
Abstract
Background
It is unknown whether high hemoglobin A1c (HbA1c) is associated with increases in the risk of cardiovascular disease among individuals with elevated genetic susceptibility. We aimed to investigate the association between HbA1c and atrial fibrillation (AF), coronary artery disease (CAD), and ischemic stroke according to the polygenic risk score (PRS).
Methods
The UK Biobank cohort included 502,442 participants aged 40–70 years who were recruited from 22 assessment centers across the United Kingdom from 2006 to 2010. This study included 305,605 unrelated individuals with available PRS and assessed new-onset AF, CAD, and ischemic stroke. The participants were divided into tertiles based on the validated PRS for each outcome. Within each PRS tertiles, the risks of incident events associated with HbA1c levels were investigated and compared with HbA1c < 5.7% and low PRS. Data were analyzed from November 2022 to May 2023.
Results
Of 305,605 individuals, 161,605 (52.9%) were female, and the mean (SD) age was 56.6 (8.1) years. During a median follow-up of 11.9 (interquartile range 11.1–12.6) years, the incidences of AF, CAD, and ischemic stroke were 4.6, 2.9 and 1.1 per 100 person-years, respectively. Compared to individuals with HbA1c < 5.7% and low PRS, individuals with HbA1c ≥ 6.5% and high PRS had a 2.67-times higher risk for AF (hazard ratio [HR], 2.67; 95% confidence interval (CI), 2.43–2.94), 5.71-times higher risk for CAD (HR, 5.71; 95% CI, 5.14–6.33) and 2.94-times higher risk for ischemic stroke (HR, 2.94; 95% CI, 2.47–3.50). In the restricted cubic spline models, while a U-shaped trend was observed between HbA1c and the risk of AF, dose-dependent increases were observed between HbA1c and the risk of CAD and ischemic stroke regardless PRS tertile.
Conclusions
Our results suggest that the nature of the dose-dependent relationship between HbA1c levels and cardiovascular disease in individuals with different PRS is outcome-specific. This adds to the evidence that PRS may play a role together with glycemic status in the development of cardiovascular disease.
Similar content being viewed by others


Introduction
Cardiovascular disease is a leading cause of mortality and a major public health issue worldwide. Although the burden of cardiovascular disease has decreased over the past decades, death caused by diabetes is still increasing [1]. Diabetes is an established risk factor for cardiovascular disease, and individuals with diabetes have an increased risk of cardiovascular mortality compared to those without diabetes [2]. Also, elevated fasting blood glucose and hemoglobin A1c (HbA1c) levels are associated with cardiovascular disease and mortality [3, 4]. Several studies have shown that glycemic status is associated with an increased risk of coronary artery disease (CAD) and ischemic stroke [5,6,7].
Atrial fibrillation (AF) increases the risk of mortality and morbidity resulting from stroke and heart failure, and also impairs the quality of life [8,9,10]. The incidence of AF is correlated with increasing age, obesity, hypertension, diabetes, heart failure, valvular heart disease, and CAD [11, 12]. In healthy individuals, high-normal blood pressure and impaired fasting glucose were important risk factors for AF [13]. Several studies have suggested that the duration of diabetes or insulin treatment were related to the development of AF [14, 15]. However, the evidence for an association between diabetes or glycemic status measured by HbA1c and risk of AF is still controversial [12, 16,17,18,19,20].
Polygenic risk scores (PRSs) provide personalized estimates of genetic information related to diseases. Several recent genome-wide association studies (GWASs) have demonstrated genetic variants associated with AF, CAD and ischemic stroke [21,22,23]. However, there are concerns about the methods to incorporate genetic variants to calculate the PRS and potential risks caused by inappropriate and biased information [24]. Recently, Thompson et al. [25] presented PRSs for several diseases, including AF, CAD, and ischemic stroke, in UK Biobank participants and released a PRS comparison tool to enable performance evaluation for different PRSs. It is currently unknown whether high HbA1c is associated with an increased risk of cardiovascular disease among individuals with elevated genetic susceptibility. This study aimed to evaluate the associations of high HbA1c and diabetes status with incident cardiovascular disease among individuals with different PRS and to investigate how PRSs interact with these associations in the UK Biobank.
Method
Study population
The UK Biobank is a large-scale database consisting of more than 500,000 participants aged 40–69 years from 22 assessment centers throughout the United Kingdom between 2006 and 2010. The participants had undergone an extensive range of physical measures, provided information on their environment, lifestyle, medical history, and genetic data at recruitment, and agreed to have their health information followed up through linkages to electronic health-related records. The details of the study design and data collection have been described previously [26]. This study included the UK Biobank participants with measurement of HbA1c at enrollment, HbA1c < 15%, and available genetic data [25]. Participants with prevalent disease outcome were excluded in each analysis (Fig. 1). UK Biobank received ethical approval from the Northwest Multicenter Research Ethics Committee. The UK Biobank data are available to researchers after acceptance of the research proposal to the UK Biobank. Written informed consent was obtained from all the participants during recruitment. This study has been conducted using the UK Biobank Resource (Application No 77,793). This study was approved by the Institutional Review Board of Yonsei University Health System (4-2023-0323).

Flowchart for the selection of the analyzed study sample from the UK Biobank study. AF, atrial fibrillation; BMI, body mass index; HbA1c, hemoglobin A1c; PRS, polygenic risk score
From the 486,157 unrelated individuals with available PRS data, 162,906 participants were excluded based on the following criteria: (1) 82,788 with missing data on HbA1c, or blood glucose, (2) 13 with HbA1c ≥ 15%, (3) 80,105 with missing data on body mass index, alcohol, smoking, physical activity, or economic status. Participants with prevalent diseases were excluded from each analysis (Fig. 1), leaving 313,331 participants for the analysis of AF; 315,698 for CAD; and 321,843 for ischemic stroke. After these exclusions, 305,605 participants were included in all of analyses.
Polygenic risk score
The PRSs available from the UK Biobank were generated by other researchers and reviewed by UK Biobank. PRS were calculated as the sum of the effect sizes of individual genetic variants multiplied by the allele dosage. The effect sizes of the single nucleotide polymorphism-disease associations were based on external GWAS data, which were estimated via a fixed-effect inverse variance meta-analysis. Details for generating the PRS have been previously described [25]. The PRS were then divided into tertiles to categorize individuals into low, intermediate, and high. In addition, we conducted a sensitivity analysis using the PRS categorized as low (quintile 1), intermediate (quintiles 2–4), or high (quintile 5).
Glycemic status and covariates
Glycemic status was evaluated using HbA1c (mmol/mol), which was measured through high-performance liquid chromatography analysis on a Bio-Rad VARIANT II Turbo using non-fasting blood samples [27]. The unit in mmol/mol was converted to percentage (%) based on the equation: (0.09148 × HbA1c in mmol/mol) + 2.152 [28]. HbA1c was classified as < 5.7%, 5.7–6.4%, and ≥ 6.5%. The diabetes status was classified as diabetes, prediabetes, or normoglycemia. Diabetes identified through self-reported medical conditions or diagnosis using the ICD-10 code (E10-14), and/or the use of insulin treatment. Undiagnosed patients were identified, according to the ADA criteria, based on HbA1c ≥ 6.5%.29 Prediabetes was defined as no diagnosis of diabetes, and HbA1c ≥ 5.7 and < 6.5%. Normoglycemia was defined as no diagnosis of diabetes or an HbA1c < 5.7%.
Ethnicity was self-reported and categorized as Asian, Black, White, or Mixed. Participants reported their history of smoking status (non-, ex-, current smokers), frequency of alcohol intake (non-, 1–3 times/month, 1–2 times/week, and ≥ 3 times/week). Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ) and was categorized as low, moderate, or high. The Townsend Deprivation Index was divided into five categories based on UK census data.
Outcomes
Disease outcomes were defined as self-reported medical conditions or the first event occurring during at least two different days of hospital visits (primary care data) or the first admission (hospital inpatient data) with the ICD-10 code. Detailed definitions of the outcomes and comorbidities are presented in eTables 1 and 2. Hospital registry-based follow-up ended on March 31, 2021, in England and Scotland, and February 28, 2018, in Wales. The cohorts were followed up until the occurrence of each outcome, death, emigration, or the end of the study, whichever occurred first.
Statistical analysis
Multivariate Cox proportional hazards regression analysis was performed to test the association of the PRS and HbA1c with incident AF, CAD and ischemic stroke. Individuals with low PRS and HbA1c levels of < 5.7% or normoglycemia were used as the reference group in each analysis. Cox regression analyses were adjusted for age; sex; ethnicity; body mass index; smoking; alcohol consumption; hypertension; dyslipidemia; heart failure; peripheral artery disease; chronic kidney disease; end-stage renal disease; physical activity; and economic status. The proportional hazards assumption was verified using Schoenfeld residuals. The Wald test was used to analyze the differences between the hazard ratios (HR) of each exposure within the PRS tertiles (Pdifference). Restricted cubic splines were used to estimate the potential nonlinearity of the associations between HbA1c levels and outcomes according to PRS tertiles. The number of knots for the restricted cubic spline models was selected using the Bayesian information criterion (BIC). The reference value for the spline curve was 5.5% of HbA1c. We used the Bonferroni correction to adjust for multiple testing and considered 2-sided P values < 0.017 (P value < 0.05, divided by the number of tests, i.e., 0.05/3) statistically significant. Statistical analyses were conducted using R software (version 4.3.3; R Foundation, www.R-project.org).
Results
Population characteristics
Of 306,605 individuals, 161,605 (52.9%) were female, and the mean (SD) age was 56.6 (8.1) years. 251,947 (82.4%) had HbA1c < 5.7%, 43,307 (14.2%) had HbA1c 5.7–6.4%, and 10,351 (3.4%) had HbA1c ≥ 6.5%. A total of 250,468 (81.9%) patients had normoglycemia, 41,522 (13.6%) had prediabetes, and 13,615 (4.5%) had diabetes. Depending on the outcome, the size of the study population varied with the prevalence of disease exclusion. Baseline characteristics according to HbA1c category are presented as PRS tertiles of AF (eTable 3), CAD (eTable 4), and ischemic stroke (eTable 5). In general, individuals with higher HbA1c levels were more likely to be male, older, have a higher body mass index, and more comorbidities, including hypertension, dyslipidemia, heart failure, peripheral artery disease, chronic kidney disease, and end-stage renal disease, than individuals with lower HbA1c levels (Table 1).
Association of PRS with incident cardiovascular disease
During a median (interquartile range) follow-up of 11.9 (11.1–12.6) years, 17,397 participants developed AF, 12,895 developed CAD and 3,489 developed ischemic stroke. eFigure 1 shows that a higher PRS was associated with a higher incidence of AF, CAD, and ischemic stroke during follow-up. In multivariable adjusted models, high PRS was associated with a higher risk of incident AF (HR, 2.46; 95% CI, 2.37–2.56; P < .001), CAD (HR, 3.26; 95% CI, 3.09–3.44; P < .001), ischemic stroke (HR, 1.57; 95% CI, 1.45–1.71; P < .001) compared with low PRS (eTable 6). The influence of the PRS tertiles of each outcome on incident AF, CAD, and ischemic stroke was comparable with other clinical risk factors, including diabetes, hypertension, heart failure, peripheral artery disease, and chronic kidney disease (eFigure 2).
Association of HbA1c and PRS with incident cardiovascular disease
Compared with HbA1c < 5.7% and low PRS, individuals with HbA1c ≥ 6.5% and high PRS were associated with high risk of AF (HR, 2.67; 95% CI 2.43–2.94; P < .001), CAD (HR, 5.71; 95% CI 5.14–6.33; P < .001) and ischemic stroke (HR, 2.94; 95% CI 2.47–3.50; P < .001) (Fig. 2). HbA1c > 6.5% was gradually associated with an increased risk of CAD (Fig. 2B) and ischemic stroke (Fig. 2C) across all PRS tertiles (Ptrend < 0.001 and Pdifference < 0.001, respectively). However, the association between HbA1c > 6.5% and AF was significant only in individuals with a low PRS. (Fig. 2A).

Associations of hemoglobin A1c with atrial fibrillation, coronary artery disease, and ischemic stroke by polygenic risk score tertiles. Adjusted for age, sex, ethnicity, body mass index, smoking, alcohol, hypertension, dyslipidemia, heart failure, peripheral artery disease, chronic kidney disease, end stage renal disease, physical activity, and economic status. Hazard ratios (HRs) are provided with 95% CIs. The vertical line indicates the reference value of 1.
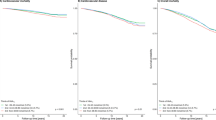
In the restricted cubic spline models, the risk of AF decreased to a nadir at 5.5% of HbA1c and then increased (Pnonlinearity < 0.001). The risks of CAD and ischemic stroke increased steadily with increasing HbA1c levels. However, compared with HbA1c < 5.7%, the effect of HbA1c on CAD risk was modest at HbA1c ≥ 5.7% (Pnonlinearity < 0.001). In individuals with low PRS, the HR of AF, CAD, and ischemic stroke at 9% HbA1c were 1.33 (95% CI 1.22–1.45), 2.19 (95% CI 2.01–2.38) and 2.27 (95% CI 1.96–2.64) respectively, compared with 5.5% HbA1c (Fig. 3).

Nonlinear dose–response analysis of hemoglobin A1c and the risk of atrial fibrillation, coronary artery disease and ischemic stroke, by polygenic risk score tertiles. The model is centered at 5.5% HbA1c with knots at 5.0%, 5.7%, and 6.5% HbA1c.
Associations of diabetes status and PRS with incident cardiovascular disease
Compared with normoglycemia and low PRS, individuals with diabetes and high PRS were associated with high risk of AF (HR, 2.69; 95% CI 2.48–2.92; P < .001), CAD (HR, 5.01; 95% CI 4.54–5.53; P < .001) and ischemic stroke (HR, 2.83; 95% CI 2.41–3.32; P < .001) (Fig. 4). Diabetes was associated with a higher risk of CAD (Fig. 4B) and ischemic stroke (Fig. 4C) in each PRS tertile (Ptrend < 0.001 and Pdifference < 0.001, respectively). However, the association between diabetes status and a higher risk of AF was significant only in the intermediate PRS tertile (Pdifference = 0.010).

Associations of diabetes status with atrial fibrillation, coronary artery disease and ischemic stroke by polygenic risk score tertiles. Adjusted for age, sex, ethnicity, body mass index, smoking, alcohol, hypertension, dyslipidemia, heart failure, peripheral artery disease, chronic kidney disease, end stage renal disease, physical activity, and economic status. Hazard ratios (HRs) are provided with 95% CIs. The vertical line indicates the reference value of 1.
Sensitivity analysis
In the sensitivity analysis, the results with PRS categorized as low (quintile 1), intermediate (quintile 2–4), or high (quintile 5) remained essentially unchanged (eFigure 3). The analyses on the European population did not indicate differential associations between HbA1c and all outcomes (eFigure 4–5). There were no significant interactions by sex in the association of HbA1c levels with AF or ischemic stroke, regardless of the PRS tertiles. However, the association between HbA1c levels and CAD showed significant interactions with sex, especially in the high PRS tertile (eFigure 6).
Discussion
Using a large-scale, population-based cohort of more than 300,000 individuals, we analyzed the association between HbA1c and cardiovascular disease in individuals with different PRSs for each outcome. Our major findings include the following: (i) PRS was associated with the risk of new-onset AF, CAD, and ischemic stroke. (ii) HbA1c > 6.5% was associated with a higher risk of CAD and ischemic stroke across all polygenic risk tertiles, but not with AF. In restricted cubic spline models, the presence of a gradual increase in the risk of CAD and ischemic stroke across HbA1c levels was evident, but a U-shaped trend was observed for AF in all polygenic risk tertiles. (iii) Diabetes status was also strongly associated with a higher risk of CAD and ischemic stroke across all polygenic risk tertiles, but not with AF. Our results suggest that the nature of the dose-dependent relationship between HbA1c levels and cardiovascular disease in individuals with different PRS is outcome-specific.
Glycemic status and cardiovascular disease
Previous studies have shown that chronic hyperglycemia, reflected by HbA1c levels, is associated with a higher risk of cardiovascular disease [20, 30, 31]. However, there are different associations between glycemic status and AF, CAD, and ischemic stroke. Eoin et al. [32] reported that higher HbA1c levels at the time of AF ablation increased post-ablation recurrence rates. The duration of diabetes and insulin use are associated with a higher risk of AF and an elevated thromboembolic risk in patients with AF [14, 15, 33, 34]. Zhang et al. [35] suggested diabetes is an independent risk factor for stroke recurrence among patients with ischemic stroke. Tight glucose control using insulin after an acute ischemic stroke is not associated with an improved prognosis [36]. Long-term insulin treatment did not improve survival in type 2 diabetic patients following myocardial infarction [37]. Shahim et al. [38] found that 2-hour plasma glucose value during a 75-g oral glucose tolerance test, but not HbA1c, added important prognostic information regarding future cardiovascular events. Also, mendelian randomization analyses support a causal link between diabetes and a higher risk of CAD and ischemic stroke but not AF [19, 39, 40].
Values of glycemic status in patient with different genetic traits
Although the performance of the PRS differs across cardiovascular diseases, a higher PRS of AF, CAD, or ischemic stroke has been found to be associated with an increased risk of new-onset AF, CAD, or ischemic stroke. However, it is unknown whether high HbA1c is associated with an increase in the risk of cardiovascular disease among individuals with different genetic susceptibilities for cardiovascular disease. In this study, HbA1c > 6.5% was significantly associated with an increased risk of CAD and ischemic stroke across all PRS tertiles. Our findings imply the strong potential benefits of lowering HbA1c levels to prevent cardiovascular diseases, regardless of PRS. The exact mechanisms underlying the association between HbA1c levels, PRS, and cardiovascular diseases are unknown. Several mechanisms may underlie the interaction between HbA1c and PRS. In this study, individuals with a higher PRS for cardiovascular diseases had more comorbidities. Recent studies have demonstrated that CAD, ischemic stroke and type 2 diabetes share a genetic background with each other and with their commonly associated risk factors [41]. Further studies are necessary to investigate the potential of optimal glycemic control based on PRS to prevent cardiovascular disease, as a randomized controlled trials demonstrated that statin therapy led to a greater relative risk reduction among individuals with high PRS of coronary heart disease [42].
Diabetes is a risk factor for the development of AF and may be related to its underlying pathogenesis, including oxidative stress, increased non-enzymatic glycosylation, structural and electrical remodeling, and autonomic dysfunction [43, 44]. Recent meta-analyses have reported an association between higher HbA1c levels and an increased risk of AF [18, 20]. However, in our study, the association between HbA1c levels and AF was insignificant in each PRS tertile. As the PRS increases, the effects of HbA1c on AF tend to decrease. The risk of AF associated with elevated HbA1c may appear to be mediated by diabetes-related comorbidities, such as hypertension and obesity [19, 45]. Likewise, several studies have suggested that low HbA1c is a marker of underlying diseases, such as hemoglobinopathy, chronic liver disease, cardiovascular mortality, and all-cause mortality [30, 46,47,48]. This hypothesis may be consistent with our results regarding the association between low HbA1c and increased risk of AF.
Strengths and limitations
The major strengths of this study were the use of a large-scale database with prospective ascertainment of outcomes and the validated PRS to facilitate subsequent research with reproducible findings. This study had several limitations. First, the UK Biobank participants were not representative of the general UK population. Due to healthy volunteer selection bias, participants differed in sociodemographic, lifestyle, and health-related characteristics from the general population [26]. However, a generalizable association between exposure and health conditions can be estimated using a sufficiently large number of participants with different levels of exposure. Second, the PRS was generated primarily based on GWAS data from individuals of European ancestry, which may be inappropriate for application to other racial and ethnic groups. Further GWAS data on individuals of non-European ancestry are needed to reduce the performance differences across ancestries. Third, there are differences in phenotype definitions between the study outcomes and the PRS. Nevertheless, in this study, the PRS has sufficient predictive performance. Fourth, the outcomes and comorbidities based on self-reported data might be susceptible to misclassification errors. These errors tend to be biased toward the null hypothesis and underestimate the association between exposure and outcomes. Finally, the trajectory of HbA1c levels during the follow-up period was not considered. Repeated exposure measurements over time may adequately represent the actual health-related conditions. Although individuals with HbA1c ≥ 15% were excluded to minimize the possibility of hemoglobinopathies, other conditions associated with falsely elevated or falsely lowered A1c were not excluded [29, 49].
Conclusion
Elevated HbA1c was associated with an increased risk of CAD and ischemic stroke across all polygenic risk tertiles. However, high HbA1c did not increased the risk of AF in patients with high PRS of AF. Our results suggest that the nature of the dose-dependent relationship between HbA1c levels and cardiovascular disease in individuals with different PRS is outcome-specific. This adds to the evidence that PRS may play a role together with glycemic status in the development of cardiovascular disease.
Data Availability
All researchers in academic, commercial and charitable settings can apply to use the UK Biobank resource for health-related research in the public interest (www.ukbiobank.ac.uk/registerapply/). Details for generating the PRS is available at https://www.medrxiv.org/content/https://doi.org/10.1101/2022.06.16.22276246v2.
Abbreviations
- AF:
-
Atrial fibrillation
- CAD:
-
Coronary artery disease
- HR:
-
Hazard ratios
- HbA1c:
-
Hemoglobin A1c
- PRS:
-
Polygenic risk score
References
Murray CJ, Barber RM, Foreman KJ, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 Diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. The Lancet. 2015;386(10009):2145–91.
Morrish N, Wang S-L, Stevens L, Fuller J, Keen H, Group WMS. Mortality and causes of death in the WHO multinational study of Vascular Disease in Diabetes. Diabetologia. 2001;44:14–S21.
Rao Kondapally Seshasai S, Kaptoge S, Thompson A, et al. Diabetes Mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364(9):829–41.
Khaw KT, Wareham N, Bingham S, Luben R, Welch A, Day N. Association of hemoglobin A1c with Cardiovascular Disease and mortality in adults: the European prospective investigation into cancer in Norfolk. Ann Intern Med. 2004;141(6):413–20.
Cavender MA, Scirica BM, Raz I, et al. Cardiovascular outcomes of patients in SAVOR-TIMI 53 by Baseline Hemoglobin A1c. Am J Med. 2016;129(3):340e341–348.
Lee WL, Cheung AM, Cape D, Zinman B. Impact of Diabetes on coronary artery Disease in women and men: a meta-analysis of prospective studies. Diabetes Care. 2000;23(7):962–8.
Mitsios JP, Ekinci EI, Mitsios GP, Churilov L, Thijs V. Relationship between glycated hemoglobin and Stroke risk: a systematic review and Meta-analysis. J Am Heart Assoc 2018;7(11).
Kim D, Yang PS, Jang E, et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am Heart J. 2018;202:20–6.
Kim D, Yang PS, Jang E, et al. Increasing trends in hospital care burden of atrial fibrillation in Korea, 2006 through 2015. Heart. 2018;104(24):2010–7.
Kim D, Yang PS, You SC, et al. Treatment timing and the effects of rhythm control strategy in patients with atrial fibrillation: nationwide cohort study. BMJ. 2021;373:n991.
Lee SS, Ae Kong K, Kim D, et al. Clinical implication of an impaired fasting glucose and prehypertension related to new onset atrial fibrillation in a healthy Asian population without underlying Disease: a nationwide cohort study in Korea. Eur Heart J. 2017;38(34):2599–607.
Lim YM, Yang PS, Jang E, et al. Body Mass Index variability and long-term risk of New-Onset Atrial Fibrillation in the General Population: a Korean Nationwide Cohort Study. Mayo Clin Proc. 2019;94(2):225–35.
Kim J, Kim D, Jang E et al. Associations of high-normal blood pressure and impaired fasting glucose with atrial fibrillation. Heart 2023.
Dublin S, Glazer NL, Smith NL, et al. Diabetes Mellitus, glycemic control, and risk of atrial fibrillation. J Gen Intern Med. 2010;25(8):853–8.
Liou YS, Yang FY, Chen HY, Jong GP. Antihyperglycemic Drugs use and new-onset atrial fibrillation: a population-based nested case control study. PLoS ONE. 2018;13(8):e0197245.
Nichols GA, Reinier K, Chugh SS. Independent contribution of Diabetes to increased prevalence and incidence of atrial fibrillation. Diabetes Care. 2009;32(10):1851–6.
Schoen T, Pradhan AD, Albert CM, Conen D. Type 2 Diabetes Mellitus and risk of incident atrial fibrillation in women. J Am Coll Cardiol. 2012;60(15):1421–8.
Qi W, Zhang N, Korantzopoulos P, et al. Serum glycated hemoglobin level as a predictor of atrial fibrillation: a systematic review with meta-analysis and meta-regression. PLoS ONE. 2017;12(3):e0170955.
Harati H, Zanetti D, Rao A, et al. No evidence of a causal association of type 2 Diabetes and glucose metabolism with atrial fibrillation. Diabetologia. 2019;62(5):800–4.
Zhao H, Liu M, Chen Z, Mei K, Yu P, Xie L. Dose-response analysis between hemoglobin A1c and risk of atrial fibrillation in patients with and without known Diabetes. PLoS ONE. 2020;15(2):e0227262.
Roselli C, Chaffin MD, Weng LC, et al. Multi-ethnic genome-wide association study for atrial fibrillation. Nat Genet. 2018;50(9):1225–33.
Nelson CP, Goel A, Butterworth AS, et al. Association analyses based on false discovery rate implicate new loci for coronary artery Disease. Nat Genet. 2017;49(9):1385–91.
Bevan S, Traylor M, Adib-Samii P, et al. Genetic heritability of ischemic Stroke and the contribution of previously reported candidate gene and genomewide associations. Stroke. 2012;43(12):3161–7.
Polygenic Risk Score Task Force of the International Common Disease A. Responsible use of polygenic risk scores in the clinic: potential benefits, risks and gaps. Nat Med. 2021;27(11):1876–84.
Thompson DJ, Wells D, Selzam S, et al. UK Biobank release and systematic evaluation of optimised polygenic risk scores for 53 Diseases and quantitative traits. MedRxiv. 2022. 2022.2006. 2016.22276246.
Fry A, Littlejohns TJ, Sudlow C, et al. Comparison of Sociodemographic and Health-related characteristics of UK Biobank participants with those of the General Population. Am J Epidemiol. 2017;186(9):1026–34.
Elliott P, Peakman TC, Biobank UK. The UK Biobank sample handling and storage protocol for the collection, processing and archiving of human blood and urine. Int J Epidemiol. 2008;37(2):234–44.
Geistanger A, Arends S, Berding C, et al. Statistical methods for monitoring the relationship between the IFCC reference measurement procedure for hemoglobin A1c and the designated comparison methods in the United States, Japan, and Sweden. Clin Chem. 2008;54(8):1379–85.
American Diabetes Association Professional Practice C. 2. Classification and diagnosis of Diabetes: standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Suppl 1):17–S38.
Selvin E, Steffes MW, Zhu H, et al. Glycated hemoglobin, Diabetes, and cardiovascular risk in nondiabetic adults. N Engl J Med. 2010;362(9):800–11.
Selvin E, Coresh J, Shahar E, Zhang L, Steffes M, Sharrett AR. Glycaemia (haemoglobin A1c) and incident ischaemic Stroke: the Atherosclerosis risk in communities (ARIC) Study. Lancet Neurol. 2005;4(12):821–6.
Donnellan E, Aagaard P, Kanj M, et al. Association between Pre-ablation Glycemic Control and outcomes among patients with Diabetes undergoing Atrial Fibrillation ablation. JACC Clin Electrophysiol. 2019;5(8):897–903.
Ashburner JM, Go AS, Chang Y, et al. Effect of Diabetes and Glycemic Control on ischemic Stroke risk in AF patients: ATRIA Study. J Am Coll Cardiol. 2016;67(3):239–47.
Patti G, Lucerna M, Cavallari I, et al. Insulin-requiring Versus Noninsulin-requiring Diabetes and thromboembolic risk in patients with Atrial Fibrillation: PREFER in AF. J Am Coll Cardiol. 2017;69(4):409–19.
Zhang L, Li X, Wolfe CDA, O’Connell MDL, Wang Y. Diabetes as an Independent risk factor for Stroke recurrence in ischemic Stroke patients: an updated Meta-analysis. Neuroepidemiology. 2021;55(6):427–35.
Cerecedo-Lopez CD, Cantu-Aldana A, Patel NJ, Aziz-Sultan MA, Frerichs KU, Du R. Insulin in the management of Acute ischemic Stroke: a systematic review and Meta-analysis. World Neurosurg. 2020;136:e514–34.
Malmberg K, Ryden L, Wedel H, et al. Intense metabolic control by means of insulin in patients with Diabetes Mellitus and acute Myocardial Infarction (DIGAMI 2): effects on mortality and morbidity. Eur Heart J. 2005;26(7):650–61.
Shahim B, De Bacquer D, De Backer G, et al. The Prognostic Value of Fasting plasma glucose, two-hour postload glucose, and HbA(1c) in patients with coronary artery Disease: a Report from EUROASPIRE IV: a Survey from the European Society of Cardiology. Diabetes Care. 2017;40(9):1233–40.
Leong A, Chen J, Wheeler E, et al. Mendelian randomization analysis of Hemoglobin A(1c) as a risk factor for coronary artery Disease. Diabetes Care. 2019;42(7):1202–8.
Larsson SC, Scott RA, Traylor M, et al. Type 2 Diabetes, glucose, insulin, BMI, and ischemic Stroke subtypes: mendelian randomization study. Neurology. 2017;89(5):454–60.
Strawbridge RJ, van Zuydam NR. Shared Genetic Contribution of type 2 Diabetes and Cardiovascular Disease: implications for prognosis and treatment. Curr Diab Rep. 2018;18(8):59.
Natarajan P, Young R, Stitziel NO, et al. Polygenic risk score identifies Subgroup with higher burden of Atherosclerosis and greater relative benefit from statin therapy in the primary Prevention setting. Circulation. 2017;135(22):2091–101.
Koektuerk B, Aksoy M, Horlitz M, Bozdag-Turan I, Turan RG. Role of Diabetes in heart rhythm disorders. World J Diabetes. 2016;7(3):45–9.
Wang A, Green JB, Halperin JL, Piccini JP. Sr. Atrial Fibrillation and Diabetes Mellitus: JACC Review topic of the Week. J Am Coll Cardiol. 2019;74(8):1107–15.
Chatterjee NA, Giulianini F, Geelhoed B, et al. Genetic Obesity and the risk of Atrial Fibrillation: causal estimates from mendelian randomization. Circulation. 2017;135(8):741–54.
Aggarwal V, Schneider AL, Selvin E. Low hemoglobin A(1c) in nondiabetic adults: an elevated risk state? Diabetes Care. 2012;35(10):2055–60.
Carson AP, Fox CS, McGuire DK, et al. Low hemoglobin A1c and risk of all-cause mortality among US adults without Diabetes. Circ Cardiovasc Qual Outcomes. 2010;3(6):661–7.
Raghavan S, Vassy JL, Ho YL, et al. Diabetes Mellitus-Related all-cause and Cardiovascular Mortality in a national cohort of adults. J Am Heart Assoc. 2019;8(4):e011295.
Radin MS. Pitfalls in hemoglobin A1c measurement: when results may be misleading. J Gen Intern Med. 2014;29(2):388–94.
Acknowledgements
The UK Biobank provided the database used in this study. The authors thank the UK Biobank for their cooperation. The authors also thank UK Biobank participants that made this study possible.
Funding
This research was supported by a grant from the Patient-Centered Clinical Research Coordinating Centre (PACEN) funded by the Ministry of Health & Welfare, Republic of Korea (HC19C0130). The funders had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
JK, and DK developed the study design, wrote the manuscript, and analyzed and interpreted the data. H-JB, B-EP, TSK, and S-HL analyzed and interpreted the data and contributed to the discussion. SYL, YHC, and JWR interpreted the results and revised the manuscript. M-YL, P-SY, and BJ interpreted the results, contributed to the discussion, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
UK Biobank received ethical approval from the Northwest Multicenter Research Ethics Committee. The UK Biobank data are available to researchers after acceptance of the research proposal to the UK Biobank. Written informed consent was obtained from all the participants during recruitment. This study was approved by the Institutional Review Board of Yonsei University Health System (4-2023-0323).
Consent for publication
Not applicable.
Competing interests
BJ has served as a speaker for Bayer, BMS/Pfizer, Medtronic, and Daiichi-Sankyo and has received research funds from Medtronic and Abbott. BJ received no fees, either directly or personally. The remaining authors have no other relationships or activities that could have influenced the submitted work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kim, J., Kim, D., Bae, HJ. et al. Associations of combined polygenic risk score and glycemic status with atrial fibrillation, coronary artery disease and ischemic stroke. Cardiovasc Diabetol 23, 5 (2024). https://doi.org/10.1186/s12933-023-02021-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-02021-0