
Abstract
Background
Spirometric small airways obstruction (SAO) is common in the general population. Whether spirometric SAO is associated with respiratory symptoms, cardiometabolic diseases, and quality of life (QoL) is unknown.
Methods
Using data from the Burden of Obstructive Lung Disease study (N = 21,594), we defined spirometric SAO as the mean forced expiratory flow rate between 25 and 75% of the FVC (FEF25-75) less than the lower limit of normal (LLN) or the forced expiratory volume in 3 s to FVC ratio (FEV3/FVC) less than the LLN. We analysed data on respiratory symptoms, cardiometabolic diseases, and QoL collected using standardised questionnaires. We assessed the associations with spirometric SAO using multivariable regression models, and pooled site estimates using random effects meta-analysis. We conducted identical analyses for isolated spirometric SAO (i.e. with FEV1/FVC ≥ LLN).
Results
Almost a fifth of the participants had spirometric SAO (19% for FEF25-75; 17% for FEV3/FVC). Using FEF25-75, spirometric SAO was associated with dyspnoea (OR = 2.16, 95% CI 1.77–2.70), chronic cough (OR = 2.56, 95% CI 2.08–3.15), chronic phlegm (OR = 2.29, 95% CI 1.77–4.05), wheeze (OR = 2.87, 95% CI 2.50–3.40) and cardiovascular disease (OR = 1.30, 95% CI 1.11–1.52), but not hypertension or diabetes. Spirometric SAO was associated with worse physical and mental QoL. These associations were similar for FEV3/FVC. Isolated spirometric SAO (10% for FEF25-75; 6% for FEV3/FVC), was also associated with respiratory symptoms and cardiovascular disease.
Conclusion
Spirometric SAO is associated with respiratory symptoms, cardiovascular disease, and QoL. Consideration should be given to the measurement of FEF25-75 and FEV3/FVC, in addition to traditional spirometry parameters.
Similar content being viewed by others


Introduction
Spirometric small airways obstruction (SAO) is characterised by an airflow limitation through the mid to late portion of a maximal forced expiratory manoeuvre. It is most commonly defined by an abnormality in either the mean forced expiratory flow rate between 25 and 75% of the forced vital capacity (FEF25-75) or the forced expiratory volume in 3 s to forced vital capacity ratio (FEV3/FVC) [1]. Despite uncertainty as to its sensitivity and specificity [2], spirometric SAO is often used as a proxy for small airways disease, suggesting the presence of airflow limitation through airways of less than 2 mm diameter [3]. The small airways are integral in the pathophysiology of obstructive lung diseases such as asthma and chronic obstructive pulmonary disease (COPD), where inflammation, mucus hypersecretion, and airway remodelling are associated with increased respiratory symptoms, cardiometabolic complications, and reduced quality of life (QoL) [4,5,6]. Whether these associations are also seen with spirometric SAO in the general population, particularly in the absence of established lung disease is unknown.
Few studies have investigated spirometric SAO in general populations. Prevalence estimates range from 7.5% to 45.9%, influenced by the choice of spirometry parameter and world region [1]. Risk factors include active and passive smoking, low body mass index (BMI), increasing age, low education level, occupational exposure to dust, previous TB, and family history of COPD [7, 8]. There is now an increasing interest in understanding isolated spirometric SAO, which is characterised by the presence of spirometric SAO in the absence of established airflow limitation (i.e. with FEV1/FVC ≥ LLN). The reason for this is that some studies have reported an association between isolated spirometric SAO and early lung injury, including gas trapping and reduced diffusing capacity on lung function testing [9], as well as functional small airways disease and emphysema on quantitative chest CT [10,11,12]. There are also data suggesting that those with isolated spirometric SAO may be at increased risk of developing COPD [13].
As COPD has been associated with respiratory symptoms, cardiometabolic diseases and reduced QoL, it is reasonable to hypothesise that spirometric SAO may hold similar associations. However, current evidence is only available in ever smokers and not representative of the general population [11, 13]. With this in mind, we investigated these associations using data from the multinational Burden of Obstructive Lung Disease (BOLD) study and compared the findings for two different spirometry parameters.
Methods
Study design and participants
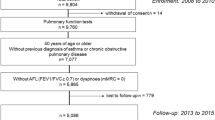
The design and rationale for the BOLD study have been previously published [14]. Non-institutionalised adults ≥ 40 years of age were recruited from 41 sites, across 34 countries, where population size was larger than 150,000. Standardised questionnaires were used to collect information on respiratory symptoms, health status, and exposure to potential risk factors. Questionnaires were translated into the local language and administered by trained fieldworkers. Measurements of height and weight were taken. Lung function was assessed before and 15 min after inhalation of 200mcg salbutamol, using the ndd EasyOne Spirometer (ndd Medizintechnik AG, Zurich, Switzerland). Spirometry parameters including the forced expiratory volume in 1 s (FEV1), FVC, FEV3, and FEF25-75 were measured. Spirograms were assigned quality scores based on the American Thoracic Society (ATS) acceptability and reproducibility criteria [15]. Quality was checked centrally, and only tests with back-extrapolated volume < 150 mL, peak expiratory flow time < 120 ms, lasting ≥ 6 s or with end-of-time volume < 40 mL, no artefact affecting the FEV1 or FVC, and with the two best blows within 200 mL of each other were used. A total of 28,604 participants had acceptable spirometry and completed the core questionnaire. Of these, 4573 were excluded as they did not have a measurement for both FEV3/FVC and FEF25-75. A further 2437 were excluded for not having complete information on respiratory symptoms, cardiometabolic diseases and QoL, leaving 21,594 participants for inclusion in the present study. Ethical approval was obtained by each site from the local ethics committee, all sites adhered to local ethics guidelines, and followed good clinical practice. Informed consent was obtained from all participants.
Spirometric small airways obstruction
Due to lack of consensus in the literature [1], we defined spirometric SAO for two different spirometry parameters: (1) pre-bronchodilator FEF25-75 less than the lower limit of normal (LLN); and (2) pre-bronchodilator FEV3/FVC less than the LLN. We also defined airflow obstruction as pre-bronchodilator FEV1/FVC < LLN, and spirometric restriction as FVC < LLN. Additionally, we defined “isolated spirometric SAO” as FEF25-75 or FEV3/FVC less than the LLN with pre-bronchodilator FEV1/FVC equal or greater than the LLN. We used reference equations for European Americans in the third US National Health and Nutrition Examination Survey (NHANES) to calculate the LLN for all parameters [16, 17].
Respiratory symptoms, cardiometabolic diseases, and QoL
Dyspnoea was assessed using the mMRC dyspnoea scale, where participants rated their breathlessness according to 5 grades: Grade 0—dyspnoea only with strenuous exercise; Grade 1—dyspnoea when hurrying on the level or up a slight hill; Grade 2—dyspnoea when walking at own pace on the level; Grade 3—dyspnoea when walking 100 yards or for a few minutes; Grade 4—too short of breath to leave the house or short of breath when dressing or undressing. We generated a binary variable where a grade of 0–1 indicates no/minimal breathlessness, and a grade ≥ 2 indicates significant breathlessness. Presence of chronic cough, chronic phlegm, and wheeze was determined by positive responses to the following questions: (1) “do you cough on most days for as much as 3 months each year?”; (2) “do you bring up phlegm on most days for as much 3 months each year?”; and (3) “have you had wheezing or whistling in the chest at any time in the last 12 months?”.
Information on self-reported, physician-diagnosed cardiometabolic diseases was obtained from the core study questionnaire. For the present analysis, we considered three outcomes: (1) cardiovascular disease (CVD) as the history of either heart disease or stroke; (2) history of hypertension; and (3) history of diabetes.
QoL was assessed using the 12-item short form health survey (SF-12). Separate scores for physical and mental health were generated and used in the analyses. Scores ranged from 0 to 100, with a score of 100 indicating the best QoL [18].
Statistical analysis
To assess the association of respiratory symptoms with spirometric SAO, we used multivariable logistic regression analysis, adjusting for potential confounders [19]: sex, education level (none, primary or middle school, secondary school, and technical/vocational college or university), BMI (underweight < 18.5 kg m−2, normal 18.5–24.9 kg m−2, overweight 25–30 kg m−2 and obese > 30 kg m−2), age (40–49, 50–59, 60–69, ≥ 70 years), smoking status (never, former, current), smoking pack-years (1–5, 6–15, 16–25 or > 25), passive smoking, occupational exposure to dust ≥ 10 years, use of solid fuels for cooking/heating for > 6 months in a lifetime, history of tuberculosis, spirometric restriction and family history of COPD. For dyspnoea only, we added history of CVD into the model.
To assess the association of cardiometabolic diseases with spirometric SAO, we used multivariable logistic regression, adjusting for known cardiovascular risk factors [20,21,22]: sex, education level, BMI, age, smoking status, smoking pack-years and spirometric restriction.
To assess the association of QoL with spirometric SAO, we performed linear regression analysis using continuous proxies for physical and mental health scores. We adjusted for the same potential confounders as in the models for respiratory symptoms with the addition of CVD, hypertension, and diabetes.
We first assessed these associations within each site and then pooled their estimates using random effects meta-analyses [23]. We then repeated these analyses stratifying by sex. We performed sensitivity analyses repeating the analyses: (1) only among never smokers; (2) after excluding participants with both spirometric SAO and FEV1/FVC < LLN (isolated spirometric SAO); and (3) for symptoms and cardiometabolic diseases, using FEF25-75 and FEV3/FVC as continuous variables. For the association with cardiometabolic diseases, we also repeated the analyses among only those with a normal FVC. Heterogeneity was summarised using the I2 statistic. All analyses were performed using Stata 17 (Stata Corp., College Station, TX, USA) and corrected for sampling weights.
Role of the funding source
The funders of the study did not contribute to the study design, data collection, data analysis or writing of the manuscript.
Results
The characteristics of study participants are displayed in Table 1. The mean age of the participants was 54 years, with 51% being female. On average, they were slightly overweight (BMI 26.4 kg/m2), and two thirds had never smoked. Overall, a fifth of participants had spirometric SAO. For FEF25-75, prevalence ranged from 5% in Tartu (Estonia) to 33% in Mysore (India). Using FEV3/FVC, prevalence of spirometric SAO ranged from 5% in Riyadh (Saudi Arabia) to 30% in Salzburg (Austria). Prevalence of isolated spirometric SAO was lower, ranging from 1% in Tartu (Estonia) to 26% in Mysore (India) for FEF25-75, and from 1% in Riyadh (Saudi Arabia) to 14% in Bergen (Norway) for FEV3/FVC (Table 2). Approximately, one in ten participants had airflow obstruction, with a third having spirometric restriction.
The prevalence of respiratory symptoms and cardiometabolic diseases also varied: dyspnoea from 0% in Mysore (India) to 28% in Uitsig and Ravensmead (South Africa); chronic cough from 0% in Ife (Nigeria) to 17% in Lexington (KY, USA); chronic phlegm from 0% in both sites in Malawi to 14% in Lexington (KY, USA); wheeze from 0% in Mysore (India) to 43% in Lexington (KY, USA); CVD from 0% in Gezeira (Sudan), Mysore (India), and Limbe (Cameroon) to 34% in Tartu (Estonia); hypertension from 2% in Ife (Nigeria) to 44% in Lexington (KY, USA); and diabetes from 1% in Ife (Nigeria) to 27% in Riyadh (Saudi Arabia) (Table 1).
Physical QoL scores were lowest (mean 42.1, SD 7.7) in Guangzhou (China) and highest (mean 53.7, SD 4.2) in Blantyre (Malawi). Mental QoL scores were lowest (mean 33.7, SD 7.7) in Adana (Turkey) and highest (mean 58.5, SD 6.4) in Mumbai (India) (Table 1).
Respiratory symptoms and spirometric SAO
Participants with spirometric SAO, based on FEF25-75, were more likely to report dyspnoea (OR = 2.16, 95% CI 1.77–2.70), chronic cough (OR = 2.56, 95% CI 2.08–3.15), chronic phlegm (OR = 2.29, 95% CI 1.77–4.05), and wheeze (OR = 2.87, 95% CI 2.50–3.40) than those without spirometric SAO (Fig. 1a and b; Additional file 1: Table S1). Associations were slightly stronger among males.

Pooled estimates for the effect of spirometric SAO measured using FEV3/FVC (a) and FEF25-75 (b) on respiratory symptoms in the BOLD study. Spirometric SAO: Small airways obstruction. Overall: spirometric SAO defined as FEV3/FVC or FEF25-75 less than the lower limit of normal (LLN). Male/Female: spirometric SAO as FEV3/FVC or FEF25-75 < LLN stratified by sex. Isolated spirometric SAO: FEV3/FVC or FEF25-75 < LLN with FEV1/FVC ≥ LLN. Dyspnoea measured according to mMRC Dyspnoea scale: 0–1 = minimal/no breathlessness, ≥ 2 = significant breathlessness. Chronic cough: cough on most days for 3 months each year. Chronic Phlegm: Phlegm on most days 3 months each year. Wheeze: Wheezing or whistling in the chest at any time in the last 12 months. OR 95% CI: odds ratio with 95% confidence intervals. I2 values of 0%, 25%, 50%, and 75% considered no, low, moderate, and high heterogeneity. Covariates in the adjusted model: sex, education level, body mass index, smoking status, accumulated cigarette pack-years, passive smoking, occupational exposure to dust, use of solid fuels for cooking/heating for > 6 months in a lifetime, reported doctor-diagnosed or history of tuberculosis, spirometric restriction, family history of COPD, and for Dyspnoea addition of CVD. The following sites could not be included in the analysis either due to a low number of participants reporting respiratory symptoms or singularity in the data: Benin (Sémé-Kpodji), Norway (Bergen), Malawi (Blantyre), China (Guangzhou), Germany (Hannover), Cameroon (Limbe), India (Mumbai) (Mysore), Austria (Salzburg), Tunisia (Sousse), Australia (Sydney), Albania (Tirana), Sweden (Uppsala)
Among never smokers, spirometric SAO based on either FEF25-75 or FEV3/FVC was still associated with increased odds of all respiratory symptoms for both parameters (Additional file 1: Table S4). Results for spirometric SAO based on FEV3/FVC were not materially different from these, except when considering only isolated spirometric SAO, which was associated with all respiratory symptoms for FEF25-75 but only wheeze when using FEV3/FVC (Fig. 1a and b). Heterogeneity across sites for the association of spirometric SAO with respiratory symptoms was generally low-moderate. The association of post-bronchodilator spirometric SAO with respiratory symptoms was not materially different from those with pre-bronchodilator spirometric SAO. Overall, respiratory symptoms were associated with FEF25-75 and FEV3/FVC in a dose–response manner (Additional file 1: Tables S6 and S7).
Cardiometabolic diseases and spirometric SAO
Participants with spirometric SAO, based on FEF25-75, were more likely to have CVD (OR = 1.30, 95% CI 1.11–1.52) but less likely to have diabetes (OR = 0.75, 95% CI 0.63, 0.90), as compared to those without spirometric SAO. Overall, spirometric SAO was not associated with a diagnosis of hypertension (OR = 1.07, 95% CI 0.96, 1.20) (Fig. 2a and b; Additional file 1: Table S2). Associations did not differ much by sex. Results for spirometric SAO based on FEV3/FVC were not materially different from these.

Pooled estimates for the effect of spirometric SAO measured using FEV3/FVC (a) and FEF25-75 (b) on cardiometabolic disease in the BOLD study. Spirometric SAO: Small airways obstruction. Overall: spirometric SAO defined as FEV3/FVC or FEF25-75 less than the lower limit of normal (LLN). Male/Female: spirometric SAO as FEV3/FVC or FEF25-75 < LLN stratified by sex. Isolated spirometric SAO: FEV3/FVC or FEF25-75 < LLN with FEV1/FVC ≥ LLN. Cardiovascular disease: self-reported history of heart disease or stroke. OR (95% CI): odds ratio with 95% confidence intervals. I2 values of 0%, 25%, 50%, and 75% considered no, low, moderate, and high heterogeneity. Covariates in the adjusted model: sex, education level, body mass index, smoking status, accumulated cigarette pack-years and spirometric restriction. The following sites could not be included in the analysis either due to a low number of participants reporting co-morbidity or singularity in the data: For CVD; Malawi (Blantyre), Malawi (Chikwawa), Nigeria (Ife), Cameroon (Limbe), India (Mysore), India (Kashmir), Malaysia (Penang), Sudan (Gezeira), Morocco (Fes), China (Guangzhou), Jamaica, Trinidad & Tobago (Port of Spain), Saudi Arabia (Riyadh), and Albania (Tirana). For Hypertension; Benin (Sémé-Kpodji), Malawi (Chikwawa), and Sudan (Gezeira). For diabetes; India (Pune), Malawi (Chikwawa), Morocco (Fes), China (Guangzhou), Nigeria (Ife), Kyrgyzstan (Naryn), Cameroon (Limbe), Philippines (Manilla), India (Mumbai), Malaysia (Penang)
Among never smokers only, spirometric SAO based on FEF25-75 was associated with CVD (OR = 1.45 95% CI 1.15–1.82) but not hypertension (OR = 1.10, 95% CI 0.97–1.25) or diabetes (OR = 0.84, 95% CI 0.69–1.02). Based on FEV3/FVC, spirometric SAO was not associated with any of the three cardiometabolic diseases (Additional file 1: Table S4).
In a sensitivity analysis in which those with low FVC were excluded, spirometric SAO based on FEF25-75 was associated with CVD (OR = 1.38, 95% CI 1.13–1.68) and hypertension (OR = 1.22, 95% CI 1.08–1.39) but not diabetes (OR = 0.86, 95% CI 0.67–1.11). Based on FEV3/FVC, spirometric SAO was not associated with any of the three cardiometabolic diseases (Additional file 1: Table S5).
Isolated spirometric SAO, based on either FEF25-75 or FEV3/FVC, was associated with CVD but not diabetes. The association with hypertension was not concordant between the two parameters used to define isolated spirometric SAO. Heterogeneity across sites was low for all estimates. The association of post-bronchodilator spirometric SAO with comorbidities was not materially different from those with pre-bronchodilator spirometric SAO. CVD was associated with FEF25-75 and FEV3/FVC in a dose–response manner (Additional file 1: Tables S6 and S7).
Quality of life and spirometric SAO
Participants with spirometric SAO, based on FEF25-75, were more likely to show lower physical (β = − 1.18, 95% CI − 1.64 to − 0.72) and mental (β = − 0.76, 95% CI − 1.19 to − 0.33) scores of QoL (Fig. 3a and b; Additional file 1: Table S3).

Pooled estimates for the effect of spirometric SAO measured using FEV3/FVC (a) and FEF25-75 (b) on physical and mental quality of life in the BOLD study. Spirometric SAO: Small airways obstruction. Overall: spirometric SAO defined as FEV3/FVC or FEF25-75 less than the lower limit of normal (LLN). Male/Female: spirometric SAO as FEV3/FVC or FEF25-75 < LLN stratified by sex. Isolated spirometric SAO: FEV3/FVC or FEF25-75 < LLN with FEV1/FVC ≥ LLN. Physical and mental QoL measured using the SF-12 questionnaire. Negative regression coefficient indicates that having SAO is associated with a reduction in SF-12 score in comparison to not having SAO. I2 values of 0%, 25%, 50%, and 75% considered no, low, moderate, and high heterogeneity. Covariates in the adjusted model: sex, education level, body mass index, smoking status, accumulated cigarette pack-years, passive smoking, occupational exposure to dust, use of solid fuels for cooking/heating for > 6 months in a lifetime, reported doctor-diagnosed or history of tuberculosis, spirometric restriction, family history of COPD, CVD, hypertension, and diabetes. Estimates based on the analysis of 31 sites, the following sites could not be included in the analysis either due to low response rate to the questionnaire; Turkey (Adana) and China (Guangzhou) or where QoL was measured using a different tool; Benin (Sémé-Kpodji), Cameroon (Limbe), Jamaica, Kyrgyzstan (Chui), Kyrgyzstan (Naryn), Malaysia (Penang), Pakistan (Karachi), Sri Lanka (Colombo)
The association of QoL, particularly of the physical component, with spirometric SAO was stronger among males than among females. Results for spirometric SAO based on FEV3/FVC were not materially different from these.
When we restricted our analyses to never smokers, lower physical and mental QoL was still associated with spirometric SAO based on either FEF25-75 or FEV3/FVC (Additional file 1: Table S4).
A lower physical score was weakly associated with isolated spirometric SAO based on FEF25-75 (β = − 0.69, 95% CI − 1.35 to − 0.02), but not with isolated spirometric SAO based on FEV3/FVC (β = 0.03, 95% CI − 0.73 to 0.80). There was no evidence of association of mental QoL score with isolated spirometric SAO. Heterogeneity across sites was low to moderate for all estimates. The association of post-bronchodilator spirometric SAO with QoL was not materially different from those with pre-bronchodilator spirometric SAO.
Discussion
In this multinational population-based study of adults, aged 40 years and above, we show that people with spirometric SAO are more likely to report dyspnoea, chronic cough, chronic phlegm, and wheeze. Additionally, they are more likely to have had a diagnosis of cardiovascular disease, but not hypertension or diabetes. A worse quality of life is also associated with spirometric SAO. All these findings are true also for people with spirometric SAO without airflow obstruction, except in terms of quality of life.
Respiratory symptoms
Both obstructive and restrictive lung patterns have been associated with respiratory symptoms [19, 24], therefore our finding of associations between spirometric SAO and increased dyspnoea, chronic cough, chronic phlegm, and wheeze is not surprising. That said, in the present study, we also found associations between isolated spirometric SAO and respiratory symptoms, especially when using FEF25-75. Only two previous studies have reported associations between isolated spirometric SAO and respiratory symptoms. Yee et al. [13] in the SPIROMICS and Dilektasli et al. [11] in the COPDGene cohorts showed associations between isolated spirometric SAO and increased respiratory exacerbations and dyspnoea. However, unlike the BOLD study where never smokers make up a considerable proportion of the study population, these studies only included current or former smokers. Therefore, our study presents the first population-based evidence on the association of respiratory symptoms with spirometric SAO. This supports the hypothesis that spirometric SAO is a precursor to future airflow obstruction [11, 13], presenting an alternative avenue of investigation for clinicians, if traditional measurement indices do not explain the presence of symptoms.
Using FEF25-75, we found that isolated spirometric SAO associates with all respiratory symptoms, while isolated spirometric SAO defined using the FEV3/FVC was only associated with wheeze. A potential explanation for this is that unlike the FEF25-75, the FEV3/FVC also includes the volume expired in the first 25% of expiration. This volume comes predominantly from emptying of the large conducting airways, which are less likely to be impacted in mild disease. Conversely, the FEF25-75 is specific to the average rate of flow through the middle 50% of expiration, and possibly more sensitive to early changes in the small airways.
There are several potential mechanisms by which isolated spirometric SAO may lead to respiratory symptoms. Chronic exposure to inhaled irritants such as cigarette smoke, damages the walls of the small airways, which has been shown to occur even before airflow obstruction becomes evident [11, 13]. Hospital-based studies have shown that individuals with isolated spirometric SAO according to FEV3/FVC have impaired diffusing capacity [9]. Therefore, feelings of dyspnoea could in part be explained by early emphysematous changes [13]. However, we found that spirometric SAO was associated with symptoms independently of cigarette smoking. It has also been shown that FEF25-75 is a sensitive predictor of airways hypersensitivity in asthma [25], so it is plausible that transient exposure to allergic and non-allergic triggers may result in acute and short-lived bouts of respiratory symptoms. While we have access to pre- and post-bronchodilator measurements, we did not investigate this mechanism further as bronchodilator reversibility does not always differentiate between asthma and COPD in population-based studies [26].
Cardiometabolic diseases
In terms of lung function, the FVC appears to have the strongest association with CVD [22]. The association of airflow obstruction with CVD is more ambiguous [27], while for measures of spirometric SAO, evidence is lacking. In this study, spirometric SAO, defined either using FEF25-75 or FEV3/FVC, was associated with CVD but not hypertension or diabetes. Isolated SAO was also associated with CVD for both parameters.
The association was slightly stronger for FEF25-75 than for the FEV3/FVC, which despite adjustment in our multivariate models, could be explained by the correlation between the FEF25-75 and FVC. However, when we excluded participants with low FVC, the magnitude of the association between spirometric SAO based on FEF25-75 and CVD did not materially change, making this explanation less likely. To rule out residual confounding by smoking from the association between CVD and spirometric SAO, we restricted our analysis to never smokers. This dismissed the association of CVD with spirometric SAO based on FEV3/FVC but not with spirometric SAO based on FEF25-75. Our finding that people with isolated spirometric SAO, i.e. in the absence of airflow obstruction, are more likely to have a diagnosis of CVD is interesting. A potential explanation for this is that spirometric SAO upregulates inflammatory processes. Castonzo et al. [28], showed that people with a lower FEF25-75 percent predicted had higher levels of C-reactive protein (CRP), a marker of systemic inflammation associated with increased risk of both heart disease and stroke [29]. However, it is also plausible that reverse causation plays a role, as it has been shown in mice that heart failure causes pulmonary remodelling, oedema, and fibrosis, all of which can impair lung function [30].
We found conflicting associations of hypertension with spirometric SAO, with no significant association for FEV3/FVC, and FEF25-75 associated with increased odds of hypertension in males and those with isolated spirometric SAO only. Few studies have investigated the association between spirometric SAO and hypertension. In a hospital-based study, Birhan et al. [31] compared the spirometry results of 61 hypertensive and 61 normotensive individuals. They found that hypertensive individuals had a significantly lower FEF25-75 compared to normotensive individuals. However, this finding was not adjusted for potential confounders, such as FVC [22].
Like hypertension, we found conflicting associations between spirometric SAO and diabetes. Spirometric SAO defined using FEV3/FVC was not associated with diabetes, whereas spirometric SAO using FEF25-75 was associated with reduced odds of diabetes. A South Korean study of over 17,000 healthy adults found no association between baseline spirometric SAO and risk of diabetes after 6 years [32]. These results are likely more applicable than those of the present study. Firstly, because it is a longitudinal study, better for investigating causality, and secondly, because the HbA1c blood test was used to diagnose diabetes.
The lack of association with two major risk factors for CVD, despite the association of spirometric SAO with CVD in this study, suggests at least two explanations. Either: (1) the mechanism by which spirometric SAO increases the risk of CVD does not act through pathways that increase blood pressure or impair blood glucose regulation, or (2) the association between spirometric SAO and CVD is not real and is confounded by some factor that we were unable to account for.
Quality of life
We found that people with spirometric SAO are more likely to have worse QoL. However, we found no evidence of association of QoL with isolated spirometric SAO. These findings are plausible, as airflow limitation may not be severe enough to impact daily living. Contrary to our results, Dilkektasli et al. [11] reported that isolated spirometric SAO associated with lower QoL. However, their study population was restricted to former and current smokers, who have been shown to have a lower QoL than non-smokers [33]. We also found that the significant association between spirometric SAO and reduced QoL was mainly seen in males and not females. In the context of our results this makes sense, as males with spirometric SAO reported more respiratory symptoms, which have been shown to be independently associated with QoL [34].
Strengths and limitations
Our study has several strengths. First, its large sample size and population-based design makes the results transferable to general populations. Spirometry was conducted by trained and certified technicians using the same protocol and model of spirometer, and lung function data was quality assured centrally with each curve visually inspected. A further strength is the administration of standardised questionnaires, in local languages, across study sites. Our study also has some limitations. The cross-sectional nature of the study precludes assessment of causality. In addition, there were instances of moderate heterogeneity in the association of spirometric SAO with symptoms and QoL. Therefore, caution should be taken when relating our pooled estimates to specific countries or world regions. Further limitations include the lack of a gold standard measure of spirometric SAO, as well as limited reference equations in suitable populations the FEV3/FVC ratio. This restricted our ability to use multi-ethnic reference values, which could have impacted the estimation of prevalence at some sites. However, the NHANES equations have been shown to give similar prevalence estimates for airflow obstruction regardless of race-correction [35], while recent evidence suggests that race-correction may misclassify individuals with underlying disease [36].
Conclusions
The main novelty of our study concerns isolated spirometric SAO. Quanjer et al. [37] recommended against the use of FEF25-75 in the clinical setting as they found little evidence of isolated spirometric SAO in a sample of people with chronic respiratory disease. In contrast with their study, we have found that isolated spirometric SAO is common in general populations and is associated with respiratory symptoms. In addition, we have shown that isolated spirometric SAO has the potential to be used to detect people at risk of cardiovascular disease. Therefore, consideration should be given to the measurement of FEF25-75 and FEV3/FVC in clinical and general populations. Future research should aim to corroborate our findings and investigate whether those with isolated spirometric SAO go on to develop airflow obstruction or cardiovascular disease later in life.
Availability of data and materials
De-identified participant data and questionnaires may be shared, after publication, on a collaborative basis upon reasonable request made to Dr Amaral (a.amaral@imperial.ac.uk). Requesting researchers will be required to submit an analysis plan.
Abbreviations
- BOLD study:
-
Burden of obstructive lung disease study
- COPD:
-
Chronic obstructive pulmonary disease
- CAO:
-
Chronic airflow obstruction
- SAO:
-
Small airways obstruction
- FEF25-75 :
-
Mean forced expiratory flow rate between 25 and 75% of the FVC
- FEV1 :
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- FEV3 :
-
Forced expiratory volume in 3 s
- FEV1/FVC:
-
Forced expiratory volume in 1 s as a ratio of the forced vital capacity
- FEV3/FVC:
-
Forced expiratory volume in 3 s as a ratio of the forced vital capacity
- LLN:
-
Lower limit of normal
- FET25-75 :
-
Forced expiratory time between 25 and 75% of the forced vital capacity
- CI:
-
Confidence interval
- SD:
-
Standard deviation
- WHO:
-
World Health Organisation
- CT:
-
Computed tomography
- Pre-BD:
-
Pre bronchodilator
- Post-BD:
-
Post bronchodilator
- BMI:
-
Body mass index
- ATS:
-
American thoracic society
- QoL:
-
Quality of life
- CVD:
-
Cardiovascular disease
- mMRC:
-
Medical research council questionnaire
References
Knox-Brown B, Mulhern O, Feary J, et al. Spirometry parameters used to define small airways obstruction in population-based studies: systematic review. Respir Res. 2022;23(1):67. https://doi.org/10.1186/s12931-022-01990-2.
Trinkmann F, Watz H, Herth FJF. Why do we still cling to spirometry for assessing small airway function? Eur Respir J. 2020. https://doi.org/10.1183/13993003.01071-2020.
Weibel ER. Morphometry of the human lung. Saint Louis: Elsevier Science & Technology; 1963.
Kraft M, Richardson M, Hallmark B, et al. The role of small airway dysfunction in asthma control and exacerbations: a longitudinal, observational analysis using data from the ATLANTIS study. Lancet Respir Med. 2022. https://doi.org/10.1016/s2213-2600(21)00536-1.
Crisafulli E, Pisi R, Aiello M, et al. Prevalence of small-airway dysfunction among COPD patients with different GOLD stages and its role in the impact of disease. Respiration. 2017;93(1):32–41. https://doi.org/10.1159/000452479.
Schneider C, Bothner U, Jick SS, et al. Chronic obstructive pulmonary disease and the risk of cardiovascular diseases. Eur J Epidemiol. 2010;25(4):253–60. https://doi.org/10.1007/s10654-010-9435-7.
Xiao D, Chen Z, Wu S, et al. Prevalence and risk factors of small airway dysfunction, and association with smoking, in China: findings from a national cross-sectional study. Lancet Respir Med. 2020;8(11):1081–93. https://doi.org/10.1016/s2213-2600(20)30155-7.
Knox-Brown B, Patel J, Potts J, et al. Small airways obstruction and its risk factors in the Burden of Obstructive Lung Disease (BOLD) study: a multinational cross-sectional study. Lancet Glob Health. 2023;11(1):e69–82. https://doi.org/10.1016/s2214-109x(22)00456-9.
Morris ZQ, Coz A, Starosta D. An isolated reduction of the FEV3/FVC ratio is an indicator of mild lung injury. Chest. 2013;144(4):1117–23. https://doi.org/10.1378/chest.12-2816.
Qin S, Yu X, Ma Q, et al. Quantitative CT analysis of small airway remodeling in patients with chronic obstructive pulmonary disease by a new image post-processing system. Int J Chron Obstruct Pulmon Dis. 2021;16:535–44. https://doi.org/10.2147/copd.S295320.
Dilektasli AG, Porszasz J, Casaburi R, et al. A novel spirometric measure identifies mild COPD unidentified by standard criteria. Chest. 2016;150(5):1080–90. https://doi.org/10.1016/j.chest.2016.06.047.
Ronish BE, Couper DJ, Barjaktarevic IZ, et al. Forced expiratory flow at 25%-75% Links COPD physiology to emphysema and disease severity in the SPIROMICS Cohort. Chronic Obstr Pulm Dis. 2022;9(2):111–21. https://doi.org/10.15326/jcopdf.2021.0241.
Yee N, Markovic D, Buhr RG, et al. Significance of FEV(3)/FEV(6) in recognition of early airway disease in smokers at risk of development of COPD: analysis of the SPIROMICS cohort. Chest. 2021. https://doi.org/10.1016/j.chest.2021.10.046.
Buist AS, Vollmer WM, Sullivan SD, et al. The Burden of Obstructive Lung Disease Initiative (BOLD): rationale and design. COPD. 2005;2(2):277–83.
American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995;152(3):1107–36. https://doi.org/10.1164/ajrccm.152.3.7663792.
Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159(1):179–87. https://doi.org/10.1164/ajrccm.159.1.9712108.
Hansen JE, Sun XG, Wasserman K. Discriminating measures and normal values for expiratory obstruction. Chest. 2006;129(2):369–77. https://doi.org/10.1378/chest.129.2.369.
Gandek B, Ware JE, Aaronson NK, et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: results from the IQOLA. Project International Quality of Life Assessment. J Clin Epidemiol. 1998;51(11):1171–8. https://doi.org/10.1016/s0895-4356(98)00109-7.
Grønseth R, Vollmer WM, Hardie JA, et al. Predictors of dyspnoea prevalence: results from the BOLD study. Eur Respir J. 2014;43(6):1610–20. https://doi.org/10.1183/09031936.00036813.
Jousilahti P, Vartiainen E, Tuomilehto J, et al. Sex, age, cardiovascular risk factors, and coronary heart disease: a prospective follow-up study of 14 786 middle-aged men and women in Finland. Circulation. 1999;99(9):1165–72. https://doi.org/10.1161/01.cir.99.9.1165.
Wickrama KA, O’Neal CW, Lott RE. Early community contexts, race/ethnicity and young adult CVD risk factors: the protective role of education. J Community Health. 2012;37(4):781–90. https://doi.org/10.1007/s10900-011-9511-2.
Kulbacka-Ortiz K, Triest FJJ, Franssen FME, et al. Restricted spirometry and cardiometabolic comorbidities: results from the international population based BOLD study. Respir Res. 2022;23(1):34. https://doi.org/10.1186/s12931-022-01939-5.
Hunter JE, Schmidt FL. Fixed effects vs. random effects meta-analysis models: implications for cumulative research knowledge. Int J Select Assess. 2000;8(4):275–92. https://doi.org/10.1111/1468-2389.00156.
Mejza F, Gnatiuc L, Buist AS, et al. Prevalence and burden of chronic bronchitis symptoms: results from the BOLD study. Eur Respir J. 2017. https://doi.org/10.1183/13993003.00621-2017.
Kim Y, Lee H, Chung SJ, et al. The usefulness of FEF(25–75) in predicting airway hyperresponsiveness to Mannitol. J Asthma Allergy. 2021;14:1267–75. https://doi.org/10.2147/jaa.S318502.
Janson C, Malinovschi A, Amaral AFS, et al. Bronchodilator reversibility in asthma and COPD: findings from three large population studies. Eur Respir J. 2019. https://doi.org/10.1183/13993003.00561-2019.
Triest FJJ, Studnicka M, Franssen FME, et al. Airflow obstruction and cardio-metabolic comorbidities. COPD. 2019;16(2):109–17. https://doi.org/10.1080/15412555.2019.1614550.
Costanzo S, Magnacca S, Bonaccio M, et al. Reduced pulmonary function, low-grade inflammation and increased risk of total and cardiovascular mortality in a general adult population: prospective results from the Moli-sani study. Respir Med. 2021;184:106441. https://doi.org/10.1016/j.rmed.2021.106441.
Kaptoge S, Di Angelantonio E, Lowe G, et al. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132–40. https://doi.org/10.1016/s0140-6736(09)61717-7.
Chen Y, Guo H, Xu D, et al. Left ventricular failure produces profound lung remodeling and pulmonary hypertension in mice: heart failure causes severe lung disease. Hypertension. 2012;59(6):1170–8. https://doi.org/10.1161/hypertensionaha.111.186072.
Birhan MM, Abebe Y. Pulmonary function tests in hypertensive patients attending Zewditu Memorial Hospital, Addis Ababa, Ethiopia. Int J Hypertens. 2018;2018:5492680. https://doi.org/10.1155/2018/5492680.
Lee HY, Shin J, Kim H, et al. Association between lung function and new-onset diabetes mellitus in healthy individuals after a 6-year follow-up. Endocrinol Metab (Seoul). 2021;36(6):1254–67. https://doi.org/10.3803/EnM.2021.1249.
García-Quero C, Carreras J, Martínez-Cerón E, et al. Small airway dysfunction impairs quality of life among smokers with no airflow limitation. Arch Bronconeumol (Engl Ed). 2020;56(1):9–17. https://doi.org/10.1016/j.arbres.2019.01.006.
Janson C, Marks G, Buist S, et al. The impact of COPD on health status: findings from the BOLD study. Eur Respir J. 2013;42(6):1472–83. https://doi.org/10.1183/09031936.00153712.
Tilert T, Dillon C, Paulose-Ram R, et al. Estimating the US prevalence of chronic obstructive pulmonary disease using pre- and post-bronchodilator spirometry: the National Health and Nutrition Examination Survey (NHANES) 2007–2010. Respir Res. 2013;14(1):103. https://doi.org/10.1186/1465-9921-14-103.
Ekström M, Mannino D. Research race-specific reference values and lung function impairment, breathlessness and prognosis: analysis of NHANES 2007–2012. Respir Res. 2022;23(1):271. https://doi.org/10.1186/s12931-022-02194-4.
Quanjer PH, Weiner DJ, Pretto JJ, et al. Measurement of FEF25-75% and FEF75% does not contribute to clinical decision making. Eur Respir J. 2014;43(4):1051–8. https://doi.org/10.1183/09031936.00128113.
Acknowledgements
We thank all participants and field workers for their time and effort put into this study.
BOLD (Burden of Obstructive Lung Disease) Collaborative Research Group members: Albania: Hasan Hafizi (principal investigator [PI]), Anila Aliko, Donika Bardhi, Holta Tafa, Natasha Thanasi, Arian Mezini, Alma Teferici, Dafina Todri, Jolanda Nikolla, and Rezarta Kazasi (Tirana University Hospital Shefqet Ndroqi, Albania); Algeria: Hamid Hacene Cherkaski (PI), Amira Bengrait, Tabarek Haddad, Ibtissem Zgaoula, Maamar Ghit, Abdelhamid Roubhia, Soumaya Boudra, Feryal Atoui, Randa Yakoubi, Rachid Benali, Abdelghani Bencheikh, and Nadia Ait-Khaled (Faculte de M edecine Annaba, Service de Epidemiologie et M edecine Preventive, El Hadjar, Algeria); Australia: Christine Jenkins (PI), Guy Marks (PI), Tessa Bird, Paola Espinel, Kate Hardaker, and Brett Toelle (Woolcock Institute of Medical Research, Sydney, Australia); Austria: Michael Studnicka (PI), Torkil Dawes, Bernd Lamprecht, and Lea Schirhofer (Department of Pulmonary Medicine, Paracelsus Medical University, Salzburg, Austria); Bangladesh: Akramul Islam (PI), Syed Masud Ahmed (Co-PI), Shayla Islam, Qazi Shafayetul Islam, Mesbah-Ul-Haque, Tridib Roy Chowdhury, Sukantha Kumar Chatterjee, Dulal Mia, Shyamal Chandra Das, Mizanur Rahman, Nazrul Islam, Shahaz Uddin, Nurul Islam, Luiza Khatun, Monira Parvin, Abdul Awal Khan, and Maidul Islam (James P. Grant School of Public Health, BRAC [Building Resources Across Communities] University, Institute of Global Health, Dhaka, Bangladesh); Benin: Herve Lawin (PI), Arsene Kpangon, Karl Kpossou, Gildas Agodokpessi, Paul Ayelo, and Benjamin Fayomi (Unit of Teaching and Research in Occupational and Environmental Health, University of Abomey Calavi, Cotonou, Benin); Cameroon: Bertrand Mbatchou (PI) and Atongno Humphrey Ashu (Douala General Hospital, Douala, Cameroon); Canada: Wan C. Tan (PI) and Wen Wang (iCapture Center for Cardiovascular and Pulmonary Research, University of British Columbia, Vancouver, BC, Canada); China: NanShan Zhong (PI), Shengming Liu, Jiachun Lu, Pixin Ran, Dali Wang, Jin-ping Zheng, and Yumin Zhou (Guangzhou Institute of Respiratory Health, First Affiliated Hospital of Guangzhou Medical College, Guangzhou, China); Estonia: Rain Jogi (PI), Hendrik Laja, Katrin Ulst, Vappu ~ Zobel, and Toomas-Julius Lill (Lung Clinic, Tartu University Hospital, Tartu, Estonia); Gabon: Ayola Akim Adegnika (PI) (Centre de Recherches Medicale de Lambarene, Lambarene, Gabon); Germany: Tobias Welte (PI), Isabelle Bodemann, Henning Geldmacher, and Alexandra Schweda-Linow (Department of Pneumology, Hannover Medical School and German Center of Lung Research, Hannover, Germany); Iceland: Thorarinn Gislason (PI), Bryndis Benedikdtsdottir, Kristin Jorundsdottir, Lovisa € Gudmundsdottir, Sigrun Gudmundsdottir, and Gunnar Gudmundsson (Department of Allergy, Respiratory Medicine, and Sleep, Landspitali University Hospital, Reykjavik, Iceland); India: Mahesh Rao (PI) (JSS Medical College, Mysuru, India); Parvaiz A. Koul (PI), Sajjad Malik, Nissar A. Hakim, and Umar Hafiz Khan (Sher-i-Kashmir Institute of Medical Sciences, Srinagar, J&K, India); Rohini Chowgule (PI), Vasant Shetye, Jonelle Raphael, Rosel Almeda, Mahesh Tawde, Rafiq Tadvi, Sunil Katkar, Milind Kadam, Rupesh Dhanawade, and Umesh Ghurup (Indian Institute of Environmental Medicine, Mumbai, India); Sanjay Juvekar (PI), Siddhi Hirve, Somnath Sambhudas, Bharat Chaidhary, Meera Tambe, Savita Pingale, Arati Umap, Archana Umap, Nitin Shelar, Sampada Devchakke, Sharda Chaudhary, Suvarna Bondre, Savita Walke, Ashleshsa Gawhane, Anil Sapkal, Rupali Argade, and Vijay Gaikwad (Vadu Health and Demographic Surveillance System, King Edward Memorial Hospital Research Centre Pune, Pune India); Sundeep Salvi (PI), Bill Brashier, Jyoti Londhe, and Sapna Madas (Chest Research Foundation, Pune India); Jamaica: Althea Aquart-Stewart (PI) and Akosua Francia Aikman (University of the West Indies, Kingston, Jamaica); Kyrgyzstan: Talant M. Sooronbaev (PI), Bermet M. Estebesova, Meerim Akmatalieva, Saadat Usenbaeva, Jypara Kydyrova, Eliza Bostonova, Ulan Sheraliev, Nuridin Marajapov, Nurgul Toktogulova, Berik Emilov, Toktogul Azilova, Gulnara Beishekeeva, Nasyikat Dononbaeva, and AijamalTabyshova (Pulmonology and Allergology Department, National Centre of Cardiology and Internal Medicine, Bishkek, Kyrgyzstan); Malawi: Kevin Mortimer (PI), Wezzie Nyapigoti, Ernest Mwangoka, Mayamiko Kambwili, Martha Chipeta, Gloria Banda, Suzgo Mkandawire, and Justice Banda (the Malawi Liverpool Wellcome Trust, Blantyre, Malawi); Malaysia: Li-Cher Loh (PI), Abdul Rashid, and Siti Sholehah (Royal College of Surgeons in Ireland and University College Dublin Malaysia Campus); Morocco: Mohamed C. Benjelloun (PI), Chakib Nejjari, Mohamed Elbiaze, and Karima El Rhazi (Laboratoire d’epid emiologie, Recherche Clinique et Sante Communautaire, F es, Morroco); Netherlands: E. F. M. Wouters and G. J. Wesseling (Maastricht University Medical Center, Maastricht, the Netherlands); Nigeria: Daniel Obaseki (PI), Gregory Erhabor, Olayemi Awopeju, and Olufemi Adewole (Obafemi Awolowo University, Ile-Ife, Nigeria); Norway: Amund Gulsvik (PI), Tina Endresen, and Lene Svendsen (Department of Thoracic Medicine, Institute of Medicine, University of Bergen, Bergen, Norway); Pakistan: Asaad A. Nafees (PI), Muhammad Irfan, Zafar Fatmi, Aysha Zahidie, Natasha Shaukat, and Meesha Iqbal (Aga Khan University, Karachi, Pakistan); Philippines: Luisito F. Idolor (PI), Teresita S. de Guia, Norberto A. Francisco, Camilo C. Roa, Fernando G. Ayuyao, Cecil Z. Tady, Daniel T. Tan, Sylvia Banal-Yang, Vincent M. Balanag, Jr., Maria Teresita N. Reyes, and Renato. B. Dantes (Lung Centre of the Philippines, Philippine General Hospital, Nampicuan and Talugtug, the Philippines); Renato B. Dantes (PI), Lourdes Amarillo, Lakan U. Berratio, Lenora C. Fernandez, Norberto A. Francisco, Gerard S. Garcia, Teresita S. de Guia, Luisito F. Idolor, Sullian S. Naval, Thessa Reyes, Camilo C. Roa, Jr., Ma. Flordeliza Sanchez, and Leander P. Simpao (Philippine College of Chest Physicians, Manila, the Philippines); Poland: Ewa Nizankowska-Mogilnicka (PI), Jakub Frey, Rafal Harat, Filip Mejza, Pawel Nastalek, Andrzej Pajak, Wojciech Skucha, Andrzej Szczeklik, and Magda Twardowska, (Division of Pulmonary Diseases, Department of Medicine, Jagiellonian University School of Medicine, Krakow, Poland); Portugal: Cristina Barbara (PI), F atima Rodrigues, Hermınia Dias, Joao Cardoso, João Almeida, Maria Joao Matos, Paula Simão, Moutinho Santos, and Reis Ferreira (the Portuguese Society of Pneumology, Lisbon, Portugal); Saudi Arabia: M. Al Ghobain (PI), H. Alorainy (PI), E. El-Hamad, M. Al Hajjaj, A. Hashi, R. Dela, R. Fanuncio, E. Doloriel, I. Marciano, and L. Safia (Saudi Thoracic Society, Riyadh, Saudi Arabia); South Africa: Eric Bateman (PI), Anamika Jithoo (PI), Desiree Adams, Edward Barnes, Jasper Freeman, Anton Hayes, Sipho Hlengwa, Christine Johannisen, Mariana Koopman, Innocentia Louw, Ina Ludick, Alta Olckers, Johanna Ryck, and Janita Storbeck, (University of Cape Town Lung Institute, Cape Town, South Africa); Sri Lanka: Kirthi Gunasekera (PI) and Rajitha Wickremasinghe (Medical Research Institute, Central Chest Clinic, Colombo, Sri Lanka); Sudan: Asma Elsony (PI), Hana A. Elsadig, Nada Bakery Osman, Bandar Salah Noory, Monjda Awad Mohamed, Hasab Alrasoul Akasha Ahmed Osman, Namarig Moham ed Elhassan, Abdel Mu‘is El Zain, Marwa Mohamed Mohamaden, Suhaiba Khalifa, Mahmoud Elhadi, Mohand Hassan, and Dalia Abdelmonam (the Epidemiological Laboratory, Khartoum, Sudan); Sweden: Christer Janson (PI), Inga Sif Olafsdottir, Katarina Nisser, Ulrike SpetzNystrom, Gunilla H € agg, and Gun-Marie Lund € (Department of Medical Sciences: Respiratory Medicine and Allergology, Uppsala University, Uppsala, Sweden); Trinidad and Tobago: Terence Seemungal (PI), Fallon Lutchmansingh, and Liane Conyette (University of the West Indies, St. Augustine, Trinidad and Tobago); Tunisia: Imed Harrabi (PI), Myriam Denguezli, Zouhair Tabka, Hager Daldoul, Zaki Boukheroufa, Firas Chouikha, and Wahbi Belhaj Khalifa (University Hospital Farhat Hached, Faculte de M edecine, Sousse, Tunisia); Turkey: Ali Kocabas¸ (PI), Attila Hancioglu, Ismail Hanta, Sedat Kuleci, Ahmet Sinan Turkyilmaz, Sema Umut, and Turgay Unalan (Department of Chest Diseases, Cukurova University School of Medicine, Adana, Turkey); UK: Peter G. J. Burney (PI), Anamika Jithoo, Louisa Gnatiuc, Hadia Azar, Jaymini Patel, Caron Amor, James Potts, Michael Tumilty, Fiona McLean, and Risha Dudhaiya (National Heart and Lung Institute, Imperial College London, London, UK); United States: A. Sonia Buist (PI) (Oregon Health & Science University, Portland, Oregon); Mary Ann McBurnie, William M. Vollmer, and Suzanne Gillespie (Kaiser Permanente Center for Health Research, Portland, Oregon); Sean Sullivan (University of Washington, Seattle, Washington); Todd A. Lee and Kevin B. Weiss (Northwestern University, Chicago, Illinois); Robert L. Jensen and Robert Crapo (Latter Day Saints Hospital, Salt Lake City, Utah); Paul Enright (University of Arizona, Tucson, Arizona); David M. Mannino (PI), John Cain, Rebecca Copeland, Dana Hazen, and Jennifer Methvin (University of Kentucky, Lexington, Kentucky). Additional local support for BOLD clinical sites was provided by: Boehringer Ingelheim China (GuangZhou, China); Turkish Thoracic Society, BoehringerIngelheim, and Pfizer (Adana, Turkey); Altana, AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Merck Sharpe & Dohme, Novartis, Salzburger Gebietskrankenkasse and Salzburg Local Government (Salzburg, Austria); Research for International Tobacco Control, the International Development Research Centre, the South African Medical Research Council, the South African Thoracic Society GlaxoSmithKline Pulmonary Research Fellowship, and the University of Cape Town Lung Institute (Cape Town, South Africa); and Landspıtali-University Hospital-Scientific Fund, GlaxoSmithKline Iceland, and AstraZeneca Iceland (Reykjavik, Iceland); GlaxoSmithKline Pharmaceuticals, Polpharma, Ivax Pharma Poland, AstraZeneca Pharma Poland, ZF Altana Pharma, Pliva Krakow, Adamed, Novartis Poland, Linde Gaz Polska, Lek Polska, Tarchominskie Zakłady Farmaceutyczne Polfa, Starostwo Proszowice, Skanska, Zasada, Agencja Mienia Wojskowego w Krakowie, Telekomunikacja Polska, Biernacki, Biogran, Amplus Bucki, Skrzydlewski, Sotwin, and Agroplon (Cracow, Poland); BoehringerIngelheim, and Pfizer Germany (Hannover, Germany); the Norwegian Ministry of Health’s Foundation for Clinical Research, and Haukeland University Hospital’s Medical Research Foundation for Thoracic Medicine (Bergen, Norway); AstraZeneca, Boehringer-Ingelheim, Pfizer, and GlaxoSmithKline (Vancouver, Canada); Marty Driesler Cancer Project (Lexington, Kentucky); Altana, Boehringer Ingelheim (Phil), GlaxoSmithKline, Pfizer, Philippine College of Chest Physicians, Philippine College of Physicians, and United Laboratories (Phil) (Manila, Philippines); Air Liquide Healthcare P/L, AstraZeneca P/L, Boehringer Ingelheim P/L, GlaxoSmithKline Australia P/L, Pfizer Australia P/L (Sydney, Australia), Department of Health Policy Research Programme, Clement Clarke International (London, UK); Boehringer Ingelheim and Pfizer (Lisbon, Portugal), Swedish Heart and Lung Foundation, The Swedish Association against Heart and Lung Diseases, Glaxo Smith Kline (Uppsala, Sweden), Seed Money Grant (PF20/0512), Aga Khan University, and Chiesi Pakistan (Pvt.) Limited (Karachi, Pakistan).
Funding
NHLI; Wellcome Trust grant (085790/Z/08/Z).
Author information
Authors and Affiliations
Contributions
BKB and AFSA conceived the study. Under the supervision of AFSA, BKB performed data analysis and prepared the initial draft. JPa and JPo assisted with the preparation of the database. BKB, RA, AAS, CB, SB, HHC, MD, ME GEE, FF, MAG, TG, CJ, AK, DM, GM, KM, AAN, DO, SNMP, LCL, AR, SS, TS, MS, WCT, EW, HA, AM, PB, and AFSA provided critical revision of the manuscript during re-drafting. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained by each site from the local ethics committee, all sites adhered to local ethics guidelines, and followed good clinical practice. Written Informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
Outside of the submitted work: DM declares being a consultant to GlaxoSmithKline, AstraZeneca, COPD Foundation. Royalties—Up to Date. Expert Witness-Schlesinger Law Firm. All other authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Table S1. Pooled estimates for the association between spirometric small airways obstruction and respiratory symptoms in the BOLD study. Table S2. Pooled estimates for the association between spirometric small airways obstruction and cardiometabolic diseases in the BOLD study. Table S3. Pooled estimates for the association between spirometric small airways obstruction and physical and mental scores of quality of life (QoL) in the BOLD study. Table S4. Pooled estimates for the association of spirometric small airways obstruction with respiratory symptoms, cardiometabolic diseases and quality of life in never smokers from the BOLD study. Table S5. Pooled estimates for the association between small airways obstruction and cardiometabolic diseases among participants with normal FVC in the BOLD study. Table S6 and S7. Pooled estimates for the association of FEV3/FVC (%) and FEF25–75 (L/s) with respiratory symptoms and cardiometabolic diseases in all participants and those with a normal FEV1/FVC ratio.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Knox-Brown, B., Patel, J., Potts, J. et al. The association of spirometric small airways obstruction with respiratory symptoms, cardiometabolic diseases, and quality of life: results from the Burden of Obstructive Lung Disease (BOLD) study. Respir Res 24, 137 (2023). https://doi.org/10.1186/s12931-023-02450-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-023-02450-1