
Abstract
Background
Data quality is a major challenge for most health institutions and organizations across the globe. The Ghana Health Service, supported by other non-governmental organizations, has instituted various strategies to address and improve data quality issues in regional and district health facilities in Ghana. This study sought to assess routine data quality of Expanded Programme on Immunization, specifically for Penta 1 and Penta 3 vaccines.
Methods
A descriptive cross-sectional study design was used for the study. A simple random sampling method was used to select thirty-four health facilities across seven sub-municipalities. Records from the Expanded Programme on Immunization (EPI) Tally Books and Monthly Vaccination Summary Report were reviewed and compared with data entered into the District Health Information Management System 2 (DHIMS2) software for the period of January to December 2020. The World Health Organization Data quality self-assessment (DQS) tool was used to compare data recorded in the EPI tally books with monthly data from summary reports and DHIMS2. Data accuracy ratio was determined by the data quality assessment tools and STATA version 14.2 was used to run additional analysis. A data discrepancy is when two corresponding data sets don’t match.
Results
The results showed discrepancies between recounted tallies in EPI tally books and summary reports submitted as well as DHIMS2. Verification factor of 97.4% and 99.3% and a discrepancy rate of 2.6 and 0.7 for Penta 1 and Penta 3 respectively were recorded for tallied data and summary reports. A verification factor of 100.5% and 99.9% and a discrepancy of -0.5 and 0.1 respectively for the same antigens were obtained for the summary reports and DHIMS2. Data timeliness was 90.7% and completeness was 100% for both antigens.
Conclusion
The accuracy of Penta 1 and Penta 3 data on EPI in the Upper East Region of Ghana was high. The data availability, timeliness and completeness were also high.
Similar content being viewed by others

Introduction
One of the most appropriate health interventions adopted for preventing and controlling diseases with minimal cost is immunization [1]. The World Health Organization (WHO) launched the Expanded Programme on Immunization (EPI) worldwide vaccination as a public health intervention in 1974 to ensure that all children have access to routinely recommended vaccines [2]. Since the launch of the EPI, the coverage for the various antigens has seen an increase in the indicators that measure them. In Ghana, donor-supported initiatives like Gavi, the Vaccine Alliance, have instituted several strategies to ensure the quality of immunization data which include electronic registers, data quality audit mechanisms and data validation [3]. These initiatives, coupled with specific regional efforts such as the WHO African Region’s EPI strategic plans of action for the periods 2001–2005 and 2006–2009 and the Reaching Every District (RED) approach, as well as the efforts of national EPIs, have seen global coverage with three doses of the diphtheria-tetanus-pertussis vaccine by 12 months of age (DTP3) rise from 5% in 1974 to 85% in 2010 [4]. However, sub-Saharan Africa reached only 77% Pentavalent coverage in 2010. The Ghana Health Service annual report for 2016 reported an increasing trend of the third dose of Penta 3 vaccine. In 2014, the coverage was 95% and this was increased to 99.0% in 2016 [6]. Although this is an acknowledged indicator of EPI performance, it is important to understand other EPI indicators in Africa [4].
There are about fourteen different antigens in the EPI programme and one of which is the Pentavalent vaccine [2]. The pentavalent vaccine is a combination vaccine that includes five components: diphtheria toxoid, tetanus toxoid, inactivated Bordetella pertussis (whole cell or acellular), hepatitis B surface antigen (HBsAg), and Haemophilus influenzae type b (Hib) conjugate vaccine. It may contain preservatives depending on the specific formulation. Pentavalent vaccine has become one of the antigens that measures access and utilization of immunization in Expanded Programme on Immunization in countries across the globe [1]. Pentavalent is an antigen that is given to children at under 5 years beginning from six weeks for first dose and subsequent doses taken at four weeks interval to protect them against five different diseases. For a child to be fully immunized against these diseases, that child must have at least three (3) doses of the antigen in four weeks apart with the first dose at six (6) weeks old.
Bottlenecks to optimal vaccination performances in Ghana varies for regions and may include programmatic bottlenecks at lower health facilities, poor access to immunization services, poor demand to immunization services on the part of the population, and hesitancy to vaccines between sub-populations. Strategies aimed at promptly addressing the challenges of routine immunization coverage must comprise enhancing the structure and data management capacities at the national, sub-national and health facility levels while improving the demand for immunization among population. The role of data in determining accurate vaccine coverage at all levels of the health system cannot be over emphasized [1].
Health service donors, managers, implementers, policy planning, monitoring and evaluators as well as stakeholders require accurate, complete and timely immunization information for decision making and improvement of programmes performance [7]. Monitoring of immunization coverage is an essential aspect of the EPI because it provides information on the progress made in the intervention. Generally, immunization coverage determined through immunization cluster surveys and routine and administrative data. Administrative data which are reports of immunization activities carried out by health care providers [8].
To improve data quality on vaccination, the Ghana Health Services provides an on-going training of health care providers and data managers at the health facilities and management levels. These trainings are usually followed with regular audit activities and programs on immunization data to correct inconsistencies and discrepancies in immunization data. Expanded Programme on Immunization data are always captured at service delivery points such as the health facility (static) Child Welfare Clinics (CWC) and community outreach Child Welfare Clinic (mobile CWC). The data recorded at these service delivery points are organized and analysed at each of the levels for informed decision-making process in the health care system [9].
Administratively, the Ghana Health Service health facilities are organized using regional, metropolitan/ municipal/ districts and sub-districts. The reporting health facility sends aggregated reports to the sub-district health facility which also sends the aggregated reports to district health office not later that the 5th of the next month. However, copies of monthly reports are kept at all levels from facility level to the district level. Also, immunization monitoring charts are displayed at all the levels to monitor the progress of immunization coverage. This monitoring chart shows cumulatively, the number of doses administered as against targets in the district, sub-district and facility in a form of cumulative frequency graph [10].
There are child health record booklets in which each child details as well as vaccinations statuses are recorded. These individual immunization booklets are usually kept by the caregivers or parents of the children. At the service delivery points, there are registers, immunization tally sheets or books, and monthly reports for data capture and these are stored at the health facility. The EPI managers at the district level receive the monthly immunization reports and perform a data quality check in terms of completeness before receiving it. Data entered in the District Health Information Management Systems 2 (DHIMS2) software are then verified and validated before the 15th of the next month for onward submission to the regional level. The EPI manager print hard copies of data from DHIMS 2 for filing at the district level and copies sent to the regional level [11]. Usually, data quality is compromised during tallying at service delivery points, aggregating, recording into the monthly vaccination summary report and entry into the DHIMS 2 as well as reporting to the district level [12].
In most districts and health facilities in Ghana, chances to under report or over report immunization data are quite high. Capturing data in the vaccination tally books, counting of tallies, and transferring data to the reporting template and entry of data into DHIMS 2 software can precipitate a lot of errors, thereby leading to poor immunization data quality [13]. In most cases at the health facility level where services are provided to clients, one may encounter challenges with data management. The health data management support system at the service delivery point is usually weak posing challenges to efficient and effective management in the health service delivery [14]. Most health facilities have challenges in data generation, analysis, storing and use of health data for decision making. Most health facilities present with discrepancies in EPI data usually from tallied data and aggregated data in the Monthly Vaccination Summary reports at the service delivery level and also that which is submitted to the District Health Directorate. For example, in the New Juabeng Municipality in the Ashanti Region of Ghana, a comparison of tallied data and reported data in summary reports recorded over reporting of Penta 1, Penta 3, Measles and Tetanus 2 + doses for January to December 2011. Tallied data for Penta 1, Penta 3, Measles and Tetanus 2 + doses were 2554, 2749, 2194 and 1647 respectively as against data recorded in summary report were 3171, 3146, 2703 and 2798 respectively [15]. The reasons for these differences are not clear and hence warrant being research into as data management could be a reason for these discrepancies. The timely and complete capture of data, collation and transmission is also challenged. Late and incomplete reporting will result in ineffective decision making for the progress of general health of the public. It is expected that by the 5th day of the ensuing month, health facilities must have submitted all monthly aggregated vaccination data to the District Health Management Team for onward processing and submission to the next level. Districts and Municipalities also have up to the 15th of the ensuing month to submit aggregated data to the Regional Health Management Team and further to the National level. There has not been any research conducted to assess the routine data quality on EPI to establish the true state of data quality in the Kassena Nankana Municipality of the Upper East Region of Ghana. This study therefore assessed the timeliness and completeness of data on Expanded Programme on Immunization in the Kassena Nankana Municipality.
Methods
Study area
The Kassena Nankana Municipality lies within the Guinea Savannah woodlands. It is located approximately between latitude 11°10’ and 10°3’ North and longitude 10°1’ West. The Administrative Capital of the Municipality is Navrongo in the Upper East of Ghana. The Municipal Health Administration oversees a total of thirty-eight (38) health facilities made up of one (1) municipal hospital, two (2) health centres and thirty-five (35) Community-bases Health Planning and Services (CHPS) compounds. These health facilities provide health care services to about one hundred and thirty (130) communities in the municipality. All the health facilities in the municipality provide Expanded Programme on Immunization (EPI) services to the people of the municipality on static and outreach bases. [16]. The municipal catchment population for 2020 is estimated at 138,518 with an expected EPI target of 5541 (4%) which is projected from 2010 population and housing census in Ghana. All facilities in the municipality capture data with paper-based (EPI tally books, registers and Monthly Vaccination Report) and electronic (DHIMS 2) system. Hard copies of aggregated reports, registers and tally books are stored in the facility archives at the facility records unit or the Reproductive and Child Health (RCH) Unit.
Study design and population
This study employed a descriptive cross-sectional study design to review data on EPI. The study included all health facilities in the municipality that provided EPI services either in the facility or outreach basis or both for the year 2020. These health facilities were both private and public health facilities that provided EPI services in the Kassena Nankana Municipality. In the Municipality, all health care facilities are basically primary health care facilities that provide outpatient and in-patient health services as well as public health services. The public health unit in these health facilities provide reproductive and child health services for the population they serve. Some of these services include: antenatal care services, delivery services, postnatal care services, family planning services and Immunization services among other. The vaccination services in all health facilities are provided free of charge to any child under 5 years regardless of the ethnicity, race or socio-economic status of their parents. There has not been any evidence of reported charges for immunization services to any beneficiary.
Sampling and sample size
Thirty-four (34) health care facilities were selected for the study. These health care facilities were drawn from the seven (7) sub-municipalities. The health facilities in the Kassena Nankana Municipality are basically primary health care facilities. They include Community-based Health Planning and Services (CHPS) centres, Clinics, Health Centres and Hospitals. This gives a total of thirty-eight (38) health facilities in the municipality located in all the seven (7) sub-municipalities. The municipality has one (1) hospital, two (2) clinics (1 Private), two (2) health centres and thirty-three (33) CHPS compounds.
The study adopted the Yamane’s formula to determine the sample size for the study at 95% confidence interval and a 5% margin of error.
Where ‘n’ is the sample size, ‘N’ is the population size and ‘e’ is the level of precision.
This will give a complete representation of the type of health facility and it will also cover all sub-municipalities so that the inference from the results can be generalized for the entire municipality.
This was achieved by developing a list of all health facilities that provide EPI services in the municipality and assigned codes to all of them. These codes are unique identifiers to the health facilities. The codes were then written on pieces of papers and kept in a cup and shuffled several times that gave each health facility an equal chance of being selected. Simple random sampling without replacement method was used to select thirty-four (34) health facilities out of the thirty-eight (38).
Data collection tools and technique
The study used WHO Data quality self-assessment tool (DQS) to review EPI records from January to December 2020 [17]. Tallied data (recounted data) were compared with the monthly summary report at the facility and also compared with DHIMS 2 report. This was achieved by organizing all vaccination tally sheets, Child Welfare Clinic Registers and Monthly Vaccination Summary Reports for every facility that was visited for the month of January through December 2020. After which the tallies for each month and each antigen were recounted from the vaccination tally sheets/books and documented on the Data Quality Self-assessment tool. This was followed by copying the recorded aggregated data of Penta 1 and Penta 3 on Monthly Vaccination Summary Report to the DQS tool. DHIMS2 data for Penta 1 and Penta 3 were also extracted and transferred on the DQS tools for further analysis.
Observation check list was used to determine the availability of tally sheets/books, Monthly Vaccination Summary Report for each month, data storage system at the health facility and availability of computers for data management. During the process, tallies from EPI tally books were used to compare with summary data at the facility and the municipal health directorate using the observation technique. Tallies in EPI books and summaries collated were observed and verified to check for discrepancies using the DQS data collection tool. Same observational checklists were used to determine whether the name of health facility, date of submission, name and signature of health facility in-charge and data element for Penta 1 and Penta 3 populated on the Monthly Vaccination Summary Reports. If tally sheet of book for the month was available for verification, it is scored one (1) and if it is not available, it is given a score of zero (0) and documented on observational checklist. Same approach was applied to the availability of Monthly Vaccination Summary Report for verification as well as computers and storage devices. The Monthly Vaccination Summary Reports were examined to determine if all data fields including background information about the facility were captured. If the name of the health facility was accurately captured on the report form, it was given a score of one (1) and if it was not captured, it was given a score of zero (0). Same applied to date of report submission and name and signature of the health facility in-charge. Data elements for Penta 1 and Penta 3 were also checked to see if it was written on the report form. In situations where no vaccination was given for a particular month, a zero (0) figure is expected to be written for that particular antigen for that month in the report form. Where no figure is written for that antigen for that month, a zero (0) score is documented on the checklist.
Data processing and analysis
On the aspect of data processing and analysis, DQS tool was used in the data entry, processing and analysis. Data was entered into the DQS tool and this was used to generate the ratio of accuracy (verification factor) and discrepancy rate in each health facility and antigen.
The formula for generating the accuracy ratio and discrepancy rate is as follows;
-
1.
Accuracy Ratio 1(%) = Total Recounted data /Facility Summary Data × 100.
-
2.
Accuracy Ratio 2(%) = Total DHIMS 2 data/Facility Summary sheet Data × 100.
-
3.
% Discrepancy = 100 – Accuracy Ratio.
If an accuracy ratio is less than 100% (< 100%) implies that data is over reported and the accuracy ratio is greater than 100% (> 100%) implies that the data is under reported. An accuracy ratio of 100% implies data is accurate.
The data completeness was assessed by examining the data fields populated on the Monthly Vaccination Reports for each Health facility and each month. These data element on the Monthly Vaccination Summary Reports that were examined include name of the reporting health facility, date of submission, timely submission, and data elements for each antigen and signature of the name health facility heads.
Also, data elements of Penta 1 and Penta 3 populated in the DHIMS2 software and timeliness of data entries were assessed to establish the timeliness and completeness rate of data. Reports that were submitted for entry into DHIMS after 5th of the ensuing month were considered as late reporting and those that were submitted before the 5th were considered as timely reporting. All entries done before 15th of the ensuing month is considered as timely data entry and entries done after 15th is considered late data entry.
Results
Completeness and timeliness of data
Table 1 presents the availability of tally books, Monthly Vaccination Reports sheets, computer, data storage devices and filing systems in health facilities. At least, 408 tally sheets, Monthly Vaccination Summary Reports and Monthly filing system were expected to be seen at the health facilities. All health facilities visited had the Vaccination Tally sheets available for all months; 408 (100%). All expected Monthly Vaccination Summary Reports were also available for review representing 408 (100%). Total availability of report files for Monthly Vaccination Reports seen at the Health Facilities for January to December 2020 was 404 out of 408 representing 99%. GC01 did not have a file for storing Monthly Vaccination Summary Reports for four (4) months. These months were January, February, March and April.
There was an assessment of hard copy storage systems for Vaccination Tally Books and Monthly Vaccination Reports. A total of 408 Monthly vaccination Summary Reports were assessed and out of which 403 were properly stored which represent 98.8%. Two (2) health facilities namely GC01 and NHC could not file the Monthly vaccination tally sheet in the appropriate storage system. GC01 had four (4) tally sheets for four months wrongly filed whereas NHC had tally sheets for one month wrongly filed. A total of 402 Monthly Vaccination Summary Reports were found to be properly filed in the appropriate filing system in the various health facilities representing 98.5%. One (1) health facility had the Monthly Vaccination Summary Reports wrongly filed for six (6) different months. These reports were found to be stored in other files containing different documents.
The availability of designated computers for data management in health facilities had a score of 7 (20.6%). Thus, majority (79.4%) of Health Facilities in the Municipality does not have a designated computer for data management. The facilities with designated computers for data management are the sub-municipal capital health facilities. Focal persons in these health facilities enter data in the DHIMS2 software for other health facilities within their catchment areas. The health facilities with designated computers for data management are WMH, NHC, KHC, MC01, PNC02, VC and WC02. Only one (2.9%) health facility, the Municipal Hospital, had an external drive for storing data and information including vaccination softcopy reports downloaded every month.
Completeness and timeliness of data
Table 2 depicts data completeness for Monthly Vaccination Report for the Kassena Nankana Municipality of the Upper East Region of Ghana. The data completeness was assessed by examining the data fields populated on the Monthly Vaccination Reports for each Health facility and each month. These data element on the Monthly Vaccination Summary Reports that were examined include name of the reporting health facility, date of submission, timely submission, and data elements for each antigen and signature of the name health facility heads.
Also, data elements of Penta 1 and Penta 3 populated in the DHIMS2 software and timeliness of data entries were assessed to establish the timeliness and completeness rate of data.
A total of 408 hard copy reports of Monthly Vaccination Reports were reviewed for all health facilities visited for January to December 2020. After the review, it was realised that 100.0% completeness rate was recorded for the name of health facility capture for all health facilities. Also, 364 (89.2%) of the reports indicated the date of submission of reports for entries at the sub-municipal head facility. About 44 (10.8%) of the reports did not have reporting date on their form templates. Out of the 364 reports that indicated the submission date on the reporting form, 225 (55.1%) were submitted to the designated staff or health information officer on time for entries to be made in the DHIMS2. The remaining 183 (44.9%) were not submitted on time for entries to be done. These reports were submitted after the 5th of the ensuing month which does not conform to the Ghana Health Services Standard Operating Procedure (GHS-SOP) for Data Management.
Out of the 408 hard copies of Monthly Vaccination reports reviewed, all data elements for Penta 1 and Penta 3 antigens were properly populated. This gave a completeness rate for 100.0%. Entries into DHIMS2 were also assessed for completeness of data for Penta 1 and Penta 3 which was 100%. However, 370 (90.7%) were entered on time and 38 (9.3%) we entered into DHIMS2 late. A total of 282 (69.1%) of the reports assessed had the names and signatures of the health facility heads captured on them.
Data accuracy
Data accuracy for Penta 1 and Penta 3 were checked by counting data captured in EPI vaccination tally books or sheets and compared them with data recorded in the Monthly Vaccination Reports to determine the verification factor and also under reporting or over reporting of the antigen. In Table 3, a total of 2730 doses of Penta 1 and 2653 doses of Penta 3 were counted in the EPI vaccination tally books for all health facilities studied. Doses that were recorded in the Monthly Vaccination Reports for Penta 1 were 2802 and that of Penta 3 was 2673. This gave a discrepancy of 2.6 and 0.7 for Penta 1 and Penta 3 respectively. The verification factor for all health facilities studied for Penta 1 was 97.4% and that of Penta 3 was 99.3%. Out of the 34 health facilities studied for data accuracy, 22 health facilities had a 100% accuracy ratio for Penta 1 and Penta 3 giving a percentage of 64.7%. The remaining 12 (35.3%) had accuracy ratio either less or more than 100%. A total of 4 (11.8%) health facilities namely; NHC, KC01, PC01 and NC02 had a verification factor more than 100% for both antigens. The health facilities that recorded less than 100% accuracy ratio for both antigens were 5 (14.7%) included WMH, GC01, YC, GC05 and KC04. Health facilities recording negative discrepancy ratio for both antigens were 4 (11.8%) which are NHC, KC01, PC01 and NC02. A total of 20 (58.8%) had a 0.0 discrepancy ratio for both Penta 1 and Penta 3 and 5 (14.7%) health facilities recorded a positive discrepancy ratio for both antigens. MC01 and GC02 Centres recorded a positive discrepancy ratio for Penta 1 and a negative discrepancy ratio for Penta 3. However, no health care facility recorded a negative discrepancy ratio for Penta 1 only and 2 (5.9%) health facilities recorded a negative ratio for Penta 3 only.
Data accuracy for Penta 1 and Penta 3 from monthly vaccination reports and DHIMS2 data
There was a comparison made between extracted data of Penta 1 and Penta 3 from Monthly Vaccination Reports for January to December 2022 and compared with extracted data of same antigens from DHIMS2 software. A total of 2802 and 2673 doses of Penta 1 and Penta 3 respectfully were counted from the Monthly Vaccination Reports from all 34 health facilities (Table 4). This was compared with the data Penta 1 and Penta 3 doses from DHIMS2 which were 2789 and 2673 respectively. A verification factor of 100.5% was recorded for Penta 1 and 99.9% was recorded for Penta 3 for all 34 health facilities. The discrepancy ratio of -0.5 was recorded for Penta 1 and that of Penta 3 was 0.1. Health facilities that had 100% verification ratios and 0.0 discrepancy rates for both Penta 1 and Penta 3 antigens were 18 (52.9%). Two (2) health facilities recorded a verification factor less than 100% for both antigens representing 5.9%. Also 2 (5.9%) health facilities recorded verification factor of more than a 100% for both antigens. A total of 3 (8.8%) health facilities had a negative discrepancy ratio for both antigens.
Discussion
The key metric for the assessment of data quality is using the Verification Factor (VF) by comparing the reported data on hardcopies or softcopies to that of the source document [18]. The scale measurement for the verification factor is from 0 to 200%. Any value less than 100% is recorded as under reporting, thus the data in the source document is higher than the reported data and any value above 100% is reported as over reporting, thus the reported data is higher than data from the source document. Verification factor of 100% is recorded as accurate, thus the reported data is exact with the data from source document [12].
A user manual on routine data quality published by USAID in page 24 suggests that the acceptable range for data accuracy using the verification factor is 90–110%. [12]. Therefore, using the comparison between data from vaccination tally books/sheets and that of monthly vaccination summary report suggested that all two antigen indicators were within the acceptable range thus, Penta 1 was 97.4% and Penta 3 was 99.3% for tallied data and data recorded in the Monthly Vaccination Summary Reports. Also, comparison between data from Monthly Vaccination Summary Report and that of DHIMS2 data showed a same picture. All two antigens were over reported for tallied data and that of Monthly Vaccination Summary Report even though the verification factors were all within the acceptable range. On the aspect of data from Monthly Vaccination Summary Reports and DHIMS2 data, Penta 1 was under reported whereas Penta 3 was over reported in spite of the verification factor falling within the acceptable range.
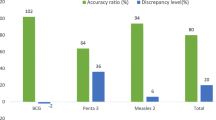
Discrepancies that were recorded were − 21.7%, -21.0% and − 23.8% for Penta 1, Penta 3 and Measles/Rubella 1 respectively. It was also realized that only two (2) out of seven (7) health facilities had accurate data with an accuracy ratio of 100% for Penta 1, Penta 3 and Measles/Rubella 1. The rest of the five (5) health facilities either over reported or under report.
A study conducted in the Kabarole District of Uganda to establish the factors contributing to immunization data quality in forty-nine (49) health care facilities revealed that the average verification factor for all health facilities was 87%. The antigen that was considered and measured for this study was Diphtheria, Pertussis and Tetanus vaccine given to children under one year old in the forty-nine (49) health facilities in the Kabarole District in Uganda. It also established that 65% of health facilities had consistent data and this implies that 35% of the health facilities either under reported or over reported immunization data [19]. This is however different from the case of Kassena Nankana Municipality. Very few health facilities in the Kassena Nankana Municipality under reported and over reported for Penta 1 and Penta 3 vaccines. In general, it was realised that Penta 1 was a little under reported while Penta 3 was also a little over reported. However, this was overall performance of both antigens were within the acceptable range for verification factor for data quality. On the case of Kabarole District of Uganda, the overall verification factor for Diphtheria, Pertussis and Tetanus vaccination is not within the acceptable range for data quality.
In Mozambique, there was an assessment of immunization data quality from routine reports. A total of seven (7) health care facilities were involved in this study and three antigens; BCG, DPT, HepB and Measles were studied. Data was extracted form vaccination tally sheets and compared with health facility monthly reports and the district reports. This study revealed the discrepancy rates for BCG, DPTHepB and Measles for tally sheets and facility reports were 7.2%, 3.2% and 7.7% respectively. The discrepancy rate for health facility reports and district reports for same antigens also revealed 0.4%, -0.5% and 2.9% for BCG, DPThepB and Measles respectively [20]. The result of discrepancy rate facility reports and district reports for measles of this study confirms the situation in Kassena Nankana Municipality. However, the other results prove the opposite even though all were within the WHO accepted range of data quality. This implies that approaches towards achieving data quality in the Kassena Nankana Municipality and Mozambique could be similar and may have similar challenges to data management.
A similar study conducted among Eight (8) health facilities in 2011 in the New Juabeng Municipality in the Ashanti Region of Ghana also revealed that six (6) out of the eight (8) health facilities recorded a discrepancy rate below 5% and two (2) health facilities recorded a discrepancy rate above 25% for Penta 3. This implies that two (2) of the health facilities exceeded the accepted accuracy ratio. In total, 2674 doses of Penta 3 was counted from source document whereas 2824 was counted from summary report at the Municipal Health Directorate giving an accuracy ratio of 105.6% which indicates over reporting [21].
This is consistent with the situation in Kassena Nankana Municipality of the Upper east Region which also recorded over reporting for Penta 1 and Penta 3 doses tallied data in vaccination tally sheets and Monthly Vaccination Summary reports. Also, there was over reporting for Penta 1 for Monthly Vaccination Summary Reports and DHIMS2 which is also consistent with the study in New Juabeng Municipality however, there was under reporting for Penta 3 which proves different.
Another similar study was conducted in the Ho Municipality of the Volta Region of Ghana to assess immunization data quality of routine reports. Three antigens were studied which were Bacillus Calmette Guerin (BCG), Penta 3 and Measles 2. Data was extracted from the Vaccination tally sheets and compared with reported data on the Monthly Vaccination Summary Sheets for three health facilities in the Ho Municipality. The results of the study revealed that BCG was under reported whereas Penta 3 and Measles 2 were over reported. The revelation for Penta 3 in the Ho Municipality is similar to that of Kassena Nankana Municipality [22].
The situation in Suhum, Ho and that of Kassena Nankana Municipality implies that Data management in Ghana needs to be improved as the data is not the exact reflection of the situation prevailing. Knowledge of service providers in reporting forms and data management process could be a factor to the over reporting and under reporting of health data. Also, availability of registers, tally books and reporting templates could be a factor to the over reporting and under reporting of data even though in Kassena Nankana Municipality all health facilities visited did not show any loss or unavailability of reporting tools. In Suhum Municipality of the Eastern Region of Ghana, assessment of the quality of Expended Programme on Immunization data was carried out where primary source data (vaccination tally sheets), Monthly Vaccination Summary Reports and DHIMS2 data was reviewed. This study established that majority (82%) of the Health Facilities in the Municipality had accurate data and the overall verification factor was 105% which is not different from the case of Kassena Nankana Municipality of the Upper East Region [23].
According to the World Health Organization, a data Verification factor for primary sources and reported data between 90% and 110% is deemed acceptable [18]. Concerning this, the data on the Expanded Programme on Immunization for Kassena Nankana Municipality can rated as quality and fit for use. The reason for this level of accuracy could be attributed to staff being trained and frequent on-the-job coaching on the EPI tally books/sheets and the Monthly Vaccination Summary Reports by the EPI coordinator and the Health Information Officer in the Municipality.
Also, there is the possibility that frequent monitoring and supervision as well as data validation exercises are being carried out in the Kassena Nankana Municipality on data management.
The level of accuracy of Penta 1 and Penta 3 data in the Kassena Nankana Municipality is an indication of the fact that the data is fit for purpose and can be used to make informed decisions on immunization. Inaccurate data will inevitably result in an inaccurate decision-making process.
Data completeness refers to whether the right details of information are provided or not [21]. In Table 1, all health facility reports that were assessed had the names of health facilities written on them and all data elements populated. Data extracted from DHIMS 2 met the nationally accepted completeness rate of data for all the health facilities. According to the 2014 Ghana Health Service Standard Operating Procedures (GHS – SOP), the expected target for completeness of data is 95%. A similar study carried out in 2015 in the Greater Accra region on the completeness and accuracy of data transfer of routine maternal health service data found that mean completeness of facility data for aggregated forms was 94.3% and that of DHIMS 2 software was 100% [24]. The data elements that had some incompleteness for the provider reports were patient names, Date of Birth of Patients, Ethnicity of patients, Patient address, provider address and patient number. The data elements that were incomplete for the laboratory reports were the sex of patients and the identification of laboratory tests performed [25]. This study confirms the state of data completeness of data on the monthly vaccination summary reports for the Kassena Nankana Municipality of the Upper East Region of Ghana.
In Vietnam, a similar study was conducted to establish the completeness of mortality data in which the results confirm the completeness level of Penta 1 and Penta 3 for Kassena Nankana Municipality. A total of 1477 identified deaths in 2014 were reviewed in two provinces in Vietnam and about 1365 household Verbal Autopsy (VA) interviews were conducted, which were reviewed by physicians who assigned multiple and Underlying Causes of Death (UCOD). These UCODs from VA were then compared with the CODs recorded in the A6 death registers, using kappa scores to assess the reliability of the A6 death register diagnoses. The study revealed the overall completeness of the A6 death registers in the two provinces was 89.3%. Some data elements were not captured in the A6 death registers which include disease condition, age and sex of the patient [26]. This result is not different from that of Kassena Nankana Municipality where some elements on the monthly vaccination summary reports were not captured.
Conclusion
The findings of this study reveal that the routine data quality of the Kassena Nankana Municipality for the period of January 2020 to December 2020 is good and fit for purpose. The timeliness and completeness indicators measured suggest that all data is populated and on time, which can be used for effective decision-making. The findings did not show any huge data discrepancy between data from tally books or sheets, monthly vaccination summary reports and that of DHIMS 2 software. However, there is a challenge in the timely submission of Monthly Vaccination Summary Reports to the designated staff or health information officers for entries into DHIMS 2 software. Several factors can be attributed to this challenge which may include: little importance attached to data management, inadequate knowledge of data management, and no data validation meetings held at the health facility, sub-municipal and municipal level. In addition, logistics such as computers and storage devices are a challenge to data management in the municipality. This makes data management challenging because there is an inadequate electronic system available to aid in data collection, transmission, analysis and decision-making. Further study should be conducted to find out reasons for high data discrepancy rate between data from monthly vaccination summary report and that of DHIMS 2.
Data availability
Data can be obtained from the corresponding author on reasonable request.
References
WHO. Expanded programme on immunization: national immunization data - EPI summaries by country. Viet Nam, 2015.
World Health Organization. The expanded Programme on Immunization. Immun Vaccines Biol, 2013.
Adeloye D, et al. Coverage and determinants of childhood immunization in Nigeria: a systematic review and meta-analysis. Vaccine. 2017;35(22):2871–81.
Machingaidze S, Wiysonge CS, Hussey GD. Strengthening the expanded Programme on Immunization in Africa: looking beyond 2015. PLoS Med, 10, 3, 2013.
Who T, States M, Form JR. WHO UNICEF Immunization Coverage estimates 2022 revision (released 18 July 2023), 2023.
Sory E. Ghana Health Service Annual Report, no. June, p. 61, 2017.
Eve R, et al. Comprehensive Multi-year Plan for Immunizations. Gazz Med Ital Arch per le Sci Mediche. 2017;2017(2):473–82.
Adokiya MN, Baguune B, Ndago JA. Evaluation of immunization coverage and its associated factors among children 12–23 months of age in Techiman Municipality, Ghana, 2016. Arch Public Heal. 2017;75(1):1–10.
WHO/USAID/University of Oslo. Health facility and community data toolkit. Who/Usaid, p. 54, 2014.
Danovaro C. Immunization Coverage Monitoring Chart: innovative simplicity Vaccination Week in. Immun Newsl Pan Am Heal Organ. 2011;XXXIII(3):1–8.
October H. STANDARD OPERATING PROCEDURES Ministry of Health, 2010.
User Manual Routine Data Quality Assessment. no. October, 2015.
Ley B et al. Analysis of erroneous data entries in paper based and electronic data collection. BMC Res Notes, 12, 1, 2019.
Collins B. Big Data and Health Economics: strengths, weaknesses, opportunities and threats. PharmacoEconomics. 2016;34(2):101–6.
Dominic Asamoah MA. Assessment of Data Quality on expanded Programme on Immunization in Ghana: the case of New Juaben Municipality. J Heal Med Inf, 06, 04, 2015.
Kassena Nankana. Municipal Health Directorate Annual Report for 2020, 2020.
WHO. The immunization data quality self-assessment (DQS) tool, pp. 1–64, 2005.
WHO (World Health Organization.), Data quality review. 2017.
Nsubuga F, Luzze H, Ampeire I, Kasasa S, Toliva OB, Riolexus AA. Factors that affect immunization data quality in Kabarole District, Uganda. PLoS ONE. 2018;13(9):1–11.
Mavimbe JC, Braa J, Bjune G. February, Assessing immunization data quality from routine reports in Mozambique. BMC Public Health, 5, no. 2005.
Mavis Adamki KR. Assessment of Data Quality on expanded Programme on Immunization in Ghana: the case of New Juaben Municipality. J Heal Med Inf, 2015.
Ziema SA, Asem L. Assessment of immunization data quality of routine reports in Ho municipality of Volta region, Ghana. BMC Health Serv Res. 2020;20(1):1–11.
Boakye BT. Assessing the quality of expanded Programme on Immunization (Epi) Data: a Case Study in the Suhum Muncipality of the Eastern Region, no. 10745147, 2019.
Amoakoh-Coleman M, et al. Completeness and accuracy of data transfer of routine maternal health services data in the greater Accra region. BMC Res Notes. 2015;8(1):1–9.
Dixon BE, et al. Completeness and timeliness of notifiable disease reporting: a comparison of laboratory and provider reports submitted to a large county health department. BMC Med Inf Decis Mak. 2017;17(1):1–8.
Hong TT, Hoa NP, Walker SM, Hill PS, Rao C. Completeness and reliability of mortality data in Viet Nam: implications for the national routine health management information system. PLoS ONE. 2018;13(1):1–16.
Acknowledgements
The authors would like to acknowledge all staff of the Kassena Nankana Municipal and Sub-Municipal Health Directorates for supporting the data extraction process.
Funding
This study received no funding support.
Author information
Authors and Affiliations
Contributions
LJP and JOM conceived and designed the study, and JOM performed the data analysis. JOM, LJP, YNA, JK and ASK interpreted the analysis for intellectual content. LJP wrote the draft manuscript. JOM, YNA, JK and ASK edited the manuscript. All authors revised the manuscript, read and approved the final manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Review Committee of the Ghana Health Service (GHS) with reference number GHS-ERC 028/01/22. Permission was sought from the Upper East Regional Health Directorate, the Kassena Nankana Municipal Health Directorate and the health facility management. This study had no human or animal subjects. Any information that was provided in this study was treated with strict confidentiality. All data obtained from health facilities for the study were stored on laptop computer with password protected. All COVID-19 protocols were strictly adhered to during data extraction at the facilities. Participants were not directly involved in the data collection.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Piu, L.J., Owusu-Marfo, J., Agyeman, Y.N. et al. Assessment of expanded programme on immunization routine data quality in the upper east region of Ghana. BMC Health Serv Res 24, 886 (2024). https://doi.org/10.1186/s12913-024-11347-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-024-11347-8