
Abstract
Type 2 diabetes mellitus (T2DM) is a chronic, complex metabolic disease characterized by chronic hyperglycemia causing from insufficient insulin signaling because of insulin resistance or defective insulin secretion, and may induce severe complications and premature death. Sodium-glucose cotransporter-2 (SGLT2) inhibitors are oral drugs used to reduce hyperglycemia in patients with T2DM, including empagliflozin, ertugliflozin, dapagliflozin and canagliflozin. The primary objective of this article is to examine the clinical benefit, safety, and tolerability of the four SGLT2 inhibitors approved by the US FDA. SGLT2 inhibitors increase urinary glucose excretion via inhibiting SGLT2 to decrease renal reabsorption of filtered glucose and reduce the renal threshold for glucose. Rather than stimulating insulin release, SGLT2 inhibitors improve β-cell function by improving glucotoxicity, as well as reduce insulin resistance and increase insulin sensitivity. Early clinical trials have confirmed the beneficial effects of SGLT2 in T2DM with acceptable safety and excellent tolerability. In recent years, SGLT2 inhibitors has been successively approved by the FDA to decrease cardiovascular death and decrease the risk of stroke and cardiac attack in T2DM adults who have been diagnosed with cardiovascular disease, treating heart failure (HF) with reduced ejection fraction and HF with preserved ejection fraction, and treat diabetic kidney disease (DKD), decrease the risk of hospitalization for HF in T2DM and DKD patients. SGLT2 inhibitors are expected to be an effective treatment for T2DM patients with non alcoholic fatty liver disease. SGLT2 inhibitors have a similar safety profile to placebo or other active control groups, with major adverse events such as Ketoacidosis or hypotension and genital or urinary tract infections.
Similar content being viewed by others


Introduction
Diabetes is a major public health problem, affecting approximately 10% of the population [1]. Type 2 diabetes mellitus (T2DM) is a chronic and complex metabolic disease [1,2,3]. T2DM is characterized by chronic hyperglycemia due to insufficient insulin signaling due to defective insulin secretion and insulin resistance, and it is also related to increased endogenous glucose production (EGP) or glucagon [4]. T2DM patients have a two- to three-fold increased risk of cardiovascular disease, which is further amplified in the presence of chronic renal impairment [3]. In addition to atherosclerotic cardiovascular disease, patients with T2DM have increased risk of developing diabetic kidney disease (DKD) and heart failure (HF) [3, 5, 6].
Hospitalizations for major diabetic complications including myocardial infarction and stroke are increasing [7]. Drug therapy is aimed at preventing microvascular complications, comprising end-stage kidney disease (ESKD) and blindness [1]. As the understanding of the underlying pathophysiological deficits continues to evolve, the therapy options for T2DM have multiplied [6]. The initial approach recommended by the American Association of Clinical Endocrinologists (AACE)/American College of Endocrinology and the American Diabetes Association (ADA) includes lifestyle changes and monotherapy, preferably metformin [6]. Drugs currently commonly used to control blood glucose such as insulin, glucagon-like peptide 1 (GLP1) receptor agonists, sulfonylureas, thiazolidinediones, dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors [6]. These drugs have achieved significant clinical success.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors increase urinary glucose excretion via inhibiting glucose reabsorption in the renal proximal tubules [8]. SGLT2 inhibitors can be combined with diet and exercise. They are available as monotherapy or in combination with some antidiabetic drugs, such as metformin [9].
SGLT2 inhibitors reduce glycated hemoglobin (HbA1c) without raising hypoglycemia risk, also they can lose weight and improve hyperuricemia, blood lipids and blood pressure [8]. Current evidence suggest that SGLT2 inhibitors improve renal and cardiovascular outcomes in T2DM patients, especially those with previous cardiovascular events, chronic kidney disease (CKD) or HF [8]. Similarly, several clinical trials using GLP1 receptor agonists and SGLT2 inhibitors have reported data showing cardiovascular benefits and delays in DKD progression [1, 5, 10].
SGLT2 inhibitors have good tolerability, with common adverse events such as genitourinary tract infection, diabetic ketoacidosis (DKA), or hypotension [8, 11,12,13,14].
Until now, empagliflozin has been approved by the FDA for T2DM, to reduce cardiovascular death in adults with T2DM, treat adults with HF with reduced ejection fraction (HFrEF) and adults with HF and preserved ejection fraction. Canagliflozin is approved for T2DM and DKD, and reduces the risk of heart attack, cardiovascular death and stroke in adults with T2DM and established cardiovascular disease, and reduces the risk of hospitalization for heart failure (HHF) in T2DM and DKD patients. Dapagliflozin is indicated for T2DM, reduce the risk of HHF, for the treatment of HF in patients with HFrEF, and for CKD patients with or without the risk of T2DM progression. Ertugliflozin is approved for T2DM [15,16,17,18].
The main purpose of this review is to examine the clinical role, clinical advantages, safety and tolerability of SGLT2 inhibitors.
Essential effects of SGLT2 inhibitors
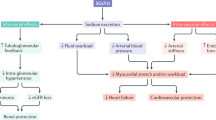
SGLT2 (Table 1) is the major transporter responsible for the reabsorption of glucose from the glomerular filtrate back into the circulation, is characterized by low affinity, high volume, as well as is predominantly expressed in the proximal tubules [19, 20]. By inhibiting SGLT2, SGLT2 inhibitors lower renal reabsorption of filtered glucose and reduce the renal threshold for glucose, thereby increasing urinary glucose excretion [19, 21,22,23,24,25,26,27]. This reduces HbA1c by approximately 0.6–1.0% [8, 28]. SGLT2 inhibitors increase sodium delivery to distal tubules through blocking SGLT2-dependent glucose and sodium reabsorption, which is thought to increase tube-ball feedback and decrease intraglomerular pressure. This may affect a variety of physiological functions, comprising reducing cardiac preload and afterload and downregulating sympathetic nerve activity [4, 19, 21,22,23,24,25,26,27,28]. Metabolism is shifted to gluconeogenesis and ketosis, which are thought to have protective effects on the heart and kidneys [28]. SGLT2 inhibitors can reduce glucotoxicity in renal tubular cells by reducing mitochondrial dysfunction and inflammation, and also reduce renal hypoxia by reducing tubular energy and oxygen demand [28].
The expression of SLC5A2 was higher in islets of non-T2DM patients than in islets of T2DM individuals or normal islets exposed to chronic hyperglycemia, with lower glucagon gene expression [4]. Glucagon secretion can be achieved by inhibiting SLC5A2 by siRNA-induced gene silencing or by inhibiting SGLT2 activation through KATP channels by dapagliflozin [4]. Glucagon secretion and hepatic gluconeogenesis were improved in normal mice treated with dapagliflozin, and fasting-induced hypoglycemia was limited [4, 29]. The effect of SGLT1 on glucagon secretion depends on glucose transport, not glucose metabolism. Canagliflozin inhibits glucagon secretion by inhibiting SGLT1 in alpha cells [29].
SGLT2 inhibitors can induce transforms in IL-6, adiponectin, and serum leptin and improve adipose tissue function, which have favorable effects on insulin sensitivity and cardiovascular disease risk [30, 31]. SGLT2 inhibitors also increase HDL, LDL levels and reduce triglyceride levels [32, 33]. SGLT2 inhibitors are able to obviously reduce systolic blood pressure (SBP) and lead to weight loss (Table 2). Additionally, a meta-analysis of 58 studies reported favorable effects of SGLT2 inhibitors on HbA1c levels (mean difference (MD) from placebo − 0.66%; active comparator − 0.06%). SGLT2 inhibitors decreased body weight (− 1.80 kg) and SBP (− 4.45 mm Hg) compared to other drugs [34].
Effect on beta cells
Rather than stimulating insulin release, SGLT2 inhibitors improve β-cell function by improving glucotoxicity and reducing β-cell workload [8, 20]. SGLT2 inhibitor-induced glucosuria improved beta-cell function and insulin sensitivity, decreased tissue glucose disposal and increased EGP following administration, thereby reducing fasting and postprandial glycemic [35]. Eight weeks of treatment with empagliflozin restored hypothalamic insulin sensitivity, possibly contributing to the beneficial effects of SGLT2 inhibitors [36].
Regulate blood lipids
A single-center, prospective trial determined that SGLT2 inhibitors increased HDL-C and apolipoprotein AI compared with sitagliptin. SGLT2 inhibitors did not change the concentration of LDL-C, while reduced small, dense LDL-C by 20% and increased large buoyant LDL-C by 18%. SGLT2 inhibitors increased HDL2-C by 18% without affecting HDL3-C [37]. A meta-analysis of 15 studies indicated no association between SGLT2 inhibitors and dyslipidemia risk [ratio risk = 1.13]. It was significantly associated with a 0.15 mmol/L increase in total cholesterol, a 0.12 mmol/L increase in LDL, a 0.07 mmol/L increase in HDL, and a reduction in triglycerides of 0.12 mmol/L compared to controls [33].
Effect on liver
Nonalcoholic fatty liver disease (NAFLD), which often coexists with T2DM, is the most prevalent chronic liver disease worldwide [38,39,40]. Clinically, SGLT2 inhibitors have shown benefit for NAFLD.
In the E-LIFT trial, SGLT2 inhibitors were obviously better at decreasing liver fat than standard therapy [MRI-Proton Density Fat Fraction (PDFF) difference − 4.0%; P < 0.0001]. MRI-PDFF was notably lower in the SGLT2 inhibitor group (P < 0.0001) compared with baseline. Two groups displayed a significant difference in serum alanine aminotransferase (ALT) levels (P = 0.005) [38]. Two meta-analyses results showed that SGLT-2 inhibitors significantly reduced serum ALT, aspartate aminotransferase and γ-glutamyltransferase levels compared with controls, and the absolute percentage of liver fat content based on magnetic resonance technology, and body composition, glycemic control, lipid parameters, and markers of inflammation were significantly improved, and there was a trend for improvement in markers of fibrosis [41, 42].
In NAFLD patients, dapagliflozin significantly reduced the fatty liver index (P < 0.01) compared with pioglitazone, and changes in the fatty liver index were significantly positively correlated with changes in insulin (P < 0.01) and HbA1c (P = 0.03) levels [43].
Cardiovascular benefits
The investigators concluded that the cardioprotective effects of SGLT2 inhibitors can be attributed to (Table 1): blood pressure control, increased plasma erythrocytes levels, decreased inflammation and oxidative stress, decreased uric acid, prevention of ischemia/reperfusion injury and improved cardiac and vascular function [8, 30, 32, 44]. The effects of SGLT2 inhibitors in the early stages, in addition to direct improvements in peripheral endothelial function, are responsible for the clinical benefit found in the Cardiovascular Outcomes Trial [45]. SGLT2 inhibitors lead to acute and chronic reductions in SBP, reductions in vasoconstrictors and increases in vasodilators. These changes may contribute to its antihypertensive effect and its benefit in congestive HF [46]. Early pathogenesis of human diabetic cardiomyopathy is associated with JunD/PPAR-γ overexpression and lipid accumulation after heart transplantation in diabetic patients. This phenomenon was decreased by therapy with SGLT2 inhibitors that act directly on the heart of diabetic patients [47].
EMPA-HEART CardioLink-6 was designed to determine whether empagliflozin causes decreased left ventricular mass in coronary artery disease patients with T2DM [48]. For patients assigned to empagliflozin and placebo, mean body surface area-related left ventricular mass regressions over 6 months was 2.6 g/m2 and 0.01 g/m2, respectively (P = 0.01) [48]. SGLT2 inhibitors was related to obviously lower extracellular volume, left ventricular mass index, and indexed extracellular compartment volume, which may be partly responsible for the beneficial cardiovascular outcomes [48, 49].
An analysis of the results of the CANVAS program (Canagliflozin Cardiovascular Assessment Study) indicated that patients with a previous cardiovascular event had higher absolute rates of cardiovascular, renal and death outcomes compared with participants without a previous cardiovascular event. Canagliflozin reduced cardiovascular outcomes overall [50]. Data from the DIVERSITY-CVR trial demonstrated that SGLT2 inhibitors were obviously more effective than sitagliptin in improving cardiometabolic risk factors [51]. Results of an exploratory analysis of EMPA-REG OUTCOME indicated that changes in hemoglobin and hematocrit mediated 48.9% and 51.8%, respectively, of the effect of empagliflozin vs. placebo on the risk of cardiovascular death, while HbA1c, fasting plasma glucose (FPG) and uric acid were less regulated (29.3%) [52]. Ertugliflozin was noninferior to placebo in terms of major adverse cardiovascular events (MACE) in patients with atherosclerotic cardiovascular disease and T2DM [11].
In a retrospective cohort study, patients administered SGLT2 inhibitors experienced a lower risk of developing HHF [hazard ratio (HR) = 0.86], all-cause mortality (HR = 0.85), and stroke (HR = 0.86) compared with DPP-4 inhibitors [53]. A multi-database retrospective cohort study also identified that SGLT2 inhibitors were related to a reduced risk of HF (0.43), cardiovascular death (0.60), MACE (HR = 0.76) and myocardial infarction (0.82) compared with DPP-4 inhibitors. Canagliflozin (HR = 0.79), dapagliflozin (0.73), and empagliflozin (0.77) had similar benefits for MACE [54].
Multiple meta-analyses have reported that SGLT2 inhibitors were related to fewer cardiovascular events, especially HHF and cardiovascular mortality. However, for non-fatal stroke and myocardial infarction differ [12, 55,56,57,58,59,60]. SGLT2 inhibitors reduced MACE by 11% (P = 0.0014), with benefit only in atherosclerotic cardiovascular disease patients (HR = 0.86) [61]. A meta-analysis of 764 studies (n = 421,346) reported that SGLT-2 inhibitors reduced non-fatal myocardial infarction, and cardiovascular death. Importantly, SGLT-2 inhibitors decreased HHF more than GLP-1 [55]. Results of a network meta-analysis of 453 studies showed that oral SGLT-2 inhibitors decreased HHF in patients at increased cardiovascular risk who had prior metformin-based therapy [12]. Another meta-analysis included data from 57 trials (n = 33,385) and 6 regulatory submissions (n = 37,525), providing data on seven SGLT2 inhibitors [60]. SGLT2 inhibitors prevented the risk of MACE (relative risk 0.84; P = 0.006), all-cause death (0.71; P < 0.0001), HF (0.65; P = 0.002), and cardiovascular death (0.63; P < 0.0001). There was no significant effect on angina (0.95; P = 0.70) or non-fatal myocardial infarction (0.88; P = 0.18) [60].
Benefits of SGLT2 inhibitors in HF, HFrEF and HHF
SGLT2 inhibitors reduce left ventricular volume in T2DM or prediabetic patients with HFrEF. Favorable reverse left ventricular remodeling may be a mechanism by which SGLT2 reduces HHF and mortality in patients with HFrEF [62]. The partial of patients receiving SGLT2 inhibitors improved significantly in lung fluid volume [63]. Elevated concentrations of N-terminal pre-B-type natriuretic peptide (NT-proBNP) are related to HF diagnosis and prediction of cardiovascular risk [64]. A significant proportion of patients in the CANVAS trial had increased NT-proBNP values. Canagliflozin reduced NT-proBNP concentrations compared with placebo. However, the reduction in NT-proBNP explains only a small fraction of the benefit of canagliflozin on HF events [64]. A meta-analysis showed that SGLT2 inhibitors was related to obviously improved diastolic function and NT-proBNP levels in T2DM patients with or without chronic HF, while it did not significantly affect the structural parameters of the heart based on body surface area. Left ventricular ejection fraction levels improved only in patients with HFrEF [65]. SGLT2 inhibitors reduce inflammation and oxidative stress in HF with preserved ejection fraction, improve NO-sGC-cGMP-cascade and PKGIα activity by reducing PKGIα oxidation and aggregation, thereby reducing pathological cardiomyocyte stiffness [66]. Results from the large multinational study CVD-REAL demonstrated that SGLT-2 inhibitors were related to lower HHF and mortality compared with other antidiabetic agents [67].
Some randomized controlled trials have also conformed the benefit of SGLT2 inhibitors in HF or HHF (Table 3) [13, 68,69,70,71,72]. In the CANVAS program, canagliflozin significantly reduced severe HF or HHF (P = 0.003) and HHF (P = 0.002) compared with placebo. Canagliflozin had a greater benefit of cardiovascular death or HHF in patients with a prior history of HF (HR 0.61 vs. 0.87; P = 0.021) compared patients without HF at baseline [72]. Empagliflozin was related to a 35 percent decrease in the relative risk of HHF compared with placebo in EMPA-REG OUTCOME [69]. In EMPEROR-Reduced, the incidence of HHF was obviously lower in empagliflozin compared to placebo in adults with or without T2DM with HFrEF (HR = 0.69). And the overall number of people with HHF was less (21.0% vs. 30.0; P < 0.001) [68]. In DAPA-HF, the risk of HHF was lower in the dapagliflozin group for patients with (12.8% vs. 16.2%; P = 0.017) or without (7.2% vs. 11.2%; P < 0.001) T2DM [71]. Approximately 12.3% patients with HFrEF accompany by COPD, and these patients were at higher risk for the primary outcome. The benefit of dapagliflozin on prespecified outcomes was consistent regardless of COPD [73]. Ertugliflozin was also able to decrease the risk of HHF to some extent compared with placebo in the VERTIS CV trial [11, 74]. The risk reduction for first HHF was similar in patients with ejection fraction ≤ 45% or preserved ejection fraction > 45% or unknown [74].
Several meta-analyses have indicated that SGLT-2 inhibitors reduce HHF and are related to lower HF compared with placebo or active control group [12, 55, 56, 59, 61, 75,76,77]. SGLT-2 inhibitors were notably related to a lower incidence of HF events (HR = 0.62) [75]. SGLT2 inhibitors decreased the risk of cardiovascular death or HHF by 23% (P < 0.0001) and HHF by 31% (P < 0.0001), similar benefits were seen in patients with or without a history of HF or atherosclerotic cardiovascular disease [61]. Canagliflozin (HR = 0.69, 0.68, 0.67, 0.58) or empagliflozin (HR = 0.70, 0.69, 0.68, 0.59) notably decreased HHF compared with duraglutide, exenatide, lixisenatide, and subcutaneous injection [56]. In a real-world meta-analysis OBSERVE-4D, the HR estimate for canagliflozin vs. a non-SGLT2 inhibitor for HHF was 0.39 [76]. In a network meta-analysis of 23 studies, compared to DPP-4 inhibitors, SGLT2 inhibitors reduced the risk of HHF [77].
SGLT2 inhibitors (all four SGLT2 inhibitors) were able to reduce the risk of HF or HHF compared with control group (such as placebo or other antidiabetic drugs), regardless of cardiovascular disease. This view is supported by the combined results of clinical trials and meta-analyses.
Cardiovascular death
The beneficial effect of SGLT2 inhibitors on cardiovascular death now appears indisputable, whether meta-analyses, retrospective studies, or large clinical trials (Table 3) showed similar data that SGLT2 inhibitors lowered the risk of cardiovascular death. All four SGLT2 inhibitors are able to achieve this and are superior to DPP-4 inhibitors [12, 54, 55, 60, 75, 77]. In CANVAS, canagliflozin was slightly related to a lower risk of cardiovascular death compared with placebo (HR = 0.87) [78]. In EMPA-REG OUTCOME, the relative risk of cardiovascular death was decreased by 38% in the empagliflozin group [69]. Interestingly, dapagliflozin in the DAPA-HF and DECLARE–TIMI 58 studies achieved different cardiovascular mortality outcomes [13, 79]. Ertugliflozin does not appear to significantly reduce cardiovascular death compared with placebo (HR = 0.92) [11]. Outcomes from a large meta-analysis showed that SGLT2 inhibitors prevented cardiovascular death (P < 0.0001). Evidence that individual agents had different effects on cardiovascular outcomes or death was not evident (all I2 < 43%) [60]. SGLT-2 inhibitors obviously decreased cardiovascular death compared to DPP-4 inhibitors (RR = 0.88), in contrast to GLP-1 receptor agonists, there was no difference [77].
Arrhythmia
Several meta-analyses have showed that SGLT2 inhibitors decreased the risk of atrial fibrillation [58, 80]. A meta-analysis of 22 trials reported SGLT2 inhibitors were related to a lower risk of atrial fibrillation (RR = 0.82), atrial fibrillation/flutter (RR = 0.82), and ventricular tachycardia (RR = 0.73). The risk reduction for atrial flutter (RR = 0.83) and cardiac arrest (RR = 0.83) did not reach statistical significance [58]. Another meta-analysis indicated that the incidence of atrial fibrillation was 0.9% in subjects who received SGLT2 inhibitors and 1.1% in subjects who received placebo. The incidence of atrial fibrillation was significantly reduced (RR = 0.79) in both T2DM and non-T2DM patients receiving SGLT2 inhibitors [80].
Although current evidence supports that SGLT2 inhibitors reduce the risk of ventricular tachycardia, and atrial fibrillation in patients with or without T2DM, this is limited to meta-analyses, while the mechanisms are not well elucidated. More clinical trials are required to support the benefit of SGLT2 inhibitors in cardiac arrhythmias.
Nonfatal myocardial infarction
Although several meta-analyses have reported reductions in non-fatal myocardial infarction with SGLT-2 inhibitors, most have shown no apparent effect [55, 59, 60, 75]. Data from representative clinical trials (Table 3) showed that SGLT-2 inhibitors did not notably reduce the risk of non-fatal myocardial infarction. In CANVAS only, canagliflozin reduced the risk of non-fatal myocardial infarction to some extent compared with placebo (HR = 0.85) [78]. When compared with GLP-1 receptor agonists, the risk of non-fatal myocardial infarction was similar for both [77]. Based on the results of the current clinical trials and meta-analyses, it can be speculated that the effect of SGLT2 inhibitors on non-fatal myocardial infarction may be neutral. Potent evidence is now needed to support this.
Stroke
Results from some randomized controlled trials indicated that only canagliflozin among SGLT-2 inhibitors (Table 3) decreased the risk of stroke to a certain extent. In the CANVAS, canagliflozin had a similar effect to placebo on fatal or non-fatal stroke in patients with (HR = 0.84) and patients without a history of HF (HR = 0.88) [72]. In EMPA-REG OUTCOME, empagliflozin slightly increased the risk of fatal or non-fatal stroke (HR = 1.18; P = 0.26), and only for non-fatal stroke (HR = 1.24) [69].
Large meta-analyses displayed that SGLT-2 inhibitors barely reduced the risk of non-fatal stroke and even increased the risk (relative risk 1.30; P = 0.049) [55, 60]. This was also the case in a large retrospective study showing that SGLT2 inhibitors were less beneficial for ischemic stroke (HR = 0.85) [54]. Notably, a meta-analysis reported that SGLT2 was related to a lower risk of embolic stroke (RR = 0.32) [58]. Interestingly, the risk of non-fatal stroke was similar between GLP-1 receptor agonists and SGLT2 inhibitors, while only GLP-1 receptor agonists decreased the risk of non-fatal stroke when compared to placebo [77].
CKD with decreased estimated glomerular filtration rate (eGFR) or increased proteinuria increases the risk of hemorrhagic and ischemic stroke [81]. Outcomes from the CREDENCE trial and meta-analysis showed that 142 patients had a stroke (HR = 0.77). Effects on stroke subtypes were: ischemic (HR = 0.88), hemorrhagic (HR = 0.50), and indeterminate (HR = 0.54) [81]. There was evidence that the effect of SGLT2 inhibitors on total stroke varies by baseline eGFR (P = 0.01), with protection in the lowest eGFR (< 45 mL/min/1.73 m2) subgroup (HR = 0.50) [81].
SGLT2 inhibitors generally do not increase the risk of non-fatal stroke, and different results are reflected between different SGLT2 inhibitors, such as canagliflozin and empagliflozin. Several meta-analyses have also shown that SGLT2 inhibitors may lower the risk of certain types of stroke, such as embolic stroke. SGLT2 inhibitors on stroke risk may vary in different populations, such as depending on the level of renal function.
Renal protection
Diabetes is the most common cause of CKD, accounting for approximately 50% renal failure cases requiring replacement therapy [82]. DKD develops in 30–50% of diabetic patients [83]. SGLT-2 inhibitors have been clearly shown in multiple studies to improve renal outcomes in patients with CKD or DKD (Table 4), and glomerular hemodynamic function, significantly reduces the risk of proteinuria and renal failure [5, 78, 82, 84,85,86].
SGLT2 inhibition was related to an acute, dose-dependent decrease in eGFR of about 5 mL/min/1.73 m2 and a reduction in albuminuria of approximately 30–40%. These effects reflect preclinical observations showing that proximal tubular sodium excretion activates tubulo-glomerular feedback by increasing the delivery of sodium and chloride, subsequently causing afferent vasoconstriction [87]. Due to reduced glomerular filtration, CKD patients have attenuated glucosuria and weight loss (eGFR < 60 mL/min/1.73 m2) [87]. A potential mechanism for the renoprotective effect of SGLT2 inhibitors may also involve uric acid reduction [88, 89]. In T2DM patients with stage 2 or 3 CKD, SGLT2 inhibitors improved HbA1c and urinary albumin/creatinine ratios without increasing serious adverse renal events [90, 91].
The National Kidney Foundation convened a scientific symposium of an international panel of more than 80 experts to elucidate and support the role of SGLT2 inhibitors in T2DM and CKD [82]. The notion that the benefits of SGLT2 inhibitors are mediated by non-glycemic mechanisms at the meeting is supported by a number of observations that CKD and cardiovascular disease risk reductions in clinical trials of these drugs have not been associated with glycemic control or the use of other antidiabetic drugs [82].
Dapagliflozin and canagliflozin are approved for CKD or DKD. In the CANVAS program, canagliflozin was related to a lower incidence of the composite of sustained doubling of serum creatinine (dSCr), ESKD, and renal death compared with placebo (HR = 0.53) [78, 85]. Canagliflozin may be beneficial for the progression of albuminuria (HR = 0.73) and the composite outcome of sustained 40% decrease in eGFR, requirement for renal replacement therapy, or renal death (HR = 0.60) [78, 85]. In CREDENCE, the risk of renal failure was lower in the canagliflozin group compared with the placebo group [70]. Results from CANTATA-SU secondary analysis showed that compared with glimepiride, canagliflozin slowed the progression of renal disease over 2 years, and that it may confer renoprotective effects independent of its glycemic effects [92]. Dapagliflozin had a reduced incidence of renal events in the DECLARE–TIMI 58 trial (4.3% vs. 5.6%) [13]. The cardio-renal secondary composite outcome was obviously lower with dapagliflozin (P < 0.0001). The sustained decline in eGFR was reduced by 46% (P < 0.0001). Compared with placebo, dapagliflozin was associated with a lower risk of renal death or ESKD (0.1% vs. 0.3%; P = 0.012) [93]. A prespecified analysis from DAPA-CKD showed that when added to ACEI or ARB therapy, dapagliflozin decreased the risk of several clinical outcomes (such as ≥50% eGFR decline and ESKD) in patients with CKD [94].
Empagliflozin demonstrated renal protection in T2DM patients, as demonstrated in EMPA-REG OUTCOME, where empagliflozin was related to slower renal disease progression and a lower incidence of clinically relevant renal events compared with placebo (Table 4) [86]. Additionally, compared with placebo, empagliflozin improved uric acid levels with a lower risk of serious renal outcomes [68, 86, 88]. A sub-analysis of EMBODY trial reported that empagliflozin prevented the decline of renal function in T2DM patients with acute myocardial infarction, especially those with a baseline eGFR ≥ 60 mL/min/1.73 m2 [88]. Uric acid reduced about 0.9 mg/dL in the empagliflozin group (P < 0.001) [88].
SGLT-2 inhibitors decrease renal failure risk in multiple meta-analyses [12, 55,56,57]. SGLT2 inhibitors reduced the risk of kidney disease progression by 45% (P < 0.0001), including in some patients, regardless of atherosclerotic cardiovascular disease. The magnitude of the benefit of SGLT2 inhibitors varies with baseline renal function [61]. A meta-analysis including 32,949 patients showed that SGLT-2 inhibitors reduced the risk of renal events (RR = 0.68) [57]. Compared with GLP-1, SGLT-2 inhibitors were related to a lower risk of renal events (RR = 0.79) [57]. Moreover, dapagliflozin (HR = 0.62, 0.60, 0.68 and 0.63) and empagliflozin (HR = 0.64, 0.61, 0.69 and 0.64) notably decreased renal function progression compared with duraglutide, exenatide, liraglutide, and lixisenatide [56].
All-cause mortality
Results from several SGLT-2 inhibitor cardiovascular outcomes investigation trials indicated that SGLT-2 inhibitors decreased the risk of all-cause mortality compared with placebo. In the CANVAS program, compared with placebo, canagliflozin displayed a greater benefit on all-cause mortality in patients with a history of HF (HR = 0.70) than in patients without HF history (HR = 0.93) [72]. In EMPA-REG OUTCOME, empagliflozin reduced the risk of all-cause mortality by 32% (P < 0.001) [69]. In contrast, dapagliflozin did not notably lower the risk of all-cause mortality compared with placebo in DECLARE–TIMI 58 (HR = 0.93) [13]. In DAPA-HF, dapagliflozin reduced cardiovascular mortality to some extent (HR = 0.83) in subjects with HFrEF regardless of a previous history of diabetes [79]. There was a similar all-cause mortality between ertugliflozin and placebo (HR = 0.93) [11].
Several meta-analyses have showed that SGLT-2 inhibitors lower the risk of all-cause mortality [12, 55, 59, 60, 95]. A network meta-analysis of 236 trials showed that SGLT-2 inhibitors (HR = 0.80) were obviously reduced all-cause mortality than controls. SGLT-2 inhibitors (HR = 0.78) were associated with lower mortality compared to DPP-4 inhibitors [75]. SGLT-2 inhibitors reduced deaths by 5–48 per 1000 patients over 5 years [55].
Overall, all SGLT2 inhibitors, except ertugliflozin, were able to significantly reduce all-cause mortality, and the corresponding meta-analyses showed results consistent with clinical trials.
Anemia
SGLT-2 inhibitors also reduce hepcidin levels, improve erythropoiesis, increase hemoglobin levels, and reduce the incidence of anemia [28, 96,97,98]. A post hoc analysis from CREDENCE displayed that 13% of the 4401 participants developed anemia or started treatment for anemia. Mean hemoglobin concentrations were 7.1 g/L higher and hematocrit was 2.4% higher in canagliflozin compared to placebo. The risk of the composite outcome of anemia or initiation of anemia treatment was lower in the canagliflozin group compared to the placebo group (HR = 0.6; P < 0.0001). Subjects received canagliflozin had a lower risk of anemia events (0.58; P < 0.0001) alone, initiation of iron preparations (0.64; P < 0.0001), and need for erythropoiesis-stimulating agents (0.65; P = 0.012) [96].
Results of a retrospective cohort study indicated that SGLT2 inhibitors usage was related to an obviously lower prevalence of anemia [odds ratio (OR) = 0.35]. The adjusted MD for hemoglobin levels between SGLT2 inhibitor subjects and non-users was 7.0 g/L [97]. A corresponding meta-analysis reported that SGLT2 inhibitors significantly increased hemoglobin levels compared with placebo (P < 0.00001), and each SGLT2 inhibitor resulted in a notable increase in hematocrit levels (P < 0.00001) [98].
T2DM, cardiovascular and renal outcomes associated with SGLT2 inhibitors
Canagliflozin
Multiple clinical trials have shown that canagliflozin significantly reduces glycemic compared to placebo (Table 2). Canagliflozin showed non-inferiority compared to the active control group, especially canagliflozin 300 mg showed superiority and reduced FPG and SBP [99,100,101]. In the CALMER study, SGLT2 inhibitor combined with DPP-4 inhibitor significantly decreased glycemic variability compared with monotherapy [102].
FDA approval of canagliflozin for reducing the risk of heart attack, stroke or cardiovascular death in adults with T2DM and established cardiovascular disease was based on a consensus report from the ADA/European Association for the Study of Diabetes, these reports supported the use of canagliflozin in a broad range of patients. For T2DM patients with cardiovascular disease, the ADA recommends pharmacological management with SGLT2 inhibitors, which in particular have proven cardiovascular benefits [16, 103, 104]. The AACE also stated that canagliflozin has been shown to reduce MACE in suitable patients [16, 104].
The CANVAS program combined data from CANVAS and CANVAS-R, recruited 10,142 T2DM subjects with high cardiovascular risk [78, 85]. The CANVAS program aimed to evaluate the effect of canagliflozin on cardiovascular disease risk in patients with poorly controlled T2DM [105]. As a result, the incidence of the primary outcome was lower with canagliflozin compared to placebo [78]. HHF or cardiovascular death was reduced in the canagliflozin-treated group compared to placebo (HR = 0.78) [72].
Canagliflozin is FDA-approved to treat DKD and reduce the risk of HHF in T2DM patients with DKD based on CREDENCE. CREDENCE is the first renal outcome study to specifically address any SGLT2 inhibitor in addition to standard of care in T2DM patients with DKD [16]. However, CREDENCE was discontinued early following a planned interim analysis based on the recommendations of the data and safety monitoring board [70]. Canagliflozin reduced the risk of the primary outcome by 30% (P = 0.00001) [70]. The relative risk of the renal-specific composite risk of ESKD, dSCr, or renal death was decreased by 34%, and the relative risk of ESKD was reduced by 32% (P = 0.002) [70].
Empagliflozin
Among the currently used SGLT2 inhibitors, empagliflozin has the highest SGLT2 specificity. The low risk of hypoglycemia and weight loss properties of empagliflozin and its cardiovascular benefits support its use as a first-line alternative to metformin [106, 107].
Multiple randomized controlled trials demonstrated that compared with placebo, empagliflozin provided reducing in HbA1c, FPG and SBP, and weight loss (Table 2). The hypoglycemic efficacy of empagliflozin was noninferior to sitagliptin or glimepiride. Empagliflozin reduced SBP and body weight compared with sitagliptin. Empagliflozin 25 mg was better than sitagliptin in decreasing HbA1c [108,109,110,111,112,113].
Several randomized controlled trials have demonstrated the efficacy of empagliflozin as an add-on in patients with T2DM [114, 115]. One 104-week phase 3 trial compared the efficacy of empagliflozin and glimepiride as an add-on to metformin in T2DM [114]. The result was that empagliflozin was noninferior to glimepiride during treatment. The adjusted MD for change from baseline in HbA1c was − 0.11% [114].
The US FDA approved empagliflozin for reducing cardiovascular death in T2DM adults due to the wonderful outcomes in EMPA-REG OUTCOME [15, 69]. The primary composite outcome was nonfatal myocardial infarction, cardiovascular death, or nonfatal stroke. The primary outcome reported in 10.5% and 12.1% of patients in the empagliflozin group and the placebo group (HR = 0.86; P = 0.04), respectively. Cardiovascular death and HHF were obviously decreased in the empagliflozin group [69]. No significant between-group difference in the key secondary outcome (P = 0.08) [69]. Similar outcomes were shown in elderly patients [116].
Two randomized controlled trials have demonstrated empagliflozin for adults with HFrEF [62, 68]. FDA approval of empagliflozin in adults with HFrEF was based on the EMPEROR-Reduced trial [68]. The primary outcome was a composite of cardiovascular death or hospitalization for worsening HF. The primary outcome events reported in 19.4% and 24.7% of the empagliflozin group and the placebo group (HR = 0.75; P < 0.001), respectively. The effect of empagliflozin on the primary outcome of patients was consistent regardless of T2DM [68].
Recently, empagliflozin was approved for the treatment of HF with preserved ejection fraction in adults. The approval was based on outcomes from the landmark EMPEROR-Preserved trial [117]. The primary outcome of this trial was a composite of cardiovascular death or HHF, those reported in 13.8% and 17.1% of subjects in the empagliflozin group and the placebo group within a median of 26.2 months (HR = 0.79; P < 0.001), respectively. Empagliflozin exerted similar effects in T2DM or non-T2DM patients. The total number of HHF was lower in the empagliflozin group compared to placebo (P < 0.001) [117].
The long-term effect of empagliflozin on the kidneys was determined by investigators in the EMPA-REG OUTCOME and EMPEROR-Reduced trials [68, 86]. The incidence of kidney disease or worsening kidney disease was 12.7% in the empagliflozin group and 18.8% in the placebo group (HR = 0.61; P < 0.001). A dSCr in the empagliflozin group had an obviously lower relative risk of 44%. The relative risk of renal replacement therapy was reduced by 55% in the empagliflozin group. No significant between-group difference in the incidence of albuminuria [86]. Empire HF Renal was a prespecified sub-study of the investigator-initiated Empire HF trial to investigate the effect of empagliflozin on GFR, plasma volume, and extracellular volume in patients with HFrEF [118]. Empagliflozin therapy led to a reduction in estimated extracellular volume (adjusted MD − 0.12 L; P = 0.00056), estimated plasma volume (− 7.3%; P < 0.0001), and measured GFR (− 7.5 mL/min; P = 0.00010) compared to placebo [118].
Dapagliflozin
The hypoglycemic effect of dapagliflozin in randomized controlled trials was similar to that of previous SGLT-2 inhibitors (Table 2) [89, 119, 120]. Add-on therapy with dapagliflozin offered additional clinical benefits for patients with poorly controlled T2DM with sitagliptin or with or without metformin [120]. Compared with monotherapy, exenatide combined with dapagliflozin improved various glycemic parameters and cardiovascular risk factors in T2DM patients who were not adequately controlled by metformin [121]. Compared with pioglitazone, dapagliflozin showed non-inferiority in glycemic control [43]. Sitting SBP was notably lower in the dapagliflozin group compared with placebo (P = 0.0002) [89]. Its hypotensive properties are particularly beneficial in patients already receiving beta-blockers or calcium channel blockers [89].
The cardiovascular safety of dapagliflozin was established in the DECLARE–TIMI 58 trial. FDA approval of dapagliflozin for reducing the risk of HHF in patients with T2DM is based on this trial. The primary outcome of DECLARE–TIMI 58 was the composite of MACE. The primary efficacy outcomes were MACE and a composite of cardiovascular death or HHF [13]. Dapagliflozin met the prespecified non-inferiority criteria for MACE (P < 0.001). Dapagliflozin did not decrease the incidence of MACE (HR = 0.93) compared with placebo, while resulted in a reduction in cardiovascular death or HHF (4.9% vs. 5.8%; P = 0.005) [13].
Based on positive outcomes from the landmark DAPA-HF trial, the FDA approved dapagliflozin for cardiovascular death and HHF in patients with HFrEF [71]. Dapagliflozin achieved a statistically and clinically meaningful decrease in cardiovascular death or HHF compared with placebo [18, 71, 79]. The primary outcome was a composite of worsening HF or cardiovascular mortality and reported in 16.3% and 21.2% of patients in the dapagliflozin group and the placebo group (P < 0.001), respectively. A first worsening HF event occurred in 10.0% of patients in the dapagliflozin group and in 13.7% in the placebo group (HR = 0.70) [79]. Among patients without diabetes and with HbA1c levels below 5.7%, the primary outcome rate was 12.1% in dapagliflozin and 16.9% in placebo. Among patients with HbA1c ≥ 5.7%, the incidence of the primary outcome was 13.7% in dapagliflozin and 18.0% in placebo (HR = 0.74) [71].
FDA approval of dapagliflozin to teart CKD patients with or without risk of T2DM progression was based on positive results from the DAPA-CKD trial [122]. An independent data monitoring committee recommended stopping the trial because of efficacy. The incidence of the primary outcome event was 14.5% in the placebo group and 9.2% in the dapagliflozin group (P < 0.001). The HR for the composite of sustained at least 50% decline in eGFR, ESKD or death from renal causes was 0.56 (P < 0.001), and was 0.71 for death from cardiovascular causes or HHF (P = 0.009) [122]. 4.7% of patients in the dapagliflozin group and 6.8% of the placebo group (P = 0.004) occurred death [122].
Ertugliflozin
Ertugliflozin received its first FDA approval for T2DM on December 2017, based on positive outcomes from multiple randomized controlled trials. These trials demonstrated that ertugliflozin, alone or as an add-on, was superior to placebo in glycemic control in T2DM as a combination in patients receiving metformin and sitagliptin, provided reductions in HbA1c and FPG, SBP and body weight, with good tolerability. Ertugliflozin 5 mg has similar effects to ertugliflozin 15 mg, sometimes ertugliflozin 5 mg may be even more effective (Table 2) [123,124,125,126,127]. Treatment with ertugliflozin led to greater reductions in SBP or body weight compared to glimepiride, sitagliptin, or placebo.
The multicenter, double-blind trial VERTIS CV determined the effect of ertugliflozin on cardiovascular outcomes (Table 3) [11]. Cardiovascular death or HHF reported in 8.1% and 9.1% patients in the ertugliflozin group and the placebo group (P = 0.11), respectively. The HR for renal death, renal replacement therapy, or dSCr was 0.81 [11]. Ertugliflozin did not notably decrease first HHF or cardiovascular death (HR = 0.88). The risk reduction was greater with an ejection fraction ≤ 45% (HR = 0.48) versus an ejection fraction > 45% (HR = 0.86). Ertugliflozin decreased the risk of total HHF (RR = 0.70) and HHF/cardiovascular death (RR = 0.83) [74]. Ertugliflozin led to reducing in SBP, HbA1c, and body weight, maintained eGFR in patients with CKD stage 3A. Results were broadly similar in the CKD stage 3B subgroup, except for the diminished HbA1c response to ertugliflozin 15 mg [128].
Safety and tolerability
Several clinical trials involving SGLT-2 inhibitors in T2DM patients have shown more adverse reactions such as genital infections, amputations, DKA, and fractures in SGLT-2 inhibitor compared with placebo. There is little or no evidence of effects of SGLT-2 inhibitors on blindness, amputation, neuropathic pain, eye disease, or health-related quality of life in large meta-analyses [55, 129]. Compared with GLP-1 agonists, SGLT-2 inhibitors were related to a lower risk of adverse events resulted in patient withdrawal [75]. SGLT2 inhibitors significantly decreased the risk of all serious adverse events (HR = 0.91, P < 0.001) and acute kidney injury (AKI) (HR = 0.74; P < 0.001) [14]. A meta-analysis reported dose-independent adverse events with SGLT2 inhibitors [130]. Compared with controls or placebo, SGLT2 inhibitors did not increase the risk of acute pancreatitis [131].
Overall adverse events and adverse event-related discontinuation rates were generally similar between placebo, sitagliptin, glimepiride, and SGLT-2 inhibitors [99, 100]. However, canagliflozin 100 mg had a higher incidence of adverse events than placebo or sitagliptin [100]. The safety profile of empagliflozin was similar to sitagliptin or metformin, and most adverse events were mild or moderate in intensity [110]. Adverse events were similar between dapagliflozin and placebo, with few adverse events associated with volume depletion (< 1% vs. 0%) or renal function (1% vs < 1%) [89]. The most common adverse events related to dapagliflozin in DURATION-8 were diarrhea, injection site nodules, nausea, and urinary tract infection [121]. In DAPA-HF, the incidence of adverse reactions associated with volume depletion, renal insufficiency, as well as hypoglycemia did not differ between placebo and dapagliflozin [79]. The incidence of hypovolemia, symptomatic hypoglycemia, and urinary tract infection did not differ obviously between groups in patients receiving ertugliflozin compared with placebo or metformin [124, 125].
Genital infection or urinary tract infection
Both retrospective studies and meta-analyses have indicated that SGLT-2 inhibitors cause genital infections at a higher risk than other antidiabetic drugs [34, 53, 55, 129]. Safety analysis indicated a continued increase in the risk of genital infections associated with SGLT-2 inhibitors (relative risk, regulatory submission 4.75; Scientific Reports 2.88) [60].
Genital fungal infections adverse events have been associated with higher rates of canagliflozin, with a minority leading to treatment discontinuation [99, 100]. Empagliflozin has a higher risk of genital infection or urinary tract infection than placebo, metformin, or sitagliptin [109, 110, 117]. Increased rates of genital infections were more commonly reported in patients receiving empagliflozin in EMPA-REG OUTCOME and EMPEROR-Reduced trials [68, 69]. Common adverse reactions commonly reported with dapagliflozin in DURATION-8 included urinary tract infections [121]. Genital infections leading to treatment discontinuation or considered serious adverse events in DECLARE–TIMI 58 were more common in the dapagliflozin group (0.9% vs. 0.1%, P < 0.001) [13]. In VERTIS MONO, the incidence of female genital fungal infections was notably higher in the ertugliflozin group than in the placebo or metformin group. In men, the 15 mg group was significantly higher compared with placebo/metformin [124]. In VERTIS SITA2, compared with placebo (0–1.9%), female and male subjects receiving ertugliflozin (3.7–14.1%) had a higher incidence of genital fungal infections [125].
Osmotic diuresis
In CANTATA-SU, canagliflozin was related to a higher risk of osmotic diuresis-related events compared with glimepiride [99]. A meta-analysis reported that for osmotic diuresis, SGLT2 inhibitors notably increased the risk by 75% (P = 0.036). Subgroup analysis clarified that this effect was entirely attributable to the increase in patients with eGFR ≥ 60 ml/min/1.73 m2 [14].
Hypoglycemia
Meta-analysis results showed that the risk of hypoglycemia with SGLT-2 inhibitors was similar to that of other drugs [34, 124]. SGLT-2 inhibitors have a low hypoglycemia risk and are noninferior to placebo when used as monotherapy or combination therapy [8, 109, 119, 124].
Canagliflozin has a higher incidence of hypoglycemia compared with placebo or sitagliptin [100]. Compared with placebo, the incidence of symptomatic hypoglycemia was higher with ertugliflozin 15 mg [123]. Empagliflozin was related to a lower risk of hypoglycemia compared with glimepiride (2% vs. 24%, P < 0.0001) [114]. Hypoglycemic events associated with dapagliflozin were rare and not serious [119].
Sarcopenia
The mechanism of fat mass reduction with SGLT2 inhibitors is thought to be the result of lipolysis in adipose tissue due to activation of gluconeogenesis. However, activation of the gluconeogenesis system induces not only lipolysis in adipose tissue but also proteolysis in skeletal muscle, which supplies amino acids as substrates to the liver, thus leading to sarcopenia [132]. Weight loss and sarcopenia have also been reported in case reports with SGLT2 inhibitors [133].
Cancer
Data from a large meta-analysis suggested that dapagliflozin was related to an unbalanced incidence of breast and bladder cancer compared with controls [34]. However, two meta-analyses achieved similar outcomes [134, 135]. Results of a meta-analysis reported that SGLT2 inhibitors were not notably related to increased cancer risk compared with other antidiabetic drugs or placebo (OR = 1.14). For prespecified cancer types, use of SGLT2 inhibitors (OR = 3.87), especially empagliflozin (OR = 4.49), would increase bladder cancer incidence. Canagliflozin may be protective against gastrointestinal cancer (OR = 0.15) [135].
Of note, the EMPA-REG OUTCOME trial accounted for more than half of the individuals and events in the entire analysis [69, 135, 136]. In the intention-to-treat analysis, bladder cancer was reported in 0.2%, 0.1%, and 0.4% of patients in the placebo, empagliflozin 10 mg, and empagliflozin 25 mg groups, respectively [136]. When exposure time (6 months) was considered, the incidence was 0.2%, 0.1% and 0.3%, respectively. Overall, no evidence of an imbalance was observed in bladder cancer cases between empagliflozin and placebo [136].
Ketoacidosis
On December 4, 2015, a safety review by the US FDA resulted in the addition of a warning to the label of SGLT2 inhibitors, stating that there was too much acid in the blood [137]. On March 19, 2020, the FDA approved changes to the prescribing information for SGLT2 inhibitor diabetes medications to reduce the risk of DKA after surgery, recommending temporary discontinuation of these medications prior to scheduled surgery [137]. Normoglycemic DKA secondary to SGLT2 inhibitors in T2DM is a rare but increasingly reported phenomenon [138]. In DECLARE–TIMI 58, the incidence of DKA was higher in the dapagliflozin group than in the placebo group (0.3% vs. 0.1%, P = 0.02) [13]. In one cohort study, the incidence of DKA was 0.43 percent [138]. Normoglycemic DKA was most common in patients taking canagliflozin, followed by empagliflozin and dapagliflozin. Infection (32.6%) was the most common trigger for DKA, followed by insulin nonadherence (13.7%). Canagliflozin was most potently associated with the development of euglycemic DKA and was associated with the highest rate of medical intensive care unit admissions (66.6%) [138].
Several meta-analyses have indicated that SGLT2 inhibitors increased the risk of DKA [139, 140]. A meta-analysis indicated that SGLT2 inhibitors were statistically related to an increased risk of DKA compared with controls (0.18% vs. 0.09%, OR = 2.13) [140]. In contrast, another meta-analysis of 109 trials reported that SGLT2 inhibitors did not increase the risk of DKA (RR = 0.66) compared with placebo [129].
The above results concluded that SGLT2 inhibitors can increase the risk of DKA, despite a meta-analysis reported that SGLT2 inhibitors did not increase that. Additional evidence is two possible mechanisms have been proposed: free fatty acid production followed by conversion to ketone bodies; SGLT2 inhibitors stimulate glucagon secretion leading to the production of ketone bodies [129].
Fracture
The U.S. FDA strengthened the warning that canagliflozin was associated with an increased risk of fractures and added novel information about reducing bone mineral density [141].
Fracture risk assessment in CANVAS program in patients with T2DM and a history of cardiovascular disease who received canagliflozin or placebo showed 496 subjects who recorded ≥ 1 fracture event. There was obvious heterogeneity in the effects of CANVAS (HR = 1.55) and CANVAS-R (HR = 0.86) on fracture (P = 0.005) [142]. However, the fracture rate of canagliflozin was not significantly different from placebo in CREDENCE [70].
In recent years, multiple meta-analyses have reported no increased fracture risk with SGLT2 inhibitors compared with placebo [129, 143,144,145]. Canagliflozin was not related to an increased risk of fracture compared with GLP-1 agonists [146].
Canagliflozin was not included, although SGLT2 inhibitors did not increase fracture risk, according to the results of the meta-analysis. Users still need to heed the warnings from the FDA.
Amputation
In the CANVAS program, the risk of amputation associated with canagliflozin (HR = 1.97) was increased, with amputations mainly at the toe or metatarsal [78]. In VERTIS CV, 2.0% of patients receiving ertugliflozin 5 mg and 2.1% receiving ertugliflozin 15 mg underwent amputation compared with 1.6% receiving placebo [11]. Additionally, a large meta-analysis reported that canagliflozin increased the risk of amputation [12]. A meta-analysis of 14 trials indicated that SGLT2 inhibitors were not significantly related to an increased risk of diabetic foot syndrome compared with placebo (OR = 1.05). Amputation rates were increased in patients with T2DM who received canagliflozin but not empagliflozin [147]. Patients with atherosclerotic cardiovascular disease had a higher risk of amputation than those without atherosclerotic cardiovascular disease (RR 1.44 vs. 0.96, P = 0.066) [139].
There was no difference in amputation rates for canagliflozin in CREDENCE [70]. In OBSERVE-4D, the HR estimates for canagliflozin vs. no SGLT2 inhibitor for lower-knee and lower extremity amputations were 0.75 and 1.01 in an intention-to-treat analysis [76].
There were no obvious differences in amputation events by type of SGLT2 inhibitor, by baseline population, and by duration of SGLT2 inhibitor use [148].
There may be a risk of amputation following the use of SGLT2 inhibitors, usually in the toe or metatarsal, and limited to canagliflozin.
Acute kidney injury
Although SGLT2 inhibitors stabilize eGFR and reduce renal function progression and uric acid, the US FDA has strengthened existing warnings about the risk of AKI with canagliflozin and dapagliflozin and recommended to assess renal function before initiating canagliflozin or dapagliflozin, followed by periodic monitoring. In the event of AKI, the drug should be discontinued immediately and renal impairment treated [149].
In clinical studies, SGLT2 inhibitors had the lowest risk of AKI (5.59%) compared with other drugs and controls [150]. Several recent meta-analyses indicated that SGLT2 inhibitors can reduce the risk of AKI [151, 152]. A network meta-analysis of 18 studies including 156,690 patients with T2DM reported that SGLT2 inhibitors were related to a lower risk of AKI compared with placebo (OR = 0.76). Furthermore, SGLT2 inhibitors were significantly related to a reduced risk of AKI compared with GLP-1 receptor agonists (OR = 0.79) and DPP-4 inhibitors (OR = 0.68) [151].
A retrospective study showed AKI in 0.3% of patients receiving SGLT2 inhibitors. After adjustment, patients who developed AKI were more likely to be male, were ≥ 65 years old, had a lower body mass index, had a history of HF, and used diuretics more frequently than those who did not [153].
Both clinical studies and meta-analyses have shown that SGLT2 inhibitors are related to lower AKI, but patients are still at risk of developing AKI. There are three mechanisms by which SGLT2 inhibitors may increase the risk of AKI: decreased effective volume due to excessive diuresis; excessive drop in transglomerular pressure; induces renal medulla hypoxic injury, associated with enhanced distal tubular transport [129, 154].
SGLT2 inhibitor pharmacogenomics
SGLT2 is encoded by the SLC5A2 gene, which is located on chromosome 16 [155]. Since SGLTs reabsorbs approximately 90% of filtered glucose, SLC5A2 mutations may affect SGLT2 expression levels to affect the proportion of glucose reabsorption, resulting in familial renal glycosuria, which is characterized by isolated glucosuria without overt hyperglycemia [155]. Common genetic variants in SLC5A2 are associated with increased AUC120minglucose, increased AUCglucose and altered 30 min glucose levels in subjects with impaired glucose tolerance and impaired fasting glucose [155]. Currently, for SGLT2 inhibitors, studies have focused on genes that affect renal glucose reabsorption (e.g., SLC5A2), but have not found an association between SLC5A2 variants and response to empagliflozin [156]. Variations in the gene encoding SGLT2 are associated with the risk of generalized or sudden-onset HF. This association is mediated by distinct metabolic and physiological changes independent of the presence of T2DM or previous cardiovascular disease events [157].
Results from a meta-analysis showed that the rs9934336 G allele was nominally associated with increased 30-min plasma glucose, 120-min insulin concentration, and AUC120minglucose (P < 0.05) [158]. Another prospective study showed that variant rs9934336 was significantly associated with decreased HbA1c in T2DM patients (P = 0.023). rs9934336 was significantly negatively correlated with the presence of T2DM (P < 0.05) [159]. The polymorphisms rs3813008 and rs3116150 were neither associated with glycemic parameters nor with T2DM [159]. Common genetic variants in the SLC5A2 gene neither affect diabetes-related metabolic profiles nor response to SGLT2 inhibitor therapy [160]. Additionally, in a randomized controlled trial, weight loss with dapagliflozin plus exenatide was associated with the variant rs10010131 A allele [161].
SGLT2 inhibitors are metabolized in vivo by the uridine 5'-diphosphate glucuronyltransferase (UGT) isoform UGT1A9. In vitro studies have shown that UGT1A9 gene variants lead to altered UGT enzyme activity. Therefore, variations in the UGT gene may affect the pharmacokinetics of SGLT2 inhibitors [156, 162]. Plasma canagliflozin exposure (Cmax,ss, 11%; AUCτ,ss, 45%) was increased in UGT1A9*3 carriers relative to wild type. Increased plasma canagliflozin exposure was observed in participants with the UGT2B4*2 genotype compared with UGT2B4*2 non-carriers (Cmax,ss, 21%; AUCt,ss, 18%) [162]. Subjects with the UGT1A9*3 allele had a 26% higher exposure to canagliflozin than those without the allele [163]. Ertugliflozin is primarily metabolized by glucuronidation of UGT1A9. A meta-analysis showed that the largest changes in ertugliflozin AUC occurred in subjects carrying the UGT1A9*3 heterozygous variant. UGT1A9 genotype did not have any clinically meaningful effect on ertugliflozin exposure in healthy subjects [164].
A missense variant (I148M) in patatin-like phospholipase domain–containing protein 3 (PNPLA3) causes susceptibility to fatty liver disease [165]. PNPLA3 is expressed in liver and adipose tissue and mediates triacylglycerol hydrolysis [156, 166]. In the EFFECT-II trial, only dapagliflozin in combination with omega-3 (n-3) carboxylic acid reduced PDFF (P = 0.046) and total liver fat volume (relative -24%, P = 0.037) compared with placebo. There was an interaction between the PNPLA3 I148M polymorphism and changes in hepatic PDFF in the active treatment group (P = 0.03) [166].
Conclusions
In conclusion, SGLT2 inhibitors could manage uncontrolled glycemic in patients with T2DM who have received prior metformin, with a safety profile similar to placebo or other hypoglycemic agents (e.g., sitagliptin). SGLT2 inhibitors do not affect insulin secretion but have been clinically shown to improve β-cell function and improve insulin sensitivity. The effect of SGLT2 inhibitor on blood lipids is manifested as the increase of LDL and HDL, and the decrease of triglyceride. Compared with pioglitazone, SGLT2 inhibitors significantly reduced the fatty liver index, which means that SGLT2 inhibitors can be preferred drugs for T2DM patients with NAFLD. The cardiovascular benefits (e.g., HHF and cardiovascular death) of SGLT2 inhibitors are diverse, and the mechanisms are partially elucidated. However, the effect of SGLT-2 inhibitors on the risk of non-fatal stroke or myocardial infarction was neutral. SGLT2 inhibitors have been clearly shown in multiple trials to improve renal outcomes in patients with CKD or DKD, improve glomerular hemodynamic function, and significantly decrease the risk of proteinuria and renal failure. Although empagliflozin is not currently approved for this use, the results of the EMPA-REG OUTCOME and EMPEROR-Reduced trials are positive. SGLT2 inhibitors were also able to reduce all-cause mortality. SGLT2 inhibitors increased hemoglobin levels and prevented the occurrence of anemia events. To date, information on the role of genetic polymorphisms in response to SGLT-2 inhibitors is rather limited, and the mechanisms underlying the effects require more studies to reveal.
Genital or urinary tract infections, amputations, fractures (canagliflozin), osmotic diuresis, ketoacidosis, sarcopenia and hypotension are common with SGLT2 inhibitors. SGLT2 inhibitors have a lower risk of hypoglycemia than glimepiride. The FDA has also issued a safety warning for canagliflozin and dapagliflozin, which may cause AKI or fractures. The balance of benefits and risks and risk mitigation strategies for SGLT2 inhibitors should be carefully considered [82].
Availability of data and materials
Not applicable.
Code availability
Not applicable.
Abbreviations
- T2DM:
-
Type 2 diabetes mellitus
- SGLT2:
-
Sodium-glucose cotransporter 2
- EGP:
-
Endogenous glucose production
- HF:
-
Heart failure
- DKD:
-
Diabetic kidney disease
- ESKD:
-
End-stage kidney disease
- ADA:
-
American Diabetes Association
- AACE:
-
American Association of Clinical Endocrinologists
- HbA1c:
-
Glycated hemoglobin
- GLP1:
-
Glucagon-like peptide 1
- DKA:
-
Diabetic ketoacidosis
- CKD:
-
Chronic kidney disease
- HFrEF:
-
HF with reduced ejection fraction
- HHF:
-
Hospitalization for heart failure
- MD:
-
Mean difference
- SBP:
-
Systolic blood pressure
- RR:
-
Ratio risk
- OR:
-
Odds ratio
- HR:
-
Hazard ratio
- NAFLD:
-
Nonalcoholic fatty liver disease
- PDFF:
-
Proton density fat fraction
- ALT:
-
Alanine aminotransferase
- MACE:
-
Major adverse cardiovascular events
- FPG:
-
Fasting plasma glucose
- NT-proBNP:
-
N-terminal pre-B-type natriuretic peptide
- eGFR:
-
Estimated glomerular filtration rate
- dSCr:
-
Doubling of serum creatinine
- AKI:
-
Acute kidney injury
- UGT:
-
Uridine 5ʹ-diphosphate glucuronyltransferase
- PNPLA3:
-
Patatin-like phospholipase domain–containing protein 3
References
Taylor SI, Yazdi ZS, Beitelshees AL. Pharmacological treatment of hyperglycemia in type 2 diabetes. J Clin Invest. 2021;131(2): e142243.
Yoon KH, Lee JH, Kim JW, et al. Epidemic obesity and type 2 diabetes in Asia. Lancet. 2006;368(9548):1681–8.
Marx N, Davies MJ, Grant PJ, et al. Guideline recommendations and the positioning of newer drugs in type 2 diabetes care. Lancet Diabetes Endocrinol. 2021;9(1):46–52.
Bonner C, Kerr-Conte J, Gmyr V, et al. Inhibition of the glucose transporter SGLT2 with dapagliflozin in pancreatic alpha cells triggers glucagon secretion. Nat Med. 2015;21(5):512–7.
Khoo CM, Deerochanawong C, Chan SP, et al. Use of sodium-glucose co-transporter-2 inhibitors in Asian patients with type 2 diabetes and kidney disease: an Asian perspective and expert recommendations. Diabetes Obes Metab. 2021;23(2):299–317.
Thrasher J. Pharmacologic management of type 2 diabetes mellitus: available therapies. Am J Cardiol. 2017;120(1S):S4–16.
Giugliano D, Longo M, Scappaticcio L, Caruso P, Esposito K. Sodium-glucose transporter-2 inhibitors for prevention and treatment of cardiorenal complications of type 2 diabetes. Cardiovasc Diabetol. 2021;20(1):17.
Saisho Y. SGLT2 inhibitors: the star in the treatment of type 2 diabetes? Diseases. 2020;8(2):14.
U.S. Food and Drug Administration. Sodium-glucose cotransporter-2 (SGLT2) inhibitors. Silver Spring: U.S. Food and Drug Administration; 2016.
Bloomgarden Z, Handelsman Y. Management and prevention of cardiovascular disease for type 2 diabetes: integrating the diabetes management recommendations of AACE, ADA, EASD, AHA, ACC, and ESC. Am J Prev Cardiol. 2020;1: 100007.
Cannon CP, Pratley R, Dagogo-Jack S, et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N Engl J Med. 2020;383(15):1425–35.
Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med. 2020;173(4):278–86.
Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
Bai Y, Jin J, Zhou W, Zhang S, Xu J. The safety outcomes of sodium-glucose cotransporter 2 inhibitors in patients with different renal function: a systematic review and meta-analysis. Nutr Metab Cardiovasc Dis. 2021;31(5):1365–74.
Jardiance. JardianceTM press releases. Boehringer Ingelheim; 2014.
LLC. InvokanaTM press releases. Raritan: Janssen Research & Development; 2020.
Steglatro. SteglatroTM press releases. Darmstadt: Merck; 2017.
Farxiga. FarxigaTM press releases. Cambridge: AstraZeneca; 2021.
Jardiance. JardianceTM prescribing information. Indianapolis: Eli Lilly; 2014.
Chen LH, Leung PS. Inhibition of the sodium glucose co-transporter-2: its beneficial action and potential combination therapy for type 2 diabetes mellitus. Diabetes Obes Metab. 2013;15(5):392–402.
Steglatro. SteglatroTM prescribing information. Darmstadt: Merck; 2017.
Dhillon S. Dapagliflozin: a review in type 2 diabetes. Drugs. 2019;79(10):1135–46.
Elkinson S, Scott LJ. Canagliflozin: first global approval. Drugs. 2013;73(9):979–88.
Markham A. Ertugliflozin: first global approval. Drugs. 2018;78(4):513–9.
Scott LJ. Empagliflozin: a review of its use in patients with type 2 diabetes mellitus. Drugs. 2014;74(15):1769–84.
Plosker GL. Dapagliflozin: a review of its use in patients with type 2 diabetes. Drugs. 2014;74(18):2191–209.
LLC. InvokanaTM prescribing information. Raritan: Janssen Research & Development; 2020.
Fonseca-Correa JI, Correa-Rotter R. Sodium-glucose cotransporter 2 inhibitors mechanisms of action: a review. Front Med. 2021;8: 777861.
Suga T, Kikuchi O, Kobayashi M, et al. SGLT1 in pancreatic α cells regulates glucagon secretion in mice, possibly explaining the distinct effects of SGLT2 inhibitors on plasma glucagon levels. Mol Metab. 2019;19:1–12.
Garvey WT, Van Gaal L, Leiter LA, et al. Effects of canagliflozin versus glimepiride on adipokines and inflammatory biomarkers in type 2 diabetes. Metabolism. 2018;85:32–7.
Mudaliar S, Henry RR, Boden G, et al. Changes in insulin sensitivity and insulin secretion with the sodium glucose cotransporter 2 inhibitor dapagliflozin. Diabetes Technol Ther. 2014;16(3):137–44.
Milonas D, Tziomalos K. Sodium-glucose cotransporter 2 inhibitors and ischemic stroke. Cardiovasc Hematol Disord Drug Targets. 2018;18(2):134–8.
Li D, Wu T, Wang T, et al. Effects of sodium glucose cotransporter 2 inhibitors on risk of dyslipidemia among patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Pharmacoepidemiol Drug Saf. 2020;29(5):582–90.
Vasilakou D, Karagiannis T, Athanasiadou E, et al. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2013;159(4):262–74.
Ferrannini E, Muscelli E, Frascerra S, et al. Metabolic response to sodium-glucose cotransporter 2 inhibition in type 2 diabetic patients. J Clin Invest. 2014;124(2):499–508.
Kullmann S, Hummel J, Wagner R, et al. Empagliflozin improves insulin sensitivity of the hypothalamus in humans with prediabetes: a randomized, double-blind, placebo-controlled, phase 2 trial. Diabetes Care. 2021. https://doi.org/10.2337/dc21-1136.
Hayashi T, Fukui T, Nakanishi N, et al. Dapagliflozin decreases small dense low-density lipoprotein-cholesterol and increases high-density lipoprotein 2-cholesterol in patients with type 2 diabetes: comparison with sitagliptin. Cardiovasc Diabetol. 2017;16(1):8.
Kuchay MS, Krishan S, Mishra SK, et al. Effect of empagliflozin on liver fat in patients with type 2 diabetes and nonalcoholic fatty liver disease: a randomized controlled trial (E-LIFT Trial). Diabetes Care. 2018;41(8):1801–8.
Sumida Y, Yoneda M, Tokushige K, et al. Antidiabetic therapy in the treatment of nonalcoholic steatohepatitis. Int J Mol Sci. 2020;21(6):1907.
Jung CH, Mok JO. The effects of hypoglycemic agents on non-alcoholic fatty liver disease: focused on sodium-glucose cotransporter 2 inhibitors and glucagon-like peptide-1 receptor agonists. J Obes Metab Syndr. 2019;28(1):18–29.
Wong C, Yaow CYL, Ng CH, et al. Sodium-glucose co-transporter 2 inhibitors for non-alcoholic fatty liver disease in asian patients with type 2 diabetes: a meta-analysis. Front Endocrinol. 2021;11: 609135.
Mantovani A, Petracca G, Csermely A, Beatrice G, Targher G. Sodium-glucose cotransporter-2 inhibitors for treatment of nonalcoholic fatty liver disease: a meta-analysis of randomized controlled trials. Metabolites. 2020;11(1):22.
Cho KY, Nakamura A, Omori K, et al. Favorable effect of sodium-glucose cotransporter 2 inhibitor, dapagliflozin, on non-alcoholic fatty liver disease compared with pioglitazone. J Diabetes Investig. 2021;12(7):1272–7.
Lopaschuk GD, Verma S. Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: a state-of-the-art review. JACC Basic Transl Sci. 2020;5(6):632–44.
Tanaka A, Shimabukuro M, Machii N, et al. Secondary analyses to assess the profound effects of empagliflozin on endothelial function in patients with type 2 diabetes and established cardiovascular diseases: the placebo-controlled double-blind randomized effect of empagliflozin on endothelial function in cardiovascular high risk diabetes mellitus: multi-center placebo-controlled double-blind randomized trial. J Diabetes Investig. 2020;11(6):1551–63.
Ghanim H, Batra M, Green K, et al. Dapagliflozin reduces systolic blood pressure and modulates vasoactive factors. Diabetes Obes Metab. 2021;23(7):1614–23.
Marfella R, D’Onofrio N, Trotta MC, et al. Sodium/glucose cotransporter 2 (SGLT2) inhibitors improve cardiac function by reducing JunD expression in human diabetic hearts. Metabolism. 2021;127: 154936.
Verma S, Mazer CD, Yan AT, et al. Effect of empagliflozin on left ventricular mass in patients with type 2 diabetes mellitus and coronary artery disease: the EMPA-HEART CardioLink-6 Randomized Clinical Trial. Circulation. 2019;140(21):1693–702.
Mason T, Coelho-Filho OR, Verma S, et al. Empagliflozin reduces myocardial extracellular volume in patients with type 2 diabetes and coronary artery disease. JACC Cardiovasc Imaging. 2021;14(6):1164–73.
Mahaffey KW, Neal B, Perkovic V, et al. Canagliflozin for primary and secondary prevention of cardiovascular events: results from the CANVAS program (Canagliflozin Cardiovascular Assessment Study). Circulation. 2018;137(4):323–34.
Fuchigami A, Shigiyama F, Kitazawa T, et al. Efficacy of dapagliflozin versus sitagliptin on cardiometabolic risk factors in Japanese patients with type 2 diabetes: a prospective, randomized study (DIVERSITY-CVR). Cardiovasc Diabetol. 2020;19(1):1.
Inzucchi SE, Zinman B, Fitchett D, et al. How does empagliflozin reduce cardiovascular mortality? Insights from a mediation analysis of the EMPA-REG OUTCOME trial. Diabetes Care. 2018;41(2):356–63.
Han SJ, Ha KH, Lee N, Kim DJ. Effectiveness and safety of sodium-glucose co-transporter-2 inhibitors compared with dipeptidyl peptidase-4 inhibitors in older adults with type 2 diabetes: a nationwide population-based study. Diabetes Obes Metab. 2021;23(3):682–91.
Filion KB, Lix LM, Yu OH, et al. Sodium glucose cotransporter 2 inhibitors and risk of major adverse cardiovascular events: multi-database retrospective cohort study. BMJ. 2020;370: m3342.
Palmer SC, Tendal B, Mustafa RA, et al. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2021;372: m4573.
Wei XB, Wei W, Ding LL, Liu SY. Comparison of the effects of 10 GLP-1 RA and SGLT2 inhibitor interventions on cardiovascular, mortality, and kidney outcomes in type 2 diabetes: a network meta-analysis of large randomized trials. Prim Care Diabetes. 2021;15(2):208–11.
Yamada T, Wakabayashi M, Bhalla A, et al. Cardiovascular and renal outcomes with SGLT-2 inhibitors versus GLP-1 receptor agonists in patients with type 2 diabetes mellitus and chronic kidney disease: a systematic review and network meta-analysis. Cardiovasc Diabetol. 2021;20(1):14.
Li HL, Lip GYH, Feng Q, et al. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) and cardiac arrhythmias: a systematic review and meta-analysis. Cardiovasc Diabetol. 2021;20(1):100.
Usman MS, Siddiqi TJ, Memon MM, et al. Sodium-glucose co-transporter 2 inhibitors and cardiovascular outcomes: a systematic review and meta-analysis. Eur J Prev Cardiol. 2018;25(5):495–502.
Wu JH, Foote C, Blomster J, et al. Effects of sodium-glucose cotransporter-2 inhibitors on cardiovascular events, death, and major safety outcomes in adults with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2016;4(5):411–9.
Zelniker TA, Wiviott SD, Raz I, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31–9.
Lee MMY, Brooksbank KJM, Wetherall K, et al. Effect of empagliflozin on left ventricular volumes in patients with type 2 diabetes, or prediabetes, and heart failure with reduced ejection fraction (SUGAR-DM-HF). Circulation. 2021;143(6):516–25.
Nassif ME, Windsor SL, Tang F, et al. Dapagliflozin effects on lung fluid volumes in patients with heart failure and reduced ejection fraction: results from the DEFINE-HF trial. Diabetes Obes Metab. 2021;23(6):1426–30.
Januzzi JL Jr, Xu J, Li J, et al. Effects of canagliflozin on amino-terminal pro-B-type natriuretic peptide: implications for cardiovascular risk reduction. J Am Coll Cardiol. 2020;76(18):2076–85.
Yu YW, Zhao XM, Wang YH, et al. Effect of sodium-glucose cotransporter 2 inhibitors on cardiac structure and function in type 2 diabetes mellitus patients with or without chronic heart failure: a meta-analysis. Cardiovasc Diabetol. 2021;20(1):25.
Kolijn D, Pabel S, Tian Y, et al. Empagliflozin improves endothelial and cardiomyocyte function in human heart failure with preserved ejection fraction via reduced pro-inflammatory-oxidative pathways and protein kinase Gα oxidation. Cardiovasc Res. 2021;117(2):495–507.
Kosiborod M, Cavender MA, Fu AZ, et al. Lower risk of heart failure and death in patients initiated on sodium-glucose cotransporter-2 inhibitors versus other glucose-lowering drugs: the CVD-REAL Study (comparative effectiveness of cardiovascular outcomes in new users of sodium-glucose cotransporter-2 inhibitors). Circulation. 2017;136(3):249–59.
Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–24.
Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–28.
Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–306.
Petrie MC, Verma S, Docherty KF, et al. Effect of dapagliflozin on worsening heart failure and cardiovascular death in patients with heart failure with and without diabetes. JAMA. 2020;323(14):1353–68.
Rådholm K, Figtree G, Perkovic V, et al. Canagliflozin and heart failure in type 2 diabetes mellitus: results from the CANVAS Program. Circulation. 2018;138(5):458–68.
Dewan P, Docherty KF, Bengtsson O, et al. Effects of dapagliflozin in heart failure with reduced ejection fraction and chronic obstructive pulmonary disease: an analysis of DAPA-HF. Eur J Heart Fail. 2021;23(4):632–43.
Cosentino F, Cannon CP, Cherney DZI, et al. Efficacy of ertugliflozin on heart failure-related events in patients with type 2 diabetes mellitus and established atherosclerotic cardiovascular disease: results of the VERTIS CV trial. Circulation. 2020;142(23):2205–15.
Zheng SL, Roddick AJ, Aghar-Jaffar R, et al. Association between use of sodium-glucose cotransporter 2 inhibitors, glucagon-like peptide 1 agonists, and dipeptidyl peptidase 4 inhibitors with all-cause mortality in patients with type 2 diabetes: a systematic review and meta-analysis. JAMA. 2018;319(15):1580–91.
Ryan PB, Buse JB, Schuemie MJ, et al. Comparative effectiveness of canagliflozin, SGLT2 inhibitors and non-SGLT2 inhibitors on the risk of hospitalization for heart failure and amputation in patients with type 2 diabetes mellitus: a real-world meta-analysis of 4 observational databases (OBSERVE-4D). Diabetes Obes Metab. 2018;20(11):2585–97.
Giugliano D, Longo M, Signoriello S, et al. The effect of DPP-4 inhibitors, GLP-1 receptor agonists and SGLT-2 inhibitors on cardiorenal outcomes: a network meta-analysis of 23 CVOTs. Cardiovasc Diabetol. 2022;21(1):42.
Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–57.
McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008.
Okunrintemi V, Mishriky BM, Powell JR, Cummings DM. Sodium-glucose co-transporter-2 inhibitors and atrial fibrillation in the cardiovascular and renal outcome trials. Diabetes Obes Metab. 2021;23(1):276–80.
Zhou Z, Jardine MJ, Li Q, et al. Effect of SGLT2 inhibitors on stroke and atrial fibrillation in diabetic kidney disease: results from the CREDENCE trial and meta-analysis. Stroke. 2021;52(5):1545–56.
Tuttle KR, Brosius FC 3rd, Cavender MA, et al. SGLT2 inhibition for CKD and cardiovascular disease in type 2 diabetes: report of a scientific workshop sponsored by the National Kidney Foundation. Am J Kidney Dis. 2021;77(1):94–109.
Piperidou A, Loutradis C, Sarafidis P. SGLT-2 inhibitors and nephroprotection: current evidence and future perspectives. J Hum Hypertens. 2021;35(1):12–25.
Oshima M, Jardine MJ, Agarwal R, et al. Insights from CREDENCE trial indicate an acute drop in estimated glomerular filtration rate during treatment with canagliflozin with implications for clinical practice. Kidney Int. 2021;99(4):999–1009.
Perkovic V, de Zeeuw D, Mahaffey KW, et al. Canagliflozin and renal outcomes in type 2 diabetes: results from the CANVAS Program randomised clinical trials. Lancet Diabetes Endocrinol. 2018;6(9):691–704.
Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–34.
Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation. 2016;134(10):752–72.
Mozawa K, Kubota Y, Hoshika Y, et al. Empagliflozin confers reno-protection in acute myocardial infarction and type 2 diabetes mellitus. ESC Heart Fail. 2021;8(5):4161–73.
Weber MA, Mansfield TA, Cain VA, Iqbal N, Parikh S, Ptaszynska A. Blood pressure and glycaemic effects of dapagliflozin versus placebo in patients with type 2 diabetes on combination antihypertensive therapy: a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Diabetes Endocrinol. 2016;4(3):211–20.
Barnett AH, Mithal A, Manassie J, et al. Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease: a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014;2(5):369–84.
Fioretto P, Stefansson BV, Johnsson E, Cain VA, Sjöström CD. Dapagliflozin reduces albuminuria over 2 years in patients with type 2 diabetes mellitus and renal impairment. Diabetologia. 2016;59(9):2036–9.
Heerspink HJ, Desai M, Jardine M, Balis D, Meininger G, Perkovic V. Canagliflozin slows progression of renal function decline independently of glycemic effects. J Am Soc Nephrol. 2017;28(1):368–75.
Mosenzon O, Wiviott SD, Cahn A, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606–17.
Wheeler DC, Stefánsson BV, Jongs N, et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9(1):22–31.
Silverii GA, Monami M, Mannucci E. Sodium-glucose co-transporter-2 inhibitors and all-cause mortality: a meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2021;23(4):1052–6.
Oshima M, Neuen BL, Jardine MJ, et al. Effects of canagliflozin on anaemia in patients with type 2 diabetes and chronic kidney disease: a post-hoc analysis from the CREDENCE trial. Lancet Diabetes Endocrinol. 2020;8(11):903–14.
Murashima M, Tanaka T, Kasugai T, et al. Sodium-glucose cotransporter 2 inhibitors and anemia among diabetes patients in real clinical practice. J Diabetes Investig. 2021. https://doi.org/10.1111/jdi.13717.
Kanbay M, Tapoi L, Ureche C, et al. Effect of sodium-glucose cotransporter 2 inhibitors on hemoglobin and hematocrit levels in type 2 diabetes: a systematic review and meta-analysis. Int Urol Nephrol. 2021. https://doi.org/10.1007/s11255-021-02943-2.
Cefalu WT, Leiter LA, Yoon KH, et al. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet. 2013;382(9896):941–50.
Lavalle-González FJ, Januszewicz A, Davidson J, et al. Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial. Diabetologia. 2013;56(12):2582–92.
Bode B, Stenlöf K, Sullivan D, Fung A, Usiskin K. Efficacy and safety of canagliflozin treatment in older subjects with type 2 diabetes mellitus: a randomized trial. Hosp Pract. 2013;41(2):72–84.
Cho KY, Nomoto H, Nakamura A, et al. Favourable effect of the sodium-glucose co-transporter-2 inhibitor canagliflozin plus the dipeptidyl peptidase-4 inhibitor teneligliptin in combination on glycaemic fluctuation: an open-label, prospective, randomized, parallel-group comparison trial (the CALMER study). Diabetes Obes Metab. 2020;22(3):458–62.
Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669–701.
Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the american association of clinical endocrinologists and american college of endocrinology on the comprehensive type 2 diabetes management algorithm—2018 executive summary. Endocr Pract. 2018;24(1):91–120.
Neal B, Perkovic V, de Zeeuw D, et al. Rationale, design, and baseline characteristics of the Canagliflozin Cardiovascular Assessment Study (CANVAS)–a randomized placebo-controlled trial. Am Heart J. 2013;166(2):217-223.e11.
Chawla G, Chaudhary KK. A complete review of empagliflozin: most specific and potent SGLT2 inhibitor used for the treatment of type 2 diabetes mellitus. Diabetes Metab Syndr. 2019;13(3):2001–8.
Levine MJ. Empagliflozin for type 2 diabetes mellitus: an overview of phase 3 clinical trials. Curr Diabetes Rev. 2017;13(4):405–23.
Roden M, Weng J, Eilbracht J, et al. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013;1(3):208–19.
Roden M, Merker L, Christiansen AV, et al. Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naïve patients with type 2 diabetes: a double-blind extension of a Phase III randomized controlled trial. Cardiovasc Diabetol. 2015;14:154.
Ferrannini E, Berk A, Hantel S, et al. Long-term safety and efficacy of empagliflozin, sitagliptin, and metformin: an active-controlled, parallel-group, randomized, 78-week open-label extension study in patients with type 2 diabetes. Diabetes Care. 2013;36(12):4015–21.
Kadowaki T, Haneda M, Inagaki N, et al. Efficacy and safety of empagliflozin monotherapy for 52 weeks in Japanese patients with type 2 diabetes: a randomized, double-blind, parallel-group study. Adv Ther. 2015;32(4):306–18.
Nishimura R, Tanaka Y, Koiwai K, et al. Effect of empagliflozin monotherapy on postprandial glucose and 24-hour glucose variability in Japanese patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled, 4-week study. Cardiovasc Diabetol. 2015;14:11.
Tikkanen I, Narko K, Zeller C, et al. Empagliflozin reduces blood pressure in patients with type 2 diabetes and hypertension. Diabetes Care. 2015;38(3):420–8.
Ridderstråle M, Andersen KR, Zeller C, et al. Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: a 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol. 2014;2(9):691–700.
Babar M, Hussain M, Ahmad M, Akhtar L. Comparison Of efficacy and safety profile of empagliflozin as a combination therapy in obese type 2 diabetic patients. J Ayub Med Coll Abbottabad. 2021;33(2):188–91.
Monteiro P, Bergenstal RM, Toural E, et al. Efficacy and safety of empagliflozin in older patients in the EMPA-REG OUTCOME® trial. Age Ageing. 2019;48(6):859–66.
Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–61.
Jensen J, Omar M, Kistorp C, et al. Effects of empagliflozin on estimated extracellular volume, estimated plasma volume, and measured glomerular filtration rate in patients with heart failure (Empire HF Renal): a prespecified substudy of a double-blind, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2021;9(2):106–16.
Bailey CJ, Gross JL, Hennicken D, Iqbal N, Mansfield TA, List JF. Dapagliflozin add-on to metformin in type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled 102-week trial. BMC Med. 2013;11:43.
Jabbour SA, Hardy E, Sugg J, Parikh S, Study 10 Group. Dapagliflozin is effective as add-on therapy to sitagliptin with or without metformin: a 24-week, multicenter, randomized, double-blind, placebo-controlled study. Diabetes Care. 2014;37(3):740–50.
Frías JP, Guja C, Hardy E, et al. Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with type 2 diabetes inadequately controlled with metformin monotherapy (DURATION-8): a 28 week, multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol. 2016;4(12):1004–16.
Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–46.
Ji L, Liu Y, Miao H, et al. Safety and efficacy of ertugliflozin in Asian patients with type 2 diabetes mellitus inadequately controlled with metformin monotherapy: VERTIS Asia. Diabetes Obes Metab. 2019;21(6):1474–82.
Aronson R, Frias J, Goldman A, Darekar A, Lauring B, Terra SG. Long-term efficacy and safety of ertugliflozin monotherapy in patients with inadequately controlled T2DM despite diet and exercise: VERTIS MONO extension study. Diabetes Obes Metab. 2018;20(6):1453–60.
Dagogo-Jack S, Liu J, Eldor R, et al. Efficacy and safety of the addition of ertugliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sitagliptin: the VERTIS SITA2 placebo-controlled randomized study. Diabetes Obes Metab. 2018;20(3):530–40.
Gallo S, Charbonnel B, Goldman A, et al. Long-term efficacy and safety of ertugliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin monotherapy: 104-week VERTIS MET trial. Diabetes Obes Metab. 2019;21(4):1027–36.
Pratley RE, Eldor R, Raji A, et al. Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with type 2 diabetes mellitus inadequately controlled with metformin: the VERTIS FACTORIAL randomized trial. Diabetes Obes Metab. 2018;20(5):1111–20.
Dagogo-Jack S, Pratley RE, Cherney DZI, et al. Glycemic efficacy and safety of the SGLT2 inhibitor ertugliflozin in patients with type 2 diabetes and stage 3 chronic kidney disease: an analysis from the VERTIS CV randomized trial. BMJ Open Diabetes Res Care. 2021;9(1): e002484.
Donnan JR, Grandy CA, Chibrikov E, et al. Comparative safety of the sodium glucose co-transporter 2 (SGLT2) inhibitors: a systematic review and meta-analysis. BMJ Open. 2019;9(1): e022577.
Shi FH, Li H, Yue J, et al. Clinical adverse events of high-dose vs. low-dose sodium-glucose cotransporter 2 inhibitors in type 2 diabetes: a meta-analysis of 51 randomized clinical trials. J Clin Endocrinol Metab. 2020;105(11):dgaa586.
Tang H, Yang K, Li X, Song Y, Han J. Pancreatic safety of sodium-glucose cotransporter 2 inhibitors in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Pharmacoepidemiol Drug Saf. 2020;29(2):161–72.
Sasaki T. Sarcopenia, frailty circle and treatment with sodium-glucose cotransporter 2 inhibitors. J Diabetes Investig. 2019;10(2):193–5.
Yasuda M, Iizuka K, Kato T, et al. Sodium-glucose cotransporter 2 inhibitor and sarcopenia in a lean elderly adult with type 2 diabetes: a case report. J Diabetes Investig. 2020;11(3):745–7.
Pelletier R, Ng K, Alkabbani W, Labib Y, Mourad N, Gamble JM. The association of sodium-glucose cotransporter 2 inhibitors with cancer: an overview of quantitative systematic reviews. Endocrinol Diabetes Metab. 2020;3(3): e00145.
Tang H, Dai Q, Shi W, Zhai S, Song Y, Han J. SGLT2 inhibitors and risk of cancer in type 2 diabetes: a systematic review and meta-analysis of randomised controlled trials. Diabetologia. 2017;60(10):1862–72.
Kohler S, Lee J, George JT, Inzucchi SE, Zinman B. Bladder cancer in the EMPA-REG OUTCOME trial. Diabetologia. 2017;60(12):2534–5.
U.S. Food and Drug Administration. FDA revises labels of SGLT2 inhibitors for diabetes to include warnings about too much acid in the blood and serious urinary tract infections. Silver Spring: U.S. Food and Drug Administration; 2016.
Ata F, Yousaf Z, Khan AA, et al. SGLT-2 inhibitors associated euglycemic and hyperglycemic DKA in a multicentric cohort. Sci Rep. 2021;11(1):10293.
Lin DS, Lee JK, Chen WJ. Clinical adverse events associated with sodium-glucose cotransporter 2 inhibitors: a meta-analysis involving 10 randomized clinical trials and 71 553 individuals. J Clin Endocrinol Metab. 2021;106(7):2133–45.
Liu J, Li L, Li S, et al. Sodium-glucose co-transporter-2 inhibitors and the risk of diabetic ketoacidosis in patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2020;22(9):1619–27.
U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA revises label of diabetes drug canagliflozin (Invokana, Invokamet) to include updates on bone fracture risk and new information on decreased bone mineral density. Silver Spring: U.S. Food and Drug Administration; 2016.
Zhou Z, Jardine M, Perkovic V, et al. Canagliflozin and fracture risk in individuals with type 2 diabetes: results from the CANVAS Program. Diabetologia. 2019;62(10):1854–67.
Cheng L, Li YY, Hu W, et al. Risk of bone fracture associated with sodium-glucose cotransporter-2 inhibitor treatment: a meta-analysis of randomized controlled trials. Diabetes Metab. 2019;45(5):436–45.
Ruanpeng D, Ungprasert P, Sangtian J, Harindhanavudhi T. Sodium-glucose cotransporter 2 (SGLT2) inhibitors and fracture risk in patients with type 2 diabetes mellitus: a meta-analysis. Diabetes Metab Res Rev. 2017. https://doi.org/10.1002/dmrr.2903.
Tang HL, Li DD, Zhang JJ, et al. Lack of evidence for a harmful effect of sodium-glucose co-transporter 2 (SGLT2) inhibitors on fracture risk among type 2 diabetes patients: a network and cumulative meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2016;18(12):1199–206.
Fralick M, Kim SC, Schneeweiss S, Kim D, Redelmeier DA, Patorno E. Fracture risk after initiation of use of canagliflozin: a cohort study. Ann Intern Med. 2019;170(3):155–63.
Li D, Yang JY, Wang T, Shen S, Tang H. Risks of diabetic foot syndrome and amputation associated with sodium glucose co-transporter 2 inhibitors: a meta-analysis of randomized controlled trials. Diabetes Metab. 2018;44(5):410–4.
See RM, Teo YN, Teo YH, et al. Effects of sodium-glucose cotransporter 2 on amputation events: a systematic review and meta-analysis of randomized-controlled trials. Pharmacology. 2021. https://doi.org/10.1159/000520903.
U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA strengthens kidney warnings for diabetes medicines canagliflozin (Invokana, Invokamet) and dapagliflozin (Farxiga, Xigduo XR). Silver Spring: U.S. Food and Drug Administration; 2016.
Shen L, Yang H, Fang X, et al. A clinical study on the association of sodium-glucose cotransporter 2 inhibitors and acute kidney injury among diabetic chinese population. Diabetes Metab Syndr Obes. 2021;14:1621–30.
Zhao M, Sun S, Huang Z, Wang T, Tang H. Network meta-analysis of novel glucose-lowering drugs on risk of acute kidney injury. Clin J Am Soc Nephrol. 2020;16(1):70–8.
Yu B, Dong C, Hu Z, Liu B. Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on renal outcomes in patients with type 2 diabetes mellitus and chronic kidney disease: a protocol for systematic review and meta-analysis. Medicine. 2021;100(8): e24655.
Horii T, Oikawa Y, Kunisada N, Shimada A, Atsuda K. Acute kidney injury in Japanese type 2 diabetes patients receiving sodium-glucose cotransporter 2 inhibitors: a nationwide cohort study. J Diabetes Investig. 2022;13(1):42–6.
Szalat A, Perlman A, Muszkat M, Khamaisi M, Abassi Z, Heyman SN. Can SGLT2 inhibitors cause acute renal failure? plausible role for altered glomerular hemodynamics and medullary hypoxia. Drug Saf. 2018;41(3):239–52.
Tönjes A, Kovacs P. SGLT2: a potential target for the pharmacogenetics of type 2 diabetes? Pharmacogenomics. 2013;14(7):825–33.
Rathmann W, Bongaerts B. Pharmacogenetics of novel glucose-lowering drugs. Diabetologia. 2021;64(6):1201–12.
Katzmann JL, Mason AM, März W, et al. Genetic variation in sodium-glucose cotransporter 2 and heart failure. Clin Pharmacol Ther. 2021;110(1):149–58.
Enigk U, Breitfeld J, Schleinitz D, et al. Role of genetic variation in the human sodium-glucose cotransporter 2 gene (SGLT2) in glucose homeostasis. Pharmacogenomics. 2011;12(8):1119–26.
Drexel H, Leiherer A, Saely CH, et al. Are SGLT2 polymorphisms linked to diabetes mellitus and cardiovascular disease? Prospective study and meta-analysis. Biosci Rep. 2019;39(8):BSR20190299.
Zimdahl H, Haupt A, Brendel M, et al. Influence of common polymorphisms in the SLC5A2 gene on metabolic traits in subjects at increased risk of diabetes and on response to empagliflozin treatment in patients with diabetes. Pharmacogenet Genom. 2017;27(4):135–42.
Pereira MJ, Lundkvist P, Kamble PG, et al. A randomized controlled trial of dapagliflozin plus once-weekly exenatide versus placebo in individuals with obesity and without diabetes: metabolic effects and markers associated with bodyweight loss. Diabetes Ther. 2018;9(4):1511–32.
Francke S, Mamidi RN, Solanki B, et al. In vitro metabolism of canagliflozin in human liver, kidney, intestine microsomes, and recombinant uridine diphosphate glucuronosyltransferases (UGT) and the effect of genetic variability of UGT enzymes on the pharmacokinetics of canagliflozin in humans. J Clin Pharmacol. 2015;55(9):1061–72.
Hoeben E, De Winter W, Neyens M, Devineni D, Vermeulen A, Dunne A. Population pharmacokinetic modeling of canagliflozin in healthy volunteers and patients with type 2 diabetes mellitus. Clin Pharmacokinet. 2016;55(2):209–23.
Marshall JC, Liang Y, Sahasrabudhe V, et al. Meta-analysis of noncompartmental pharmacokinetic parameters of ertugliflozin to evaluate dose proportionality and UGT1A9 polymorphism effect on exposure. J Clin Pharmacol. 2021;61(9):1220–31.
Mitsche MA, Hobbs HH, Cohen JC. Patatin-like phospholipase domain–containing protein 3 promotes transfer of essential fatty acids from triglycerides to phospholipids in hepatic lipid droplets. J Biol Chem. 2018;293(18):6958–68.
Eriksson JW, Lundkvist P, Jansson PA, et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: a double-blind randomised placebo-controlled study. Diabetologia. 2018;61(9):1923–34.
Acknowledgements
Not applicable.
Funding
This study was supported by the NSFC (82003872), Natural Science Foundation of Hunan Province (No. 2020JJ5513), Scientific research Fund of hunan provincial education department (No. 19A418), Scientific Research Fund Project of Hunan Provincial Health Commission (No. 20201973), Central government funds for guiding local scientific and Technological Development (2021QZY016), Hunan Province Clinical Medical Technology Innovation Guidance Project (2020SK51823), Postgraduate Scientific Research Innovation Project of Hunan Province (CX20210974).
Author information
Authors and Affiliations
Contributions
BX and SL completed the preparation of the manuscript and provided the tables. All authors provided revisions and reviewed the manuscript. Jiecan Zhou provided topics and ideas. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, B., Li, S., Kang, B. et al. The current role of sodium-glucose cotransporter 2 inhibitors in type 2 diabetes mellitus management. Cardiovasc Diabetol 21, 83 (2022). https://doi.org/10.1186/s12933-022-01512-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-022-01512-w