
Abstract
Background
We assessed the impact of 24 months of treatment with ipragliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, on endothelial function in patients with type 2 diabetes as a sub-analysis of the PROTECT study.
Methods
In the PROTECT study, patients were randomized to receive either standard antihyperglycemic treatment (control group, n = 241 ) or add-on ipragliflozin treatment (ipragliflozin group, n = 241) in a 1:1 ratio. Among the 482 patients in the PROTECT study, flow-mediated vasodilation (FMD) was assessed in 32 patients in the control group and 26 patients in the ipragliflozin group before and after 24 months of treatment.
Results
HbA1c levels significantly decreased after 24 months of treatment compared to the baseline value in the ipragliflozin group, but not in the control group. However, there was no significant difference between the changes in HbA1c levels in the two groups (7.4 ± 0.8% vs. 7.0 ± 0.9% in the ipragliflozin group and 7.4 ± 0.7% vs. 7.3 ± 0.7% in the control group; P = 0.08). There was no significant difference between FMD values at baseline and after 24 months in both groups (5.2 ± 2.6% vs. 5.2 ± 2.6%, P = 0.98 in the ipragliflozin group; 5.4 ± 2.9% vs. 5.0 ± 3.2%, P = 0.34 in the control group). There was no significant difference in the estimated percentage change in FMD between the two groups (P = 0.77).
Conclusions
Over a 24-month period, the addition of ipragliflozin to standard therapy in patients with type 2 diabetes did not change endothelial function assessed by FMD in the brachial artery.
Trial registration
Registration Number for Clinical Trial: jRCT1071220089 (https://jrct.niph.go.jp/en-latest-detail/jRCT1071220089).
Similar content being viewed by others

Introduction
Sodium glucose cotransporter 2 (SGLT2) inhibitors are oral glucose medicines that lower glucose levels by reducing the renal reabsorption of glucose. Some meta-analyses and large clinical trials have shown that SGLT2 inhibitors reduce cardiovascular events in patients with type 2 diabetes and reduced the rate of hospitalization for heart failure in patients with heart failure [1,2,3,4,5,6,7,8,9,10]. Inzucchi et al. [11] showed that changes in hematocrit and hemoglobin levels in the EMPA-REG OUTCOME trial might be major mediators of empagliflozin-induced decreases in the incidence of cardiovascular events. SGLT2 inhibitors induce diuresis and glycosuria to decrease the intravascular volume and lower the cardiac preload and afterload, which consequently increase the cardiac output. These impacts of SGLT2 inhibitors may lead to improvements in endothelial function. Unfortunately, the effect of long-term treatment with SGLT2 inhibitors on endothelial function in patients with type 2 diabetes is still unclear.
Endothelial dysfunction is regarded as the first stage in the etiology of atherosclerosis and plays a significant role in the progression of atherosclerosis, leading to cardiovascular issues [12, 13]. Measurements of flow-mediated vasodilation (FMD) have been widely used as an indication of endothelial function in the brachial artery [14, 15]. Several studies have shown that endothelial dysfunction predicts cardiovascular events [16, 17].
The PROTECT study was a multicenter prospective study designed to test the inhibitory impact of an SGLT2 inhibitor on the development of atherosclerosis based on intima-media thickness over a 24-month follow-up period [18, 19]. FMD of the brachial artery was assessed in some participants. The present study’s purpose, which was a sub-analysis of the PROTECT study, was to determine the impacts of 24 months of treatment using SGLT2 inhibitors on endothelial function as measured by FMD in the brachial artery in patients with type 2 diabetes.
Methods
Study design and patients
The rationale and design of the PROTECT study (University Hospital Medical Information Network Center: ID000018440) have already been explained [18]. In brief, the PROTECT study was a multicenter, prospective, randomized, open-label, blinded-endpoint investigator-initiated clinical trial in which 39 Japanese institutions that participated in patients with HbA1c levels of 6.0–10.0% despite conventional treatment with diet, exercise, and/or pharmacological therapy with prescribed diabetic drugs for more than 3 months before randomization were eligible for the study if they were at least 20 years old and had type 2 diabetes. Patients who had taken an SGLT2 inhibitor one month before randomization were excluded. The other exclusion criteria have been described elsewhere [18].
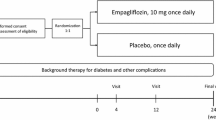
Between September 2015 and June 2018, 488 patients with type 2 diabetes were enrolled, and 482 patients were randomized to receive either standard antihyperglycemic treatment (control group, n = 241) or add-on ipragliflozin treatment (ipragliflozin group, n = 241) at a 1:1 ratio (Fig. 1). The treatment randomization was conducted on the basis of age (< 65 or ≥ 65 years), HbA1c level (< 7% or ≥ 7%), office systolic blood pressure (< 135 or ≥ 135 mm Hg), use of statins, and use of metformin at the time of screening [18]. Patients in the ipragliflozin group were initiated with ipragliflozin at a dose of 50 mg daily. If a personalized goal in accordance with the official recommendations regarding HbA1c levels from the Japan Diabetes Society was not achieved, the dose of ipragliflozin was increased to 100 mg daily, and the background treatment for participants in the control group continued. The background therapy for the participants remained unaltered in both groups throughout the trial, within the acceptable limits of the therapeutic goal. If the personalized goal was not achieved, antihyperglycemic agents other than SGLT2 inhibitors and/or insulin were administered to both groups. However, because pioglitazone has a suppressive effect on the progression of intima-media thickness (IMT) [20], the prescription of pioglitazone or a change in its dose was prohibited during the study. All patients were followed up for 24 months after starting the study protocol.

Flow diagram of participants in the PROTECT study
In the PROTECT study, the primary endpoint in the main analysis was the change in the mean common carotid artery IMT from baseline to 24 months after the start of treatment; the results have already been reported [19]. The main objective of the present sub-analysis of the change in FMD in the brachial artery from baseline to 24 months after the start of treatment was to analyze one of the prespecified secondary endpoints [18]. FMD of the brachial artery was assessed at some participating institutions as an additional examination.
Of the 488 patients, serial FMD measurements were performed in 32 patients in the control group and 26 patients in the ipragliflozin group before and after 24 months of treatment (Fig. 1). In the present study, data from 58 patients from six institutions were examined. The study protocol for this sub-analysis was approved by the Ethics Committee of Saga University Hospital (2022-09-02) and registered (jRCT1071220089). All the individuals provided written informed consent to participate in the study. All methods were performed in accordance with the Declaration of Helsinki and relevant guidelines and regulations in Japan.
FMD measurement protocol
After overnight fasting, all experiments were conducted in the morning. All of the patients were kept in the supine position in a calm, dark, air-conditioned room with a constant temperature of 22 ℃–25 ℃ throughout the study. A 23-gauge polyethylene catheter was placed in the left deep antecubital vein to collect blood samples. Endothelium-dependent FMD was assessed based on the vascular response to reactive hyperemia in the brachial artery. Observers were blinded to the examinations.
FMD was measured using the same ultrasound device designed for FMD measurements and the same protocol in all institutions. A high-resolution linear artery transducer was coupled to computer-assisted analysis software (UNEXEF18G, UNEX Co, Nagoya, Japan), which uses an automated edge detection system for the measurement of brachial artery diameter [21]. A blood pressure cuff was placed around the forearm. The brachial artery was scanned longitudinally 5–10 cm above the elbow. When the clearest B-mode image of the anterior and posterior intimal interfaces between the lumen and the vessel wall was obtained, the transducer was held at the same point throughout the scan using a special probe holder (UNEX Co.) to ensure image consistency. The depth and gain were set to optimize the images of the arterial lumen wall interface. When the tracking gate was placed on the intima, the artery diameter was automatically tracked, and the waveform of the diameter changed over the cardiac cycle was displayed in real-time using the FMD mode of the tracking system. This allowed the ultrasound images to be optimized at the start of the scan, and the transducer position to be adjusted immediately for optimal tracking performance throughout the scan. Pulsed Doppler flow was assessed at baseline and during peak hyperemic flow, which was confirmed to occur within 15 s after cuff deflation. The blood flow velocity was calculated from color Doppler data and displayed as a waveform in real time. Baseline longitudinal images of the artery were acquired for 30 s, and the blood pressure cuff was inflated to 50 mmHg above the systolic pressure for 5 min. Longitudinal images of the artery were recorded continuously for 5 min after cuff deflation. Pulsed Doppler velocity signals were obtained for 20 s at baseline and 10 s immediately after cuff deflation. Changes in the brachial artery diameter were immediately expressed as percentage changes relative to the vessel diameter before cuff inflation. FMD was automatically calculated as the percentage change in the peak vessel diameter from the baseline value. The percentage of FMD [(peak diameter–baseline diameter)/baseline diameter] was used for the analysis. The blood flow volume was calculated by multiplying the Doppler flow velocity (corrected for the angle) with the heart rate and vessel cross-sectional area (r2). Reactive hyperemia was calculated as the maximum percentage increase in flow after cuff deflation compared with the baseline flow. In our laboratory, the inter- and intra-coefficients of variation for the brachial artery diameter were 1.6% and 1.4%, respectively, in our laboratory [22].
Statistical analysis
Results are presented as means ± SD. Statistical significance was defined as a probability value < 0.05, and all stated probability values were two-sided. The chi-square test was used to compare categorical variables and an unpaired Student’s t-test was used to compare the mean values of continuous variables between the groups. A paired Student’s t-test was used to assess the differences in the mean values of continuous variables between baseline and 24 months. A linear regression model was used to estimate the changes in FMD over time by treatment (control vs. ipragliflozin group). To estimate the group differences in the percentage changes in FMD, the models included treatment, age, sex, and baseline FMD. Data were processed using R 4.0.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline clinical characteristics
The baseline clinical characteristics of all patients are shown in Table 1, along with the impacts of each therapy on baseline variables in the ipragliflozin and control groups. Of the 58 patients, 39 (67.2%) were men, and 19 (32.8%) were women. Nine patients (15.5%) were current smokers, 37 (63.8%) had hypertension, 28 (48.3%) had dyslipidemia, 22 (37.9%) had atherosclerotic cardiovascular disease, and 4 (6.9%) had a previous stroke.
The mean fasting plasma glucose level was 8.25 ± 1.31 mmol/L and mean HbA1c was 7.4 ± 0.7%. The mean value of FMD was 5.3 ± 2.7%. None of the variables, except high-density lipoprotein (HDL) cholesterol, showed significant differences between the two groups.
Changes in clinical characteristics after 24 months
In the ipragliflozin group, body mass index was significantly decreased after 24 months (28.4 ± 3.8 vs. 26.7 ± 3.8 kg/m2; P < 0.01) and HDL was significantly increased after 24 months (1.12 ± 0.26 vs. 1.20 ± 0.20 mmol/L; P = 0.03). In the control group, total cholesterol and low-density lipoprotein (LDL) cholesterol were significantly decreased after 24 months (4.61 ± 0.55 vs. 4.32 ± 0.87 mmol/L for total cholesterol and 2.62 ± 0.69 vs. 2.40 ± 0.55 mmol/L for LDL; P = 0.01 and P = 0.04, respectively). No significant differences were observed in any other variables after 24 months in either group. The total cholesterol and LDL cholesterol levels after 24 months were significantly higher in the ipragliflozin group than in the control group. The body mass index and estimated glomerular filtration rate after 24 months were significantly lower in the ipragliflozin group than in the control group.
Glycemic control
The baseline HbA1c and fasting plasma glucose levels were comparable between the two groups. The HbA1c level significantly decreased after 24 months of treatment compared to the baseline value in the ipragliflozin group (7.4 ± 0.8% vs. 7.0 ± 0.9%; P < 0.01), but not in the control group (7.4 ± 0.7% vs. 7.3 ± 0.7%; P = 0.27). However, there was no significant difference between changes in HbA1c levels in the two groups (7.4 ± 0.8% vs. 7.0% ± 0.9% in the ipragliflozin group and 7.4 ± 0.7% vs. 7.3 ± 0.7% in the control group; P = 0.08 Table 1). There was no significant difference in the fasting plasma glucose levels between the two groups during the study period.
Endothelial function
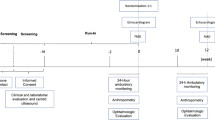
Figure 2 shows the impacts of glycemic management on FMD after 24 months of treatment in the ipragliflozin and control groups. Baseline FMD values were comparable between the two groups. There was no significant difference between FMD values at baseline and after 24 months in either group (5.2 ± 2.6% vs. 5.2 ± 2.6%, P = 0.98 in the ipragliflozin group and 5.4 ± 2.9% vs. 5.0 ± 3.2%, P = 0.34 in the control group). There was no significant difference in the estimated percentage change in FMD between the two groups (P = 0.77).

Changes in estimated percentage change in flow-mediated vasodilation (FMD) in the ipragliflozin group and the control group. The mixed-effects model included treatment, age, sex, and FMD at baseline
Discussion
The present study demonstrated that adding ipragliflozin to standard therapy for 24 months in patients with type 2 diabetes did not change endothelial function as measured by FMD in the conduit brachial artery.
Impact of SGLT2 inhibitors on FMD
The short-term impacts of SGLT2 inhibitors on the vascular function in patients with type 2 diabetes are controversially reported [23,24,25]. The DEFENCE study, a randomized, open-label, blinded-endpoint, parallel-group, comparative clinical trial, showed that dapagliflozin add-on therapy with metformin for four months improved FMD in patients with type 2 diabetes [23]. Sposito et al. [24] showed that 12 weeks of dapagliflozin add-on therapy to metformin improved FMD in patients with type 2 diabetes. Conversely, Zainordin et al. [25] showed that 12 weeks of dapagliflozin add-on therapy to metformin and insulin did not alter FMD, and that there was no significant difference in FMD between the control and dapagliflozin groups. Sposito et al. [26] showed that 16-week treatment with empagliflozin did not alter FMD. The EMBLEM trial, a multicenter, randomized, placebo-controlled, double-blind trial, showed that empagliflozin administered for 24 weeks did not alter the reactive hyperemia peripheral arterial tonometry index as an indication of endothelial function in patients with type 2 diabetes [27]. These findings suggest that the impacts of short-term dapagliflozin administration on endothelial function remain unclear. In addition, the long-term impacts of dapagliflozin on endothelial function remain unclear. The present study showed that 24 months of ipragliflozin treatment did not alter FMD in patients with type 2 diabetes.
Impact of SGLT2 inhibitors on endothelial function
Several clinical trials have shown that SGLT2 inhibitors can prevent cardiovascular events in patients with type 2 diabetes and heart failure [4,5,6,7,8,9,10]. In addition, a meta-analysis revealed that SGLT2 inhibitors prevent major adverse cardiovascular events in patients with type 2 diabetes [1,2,3]. Suzuki et al. [28] showed that the cardiovascular risk associated with individual SGLT2 inhibitors in patients with type 2 diabetes was comparable, based on large-scale real-world data. These findings suggest that SGLT2 inhibitors exert anti-atherosclerotic impacts. However, the exact mechanisms underlying the anti-atherosclerotic impacts of SGLT2 inhibitors remain unclear. It has been postulated that one of the anti-atherosclerotic impacts of SGLT2 inhibitors is improvement of endothelial function. Several investigators have shown that SGLT2 inhibitors improve nitric oxide (NO) bioavailability by inhibiting inflammatory reactions and decreasing oxidative stress [29,30,31]. Salim et al. [32] showed that ipragliflozin improves endothelial function in diabetic mice through enhancement of phosphorylation of Akt and endothelial NO synthase and reduced urinary excretion of 8-hydroxy-2’-deoxyguanosine as an index of oxidative stress. D’Onofrio et al. [33] showed that treatment with SGLT2 inhibitors improved plaque stability and decreased 2-year outcomes in diabetic patients, potentially by modulating the SGLT2/SIRT6 pathway. Ripoll et al. [34] showed that the beneficial effects of dapagliflozin on endothelial barrier integrity are mediated through a critical downstream link involving the apolipoprotein M/sphingosine-1-phosphate pathway. However, in the present study, ipragliflozin did not alter FMD in patients with type 2 diabetes.
Study limitations
This study has some limitations. First, the number of subjects in the present study, as a sub-analysis of the PROTECT trial, was relatively small. Because FMD was an optional measurement in the PROTECT trial, there was an insufficient sample size for power calculation, and the analysis may have been underpowered. However, the results of analysis of the PROTECT trial, a multicenter, prospective, randomized, open-label, and blinded-endpoint investigator-initiated clinical trial, provide valuable information that may help us to understand the impact of ipragliflozin on endothelial function in patients with type 2 diabetes. Further studies with a larger number of participants are required to validate the long-term impacts of SGLT2 inhibitors on endothelial function in patients with type 2 diabetes. Second, LDL cholesterol levels in the control group after 24 months were significantly lower than those in the ipragliflozin group after 24 months, although there was no change in the use of dyslipidemia-improving drugs, including statins, ezetimibe, fibrates, and eicosapentaenoic acid, in either group. Lowering LDL cholesterol levels improves vascular endothelial function. The lower LDL cholesterol level in the control group at 24 months may have been one reason for the lack of a significant difference in FMD between the two groups. However, there was no significant difference in FMD between the two groups after adjusting for LDL cholesterol.
Conclusion
Over a 24-month period, the addition of ipragliflozin to standard therapy in patients with type 2 diabetes did not change the endothelial function assessed by FMD in the brachial artery.
Availability of data and materials
The data are available upon reasonable request from researchers who submit a detailed proposal outlining their intended use of the data and after approval by the principal investigators and steering committee of the PROTECT study. Inquiries must be addressed to the corresponding author (or the study secretariat: substudy_protect@clin-med.org).
Abbreviations
- FMD:
-
Flow-mediated vasodilation
- HDL:
-
High-density lipoprotein
- IMT:
-
Intima-media thickness
- LDL:
-
Low-density lipoprotein
- NO:
-
Nitric oxide
- SGLT2:
-
Sodium-glucose cotransporter 2
References
Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Furtado RHM, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019;393(10166):31–9.
McGuire DK, Shih WJ, Cosentino F, Charbonnel B, Cherney DZI, Dagogo-Jack S, Pratley R, Greenberg M, Wang S, Huyck S, et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: a meta-analysis. JAMA Cardiol. 2021;6(2):148–58.
Arnott C, Li Q, Kang A, Neuen BL, Bompoint S, Lam CSP, Rodgers A, Mahaffey KW, Cannon CP, Perkovic V, et al. Sodium-glucose cotransporter 2 inhibition for the prevention of cardiovascular events in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. J Am Heart Association. 2020;9(3):e014908.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–28.
Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, Januzzi J, Verma S, Tsutsui H, Brueckmann M, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–24.
Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, Brunner-La Rocca HP, Choi DJ, Chopra V, Chuquiure-Valenzuela E, et al. Empagliflozin in Heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–61.
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR. Canagliflozin and Cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–57.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, et al. Dapagliflozin and Cardiovascular Outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Bělohlávek J, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008.
Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, Inzucchi SE, Kosiborod MN, Lam CSP, Martinez F, et al. Dapagliflozin in Heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387(12):1089–98.
Inzucchi SE, Zinman B, Fitchett D, Wanner C, Ferrannini E, Schumacher M, Schmoor C, Ohneberg K, Johansen OE, George JT, et al. How does Empagliflozin reduce Cardiovascular Mortality? Insights from a mediation analysis of the EMPA-REG OUTCOME Trial. Diabetes Care. 2018;41(2):356–63.
Ross R. Atherosclerosis–an inflammatory disease. N Engl J Med. 1999;340(2):115–26.
Higashi Y, Noma K, Yoshizumi M, Kihara Y. Endothelial function and oxidative stress in cardiovascular diseases. Circ J. 2009;73(3):411–8.
Benjamin EJ, Larson MG, Keyes MJ, Mitchell GF, Vasan RS, Keaney JF Jr, Lehman BT, Fan S, Osypiuk E, Vita JA. Clinical correlates and heritability of flow-mediated dilation in the community: the Framingham Heart Study. Circulation. 2004;109(5):613–9.
Kishimoto S, Maruhashi T, Kajikawa M, Harada T, Yamaji T, Han Y, Mizobuchi A, Hashimoto Y, Yoshimura K, Nakano Y, et al. White blood cell count is not associated with flow-mediated vasodilation or nitroglycerine-induced vasodilation. Sci Rep. 2022;12(1):8201.
Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI, Sullivan ID, Lloyd JK, Deanfield JE. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992;340(8828):1111–5.
Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, Deanfield J, Drexler H, Gerhard-Herman M, Herrington D, et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial artery reactivity Task Force. J Am Coll Cardiol. 2002;39(2):257–65.
Tanaka A, Murohara T, Taguchi I, Eguchi K, Suzuki M, Kitakaze M, Sato Y, Ishizu T, Higashi Y, Yamada H, et al. Rationale and design of a multicenter randomized controlled study to evaluate the preventive effect of ipragliflozin on carotid atherosclerosis: the PROTECT study. Cardiovasc Diabetol. 2016;15(1):133.
Tanaka A, Sata M, Okada Y, Teragawa H, Eguchi K, Shimabukuro M, Taguchi I, Matsunaga K, Kanzaki Y, Yoshida H, et al. Effect of ipragliflozin on carotid intima-media thickness in patients with type 2 diabetes: a multicenter, randomized, controlled trial. Eur Heart J Cardiovasc pharmacotherapy. 2023;9(2):165–72.
Mazzone T, Meyer PM, Feinstein SB, Davidson MH, Kondos GT, D’Agostino RB, Sr., Perez A, Provost JC, Haffner SM. Effect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes: a randomized trial. JAMA. 2006;296(21):2572–81.
Maruhashi T, Soga J, Fujimura N, Idei N, Mikami S, Iwamoto Y, Kajikawa M, Matsumoto T, Hidaka T, Kihara Y, et al. Nitroglycerine-induced vasodilation for assessment of vascular function: a comparison with flow-mediated vasodilation. Arterioscler Thromb Vasc Biol. 2013;33(6):1401–8.
Kishimoto S, Kajikawa M, Maruhashi T, Iwamoto Y, Matsumoto T, Iwamoto A, Oda N, Matsui S, Hidaka T, Kihara Y, et al. Endothelial dysfunction and abnormal vascular structure are simultaneously present in patients with heart failure with preserved ejection fraction. Int J Cardiol. 2017;231:181–7.
Shigiyama F, Kumashiro N, Miyagi M, Ikehara K, Kanda E, Uchino H, Hirose T. Effectiveness of dapagliflozin on vascular endothelial function and glycemic control in patients with early-stage type 2 diabetes mellitus: DEFENCE study. Cardiovasc Diabetol. 2017;16(1):84.
Sposito AC, Breder I, Soares AAS, Kimura-Medorima ST, Munhoz DB, Cintra RMR, Bonilha I, Oliveira DC, Breder JC, Cavalcante P, et al. Dapagliflozin effect on endothelial dysfunction in diabetic patients with atherosclerotic disease: a randomized active-controlled trial. Cardiovasc Diabetol. 2021;20(1):74.
Zainordin NA, Hatta S, Mohamed Shah FZ, Rahman TA, Ismail N, Ismail Z, Abdul Ghani R. Effects of Dapagliflozin on endothelial dysfunction in type 2 diabetes with established ischemic heart disease (EDIFIED). J Endocr Soc. 2020;4(1):bvz017.
Sposito AC, Breder I, Barreto J, Breder J, Bonilha I, Lima M, Oliveira A, Wolf V, Luchiari B, do Carmo HR, et al. Evolocumab on top of empagliflozin improves endothelial function of individuals with diabetes: randomized active-controlled trial. Cardiovasc Diabetol. 2022;21(1):147.
Tanaka A, Shimabukuro M, Machii N, Teragawa H, Okada Y, Shima KR, Takamura T, Taguchi I, Hisauchi I, Toyoda S, et al. Effect of Empagliflozin on endothelial function in patients with type 2 diabetes and Cardiovascular Disease: results from the Multicenter, Randomized, Placebo-Controlled, double-blind EMBLEM Trial. Diabetes Care. 2019;42(10):e159–61.
Suzuki Y, Kaneko H, Okada A, Itoh H, Matsuoka S, Fujiu K, Michihata N, Jo T, Takeda N, Morita H, et al. Comparison of cardiovascular outcomes between SGLT2 inhibitors in diabetes mellitus. Cardiovasc Diabetol. 2022;21(1):67.
Park SH, Belcastro E, Hasan H, Matsushita K, Marchandot B, Abbas M, Toti F, Auger C, Jesel L, Ohlmann P, et al. Angiotensin II-induced upregulation of SGLT1 and 2 contributes to human microparticle-stimulated endothelial senescence and dysfunction: protective effect of gliflozins. Cardiovasc Diabetol. 2021;20(1):65.
Uthman L, Homayr A, Juni RP, Spin EL, Kerindongo R, Boomsma M, Hollmann MW, Preckel B, Koolwijk P, van Hinsbergh VWM, et al. Empagliflozin and Dapagliflozin reduce ROS Generation and restore NO bioavailability in Tumor necrosis factor α-Stimulated human coronary arterial endothelial cells. Cell Physiol Biochem. 2019;53(5):865–86.
Khemais-Benkhiat S, Belcastro E, Idris-Khodja N, Park SH, Amoura L, Abbas M, Auger C, Kessler L, Mayoux E, Toti F, et al. Angiotensin II-induced redox-sensitive SGLT1 and 2 expression promotes high glucose-induced endothelial cell senescence. J Cell Mol Med. 2020;24(3):2109–22.
Salim HM, Fukuda D, Yagi S, Soeki T, Shimabukuro M, Sata M. Glycemic Control with Ipragliflozin, a Novel Selective SGLT2 inhibitor, ameliorated endothelial dysfunction in Streptozotocin-Induced Diabetic mouse. Front Cardiovasc Med. 2016;3:43.
D’Onofrio N, Sardu C, Trotta MC, Scisciola L, Turriziani F, Ferraraccio F, Panarese I, Petrella L, Fanelli M, Modugno P, et al. Sodium-glucose co-transporter2 expression and inflammatory activity in diabetic atherosclerotic plaques: Effects of sodium-glucose co-transporter2 inhibitor treatment. Mol Metabolism. 2021;54:101337.
Ripoll CV, Guo Z, Kumari T, Girardi A, Diab A, Ozcan M, He L, Oscarsson J, Esterline R, Schilling J, et al. Dapagliflozin improves endothelial integrity and cardiac loading through a sphingosine-a-phosphate / apolipoprotein M dependent pathway. J Card Fail. 2022;28(Suppl):S3.
Acknowledgements
The authors thank all the participants, investigators, board members, and medical staff involved in the RPOTECT study. The authors are also grateful to the members of the Data and Safety Monitoring Board: Munehide Matsuhisa, MD, PhD (Tokushima University Graduate School, Tokushima, Japan), Junya Ako, MD, PhD, (Kitasato University, Sagamihara, Japan), Yoshimasa Aso, MD, PhD (Dokkyo Medical University, Mibu, Japan), Masaharu Ishihara, MD, PhD (Hyogo College of Medicine, Nishinomiya, Japan), Kazuo Kitagawa, MD, PhD (Tokyo Women’s Medical University, Tokyo, Japan), and Akira Yamashina, MD, PhD (Kiryu University, Midori, Japan). Protect study investigators and organization:Principal Investigators: Koichi Node, MD, PhD (Saga University, Saga, Japan) and Toyoaki Murohara, MD, PhD (Nagoya University, Naogya, Japan). Masafumi Kitakaze, MD, PhD (Hanwa Daini Senboku Hospital, Sakai, Japan). Steering Committee: Yoshihiko Nishio, MD, PhD (Kagoshima University, Kagoshima, Japan), Teruo Inoue, MD, PhD (Dokkyo Medical University, Mibu, Japan), Mitsuru Ohishi, MD, PhD (Kagoshima University, Kagoshima, Japan), Kazuomi Kario, MD, PhD (Jichi Medical University School of Medicine, Shimotsuke, Japan), Masataka Sata, MD, PhD (Tokushima University Graduate School, Tokushima, Japan), Michio Shimabukuro, MD, PhD (Fukushima Medical University, Fukushima, Japan), Wataru Shimizu, MD, PhD (Nippon Medical School, Tokyo, Japan), Hideaki Jinnouchi, MD, PhD, (Jinnouchi Hospital, Kumamoto, Japan), Isao Taguchi, MD, PhD, (Dokkyo Medical University, Saitama Medical Center, Saitama, Japan), Hirofumi Tomiyama, MD, PhD (Tokyo Medical University, Tokyo, Japan), and Koji Maemura, MD, PhD (Nagasaki University, Nagasaki, Japan). Executive Committee: Makoto Suzuki, MD, PhD (Yokohama Minami Kyosai Hospital, Yokohama, Japan), Shinichi Ando, MD, PhD (Saiseikai Futsukaichi Hospital, Chikushino, Japan), Kazuo Eguchi, MD, PhD (Saitama Red Cross Hospital, Saitama, Japan), Haruo Kamiya, MD, PhD (Japanese Red Cross Nagoya Daiichi Hospital, Nagoya, Japan), Tomohiro Sakamoto, MD, PhD (Saiseikai Kumamoto Hospital, Kumamoto, Japana), Hiroki Teragawa, MD, PhD (JR Hiroshima Hospital, Hiroshima, Japan), and Mamoru Nanasato, MD, PhD (Sakakibara Heart Institute, Fuchu, Japan). Data and Safety Monitoring Board: Munehide Matsuhisa, MD, PhD (Tokushima University Graduate School, Tokushima, Japan), Junya Ako, MD, PhD, (Kitasato University, Sagamihara, Japan), Yoshimasa Aso, MD, PhD (Dokkyo Medical University, Mibu, Japan), Masaharu Ishihara, MD, PhD (Hyogo College of Medicine, Nishinomiya, Japan), Kazuo Kitagawa, MD, PhD (Tokyo Women’s Medical University, Tokyo, Japan), and Akira Yamashina, MD, PhD (Kiryu University, Midori, Japan). Imaging Core Laboratory: Tsukuba Echo Core Laboratory. LLC, Tomoko Ishizu, MD, PhD (Tsukuba University, Tsukuba, Japan). Monitoring: Yumi Ikehara, MSc and Shinichiro Ueda, MD, PhD (Clinical Trial and Management Center, University of Ryukyus Hospital, Nishihara, Japan). Audit Team: Clinical Research Support Center, University of the Ryukyus, Nishihara, Japan. Data Center and Data Management: Ayako Takamori, Ph.D. (Clinical Research Center, Saga University Hospital, Saga, Japan). Statistical Analysis: Hisako Yoshida, PhD (Osaka Metropolitan University Graduate School of Medicine, Osaka, Japan) and Takumi Imai, PhD (Osaka Metropolitan University Graduate School of Medicine, Osaka, Japan). Study Secretariat: Atsushi Tanaka, MD, PhD (Saga University, Saga, Japan), Miki Mori (Saga University, Saga, Japan), Kaori Yamaguchi (Saga University, Saga, Japan), Soiken Inc., Tokyo, Japan, and the Organization for Clinical Medicine Promotion, Tokyo, Japan. Site Investigators (duplicates excluded): Drs. Machiko Asaka and Tetsuya Kaneko (Saga University, Saga, Japan), Drs. Masashi Sakuma, Shigeru Toyoda, Takahisa Nasuno, Michiya Kageyama, Jojima Teruo, Iijima Toshie, and Haruka Kishi (Dokkyo Medical University, Mibu, Japan), Dr. Hirotsugu Yamada, Kenya Kusunose, Daiju Fukuda, Shusuke Yagi, Koji Yamaguchi, Takayuki Ise, Yutaka Kawabata, and Akio Kuroda (Tokushima University Graduate School, Tokushima, Japan), Drs. Yuichi Akasaki and Mihoko Kurano (Kagoshima University, Kagoshima, Japan), Drs. Satoshi Hoshide, Takahiro Komori, Tomoyuki Kabutoya, and Yukiyo Ogata (Jichi Medical University School of Medicine, Shimotsuke, Japan), Drs. Yuji Koide, Hiroaki Kawano, Satoshi Ikeda, Satoki Fukae and Seiji Koga (Nagasaki University, Nagasaki, Japan), Dr. Yukihito Higashi, Shinji Kishimoto, Masato Kajikawa, and Tatsuya Maruhashi (Hiroshima Universsity, Hiroshima, Japan), Dr. Yoshiaki Kubota (Nippon Medical School, Tokyo, Japan), Drs. Yoshisato Shibata and Nehiro Kuriyama (Miyazaki Medical Association Hospital, Miyazaki, Japan), Dr. Ikuko Nakamura (Saga-Ken Medical Centre Koseikan, Saga, Japan), Dr. Kanemitsu Hironori (International University of Health and Welfare, Nasushiobara, Japan), Dr. Bonpei Takase (National Defense Medical College, Tokorozawa, Japan), Drs. Yuichi Orita, Chikage Oshita, and Yuko Uchimura (JR Hiroshima Hospital, Hiroshima, Japan), Drs. Ruka Yoshida, Yukihiko Yoshida, Hirohiko Suzuki, Yasuhiro Ogura, Mayuho Maeda, Masaki Takenaka, Takumi Hayashi, and Mirai Hirose (Nagoya Daini Red Cross Hospital, Nagoya, Japan), Dr. Itaru Hisauchi (Dokkyo Medical University, Saitama Medical Center, Saitama, Japan), Drs. Toshiaki Kadokami and Ryo Nakamura (Saiseikai Futsukaichi Hospital, Chikushino, Japan), Dr. Junji Kanda (Asahi General Hospital, Asahi, Japan), Dr. Kazuo Matsunaga (Imari Arita Kyoritsu Hospital, Matsuura, Japan), Drs. Masaaki Hoshiga, Koichi Sohmiya, and Yumiko Kanzaki (Osaka Medical and Pharmaceutical University), Dr. Arihiro Koyosue (Tokyo-Eki Center-Building Clinic, Tokyo, Japan), Drs. Hiroki Uehara, Naoto Miyagi, Toshiya Chinen, Kentaro Nakamura, Chikashi Nago, Suguru Chiba, Sho Hatano, Yoshikatsu Gima, and Masami Abe (Urasoe General Hospital, Urasoe, Japan), Drs. Masayoshi Ajioka, Hiroshi Asano, Yoshihiro Nakashima, Hiroyuki Osanai, Takahiro Kanbara, and Yusuke Sakamoto (Tosei General Hospital, Seto, Japan), Drs. Mitsutoshi Oguri, Shiou Ohguchi, Kunihiko Takahara, Kazuhiro Izumi, and Kenichiro Yasuda (Kasugai Municipal Hospital, Kasugai, Japan), Drs. Akihiro Kudo and Noritaka Machii (Fukushima Medical University, Fukushima, Japan), Drs. Ryota Morimoto, Yasuko Bando, Takahiro Okumura, and Toru Kondo (Nagoya University, Naogya, Japan), Drs. Shin-ichiro Miura, Yuhei Shiga, Joji Mirii, Makoto Sugihara, and Tadaaki Arimura (Fukuoka University School of Medicine, Fukuoka, Japan), Dr. Junko Nakano (Saiseikai Fukushima General Hospital, Fukushima, Japan), Drs. Tomohiro Sakamoto and Kazuhisa Kodama (Saiseikai Kumamoto Hospital, Kumamoto, Japan), Drs. Nobuyuki Ohte, Tomonori Sugiura, and Kazuaki Wakami (Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan), Drs. Yasuhiko Takemoto, Minoru Yoshiyama, Taichi Shuto, and Kazuo Fukumoto (Osaka City University, Osaka, Japan), Drs. Yosuke Okada, Kenichi Tanaka, Satomi Sonoda, Akemi Tokutsu, Takashi Otsuka, Fumi Uemura, Kenji Koikawa, Megumi Miyazaki, Maiko Umikawa, and Manabu Narisawa (University of Occupational and Environmental Health, Japan, Kitakyusyu, Japan), Dr. Machi Furuta (Wakayama Medical University, Wakayama, Japan), Dr. Hiroshi Minami (Aidu Chuo Hospital, Aiduwakamatsu, Japan), Dr. Masaru Doi (Doi Naika Clinicm Kumamoto, Japan), Drs. Kazuhiro Sugimoto and Susumu Suzuki (Ohta Nishinouchi Hospital, Koriyama, Japan), and Drs. Akira Kurozumi and Kosuke Nishio (Wakamatsu Hospital of the University of Occupational and Environmental Health, Japan, Kitakyusyu, Japan).
Funding
This study was funded by Astellas Pharma Inc. Japan, and Prof. Koichi Node received the funding. The funding agency of the trial had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
YH and SK drafted the manuscript and conceived the study. TI performed statistical analyses. SK, YH, KE, KF, HT, and KM measured the FMD. AT and KN critically revised the manuscript for important intellectual content. All the authors contributed to the manuscript and approved the submitted version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol for this sub-analysis was approved by the Ethics Committee of Saga University Hospital (2022-09-02) and registered (jRCT1071220089). All the individuals provided written informed consent to participate in the study. All methods were performed in accordance with the Declaration of Helsinki and relevant guidelines and regulations in Japan.
Consent for publication
All authors have read and approved the submission of the manuscript.
Competing interests
Competing interestsYH received honoraria from Astellas, AstraZeneca, MSD, Boehringer Ingelheim, Takeda, Bayer, Novo Nordisk, Fuji, Mochida, Eli Lilly, Teijin Pharma, Daiichi Sankyo, Otsuka, Kowa, Novartis, and Mitsubishi Tanabe and a research grant from Kao. TI received lecture fees from JCR Pharmaceuticals and Kyowa Kirin and outsourcing fees from the Organization for Clinical Medicine Promotion. KM received honoraria from Daiichi Sankyo, Novartis, Takeda, and Pfizer and a research grant from Daiichi Sankyo and Biotronik. AT received honoraria from Boehringer Ingelheim and research funding from GlaxoSmithKline, Takeda, Bristol, Myers Squibb, and Novo Nordisk. NK has received honoraria from AstraZeneca, Bayer Yakuhin, Boehringer Ingelheim Japan, Daiichi Sankyo, Eli Lilly Japan, Mitsubishi Tanabe Pharma, MSD, Novartis Pharma, Ono Pharmaceutical, Otsuka; Research grants from Asahi Kasei, Astellas, Boehringer Ingelheim Japan, Fujiyakuhin, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Novartis Pharma, and Teijin Pharma; and scholarships from Bayer Yakuhin, Japan Lifeline, and Teijin Pharma. The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kishimoto, S., Higashi, Y., Imai, T. et al. Lack of impact of ipragliflozin on endothelial function in patients with type 2 diabetes: sub-analysis of the PROTECT study. Cardiovasc Diabetol 22, 119 (2023). https://doi.org/10.1186/s12933-023-01856-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01856-x