
Abstract
Background
Emerging evidence supports that dihydroceramides (DhCer) and ceramides (Cer) contribute to the pathophysiology of insulin resistance and liver steatosis, and that their circulating concentrations are independently associated with cardiovascular outcomes. Circulating DhCer levels are increased in patients with type 2 diabetes (T2D). On the other hand, the GLP-1 receptor agonist liraglutide reduces major adverse cardiac events, insulin resistance and liver steatosis in T2D patients. The main purpose of the present study was therefore to investigate whether liraglutide decreases circulating levels of DhCer and Cer in T2D patients, which could be a mechanism involved in its cardiometabolic benefits. The secondary purpose was to assess the relationship between liraglutide-induced changes in DhCer/Cer levels and insulin resistance and liver steatosis.
Methods
Plasma concentrations of 11 DhCer and 15 Cer species were measured by a highly-sensitive mass spectrometry system in 35 controls and 86 T2D patients before and after 6 months of liraglutide (1.2 mg/day). Insulin resistance was estimated by the triglyceride-glucose (TyG) index. Liver fat content (LFC) was assessed in 53 patients by proton magnetic resonance spectroscopy.
Results
Plasma levels of total DhCer, 7 DhCer and 7 Cer species were increased in T2D patients compared to controls. Liraglutide decreased total DhCer by 15.1% (p = 0.005), affecting 16:0 (p = 0.037), 18:0 (p < 0.0001), 18:1 (p = 0.0005), 20:0 (p = 0.0003), 23:0 (p = 0.005) and 24:1 (p = 0.04) species. Total plasma Cer did not significantly change after liraglutide (p = 0.18), but 5 Cer species decreased significantly, i.e. 18:0 and 18:1 (both p < 0.0001), 19:0 and 24:1 (both p < 0.01) and 26:1 (p = 0.04). In multivariate analysis, the reduction in DhCer after liraglutide was independently associated with the reduction in LFC (p = 0.0005) and in TyG index (p = 0.05).
Conclusions
Liraglutide reduces plasma levels of numerous DhCer and Cer species in T2D patients, which may contribute to the cardiovascular benefit observed in the LEADER trial. The independent association between the decrease in plasma DhCer level with the reduction in LFC and TyG index adds new insights regarding the relationship between DhCer, liver steatosis and insulin resistance.
Trial registration ClinicalTrials.gov identifier: NCT02721888.
Similar content being viewed by others


Background
Dihydroceramides (DhCer) and ceramides (Cer) are bioactive sphingolipids that are implicated in several processes related to cardiometabolic diseases. Growing evidence suggests that they play a causative role in the pathophysiology of type 2 diabetes (T2D) and cardiovascular diseases [1]. One of the best-known negative effects of Cer is their ability to promote insulin resistance, and plasma Cer concentrations are positively associated with the degree of insulin resistance in humans [2,3,4]. In addition, recent studies reveal that circulating Cer levels are also strongly associated with cardiovascular outcomes, independently of traditional risk factors [5, 6].
DhCer have long been regarded only as inactive precursors of Cer. However, recent studies suggest that DhCer are directly involved in many processes relative to T2D and atherosclerosis, like insulin resistance [2]. Interestingly, plasma DhCer concentrations are increased in patients with coronary artery disease [7], and are linked to cardiovascular risk [8]. Moreover, circulating DhCer are inversely associated with the degree of insulin sensitivity [2, 9, 10], and are long-term strong predictors of T2D onset [11].
Emerging evidence indicates that Cer and DhCer also play a significant role in metabolic-associated fatty liver disease (MAFLD), which is highly prevalent during T2D. Cer are key mediators of several processes involved in MAFLD, such as hepatic insulin resistance, endoplasmic reticulum stress and mitochondrial dysfunction [12]. For instance, the inhibition of Cer synthesis in rats was found to protect against lipid accumulation in the liver [13]. Clinical studies reveal that circulating DhCer and Cer levels are increased in patients with MAFLD [10, 14], and that they mirror the hepatic content of DhCer and Cer [14]. In addition, it was recently reported that circulating DhCer concentrations are associated with the severity of liver steatosis in T2D patients whereas plasma Cer levels are not, suggesting that DhCer has a specific role [15].
Liraglutide, a glucagon-like peptide-1 receptor agonist (GLP-1 RA), significantly reduces the incidence of major adverse cardiovascular events (MACE) in the LEADER trial, and has beneficial effects on insulin resistance, liver steatosis and dyslipidemia in T2D patients [16,17,18,19]. Because DhCer and Cer play a role in the pathophysiology of cardiometabolic diseases and are associated with cardiovascular outcomes, the main purpose of the present study was to investigate whether liraglutide reduces the circulating levels of these lipids in T2D patients. Such a reduction may contribute to its cardiovascular and metabolic benefits. In addition, since DhCer and Cer play a role in the pathogenesis of MAFLD and insulin resistance, the secondary purpose of the study was to evaluate the relationship between the liraglutide-induced changes in circulating DhCer/Cer and liver fat content (LFC) and insulin resistance.
Methods
Subjects
This prospective single-center study was an ancillary study of the LIRA-NAFLD/LIP trial (ClinicalTrials.gov identifier: NCT02721888). We included 86 T2D patients treated with metformin and/or sulfonylurea (or glinides) and/or insulin, and for whom liraglutide was indicated because of poorly controlled diabetes (glycated hemoglobin A1c [HbA1c] > 7%). Exclusion criteria were severe liver impairment, estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73m2, pregnancy, alcohol abuse, treatment with dipeptidyl peptidase-4 inhibitors during the three previous months, or previous treatment with thiazolidinediones or any GLP-1 RA.
The results obtained in patients treated with liraglutide were compared to samples obtained from 35 healthy control subjects who had normal fasting glycemia (< 6.10 mmoL/L), normal triglyceridemia (< 1.7 mmoL/L), eGFR > 60 mL/min/1.73m2, and serum HDL-cholesterol (HDL-C) > 1.30 mmol/L for females and > 1.03 mmol/L for males. Exclusion criteria for control subjects were thyroid or kidney diseases, and the use of antidiabetic agents or medications known to affect lipid metabolism. This study was approved by our regional ethics committee, and written informed consent was obtained from all participants before study inclusion.
Study design and intervention
At baseline, T2D patients had a physical examination, and blood samples were collected in tubes containing in particular EDTA as preservative for lipidomic analyses. The plasma/serum was immediately separated by centrifugation, and analyzed for routine parameters or frozen < − 70 °C awaiting lipidomic analyses. LFC was assessed in a subgroup of 53 T2D patients using a 3.0-Tesla magnetic resonance system (Magnetom Trio Tim; Siemens, Erlangen, Germany).
Treatment with liraglutide (Victoza™; Novo Nordisk A/S, Kalundborg, Denmark) was started the following day at a dose of 0.6 mg/day, which was up-titrated to 1.2 mg/day after one week until the end of the study. After six months of treatment, patients underwent the same series of examinations.
Routine laboratory analyses
HbA1c was measured by high performance liquid chromatography (Variant II; Biorad, Richmond, CA). Routine biochemical parameters were determined on a Dimension Vista platform (Siemens, Saint-Denis, France). LDL-cholesterol (LDL-C) was estimated by the Friedewald's equation. eGFR was calculated according to the 2021-CKD-EPI equation. The triglyceride-glucose (TyG) index, determined as ln(fasting triglycerides [mg/dL] × fasting glucose [mg/dL]/2), was chosen as the marker of insulin resistance since it performs better than HOMA-IR [20, 21].
Plasma DhCer and Cer measurements
Lipid extraction
DhCer/Cer were extracted as previously described [22]. Briefly, 100 µL plasma (+ 100 µL PBS) were mixed with 10 µL of an internal standard mix (15 and 20 ng of 12:0 DhCer and Cer, respectively), then extracted with 750 µL of 1:2 chloroform/methanol for 10 min. Chloroform (250 µL) was then added and extraction continued for 10 min more. Water (250 µL) was then added and extraction continued for 10 min more. After centrifugation (9400 g, 5 min), the organic phase was collected. The aqueous phase was acidified with 8 µL of 3 mol/L of hydrochloric acid, and further extracted with 600 µL of chloroform for 10 min. After centrifugation (9400 g, 5 min), the two organic phases were combined, and washed with 800 µL of the upper phase from a chloroform/methanol/water (96.7:93.3:90) mixture. After centrifugation (9400 g, 5 min), the organic phase was evaporated under vacuum. Extracts were finally dissolved with 100 µL of 60:30:4.5 chloroform/methanol/water.
Liquid chromatography—tandem mass spectrometry (LC–MS/MS)
One microliter of extract was injected on a Vanquish Flex LC system coupled with a TSQ Altis MS/MS system (ThermoFisher Scientific). Separation was achieved on a Poroshell C8 column 2.1 × 3x100 mm, 2.7-µm (Agilent Technologies) using the following gradient conditions (0.3 mL/min): 1 min at 80% mobile phase B, 80% to 100% B over 8 min, 3 min at 100% B, then 5 min at 80% B. Mobile phases A and B consisted of water and methanol, respectively, both containing 1 mmol/L ammonium formate and 0.2% (v/v) formic acid. Individual DhCer and Cer species were identified using multiple-reaction monitoring (Additional file 1: Table S1). Calibration lines were obtained using external standards. Total lipids of each class (DhCer and Cer) were calculated by summing the individual lipid species.
Statistical analysis
For each parameter, the modification from baseline after liraglutide treatment in T2D patients, named “delta”, was calculated as final value minus initial value. Statistics and graphs were performed using GraphPad Prism (version 9.1.1). Comparisons of proportions were performed using the chi-square test with Yates’ correction. Normality of continuous variables was assessed using the D'Agostino-Pearson test. Plasma DhCer and Cer levels and the delta after liraglutide treatment did not follow a Gaussian distribution, and this was not due to outliers (checked with the ROUT method). Data are therefore reported as medians [1st-3rd quartiles]. The study required a sample size of 73 patients to achieve a power of 80% and a level of significance of 5%, for detecting a mean of the changes in DhCer levels of 50 nmol/L after treatment, assuming the standard deviation of the differences to be 150 nmol/L. We used nonparametric tests, which do not assume a Gaussian distribution. Thus, quantitative results between T2D patients and control subjects were compared using the Mann–Whitney U test. The paired Wilcoxon test was used for comparisons between baseline and after six months of liraglutide. For correlation analysis, univariate Spearman correlation coefficients (rho) were determined for continuous variables, and point biserial correlation was used to assess the correlations between continuous variables and categorical variables. Multivariate analyses were performed by multivariate linear regression. A Benjamini–Hochberg procedure was applied for controlling false positives in multiple testing, using a false discovery rate of 5%. A two-tailed probability level of 0.05 was considered statistically significant.
Results
Participant characteristics at baseline
Baseline characteristics of the 86 T2D patients and 35 control subjects are shown in Table 1. Patients had typical features of T2D, such as increased body mass index (BMI) (> 25 and > 30 kg/m2 for 98.8 and 79.1% of patients, respectively), elevated plasma triglyceride levels (≥ 1.70 mmol/L for 64.0% of patients), and low HDL-C concentrations (≤ 1.30 mmol/L for 64.9% of females and ≤ 1.03 mmol/L for 69.4% of males). Not surprisingly, the insulin resistance index TyG was higher in T2D patients than in controls (p < 0.0001).
Plasma DhCer and Cer at baseline
The median of total DhCer concentration in plasma was 12.7% higher in T2D patients at baseline than in controls (p = 0.047) (Table 2 and Fig. 1A). More precisely, T2D patients had higher plasma concentrations than controls for 7 of the 11 DhCer species we measured, i.e. 14:0. DhCer (p = 0.0001), 16:0 DhCer (p = 0.016), 18:0 DhCer (p < 0.0001), 18:1 DhCer (p < 0.0001), 20:0 DhCer (p < 0.0001), 22:0 DhCer (p = 0.0003) and 24:1 DhCer (p = 0.041). On the contrary, the levels of 26:0 and 26:1 DhCer were decreased in T2D patients (p-values of 0.013 and 0.012, respectively). The plasma concentrations of 23:0 and 24:0 DhCer were not significantly different between T2D patients and controls (p-values of 0.64 and 0.46, respectively).

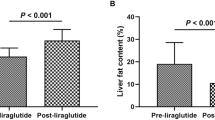
Plasma concentrations of total A dihydroceramides and B ceramides in control subjects and in patients with T2D at baseline (Lira-M0) and after 6 months of liraglutide (Lira-M6). Values correspond to p-values. The right panels represent the differences in percentage. The horizontal lines in the right panels represent medians
The total Cer level in plasma was increased by 90% in T2D patients at baseline compared with control subjects, but without reaching significance (difference of medians, p = 0.09) (Table 2 and Fig. 1B). However, the increase was statistically significant for 7 Cer species, i.e. 18:0 Cer (p < 0.0001), 18:1 Cer (p = 0.0004), 19:0 Cer (p < 0.0001), 20:0 Cer (p = 0.002), 21:0 Cer (p = 0.0001), 23:0 Cer (p = 0.02) and 24:1 Cer (p = 0.006). On the contrary, the plasma concentrations of 25:0 and 26:0 Cer were decreased in T2D patients (both p < 0.0001). The plasma levels of the remaining 6 Cer species were not statistically different between T2D patients and controls.
Effects of six months of liraglutide treatment
The observed changes in the clinical and routine biological parameters after six months of treatment with liraglutide are shown in Table 1. BMI decreased significantly by 1.0 units [median of differences, 95% confidence interval (CI) 0.5–1.6 kg/m2, p < 0.0001], HbA1c by 1.85 units (95%CI 1.40–2.50%, p < 0.0001), serum triglycerides by 0.19 mmol/L (95%CI 0.06–0.39 mmol/L, p = 0.002) and the TyG index by 2.6% (95%CI 1.2–4.0%, p < 0.0001). In the subgroup of the 53 T2D patients in whom a proton-spectroscopy of the liver was performed, the LFC significantly decreased from 17.3% (1st-3rd quartiles, 8.1–27.6%) at baseline to 10.5% (5.1–17.8%) after liraglutide (p < 0.0001).
After treatment with liraglutide, total plasma concentration of DhCer significantly decreased by 15.1% (median of differences, 95%CI 4.7–23.6%), corresponding to a median difference of 48 nmol/L (95%CI 19–62 nmol/L, p = 0.005) (Table 2 and Fig. 1A). After treatment, the total DhCer concentration in patients was not different from that of control subjects (p = 0.33, Table 2 and Fig. 1A). As shown in Table 2, the decrease affected 6 DhCer species, reaching 11.0% for 16:0 DhCer (p = 0.037), 26.0% for 18:0 DhCer (95%CI 13.9–37.0%, p < 0.0001), 19.9% for 18:1 DhCer (95%CI 10.5–31.6%, p = 0.0005), 17.9% for 20:0 DhCer (95%CI 0.2–26.3%, p = 0.0003), 13.4% for 23:0 DhCer (95%CI 3.3–32.1%, p = 0.005) and 15.8% for 24:1 DhCer (95%CI 1.4–22.1%, p = 0.04). Plasma levels of 22:0, 24:0, 26:0 and 26:1 DhCer were not significantly different after liraglutide treatment compared to baseline.
Although the total plasma concentration of Cer was not statistically modified by liraglutide treatment (p = 0.18) (Table 2 and Fig. 1B), circulating concentrations were significantly lower after treatment for 5 Cer species. This decrease reached 17.4% for 18:0 Cer (95%CI 8.8–23.4%, p < 0.0001), 16.0% for 18:1 Cer (95%CI 7.2–21.3%, p < 0.0001), 11.0% for 19:0 Cer (95%CI 1.5–19.9%, p = 0.006), 16.2% for 24:1 Cer (95%CI 5.7–20.0%, p = 0.006) and 11.8% for 26:1 Cer (95%CI 3.3–17.0%, p = 0.04).
Correlation analysis
Figure 2A shows the univariate correlations between changes in total plasma DhCer and Cer concentrations and changes in clinical and biological parameters after 6 months of treatment. The reduction in total DhCer level after liraglutide correlated positively with the decrease in total plasma Cer concentration (r = 0.619, p < 0.0001), in LFC (r = 0.493, p = 0.0002), in TyG index (r = 0.333, p = 0.002), in LDL-C (r = 0.280, p = 0.009) and in serum triglycerides (r = 0.265, p = 0.01). In multivariate analysis (Table 3), the decrease in total plasma DhCer concentration remained significantly associated with the reduction in LFC (β = 0.576, 95%CI 0.266–0.886, p = 0.0005), in total plasma Cer concentration (β = 0.489, 95%CI 0.192–0.786, p = 0.002), in serum triglycerides (β = 0.586, 95%CI 0.093–1.079, p = 0.021), in plasma glucose (β = 0.369, 95%CI 0.015–0.724, p = 0.04) and in TyG index (β = 0.126, 95%CI 0.020–0.232, p = 0.05). Interestingly, the baseline total plasma DhCer concentration in T2D subjects was strongly and positively associated with the baseline LFC (r = 0.468, p = 0.0002) and TyG index (r = 0.400, p = 0.0002) (Fig. 2B). Besides total DhCer, the significant decreases after liraglutide in the 20:0, 23:0 and 24:1 DhCer species were all positively associated with the reduction in both LFC and TyG index (Fig. 2C).

The heatmaps show univariate correlations A between changes in total plasma DhCer and Cer levels and modifications in clinical and biological parameters after six months of liraglutide treatment in T2D patients, B between total plasma DhCer and Cer levels and clinical and biological parameters at baseline, and C between changes in plasma levels of DhCer and Cer species and modifications in clinical and biological parameters after treatment in T2D patients. Only the correlations remaining significant after Benjamini–Hochberg correction to control the false discovery rate are reported in the heatmaps. Grey cells correspond to non-applicable calculations
In univariate regression analysis, the reduction in TyG index after liraglutide treatment correlated positively with the decrease in plasma glucose (r = 0.757, p < 0.0001), serum triglycerides (r = 0.718, p < 0.0001), LFC (r = 0.531, p < 0.0001), HbA1c (r = 0.494, p < 0.0001), serum total cholesterol (r = 0.399, p = 0.0002), total plasma Cer (r = 0.346, p = 0.001) and total plasma DhCer (r = 0.333, p = 0.002) (Fig. 3). Interestingly, in multivariate analysis the reduction in TyG index remained significantly associated with the decrease in total plasma DhCer (β = 0.149, 95%CI 0.006–0.292, p = 0.04) (Table 3).

The heatmap show univariate correlations between reduction in TyG index and LFC after six months of liraglutide treatment in T2D patients and changes in clinical and biological parameters. Only the correlations remaining significant after Benjamini–Hochberg correction to control the false discovery rate are reported in the heatmap. Grey cells correspond to non-applicable calculations
In univariate regression analysis, the reduction in LFC after liraglutide treatment correlated positively with the decrease in TyG index (r = 0.531, p < 0.0001), BMI (r = 0.524, p < 0.0001), plasma DhCer (r = 0.493, p = 0.0002), plasma glucose (r = 0.431, p = 0.001) and HbA1c (r = 0.413, p = 0.002) (Fig. 3). Interestingly, the reduction in LFC was strongly associated with the decrease in total plasma DhCer (β = 0.442, 95%CI 0.209–0.675, p = 0.0004) in multivariate analysis, independently of changes in BMI, HbA1c, serum triglycerides and total plasma Cer level (Table 3).
Discussion
In the present study, we report for the first time that liraglutide treatment significantly reduces the plasma concentrations of numerous DhCer species in patients with T2D. Firstly, we found that T2D patients had an increased total plasma DhCer at baseline compared with controls. A similar result has already been reported, but with a smaller number of either T2DM patients or control subjects and with a lower number of quantified DhCer species [2, 23]. Thus, Zarini et al. found increased plasma levels of 18:0, 20:0, 22:0 and 24:1 DhCer in T2D patients [2]. Our results are also consistent with those of Szpigel et al., except for the 24:1 DhCer for which they found a decrease in T2D [23]. However, the 24:1 DhCer species was found to be increased in T2D adolescents [24]. We observed no difference in total plasma Cer level between T2D patients and controls. Previous studies reported either a similar observation [2, 23], or a slight increase in total plasma Cer in T2DM patients [3]. Increased plasma levels of 18:0, 20:0 and 24:1 Cer we observed have already been reported in T2D patients [3, 25].
After six months of liraglutide treatment, the T2D patients in our cohort exhibited typical features of this treatment, including lower HbA1c and weight loss. While there was no change in total plasma Cer levels, we did observe a significant decrease in the plasma levels of 5 Cer species after liraglutide. Using the short-acting GLP-1 RA exenatide in 35 T2D patients, Zhang et al. recently found no reduction in plasma levels of Cer species, but exenatide is less potent for metabolic control than liraglutide [26], and the treatment duration was only 3 months compared to the 6 months of liraglutide in our study [25]. Using a metabolomic approach in 33 T2D patients, Jendle et al. recently reported that 18 weeks of a treatment with liraglutide induced no significant change in total plasma Cer levels, like in our study, but unfortunately they did not provide data on individual Cer species [27]. Zobel et al. found a reduction in 19:0 and 20:0 Cer species in 51 T2D patients after 26 weeks of treatment with liraglutide, but without reporting the levels of total Cer [28]. The decrease in plasma 24:1 Cer we observed is of particular interest, since the circulating concentration of this species predicts incident MACE independently of traditional cardiovascular risk factors in general [29], high cardiovascular risk [6], and T2D population [30]. The decrease in 18:0 Cer we observed after liraglutide is also noteworthy since an increase in one standard deviation of plasma 18:0 Cer concentration was associated with a 21% increase in MACE in the FinRisk study, independently of traditional cardiovascular risk factors [29].
Regarding DhCer, we reported for the first time that the plasma levels of total, 16:0, 18:1, 20:0, 23:0 and 24:1 DhCer significantly decreased in T2D patients after liraglutide treatment, which is particularly interesting since their plasma concentrations were reported to be associated with incident cardiovascular diseases, even after adjustment for traditional cardiovascular risk factors [7, 8]. For instance, an increase of one standard deviation in total plasma DhCer level was associated with a 146% increase in the risk of coronary artery disease [7]. To the best of our knowledge, only one study reported that liraglutide decreases circulating levels of 24:0 DhCer, but they did not provide data on other DhCer species [28]. Overall, the liraglutide-induced reduction in numerous DhCer and Cer species could be one of the mechanisms contributing to the beneficial cardiovascular effects of this treatment.
The mechanisms underlying the decrease in numerous DhCer/Cer species are intriguing. The fact that reductions in DhCer and Cer levels after liraglutide treatment were strongly and positively associated suggests that liraglutide acts on a step in the metabolism that is in common with both DhCer and Cer. DhCer are produced by the canonical de novo Cer synthesis pathway, and it may be hypothesized that liraglutide downregulates this pathway. In agreement with this hypothesis, Somm et al. recently found that liraglutide administered in mice reduces the liver gene expression of the serine palmitoyltransferase (SPT)-2, involved in the first step of de novo DhCer/Cer synthesis [31]. The expression of SPT was also downregulated after treatment of cardiac cells with exenatide [32]. Liraglutide-treated mice exhibited a decreased liver gene expression of Cer synthase-4, which preferentially adds C18 to C20 fatty acids to the sphingoid basis, in agreement with the liraglutide-induced reduction in plasma C18, C19, C20 DhCer and Cer that are reported in our study.
The significant decrease observed in the insulin resistance index TyG after treatment is consistent with previous studies showing that liraglutide improves insulin sensitivity in T2D patients [33]. Interestingly, we report for the first time that the decrease in total plasma DhCer level after liraglutide was positively and independently associated with the reduction in the TyG index in our cohort. In addition, total plasma DhCer concentration at baseline was positively and strongly associated with the TyG index. Similarly, recent studies reported that total plasma DhCer in humans was inversely associated with insulin sensitivity, measured with a hyperinsulinemic euglycemic clamp [2, 10]. In addition to total DhCer, the significant decrease in 20:0 and 24:1 DhCer after liraglutide treatment correlated with the reduction in the TyG index in our study, and it has been shown that the circulating levels of these two DhCer were negatively associated with insulin sensitivity in a recent study [2]. The relationship between DhCer and insulin resistance may be causative, since a recent study reported that the delivery of DhCer carried in liposomes into skeletal muscle cells counteracts the stimulating effect of insulin on glycogen synthesis, without affecting cellular Cer levels [2]. Regarding Cer, their role in the pathogenesis of insulin resistance is better established, and it is known that they are able to antagonize the insulin-dependent glucose uptake. The decrease in plasma 18:0 Cer we observed after liraglutide is notable because the plasma level of this species is inversely associated with insulin sensitivity in humans [2]. Taken together, these data suggest that the reduction in circulating levels of numerous Cer and DhCer species might contribute to the improvement of insulin sensitivity in liraglutide-treated T2D patients.
Liver steatosis was significantly reduced after liraglutide treatment in our study, which is concordant with previous reports [17]. Interestingly, we report for the first time that the reduction in LFC positively and independently correlated with the decrease in total plasma DhCer in multivariate analysis, but not with the change in Cer. Moreover, plasma DhCer level at baseline was strongly associated with LFC, unlike Cer. Besides total DhCer, the significant decrease in 20:0 and 24:1 DhCer after liraglutide correlated with the reduction in LFC in our study. Accordingly, the circulating levels of the two species have been shown to be positively associated with histological liver steatosis in obese individuals [14] and with the non-invasive SteatoTest™ in T2D patients [15]. In another study including T2D patients, Carlier et al. also found that total plasma DhCer levels correlate with the intensity of liver steatosis assessed by SteatoTest™, whereas total plasma Cer levels do not [15]. Interestingly, the inhibition in human liver cells of the DhCer desaturase, which converts DhCer into Cer, upregulated triglyceride storage in lipid droplets in relation with an increased level of DhCer [34]. All of these findings suggest that DhCer have a specific role independent from Cer in the pathophysiology of liver steatosis in T2D.
The strengths of our study include the novelty of reporting the effect of liraglutide treatment in T2D patients on circulating DhCer, which are increasingly seen as important bioactive sphingolipids involved in many processes occurring in T2D and atherosclerosis. Using a highly sensitive LC–MS/MS, we quantified a panel of DhCer and Cer species that is more extensive than the panels usually reported in clinical studies. Another strength is the novelty of investigating the association between changes in plasma DhCer/Cer after liraglutide treatment and those in LFC and the TyG index, thus providing new insights into the relationship between these sphingolipids and liver steatosis and insulin resistance in T2D. A limitation of our study is the lack of histological measures of liver steatosis. However, we assessed the LFC with proton-spectroscopy, which is recognized as a gold-standard method. Another limitation is the lack of in vivo measurements of insulin sensitivity, such as with a euglycemic insulin clamp. However, we used TyG index as surrogate, which is a strong predictor of MACE [21], and a reliable marker of insulin resistance that performs better than HOMA-IR [20]. Lastly, the age and sex ratio were different between controls and patients. However, we assume that this has no impact on our results since the changes in total plasma DhCer/Cer levels after liraglutide did not correlate with age and gender, and no correlation occurred at baseline in T2D patients and all subjects.
Conclusion
Liraglutide significantly reduces plasma levels of numerous DhCer and Cer species in patients with T2D, which is of particular interest due to the emerging role of these lipids in the pathophysiology of cardiometabolic diseases and their association with cardiovascular outcomes. Further investigations are needed to determine whether the measurement of Cer/DhCer levels is of additional interest in clinical practice, in T2D patients with MAFLD regarding cardiovascular and steatosis risks. In addition, these metrics could be relevant outcomes to consider during the development of new antidiabetic medications.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- Cer:
-
Ceramide
- DhCer:
-
Dihydroceramide
- eGFR:
-
Estimated glomerular filtration rate
- GLP-1 RA:
-
Glucagon-like peptide-1 receptor agonist
- LFC:
-
Liver fat content
- MACE:
-
Major adverse cardiovascular event
- MAFLD:
-
Metabolic-associated fatty liver disease
- SPT:
-
Serine palmitoyl-transferase
- T2D:
-
Type 2 diabetes
- TyG:
-
Triglyceride-glucose
References
Choi RH, Tatum SM, Symons JD, Summers SA, Holland WL. Ceramides and other sphingolipids as drivers of cardiovascular disease. Nat Rev Cardiol. 2021;18(10):701–11.
Zarini S, Brozinick JT, Zemski Berry KA, Garfield A, Perreault L, Kerege A, et al. Serum dihydroceramides correlate with insulin sensitivity in humans and decrease insulin sensitivity in vitro. J Lipid Res. 2022;63(10): 100270.
Haus JM, Kashyap SR, Kasumov T, Zhang R, Kelly KR, Defronzo RA, et al. Plasma ceramides are elevated in obese subjects with type 2 diabetes and correlate with the severity of insulin resistance. Diabetes. 2009;58(2):337–43.
Chew WS, Torta F, Ji S, Choi H, Begum H, Sim X, et al. Large-scale lipidomics identifies associations between plasma sphingolipids and T2DM incidence. JCI Insight. 2019;5(13):e126925, 126925.
Laaksonen R, Ekroos K, Sysi-Aho M, Hilvo M, Vihervaara T, Kauhanen D, et al. Plasma ceramides predict cardiovascular death in patients with stable coronary artery disease and acute coronary syndromes beyond LDL-cholesterol. Eur Heart J. 2016;37(25):1967–76.
Wang DD, Toledo E, Hruby A, Rosner BA, Willett WC, Sun Q, et al. Plasma ceramides, mediterranean diet, and incident cardiovascular disease in the PREDIMED trial. Circulation. 2017;135(21):2028–40.
Poss AM, Maschek JA, Cox JE, Hauner BJ, Hopkins PN, Hunt SC, et al. Machine learning reveals serum sphingolipids as cholesterol-independent biomarkers of coronary artery disease. J Clin Invest. 2020;130(3):1363–76.
Wittenbecher C, Cuadrat R, Johnston L, Eichelmann F, Jäger S, Kuxhaus O, et al. Dihydroceramide- and ceramide-profiling provides insights into human cardiometabolic disease etiology. Nat Commun. 2022;13(1):936.
Brozinick JT, Hawkins E, Hoang Bui H, Kuo MS, Tan B, Kievit P, et al. Plasma sphingolipids are biomarkers of metabolic syndrome in non-human primates maintained on a Western-style diet. Int J Obes. 2013;37(8):1064–70.
Apostolopoulou M, Gordillo R, Koliaki C, Gancheva S, Jelenik T, De Filippo E, et al. Specific hepatic sphingolipids relate to insulin resistance, oxidative stress, and inflammation in nonalcoholic steatohepatitis. Diabetes Care. 2018;41(6):1235–43.
Wigger L, Cruciani-Guglielmacci C, Nicolas A, Denom J, Fernandez N, Fumeron F, et al. Plasma dihydroceramides are diabetes susceptibility biomarker candidates in mice and humans. Cell Rep. 2017;18(9):2269–79.
Hajduch E, Lachkar F, Ferré P, Foufelle F. Roles of ceramides in non-alcoholic fatty liver disease. J Clin Med. 2021;10(4):792.
Kurek K, Piotrowska DM, Wiesiołek-Kurek P, Łukaszuk B, Chabowski A, Górski J, et al. Inhibition of ceramide de novo synthesis reduces liver lipid accumulation in rats with nonalcoholic fatty liver disease. Liver Int. 2014;34(7):1074–83.
Ooi GJ, Meikle PJ, Huynh K, Earnest A, Roberts SK, Kemp W, et al. Hepatic lipidomic remodeling in severe obesity manifests with steatosis and does not evolve with non-alcoholic steatohepatitis. J Hepatol. 2021;75(3):524–35.
Carlier A, Phan F, Szpigel A, Hajduch E, Salem JE, Gautheron J, et al. Dihydroceramides in triglyceride-enriched VLDL are associated with nonalcoholic fatty liver disease severity in type 2 diabetes. Cell Rep Med. 2020;1(9): 100154.
Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JFE, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–22.
Li X, Wu X, Jia Y, Fu J, Zhang L, Jiang T, et al. Liraglutide decreases liver fat content and serum fibroblast growth factor 21 levels in newly diagnosed overweight patients with type 2 diabetes and nonalcoholic fatty liver disease. J Diabetes Res. 2021;2021:3715026.
Zinman B, Gerich J, Buse JB, Lewin A, Schwartz S, Raskin P, et al. Efficacy and safety of the human glucagon-like peptide-1 analog liraglutide in combination with metformin and thiazolidinedione in patients with type 2 diabetes (LEAD-4 Met+TZD). Diabetes Care. 2009;32(7):1224–30.
Vergès B, Duvillard L, De Pais BJP, Bouillet B, Baillot-Rudoni S, Rouland A, et al. Liraglutide reduces postprandial hyperlipidemia by increasing apoB48 (apolipoprotein B48) catabolism and by reducing apoB48 production in patients with type 2 diabetes mellitus. Arterioscler Thromb Vasc Biol. 2018;38(9):2198–206.
Luo P, Cao Y, Li P, Li W, Song Z, Fu Z, et al. TyG index performs better than HOMA-IR in chinese type 2 diabetes mellitus with a BMI < 35 kg/m2: a hyperglycemic clamp validated study. Medicina. 2022;58(7):876.
Tao LC, Xu J, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68.
Tran TTT, Postal BG, Demignot S, Ribeiro A, Osinski C, de Pais Barros JP, et al. Short term palmitate supply impairs intestinal insulin signaling via ceramide production. J Biol Chem. 2016;291(31):16328–38.
Szpigel A, Hainault I, Carlier A, Venteclef N, Batto AF, Hajduch E, et al. Lipid environment induces ER stress, TXNIP expression and inflammation in immune cells of individuals with type 2 diabetes. Diabetologia. 2018;61(2):399–412.
Lopez X, Goldfine AB, Holland WL, Gordillo R, Scherer PE. Plasma ceramides are elevated in female children and adolescents with type 2 diabetes. J Pediatr Endocrinol Metab. 2013;26(9–10):995–8.
Zhang L, Hu Y, An Y, Wang Q, Liu J, Wang G. The changes of lipidomic profiles reveal therapeutic effects of exenatide in patients with type 2 diabetes. Front Endocrinol. 2022;13: 677202.
Buse JB, Rosenstock J, Sesti G, Schmidt WE, Montanya E, Brett JH, et al. Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet. 2009;374(9683):39–47.
Jendle J, Hyötyläinen T, Orešič M, Nyström T. Pharmacometabolomic profiles in type 2 diabetic subjects treated with liraglutide or glimepiride. Cardiovasc Diabetol. 2021;20(1):237.
Zobel EH, Wretlind A, Ripa RS, Rotbain Curovic V, von Scholten BJ, Suvitaival T, et al. Ceramides and phospholipids are downregulated with liraglutide treatment: results from the LiraFlame randomized controlled trial. BMJ Open Diabetes Res Care. 2021;9(1): e002395.
Havulinna AS, Sysi-Aho M, Hilvo M, Kauhanen D, Hurme R, Ekroos K, et al. Circulating ceramides predict cardiovascular outcomes in the population-based FINRISK 2002 cohort. Arterioscler Thromb Vasc Biol. 2016;36(12):2424–30.
Alshehry ZH, Mundra PA, Barlow CK, Mellett NA, Wong G, McConville MJ, et al. Plasma lipidomic profiles improve on traditional risk factors for the prediction of cardiovascular events in type 2 diabetes mellitus. Circulation. 2016;134(21):1637–50.
Somm E, Montandon SA, Loizides-Mangold U, Gaïa N, Lazarevic V, De Vito C, et al. The GLP-1R agonist liraglutide limits hepatic lipotoxicity and inflammatory response in mice fed a methionine-choline deficient diet. Transl Res. 2021;227:75–88.
Leonardini A, D’Oria R, Incalza MA, Caccioppoli C, Andrulli Buccheri V, Cignarelli A, et al. GLP-1 receptor activation inhibits palmitate-induced apoptosis via ceramide in human cardiac progenitor cells. J Clin Endocrinol Metab. 2017;102(11):4136–47.
Jinnouchi H, Sugiyama S, Yoshida A, Hieshima K, Kurinami N, Suzuki T, et al. Liraglutide, a glucagon-like peptide-1 analog, increased insulin sensitivity assessed by hyperinsulinemic-euglycemic clamp examination in patients with uncontrolled type 2 diabetes mellitus. J Diabetes Res. 2015;2015:e706416.
Lee AY, Lee JW, Kim JE, Mock HJ, Park S, Kim S, et al. Dihydroceramide is a key metabolite that regulates autophagy and promotes fibrosis in hepatic steatosis model. Biochem Biophys Res Commun. 2017;494(3–4):460–9.
Acknowledgements
The authors thank Véronique Grivet and Cécile Breuiller for their help during the recruitment of patients, and to Suzanne Rankin for the language revision of the manuscript. All of the above are affiliated to the CHU Dijon Bourgogne.
Funding
The authors acknowledge Grants from Novo Nordisk and from the French National Research Agency (ANR) under the program “Investissements d’Avenir” with reference ANR11-LABX-0021 (LipSTIC Labex). Novo Nordisk had no role in collection, analysis, and interpretation of data, in writing the paper, and in the decision to submit the paper for publication. The authors also acknowledge financial support from the University of Burgundy-Franche-Comté, the National Institute of Health and Medical Research (Institut National de la Santé et de la Recherche Médicale [INSERM]), the Region Burgundy-Franche Comté and the Fonds Européens de Développement Régional.
Author information
Authors and Affiliations
Contributions
DD, LD and BV were involved in the conception, design, and conduct of the study and interpretation of the results. DD, VB, JPdB, IS, LD, PPD, BB, JMP, AR, AB participated to the recruitment of patients, acquisition of data and analysis. DD wrote the first draft of the manuscript, and all authors edited, reviewed, and approved the final version of the manuscript. DD is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study complies with the Declaration of Helsinki and was approved by the our regional ethics committee.
Consent for publication
Not applicable.
Competing interests
The authors’ employer (University Hospital of Dijon, France) received funding from Novo Nordisk for this study. Novo Nordisk had no role in collection, analysis, and interpretation of data, in writing the paper, and in the decision to submit the paper for publication. Otherwise, no potential competing interests relevant to this article are reported.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
12933_2023_1845_MOESM1_ESM.docx
Additional file 1: Table S1. Quantified dihydroceramide and ceramide species and conditions for mass spectrometry acquisition. CE, collision energy; IS, internal standard used for quantitation.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Denimal, D., Bergas, V., Pais-de-Barros, JP. et al. Liraglutide reduces plasma dihydroceramide levels in patients with type 2 diabetes. Cardiovasc Diabetol 22, 104 (2023). https://doi.org/10.1186/s12933-023-01845-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01845-0