, entorhinal cortex, and frontal cortex, regions that are integral to the brain’s cognitive functions. In addition, insulin confers protection against the Aβ protein, thereby influencing lipid metabolism and proteases [29, 30]. Consequently, abnormalities in insulin function may precipitate neurodegeneration or cognitive decline. IR, characterized by reduced sensitivity of the body’s target tissues and cells to insulin, rendering them unable to function normally, has been proposed as a potential culprit for these deleterious effects [31]. Prior research indicated that the TyG index, derived from fasting glucose and triglyceride levels, is proposed as a straightforward surrogate marker of IR, predicated on the notion that insulin’s impact on lipolysis is somewhat less pronounced than on glucose metabolism [32, 33]. Compared to the HOMA-IR (Homeostasis model assessment of IR) index, the TyG index showed superior predictive ability for IR as determined by the hyperglycemic clamp test [34]. This easily measurable index is more amenable to large-scale population studies and was used in this study to test the hypothesis of a possible association in patients with delirium.
Up to now, no definitive studies have established a link between IR and delirium, and only some studies have focused on the progression between IR and prevention of postoperative delirium in patients from a therapeutic perspective [11]. some clinical trials of IR in the treatment of postoperative delirium in elderly patients have been published [35, 36]. A clinical trial study determined the safety and effectiveness of IR in preventing delirium after 6 months of IR treatment in patients with postoperative delirium, which indirectly supports the hypothesis of this study that the TyG index, a marker of IR, predicts the incidence of delirium [37]. In addition, the etiology of delirium and dementia has long been suspected to have significant overlap, and a number of studies have confirmed the potential association of IR with cognitive decline and dementia. A retrospective cohort study from the US National Health Information Database published in 2021 found that TyG index as a marker of IR can independently but small predict the development of dementia [32]. Meanwhile, Kai Wang et al. proposed an association between increased TyG index and a higher risk of cognitive decline in men [38]. From a neuropathological perspective, dementia and delirium are closely related, and based on this background, these findings above potentially bridge the link between IR and delirium. The present study was the first to examine the association between the TyG index and the risk of developing delirium in ICU patients aged 65 years and older and found that an elevated TyG index was a strong independent predictor of an increased risk of delirium in ICU patients aged 65 years and older. This association persisted after adjustment for several clinical and laboratory variables. The present study differs from previous studies in that [18], first, we used large multicenter data, MIMIC-IV and eICU-CRD covering multiple centers, allowing for better confidence in the findings. Second, we performed sensitivity analyses using PSM analysis and excluding patients with a diagnosis of diabetes and adverse outcomes to ensure the robustness of the results. Third, we performed the subgroup analysis and found that significant differences in the subgroups of white males aged over 80 with comorbidities of congestive heart failure, chronic pulmonary disease, and sepsis. We also performed an additional analysis of the adverse prognosis of delirium and found that the increased risk of delirium with a high TyG index showed an incremental prediction of the rate of death.
While the exact pathophysiological mechanisms linking the TyG index to delirium remain unclear, the prevailing hypothesis suggests an underlying IR. However, the possibility that this association is mediated by latent diabetes cannot be completely ruled out. Several lines of evidence support this theory. Firstly, extensive animal studies suggest that tau proteins, which are regulated by insulin signaling in the brain, play a central role in the central nervous system, particularly in the hippocampal response to insulin [39, 40]. These changes are exacerbated by the effects of IRS-1 and phosphatase and tension homolog (PTEN) [41]. IR, characterized by a diminished response to insulin from target tissues, plays an important role in neurodegenerative diseases that affect neuronal metabolism. IR could potentially increase tau hyperphosphorylation by inhibiting PI3-K/AKT and enhancing GSK3-β activation, while an imbalance in tau protein phosphorylation is a pathological indicator of cognitive decline. Therefore, dysregulation of insulin signaling pathways may trigger cognitive impairments such as delirium [42]. Secondly, the mechanisms linking IR and neurodegenerative diseases have been explored previously. Abnormal accumulation of Aβ protein has emerged as a new theory in the pathogenesis of psychosis. Insulin inhibits the formation of Aβ fibers and promotes the internalization of Aβ oligomers, thereby limiting their neuronal binding and protecting synapses from Aβ oligomers [43]. With the onset of IR in the brain, degradation and clearance of Aβ are impeded, and abnormal Aβ deposition stimulates glial cells to release a variety of inflammatory factors and generate oxygen free radicals that induce oxidative stress and activate apoptosis [44]. IR may also induce impairment of macrophage endothelial function and exacerbate arterial atherosclerosis and dyslipidemia, all of which could potentially contribute to the development of delirium. Some clinical studies have provided evidence to support this notion [45]. Thirdly, a meta-analysis has shown that patients with type 2 diabetes are more likely to develop Alzheimer’s disease (AD). In type 2 diabetes, IR leads to a high risk of Aβ protein deposition and tau pathology leading to AD symptoms [46, 47]. Importantly, our research findings have practical implications, especially for the early clinical prediction of delirium in critically ill elderly patients, offering support for early interventions to mitigate the risk of adverse outcomes induced by IR. Our research provides new perspectives on the relationship between delirium and IR in ICU patients aged 65 years and older. However, we cannot conclusively establish a causal relationship between a high TyG index and the subsequent presence of delirium.
There are several limitations of this study. First, the retrospective design of our study constrained our ability to capture detailed and dynamic clinical parameters, such as the duration and recovery patterns of delirium. Understanding the association between the TyG index and the course of recovery from delirium in elderly patients is of potential clinical significance. Consequently, prospective studies are needed in the future to further explore this aspect, this will contribute to a more comprehensive understanding of the role of the TyG index in managing delirium within critical care settings. Second, owing to the inherent limitations of our multi-center study design, this research was restricted to variables consistently available in the MIMIC-IV and eICU-CRD. Despite our utmost efforts to adjust for available variables that might affect delirium outcomes in accordance with the clinical context and applying PSM to observable biases, there still exists the possibility of data bias affecting the results due to unincorporated covariates, such as APACHE and SOFA severity of illness scores for critical diseases. Third, although our findings were externally validated, the majority of our patient data were from the United States, which may limit the generalizability of our results to patients aged 65 years and older in other geographic regions. Therefore, caution should be exercised when extrapolating these findings to other population cohorts. Fourth, delirium manifests in different subtypes, including hyperactive, hypoactive, and mixed. Our study did not address these subtypes, which may limit our comprehensive understanding and management of delirium. Fifthly, given that our study was a retrospective analysis from an observational study, it primarily established a correlation between the TyG index and delirium, without effectively substantiating a causal relationship. Subsequent studies are indispensable to establish causality and to observe the dynamics of TyG index over time, thereby affirming its positive prognostic significance in critically ill patients. Finally, our study focused primarily on patients aged 65 years and older in the ICU, and it is uncertain whether these findings can be extrapolated to older patients in general wards or nursing homes. Future research should aim to expand sample sources to include a wider range of regions and patient types to improve the generalizability of the findings.
Conclusions
In conclusion, the increased IR was independently and positively correlated with an increased risk of critical delirium in patients aged 65 years and older. This finding suggests the potential of the TyG index as an effective cardio-cerebrovascular metabolic marker for risk classification and management in a high-risk geriatric population. Future research should aim to investigate the clinical significance of the dynamic changes in the TyG index under different clinical conditions.
Data availability
The data were available on the MIMIC-IV website at https://mimic.physionet.org/ and eICU-CRD at https://eicu-crd.mit.edu/. The data in this article can be reasonably applied to the corresponding author.
Abbreviations
- TyG:
-
Triglyceride-glucose
- ICU:
-
Intensive care unit
- eICU-CRD:
-
eICU Collaborative Research Database
- MIMIC-IV:
-
Medical Information Mart for Intensive Care IV
- IR:
-
Insulin resistance
- FBG:
-
Fasting blood glucose
- WBC:
-
White blood cell
- ICD:
-
International Classification of Diseases
- LOS:
-
Length of stay
- IQR:
-
Interquartile range
- VIF:
-
Variance inflation factor
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
- RCS:
-
Restricted cubic spline
- PSM:
-
Propensity score matching
- HOMA-IR:
-
Homeostasis model assessment of IR
- MI:
-
Myocardial infarction
- RRT:
-
Renal replacement therapy
- MV:
-
Mechanical ventilation
- CAM-ICU:
-
Confusion Assessment Method in the Intensive Care Unit
- ICDSC:
-
Intensive Care Unit Delirium Screening Checklist
References
Stollings JL, Kotfis K, Chanques G, Pun BT, Pandharipande PP, Ely EW. Delirium in critical illness: clinical manifestations, outcomes, and management. Intens care med. 2021;47:1089–103.
Toft K, Tontsch J, Abdelhamid S, Steiner L, Siegemund M, Hollinger A. Serum biomarkers of delirium in the elderly: a narrative review. ANN INTENSIVE CARE. 2019;9:76.
Wilcox ME, Girard TD, Hough CL. Delirium and long term cognition in critically ill patients. BMJ-BRIT MED J. 2021;373:n1007.
Girard TD, Jackson JC, Pandharipande PP, Pun BT, Thompson JL, Shintani AK, et al. Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Crit care med. 2010;38:1513–20.
Girard TD, Thompson JL, Pandharipande PP, Brummel NE, Jackson JC, Patel MB, et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study. Lancet Resp Med. 2018;6:213–22.
Nassar AP, Ely EW, Fiest KM. Long-term outcomes of intensive care unit delirium. INTENS CARE MED. 2023;49:677–80.
Volpe JJ. Brain injury in premature infants: a complex amalgam of destructive and developmental disturbances. LANCET NEUROL. 2009;8:110–24.
Bellelli G, Brathwaite JS, Mazzola P. Delirium: a marker of vulnerability in older people. FRONT AGING NEUROSCI. 2021;13:626127.
Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383:911–22.
Kakuma R, du Fort GG, Arsenault L, Perrault A, Platt RW, Monette J, Moride Y, Wolfson C. Delirium in older emergency department patients discharged home: effect on survival. J AM GERIATR SOC. 2003;51:443–50.
Shpakov AO, Zorina II, Derkach KV. Hot spots for the use of intranasal insulin: cerebral ischemia, brain injury, diabetes mellitus, endocrine disorders and postoperative delirium. Int J Mol Sci 2023;24.
Wang J, Shuang P, Li Z, Zhao L, Wang X, Liu P. Association of insulin resistance with delirium and CSF biomarkers of Alzheimer’s Disease in elderly patients with hip fracture. Aging Clin Exp Res. 2023;35:1521–9.
Di Pino A, DeFronzo RA. Insulin resistance and Atherosclerosis: implications for insulin-sensitizing agents. ENDOCR REV. 2019;40:1447–67.
Fritz J, Bjørge T, Nagel G, Manjer J, Engeland A, Häggström C, Concin H, Teleka S, Tretli S, Gylling B, Lang A, Stattin P, Stocks T, Ulmer H. The triglyceride-glucose index as a measure of insulin resistance and risk of obesity-related cancers. INT J EPIDEMIOL. 2020;49:193–204.
Wang A, Wang G, Liu Q, Zuo Y, Chen S, Tao B, et al. Triglyceride-glucose index and the risk of stroke and its subtypes in the general population: an 11-year follow-up. Cardiovasc Diabetol. 2021;20:46.
Ye Z, An S, Gao Y, Xie E, Zhao X, Guo Z, et al. Association between the triglyceride glucose index and in-hospital and 1-year mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit. Cardiovasc Diabetol. 2023;22:110.
Liao Y, Zhang R, Shi S, Zhao Y, He Y, Liao L, Lin X, Guo Q, Wang Y, Chen L, Li W, Li S, Chen K, Fang Y. Triglyceride-glucose index linked to all-cause mortality in critically ill patients: a cohort of 3026 patients. CARDIOVASC DIABETOL. 2022;21:128.
Wang K, Xu L, Liu L, Zhan S, Wang S, Song Y. Sex differences in the association between the change in triglyceride–glucose index and cognitive decline: a population-based cohort study. J AFFECT DISORDERS. 2022;316:42–9.
Yang J, Li Y, Liu Q, Li L, Feng A, Wang T, Zheng S, Xu A, Lyu J. Brief introduction of medical database and data mining technology in big data era. J EVID-BASED MED. 2020;13:57–69.
Wu WT, Li YJ, Feng AZ, Li L, Huang T, Xu AD, Lyu J. Data mining in clinical big data: the frequently used databases, steps, and methodological models. MILITARY MED RES. 2021;8:44.
Pollard TJ, Johnson A, Raffa JD, Celi LA, Mark RG, Badawi O. The eICU collaborative research database, a freely available multi-center database for critical care research. Sci Data. 2018;5:180178.
Zhang B, Liu L, Ruan H, Zhu Q, Yu D, Yang Y, et al. Triglyceride-glucose index linked to hospital mortality in critically ill stroke: an observational multicentre study on eICU database. Front Med-Lausanne. 2020;7:591036.
Cheng L, Zhang F, Xue W, Yu P, Wang X, Wang H, et al. Association of dynamic change of triglyceride-glucose index during hospital stay with all-cause mortality in critically ill patients: a retrospective cohort study from MIMIC-IV 2.0. Cardiovasc Diabetol. 2023;22:142.
Young M, Holmes N, Kishore K, Marhoon N, Amjad S, Serpa-Neto A, Bellomo R. Natural language processing diagnosed behavioral disturbance vs confusion assessment method for the intensive care unit: prevalence, patient characteristics, overlap, and association with treatment and outcome. INTENS CARE MED. 2022;48:559–69.
Frenette AJ, Bebawi ER, Deslauriers LC, Tessier AA, Perreault MM, Delisle MS, et al. Validation and comparison of CAM-ICU and ICDSC in mild and moderate traumatic brain injury patients. Intens Care Med. 2016;42:122–3.
Chen TJ, Chung YW, Chang HR, Chen PY, Wu CR, Hsieh SH, et al. Diagnostic accuracy of the CAM-ICU and ICDSC in detecting intensive care unit delirium: a bivariate meta-analysis. Int J Nurs Stud. 2021;113:103782.
Deb S, Austin PC, Tu JV, Ko DT, Mazer CD, Kiss A, Fremes SE. A review of propensity-score methods and their use in cardiovascular research. CAN J CARDIOL. 2016;32:259–65.
Unger JW, Betz M. Insulin receptors and signal transduction proteins in the hypothalamo-hypophyseal system: a review on morphological findings and functional implications. HISTOL HISTOPATHOL. 1998;13:1215–24.
Pandini G, Pace V, Copani A, Squatrito S, Milardi D, Vigneri R. Insulin has multiple antiamyloidogenic effects on human neuronal cells. Endocrinology. 2013;154:375–87.
Zhao WQ, Lacor PN, Chen H, Lambert MP, Quon MJ, Krafft GA, et al. Insulin Receptor Dysfunction Impairs Cellular Clearance of Neurotoxic Oligomeric Aβ. J Biol Chem. 2009;284:18742–53.
Mielke JG, Taghibiglou C, Liu L, Zhang Y, Jia Z, Adeli K, Wang YT. A biochemical and functional characterization of diet-induced brain insulin resistance. J NEUROCHEM. 2005;93:1568–78.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, Jacques-Camarena O, Rodríguez-Morán M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J CLIN ENDOCR METAB. 2010;95:3347–51.
Bloom GS. Amyloid-β and tau: the trigger and bullet in Alzheimer Disease pathogenesis. Jama Neurol. 2014;71:505–8.
Torres AK, Jara C, Park-Kang HS, Polanco CM, Tapia D, Alarcón F, et al. Synaptic mitochondria: an early target of amyloid-β and tau in Alzheimer’s Disease. J Alzheimers Dis. 2021;84:1391–414.
Huang Q, Li Q, Qin F, Yuan L, Lu Z, Nie H, Gong G. Repeated preoperative intranasal administration of insulin decreases the incidence of postoperative delirium in elderly patients undergoing laparoscopic radical gastrointestinal Surgery: a randomized, placebo-controlled, double-blinded clinical study. AM J GERIAT PSYCHIAT. 2021;29:1202–11.
Huang Q, Shi Q, Yi X, Zeng J, Dai X, Lin L, et al. Effect of repeated intranasal administration of different doses of insulin on postoperative delirium, serum τ and Aβ protein in elderly patients undergoing radical esophageal cancer surgery. Neuropsych Dis Treat. 2023;19:1017–26.
Nitchingham A, Milne A, Toson B, Tuch B, Agar M, Close J, Caplan G. Intranasal insulin for treatment of delirium in older hospitalised patients: study protocol for a randomised controlled trial. BMJ OPEN. 2021;11:e50765.
Hong S, Han K, Park CY. The insulin resistance by triglyceride glucose index and risk for Dementia: population-based study. ALZHEIMERS RES THER. 2021;13:9.
Schubert M, Brazil DP, Burks DJ, Kushner JA, Ye J, Flint CL, Farhang-Fallah J, Dikkes P, Warot XM, Rio C, Corfas G, White MF. Insulin receptor substrate-2 deficiency impairs brain growth and promotes tau phosphorylation. J NEUROSCI. 2003;23:7084–92.
Lei P, Ayton S, Finkelstein DI, Spoerri L, Ciccotosto GD, Wright DK, et al. Tau deficiency induces parkinsonism with dementia by impairing app-mediated iron export. Nat Med. 2012;18:291–5.
Rodriguez-Rodriguez P, Sandebring-Matton A, Merino-Serrais P, Parrado-Fernandez C, Rabano A, Winblad B, Ávila J, Ferrer I, Cedazo-Minguez A. Tau hyperphosphorylation induces oligomeric insulin accumulation and insulin resistance in neurons. Brain. 2017;140:3269–85.
Avila J, León-Espinosa G, García E, García-Escudero V, Hernández F, Defelipe J. Tau phosphorylation by gsk3 in different conditions. Int J Alzheimers Dis. 2012;2012:578373.
Micci MA, Krishnan B, Bishop E, Zhang WR, Guptarak J, Grant A, et al. Hippocampal stem cells promotes synaptic resistance to the dysfunctional impact of amyloid beta oligomers via secreted exosomes. Mol Neurodegener. 2019;14:25.
Agostinho P, Cunha RA, Oliveira C. Neuroinflammation, oxidative stress and the pathogenesis of Alzheimer’s Disease. Curr Pharm Design. 2010;16:2766–78.
Wakabayashi T, Yamaguchi K, Matsui K, Sano T, Kubota T, Hashimoto T, et al. Differential effects of diet- and genetically-induced brain insulin resistance on amyloid pathology in a mouse model of Alzheimer’s Disease. Mol Neurodegener. 2019;14:15.
Li T, Cao HX, Ke D. Type 2 diabetes mellitus easily develops into Alzheimer’s Disease via hyperglycemia and insulin resistance. Curr Med Sci. 2021;41:1165–71.
Sędzikowska A, Szablewski L. Insulin and insulin resistance in Alzheimer’s Disease. Int J Mol Sci. 2021;22:9987.
Acknowledgements
The present study data was based on the MIMIC-IV and eICU database. We would like to thank all staff and patients involved in the construction of the MIMIC-IV and eICU database.
Funding
This research was supported by Guangdong Provincial Key Laboratory of Traditional Chinese Medicine Informatization (2021B1212040007), Clinical Frontier Technology Program of the First Affiliated Hospital of Jinan University, China (No. JNU1AF-CFTP-2022-a01235) and the Science and Technology Projects in Guangzhou, China (No. 202201020054, No. 2023A03J1032).
Author information
Authors and Affiliations
Contributions
XH, SY guided the literature review and planned the analyses. HC extracted the data from the MIMIC-IV and eICU database. ST and YL participated in data analysis and interpretation. SY, NC and YT confirmed the data and assisted with the statistical analyses. XH, HC wrote the first draft of the paper and critically revised the manuscript. JL conceptualized the research aims, read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed according to the guidelines of the Helsinki Declaration. The Medical Information Mart for Intensive Care IV (MIMIC-IV) database was supported by grants from the National Institute of Biomedical Imaging and Bioengineering (NIBIB) of the National Institutes of Health (NIH) under award numbers R01-EB001659 (2003–2013) and R01-EB017205 (2014–2018) and approved by the Institutional Review Boards of Beth Israel Deaconess Medical Center (Boston, MA) and the Massachusetts Institute of Technology (Cambridge, MA). The eICU Collaborative Research Database was released under the Health Insurance Portability and Accountability Act (HIPAA) safe harbor provision. The re-identification risk was certified as meeting safe harbor standards by Privacert (Cambridge, MA) (HIPAA Certification no. 1031219-2). The data is publicly available (in the MIMIC-IV and eICU database), therefore, the ethical approval statement and the requirement for informed consent were waived for this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, X., Cheng, H., Yuan, S. et al. Triglyceride-glucose index as a valuable predictor for aged 65-years and above in critical delirium patients: evidence from a multi-center study. BMC Geriatr 23, 701 (2023). https://doi.org/10.1186/s12877-023-04420-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-04420-0